Mild placental abruption
Placental Abruption | March of Dimes
Placental abruption is an uncommon condition that can cause serious bleeding during pregnancy.
If you experience placental abruption, it can cause problems for your baby, including growth issues, preterm birth or stillbirth.
If you have bleeding from your vagina while you’re pregnant, get help from your provider immediately or go to the hospital for evaluation
If the bleeding is severe, it could be an abruption and your provider may recommend that you give birth right away.
The placenta attaches to the wall of the uterus (womb) and supplies the baby with food and oxygen through the umbilical cord.
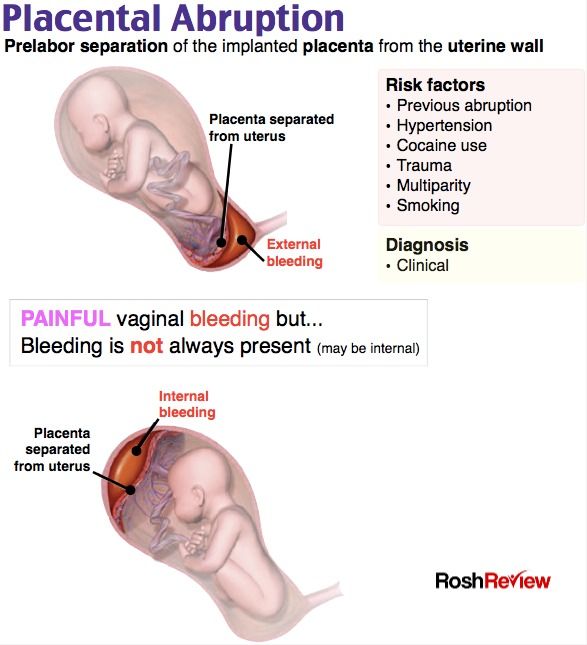
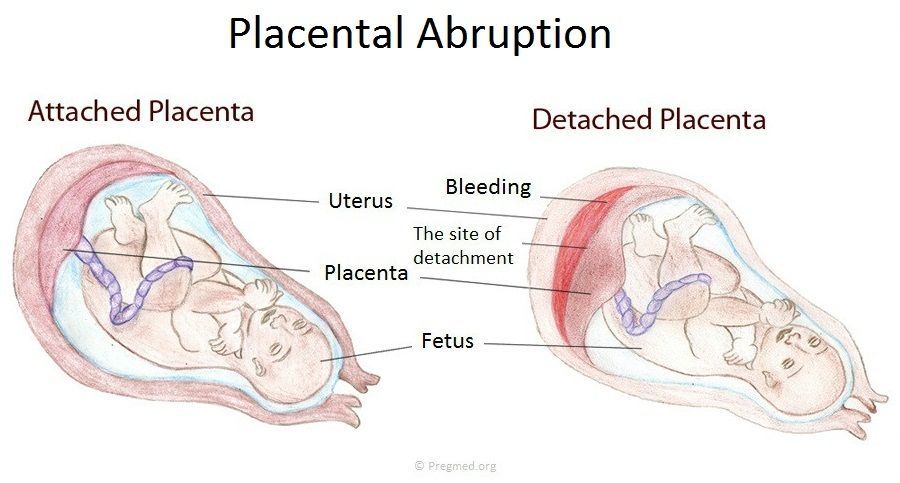
Placental abruption is a serious condition in which the placenta separates from the wall of the uterus before birth. It can separate partially or completely. If this happens, your baby may not get enough oxygen and nutrients in the womb. You also may have pain and serious bleeding.
Normally, the placenta grows onto the upper part of the uterus and stays there until your baby is born. During the last stage of labor, after the baby is born, the placenta separates from the uterus, and your contractions help push it into the vagina (birth canal). This is also called the afterbirth.
About 1 in 100 pregnant people (1 percent) have placental abruption. It usually happens in the third trimester but it can happen any time after 20 weeks of pregnancy. Mild cases may cause few problems. An abruption is mild if only a very small part of the placenta separates from the uterus wall. A mild abruption usually isn’t dangerous but needs to be followed closely because it can lead to complete separation.
If you have a placental abruption (greater separation between the placenta and the uterus), your baby is at higher risk for:
- Growth problems, called intrauterine growth restriction; identified by ultrasound
- Preterm birth (birth that happens too early, before 37 weeks of pregnancy).
 An early delivery can be done to save you and your baby
An early delivery can be done to save you and your baby - Stillbirth (when a baby dies in the womb after 20 weeks of pregnancy) if the separation of the placenta is sudden and severe.
Placental abruption is related to about 1 in 10 premature births (10 percent). Premature babies (born before 37 weeks of pregnancy) are more likely than babies born later to have health problems during the first weeks of life, lasting disabilities, and even death.
Placental abruption can cause anemia and life threatening complications for a pregnant person. If it’s not diagnosed and treated immediately there can be hemorrhage and blood clotting complications for both the baby and the pregnant person. Delivery by cesarean birth (c-section) section may be required.
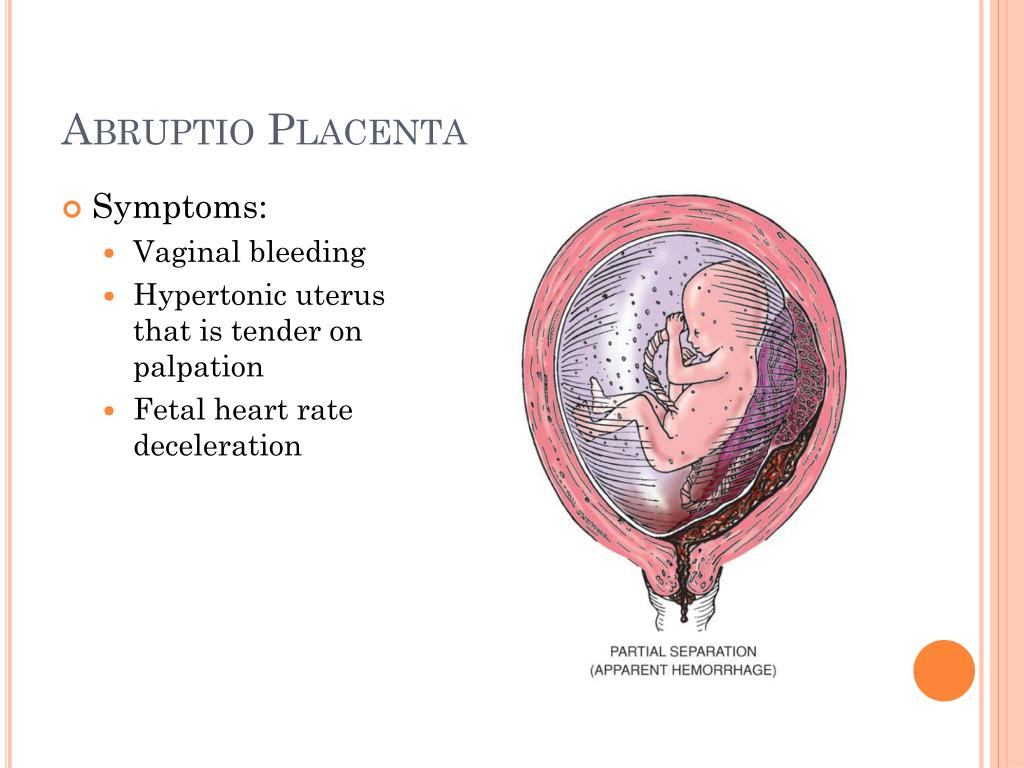
What are the symptoms of placental abruption?
The main symptom of placental abruption is vaginal bleeding. You also may have pain, contractions, discomfort and tenderness or sudden, ongoing belly or back pain. Sometimes, these symptoms may happen without vaginal bleeding because the blood is trapped behind the placenta. If you have any of these symptoms, call your health care provider and go to the hospital right away.
Sometimes, these symptoms may happen without vaginal bleeding because the blood is trapped behind the placenta. If you have any of these symptoms, call your health care provider and go to the hospital right away.
How is placental abruption diagnosed?
If your provider thinks you are having an abruption, you may need to get checked at the hospital. Your provider can look for abruption by doing a physical exam and an ultrasound. An ultrasound can find many, but not all, abruptions. Your provider will also monitor your baby’s heartbeat.
How is placental abruption treated?
Treatment depends on how serious the abruption is and how far along you are in your pregnancy.
Your provider may simply monitor you and your baby. But sometimes you may need to give birth right away.
If you need to give birth right away and if there is time, your provider may give you medicines called corticosteroids. These medicines help speed up the development of your baby’s lungs and other organs.![]()
Mild placental abruption
If you have a mild abruption at 24 to 34 weeks of pregnancy, you need careful monitoring in the hospital. If tests show that you and your baby are doing well, your provider may give you treatment to try to keep you pregnant for as long as possible. Your provider may want you to stay in the hospital until you give birth. If the bleeding stops, you may be able to go home.
If you have a mild abruption at or near full term, your provider may recommend inducing labor or c-section. You may need to give birth right away if:
- The abruption gets worse and you are having increased pain.
- You are bleeding heavily or show signs in your blood tests of severe anemia.
- Your baby has heart rate changes that indicate it is having problems.
Moderate or severe placental abruption
If you have a moderate to severe abruption, you are in a medical emergency and usually need to give birth right away.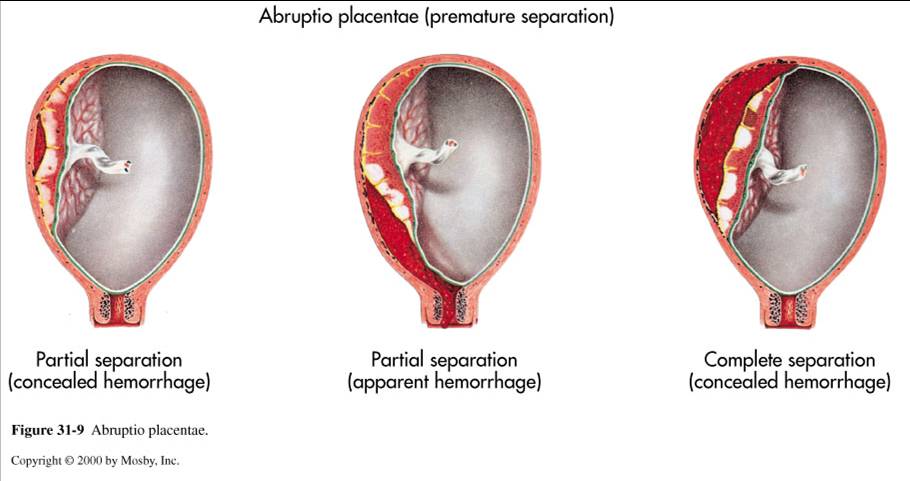 Needing to give birth quickly may increase your chances of having a c-section.
Needing to give birth quickly may increase your chances of having a c-section.
If you lose a lot of blood due to the abruption, you may need a blood transfusion. An emergency c-section may be needed to save you and your baby. It’s very rare, but if you have heavy bleeding that can’t be controlled, you may need to have your uterus removed by surgery (hysterectomy). A hysterectomy can prevent deadly bleeding and other problems in your body. But it also means that you can’t get pregnant again in the future.
What causes placental abruption?
We don’t really know what causes placental abruption. You may be at higher risk for placental abruption if:
- You had an abruption in a previous pregnancy.
- You have high blood pressure.
- You smoke cigarettes.
- You use cocaine.
- Your belly is harmed from a car accident or physical abuse.
- You’re a person who is 35 or older.
- You have an infection in your uterus.
- You are in preterm labor.

- Your water breaks before 37 weeks.
- You have problems with the uterus or umbilical cord.
- You have more fluid around the baby than is normal.
- You’re pregnant with twins, triplets or more.
- You have asthma.
- You have a sibling who had placental abruption.
- You’ve had a cesarean section in a previous pregnancy.
- You’ve been exposed to air pollution.
- Your sonogram shows evidence of mild separation of the placenta
If I’ve had a placental abruption before, what are my chances of having it again?
If you’ve had a placental abruption in a past pregnancy, you have about a 1 in 10 (10 percent) chance of it happening again in a later pregnancy.
How can you reduce your risk for abruption?
In most cases, you can’t prevent abruption. But you may be able to reduce your risk by getting closely monitored and treated for high blood pressure, not smoking or using street drugs, and always wearing a seatbelt when riding in a car. Your health care provider may also recommend that you take prenatal vitamins, including folic acid.
Your health care provider may also recommend that you take prenatal vitamins, including folic acid.
Last reviewed: September 2021
Symptoms, Causes & Effects On Baby
Overview
What is a placental abruption?
Placental abruption is a complication of pregnancy that happens when the placenta separates from your uterus before delivery. The placenta is a temporary organ that connects a growing fetus to your uterus during pregnancy. It attaches to the wall of your uterus, usually on the top or side and acts as a lifeline that gives nutrients and oxygen to the fetus through the umbilical cord. The placenta also removes waste from the fetus's blood.
In placental abruption, the placenta may completely detach or partially detach. This can decrease the amount of oxygen and nutrients to the fetus and cause heavy bleeding in the birthing parent. Placental abruption is a serious condition that requires medical treatment.
What are the different types of placental abruption?
- A partial placental abruption occurs when the placenta does not completely detach from the uterine wall.
- A complete or total placental abruption occurs when the placenta completely detaches from the uterine wall. There is usually more vaginal bleeding associated with this type of abruption.
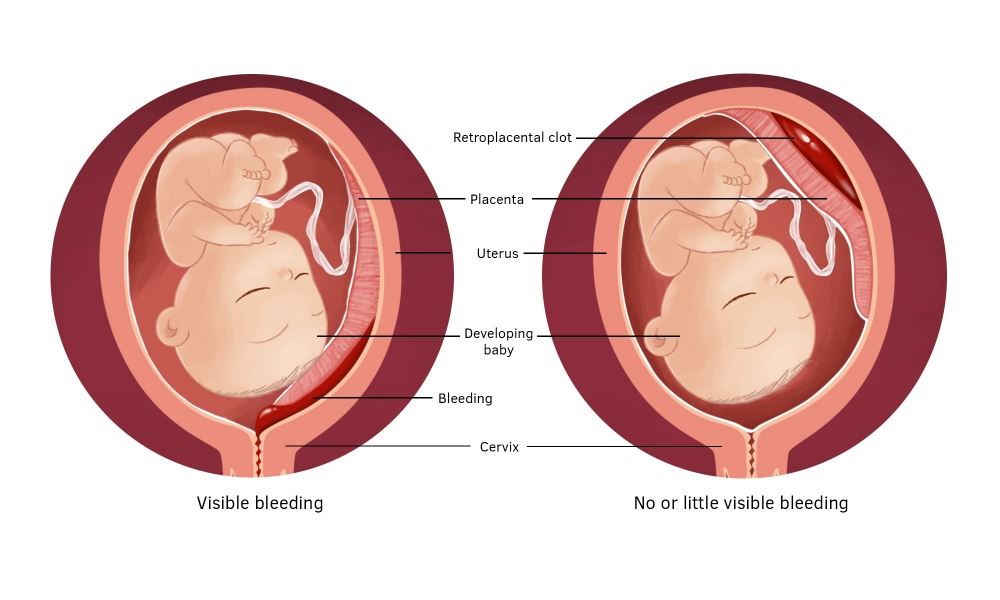
- Revealed placental abruptions have moderate to severe vaginal bleeding that you can see.
- Concealed placental abruptions have little or no visible vaginal bleeding. Blood is trapped between the placenta and uterine wall.
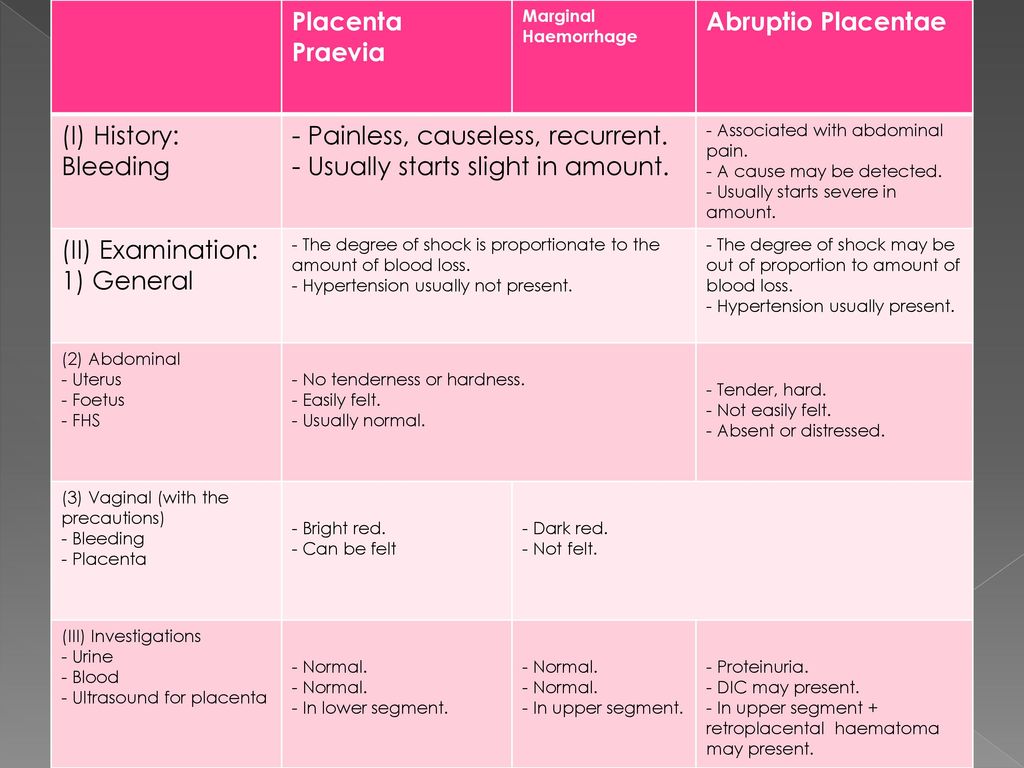
What is the difference between placental abruption and placenta previa?
In placenta previa, the placenta is covering all or part of the birthing parent's cervix. It's also called low-lying placenta. Think of it as an obstacle that’s blocking the exit from the uterus. Even though the placenta is in a complicated position, it’s still attached to the uterus. When the placenta detaches from the uterus, this is a placental abruption. Both conditions can cause vaginal bleeding during pregnancy and labor.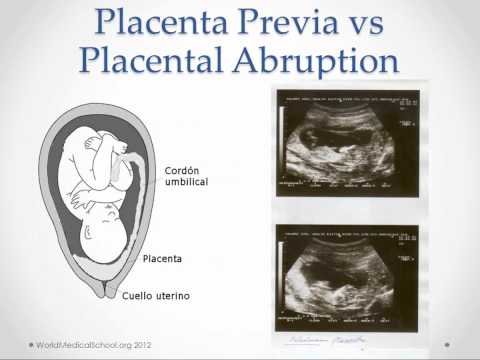
How common is a placental abruption?
About 1 out of 100 pregnancies has placental abruption. This condition is usually seen in the third trimester, but it can happen any time after 20 weeks of pregnancy up until delivery.
What are the effects of placental abruption?
Placental abruption can be life-threatening to the fetus and sometimes to you. Complications from a placental abruption include:
For baby:
- Premature birth.
- Low birth weight.
- Growth problems.
- Brain injury from lack of oxygen.
- Stillbirth.
For birthing parent:
- Blood loss.
- Blood clotting issues.
- Blood transfusion.
- Hemorrhage.
- Kidney failure.
Symptoms and Causes
What causes placental abruption?
The cause of placental abruption is often unknown. Certain lifestyle choices or abdominal trauma can increase your risk for placental abruption.
What are the risk factors for placental abruption?
You are at higher risk for placental abruptions if you have any of the following:
- Trauma or injury to your uterus (like a car accident, fall or blow to the stomach).
- Previous placental abruption.
- Multiple gestations (twins or triplets).
- High blood pressure (hypertension), gestational diabetes or preeclampsia.
- If you smoke or have a history of drug use.
- Short umbilical cord.
- Maternal age 35 or greater.
- Uterine fibroids.
- Thrombophilia (a blood clotting disorder).
- Premature rupture of membranes (the water breaks before the fetus is full term).
- Rapid loss of the amniotic fluid.
What are the signs and symptoms of placental abruption?
Each person can have different symptoms of placental abruption. However, the most common symptom is vaginal bleeding with cramping during the third trimester of pregnancy. Symptoms or signs can also include:
- Abdominal pain.
- Uterine contractions that are longer and more intense than average labor contractions.
- Uterine tenderness.
- Backache or back pain.
- Decreased fetal movement.

Vaginal bleeding can vary and is not an indication of how much the placenta has separated. In some instances, there could be no visible bleeding because the blood is trapped between the placenta and the uterine wall. Pain can range from mild cramping to strong contractions and often begins suddenly.
These symptoms can resemble other pregnancy conditions. Always consult with your healthcare provider for a diagnosis.
Do you always bleed during a placental abruption?
Most of the time, you will see some blood during a placental abruption. In the event of a concealed abruption, the blood will be behind the placenta. In that case, there will be no bleeding. In other cases, the abruption develops slowly, which can cause occasional, light bleeding.
Talk to your healthcare provider about any vaginal bleeding you experience during your pregnancy.
What does placental abruption feel like?
You may experience sudden or sharp pain, cramping, or tenderness in your lower pelvic region or back during a placental abruption. You could also feel less movement from the fetus. You should discuss these symptoms with your healthcare provider immediately.
You could also feel less movement from the fetus. You should discuss these symptoms with your healthcare provider immediately.
What are the first signs of a placental abruption?
The most common symptom of a placental abruption is vaginal bleeding, although you will not always bleed. You may also have sudden, ongoing pain in your abdomen or back.
Diagnosis and Tests
How is a placental abruption diagnosed?
Placental abruption is diagnosed through an exam and monitoring. You may be admitted to the hospital depending on the severity of the abruption or you may be able to rest at home. Your healthcare provider will:
- Ask how much bleeding has occurred.
- Ask where you feel pain and how intense the pain is.
- Ask when symptoms started.
- Monitor your blood pressure.
- Monitor the fetal heart rate and movement.
- Monitor your contractions.
- Use ultrasound to locate the bleeding and to check the fetus.
- Recommend blood or urine tests.
There are typically three grades of placental abruption a healthcare provider will diagnose:
- Grade 1: Small amount of bleeding, some uterine contractions, and no signs of stress to you or the fetus.
- Grade 2: Mild to moderate amount of bleeding, some uterine contractions, and signs of fetal stress.
- Grade 3: Moderate to severe bleeding or concealed bleeding, uterine contractions that do not relax, abdominal pain, low blood pressure, and fetal death.
It is important to discuss any symptoms or changes in symptoms with your healthcare provider.
Management and Treatment
How is a placental abruption treated?
Once the placenta has separated from the uterus, it cannot be reconnected or repaired. A healthcare provider will recommend treatment based on:
- The severity of the abruption.
- How long the pregnancy is/gestational age of the fetus.
- Signs of distress from the fetus.
- Amount of blood you've lost.
Generally, the severity of the abruption and gestational age of the fetus are the two most important factors:
If the fetus isn't close to full term:
- If it's too soon for your baby to be born and your abruption is mild, you will be closely monitored until you reach 34 weeks of pregnancy. If the fetal heart rate is normal and you're not bleeding, your healthcare provider may allow you to go home to rest. They may give you medication to help with fetal lung development.
- If your abruption is severe and the health of you or the fetus are at risk, immediate delivery may be necessary.
If the fetus is near full term:
- If your abruption is mild and the fetal heart rate is stable, a closely monitored vaginal delivery is possible. This is generally determined around 34 weeks of pregnancy.
- If the abruption gets worse or you or the fetus are in danger at any time, the baby will be delivered via emergency Cesarean section.
Prevention
Can I prevent a placental abruption?
Placental abruptions are typically unpreventable. You can reduce your risk by:
- Not smoking or using drugs.
- Keeping your blood pressure at a healthy level.
- Keeping diabetes under control.
- Taking health and safety precautions like wearing a seat belt.
- Reporting any abdominal trauma to your healthcare provider.
- Talking to your healthcare provider about any vaginal bleeding.
Outlook / Prognosis
What can I expect if I have a placental abruption?
This can vary depending on the severity of your symptoms and how far along you are in your pregnancy. You can expect to be monitored closely and often. Watch for any changes in symptoms and discuss them with your healthcare provider immediately.
What is my baby’s survival rate after a placental abruption?
The two factors that affect survival rate are gestational age at birth and the severity of the abruption.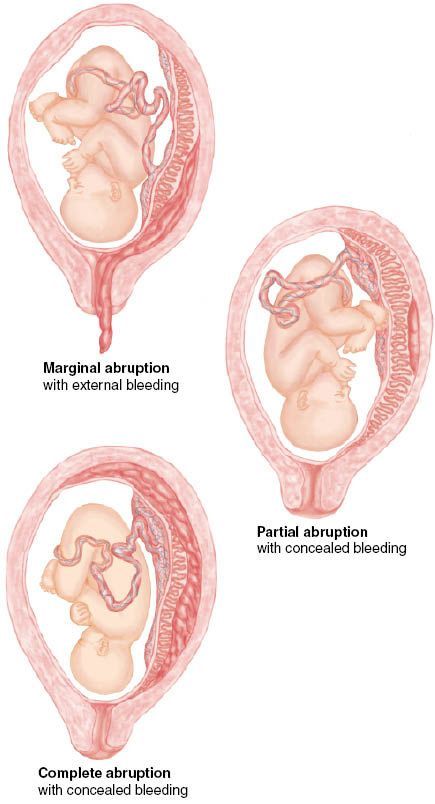 Early detection, close monitoring, and quick treatment can help reduce complications.
Early detection, close monitoring, and quick treatment can help reduce complications.
Can I have another placental abruption?
You have about a 15% chance of having another abruption in a future pregnancy. With two prior abruptions, this chance increases to about 25%. If you have had a previous abruption, please let your healthcare provider know.
What are questions I should ask my healthcare provider?
Your healthcare provider should be able to answer your questions and prepare you for treatment of placental abruption. Here are some questions you might ask:
- Is my baby’s life in danger? Is mine?
- What are my treatment options?
- Can I give birth now?
- How will I know if my abruption is worsening?
- What are potential complications?
- Do I need additional tests?
Frequently Asked Questions
Can sex cause a placental abruption?
Sexual intercourse is not a direct cause of placental abruption.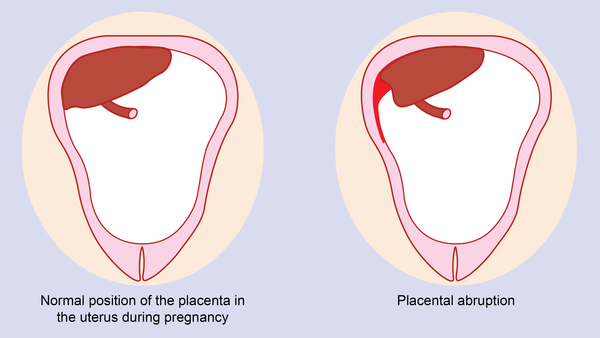 In most cases, it’s perfectly safe to have sex during pregnancy. Activities with a high risk of falling or abdominal trauma should be avoided during pregnancy.
In most cases, it’s perfectly safe to have sex during pregnancy. Activities with a high risk of falling or abdominal trauma should be avoided during pregnancy.
Can sneezing cause a placental abruption?
Sneezing is a normal thing your body does and is not a cause for placental abruption. It can't harm the fetus in any way. If you have any concerns about frequent and forceful sneezing or coughing, reach out to your healthcare provider for guidance.
Can smoking cause a placental abruption?
Smoking can increase your risk of many complications during pregnancy, including placental abruption. Ask your healthcare provider about ways to quit smoking.
When do I call my healthcare provider if I suspect a placental abruption?
Call your healthcare provider immediately if are bleeding, cramping or experience pelvic pain during your pregnancy, especially in the third trimester.
A note from Cleveland Clinic
Placental abruption is an uncommon, yet serious condition people can experience during pregnancy.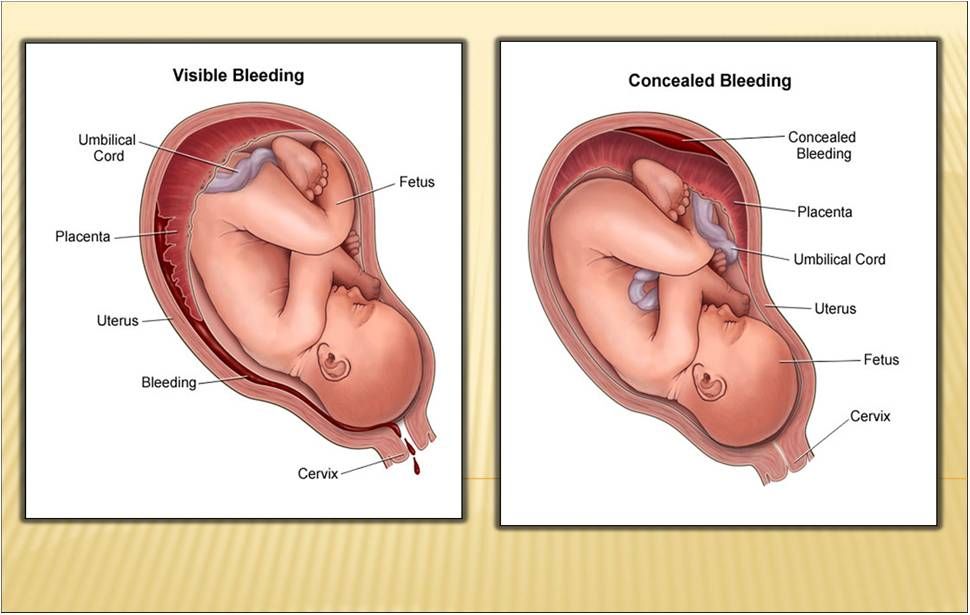 Talk to your healthcare provider if you experience vaginal bleeding, pelvic pain or cramping. Placental abruption should be diagnosed and treated promptly to ensure you and your baby are healthy.
Talk to your healthcare provider if you experience vaginal bleeding, pelvic pain or cramping. Placental abruption should be diagnosed and treated promptly to ensure you and your baby are healthy.
Premature placental abruption: what a future mother needs to know and how not to miss its signs | Blog
First, let's talk about what is the placenta?
The placenta is the embryonic organ that connects the body of mother and child. Its uniqueness lies in the fact that it is the only "disposable" organ. The placenta begins to develop from the 2nd week of pregnancy, forms up to 15-16 weeks and reaches full functional maturity by 36 weeks. And after the birth of the fetus (in the third stage of childbirth), it separates and leaves the mother's body, starting the process of lactation at the endocrinological level.
The placenta performs important functions such as gas exchange, nutrient exchange between the mother and the child, provides immunological protection and works as an endocrine gland, producing hormones necessary for the development of the fetus and the normal course of pregnancy.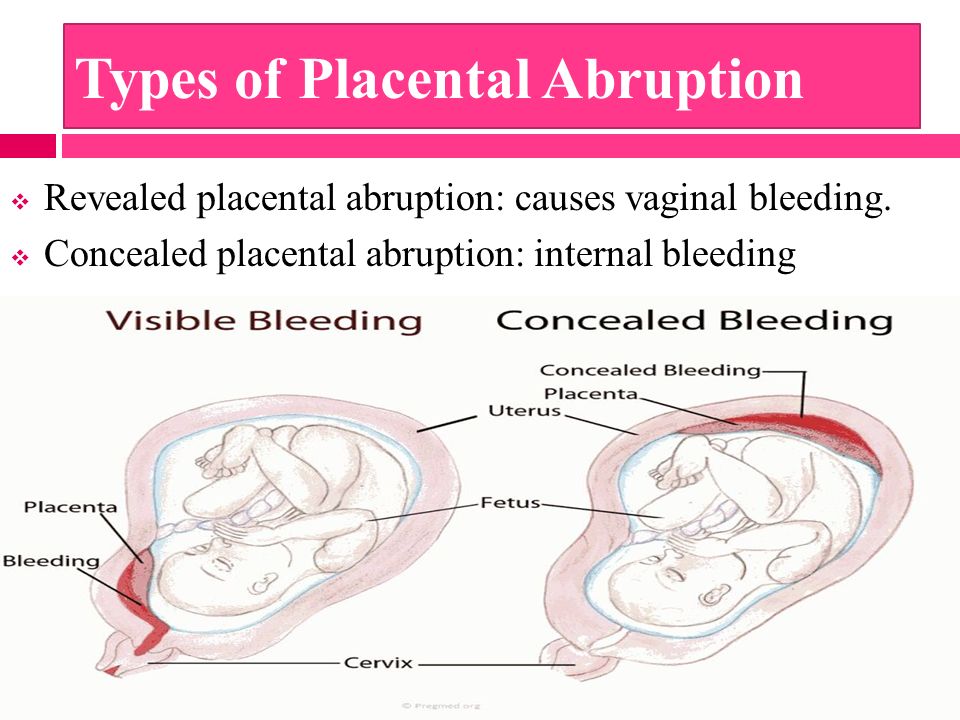 Every minute, about 500 ml of blood enters the placenta, but at the same time it is a kind of barrier that does not allow the blood of the mother and child to mix, and also prevents many toxic substances from entering the bloodstream of the baby.
Every minute, about 500 ml of blood enters the placenta, but at the same time it is a kind of barrier that does not allow the blood of the mother and child to mix, and also prevents many toxic substances from entering the bloodstream of the baby.
In this article we will talk about placental abruption.
This condition is quite rare (up to 1.5% of all pregnancies), but causes such threatening complications as massive bleeding and hemorrhagic shock, fetal distress, which in some cases can cause fetal death. Normally, the detachment of the placenta from the inner wall of the uterus occurs only after the birth of the fetus. If this happens before the onset of labor, as well as in the first or second stage of labor, this is the premature detachment of a normally located placenta. This condition is a very dangerous pathology that requires immediate diagnosis and decision of further medical tactics in the near future.
Causes of premature placental abruption
The only cause of premature placental abruption, unfortunately, has not been established to date. There are many theories, but in general, the occurrence of this condition is associated with many provoking factors.
There are many theories, but in general, the occurrence of this condition is associated with many provoking factors.
Major risk factors include:
- arterial hypertension,
- diabetes mellitus
- pregnant age over 40
- multiple pregnancy
- polyhydramnios
- postterm pregnancy and large fetus
- past uterine surgery
- blood clotting disorder,
- autoimmune diseases
- kidney disease
- bad habits such as smoking and drug use
- inflammatory diseases of the uterus and placenta, abnormal development of the uterus.
Causes that can provoke placental abruption: physical trauma of a pregnant woman (accident, fall, blow to the stomach), disruption of the contractile activity of the uterus, stress, gross obstetric manipulations.
Types of placental abruption
There are the following types of placental abruption: partial and complete.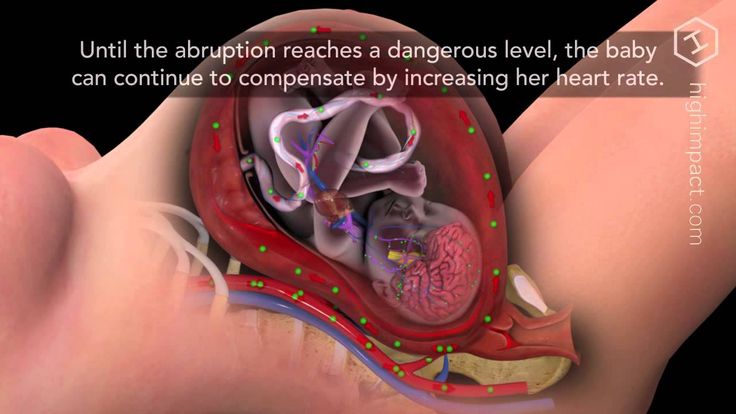
Partial detachment, in turn, can be central and marginal.
Why is this classification so important? And because both the clinical picture and medical tactics depend on the place and volume of the detachment. Partial detachment can be progressive or non-progressive.
Non-progressive detachment has a significantly better prognosis for a pregnant woman, because in this case, conservative treatment is possible with preservation of pregnancy.
Symptoms of placental abruption:
Here is a triad of main symptoms that may be a sign of placental abruption:
- abdominal pain, feeling of increased uterine tone;
- bleeding from the genital tract;
- violation of the fetal heartbeat, indicating fetal distress.
Also, a woman can feel the baby's reaction to a decrease in the amount of oxygen supplied to him due to placental abruption - he begins to move more actively, reacting to hypoxia.
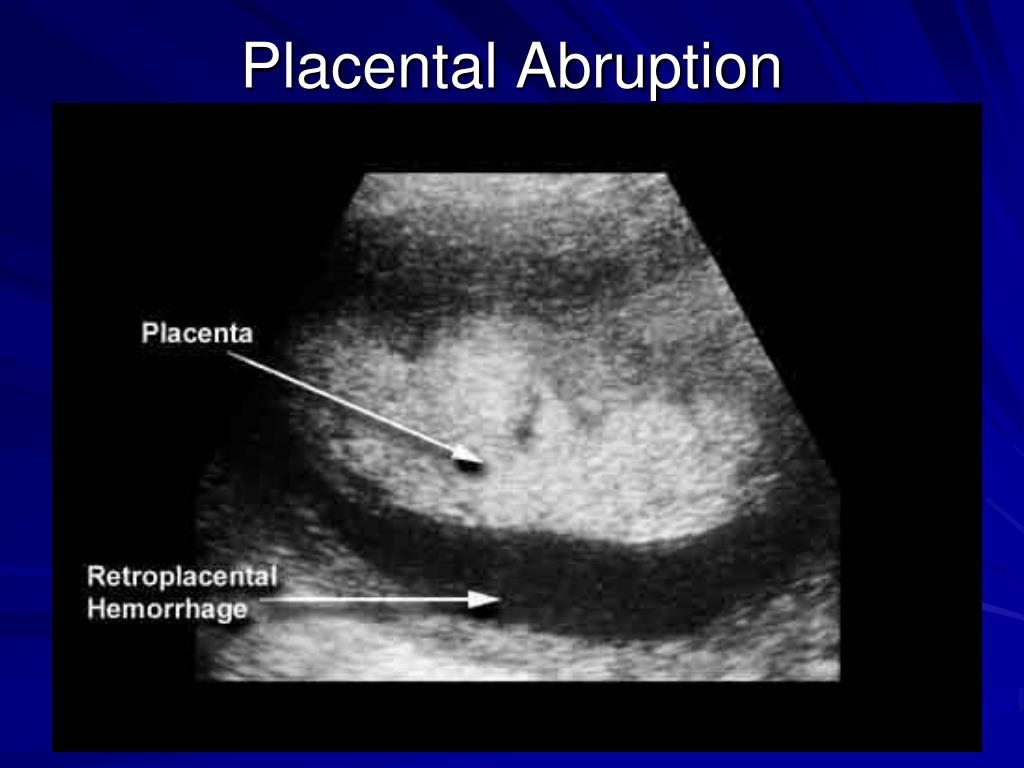
These symptoms do not always appear at the same time! For example, with marginal abruption of the placenta, blood flows into the vagina, which means that the woman sees signs of bleeding. With central detachment, a retroplacental hematoma is formed. Bleeding is internal, which means that a pregnant woman may not notice its signs. The appearance of an accelerated heartbeat in a woman, a decrease in blood pressure, nausea, dizziness, and severe weakness may indicate internal bleeding.
With central detachment, a retroplacental hematoma is formed. Bleeding is internal, which means that a pregnant woman may not notice its signs. The appearance of an accelerated heartbeat in a woman, a decrease in blood pressure, nausea, dizziness, and severe weakness may indicate internal bleeding.
However, with central placental abruption, blood accumulates in front of the placenta and begins to “press” on nearby tissues. As a result, a pronounced pain syndrome occurs.
It must be emphasized that if at least one of the symptoms appears, it is necessary to immediately inform the doctor about this! This condition can be very dangerous for you and your baby, so it is important to diagnose it in a timely manner.
Diagnosis of placental abruption
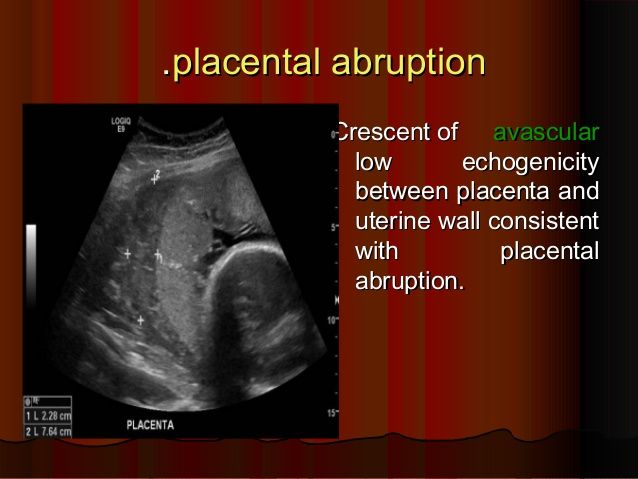
Diagnosis of placental abruption is based not only on clinical symptoms and gynecological examination. Ultrasound diagnostics is the main method that allows you to accurately assess the location and area of the exfoliated area of the placenta and see the presence or absence of a hematoma.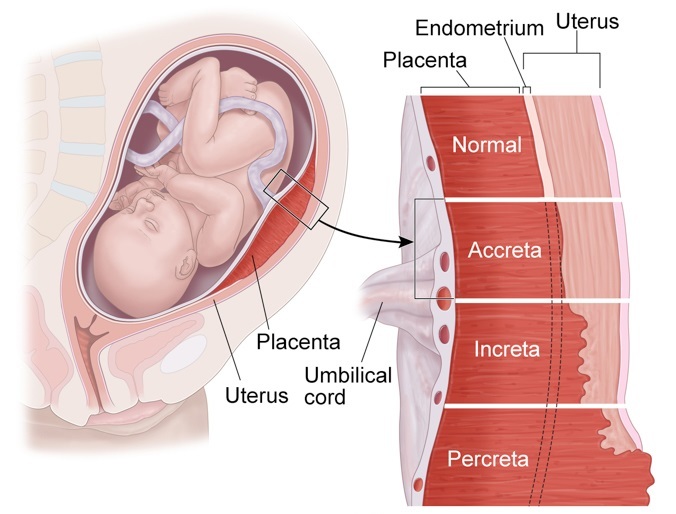 Also, ultrasound can distinguish premature detachment from placenta previa (its abnormal location, in which it overlaps the internal pharynx of the cervix). This condition can have similar symptoms, as it is often accompanied by bleeding. The condition of the fetus and the degree of its hypoxia will be determined using cardiotocography, and Dopplerography, in turn, assesses violations of the uteroplacental circulation. Based on these examination results, the obstetrician-gynecologist, and more often a council of doctors, decides on the type of further medical tactics.
Also, ultrasound can distinguish premature detachment from placenta previa (its abnormal location, in which it overlaps the internal pharynx of the cervix). This condition can have similar symptoms, as it is often accompanied by bleeding. The condition of the fetus and the degree of its hypoxia will be determined using cardiotocography, and Dopplerography, in turn, assesses violations of the uteroplacental circulation. Based on these examination results, the obstetrician-gynecologist, and more often a council of doctors, decides on the type of further medical tactics.
Treatment of placental abruption
Treatment of placental abruption always requires hospitalization of the pregnant woman in the maternity hospital for constant monitoring of her condition. In cases of non-progressive mild placental abruption with a stable state of the mother and fetus, conservative tactics with drug therapy and preservation of pregnancy are possible. Progressive detachment, as well as severe detachment, certainly requires an emergency caesarean section.
In case of complete detachment of the placenta, with the rapid progression of this condition, massive bleeding occurs, which threatens the life of both the pregnant woman and the child. In such a situation, surgeons always prioritize the life of a woman and do everything necessary to save her. Some cases may, unfortunately, require even such radical surgical tactics as removal of the uterus. However, at the current level of development of medicine, more and more technologies are emerging that, with timely assistance, can save not only the life of the mother and child, but also the reproductive functions of a woman. In particular, our obstetrician-gynecologists and anesthesiologists use up-to-date international medical protocols to ensure the safest possible delivery. Appropriate algorithms have also been developed for surgical interventions with a high risk of bleeding. Thanks to the latest technologies in vascular surgery with X-ray and ultrasound control, massive bleeding can be quickly and safely stopped. That is why we make sure that our maternity hospital always has the necessary amount of blood products and all the necessary modern equipment that may be needed in critical situations.
Quite often, expectant mothers ask about the prevention of such complications as placental abruption.
We advise you to adhere to the following recommendations:
- avoid stressful situations, excessive physical activity, factors that can lead to physical injury,
- do not smoke or use drugs
- control your blood pressure during pregnancy.
And of course, our patients who have certain chronic diseases require special attention. They need to undergo all the necessary examinations in a timely manner and adhere to the prescribed treatment and recommendations.
If you still have questions about this topic, please contact our specialists! Take care of yourself and be attentive to your well-being!
I wish your pregnancy to be a source of only positive emotions!
Premature placental abruption.
IMPORTANT
The information in this section should not be used for self-diagnosis or self-treatment. In case of pain or other exacerbation of the disease, only the attending physician should prescribe diagnostic tests. For diagnosis and proper treatment, you should contact your doctor.
Premature placental abruption is the early separation of the placenta from the walls of the uterus, which occurred before the birth of the fetus. The classic manifestations of placental abruption are pain, bleeding, uterine muscle tension, and fetal disorders. Premature abruption of the placenta is diagnosed based on the complaints of the pregnant woman, the data of the vaginal examination, ultrasound. Treatment of premature placental abruption consists in carrying out tocolytic, antispasmodic, hemostatic, antianemic therapy; in some cases, the question of operative delivery is raised.
- Causes of premature placental abruption
- Placental abruption variants
- Symptoms of placental abruption
- Diagnosis of premature placental abruption
- Treatment of placental abruption
- Prognosis and prevention of premature placental abruption
- Prices for treatment
General
Premature abruption of the placenta is a serious complication that endangers the life of the mother and fetus and requires urgent medical measures.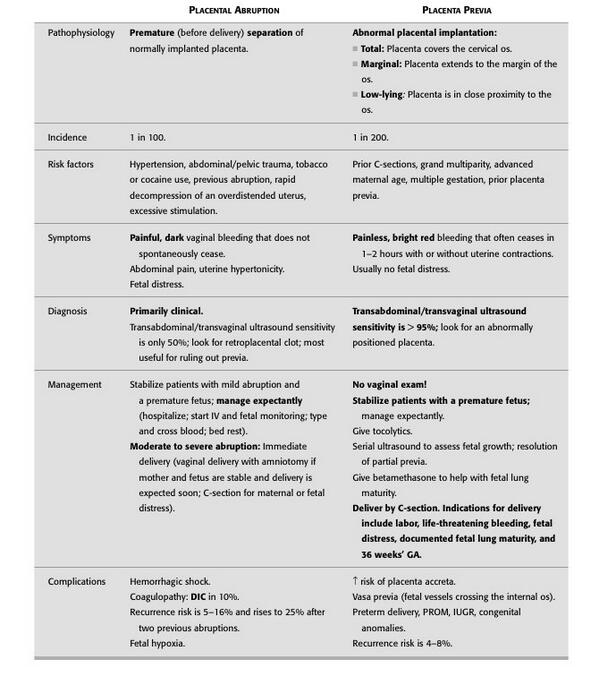 In obstetrics and gynecology, premature detachment of a normally located placenta is distinguished when it is localized in the upper sections of the uterus, on the walls of the body or bottom, and detachment of the placenta previa, located in the area of the uterine os. Premature abruption of the placenta can develop both during pregnancy and during childbirth. The frequency of this pathology occurs in 0.4-1.4% of all pregnancies.
In obstetrics and gynecology, premature detachment of a normally located placenta is distinguished when it is localized in the upper sections of the uterus, on the walls of the body or bottom, and detachment of the placenta previa, located in the area of the uterine os. Premature abruption of the placenta can develop both during pregnancy and during childbirth. The frequency of this pathology occurs in 0.4-1.4% of all pregnancies.
During pregnancy, pressure is exerted on the placenta, on the one hand, by the muscles of the uterus, and on the other, by the fetal egg and amniotic fluid. Normally, these forces are balanced by the significant elasticity of the placental tissue due to its spongy structure and less ability to contract the area of \u200b\u200bthe uterus to which the placenta is attached. These mechanisms in normal pregnancy exclude the development of premature detachment of the placenta.
Premature placental abruption
Causes of premature placental abruption
Modern views on the etiology of premature placental abruption single out the development of vasculopathy as a leading factor - vascular changes that disrupt uteroplacental circulation.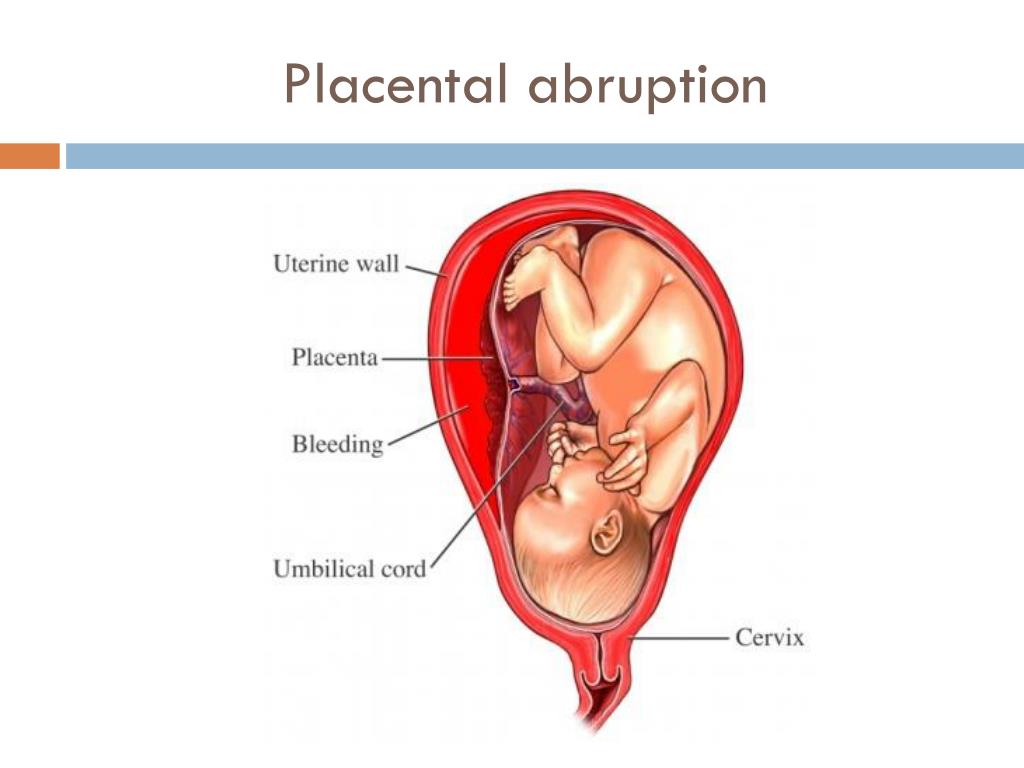 Vascular disorders can occur if a pregnant woman has somatic diseases (pyelonephritis, hypertension, obesity, diabetes mellitus), toxicosis (preeclampsia), etc.
Vascular disorders can occur if a pregnant woman has somatic diseases (pyelonephritis, hypertension, obesity, diabetes mellitus), toxicosis (preeclampsia), etc.
Vasculopathies are characterized by increased permeability, fragility and fragility of capillaries, multiple infarcts and thrombosis in the placental tissue. Violation of the contact of the placenta and the uterine wall is accompanied by the accumulation of blood between the uterine wall and the placenta with the formation of a retroplacental (posterior placental) hematoma, which further exacerbates placental abruption.
There is a theory that the development of premature placental abruption is a consequence of chronic uteroplacental insufficiency, the causes of which lie in inflammatory, degenerative and other pathological processes of the uterus and placenta. Such changes are found in chronic endometritis, endocervicitis, uterine myoma, anatomical abnormalities of the uterus, post-term pregnancy.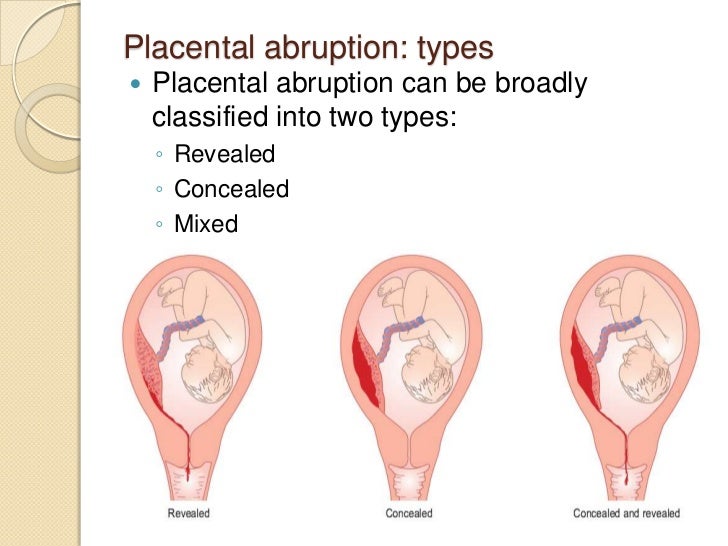
Abdominal trauma, multiple pregnancy, polyhydramnios, short umbilical cord, multiple births or abortions, delayed opening of the membranes, anemia, bad habits, autoimmune diseases (SLE) are also distinguished as risk factors for premature placental abruption. In rare cases, premature detachment of the placenta develops in response to the introduction of any drugs (protein solutions, donor blood).
Placental abruption options
According to the area of the rejected area, partial and complete total premature detachment of the placenta are distinguished. Total (complete) detachment is accompanied by the death of the child due to the cessation of gas exchange between the organisms of the mother and fetus.
Partial abruption of the placenta occurs in a limited area and may have a progressive or non-progressive course. With the non-progressive nature of premature detachment of the placenta, thrombosis of the uterine vessels occurs and further separation of the placenta is suspended. The subsequent course of pregnancy and childbirth is not disturbed. In the case of progressive detachment, the hematoma grows, the separation of the placenta continues, which leads to a pathological course of pregnancy and childbirth.
The subsequent course of pregnancy and childbirth is not disturbed. In the case of progressive detachment, the hematoma grows, the separation of the placenta continues, which leads to a pathological course of pregnancy and childbirth.
According to the localization of the placental tissue separation zone, marginal (peripheral) and central premature detachment of the placenta are distinguished. In case of premature detachment of the central part of the placenta, external bleeding may be absent; exfoliation of the marginal part is usually accompanied by leakage of blood from the genital tract. In the absence of external bleeding, blood permeates the thickness of the myometrium, which leads to damage to the neuromuscular apparatus of the uterus, loss of its excitability and contractility. In severe cases, blood can enter the amniotic fluid and the abdominal cavity.
Symptoms of placental abruption
Signs of placental abruption include bleeding, uterine pain and tension, hypoxia, and fetal cardiac abnormalities.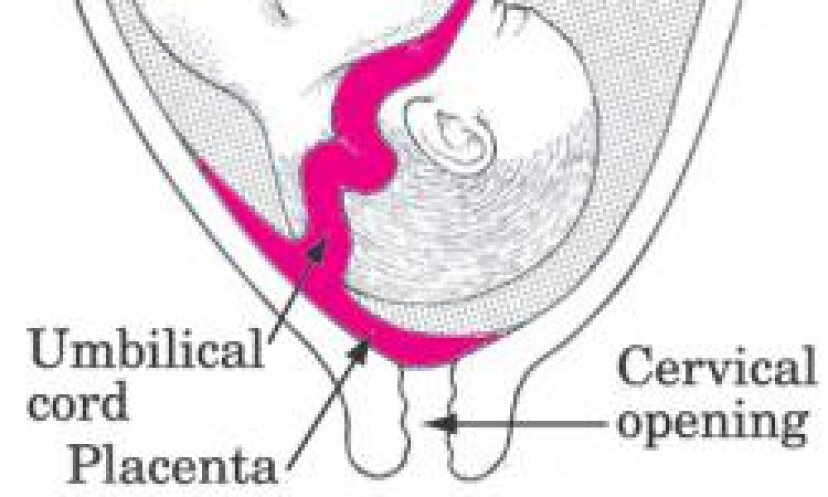 Bleeding in premature placental abruption can be external, internal and mixed (internal-external) with the release of scarlet or dark blood, depending on the duration of detachment. It is difficult to determine the amount of blood loss during internal or internal-external bleeding, therefore, in practice, they are guided by the volume of external blood loss and the condition of the pregnant woman (indicators of pulse, pressure, Hb, etc.).
Bleeding in premature placental abruption can be external, internal and mixed (internal-external) with the release of scarlet or dark blood, depending on the duration of detachment. It is difficult to determine the amount of blood loss during internal or internal-external bleeding, therefore, in practice, they are guided by the volume of external blood loss and the condition of the pregnant woman (indicators of pulse, pressure, Hb, etc.).
Tension of the uterus and pain in the abdomen with premature detachment of the placenta are almost always present. The pain can be dull, paroxysmal, radiating to the bosom, thigh or lower back, local or diffuse. On palpation, the gynecologist determines that the uterus is tense and has a dense texture. The degree of intrauterine suffering of the fetus with premature detachment of the placenta is due to the area of the calved area of the placental tissue. With detachment of more than 1/4 of the area of the placenta, the fetus begins to experience hypoxia, with detachment of 1/3 - severe hypoxia; with rejection of more than 1/3-1/2 of the surface of the placenta, intrauterine fetal death occurs.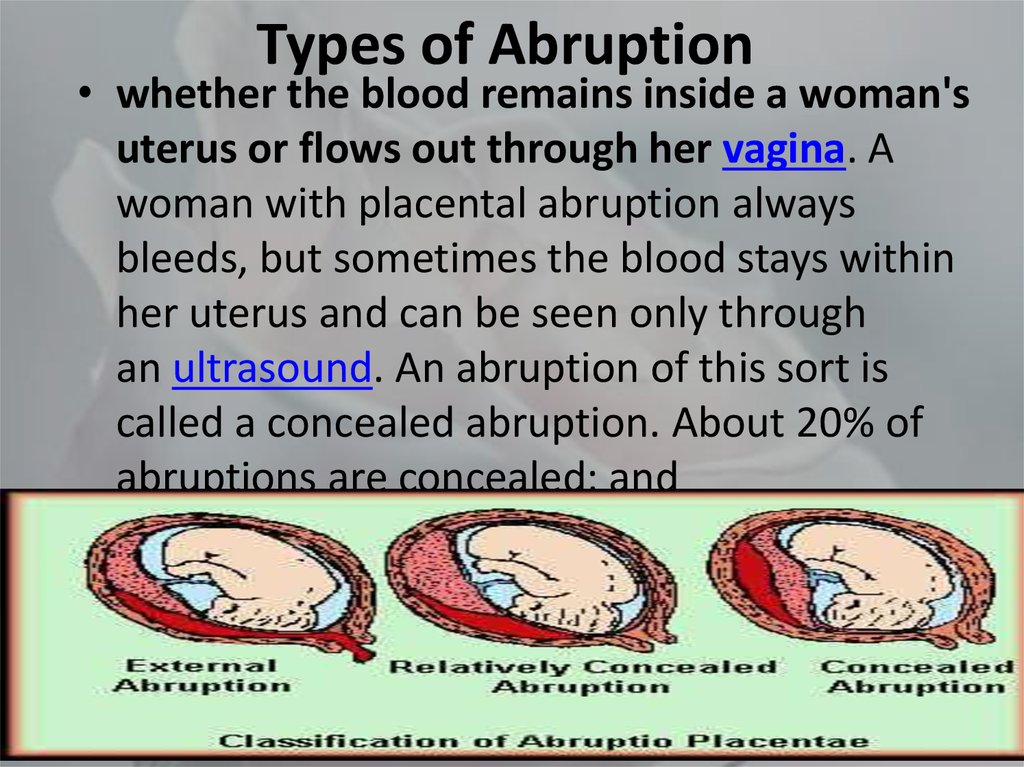
According to the severity of clinical manifestations, mild, moderate and severe forms of premature detachment of the placenta are distinguished. Mild placental abruption may not present with clear symptoms and is often found on routine ultrasound or postpartum examination of the placenta. The moderate form of the pathology is characterized by pain in the abdomen and minor secretions of blood and clots from the genital tract. Palpation is determined by a somewhat tense uterus, local moderate pain. During auscultation of the fetus, cardiac abnormalities are heard, indicating hypoxia of varying degrees.
In a severe form of premature detachment of the placenta, sudden intense arching pains in the abdomen, severe weakness, dizziness, sometimes fainting, pallor of the skin, tachycardia, hypotension are observed. A moderate amount of dark blood is secreted from the genital tract. There is a sharp tension and asymmetry of the uterus: on one side of it, a painful protrusion is palpated.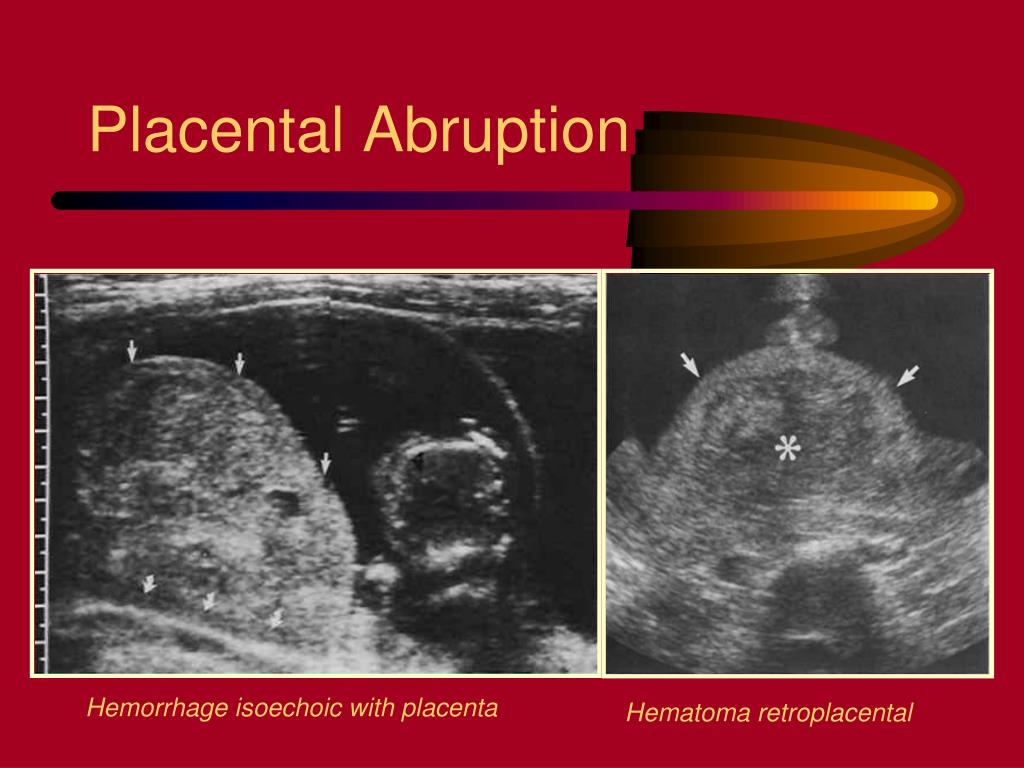 The fetal heartbeat is not determined by auscultation.
The fetal heartbeat is not determined by auscultation.
Diagnosis of premature placental abruption
With advanced manifestations of premature placental abruption, the diagnosis is not difficult. This takes into account the presence of pain, bleeding, hemodynamic disorders, hypoxic suffering of the fetus. A gynecological examination reveals uterine hypertonicity, its local or diffuse soreness, and asymmetry.
In the process of ultrasound, the localization of the placenta, the size of the detachment area are established. Dopplerography of the uteroplacental blood flow reveals violations of transplacental hemodynamics. The degree of fetal hypoxia is established using fetal cardiotocography or phonocardiography. A mild degree of premature detachment can be detected when examining an already born placenta by a characteristic small depression on its surface, filled with dark blood clots.
Treatment of placental abruption
Tactics for premature detachment of the placenta depends on the time of development of the pathology (pregnancy, childbirth), the severity of bleeding, the condition of the pregnant woman and the fetus.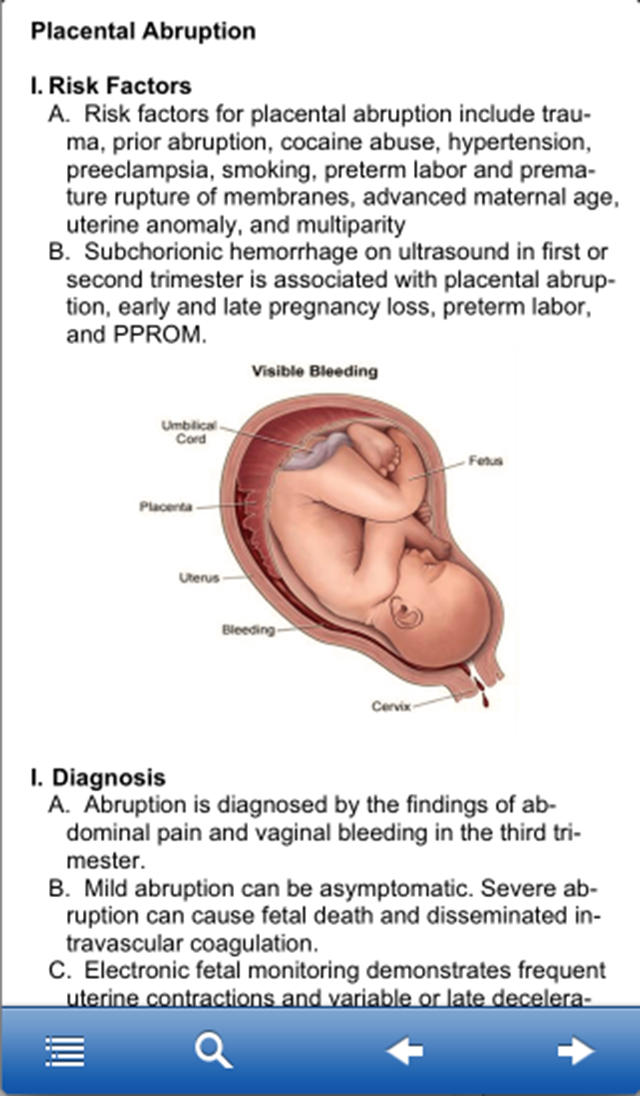 Pregnant women with signs of premature detachment of the placenta are hospitalized in the obstetric department of the hospital.
Pregnant women with signs of premature detachment of the placenta are hospitalized in the obstetric department of the hospital.
With partial non-progressive detachment for up to 36 weeks. bed rest, antispasmodic, tocolytic, hemostatic, antianemic therapy is prescribed. Treatment is carried out under the control of coagulogram, dynamic ultrasound and Doppler sonography. With indications of the progression of premature placental abruption, there is a need for early delivery. When the birth canal is ready (shortening, softening of the cervix, patency of the cervical canal), an amniotomy is performed; childbirth can be managed naturally with careful cardiac monitoring.
With moderate and severe premature detachment of the placenta, the choice is made in favor of operative delivery. With a severe degree of detachment, a cesarean section is performed regardless of the gestational age and viability of the fetus. After the extraction of the fetus and separation of the placenta, clots are removed, the walls of the uterus are examined, the state of the myometrium is specified. With pronounced changes in the uterus, a hysterectomy is indicated.
With pronounced changes in the uterus, a hysterectomy is indicated.
Regardless of the method of delivery, restoration of blood loss, anti-shock therapy, correction of anemia and blood clotting disorders with the help of infusion and transfusion therapy are carried out. To prevent postpartum hemorrhage, uterotonic drugs (oxytocin, prostaglandins, methylergometrine) are prescribed.
Prognosis and prevention of premature placental abruption
The mild form of non-progressive premature detachment of the placenta is prognostically the most favorable. With a more severe course, there is a danger to the pregnant woman and the fetus. In severe cases, intrauterine fetal death may occur. The main threat for a woman is the development of hemorrhagic shock with DIC.
Prevention of premature placental abruption consists in the timely treatment of general somatic and gynecological pathology of women planning a pregnancy; treatment of late toxicosis, dynamic monitoring of uteroplacental blood flow at all stages of pregnancy.