Normal birth after c section
Vaginal birth after cesarean | March of Dimes
If you’ve already had a cesarean birth (also called c-section), you may be able to have your next baby vaginally. This is called vaginal birth after cesarean (also called VBAC).
You may be able to have a VBAC if your pregnancy is healthy and the incision (cut) in your last c-section was low transverse.
VBAC isn’t safe for all women. Talk to your provider to make sure it’s right for you and your baby.
If you are able to have a VBAC, there are some benefits like needing less time to recover and not needing surgery.
Not all providers, hospitals and birthing centers offer VBAC. Talk to your provider to see if VBAC is available where you’re planning to have your baby.
If you’ve already had a cesarean birth (also called c-section), you may be able to have your next baby vaginally. This is called a vaginal birth after cesarean (also called VBAC). Cesarean birth is surgery in which your baby is born through a cut that your health care provider makes in your belly and uterus.
More than 6 to 8 out of 10 women (more than 60-80 percent) who try VBAC are successful in having their baby vaginally. Talk to your health care provider early in your pregnancy to find out if VBAC may be a good choice for you and your baby.
How do you know if having a VBAC is right for you?
Talk to your provider if you’re thinking about having a VBAC. Your provider can help you look at the risks and benefits. If your risks are low and your chances of having a successful VBAC are high, then you may decide that VBAC is right for you.
Your chances of having a successful VBAC are better if:
- You’ve had a vaginal birth before.
- You’ve had just one c-section in the past with a low transverse incision (also called a bikini cut).
- This means the cut was horizontal (side-to-side) and low on the uterus. This is the most common kind of c-section incision. It usually bleeds less than other incisions. It also makes a stronger scar on the uterus, which makes it less likely to tear.

- You and your baby are in good health during pregnancy.
- Your labor starts on its own just before or on your due date.
Your chances of having a successful VBAC are worse if:
- You have the same condition in this pregnancy that made your c-section necessary in a past pregnancy. For example, your baby has problems with his heart rate or is lying sideways in the womb.
- You’re past your due date or your labor is induced.
- You’re obese or you gained excessive weight during pregnancy. If you're obese, you have an excess amount of body fat and your body mass index (also called BMI) is 30 or higher. To find out your BMI, go to www.cdc.gov/bmi.
- You have preeclampsia. This is a condition that can happen after the 20th week of pregnancy or right after pregnancy. It’s when a pregnant woman has high blood pressure and signs that some of her organs, like her kidneys and liver, may not be working properly. Signs of preeclampsia include having protein in the urine, changes in vision and severe headache.
- There’s less than 18 months between your last pregnancy and your current pregnancy (called a short interpregnancy interval).
- Your baby is very large.
- Your provider, hospital or birthing center isn’t prepared to handle an emergency c-section if you need one. Talk to your provider about the level of medical care that’s available in the hospital or birthing center where you plan to have your baby.
- You’re older than 35 or a race other than white.
- Some providers may not offer VBAC if you’ve had more than two past C-sections or if you are pregnant with triplets or a higher number of multiples
It’s not safe to have a VBAC if:
- You had a c-section in the past and your incision was not low transverse and instead was high vertical. A high vertical incision cuts up and down through muscles in the upper part of the uterus that strongly contract during labor. This can lead to a uterine rupture (tear in the uterine muscle).
- You had a uterine rupture in a previous pregnancy.
 This is when the uterus (womb) tears during labor. It happens very rarely.
This is when the uterus (womb) tears during labor. It happens very rarely. - You’ve had certain types of surgery on your uterus.
- You have certain health conditions or complications during pregnancy, like diabetes, heart disease, genital herpes or placenta previa, that make a c-section necessary.
What are the benefits of having a VBAC?
Having a VBAC has some benefits, including:
- There’s no need for surgery.
- Your recovery time is shorter than after having a c-section.
- There’s less blood loss.
- Your risk is lower for infection and other complications, like problems with the placenta called placenta previa and placent acreta.
- If you’re planning to have a lot of children, there’s less risk of complications from repeated surgeries, including scarring or injuries to the bowel or bladder.
- You may want to have the experience of a vaginal delivery.
What are the risks of having a VBAC?
VBAC can have some risks, even if both you and your baby are healthy during pregnancy. These risks include:
These risks include:
- Your labor doesn’t go well and you need a c-section anyway.
- Infection, injury and blood loss
- Your uterus ruptures (tears). This is rare, but it can be life-threatening.
How do I prepare for a VBAC?
- If you previously had a C-section and you’re pregnant, talk to your provider about VBAC at your first prenatal visit.
- You may be able to take a childbirth class on VBAC.
- Be flexible and know that sometimes complications can happen that require needing a C-section. Ask your provider if your hospital of delivery has what it needs in case of an emergency C-section. A home delivery is not appropriate for VBAC. VBAC should take place in a hospital.
See also: Medical reasons for a c-section, Inducing labor, Stages of labor
Last reviewed March 2020
Vaginal Birth After Cesarean Delivery - StatPearls
Patricia J. Habak; Martha Kole.
Author Information
Last Update: July 19, 2022.
Continuing Education Activity
Vaginal birth after cesarean section (VBAC) describes a vaginal delivery in a women who has given birth via cesarean section in a former pregnancy. Patients desiring VBAC delivery undergo a trial of labor (TOL), also called trial of labor after cesarean section (TOLAC). While TOL is an accepted and generally safe practice, serious potential complications include uterine rupture or uterine dehiscence and associated maternal and/or neonatal morbidity. Providers caring for patients with prior cesarean section need to counsel patients regarding potential risks and benefits of TOL and the factors which affect the likelihood of successful vaginal delivery. These providers must be knowledgeable regarding intrapartum management of patients undergoing TOLAC and able to recognize and appropriately manage potential complications. This activity reviews the evaluation and management of patients undergoing vaginal birth after cesarean delivery and highlights the role of interprofessional team members in collaborating to provide well-coordinated care and enhance outcomes for affected patients.
Objectives:
List the potential risks of vaginal birth after cesarean section.
List the potential benefits of vaginal birth after cesarean section.
Describe the factors that influence the outcomes of vaginal birth after cesarean section.
Explain the importance of improving care coordination, with particular emphasis on communication between interprofessional medical teams, to enhance outcomes for patients undergoing vaginal birth after cesarean section.
Access free multiple choice questions on this topic.
Introduction
Vaginal birth after cesarean section (VBAC) is the term applied to women who undergo vaginal delivery following cesarean delivery in a prior pregnancy. Patients desiring VBAC delivery undergo a trial of labor (TOL) or trial of labor after cesarean section (TOLAC). While TOL is an acceptable, generally safe practice, serious, potential complications include uterine rupture or dehiscence with associated maternal and/or neonatal morbidity. Providers caring for patients with prior cesarean section need to be aware of and able to counsel patients regarding risks and benefits of attempting TOL, factors which affect the likelihood of successful vaginal delivery, and knowledgeable regarding intrapartum management of patients undergoing TOLAC.
Providers caring for patients with prior cesarean section need to be aware of and able to counsel patients regarding risks and benefits of attempting TOL, factors which affect the likelihood of successful vaginal delivery, and knowledgeable regarding intrapartum management of patients undergoing TOLAC.
Etiology
As the cesarean delivery rate has increased so has the number of patients becoming pregnant who have experienced cesarean section in a prior pregnancy. Patients may undergo vaginal birth after cesarean section either as a planned procedure or due to precipitant labor.
Epidemiology
Since 1970, the rate of cesarean delivery has increased dramatically from 5% in 1970 to 30% in 2005.[1]The rate of cesarean delivery peaked in 2009 at 32.9% and was 31.9% in 2016.[2] In the early 1970s, when the cesarean delivery rate first began to rise, it was generally felt by medical providers that if a patient had had a cesarean section, she should deliver all future babies by this route. Healthcare professionals began to question the dictum, "once a cesarean, always a cesarean," and subsequently, the number of patients undergoing VBAC delivery began to increase. From the mid-1980s to the mid-1990s, TOLAC was encouraged, and an increase in VBAC delivery was seen along with a concomitant decrease in cesarean delivery rate. Between 1985 and 1995, the VBAC rate increased by over 20% with an associated decrease in cesarean section rates. As VBAC became more common over this time, so did the number of reported significant complications. Such complications and accompanying malpractice suits let to a decrease in VBAC.
Healthcare professionals began to question the dictum, "once a cesarean, always a cesarean," and subsequently, the number of patients undergoing VBAC delivery began to increase. From the mid-1980s to the mid-1990s, TOLAC was encouraged, and an increase in VBAC delivery was seen along with a concomitant decrease in cesarean delivery rate. Between 1985 and 1995, the VBAC rate increased by over 20% with an associated decrease in cesarean section rates. As VBAC became more common over this time, so did the number of reported significant complications. Such complications and accompanying malpractice suits let to a decrease in VBAC.
Complications in patients undergoing TOLAC can occur; however, appropriately selected patients can benefit from attempting a vaginal delivery in the appropriate setting. When successful, VBAC is associated with a decrease in maternal morbidity and decreased risk of complications in future pregnancies. Patients who have undergone successful VBAC benefit from the avoidance of surgical recovery in the postpartum period. Increase in VBAC deliveries also will serve to decrease the overall cesarean delivery rate. More recently it is recognized that as the number of cesarean sections a patient undergoes increases so does the risk of significant obstetrical complications. These complications include massive postpartum hemorrhage, placenta previa, and related placental disorders. [3]By avoiding multiple cesarean deliveries, patients planning large families may particularly stand to benefit from undergoing vaginal birth after cesarean section.
Increase in VBAC deliveries also will serve to decrease the overall cesarean delivery rate. More recently it is recognized that as the number of cesarean sections a patient undergoes increases so does the risk of significant obstetrical complications. These complications include massive postpartum hemorrhage, placenta previa, and related placental disorders. [3]By avoiding multiple cesarean deliveries, patients planning large families may particularly stand to benefit from undergoing vaginal birth after cesarean section.
History and Physical
All pregnant patients should have a comprehensive history and physical exam at the initial prenatal visit as well as on admission to labor and delivery. History should include a detailed obstetric history consisting of the year of any prior pregnancies, and pregnancy outcome (abortion, ectopic, or delivery). Weight and gestational age of the infant at delivery should be recorded. If patients have had complications with prior pregnancies, this should be noted and pertinent details described. In some cases, it will be beneficial to obtain records from prior prenatal care providers or from the hospital at which the patient delivered her other babies.
In some cases, it will be beneficial to obtain records from prior prenatal care providers or from the hospital at which the patient delivered her other babies.
Concerning mode of delivery, it is important to note if prior babies were delivered vaginally or by cesarean section. For patients experiencing prior operative delivery (either operative vaginal delivery or cesarean section) details about the indications for operative delivery should be noted. Ideally, the operative notes of any prior delivery should be obtained and a copy available in the patient's chart.
General physical exam in a patient with a prior cesarean section is performed. The pelvic exam may include an assessment of clinical pelvimetry which is a series of assessments designed to predict the likelihood of vaginal delivery. While clinical pelvimetry is frequently performed, this assessment has not been found to be highly predicted of successful VBAC or vaginal delivery and should not be used as a sole predictor to determine if a patient can undergo a trial of labor.
For patients planning a trial of labor after cesarean section, a pelvic exam close to term may provide additional guidance regarding delivery planning. Ripening of the cervix (softening and effacement) and low station of the fetal head provide some encouragement that patient may be more likely to enter labor spontaneously. A near-term attempt should be made to estimate the fetal weight either by physical exam or using ultrasonographic assessment. This information should be considered but should not be used singularly to determine if a trial of labor should be attempted, as no methods for determination of fetal birth weight are highly accurate.
Evaluation
Some women will not be candidates for TOLAC. Patients having had prior classical cesarean section or prior incision into the contractile portion of the uterus have higher rates of uterine rupture, and thus, a planned, repeat cesarean section is the recommended mode of delivery. Ideally, operative reports from prior surgeries should be obtained and reviewed for a description of the previous uterine incision. When this is not possible, for example when prior surgery was performed in another country, the patient is considered to have an "unknown scar." Because the vast majority of cesarean sections are performed with a low, transverse, uterine incision, it is reasonable to query the patient about the circumstances surrounding her delivery. If the history does not suggest a scenario in which vertical incision would have been likely, for example, cesarean section performed at 24 weeks when the lower uterine segment is less likely to be developed, it is reasonable to allow TOL. The rate of uterine rupture in this situation has been found to be similar to the rate for patients with prior low transverse cesarean section.[4]
When this is not possible, for example when prior surgery was performed in another country, the patient is considered to have an "unknown scar." Because the vast majority of cesarean sections are performed with a low, transverse, uterine incision, it is reasonable to query the patient about the circumstances surrounding her delivery. If the history does not suggest a scenario in which vertical incision would have been likely, for example, cesarean section performed at 24 weeks when the lower uterine segment is less likely to be developed, it is reasonable to allow TOL. The rate of uterine rupture in this situation has been found to be similar to the rate for patients with prior low transverse cesarean section.[4]
Likewise, the rate of uterine rupture is felt to increase with increasing number of prior cesarean sections. With 1 prior LTCS, the rate of uterine rupture is less than 1%; whereas, the rate is slightly higher with 2 prior cesarean sections at 1% to 2%. Most practitioners consider patients with up to two prior cesarean deliveries to be candiates for TOLAC, this recommendation is also endorsed by the American College of Obstetrics and Gynecology. [4]
[4]
Patients with other conditions involving incision into the upper or contractile portion of the uterus are generally felt not to be candidates for TOLAC as the rate of uterine rupture is unacceptably high in these situations. In addition to prior classical uterine incision such conditions would include prior "T" or "J" type incision at cesarean delivery or prior transmyometrial incisions to resect uterine fibroids or to facilitate open fetal surgery. Patients with a prior history of uterine rupture also have a high rate of uterine rupture and planned repeat cesarean delivery is recommended prior to the onset of labor at approximately 36 to 38 6/7 weeks estimated gestational age.[4]
Facilities offering TOLAC should have the capability to perform an emergency cesarean delivery. While the availability of such resources seems prudent concern has been raised that this requirement limits some patients, such as those living in rural areas, from having the option of vaginal delivery after cesarean section.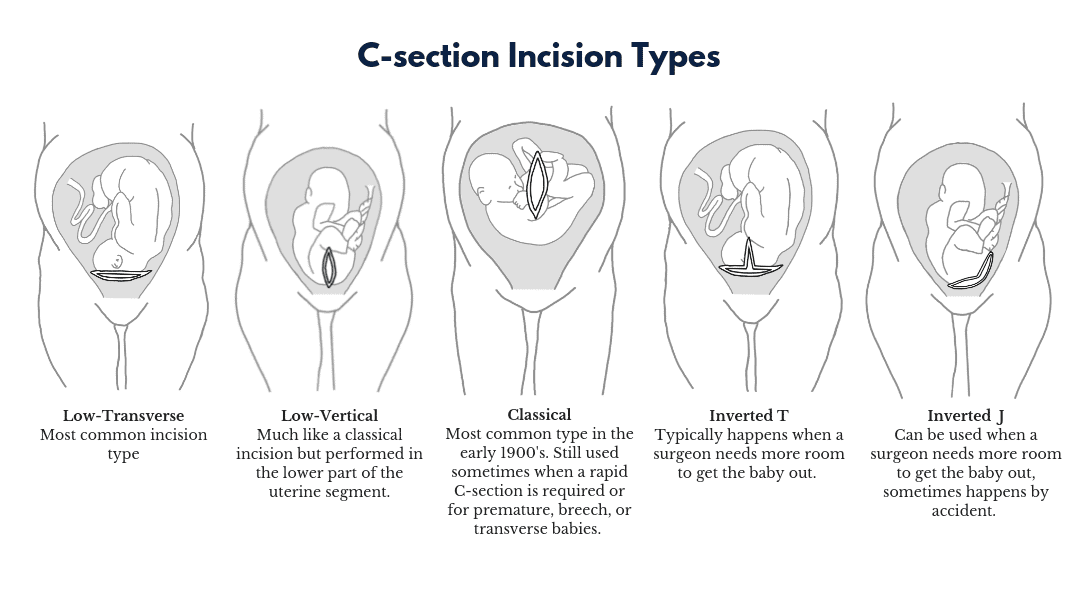 In the most recent ACOG Practice Bulletin on this topic, it was recommended to consider referral of such patients to sites able to offer TOLAC when appropriate. It was also noted that with careful counseling some patients might choose TOLAC even in situations where resources are limited.[4]
In the most recent ACOG Practice Bulletin on this topic, it was recommended to consider referral of such patients to sites able to offer TOLAC when appropriate. It was also noted that with careful counseling some patients might choose TOLAC even in situations where resources are limited.[4]
In considering TOLAC versus PRCD patients may also benefit from counseling regarding liklihood of vaginal delivery. The rate of successful vaginal delivery after a prior cesarean section is found to be 60% to 80%.[1] In general, patients with non-recurring indications for cesarean section, for example, breech presentation, are thought to have higher liklihood of vaginal delivery. Patients with prior vaginal delivery also are found to have higher success rates of vaginal delivery. VBAC caluculators are also available to facilitate estimation of success such as the one developed from Maternal-Fetal Medicine Units Network.[5]
Patiets entering labor spontaneously have higher success rates as well, when compared to women undergoing induction of labor.
Treatment / Management
Patients planning a trial of labor after cesarean section require typical prenatal care with additional counseling regarding the option of TOLAC versus PRCD. Additionally, early ultrasound to confirm gestational age can be helpful if a cesarean section is scheduled.
With regards to labor management, spontaneous entry into labor is preferred as spontaneous labor carries a higher risk of successful vaginal delivery and a lower risk of uterine rupture.[6] Induction of labor remains an option when indicated however use of prostaglandins for cervical ripening as several studies have demonstrated increased risks of uterine rupture when prostaglandins (such as misoprostol or dinoprostone) are used for cervical ripening. In some centers use of low-dose oxytocin and/or mechanical dilation with intracervical balloons is used to facilitate induction in patients undergoing TOLAC with an unripe cervix. Studies of use of mechanical dilators when used in the setting of VBAC are limited and show mixed results. [4]
[4]
While not required, epidural analgesia may be useful in improving patient comfort with the benefit of providing a rapid option for anesthesia if cesarean delivery is required.
Patients should have fetal heart tones monitored closely in labor and attention should be made to appropriate labor progress. Continuous fetal heart rate monitoring is strongly recommended. If concerns arise about possible uterine dehiscence or rupture cesarean delivery should be performed promptly. The most common sign of uterine rupture is an abnormality of the fetal heart rate tracing, which is seen in approximately 70% of cases of uterine rupture. [4]Other findings which may be seen if uterine rupture occurs include increase or decrease in uterine contractions, severe abdominal pain/pain out of proportion for labor, sudden loss of fetal station or finding of blood in the urine or urine collection bag. Even with close and meticulous monitoring uterine rupture can occur suddenly and without warning resulting in fetal compromise, fetal damage or death.
Vaginal delivery, delivery of the placenta and postpartum support is typical for patients undergoing VBAC delivery. Rarely, manual exploration of the uterus following placental delivery may lead to suspicion or discovery of previously undetected dehiscence of the uterine scar. Repair of such a defect is not required unless there is ongoing bleeding. Likewise, patients may experience occult uterine rupture which can lead to bleeding following delivery. VBAC patients experiencing post-delivery hypotension or other signs of hypovolemia should be evaluated promptly with consideration given to the possible diagnosis of uterine rupture.
Differential Diagnosis
Amnionitis
False labour
Malpresentation
Obstruction
Pregnancy, Delivery
Uterine anomaly
Complications
The most significant complication which can occur in patients undergoing TOLAC is uterine rupture which involves the incision made into the uterus at the time of the prior cesarean delivery. Uterine rupture is a medical emergency and patients must be taken immediately for laparotomy for delivery of the fetus and to address and additional complications. When uterine rupture occurs, transfer of blood and oxygen to the baby is interrupted, and this can result in fetal complications including fetal acidosis, a need for neonatal intensive care unit (NICU) admission, and even death. While the absolute risk of perinatal mortality is low with TOLAC, the risk is slightly higher when compared to babies born to mothers undergoing planned repeat cesarean delivery (.13 versus 0.05%).[7]
Uterine rupture is a medical emergency and patients must be taken immediately for laparotomy for delivery of the fetus and to address and additional complications. When uterine rupture occurs, transfer of blood and oxygen to the baby is interrupted, and this can result in fetal complications including fetal acidosis, a need for neonatal intensive care unit (NICU) admission, and even death. While the absolute risk of perinatal mortality is low with TOLAC, the risk is slightly higher when compared to babies born to mothers undergoing planned repeat cesarean delivery (.13 versus 0.05%).[7]
In cases of uterine rupture risk to the mother is also significant. Patients may experience significant hemorrhage. When hemorrhage occurs in this setting transfusion, and sometimes hysterectomy, is necessary to control bleeding and can be life-saving.
Uterine dehiscence is also described. Dehiscence differs from a uterine rupture in that the outer serosal layer of the uterus may remain intact while the underlying muscular layers have opened allowing for visualization of the amniotic sac and fetus. Alternatively, all layers of the uterus may have separated however the fetus remains safe within the uterus thru this small opening. Such a finding is often referred to as a "uterine window." Patients with uterine dehiscence are most often asymptomatic, and the more serious sequela that can occur with uterine rupture are not encountered. When reviewing scholarly articles about uterine scar rupture and dehiscence the distinction between the two is not always clear sometimes making study conclusions difficult to interpret.
Alternatively, all layers of the uterus may have separated however the fetus remains safe within the uterus thru this small opening. Such a finding is often referred to as a "uterine window." Patients with uterine dehiscence are most often asymptomatic, and the more serious sequela that can occur with uterine rupture are not encountered. When reviewing scholarly articles about uterine scar rupture and dehiscence the distinction between the two is not always clear sometimes making study conclusions difficult to interpret.
Some patients attempting TOLAC may require a cesarean delivery. When this occurs after labor, the risks of postpartum infection, uterine atony, and wound separation are higher in comparison to patients who have planned repeat cesarean section.
Enhancing Healthcare Team Outcomes
The management of patients undergoing vaginal delivery after a prior cesarean section is best done with an interprofessional team that includes labor and delivery nurses. An obstetrician should always be present and an operating room with anesthesia stand by must be ready in case a cesarean section is needed. While successful vaginal deliveries have occured following prior cesarean sections, there are ample reports of uterine rupture- hence clinical acumen in decision making is necessary to avoid litigation.
Review Questions
Access free multiple choice questions on this topic.
Comment on this article.
References
- 1.
Scott JR. Vaginal birth after cesarean delivery: a common-sense approach. Obstet Gynecol. 2011 Aug;118(2 Pt 1):342-350. [PubMed: 21775851]
- 2.
Martin JA, Hamilton BE, Osterman MJK. Births in the United States, 2016. NCHS Data Brief. 2017 Sep;(287):1-8. [PubMed: 29155684]
- 3.
Marshall NE, Fu R, Guise JM. Impact of multiple cesarean deliveries on maternal morbidity: a systematic review. Am J Obstet Gynecol. 2011 Sep;205(3):262.e1-8. [PubMed: 22071057]
- 4.
ACOG Practice Bulletin No. 205: Vaginal Birth After Cesarean Delivery. Obstet Gynecol. 2019 Feb;133(2):e110-e127.
[PubMed: 30681543]
- 5.
Grobman WA, Lai Y, Landon MB, Spong CY, Leveno KJ, Rouse DJ, Varner MW, Moawad AH, Caritis SN, Harper M, Wapner RJ, Sorokin Y, Miodovnik M, Carpenter M, O'Sullivan MJ, Sibai BM, Langer O, Thorp JM, Ramin SM, Mercer BM., National Institute of Child Health and Human Development (NICHD) Maternal-Fetal Medicine Units Network (MFMU). Development of a nomogram for prediction of vaginal birth after cesarean delivery. Obstet Gynecol. 2007 Apr;109(4):806-12. [PubMed: 17400840]
- 6.
Guise JM, Eden K, Emeis C, Denman MA, Marshall N, Fu RR, Janik R, Nygren P, Walker M, McDonagh M. Vaginal birth after cesarean: new insights. Evid Rep Technol Assess (Full Rep). 2010 Mar;(191):1-397. [PMC free article: PMC4781304] [PubMed: 20629481]
- 7.
Guise JM, Denman MA, Emeis C, Marshall N, Walker M, Fu R, Janik R, Nygren P, Eden KB, McDonagh M. Vaginal birth after cesarean: new insights on maternal and neonatal outcomes. Obstet Gynecol.
2010 Jun;115(6):1267-1278. [PubMed: 20502300]
Natural childbirth after caesarean section: is it possible? If necessary?
Tells Inga Yurievna Kokaya, obstetrician-gynecologist, PhD, head of the maternity hospital at City Clinical Hospital No. 52 .
“I have a scar on my uterus – will I be able to give birth on my own?”
The possibility of natural childbirth in women who have a scar on the uterus after operative delivery or other operations is a frequently discussed topic among expectant mothers. Modern obstetrics refutes the old stereotypes "one caesarean section - always a second caesarean section." About half of our patients with a history of caesarean section can give birth spontaneously in the absence of absolute medical contraindications to physiological childbirth.
Can everyone expect a natural childbirth?
An informed decision is made in each case. It is strictly individual and is taken on the basis of a competent and thorough analysis of the obstetric-gynecological and general somatic situation, an assessment of risk factors and the benefits of independent childbirth for the mother and fetus. At the same time, it is extremely important for a woman planning pregnancy in the future to know that it is POSSIBLE to give birth herself after a cesarean section. We are always ready to discuss these issues.
It is strictly individual and is taken on the basis of a competent and thorough analysis of the obstetric-gynecological and general somatic situation, an assessment of risk factors and the benefits of independent childbirth for the mother and fetus. At the same time, it is extremely important for a woman planning pregnancy in the future to know that it is POSSIBLE to give birth herself after a cesarean section. We are always ready to discuss these issues.
Cesarean section - only according to indications!
Cesarean sections, both planned and emergency, are performed according to strict indications. Like any abdominal surgery, the operation has a high risk of complications and adverse consequences for women's health and even sometimes for life. Natural childbirth with a scar on the uterus is often a real opportunity to avoid these risks, as well as to live independently with the baby every second of his birth, which is sometimes especially valuable for mothers who have never experienced this.
We motivate for natural childbirth
Our maternity hospital welcomes the conscious decision of the future mother to give birth herself, if it meets the standards of safety for mother and child. We have all the necessary medical and technical resources to make these births safe. We will never take unreasonably high risks and openly tell a woman if we have any doubts that, first of all, her children need a live and healthy mother.
Experienced doctors, modern equipment of each delivery unit with the possibility of continuous cardiac monitoring during childbirth, expanded operating rooms allow, if necessary, to perform an emergency operation by caesarean section in a timely manner already in the process of spontaneous childbirth.
Come and discuss everything!
If you want to discuss with our doctors the possibility of natural childbirth in your situation, we invite you to the Maternity Hospital in advance, starting from the 36th week of pregnancy.
Working hours on weekdays from 8.00 to 15.40, make an appointment by phone +7 (919) 764-68-70 (appointment 8:00 - 15:30), take your passport, CHI policy, SNILS, exchange card and other medical documentation that is relevant to the current pregnancy. Address st. Sosnovaya, 11, LCD building, 4th floor on the left
We will be glad to help you!
Childbirth after caesarean section - Raduga Family Childbirth Center
In medicine, this is called “Vaginal birth in women with a scar on the uterus”. A scar on the uterus can appear as a result of various operations, but we will consider a caesarean section. At present, the attitude towards the need for a second c/s has been revised. In principle, you can give birth yourself, if the reason for which the operation was performed is absent. The reasons might be many, for example, weakness of labor, severe preeclampsia, clinical discrepancy between the size of the child and the mother's pelvis, hypoxia of the child during childbirth, incorrect position of the child (pelvic, with an unfolded head), etc.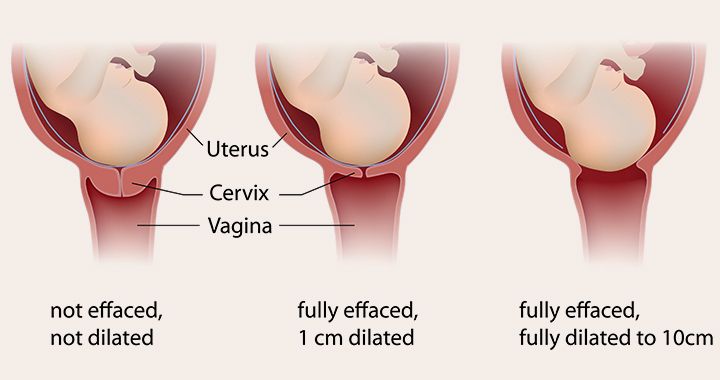 At the next birth, all m.b. normal and only the presence of a scar can alert the doctor, because there is some risk of uterine rupture along the scar. The ideal difference between pregnancies is now considered a break of 2-5 years. Previously, it was considered the opposite, that the difference should be more than 5 years. In order to determine the condition of the scar, it is necessary to do an ultrasound scan at full-term pregnancy (at 38 weeks), when the scar is pulled over the baby's head.
At the next birth, all m.b. normal and only the presence of a scar can alert the doctor, because there is some risk of uterine rupture along the scar. The ideal difference between pregnancies is now considered a break of 2-5 years. Previously, it was considered the opposite, that the difference should be more than 5 years. In order to determine the condition of the scar, it is necessary to do an ultrasound scan at full-term pregnancy (at 38 weeks), when the scar is pulled over the baby's head.
Favorable factors for vaginal delivery with uterine scar:
- Birth interval greater than 24 months (18 in some countries). Better 24+9 months.
- Previous CS at full term
- There was labor activity
- There was no fever in the postoperative period
- There was no large blood loss
- Mom's wish!!!! Family support.
- Estimated fetal weight less than 3700, singleton pregnancy
- One scar on the uterus
- Head presentation
- Timely delivery with spontaneous onset
they cannot be stimulated, they must be carried out very carefully, and after the birth of the placenta, it is sometimes necessary to examine the scar from the inside. This procedure takes 5 minutes and is performed under general anesthesia. Despite the widespread promotion among specialists of the possibility of such childbirth, they are few, less than 30% of women with a scar on the uterus give birth themselves, and then mostly those who did not lie at the antenatal department, examining their scar, but arrived at the r / d already in labor . Therefore, if you want to give birth yourself, which is welcome, you need to look for a doctor who has the appropriate experience. In the West, the percentage of women who give birth on their own is growing all the time and already exceeds 70% in some clinics.
This procedure takes 5 minutes and is performed under general anesthesia. Despite the widespread promotion among specialists of the possibility of such childbirth, they are few, less than 30% of women with a scar on the uterus give birth themselves, and then mostly those who did not lie at the antenatal department, examining their scar, but arrived at the r / d already in labor . Therefore, if you want to give birth yourself, which is welcome, you need to look for a doctor who has the appropriate experience. In the West, the percentage of women who give birth on their own is growing all the time and already exceeds 70% in some clinics.
It should be noted that many psychologists note a state of dissatisfaction and a desire to give birth to a child in a natural way in women who have experienced C/S. Children born as a result of s/s often adapt worse in kindergarten and school. In addition, there is a fundamental difference between children born as a result of a “planned” c / s and emergency, when the mother was in labor for some time.