Miscarriage at 5 weeks do i need to see a doctor
Miscarriage: Signs, Symptoms, Diagnosis, Treatment
Series Miscarriage
Written by WebMD Editorial Contributors
What Are the Treatments for Miscarriage?
The first thing your doctor will try to do is prevent you from having a miscarriage. If the doctor thinks you’re at risk for having one, they may tell you to cut back on activity, including sex, until the signs are gone. Some recommend bed rest, although there’s no scientific evidence it’ll prevent a miscarriage. It can also raise your risk for other health issues. More often than not, there isn’t a lot your doctor can do to stop a miscarriage.
Treatment of a miscarriage, once it starts, depends on your symptoms. The main goal of treatment during and after a miscarriage is to prevent heavy bleeding (they’ll call it hemorrhaging) and infection.
If vaginal bleeding fills more than one super sanitary pad an hour for 2 hours, call your doctor. Heavier bleeding and cramping often indicate that a miscarriage is happening. Most of the time, your body will pass all of the pregnancy-related tissue. The earlier you are in the pregnancy, the more likely your body will complete the miscarriage on its own.
If all of the tissue didn’t come out, a condition known as an incomplete miscarriage, you may need treatment to stop the bleeding and prevent infection. The most common procedure is a dilation and curettage (D&C), which involves widening your cervix and scraping the uterine lining, or endometrium. Sometimes the doctor uses suction along with scraping. This procedure can be uncomfortable, so you’ll probably get general anesthesia to put you to sleep if you need it. Another option is to take medication (misoprostol), which will help your body pass the tissue. Talk to your doctor to figure out what’s right for you.
You may get antibiotics or other medications afterward to slow the bleeding. Let your doctor know if you have any additional vaginal bleeding.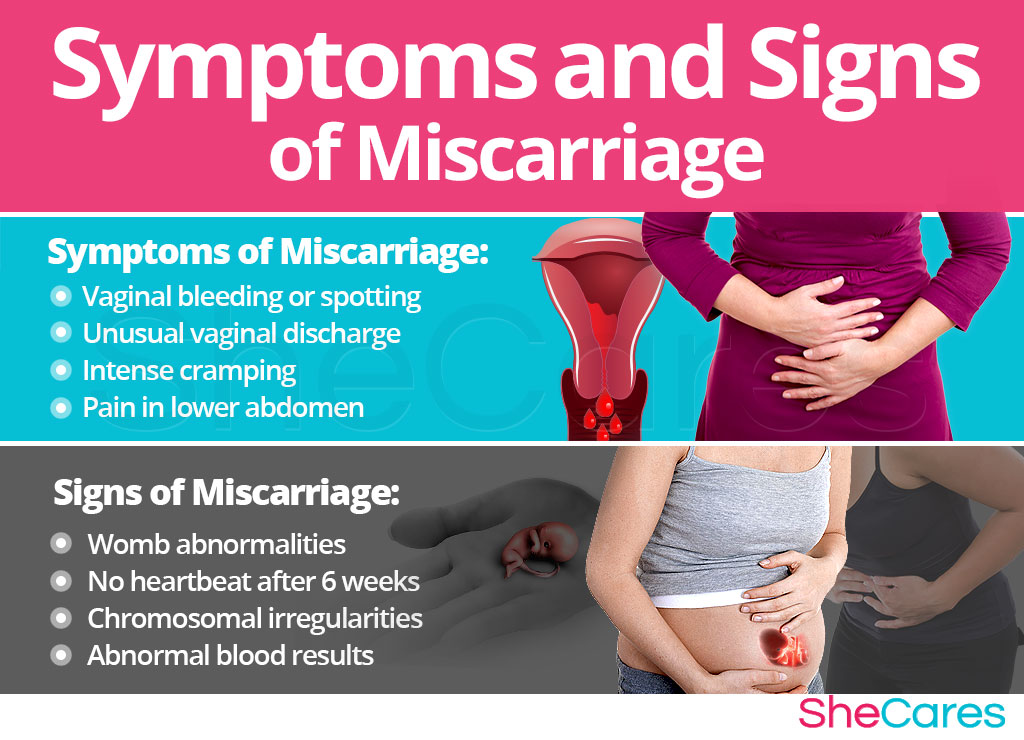 You should also find out whether you have Rh-negative blood. If you do, you’ll probably need a shot of Rh immune globulin to prevent problems in future pregnancies.
You should also find out whether you have Rh-negative blood. If you do, you’ll probably need a shot of Rh immune globulin to prevent problems in future pregnancies.
Call your doctor after a miscarriage if:
You have a fever or chills. Septic (infected) abortions are rare in cases of miscarriage, but a fever or chills could mean you have an infection. The doctor will make sure they remove any remaining pregnancy-related tissue, and you should take antibiotics to prevent serious illness.
Tests After a Miscarriage
Most of the time, chances are good that the next pregancy after a miscarriage will be healthy. But if you have two or more miscarriages in a row, the doctor may suggest tests to find out if there’s a problem that you should treat before you try again. These could include:
Imaging tests. There may be something wrong with the structure of your uterus that’s keeping you from carrying a baby to term.
 The doctor can check for this with an ultrasound, an X-ray or a hysteroscopy.
The doctor can check for this with an ultrasound, an X-ray or a hysteroscopy.Endometrial biopsy. During a hysteroscopy, your doctor may take a small piece of the lining of your uterus to look for abnormal cells.
Genetic tests.Chromosome problems are a common cause of miscarriages. You and your partner may get a karyotype test, which checks your chromosomes for anything unusual.
Blood tests. The doctor may check levels of certain hormones. Blood tests can also reveal risk factors for miscarriage, like diabetes, autoimmune disorders, and blood clotting problems.
Physical Recovery After Miscarriage
It usually doesn’t take long for your body to recover from a miscarriage. You may feel better within a few hours, or it could take a few weeks. Doctors recommend you don’t have sex or put anything in your vagina, like a tampon, for 2 weeks. That’s to lower the chances of an infection. You‘ll probably have your period again in 4-6 weeks.
That’s to lower the chances of an infection. You‘ll probably have your period again in 4-6 weeks.
Emotional Recovery After Miscarriage
It's common to feel sad after losing a pregnancy. Many couples feel the grief of losing a child. This is normal, so allow yourself time to grieve. Consider joining a support group where you can talk about your experience and feelings with others who’ve had a miscarriage. Family and friends may want to comfort you, but may feel like they don't know how. If you can, let them know that you need their support, tell them what they can do, and rely on their help.
Miscarriage can be a physical and emotional challenge for you and your partner. It can put a high amount of stress on your relationship. You may be tempted to blame yourself or your partner for the miscarriage. Don’t. It's highly unlikely either of you did anything to cause the miscarriage or could have done anything to prevent it.
Keep in mind that there is a good chance that you will give birth to a healthy baby in the future. Only about 20% of women who have had a miscarriage have another miscarriage the next time they become pregnant.
Only about 20% of women who have had a miscarriage have another miscarriage the next time they become pregnant.
Although it's possible to become pregnant right after a miscarriage, most experts recommend waiting until after you have had one or two normal menstrual cycles before trying to get pregnant again.
Next In Miscarriage Series:
PreventionEarly miscarriage: what to do and how to cope
In this article
- What is an early miscarriage and how common is it?
- What causes an early miscarriage?
- How will I know if I'm having a miscarriage?
- What should I do if I think I'm having a miscarriage?
- Is there anything I can do to stop the bleeding?
- What happens next?
- How long does the bleeding last after a miscarriage?
- What can I do to recover afterwards?
- More information and support
The loss of a pregnancy can be very difficult to come to terms with. As well as the emotional shock for you and your loved ones, you may find the physical symptoms hard to bear. Here, you'll find information about what may cause a miscarriage and advice on where you can find support.
As well as the emotional shock for you and your loved ones, you may find the physical symptoms hard to bear. Here, you'll find information about what may cause a miscarriage and advice on where you can find support.
What is an early miscarriage and how common is it?
Doctors describe an early miscarriage as one that happens in the first 12 weeks of pregnancy (RCOG 2016a). After 12 weeks, and before 24 weeks of pregnancy, it’s called a late miscarriage.
Sadly, early miscarriages are very common (NICE 2018). Around one in four pregnancies end in miscarriage, with most miscarriages happening in the first 12 weeks of pregnancy (Tommy’s nd). But no matter when in your pregnancy you miscarry, you’re likely to need some support to help you to come to terms with what’s happened.
What causes an early miscarriage?
In most cases, it’s not possible to identify why an early miscarriage has happened. However, chromosomal problems, or other problems with the baby’s development, are thought to be the most common cause (NHS 2018). These problems usually happen during fertilisation. The older a pregnant woman is, the higher the chance of chromosomal abnormalities, although they can happen at any age.
However, chromosomal problems, or other problems with the baby’s development, are thought to be the most common cause (NHS 2018). These problems usually happen during fertilisation. The older a pregnant woman is, the higher the chance of chromosomal abnormalities, although they can happen at any age.
Chromosomal abnormalities can prevent a baby from developing. A baby usually has 23 chromosomes from the mother and 23 chromosomes from the father. Abnormalities may happen when there are too many, or too few, chromosomes (NHS 2018), or because there are changes to a chromosome's structure. When this happens, it can cause miscarriage.
How will I know if I'm having a miscarriage?
Symptoms of early miscarriage will often be bleeding and strong, period-type pains and cramps. The bleeding can vary from brown discharge to bright red, heavy bleeding, including blood clots (MA 2019, NHS 2018).
The bleeding may come and go for a few days or longer. It can be very difficult for you to know what’s going on (MA 2019, MA nd, NHS 2018). The physical process of miscarriage is a distressing experience, and you're bound to feel upset, frightened and helpless.
It can be very difficult for you to know what’s going on (MA 2019, MA nd, NHS 2018). The physical process of miscarriage is a distressing experience, and you're bound to feel upset, frightened and helpless.
However, spotting or light bleeding is common in early pregnancy. It doesn't necessarily mean that a miscarriage is happening. Always call your midwife or GP if you have any bleeding during pregnancy .
What should I do if I think I'm having a miscarriage?
If you're having the symptoms of miscarriage, call your hospital's early pregnancy unit (EPU), if it has one. Check the Association of Early Pregnancy Units (AEPU) to find your nearest EPU.
If there is no EPU near you, call your GP or your hospital's out-of-hours gynaecology service (NICE 2019a, NHS 2018). Medical staff will be able to offer you specific advice over the phone.
If you're less than six weeks pregnant and you’re not experiencing pain that‘s hard to bear, you may be advised to stay at home and keep an eye on your symptoms (NICE 2019a).
If you're a little further along, hospital staff may ask you to come to the hospital for an ultrasound scan or other tests (NICE 2019a, RCOG 2016a). A sonographer will offer to carry out a scan using an ultrasound wand inserted into your vagina. This type of scan gives the best view of your womb (uterus) and is safe. It shouldn't cause you any discomfort.
Scans and tests will check your health and should give you a clear answer about whether or not your pregnancy has been lost (NICE 2019a). Doctors may be able to tell from the scan whether you are having, have had a miscarriage or are likely to have a miscarriage (NICE 2019a). You may need more than one scan to confirm this (NICE 2018, RCOG 2016a).
Afterwards you'll be sent home to rest. Hospital staff may give you a 24-hour telephone number that you or your partner can call at any time, if you have any questions or concerns about what’s happening (NICE 2019a, NICE 2019b, NICE 2018).
Meanwhile, you will need lots of comfort and support from your partner, as well as some practical items to help you through.
You'll need a good supply of super-plus, night-time or maternity-type sanitary towels to absorb any bleeding. Don't use tampons, as they can increase the risk of infection (MA 2019). You may also need painkillers, such as paracetamol. If your doctor or the EPU team have confirmed that you've had a miscarriage, you can take ibuprofen too. Ask your partner or someone else to buy these things for you if you don't have them in.
Hugging a hot water bottle to your tummy may help to ease any cramps. If you can't cope with the strong, cramping pains, call your EPU or doctor and ask about further painkillers.
Is there anything I can do to stop the bleeding?
Unfortunately, once a miscarriage has started, there isn't really anything that you or anyone else can do to stop it (MA nd, RCOG 2016a). If you want to go to bed, or want to carry on with your usual routine, that's fine. Just try to stay as comfortable as you can. Resting in bed is unlikely to make any difference to what is happening (MA nd, McCall et al 2013).
If you want to go to bed, or want to carry on with your usual routine, that's fine. Just try to stay as comfortable as you can. Resting in bed is unlikely to make any difference to what is happening (MA nd, McCall et al 2013).
Lying down may make it feel as though the bleeding is slowing down or stopping. But sadly this is because the blood collects at the top of the vagina and moves down when you get up or go to the toilet (MA nd).
What happens next?
All you can do is give your body time to adjust and get plenty of rest. Hopefully, your partner can be around to comfort you and keep an eye on you.
If the bleeding is not too heavy, or if you're not in pain, you’re fine to rest at home. Keep in touch with your EPU, out-of-hours gynaecology service, or doctor, though, just to let them know what’s happening (NICE 2019a).
If your partner can't be there all the time, perhaps someone else can stay with you or be available to pop round and check on you. That's because, occasionally, pregnancy loss can lead to complications. If you experience any of the following, call the EPU or go straight to accident and emergency (A&E) (MA 2019, NICE 2018):
That's because, occasionally, pregnancy loss can lead to complications. If you experience any of the following, call the EPU or go straight to accident and emergency (A&E) (MA 2019, NICE 2018):
- The bleeding becomes very heavy (soaking more than one maternity-sized pad in an hour), or you feel unwell or faint, and are unable to cope with the bleeding. This means you may be losing too much blood.
- You have one-sided pain or tenderness in your belly, pelvis or in your shoulder tip, feel dizzy, have a fast heartbeat, or have pain when you go to the toilet. These may be signs of an ectopic pregnancy. If you have an ectopic pregnancy, you’ll need treatment quickly, for the benefit of your own health ( NICE 2018, NICE 2019a, NICE 2019b, RCOG 2016b).
- You feel feverish and generally unwell, as if you have flu, have pain in your belly which is getting worse, or your vaginal discharge smells bad. These may be signs of an infection (MA 2019).
How long does the bleeding last after a miscarriage?
The bleeding is likely to tail off in a week to 10 days and will usually have stopped after two weeks (NHS 2018, NICE 2019a, RCOG 2016a). Although a week or two may have passed, you'll still need to take care of yourself as you recover physically and emotionally.
Although a week or two may have passed, you'll still need to take care of yourself as you recover physically and emotionally.
If the bleeding hasn't stopped by two weeks, contact your EPU or doctor (NICE 2019b, RCOG 2016a). Bleeding after this time can still be normal, but a doctor or nurse should check your health (NICE 2019a).
Continued bleeding and pain may mean you have some pregnancy tissues left in your womb. Alternatively, the bleeding could be caused by an infection in your womb lining. In both of these cases, you will need follow-up treatment to get better.
What can I do to recover afterwards?
Whether the miscarriage settles on its own or you need further treatment, you and your partner need to take time to come to terms with what's happened. Even if it happens very early on in pregnancy, don't feel that you can’t grieve.
If you're recovering at home, you may feel up to walking around after a couple of days. You'll probably need at least several days or longer off work, though (MA 2011). See your GP about taking the time as sick leave. Your GP can supply you with a fit note to give to your employer (Sands 2013).
You'll probably need at least several days or longer off work, though (MA 2011). See your GP about taking the time as sick leave. Your GP can supply you with a fit note to give to your employer (Sands 2013).
Your EPU or GP will offer you a follow-up appointment for a check-up if you wish to have one (NICE 2019a, NICE 2018). You may also be offered a follow-up scan to confirm that the miscarriage has completed.
If you were treated in hospital, you may be able to hold a memorial, cremation or burial service after the miscarriage. Hospital staff will explain to you which options are available to you. If you wish, you can sign the hospital's book of remembrance (Titherly 2017).
More information and support
- For more information, see our article on coping with miscarriage.
- You may find comfort from talking to others who've been through a similar experience in our supportive BabyCentre community.
References
Aleman A, Althabe F, Belizán JM, et al. 2005. Bed rest during pregnancy for preventing miscarriage. Cochrane Database Syst Rev. 4: CD003576. www.ncbi.nlm.nih.gov
2005. Bed rest during pregnancy for preventing miscarriage. Cochrane Database Syst Rev. 4: CD003576. www.ncbi.nlm.nih.gov
MA. 2011. Miscarriage and the workplace. A guide for employers. Miscarriage Association.
MA. 2019. Management of miscarriage: your options. Miscarriage Association. www.miscarriageassociation.org.uk
MA. nd. Signs & symptoms Miscarriage Association. www.miscarriageassociation.org.uk
McCall CA, Grimes DA, Lyerly AD. 2013. "Therapeutic" bed rest in pregnancy: unethical and unsupported by data. Obstet Gynecol. 121: 1305-1308. www.ncbi.nlm.nih.gov
NHS. 2018. Miscarriage. NHS, Health A-Z. www.nhs.uk
NICE. 2019a. Ectopic pregnancy and miscarriage: Diagnosis and initial management. National Institute for Health and Care Excellence. NG126. www.nice.org.uk
NICE. 2019b. Ectopic pregnancy and miscarriage: Diagnosis and initial management. Information for the public. National Institute for Health and Care Excellence. NG126. www.nice.org.uk
NG126. www.nice.org.uk
NICE. 2018. Miscarriage. National Institute for Health and Care Excellence. Clinical Knowledge Summaries. cks.nice.org.uk
RCOG. 2016a. Early miscarriage. Information for you. Royal College of Obstetricians and Gynaecologists. www.rcog.org.uk
RCOG. 2016b. Ectopic pregnancy. Information for you. Royal College of Obstetricians and Gynaecologists. www.rcog.org.uk
Sands. 2013. Returning to work after the death of your baby. 3rd ed. Stillbirth & Neonatal Death Charity). www.sands.org.uk Titherly C. 2017. Pregnancy loss and the death of a baby: grief and bereavement care. In: Macdonald S, Johnson G. eds. Mayes’ Midwifery. 15th ed. Edinburgh: Elsevier, 1109-1125.
Tommy’s. nd. Miscarriage statistics. Our research. Tommy’s. www.tommys.org
Show references Hide references
Miscarriage, how to avoid - Planning and management of pregnancy in the gynecology of the Literary Fund polyclinic after a miscarriage
- Gallery
- News
- Blog
- Reviews
- Jobs
- Licenses
- Insurance partners
- Controlling organizations
- Schedule of reception of citizens on personal appeals
- What you need to know about coronavirus infection?
- Rules for patients
- Online doctor's consultation
- to corporative clients
- Documentation
A miscarriage is always associated with severe consequences for the whole body of a woman and for her reproductive organs in particular, it also affects the family situation, disrupts the woman's work schedule. An unfavorable outcome of pregnancy requires great mental and physical costs on the part of parents. Therefore, contacting doctors to find out the causes of the problem is the very first and correct step towards the birth of a child.
An unfavorable outcome of pregnancy requires great mental and physical costs on the part of parents. Therefore, contacting doctors to find out the causes of the problem is the very first and correct step towards the birth of a child.
Any competent gynecologist will tell you that the problem of miscarriage can be solved. With proper preparation for pregnancy and its management, the next time you will have a successful pregnancy. Most girls after a miscarriage go to extremes: they try to get pregnant again as soon as possible. And if this succeeds, then the miscarriage is very often repeated. And you need to give the body a rest for 2-3 months, then identify and eliminate the cause. And only then try.
Causes of miscarriage
Many are convinced that miscarriages are due to a fall, bruise, or some other physical shock. Any woman who has had a miscarriage can remember that not long before she either fell or lifted something heavy. And I am sure that she lost her unborn child precisely because of this. However, those women whose pregnancy was normal also fall and lift heavy things. Most sudden miscarriages do not occur for this reason. The reason is in violations of the pregnancy itself. Approximately half of miscarriages are due to abnormal genetic development of the fetus, which can be hereditary or accidental. Merciful nature, following the principles of natural selection in everything, destroys the defective and unviable fetus. But you should not be afraid of this. The fact that there is a defect in one embryo does not mean at all that all the others will be the same.
However, those women whose pregnancy was normal also fall and lift heavy things. Most sudden miscarriages do not occur for this reason. The reason is in violations of the pregnancy itself. Approximately half of miscarriages are due to abnormal genetic development of the fetus, which can be hereditary or accidental. Merciful nature, following the principles of natural selection in everything, destroys the defective and unviable fetus. But you should not be afraid of this. The fact that there is a defect in one embryo does not mean at all that all the others will be the same.
The woman's body is almost always to blame for the other half of miscarriages. They are caused by various known and unknown factors, such as: acute infectious diseases suffered in the first trimester of pregnancy, poor environment or difficult working conditions, excessive psychological or physical stress, abnormal development of the uterus, radiation, alcohol, smoking and certain types of drugs.
The causes of early and late miscarriage may differ, although they may overlap. The most important thing is to find out and eliminate or compensate for your own cause of miscarriage. Having discovered the cause, the gynecologist will tell you how to avoid another loss.
The most important thing is to find out and eliminate or compensate for your own cause of miscarriage. Having discovered the cause, the gynecologist will tell you how to avoid another loss.
Miscarriage
Miscarriage statistics also include “missed pregnancy”. Sometimes it happens that the embryo dies and lingers in the uterine cavity. Most often, this fact is detected by ultrasound. The dead fetus may begin to decompose, and this, thereby, will lead to poisoning of the mother's body.
Doctors resort to surgical curettage, which is associated with a risk of inflammation and complications. With such a miscarriage, the next pregnancy is planned after the body is fully restored - not earlier than a year. During this year, you will have to find out the cause of the missed pregnancy and treat it.
Miscarriage up to 6 weeks
The main causes of miscarriage on this line are malformations of the embryo itself. Statistics say that from 70-90% of embryos had chromosomal abnormalities: they are random and will not occur in other pregnancies. You may have been ill, taken medication, or were under the influence of other harmful factors. Fate saved you from a child with malformations.
You may have been ill, taken medication, or were under the influence of other harmful factors. Fate saved you from a child with malformations.
The human body is perfect and finds a way to correct the situation by miscarriage. Today is a tragedy for you. The real tragedy would be the preservation and birth of a sick, non-viable child. So don’t cry and understand: everything is for the best, you won’t help grief with tears ... And after three months, try again - it will almost certainly turn out to be successful.
It should also be noted that the fact of a miscarriage does not mean that you have lost something. So for a period of 7-8 weeks, the absence of an embryo in the fetal egg is found - "anembryony". It is believed that in 80-90% of cases, miscarriages are undiagnosed non-developing pregnancies.
Miscarriage between 6 and 12 weeks
Miscarriage in this period is also considered early. Its most common causes are:
Endocrine disorders
Endocrine disorders, when the ovaries do not synthesize enough hormones to keep the fetus in the womb, or the amount of male sex hormones is increased, is one of the most common causes of miscarriage and miscarriage.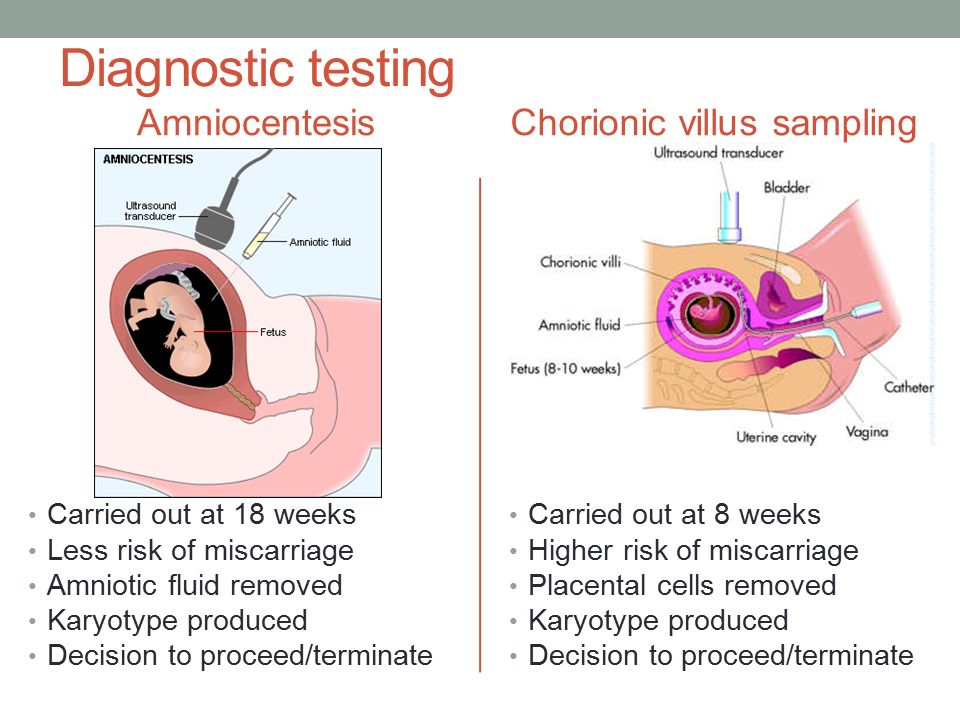
Imbalance of hormones in a woman's body is very likely to lead to an early termination of pregnancy. With a lack of the main hormone progesterone produced by the ovaries, this happens most often. Another hormonal problem is an increase in the tone of the uterus, which provokes the expulsion of the fetus.
Progesterone prepares the uterine mucosa for implantation and is the hormone for maintaining pregnancy in the first months. If conception occurs, the fetus cannot properly establish itself in the uterus. As a result, the fertilized egg is rejected. But pregnancy can be saved with the help of progesterone preparations if this problem is detected in time.
An excess of male sex hormones that suppress the production of estrogen and progesterone can also be the cause of an early miscarriage. Often, the cause of recurrent miscarriages are androgens that affect the formation and development of pregnancy; as well as thyroid and adrenal hormones. Therefore, a change in the function of these glands can lead to miscarriage.
Undertreated sexual infections
This problem must be solved before conception. Often the cause of miscarriage is sexually transmitted infections: syphilis, trichomoniasis, toxoplasmosis, chlamydia, cytomegalovirus and herpetic infections. Their effect on the fetus and the course of pregnancy is different for each woman and depends on the timing of infection, the activity of the microorganism, the degree of immune protection and the presence of other adverse factors. Depending on the situation, they can lead to the formation of fetal malformations, intrauterine infection, feto-placental insufficiency, early miscarriage or premature birth. Infection of the fetus and damage to the membrane of the fetus leads to miscarriage. To avoid this, infections should be treated before pregnancy. The use of therapy is possible during pregnancy as prescribed by a doctor.
Viral infections and other diseases
Any disease accompanied by intoxication and fever above 38 about C can lead to a miscarriage. Rubella, influenza and viral hepatitis occupy a leading position in this list. At a period of 4-10 weeks for pregnancy, ordinary tonsillitis can also become tragic, pneumonia carries a more serious risk. Pyelonephritis and appendicitis can cause early labor. When planning a pregnancy, it is imperative to undergo a medical examination in order to identify and treat foci of infections.
Rubella, influenza and viral hepatitis occupy a leading position in this list. At a period of 4-10 weeks for pregnancy, ordinary tonsillitis can also become tragic, pneumonia carries a more serious risk. Pyelonephritis and appendicitis can cause early labor. When planning a pregnancy, it is imperative to undergo a medical examination in order to identify and treat foci of infections.
Extremely dangerous during pregnancy rubella - it leads to severe fetal malformations, so infection during pregnancy is an indication for medical abortion.
Any disease during pregnancy can lead to non-viability of the fetus. And the body, through a miscarriage, insures you against unwanted offspring. With such a miscarriage, the next pregnancy has every chance of going well.
Immune causes of miscarriage
Sometimes antibodies that are hostile to the fetus are formed in the blood of a pregnant woman. This cause can be predicted and eliminated in advance. Most often, the conflict occurs when the embryo inherits the positive Rh factor of the father, and the negative Rh factor, the mother's body rejects the embryonic tissues that are alien to it. Constant monitoring of antibody titer and the introduction of anti-Rhesus immunoglobulins allows you to maintain and maintain pregnancy. In case of an immune conflict, progesterone preparations are also used to prevent miscarriage, which in this case has an immunomodulatory effect.
Most often, the conflict occurs when the embryo inherits the positive Rh factor of the father, and the negative Rh factor, the mother's body rejects the embryonic tissues that are alien to it. Constant monitoring of antibody titer and the introduction of anti-Rhesus immunoglobulins allows you to maintain and maintain pregnancy. In case of an immune conflict, progesterone preparations are also used to prevent miscarriage, which in this case has an immunomodulatory effect.
Reduced immunity
Reduced immunity during pregnancy also refers to immune causes. The body is simply not able to grow a new life in itself. You need to take care of yourself and recover before the next conception.
Anatomical causes of miscarriage
Anatomical causes of miscarriage are the most intractable. Malformations of the uterus are a serious reason for miscarriage. Sometimes you just have to deal with it.
Miscarriage between 12 and 22 weeks
Such a miscarriage is considered late. Its causes coincide with the causes of miscarriages in the early stages (anatomical, immune, infectious, endocrine).
Its causes coincide with the causes of miscarriages in the early stages (anatomical, immune, infectious, endocrine).
At this time, miscarriage also occurs due to isthmic-cervical insufficiency - a weak cervix cannot hold the fetus and opens. For this reason, a miscarriage can occur in the 2nd or 3rd trimester. Isthmic-cervical insufficiency is observed in 15.0-42.7% of women suffering from miscarriage. Careful monitoring of the pregnant woman allows you to identify the problem in time and make surgical correction of the cervix before the onset of childbirth.
In isthmic-cervical insufficiency, there is only one method of treatment - mechanical narrowing of the cervical canal. To do this, the neck is either sewn up or a special ring is put on it. However, the latter method is less efficient, because the ring can easily slide off the neck, then it will no longer hold back the process of opening it.
After suturing, if necessary, it is possible to use antibiotics and drugs that normalize the microflora of the vagina. The treatment of the vagina and the control of the state of the seams are carried out daily for 5 days. Stitches are removed at 37-38 weeks and with premature onset of labor.
The treatment of the vagina and the control of the state of the seams are carried out daily for 5 days. Stitches are removed at 37-38 weeks and with premature onset of labor.
Isthmic-cervical insufficiency may be primary (for no apparent reason), may be the result of abortion or hormonal disorders (increased levels of androgens - male sex hormones or their precursors).
Miscarriage after 22 weeks
Such a loss is hard to forget. Obstetricians talk about premature birth after the 28th week of pregnancy. Traditionally, a child born after this period is considered viable. But medicine knows many cases when it was possible to save the life of earlier children.
We recommend that you be carefully examined for miscarriage, check the above factors. In addition to them, the cause of a miscarriage can be antiphospholipid syndrome, while the woman's body perceives the child as something alien and rejects it. This disease, like the others listed, can be corrected; you have a very real chance of bearing a child.
Miscarriages due to hemostasis disorders
All of the above causes account for only 30-40%. Up to 70% of miscarriages are caused by disorders in the blood coagulation system (hemostasis).
Blood coagulation disorders leading to pregnancy loss can be divided into thrombophilic (increased clotting) and hemorrhagic (bleeding tendencies). Both of these extremes are dangerous to the fetus. Various disorders leading to the formation of small blood clots lead to the fact that the fetus loses sufficient blood supply, development is disturbed and the fetus is rejected.
The main hemorrhagic changes can appear even in childhood in the form of increased bleeding during cuts, tooth extractions, the onset of menstruation. But sometimes they declare themselves only during pregnancy and are the cause of a miscarriage. Bleeding in the early stages and detachment of the chorion is difficult to stop.
You may not guess, but incomprehensible headaches, weakness, fatigue, temporary loss of smell or hearing may be symptoms of disorders in the blood coagulation system.
When planning a pregnancy, a genetic examination should be carried out and, if necessary, treatment should be started.
It is advisable to be examined for hidden hemostasis defects even for those who consider themselves healthy. This will allow you to predict the occurrence of complications and prevent loss. Early therapy can prevent miscarriage at 98% of cases. If defects in hemostasis are already detected during pregnancy, it can be difficult to maintain it.
What to do after a miscarriage?
Find the cause! The ideal option is to be examined by future parents: it is much more reasonable to postpone conception and spend two or three months to identify the causes than to risk getting pregnant again, spend two months waiting, and then lose everything again and still go to the doctors.
Until you understand the reason, it will not evaporate. In most cases, the answers lie on the surface. Take care of your health and your future baby.
Sign up for a consultation with an obstetrician-gynecologist by phone +7 (495) 150-60-01
Tyan Oksana Aleksandrovna
Obstetrician-gynecologist Doctor of the highest category Work experience: 26 years
Volkova Polina Dmitrievna
Obstetrician-gynecologist, doctor of ultrasound diagnostics Doctor of the highest category Work experience: 35 years
Postnikova Nadezhda Anatolyevna
Obstetrician-gynecologist, ultrasound specialist Experience: 35 years
Moiseeva Alla Vitalievna
Obstetrician-gynecologist, doctor of ultrasound diagnostics Doctor of the first category Work experience: 37 years
Zabolotnova Olga Valentinovna
Obstetrician-gynecologist Doctor of the first category Experience: 26 years
Shchelokova Elena Nikolaevna
Obstetrician-gynecologist Doctor of the highest category Experience: 38 years
Maksimova Tamara Anatolyevna
Obstetrician-gynecologist Work experience: 7 years
Pass or medical card number:
Contact phone: *
Select the day of your appointment:
Additional information:
I am not a robot
By clicking the "Submit Application" button, you agree to the terms Privacy Policy and User Agreement
miscarriage, symptoms - Health Clinic 365 G.
 Yekaterinburg
Yekaterinburg Causes of miscarriage
Questions to the doctor about miscarriage
Diagnostics of miscarriages
Treatment and prevention of miscarriage
- this is a denture . According to statistics, 10 to 20% of all pregnancies end in miscarriage. However, the real numbers could be much higher, as a large number of miscarriages happen very early, and women are not even aware of their pregnancy. Most miscarriages happen due to abnormal development of the fetus.
Miscarriage is quite common, but this fact does not make things easier. It is always difficult to cope with the realization that there was a pregnancy, but no child. Try to deal with the situation psychologically and understand what could be causing the miscarriage, what increases the risk of it, and what type of treatment might be needed.
Miscarriage symptoms .
Most miscarriages occur before 12 weeks. Signs and symptoms of a miscarriage include:
- Vaginal bleeding or spotting (although quite common in early pregnancy)
- Pain or cramps in the abdomen or lower back
- Fluid vaginal discharge or tissue fragments
It is important to consider the fact that in early pregnancy, spotting or vaginal bleeding is quite common. In most cases, women who experience light bleeding during the first three months have an uneventful pregnancy thereafter. In some cases, even with heavy bleeding, the pregnancy does not end in a miscarriage.
In most cases, women who experience light bleeding during the first three months have an uneventful pregnancy thereafter. In some cases, even with heavy bleeding, the pregnancy does not end in a miscarriage.
Some women who have a miscarriage develop an infection in the uterus. This infection, also called septic miscarriage, can cause:
- Fever (feeling hot, chills)
- Body pains
- Thick, foul-smelling vaginal discharge
When to see a doctor.
Call your doctor if:
- Bleeding, even if only light spotting occurs
- Profuse, liquid vaginal discharge without pain or bleeding
- Isolation of tissue fragments from the vagina
You can place a piece of tissue to be isolated in a clean container and take it to your doctor for examination. It is unlikely that the study will give any accurate results, but if it is determined that the fragments of the excreted tissue are from the placenta, the doctor will be able to conclude that the symptoms that appear are not associated with the presence of a tubal (ectopic) pregnancy.