Magnesium supplements during pregnancy
Effect of Magnesium Supplement on Pregnancy Outcomes: A Randomized Control Trial
Adv Biomed Res. 2017; 6: 109.
Published online 2017 Aug 31. doi: 10.4103/2277-9175.213879
Author information Article notes Copyright and License information Disclaimer
Background:
Magnesium (Mg) is an essential mineral required to regulate body temperature, nucleic acid, and protein synthesis with an important role in maintaining nerve and muscle cell electrical potentials. It may reduce fetal growth restriction and preeclampsia as well as increase birth weight. This study aimed to assess the effects of consuming Mg supplementation during pregnancy on pregnancy outcomes.
Materials and Methods:
This is a randomized controlled trial with three sixty populated groups of pregnant women. Participants were randomized to treatment or control groups through random table numbers. Participants with Mg serum levels more than 1.9 mg/dl considered as control group A randomly. They just received one multimineral tablet once a day until the end of pregnancy participants with hypomagnesemia consider as Group B and C. Participants in Group B received one multimineral tablet daily until the end of pregnancy. Participants in Group C received 200 mg effervescent Mg tablet from Vitafit Company once daily for 1 month, and also they consumed one multimineral tablet from Alhavi Company, which contains 100 mg Mg, once a day until the end of pregnancy. Intrauterine growth retardation, preterm labor, maternal body mass index, neonatal weight, pregnancy-induced hypertension, preeclampsia, gestational diabetes mellitus, cramps of the leg Apgar score were compared between three groups.
Results:
In all pregnancy outcomes, Group C that received effervescent Mg tablet plus multimineral showed a better result than other groups, and frequency of complications of pregnancy was fewer than the other two groups and showed a significant difference.
Conclusion:
Mg supplement during pregnancy likely decrease probability occurrence of many complications of pregnancy.
Keywords: Magnesium Supplement, Pregnancy, Outcomes
Magnesium (Mg) is one of the essential minerals needed by humans in substantial large amounts. Mg work with many enzymes to regulate body temperature, synthesis nucleic acids, and proteins as well as maintaining electrical potentials in nerves and muscle membranes.[1,2]
Mg also has an important role in modulating vasomotor tone and cardiac excitability. Mg is used widely in many foods; dairy products, breads and cereals, legumes, vegetables, and meats are all good sources.[3] It is, therefore, not surprising that frank Mg deficiency has never been reported to occur in healthy individuals who eat varied diets. However, processing of the above foods can lead to high depletion of Mg.[4,5]
Common causes of Mg deficiency include inadequate dietary intake or gastrointestinal absorption, increased losses through the gastrointestinal or renal systems, and increased the requirement for Mg, such as in pregnancy. [6,7]
[6,7]
There are many important complications during pregnancy (gestational diabetes mellitus [GDM], pregnancy-induced hypertension [HTN], leg cramps, and preeclampsia), and a lot of them will occur the first time in pregnancy. Many of these complications are due to pregnancy or risk of occurrence that will increase during pregnancy so there are many diagnosis criteria such as Apgar score, birth weight, intrauterine growth retardation [IUGR], and preterm birth.
A study measuring serum Mg during low-risk pregnancies reported that both ionized and total serum Mg were significantly reduced after the 18th week of gestation compared to measurements before this time.[8]
Dietary intake studies during pregnancy consistently demonstrate that many women, especially those from disadvantaged backgrounds, have intakes of Mg below the recommended levels.[9]
Although present in grains, green vegetables, and seeds, insufficient Mg intake is common, especially in low-income regions. Adolescents and women are more prone to Mg deficiency.[10] It is recommended that women consume 280 mg of Mg/day,[11] increasing in pregnancy.[12] Most Mg (99%) is intracellular, such that serum levels have a low accuracy for Mg deficiency.[13] Total and ionized Mg++ are inversely associated with gestational age in pregnancy.[14] Mg deficiency in pregnancy has been associated with a higher risk of chronic HTN, preeclampsia, placental dysfunction, and premature labor.[15]
Adolescents and women are more prone to Mg deficiency.[10] It is recommended that women consume 280 mg of Mg/day,[11] increasing in pregnancy.[12] Most Mg (99%) is intracellular, such that serum levels have a low accuracy for Mg deficiency.[13] Total and ionized Mg++ are inversely associated with gestational age in pregnancy.[14] Mg deficiency in pregnancy has been associated with a higher risk of chronic HTN, preeclampsia, placental dysfunction, and premature labor.[15]
More recent data suggest that maternal Mg supplementation in pregnancy may have other perinatal benefits. Treatment was begun after 22 weeks’ gestation in most women and was sustained for a mean of about 28 days in both groups. The risk of the primary outcome of hypoxic-ischemic encephalopathy was nonsignificantly lower in the Mg++ group, but the overall event rate was lower than expected in both groups. Interestingly, the risk of third trimester stillbirth was lower in Mg group.[16]
In a retrospective study of medical records reported that Mg supplementation during pregnancy was associated with a reduced risk of fetal growth retardation and preeclampsia. [17]
[17]
In addition, there are many evidence that Mg supplementation during pregnancy may lead to prevent some pregnancy complications and improved many health indicators and pregnancy outcomes;[18,19,20,21,22,23] but as stated by others, there is not enough high-quality evidence to show that Mg supplementation during pregnancy is beneficial.[24]
Thus, according to the above mentioned, Mg supplementation during pregnancy may be able to reduce growth restriction of the fetus and preeclampsia (high blood pressure and protein in the urine during pregnancy) and increase birth weight. This study aimed to assess the effects of Mg supplementation on pregnancy outcome by randomized controlled trial with this dosage of Mg, In the previous studies, they use different dosage.
In this randomized controlled trial study, the required sample size was calculated as 60 patients in each group (totally 180 patients) using sample size formula to compare the two means’ value at 95% confidence level, the power of 80% and considering the standard deviation (SD) of serum Mg levels in the normal population which is about 1. 5 mg/dl and also taking into account the significant differences between the two groups as (d = 0.75).
5 mg/dl and also taking into account the significant differences between the two groups as (d = 0.75).
To continue the study, 180 pregnant women were recruited into three randomized groups. Maternal serum Mg levels of pregnant women with gestational age 12–14 weeks were measured and those whose serum Mg levels were < 1.9 mg/dl selected. Participants were randomized to treatment or control groups through random table numbers. Participants with Mg serum levels more than 1.9 mg/dl considered as control Group A randomly. They just received one multimineral tablet once a day until the end of pregnancy (N = 60). Participants with Mg levels < 1.9 consider as Group B and C. Participants in Group B received one multimineral tablet daily until the end of pregnancy (N = 60). Participants in Group C received 200 mg effervescent Mg tablet from Vitafit company once daily for 1 month, and also they consumed one multimineral tablet from Alhavi Company, that contains 100 mg Mg, once a day until the end of pregnancy (N = 60) [].
We compared the outcomes of pregnancy, including IUGR, preterm labor, maternal body mass index (BMI), neonatal weight, pregnancy-induced HTN, preeclampsia, GDM, cramps of the leg, and Apgar score between three groups.
Inclusion criteria were: have tendency to involve in this study and sign the agreement; single pregnancy; gestational age 12–14 weeks; lack of acute renal disease; hypomagnesemia in interventional group and normal Mg; lack of history chronic HTN; lack of history of overt diabetes; lack of history of severe anemia; lack of history of diagnostic heart disease; lack of anomaly in this pregnancy and previous ones; lack of use cigarette and alcohol; lack of molar pregnancy; lack of acute pancreatitis; multiparty.
Exclusion criteria were: withdrawal the study; inappropriate use of Mg; intractable vomiting.
Participants selected from the population that referred to hospital clinics. Individuals who fulfill the inclusion criteria invited to participate in this study. The trial protocol was in accordance with the Declaration of Helsinki and was approved by the Research and Ethics Committee of Isfahan University of Medical Sciences.
The trial protocol was in accordance with the Declaration of Helsinki and was approved by the Research and Ethics Committee of Isfahan University of Medical Sciences.
The trial was registered under trial registry code IRCT2015121925611N1 at the National Registry for Clinical Trials, which is a member of the World Health Organization. After providing detailed information, informed consent was signed by the participant, and oral assent from participants was obtained.
The Statistical Package for Social Sciences (SPSS) version 20.0 for Windows (SPSS, Chicago, IL, USA) was used for statistical analysis. Descriptive data were expressed as mean ± SD. Frequency tables were generated for relevant variables. Proportions were compared with the Pearson Chi-square test. A low Apgar score at 1 or 5 min was defined as a score of 7 or less. For comparisons of continuous variables in three groups, we used one-way analysis of variance (ANOVA). P < 0.05 was considered statistically significant.
The baseline characteristics of multiparous pregnant women in three groups were shown in . As shown in , no significant difference in all variables of the characteristics of the study population, except for a history of diabetes that was significantly different between three groups (P = 0.006).
Table 1
Baseline characteristics of study population
Open in a separate window
shows the standard weight gain according to BMI. For each group, we calculated difference weight in early of pregnancy and weight in delivery. Then, for all category of BMI in three groups, calculate the excess weight gain. Chi-square test did not show a significance difference between three groups, although the percentage of excess weight gain had different in three groups. The shown the excess weight gain in three groups of the study. Type of delivery and sex of neonate have been shown in .
Table 2
Standard weight gain according to body mass index
Open in a separate window
Open in a separate window
Excess weight gain in three groups of study
Table 3
Type of delivery and sex of neonate
Open in a separate window
shows the frequency of pregnancy outcomes between groups. We compared the frequency of IUGR, preterm birth, low birth weight (LBW), preeclampsia, GDM, cramps of the leg, Apgar score, stillbirth, and premature rupture of membranes with Pearson Chi-square test between three groups. A low Apgar score at 1 or 5 min was defined as a score of 7 or less. Furthermore, the mean weight of neonate between groups was assessed by one-way ANOVA. As shown in , in all pregnancy outcome, Group C that received effervescent Mg tablet plus multimineral tablet showed a better result than other groups and frequency of pregnancy complications as said above was fewer than the other two groups and demonstrated a significant difference.
We compared the frequency of IUGR, preterm birth, low birth weight (LBW), preeclampsia, GDM, cramps of the leg, Apgar score, stillbirth, and premature rupture of membranes with Pearson Chi-square test between three groups. A low Apgar score at 1 or 5 min was defined as a score of 7 or less. Furthermore, the mean weight of neonate between groups was assessed by one-way ANOVA. As shown in , in all pregnancy outcome, Group C that received effervescent Mg tablet plus multimineral tablet showed a better result than other groups and frequency of pregnancy complications as said above was fewer than the other two groups and demonstrated a significant difference.
Table 4
Frequency of pregnancy outcomes between groups
Open in a separate window
The present study showed the preventive effect of oral Mg tablet in the many of pregnancies with difficulty. Moreover, because this study set a normal group without hypo Mg, we found that hypo Mg may be a risk factor for some pregnancies with complications.
The results of the present study showed that Mg supplement administered to mothers’ antenatal leads to a reduction in many bad pregnancy outcomes. Many studies have examined the therapeutic or preventive effect of Mg in pregnancy outcomes, and some of them supported our findings. Czeizel et al., in agreement with our result, found that effect of periconceptional multivitamin on 5502 pregnant females was positive and increase fertility.[25] In addition, our results showed that IUGR was considerably reduced in oral Mg supplement groups compared with other two groups. Likewise, Roman et al. showed that maternal oral Mg supplementation reduced pregnancy-induced IUGR by 64% and suppressed cytokine/chemokine levels in the individual amniotic fluid and placentas.[26]
Today, the importance of Mg during pregnancy has been more understanding. Various studies focus on the effect of Mg on prevention or treatment of numerous pregnancy complications or pathological condition in pregnancy period. [24] Mg has an important role in homeostasis, enzyme system, and bone calcium stability.[27] As we found the beneficial effect of Mg on our oral mg supplement group such as decrease preeclampsia (P = 0.018), lower preterm birth (P = 0.044) as well as lower rate of LBW (P = 0.002), in the various clinical studies which were reviewed by Duley in 2010[28] and McDonald in 2012,[29] it has also been declared that efficiency of Mg during pregnancy is noticeable, and Mg prevents many bad effects in pregnant women, and Mg component like MgSO4 found to be efficient for preeclampsia and eclampsia.
[24] Mg has an important role in homeostasis, enzyme system, and bone calcium stability.[27] As we found the beneficial effect of Mg on our oral mg supplement group such as decrease preeclampsia (P = 0.018), lower preterm birth (P = 0.044) as well as lower rate of LBW (P = 0.002), in the various clinical studies which were reviewed by Duley in 2010[28] and McDonald in 2012,[29] it has also been declared that efficiency of Mg during pregnancy is noticeable, and Mg prevents many bad effects in pregnant women, and Mg component like MgSO4 found to be efficient for preeclampsia and eclampsia.
Our evaluation demonstrated that all pregnancy outcomes such as preeclampsia (P = 0.018), IUGR (P < 0.001), preterm birth (P = 0.044), LBW (P = 0.002), GDM (P = 0.003), cramps of leg (P < 0.001), Apgar score (under 7) (P = 0.006), birth weight (continuous) (P = 0.002), and Apgar (continuous) (P = 0. 01) was significantly better in Mg received group than control and multimineral tablet used groups. In accordance with our results, Shaikh et al. in his observational study found that in many pregnancy outcomes such as toxemia of pregnancy, preterm birth, Intra Uterine Growth Restriction (IUGR), and leg cramps, and pregnant women with hypo Mg have more frequent complications than normal groups.[30] Another investigation done by Doyle et al. demonstrated that Mg intakes of 513 women toward the end of the first trimester of pregnancy (300 mg/day) was associated with optimum birth weight, length, and head circumference.[31] We used 300 mg Mg pill for our Mg received group same as Doyle et al. did[31] although in the other studies they used various doses.[32] In addition, it would be beneficial for control group to administrate low-dose Mg.[32] We believe that the standard methodological usage should be created to use worldwide as the standard pattern as it recently has been noticed and discussed comprehensively.
01) was significantly better in Mg received group than control and multimineral tablet used groups. In accordance with our results, Shaikh et al. in his observational study found that in many pregnancy outcomes such as toxemia of pregnancy, preterm birth, Intra Uterine Growth Restriction (IUGR), and leg cramps, and pregnant women with hypo Mg have more frequent complications than normal groups.[30] Another investigation done by Doyle et al. demonstrated that Mg intakes of 513 women toward the end of the first trimester of pregnancy (300 mg/day) was associated with optimum birth weight, length, and head circumference.[31] We used 300 mg Mg pill for our Mg received group same as Doyle et al. did[31] although in the other studies they used various doses.[32] In addition, it would be beneficial for control group to administrate low-dose Mg.[32] We believe that the standard methodological usage should be created to use worldwide as the standard pattern as it recently has been noticed and discussed comprehensively. [33]
[33]
Mg is pivotal element for preventing some diseases during whole pregnancy. Mg has been stablished to be used for avoiding some unwanted condition. It could be used by food intake among pregnant women.[34,35,36] Furthermore, Mg has various physiological benefits. Numerous studies assessed the effect of Mg supplement in preventing of preeclampsia in pregnant women. Bullarbo et al. in a clinical trial designed study concluded that Mg supplementation prevents increasing of diastolic blood pressure during the last weeks of pregnancy.[37] Rudnecki et al. in a double-blind, randomized controlled study found that using Mg chloride until the end of pregnancy has a positive effect on decreasing of blood pressure during pregnancy and delivery time.[38] In agreement with them, we also found oral mg supplement group had lower rate of preeclampsia (P = 0.018). In addition, in a study by Dawson, the result showed that preeclampsia women had lower range of Mg compared to the nonpreeclampsia women. [18]
[18]
Our assessments revealed that Mg had a beneficial effect on preventing of LBW (P = 0.002). Similar to our findings, in a double-blind, randomized controlled study which was done on 985 pregnant women, using of Mg aspartate was beneficial for preventing of preterm light weight children and also preterm deliveries.[39] Other investigations also proved our result in term of low-weight delivery.[40]
Mg has a pivotal role in various body homeostasis, especially pregnancy period. Undoubtedly, the functioning of Mg in many different organs has already established. According to our result and other researchers’ findings, it should be said that Mg supplement during pregnancy could decrease the probability of occurrence of many complications of pregnancies. We believe that using the right dose of Mg plays a crucial role in the treatment of unwanted pregnancy disorders as well as preventing of preterm weight, LBW, and preeclampsia.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
1. Makrides M, Crosby DD, Bain E, Crowther CA. Magnesium supplementation in pregnancy. Cochrane Database Syst Rev. 2014;(4):C:CD000937. [PMC free article] [PubMed] [Google Scholar]
2. McNamara HC, Crowther CA, Brown J. Different treatment regimens of magnesium sulphate for tocolysis in women in preterm labour. Cochrane Database Syst Rev. 2015;12:CD011200. [PMC free article] [PubMed] [Google Scholar]
3. Zaloga GP. Interpretation of the serum magnesium level. Chest. 1989;95:257–8. [PubMed] [Google Scholar]
4. Mepba H, Eboh L, Banigo D. Effects of processing treatments on the nutritive composition and consumer acceptance of some Nigerian edible leafy vegetables. Afr J Food Agric Nutr Dev. 2007;7:1–18. [Google Scholar]
5. Rock CL, Lovalvo JL, Emenhiser C, Ruffin MT, Flatt SW, Schwartz SJ. Bioavailability of beta-carotene is lower in raw than in processed carrots and spinach in women. J Nutr. 1998;128:913–6. [PubMed] [Google Scholar]
1998;128:913–6. [PubMed] [Google Scholar]
6. Seelig MS. Magnesium Deficiency in the Pathogenesis of Disease: Early Roots of Cardiovascular, Skeletal, and Renal Abnormalities. Newyourk, Springer Science and Business Media. 1980 [Google Scholar]
7. Hurley L. Magnesium-deficiency in pregnancy and its effects on the fetus. Magnes Bull. 1981;3:202–8. [Google Scholar]
8. Arikan G, Guecer F, Schoell W, Weiss P. Preterm labour during oral magnesium supplementation in uncomplicated pregnancies. Geburtshilfe Frauenheilkd. 1997;57:491–5. [Google Scholar]
9. Luke B. Nutrition During Pregnancy: Part I, Weight Gain; Part II, Nutrient Supplements. JAMA. 1991;265(2):281–2. [Google Scholar]
10. King DE, Mainous AG, 3rd, Geesey ME, Woolson RF. Dietary magnesium and C-reactive protein levels. J Am Coll Nutr. 2005;24:166–71. [PubMed] [Google Scholar]
11. Becker W, Lyhne N, Pedersen AN, Aro A, Fogelholm M, Phorsdottir I, et al. Nordic nutrition recommendations 2004-integrating nutrition and physical activity. Scand J Nutr. 2004;48:178–87. [Google Scholar]
Scand J Nutr. 2004;48:178–87. [Google Scholar]
12. Young VR. Dietary Reference Intakes: For Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride. Washington (DC): National Academies Press; 1997. [Google Scholar]
13. Mittendorf R, Dambrosia J, Dammann O, Pryde PG, Lee KS, Ben-Ami TE, et al. Association between maternal serum ionized magnesium levels at delivery and neonatal intraventricular hemorrhage. J Pediatr. 2002;140:540–6. [PubMed] [Google Scholar]
14. Arikan GM, Panzitt T, Gücer F, Scholz HS, Reinisch S, Haas J, et al. Course of maternal serum magnesium levels in low-risk gestations and in preterm labor and delivery. Fetal Diagn Ther. 1999;14:332–6. [PubMed] [Google Scholar]
15. Wynn A, Wynn M. Magnesium and other nutrient deficiencies as possible causes of hypertension and low birthweight. Nutr Health. 1988;6:69–88. [PubMed] [Google Scholar]
16. Harrison V, Fawcus S, Jordaan E. Magnesium supplementation and perinatal hypoxia: Outcome of a parallel group randomised trial in pregnancy. BJOG. 2007;114:994–1002. [PubMed] [Google Scholar]
BJOG. 2007;114:994–1002. [PubMed] [Google Scholar]
17. Conradt A, Weidinger H, Algayer H. On the role of magnesium in fetal hypotrophy, pregnancy induced hypertension, and pre-eclampsia. Magnes Bull. 1984;6:68–76. [Google Scholar]
18. Dawson EB, Evans DR, Kelly R, Van Hook JW. Blood cell lead, calcium, and magnesium levels associated with pregnancy-induced hypertension and preeclampsia. Biol Trace Elem Res. 2000;74:107–16. [PubMed] [Google Scholar]
19. Dasgupta S, Ghosh D, Seal SL, Kamilya G, Karmakar M, Saha D. Randomized controlled study comparing effect of magnesium sulfate with placebo on fetal umbilical artery and middle cerebral artery blood flow in mild preeclampsia at=34 weeks gestational age. J Obstet Gynaecol Res. 2012;38:763–71. [PubMed] [Google Scholar]
20. Crowther CA, Brown J, McKinlay CJ, Middleton P. Magnesium sulphate for preventing preterm birth in threatened preterm labour. Cochrane Database Syst Rev. 2014;4:CD001060. [PubMed] [Google Scholar]
21. Ariza AC, Bobadilla N, Fernández C, Muñoz-Fuentes RM, Larrea F, Halhali A. Effects of magnesium sulfate on lipid peroxidation and blood pressure regulators in preeclampsia. Clin Biochem. 2005;38:128–33. [PubMed] [Google Scholar]
Ariza AC, Bobadilla N, Fernández C, Muñoz-Fuentes RM, Larrea F, Halhali A. Effects of magnesium sulfate on lipid peroxidation and blood pressure regulators in preeclampsia. Clin Biochem. 2005;38:128–33. [PubMed] [Google Scholar]
22. Alves JG, de Araújo CA, Pontes IE, Guimarães AC, Ray JG. The BRAzil MAGnesium (BRAMAG) trial: A randomized clinical trial of oral magnesium supplementation in pregnancy for the prevention of preterm birth and perinatal and maternal morbidity. BMC Pregnancy Childbirth. 2014;14:222. [PMC free article] [PubMed] [Google Scholar]
23. Abdul MA, Nasir UI, Khan N, Yusuf MD. Low-dose magnesium sulphate in the control of eclamptic fits: A randomized controlled trial. Arch Gynecol Obstet. 2013;287:43–6. [PubMed] [Google Scholar]
24. Spatling LU, Spatling GA. Magnesium supplementation in pregnancy. A double-blind study. Br J Obstet Gynaecol. 1988;95(2):120–5. [PubMed] [Google Scholar]
25. Czeizel AE, Dudás I, Métneki J. Pregnancy outcomes in a randomised controlled trial of periconceptional multivitamin supplementation. Final report. Arch Gynecol Obstet. 1994;255:131–9. [PubMed] [Google Scholar]
Final report. Arch Gynecol Obstet. 1994;255:131–9. [PubMed] [Google Scholar]
26. Roman A, Desai N, Rochelson B, Gupta M, Solanki M, Xue X, et al. Maternal magnesium supplementation reduces intrauterine growth restriction and suppresses inflammation in a rat model. Am J Obstet Gynecol. 2013;208:383.e1–7. [PubMed] [Google Scholar]
27. de Baaij JH, Hoenderop JG, Bindels RJ. Magnesium in man: Implications for health and disease. Physiol Rev. 2015;95:1–46. [PubMed] [Google Scholar]
28. Duley L, Gülmezoglu AM, Henderson-Smart DJ, Chou D. Magnesium sulphate and other anticonvulsants for women with pre-eclampsia. Cochrane Database Syst Rev. 2010;11:CD000025. [PMC free article] [PubMed] [Google Scholar]
29. McDonald SD, Lutsiv O, Dzaja N, Duley L. A systematic review of maternal and infant outcomes following magnesium sulfate for pre-eclampsia/eclampsia in real-world use. Int J Gynaecol Obstet. 2012;118:90–6. [PubMed] [Google Scholar]
30. Shaikh K, Das CM, Baloch GH, Abbas T, Fazlani K, Jaffery MH, et al. Magnesium associated complications in pregnant women. World Appl Sci J. 2012;17:1074–8. [Google Scholar]
Magnesium associated complications in pregnant women. World Appl Sci J. 2012;17:1074–8. [Google Scholar]
31. Doyle W, Crawford MA, Wynn AH, Wynn SW. Maternal magnesium intake and pregnancy outcome. Magnes Res. 1989;2:205–10. [PubMed] [Google Scholar]
32. Franz KB. Magnesium intake during pregnancy. Magnesium. 1987;6:18–27. [PubMed] [Google Scholar]
33. Liu FL, Zhang YM, Parés GV, Reidy KC, Zhao WZ, Zhao A, et al. Nutrient intakes of pregnant women and their associated factors in eight cities of China: A cross-sectional study. Chin Med J (Engl) 2015;128:1778–86. [PMC free article] [PubMed] [Google Scholar]
34. Schoenaker DA, Soedamah-Muthu SS, Mishra GD. The association between dietary factors and gestational hypertension and pre-eclampsia: A systematic review and meta-analysis of observational studies. BMC Med. 2014;12:157. [PMC free article] [PubMed] [Google Scholar]
35. Sibai BM, Villar MA, Bray E. Magnesium supplementation during pregnancy: A double-blind randomized controlled clinical trial. Am J Obstet Gynecol. 1989;161:115–9. [PubMed] [Google Scholar]
Am J Obstet Gynecol. 1989;161:115–9. [PubMed] [Google Scholar]
36. Rylander R, Vormann J. Magnesium intervention studies-methodological aspects. Magnes Res. 2015;28:75–8. [PubMed] [Google Scholar]
37. Bullarbo M, Ödman N, Nestler A, Nielsen T, Kolisek M, Vormann J, et al. Magnesium supplementation to prevent high blood pressure in pregnancy: A randomised placebo control trial. Arch Gynecol Obstet. 2013;288:1269–74. [PubMed] [Google Scholar]
38. Rudnicki M, Frölich A, Rasmussen WF, McNair P. The effect of magnesium on maternal blood pressure in pregnancy-induced hypertension. A randomized double-blind placebo-controlled trial. Acta Obstet Gynecol Scand. 1991;70:445–50. [PubMed] [Google Scholar]
39. Kovács L, Molnár BG, Huhn E, Bódis L. Magnesium substitution in pregnancy. A prospective, randomized double-blind study. Geburtshilfe Frauenheilkd. 1988;48:595–600. [PubMed] [Google Scholar]
40. Zarcone R, Cardone G, Bellini P. Role of magnesium in pregnancy. Panminerva Med. 1994;36:168–70. [PubMed] [Google Scholar]
1994;36:168–70. [PubMed] [Google Scholar]
Benefits of Magnesium During Pregnancy
Benefits of Magnesium During Pregnancy - NatalistHome > Learn > Pregnancy > >Benefits of Magnesium During Pregnancy
Feb 01, 22 ● 5 min
Taking magnesium during pregnancy can have multiple benefits. Read on to learn how this supplement can help.
By OBGYN and fertility expert Dr. Kenosha Gleaton
Supplementing with just one important mineral (on top of your prenatal daily packets) may increase your chances of having a healthy pregnancy. From helping prevent high blood pressure to helping with the adverse effect of muscle cramps, oral magnesium supplementation is something to explore. Let's break down what the relationship between magnesium and pregnancy is and how it works.
What is magnesium?
Magnesium is a mineral found in many foods including nuts, seeds, grains, greens, and beans and is necessary for a healthy, functioning body. Magnesium is important for maintaining normal blood pressure, protein synthesis, muscle and nerve function, and much more. About half of the magnesium in an adult body is found in the bones and the other half is in soft tissues.
Magnesium is important for maintaining normal blood pressure, protein synthesis, muscle and nerve function, and much more. About half of the magnesium in an adult body is found in the bones and the other half is in soft tissues.
What pregnancy ailments can magnesium help remedy?
Maintaining a healthy and adequate magnesium level can be important for a pregnant woman, but how exactly does it help? A 2017 randomized control trial found that supplementing magnesium while pregnant may help reduce some pregnancy complications such as preeclampsia, low preterm weight, and low birthweight and may reduce the risk of stillbirth. Specifically, this study showed that:
- Magnesium supplementation shows to be especially beneficial during pregnancy as women are a high risk group for magnesium deficiency. Other high risk groups include individuals with gastrointestinal diseases, type 2 diabetes, alcohol dependence, and older adults.
- Magnesium supplementation shows better pregnancy outcomes by reducing the risk of stillbirth, fetal growth restrictions, and preeclampsia, a blood pressure condition developed during pregnancy.

- Some magnesium compounds such as magnesium sulfate are especially effective at preventing preeclampsia.
- In the trial, the group that received a 300mg effervescent magnesium tablet once a day for one month showed the best pregnancy outcomes and experienced reduced pregnancy complications.
Shop other Pregnancy Products For Expectant Mothers
✨Shop Magnesium Plus Drink Mix ✨
Other benefits of magnesium supplementation during pregnancy
By now you know some of the benefits associated with a sufficient magnesium level. However, not only is magnesium great for bone, muscle, cardiovascular health, and pregnancy outcomes, there are other benefits associated with magnesium supplementation.
- Boosts mood: Magnesium acts as a coenzyme that helps to convert tryptophan to serotonin, a mood boosting neurotransmitter. While there is some conflicting data, research supports the notion that magnesium supplementation may be beneficial for boosting mental health and helping to prevent postpartum depression and anxiety.

- Helps with sleep: Magnesium’s NMDA antagonist activity along with its GABA receptor work to provide the body with a relaxant effect, helping you to de-stress and get a good night’s sleep. Find more ways to relieve stress during pregnancy
- Supports bone health: Magnesium is helpful for bone structure development, important for mom and the growing baby.
- Helps with cramping: Some research shows that magnesium supplementation may be helpful for leg cramps in pregnant women, although more research is needed to confirm these claims.
- Aids in hydration: Magnesium’s chemical properties make it an essential mineral for hydration. Potassium is a must for hydration, and without magnesium stores, our body would be unable to hold on to potassium as needed.
Upper limits of magnesium
According to the NIH, the upper limits for magnesium are:
- Birth to 12 months: no dosage established
- 1-3 years: 65mg
- 4-8 years: 110mg
- 9-18 years (includes pregnant and lactating females): 350mg
- 19+ years (includes pregnant and lactating females): 350mg
Natalist Magnesium Plus drink mix contains 300mg per serving (and tastes delicious)
Medication interactions
It is important to note that some medicines may interact poorly with magnesium. Some examples include:
Some examples include:
- Oral bisphosphonates
- Various antibiotics
- Loop diuretics
- Proton pump inhibitors
For specifics on medication interactions, consult with your doctor.
Find more blog posts and products for pregnancy, supplements, and fertility on the Natalist homepage.
Take-aways
- Magnesium is a naturally occurring mineral that is essential for many bodily functions including protein synthesis, muscle and nerve function, and blood pressure homeostasis.
- Supplementing with magnesium shows many benefits during pregnancy including a reduced risk of preeclampsia, stillbirth, low birth weight, and fetal growth restriction.
- Magnesium supplementation also aids in sleep, supports bone health, helps with muscle cramps, and has mood-boosting properties.
- There are upper limits for magnesium supplementation, so make sure to stay at or below healthy limits if you do decide to take a magnesium supplement.
- Some groups are at a higher risk for magnesium deficiency.
Featured Image by ready made
Shop Products From This Article
Subscribe & Save $3.00
Magnesium Plus
Pregnancy-safe drink mix to support relaxation‡
$35 $32
Subscribe & Save $5.00
Prenatal Daily Packets
Vegan prenatal daily packets
$60 $55
Share on:
Related Blogs
Pregnancy 4 min
Gift Guide for Expectant Mamas
Read MorePregnancy 8 min
Can I Use Botox While TTC, Pregnant, or Breastfeeding?
Read MorePregnancy 3 min
What Does a Positive Pregnancy Test Strip Look Like?
Read MorePregnancy 4 min
5 Reasons Why We Developed Prenatal Gummies
Read MoreShop Products
Subscribe & Save $3. 00
00
Magnesium Plus
Pregnancy-safe drink mix to support relaxation‡
$35 $32
Subscribe & Save $5.00
Prenatal Daily Packets
Vegan prenatal daily packets
$60 $55
Subscribe & Save $3. 00
00
Prenatal Gummies
Doctor-formulated & delicious prenatal gummies
$29 $26
Shop All
Subscribe & Save $4.00
Postnatal Vitamin
Nutritional & energy boost for breastfeeding‡
$40 $36
Subscribe & Save $8. 00
00
Magnesium & Multi Pack
Bundle & save on top sellers
$85 $77
Subscribe & Save $15.00
Trimester Pack: Prenatal Daily Packets
A full trimester worth of prenatals at a great price
$165 $150
Subscribe & Save $5. 00
00
Prenatal Daily Packets
Vegan prenatal daily packets
$60 $55
Shop All
Shop All
Sign Up For 10% Off Your First Order!
Sign up for insider access, exclusive deals, and OBGYN insights!
is prescribed for what, how much to drink and how to take magnesium during pregnancy?
Participates in all energy processes, activates enzymes, regulates blood pressure, normalizes the functioning of the nervous system and performs a number of other useful functions. All this is about one of the most important macronutrients for our body - magnesium. It is not difficult to guess that with its shortage, it is unlikely that health problems will be avoided. And of course, it is especially important to monitor the balance of this mineral for pregnant women, because the formation and development of the fetus depends on the well-being of the expectant mother. At the same time, it is worth considering that magnesium is not synthesized in the body - it comes from outside with food and water. In addition, special drugs can be prescribed to prevent and correct magnesium deficiency.
At the same time, it is worth considering that magnesium is not synthesized in the body - it comes from outside with food and water. In addition, special drugs can be prescribed to prevent and correct magnesium deficiency.
In the article we will tell you why pregnant women are prescribed magnesium and how to take such drugs.
Normally, the magnesium content in the body is only 0.027% of a person's body weight. It would seem that such an insignificant amount and at the same time a colossal value for health! Getting into the cell, the macroelement changes its permeability and excitability: this is how the cell gets the opportunity to respond to external impulses. Thanks to the work of 500 magnesium-dependent proteins and 300 enzymes, energy reserves at the cellular level are replenished, proteins and nucleic acids are formed (the basis of DNA and RNA for storing genetic information), muscle cells contract, the functioning of the nervous system and active biological substances responsible for stress are regulated ( catecholamines).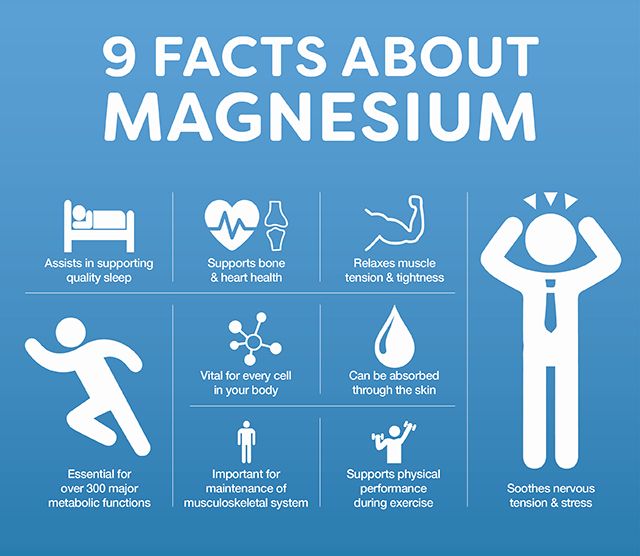
During pregnancy, a woman's body undergoes great changes. Take, for example, the fact that the mass of the uterus increases from 100 to 1000 grams. But every month the fetus grows. Therefore, it is obvious that the need for magnesium is increasing, which is involved in the development of all tissues, organs and systems of the unborn child [1].
Note
The optimal daily dose of magnesium for women is 280 mg, while the norm of magnesium during pregnancy and lactation is already 360–400 mg[2] .
The greatest need for magnesium is experienced by intensively working organs with a large number of mitochondria - intracellular "batteries" responsible for energy accumulation. These organs include the placenta, uterus, brain, heart, and muscle tissue. Therefore, with the development of magnesium deficiency, they suffer first.
Acting at the cellular level, magnesium during pregnancy:
- ensures the full development of the fetus;
- contributes to the maintenance of normal uterine tone;
- relieves symptoms of irritability and improves mood;
- helps promote healthy sleep;
- reduces the risk of seizures.

When a mother-to-be needs extra magnesium intake
It is difficult to detect magnesium deficiency with the help of tests. Existing physicochemical methods, such as atomic absorption spectroscopy, colorimetry, enzymatic analysis, fluorometry, cannot be called fast and accurate [3]. Therefore, the lack of an element is more often recognized by the symptoms [4]. Moreover, two types of violations are distinguished:
- quick that are immediately noticeable. These include irritability, convulsions, and arrhythmia. The fact is that with a lack of magnesium, muscle and nerve cells are constantly in a state of increased excitability. This leads to emotional instability, mood swings, excessive muscle contractions. Convulsions often occur in the calf muscles, and in the heart - excessive contractions are manifested by heart rhythm disturbances, or arrhythmia. Increased excitability of vascular smooth muscle cells leads to sudden changes in blood pressure, headache and fatigue [5].
 Violations in the contraction of the muscle cells of the uterus create a threat of premature contractions and childbirth [6];
Violations in the contraction of the muscle cells of the uterus create a threat of premature contractions and childbirth [6]; - appearing after a time . The consequences of prolonged magnesium deficiency, the main regulator of energy metabolism and protein formation, are especially dangerous for the fetus. This threatens with malnutrition (lack of body weight), slowing intrauterine growth. In addition, in the future, the child has an increased risk of developing diabetes and cardiovascular diseases.
Lack of magnesium during pregnancy increases the risk of developing diabetes in the mother. In addition, the elasticity of the connective tissue depends on the macroelement, therefore, with its deficiency, stretch marks appear more often in pregnant women, and perineal ruptures are possible during childbirth.
Stress and irritability are also consequences of magnesium deficiency. Pregnancy is a test for the body due to the heavy load on organs and systems. To cope with stress, catecholamines are actively produced during this period. In large quantities, they pose a threat to the fetus, as they narrow the blood vessels in the placenta and impede the flow of nutrients. A sufficient amount of magnesium reduces such negative effects, increases resistance to stress, having a positive effect on the condition of the mother and child [7].
To cope with stress, catecholamines are actively produced during this period. In large quantities, they pose a threat to the fetus, as they narrow the blood vessels in the placenta and impede the flow of nutrients. A sufficient amount of magnesium reduces such negative effects, increases resistance to stress, having a positive effect on the condition of the mother and child [7].
Thus, when planning and carrying a pregnancy, it is imperative to monitor the balance of magnesium. As we have already said, an element can enter the body with food or as part of drugs. As for the first method, it is difficult even for a non-pregnant woman to get the daily intake of magnesium from food alone. And with an increased need for an element, this is simply impossible, so doctors prescribe special preparations with magnesium.
This is important
Studies have shown that the use of magnesium during pregnancy (from the fourth to fifth week) reduces the rate of spontaneous miscarriages [8].
Rules for taking medications
Products with magnesium are divided into two categories:
- non-drug products are dietary supplements and vitamin-mineral complexes. The amount of magnesium in them is much lower than the daily value, so they are not suitable for treating a deficiency of the element and are generally not recommended for use during pregnancy and for children. The use of such funds is justified only for healthy people with errors in nutrition [9];
- medicines containing a fixed daily dose of magnesium - these are prescribed during pregnancy.
Like any medicine, magnesium preparations are prescribed by a doctor: self-medication is unacceptable and can harm both mother and baby. Recommendations for admission are described in the instructions for each specific drug, however, the specialist can adjust the course and dosage - if required by the individual characteristics of the patient's body.
It should be noted that magnesium is better absorbed in combination with vitamin B6, or pyridoxine. Thanks to pyridoxine, the mineral enters the cells and remains in them longer. In addition, B6 deficiency and magnesium deficiency often co-occur [10], so specialists may prescribe both at the same time.
Thanks to pyridoxine, the mineral enters the cells and remains in them longer. In addition, B6 deficiency and magnesium deficiency often co-occur [10], so specialists may prescribe both at the same time.
Carrying a fetus is a big burden on a woman's body. At the same time, the formation and development of the fetus depends on the state of health of the expectant mother. Therefore, during pregnancy, it is especially important to monitor the balance of nutrients in the body.
Answers to questions. Borovkova E.I.
Ekaterina Igorevna Borovkova Professor:
– What is the most effective use of magnesium during pregnancy, as a tocolytic or for nutritional support and nutrition? Thanks for the question, but there are two completely different indications for prescribing magnesium supplements. That is, if the threat of preterm birth develops, we prescribe magnesium preparations for tocolysis and use them only in the form of intravenous infusions. If we want to replenish the patient's diet with you and supplement it with magnesium preparations, then we will use the tablet forms of the drug with you and achieve the necessary desired effectiveness with you. Accordingly, the effective use of magnesium preparations in parenteral forms for acute and massive tocolysis has been proven, and the effectiveness of the use of magnesium preparations in tablet mode for the prevention of preeclampsia, for the prevention and treatment of threatened miscarriage, and for the nutritional support of patients with obesity and gestational diabetes has been proven.
What dosage of magnesium is preventive? Preventive, according to available studies, including studies in 33 countries - from 300 to 500 milligrams of magnesium were prescribed per day in tablets and the high effectiveness of the drug was shown. In accordance with this, it is recommended to use the average daily dose, which we calculate from the mass of patients. On average, this is about 300-400 milligrams of magnesium, depending on the mass. If we talk about magnesium preparations, which we most widely use, then in Russia the use of Magne B6 preparations is most common due to the fact that it also contains Pyridoxine, which also has a beneficial effect on the course of pregnancy. So, when using Magne B6 preparations, we recommend using Magne B6 Forte, since by prescribing only 3 tablets per day, we achieve exactly the daily required dosage. If using Magne B6 is easy, there should be 4 to 6 tablets. Another very important remark: Magne B6 Forte contains magnesium citrate. The use of citrate forms both improves absorption and improves the stabilization of some metabolic processes, and restores the sensitivity of insulin receptors.
Is it possible to take magnesium throughout the pregnancy, are there any contraindications? Individual intolerance may be one of the contraindications. When prescribing drugs in a daily dosage, as a rule, we do not achieve any overdoses and, in general, side effects are practically not expressed. But any medicine that we prescribe during pregnancy must be justified. That is, we cannot just give you a magnesium preparation just like that. That is, if a woman is at risk for developing preeclampsia, we substantiate this in history and can prescribe magnesium preparations to her. If the patient has a history and habitual miscarriage, in order to prevent miscarriage or premature birth, we can also prescribe her throughout her pregnancy. However, the prescription of parenteral drugs requires mandatory monitoring of diuresis, respiratory rate and knee jerk, since we can cause an overdose of magnesium, and an overdose is possible only when magnesium is administered parenterally. That is, tablet forms will not lead to an overdose of magnesium.
Is it possible to consider magnesium deficiency in a woman's body as the central cause of chronic miscarriage? I think not. It is possible that magnesium deficiency can contribute to the manifestation of abortion, but, of course, all over the world it is believed that the main causes of miscarriage, that is, early termination of pregnancy, are infectious pathology, gene and chromosomal abnormalities and endocrine pathologies. These are the main reasons, after all, not magnesium deficiency. Although he can, of course, join them and aggravate the situation.
Should magnesium supplements be included in the list of therapeutic recommendations for metabolic syndrome? Yes. And such recommendations abroad already exist. And all patients who are undergoing therapy for obesity or with a detected metabolic syndrome, they, as a rule, being on some limited diet, are required to receive multivitamin preparations, which also include magnesium, including in a small dosage, but present. Separately prescribe magnesium preparations in the treatment of patients with metabolic syndrome - I have not seen such studies that such preparations were prescribed separately, but if we talk about pregnant patients with metabolic syndrome, then for such patients we really prescribe magnesium preparations separately from multivitamins, but not so much, how much for the treatment and correction of metabolic abnormalities, and how much to prevent the aggravation of the development of insulin resistance, to prevent and reduce the likelihood of preterm birth or preeclampsia. Because women with metabolic syndrome, they develop placental insufficiency in more than 80% of cases, preeclampsia - in 50%, premature birth - about 62%, that is, these are patients who are colossally threatened by the development of these complications.
Pregnancy has been turned into a disease. Does everyone need so many drugs? Thank you for this question! You know, when managing pregnant patients, I always tell them that pregnancy is not a disease. That is, almost all patients who do not have any serious extragenital diseases are treated with a minimum prescription of drugs. Fortunately, according to the order, which is also valid and working in Russia, we prescribe no more than 4 medicines at a time during pregnancy, which include multivitamins. That is, if we prescribe a multivitamin and magnesium preparations, then we will have only 2 drugs left for medicines. Therefore, of course, no, no extra medicines are needed. And all the drugs that we prescribe are justified according to strict indications.
If the daily requirement for calcium covers one glass of milk, then what product contains the daily requirement of magnesium? This is very arbitrary about calcium, this test program was developed in the USA, and they tested it according to a glass of milk in order to simplify the identification of patients who are not receiving calcium. Everything is more complicated with magnesium, because it is very difficult to estimate the concentration of magnesium even in the human body, because, in general, it is contained in so many protein structures, and it is difficult to say which product. I find it difficult to answer.
Vladimir Trofimovich Ivashkin Academician of the Russian Academy of Medical Sciences, Doctor of Medical Sciences:
- Probably a bunch of parsley.
Borovkova E.I. :
– Not only dairy products.
Elena Sergeevna Akarachkova Doctor of Medical Sciences:
- Goat's milk covers the daily requirement of magnesium. But goat's milk must be fresh.
Borovkova E.I. :
– Will it be digested in the intestines? Is there intolerance? In principle, with a balanced diet, if the patient receives a sufficient amount of protein and carbohydrates, she, in theory, will receive the necessary dose of magnesium. Another thing is that during pregnancy, the concentration of magnesium in the uterus must increase a thousandfold in order for it to be in a relaxed state. In this regard, the general recommendations are such that we prescribe either as part of a multivitamin or as part of a monopreparation of an additional magnesium agent. Thank you very much for this question.
Ivashkin V.T. :
- Thank you very much, Ekaterina Igorevna, that you, from the standpoint of high science, shed light on a process known to mankind for centuries. This is the first. And secondly, do you remember how one of the heroes of Molière's "The Philistine in the Nobility" found out with surprise that he had been speaking prose all his life? Today we learned with you one more important truth, that after all, pregnancy is not a disease.