How long should i keep my child rear facing
How Long Should You Keep Your Child Rear Facing in a Car Seat? – Cleveland Clinic
As a parent, you celebrate each milestone your child achieves — sitting up, crawling, taking first steps and saying their first word. But graduating to a front-facing car seat? That’s one such milestone that shouldn’t be rushed, according to guidelines from the American Academy of Pediatrics (AAP).
For years, parents have learned that keeping their child rear-facing in a car seat until age 2 is the best practice. But that recommendation has since been updated and now suggests that parents keep their children in rear-facing seats for as long as possible.
Purva Grover, MD, Director of Cleveland Clinic Children’s Pediatric Emergency Departments, says a child in a rear-facing seat has less risk for serious (or fatal) injury if involved in a crash.
“Because of the way their head and neck is positioned, when there is a big car crash involving a massive force — if they were to be front-facing, the positioning of the head and neck would give them bad whiplash, and with small children, it could actually cause much more damage,” Dr. Grover explains.
Types of rear-facing seats
There are a few options when it comes to rear-facing seats.
All-in-one seats
As the name implies, all-in-one seats have multiple uses. They can be used as a booster seat, a rear-facing seat or a forward-facing seat. However, they should only be used for car rides. All-in-one seats don’t have handles or bases. They’re also much larger in size and have higher weight and height limits than other styles of rear-facing seats. If you decide to buy an all-in-one car seat, make sure it’ll fit in your car when it’s rear-facing as it’s a bigger seat.
Convertible seats
With these seats, you can start off using them as rear-facing and then transition to forward-facing when your child outgrows the weight and height limits for rear-facing seats. Convertible seats tend to be larger than rear-facing seats and they don’t have carrying handles or bases. They also tend to have a five-point harness that attaches between the legs and at the hips and shoulders.
Advertising Policy
Rear-facing only seats
These seats are small and can carry infants between 22 and 35 pounds or 26 and 35 inches. Rear-facing only seats tend to have a base that stays in the car. However, rear-facing seats should only be used for travel and not for sleep or feeding times.
Rear-facing car seat guidelines for installation
Here are a few things to keep in mind when placing a rear-facing car seat in your vehicle.
Make sure the harness is in the right place
The car seat harness should be at or below your little one’s shoulders. Once situated, it should be snug. The harness’ chest clip should be in the middle of your child’s chest and lined up with their armpits.
Don’t place the seat in front of an active airbag
If the airbag for the front passenger’s seat is active, don’t put a rear-facing car seat there. Doing this could lead to serious injuries or even death. The reason being is if the airbag inflates, it’ll knock the car seat into your child’s head or worse.
Make sure the seatbelt is attached correctly
For rear-facing convertible or all-in-one seats, make sure the seat belt or lower anchor webbing is in the correct belt path. If you’re not sure, review the instructions.
Check the car seat’s angle after installation
To ensure that your child’s head doesn’t flop around, refer to the manual for the right seat angle. Once you find it, adjust the seat as needed.
Advertising Policy
If you need help with car seat installation, a Child Passenger Safety Technician (CPST) can make sure that it’s properly secured and ready for use.
When can you turn the car seat forward?
According to the AAP and the National Highway Traffic Safety Administration (NHTSA), children up to 3 years old should stay in a rear-facing car seat until they reach the top height or weight limit suggested by the car seat’s manufacturer. When your child hits one of these limits, they can ride in a forward-facing car seat with a harness and tether.
The best way to protect your child
According to the Centers for Disease Control and Prevention (CDC), car accidents are a leading cause of death for children in the U.S. In 2019, more than 600 children age 12 and younger died in motor vehicle crashes, and more than 91,000 were injured.
However, the CDC also states that car seat use reduces the risk for injury in crashes by 71% to 82% for children, when compared with seat belt use alone.
The updated recommendations also say that once a car seat has been turned around, it should remain forward-facing until your child reaches the seat’s weight and length limits. Then, your child should start using a booster seat. Children who exceed booster seat limits should use a lap and shoulder seat belt in the back seat of the car until they’re 13 years old.
Convenience shouldn’t come before safety
Dr. Grover agrees with the recommendations and says that when it comes to minimizing injury risk, safety should always come before convenience. She adds that it’s important for pediatricians to talk to parents about the guidelines and explain why they’re in place. The complete recommendation is available through the American Academy of Pediatrics.
She adds that it’s important for pediatricians to talk to parents about the guidelines and explain why they’re in place. The complete recommendation is available through the American Academy of Pediatrics.
The Car Seat LadyWhen Should Your Child Turn Forward-Facing?
- Rear-Facing: It's Not Just for Babies Anymore
The nation’s top scientists, researchers, and physicians recommend that kids sit rear-facing in the car for as long as possible, because rear-facing is safer. Here’s why your 2, 3, 4 or even 5 year old should be riding rear-facing.
The American Academy of Pediatrics (AAP) has for 20+ years recommended keeping kids rear-facing until they are too big for rear-facing in their convertible seat. The AAP reiterated this in their 2018 policy statement.
The National Highway Traffic Safety Administration (NHTSA) also updated their recommendations, now specifying that children remain rear-facing until reaching “the top height or weight limit allowed by your car seat’s manufacturer. ”
”
The main questions we get concerning extended rear-facing have to do with WHY it’s safer, and HOW bigger kids can stay comfortable rear-facing (jump there now). It’s a big topic but we’ve tried to address it clearly and thoroughly here. Please let us know if you have questions about this critical safety issue!
Crash Simulation: Why rear-facing is safer
At a trade show, The Car Seat Lady used a crash simulator. She wore a heavy helmet to mimic the size and weight of a child’s head to really get a full body experience. Watch to see what happens and how she tolerates the different positions, and listen to her excellent description of why rear-facing is safer.
Crash Test: See how rear-facing is safer
This video shows two 12-month-old crash test dummies each secured in the same car seat. One seat is rear-facing and one is forward-facing. Watch how much the forward-facing dummy’s head and neck move! Remember that this video is slowed down tremendously since crashes happen faster than the blink of an eye. For more on the physics behind why rear-facing is safer, see here.
For more on the physics behind why rear-facing is safer, see here.
What was going on in those crash test videos?
What is so bad about how the forward-facing dummy moved?
In a crash everyone moves towards the point of impact, so in a frontal crash everyone moves toward the front of the car. If you’re forward-facing in a car-seat or a seat belt, your upper body stops quickly because the chest strap on the car seat or the seat belt holds you back. However, your head doesn’t stop as quickly! Instead, it moves all the way forward until your chin touches your chest, and then goes all the way back. It whips forward and back in the blink of an eye (and is called whiplash).
Since an adult’s head is just 6% of their body weight, you can withstand having your head pulled violently away from your body. You will be sore for a few days, but you hopefully won’t have any lasting injury.
It’s quite different for a newborn, whose head is a whopping 25% of its body. This means that if a newborn were forward-facing in a frontal crash, their head would pull forward with four times as much force as would an adult’s!
This means that if a newborn were forward-facing in a frontal crash, their head would pull forward with four times as much force as would an adult’s!
Strength and rigidity of the bones in the spine also contribute to how well you can tolerate your head being pulled forward and back in a crash. The bones of an infant’s spine are made up of soft, stretchy cartilage. The ligaments that connect these cartilaginous bones are also underdeveloped and stretchy. Scientists have found that a newborn’s spinal column (bones + ligaments) can stretch up to 2 inches, whereas the spinal cord inside can stretch only 1/4 of an inch. If the spinal cord is forced to stretch more than it can, it breaks, leaving the baby paralyzed or worse.
Children are not just smaller adults; their bodies are differently proportioned and structured, and this difference affects their ability to tolerate the whiplash motion.
Physics: How rear-facing works to avoid injury in a crash
In a frontal crash, when everyone moves to the point of impact–the front of the car–a rear-facing baby will move in a different way. A rear-facing baby will move into the back of his car seat and will slide gently up the car seat. This allows the back of the car seat to absorb the brunt of the impact and distribute the remaining forces along the child’s entire back, which is the strongest part of his body. The most important part: because he sits rear-facing, the child’s head, neck, and torso all move together in a straight line. The whiplash motion is avoided totally.
A rear-facing baby will move into the back of his car seat and will slide gently up the car seat. This allows the back of the car seat to absorb the brunt of the impact and distribute the remaining forces along the child’s entire back, which is the strongest part of his body. The most important part: because he sits rear-facing, the child’s head, neck, and torso all move together in a straight line. The whiplash motion is avoided totally.
What about rear-facing in a rear-end crash?
A recent study looked at rear-facing car seats in rear impacts. They study found that rear-facing car seats mitigate and manage crash forces in a variety of ways that allow them to provide good protection for rear-facing kids. This finding is backed up by epidemiological and field data which also show that real kids riding rear-facing in real rear-end crashes typically do very well.
What about their legs?
Won't my child's legs be injured?
Is my child comfortable with their legs like that?
We get A LOT of questions about rear-facing kids’ legs! We want to assure you that no, their legs will not be injured, and yes, they are quite comfortable with their legs like that.
There are ZERO documented cases of rear-facing children breaking their legs, hips, feet, etc., due to their feet touching the back of the vehicle seat. In fact, studies show that forward-facing kids suffer many more leg injuries than rear-facing kids. The leg injuries to forward-facing children occur when the child’s legs fly up and hit the back of the front seat as the child and car seat are moving forward. This traps the child’s legs, putting tremendous pressure into the leg bones. This pressure can break the legs.
This traps the child’s legs, putting tremendous pressure into the leg bones. This pressure can break the legs.
Instead of worrying about a rear-facing child’s legs, we should be worrying about a forward-facing child’s head and neck! Notice how the forward-facing child’s head and neck are thrown forward in the video (snug straps only hold the chest back, not the head & neck), whereas the rear-facing child’s head and neck are cradled within the shell of the car seat. The forward-facing child’s head being thrown violently forward IS a cause for injury. This brain and spinal cord can be prevented by keeping a child rear-facing.
The Comfort QuestionBesides worrying about leg injuries, many parents worry about leg discomfort in the rear-facing child. As kids get older, their feet will touch the back of the vehicle seat; this is both comfortable and safe.
Ever wonder why a 5-year-old can sleep comfortably with his chin on his chest and never wake up complaining of a stiff neck? It’s because kids’ joints aren’t fully formed, which lets them sit comfortably in positions that would be painful for even a yoga master. Kids have much more flexibility and range of motion in their ankle, knee and hip joints than adults do. For this reason, a 3-year-old can sit comfortably rear-facing with their legs crossed or in the “frog leg” position.
Kids have much more flexibility and range of motion in their ankle, knee and hip joints than adults do. For this reason, a 3-year-old can sit comfortably rear-facing with their legs crossed or in the “frog leg” position.
Parents of forward-facing children will know that kids often try to put their feet up wherever they can – often the back of the front seat (which drives many adults crazy!). Forward-facing kids are doing this because they’re not comfortable! Just like you aren’t comfortable when you sit on a bar stool without a foot rest and your legs are left to dangle, kids don’t like their legs dangling in the car seat as happens forward-facing (but doesn’t happen rear-facing).
Proof kids are comfy rear-facing
I thought my child could turn forward-facing at 12 months?
This is NOT correct. Many (many) years ago, in the days before the iPhone was invented, the minimum to turn forward facing was 1 year and 20 pounds.
In 2011 both the AAP and NHTSA updated their recommendations to reflect the latest research in child passenger safety. The AAP now recommends that kids sit rear-facing until at least age 2 and for longer if possible. NHTSA now recommends: “Your child should remain in a rear-facing car seat until he or she reaches the top height or weight limit allowed by your car seat’s manufacturer.”
The AAP now recommends that kids sit rear-facing until at least age 2 and for longer if possible. NHTSA now recommends: “Your child should remain in a rear-facing car seat until he or she reaches the top height or weight limit allowed by your car seat’s manufacturer.”
But my child’s convertible car seat only goes to 20 or 22 pounds rear-facing. What do I do?
Your car seat is confusing you! Really! All convertible seats on the market in the US have for many, many years allowed rear-facing until at least 30 pounds, with most going to 40 or more pounds rear-facing. However, the labels on the car seat confuse many families, leading them to think a child must be forward-facing starting at 22 lbs.
Why? Because our government requires manufacturers to include some exceptionally confusing wording on the labels of every convertible car seat (car seats that start out rear-facing & then go forward-facing). The sentence that confuses most people is “Use only in a rear-facing position when using it with an infant weighing less than 20 lbs. ” What this sentence is trying to say, is that for kids who weigh less than 20 lbs. the only direction you are allowed to install this car seat is rear-facing – i.e. a child under 20 pounds may never ride forward-facing in this car seat. However, many people confuse this to mean that after 20 pounds you must turn the car seat forward-facing – which is NOT what it is trying to say.
” What this sentence is trying to say, is that for kids who weigh less than 20 lbs. the only direction you are allowed to install this car seat is rear-facing – i.e. a child under 20 pounds may never ride forward-facing in this car seat. However, many people confuse this to mean that after 20 pounds you must turn the car seat forward-facing – which is NOT what it is trying to say.
In another sentence, likely very close to where you found the confusing one, you’ll see the rear-facing maximum weight for your convertible seat, likely 40 pounds or even higher.
When is my child too big for rear-facing?
A child can be either too heavy, too tall, or both–but all of this depends on the specifications of the car seat. Each car seat has its own height and weight limits for rear-facing children. Most convertible seats allow children to sit rear-facing up to 35, 40 or 50 pounds. The height limit for most rear-facing car seats is that there must be at least 1 inch of room between the top of the child’s head and the top of the car seat.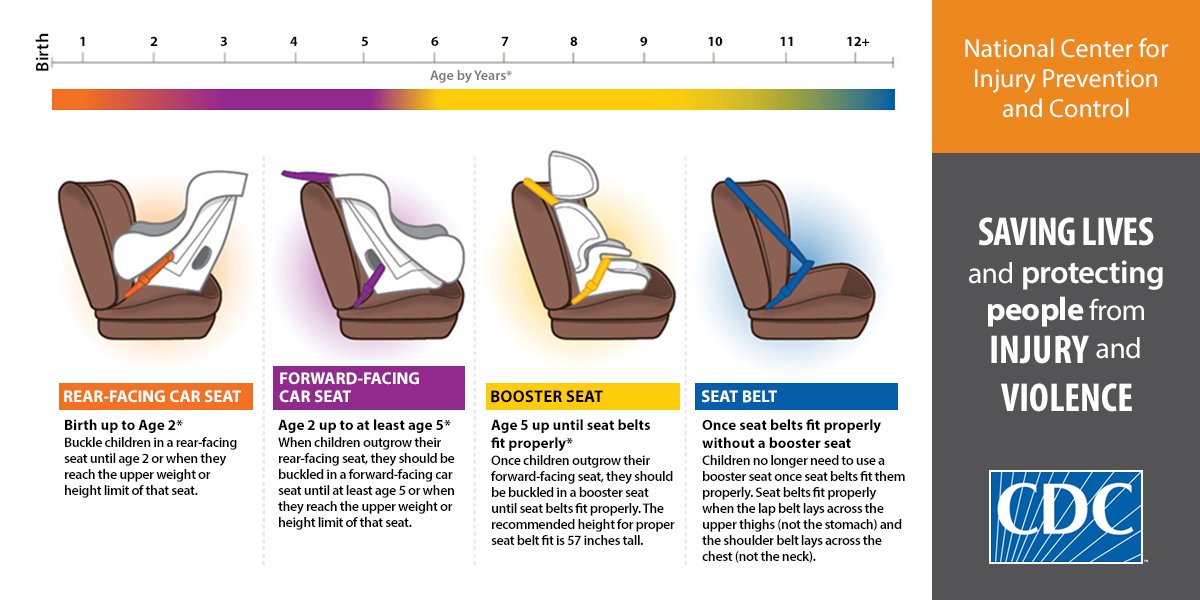 This inch ensures that as the child slides up the seat in a crash, his head will stay protected.
This inch ensures that as the child slides up the seat in a crash, his head will stay protected.
Given the design of most car seats, the majority of children become too tall for rear-facing seats before they become too heavy. Therefore, when you purchase a convertible car seat, try to select one that is taller in seated height.
What about "off the charts" big kids?
A 95th percentile child may look stronger than his 5th percentile friend, but in a crash the bigger child is MORE at risk if he’s riding forward-facing. The rigidity of bones and the strength of ligaments in the spine is likely the same in children of the same age, no matter their size. And a 95th percentile baby likely has a much larger, heavier head, which will pull forward which much more force than that of a 5th percentile child. Click here to learn about seats that can best accommodate the biggest kids rear-facing.
How to keep your child entertained while rear-facing
Rear-facing doesn’t have to be boring! Older kids can ride quite upright so they can see out the side and rear windows. If there’s a head rest blocking your child’s view out the back window, you can usually remove it. By 9-12 months your baby knows you’re there when you talk to them from the front – even though they can’t see you. So you can calm and entertain your child with songs, stories, and for older children games of “I spy,” all while they’re rear-facing.
If there’s a head rest blocking your child’s view out the back window, you can usually remove it. By 9-12 months your baby knows you’re there when you talk to them from the front – even though they can’t see you. So you can calm and entertain your child with songs, stories, and for older children games of “I spy,” all while they’re rear-facing.
We’ve got lots of suggestions for great car seat & travel toys for babies & toddlers (and big kids too) because sometimes we all get a little cranky when we’re bored!
The dreaded Motion Sickness! Won't it help to turn around my child?
The long and short: most kids do not puke less when forward-facing compared to rear-facing.
We’ve got lots of information on motion-sickness over here – including an explanation of why it is believed to occur, things you can do to decrease the chance of your kid puking, and how to minimize the mess and clean up if your kid does puke.
I already turned my kid forward-facing.
 Should I really turn my 2 or 3 year old back rear-facing?
Should I really turn my 2 or 3 year old back rear-facing? Yes! When we know better, we must do better. A few months ago when you turned her forward facing you did what you thought was best, but now you know differently. Avoid regrets, and give your child the best protection.
Many parents worry that it will be a disaster turning an older child back rear-facing. Here is one mom’s experience turning her almost-3-year-old son back rear-facing:
“I was initially very hesitant to move my almost three year old son to rear facing from forward facing. He has been sitting forward facing for over a year and can be strong willed when it comes to change. However, after hearing how much safer it is I was willing to try. The first three or so drives were very difficult as he asked to “look out mama and dada’s window” almost the entire time. We ignored and distracted and I was about to give up when I noticed that although he still complained about sitting rear facing it happened less and less. Now (after about three weeks) he asks maybe once every other drive if he can sit forward facing and was even (mostly) fine the other day when his friend joined us and sat forward facing. It was a tough first few drives, but I am very happy we did it and I feel so much safer.
Now (after about three weeks) he asks maybe once every other drive if he can sit forward facing and was even (mostly) fine the other day when his friend joined us and sat forward facing. It was a tough first few drives, but I am very happy we did it and I feel so much safer.
My 20 month old is too big for rear-facing in his current seat. Should I really buy another one to keep him rear-facing?
Imagine it’s November and your 20-month-old has outgrown all of their winter clothes from last year. Would you not buy them new winter clothes because “it will be warmer in four months”? Of course you would buy them the clothes! The same should go for the car seat!
The car seat is one of the only products you will ever buy for your child that has the potential to save their life! Just like your child needs new clothes frequently, they may need a new car seat sooner than you thought. If you are in a crash, you will be relieved knowing that you gave them the best protection possible.
What's the law?
The laws of physics don’t care about the laws of the state… but with that said, it is now law in 15 states that children ride rear-facing until at least age 2.
- California
- Connecticut
- Illinois
- Louisiana
- Maine
- Nebraska
- New Jersey
- New York
- Oklahoma
- Oregon
- Pennsylvania
- Rhode Island
- South Carolina
- Virginia
- Washington
What's the evidence?
The recommendation to keep children under age 2 rear-facing is not based on a single study, but rather on a broad body of research from the US and Sweden. These citations are included below for easy reference.
- Sherwood CP, Crandall JR. Frontal sled tests comparing rear and forward facing child restraints with 1-3 year old dummies. Annual Proceedings of the Association for the Advancement of Automotive Medicine. Association for the Advancement of Automotive Medicine, 2007,51: 169-80.
- Planath I, Rygaard C, Nilsson S. Synthesis of data towards neck protection criteria for children. Proceedings of the 1992 International IRCOBI Conference on the Biomechanics of Impacts. Verona, Italy:155-66.
- Kamren B, Koch M, Kullgren A, et al. The protective effects of rearward facing CRS: an overview of possibilities and problems associated with child restraints for children aged 0-3 years. Child Occupant Protection Symposium: SAE International, 1993.
- Klinich KD, Manary MA, Weber KB. Crash protection for child passengers: rationale for best practice. UMTRI Res Rev 2012;43:1-35.
- Isaksson-Hellman I, Jakobsson L, Gustafsson C, et al. Trends and effects of child restraint systems based on Volvo’s Swedish accident database.
 41st Stapp Car Crash Conference: SAE International, 1997.
41st Stapp Car Crash Conference: SAE International, 1997. - Jakobsson L, Isaksson-Hellman I, Lundell B. Safety for the growing child: experiences from Swedish accident data. Proceedings of the 17th ESV Conference, 2005.
- American Academy of Pediatrics, Committee on Injury, Violence & Poison Prevention. Child Passenger Safety. Pediatrics. 2018.
- Arbogast KB, et al. Injuries to Children in Forward Facing Child Restraints. Annual Proceedings Association for the Advancement of Automotive Medicine. 2002; 46: 213-30.
Why 2, 3, 4, and even 5 year olds should be rear-facing!
The American Academy of Pediatrics (AAP) has for 20+ years recommended keeping kids rear-facing until they are too big for rear-facing in their convertible seat. This was reiterated in their 2018 policy statement.
The National Highway Traffic Safety Administration (NHTSA) also updated their recommendations, now specifying that children remain rear-facing until reaching “the top height or weight limit allowed by your car seat’s manufacturer. ”
”
Our Favorite Seats for
Keeping Big Kids Rear-facing
Clek FoonfSplurge-worthy, high capacity rear-facing seat with max safety features: anti-rebound bar and rear-facing tether. Optimized for installation on side seats. Narrow exterior and wide interior gives child max room while taking up less room in car than many infant seats. Also has max safety features for forward-facing: rigid LATCH + crumple zone.Buy HereClek FlloHigh capacity rear-facing seat with max safety features: anti-rebound bar and rear-facing tether. Optimized for installation in center seat. Narrow exterior and wide interior gives child max room. Great in 3-across when RF in center seat.Buy HereGraco Extend2FitHighest rear-facing capacity of any seat in US for both tallest and heaviest kids. Fits well in small cars behind tall drivers while giving child lots of leg room. Budget friendly! Note: we do not recommend the Platinum or 4Ever models – we like the basic 2-in-1 model best!Buy Here
Narrow exterior and wide interior gives child max room. Great in 3-across when RF in center seat.Buy HereGraco Extend2FitHighest rear-facing capacity of any seat in US for both tallest and heaviest kids. Fits well in small cars behind tall drivers while giving child lots of leg room. Budget friendly! Note: we do not recommend the Platinum or 4Ever models – we like the basic 2-in-1 model best!Buy Here
Previous
Next
15 states now require kids to remain rear-facing until at least their 2nd birthday.
Whoa… you might be thinking “how does a 2-year-old fit rear-facing”… take 90 seconds and watch the following video – and you’ll see how these 90 different 2 year olds all ride safely and comfortably rear-facing.
Common Questions about Rear-facing
What about their legs? Isn’t it unsafe and/or uncomfortable?
The video above shows a side by side comparison of a forward-facing car seat (on the left) and a rear-facing car seat (on the right) using the same crash test dummy and the same crash speed.
Notice how the rear-facing dummy tucks into a cannonball position? No matter how scrunched the rear-facing child’s legs start, they end up super scrunched during the crash and it does NOT cause injury to the legs (or other parts of the body either).There are ZERO documented cases of rear-facing children breaking their legs, hips, feet, etc., due to their feet touching the back of the vehicle seat. In fact, studies show that forward-facing kids suffer many more leg injuries than rear-facing kids. The leg injuries to forward-facing children occur when the child’s legs fly up and hit the back of the front seat all the while the child & car seat are moving forward which traps the child’s legs and puts tremendous pressure into the leg bones which can break them.
What you should be asking is “What about the HEAD & NECK?” – notice how the forward-facing child’s head and neck are thrown forward (snug straps only hold the chest back, not the head & neck) – whereas the rear-facing child’s head and neck are cradled within the shell of the car seat. The forward-facing child’s head being thrown violently forward IS a cause for brain and spinal cord injury… injury we can prevent by keeping a child rear-facing.
3-year-old happily rear-facing
Besides worrying about leg injuries, many parents worry about leg discomfort in the rear-facing child. As kids get older, their feet will touch the back of the vehicle seat; this is both comfortable and safe. Ever wonder why a 5-year-old can sleep comfortably with his chin on his chest and never wake up complaining of a stiff neck? It’s because kids’ joints aren’t fully formed, which lets them sit comfortably in positions that would be painful for even a yoga master. Kids have much more flexibility and range of motion in their ankle, knee and hip joints than we do. For this reason, a 3-year-old can sit comfortably rear-facing with her legs crossed or in the “frog leg” position.
For this reason, a 3-year-old can sit comfortably rear-facing with her legs crossed or in the “frog leg” position.
Parents of forward-facing children will know that the kids often try and put their feet up wherever they can – often the back of the front seat (which drives many adults crazy!). Forward-facing kids are doing this as just like you aren’t comfortable when you sit on a bar stool without a foot rest and your legs are left to dangle, they don’t like their legs dangling in the car seat as happens forward-facing (but doesn’t happen rear-facing).
What about rear-facing in a rear-end crash?
A recent study looked at rear-facing car seats in rear impacts. They study found that rear-facing car seats mitigate and manage crash forces in a variety of ways that allow them to provide good protection for rear-facing kids. This finding is backed up by epidemiological and field data which also show that real kids riding rear-facing in real rear-end crashes typically do very well.
Someone told me I can turn my child forward-facing at 1 year and 20 pounds. Is this correct?
This is NOT correct. Many years ago, in the days before the iPhone was invented, the minimum to turn forward facing was 1 year and 20 pounds.
In 2011 both the AAP and NHTSA updated their recommendations to reflect the latest research in child passenger safety. The AAP now recommends that kids sit rear-facing until at least age 2. NHTSA now recommends: “Your child should remain in a rear-facing car seat until he or she reaches the top height or weight limit allowed by your car seat’s manufacturer.”
But my child’s convertible car seat only goes to 20 or 22 pounds rear-facing. What do I do?
Our government requires manufacturers to include some exceptionally confusing wording on the labels of every convertible car seat (car seats that start out rear-facing & then go forward-facing). The sentence that confuses most is “Use only in a rear-facing position when using it with an infant weighing less than 20 lbs.” What this sentence is trying to say, is that for kids who weigh less than 20 lbs. the only direction you are allowed to install this car seat is rear-facing – i.e. a child under 20 pounds may never ride forward-facing in this car seat. However, many people confuse this to mean that after 20 pounds you must turn the car seat forward-facing – which is NOT what it is trying to say. In another sentence, likely very close to where you found the confusing one, it will give the rear-facing minimum and maximum weights for your convertible seat. All convertible seats on the market in the US for many years now go rear-facing until at least 30 pounds, with most going to 40 or more pounds rear-facing.
The sentence that confuses most is “Use only in a rear-facing position when using it with an infant weighing less than 20 lbs.” What this sentence is trying to say, is that for kids who weigh less than 20 lbs. the only direction you are allowed to install this car seat is rear-facing – i.e. a child under 20 pounds may never ride forward-facing in this car seat. However, many people confuse this to mean that after 20 pounds you must turn the car seat forward-facing – which is NOT what it is trying to say. In another sentence, likely very close to where you found the confusing one, it will give the rear-facing minimum and maximum weights for your convertible seat. All convertible seats on the market in the US for many years now go rear-facing until at least 30 pounds, with most going to 40 or more pounds rear-facing.
When is a child TOO BIG for rear-facing?
A child can be either too heavy, too tall, or both–but all of this depends on the specifcations of the car seat. Each car seat has its own height and weight limits for rear-facing children. Most convertible seats allow children to sit rear-facing up to 35, 40 or 50 pounds. The height limit for most rear-facing car seats is that there must be at least 1 inch of room between the top of the child’s head and the top of the car seat. This inch ensures that as the child slides up the seat in a crash, his head will stay protected. Given the design of most car seats, the majority of children become too tall for rear-facing seats before they become too heavy. Therefore, when you purchase a convertible car seat, try to select one that is taller in seated height.
Each car seat has its own height and weight limits for rear-facing children. Most convertible seats allow children to sit rear-facing up to 35, 40 or 50 pounds. The height limit for most rear-facing car seats is that there must be at least 1 inch of room between the top of the child’s head and the top of the car seat. This inch ensures that as the child slides up the seat in a crash, his head will stay protected. Given the design of most car seats, the majority of children become too tall for rear-facing seats before they become too heavy. Therefore, when you purchase a convertible car seat, try to select one that is taller in seated height.
What about big kids – those who are “off the charts”?
A 95th percentile child may look stronger than his 5th percentile friend, but in a crash the bigger child is MORE at risk if he’s riding forward-facing. The rigidity of bones and the strength of ligaments in the spine is likely the same in children of the same age, no matter their size. And a 95th percentile baby likely has a much larger, heavier head, which will pull forward which much more force than that of a 5th percentile child. Click here to learn about seats that can best accommodate the biggest kids rear-facing.
And a 95th percentile baby likely has a much larger, heavier head, which will pull forward which much more force than that of a 5th percentile child. Click here to learn about seats that can best accommodate the biggest kids rear-facing.
What if my child is unhappy riding rear-facing?
Rear-facing does not have to be boring! Older kids can ride quite upright so they can see out the side and rear windows. If there is a head rest blocking your child’s view out the back window, you can usually remove it. By 9-12 months your baby knows you’re there when you talk to them from the front – even though they can’t see you. So you can calm and entertain your child with songs, stories – and for older children games of “I spy” – all while they are rear-facing.
We’ve got lots of suggestions for great car seat & travel toys for babies & toddlers (and big kids too) – check them out here – because sometimes we all get a little cranky when we’re bored!
What are some good toys for rear-facing kiddos?
We’ve got a pediatrician-curated selection of toys, teethers, and games that are car seat & travel friendly for babies, toddlers & big kids. We all get a little cranky when we’re bored – and these are sure to keep boredom at bay!
We all get a little cranky when we’re bored – and these are sure to keep boredom at bay!
What about kids who get motion sick?
The long and short: most kids do not puke less when forward-facing compared to rear-facing.
We’ve got lots of information on motion-sickness over here – including an explanation of why it is believed to occur, things you can do to decrease the chance of your kid puking, and how to minimize the mess and clean up if your kid does puke.
I already turned my 1 year old forward-facing – should I really turn her back rear-facing?
Yes! When we know better, we must do better. Three months ago when you turned her forward facing you did what you thought was best, but now you know differently. Avoid regrets, and give her the best protection.
Many parents worry that it will be a disaster turning an older child back rear-facing. Here is one mom’s experience turning her almost-3-year-old son back rear-facing:
“I was initially very hesitant to move my almost three year old son to rear facing from forward facing. He has been sitting forward facing for over a year and can be strong willed when it comes to change. However, after hearing how much safer it is I was willing to try. The first three or so drives were very difficult as he asked to “look out mama and dada’s window” almost the entire time. We ignored and distracted and I was about to give up when I noticed that although he still complained about sitting rear facing it happened less and less. Now (after about three weeks) he asks maybe once every other drive if he can sit forward facing and was even (mostly) fine the other day when his friend joined us and sat forward facing. It was a tough first few drives, but I am very happy we did it and I feel so much safer.
He has been sitting forward facing for over a year and can be strong willed when it comes to change. However, after hearing how much safer it is I was willing to try. The first three or so drives were very difficult as he asked to “look out mama and dada’s window” almost the entire time. We ignored and distracted and I was about to give up when I noticed that although he still complained about sitting rear facing it happened less and less. Now (after about three weeks) he asks maybe once every other drive if he can sit forward facing and was even (mostly) fine the other day when his friend joined us and sat forward facing. It was a tough first few drives, but I am very happy we did it and I feel so much safer.
I already turned my 1 year old forward-facing – should I really turn her back rear-facing?
Yes! When we know better, we must do better. Three months ago when you turned her forward facing you did what you thought was best, but now you know differently. Avoid regrets, and give her the best protection.
Many parents worry that it will be a disaster turning an older child back rear-facing. Here is one mom’s experience turning her almost-3-year-old son back rear-facing:
“I was initially very hesitant to move my almost three year old son to rear facing from forward facing. He has been sitting forward facing for over a year and can be strong willed when it comes to change. However, after hearing how much safer it is I was willing to try. The first three or so drives were very difficult as he asked to “look out mama and dada’s window” almost the entire time. We ignored and distracted and I was about to give up when I noticed that although he still complained about sitting rear facing it happened less and less. Now (after about three weeks) he asks maybe once every other drive if he can sit forward facing and was even (mostly) fine the other day when his friend joined us and sat forward facing. It was a tough first few drives, but I am very happy we did it and I feel so much safer.
My 20-month-old is too heavy for rear-facing in his current seat – should I really buy a different seat so he can ride rear-facing longer?
Imagine it’s November and your 20-month-old has outgrown all of her winter clothes from last year. Would you not buy her new winter clothes because “it will be warmer in four months”? The car seat is one of the only products you will ever buy for your child that has the potential to save her life! Just like your child needs new clothes frequently, they may need a new car seat sooner than you thought. If you are in a crash, you will be relieved knowing that you gave her the best protection possible.
What is the law?
The laws of physics don’t care about the laws of the state… but with that said, it is now law in 15 states that children ride rear-facing until at least age 2.
- California
- Connecticut
- Illinois
- Louisiana
- Maine
- Nebraska
- New Jersey
- New York
- Oklahoma
- Oregon
- Pennsylvania
- Rhode Island
- South Carolina
- Virginia
- Washington
What is the evidence?
It is critically important to understand that the recommendation to keep children under age 2 rear-facing is not based on a single study, but rather on a broad body of research from the US and Sweden. These citations are included below for easy reference.
These citations are included below for easy reference.
- Sherwood CP, Crandall JR. Frontal sled tests comparing rear and forward facing child restraints with 1-3 year old dummies. Annual Proceedings of the Association for the Advancement of Automotive Medicine. Association for the Advancement of Automotive Medicine, 2007,51: 169-80.
- Planath I, Rygaard C, Nilsson S. Synthesis of data towards neck protection criteria for children. Proceedings of the 1992 International IRCOBI Conference on the Biomechanics of Impacts. Verona, Italy:155-66.
- Kamren B, Koch M, Kullgren A, et al. The protective effects of rearward facing CRS: an overview of possibilities and problems associated with child restraints for children aged 0-3 years. Child Occupant Protection Symposium: SAE International, 1993.
- Klinich KD, Manary MA, Weber KB. Crash protection for child passengers: rationale for best practice. UMTRI Res Rev 2012;43:1-35.
- Isaksson-Hellman I, Jakobsson L, Gustafsson C, et al.
 Trends and effects of child restraint systems based on Volvo’s Swedish accident database. 41st Stapp Car Crash Conference: SAE International, 1997.
Trends and effects of child restraint systems based on Volvo’s Swedish accident database. 41st Stapp Car Crash Conference: SAE International, 1997. - Jakobsson L, Isaksson-Hellman I, Lundell B. Safety for the growing child: experiences from Swedish accident data. Proceedings of the 17th ESV Conference, 2005.
- American Academy of Pediatrics, Committee on Injury, Violence & Poison Prevention. Child Passenger Safety. Pediatrics. 2018.
- Arbogast KB, et al. Injuries to Children in Forward Facing Child Restraints. Annual Proceedings Association for the Advancement of Automotive Medicine. 2002; 46: 213-30.
We are a reader supported site. We earn an affiliate commission when you buy through our links.
FTC Disclosure: Affiliate links are included in this page. No monetary compensation was provided, however, some of the reviewed products were supplied by the manufacturer or distributor to help facilitate the review. All opinions are those of The Car Seat Lady LLC.
How to properly hold a baby in your arms
Bagdasaryan Kristina Genrihovna
Obstetrician-gynecologist, Ultrasound specialist
Clinic "Mother and Child" St. Petersburg
So, how to take the child from the supine position. Grasp his chest with both hands - thumbs in front, and the rest hold the back. If the baby is not yet able to hold his head, support it with your index fingers. Gently lift your baby up. Do not forget, your face turned to the child should always express the kindest feelings. Talk to the baby, tell him what you are doing, the voice should not be very loud, gentle.
Those who take a small child in their arms are divided into two categories: relatives who live with him under the same roof, and visitors. You should not allow a visitor to the child who has not taken off his outerwear, hat, street shoes, has not washed his hands with soap, has not freed his hands from rings, rings, watches, bracelets. The baby can be frightened by sharp extraneous odors, for example, the smell of tobacco, alcohol, perfume.
The baby can be frightened by sharp extraneous odors, for example, the smell of tobacco, alcohol, perfume.
Sick people should not be allowed near the child - coughing, sneezing, as well as complaining of indigestion, suffering from skin diseases.
Even if loving relatives have come a long way on trains and planes to visit the baby, be persistent and keep the guests “in quarantine” for several days - will the infection picked up on the road show up? They may be offended, but the child will remain healthy! In order to more reliably protect the psyche and immune system of the child, it is useful in his first six months of life to limit the circle of people admitted to him. These are the rules, and no one - neither the formidable mother-in-law, nor the neighbor, nor the beloved boss - deserves an exception.
Some parents take the baby in their arms with unthinkable precautions, others, on the contrary, snatch it from the crib so famously. All these are extremes. So how should it be?
So how should it be?
- do not make sudden movements when holding the baby
- never take it with one hand - only with both
- do not raise or lower the baby quickly, rapidly
- do not take it out of the crib by pulling on the handles
The position of the baby in the arms of the mother (or another adult), first of all, depends on his age, as well as on whether he will sleep or be awake. Up to 2-2.5 months (and sometimes longer), the baby’s head must be supported, so in a horizontal position (face up), arrange the baby on your arm so that the back of his head lies on your elbow, the back rests on your forearm, and your hands should support the buttocks and hips of the baby. You can put the baby on your forearm and stomach. In this case, the baby's head should be in the crook of the elbow, and your hands will close on the baby's stomach, and one hand will pass between the legs of the little one. If you want to hold the child in an upright position, for example, in order for him to burp excess air, then support his head and back: put one of your palms on the back of the baby’s head, with your forearm firmly press his body to you. With the other hand, fix the buttocks of the crumbs. In no case do not sit the child on your arm until he has confidently mastered the skill of sitting, which happens on average at the age of 6 months. From 2.5-3 months, you can already carry the baby, turning him away from you, holding him with one hand at chest level, with the other at hip level.
Depending on the age of the child, there are 6 ways to hold him in your arms.
Hanging. This method is good for babies up to 3 months old, when they still have trouble holding their head. With one hand support the neck and back of the baby's head, with the other - the buttocks, while his torso may be slightly bent, and his face turned towards you. This situation opens up scope for the much-needed emotional contact with the mother and other loved ones for a small child.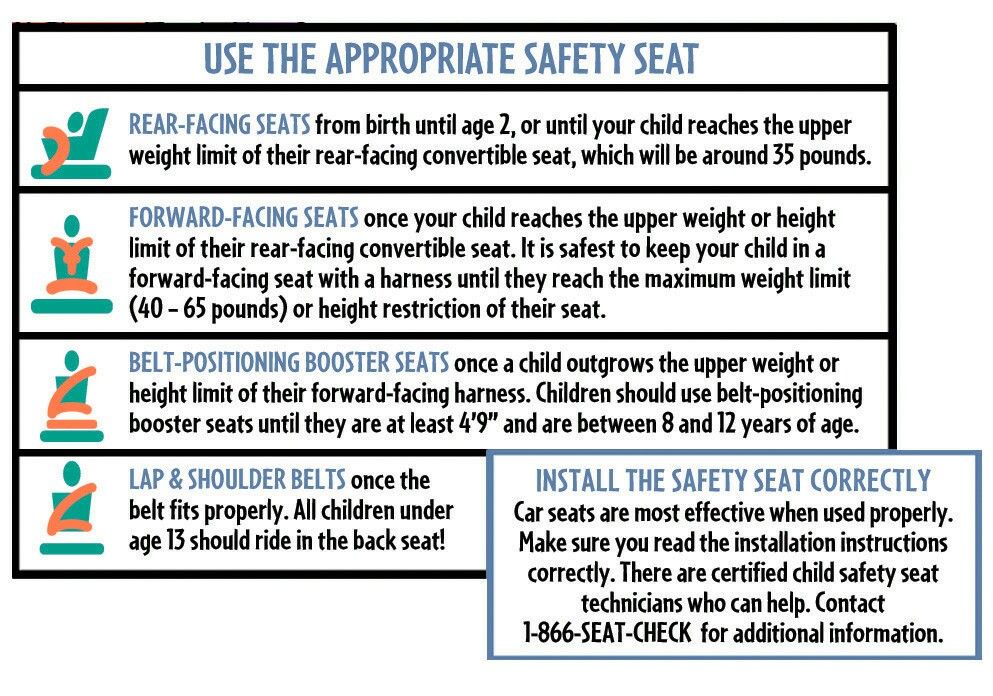 Do not forget that in order to avoid the development of one-sidedness, the baby's head must be supported either with the left or with the right hand - periodically changing them.
Do not forget that in order to avoid the development of one-sidedness, the baby's head must be supported either with the left or with the right hand - periodically changing them.
On the arm. Ideal for babies aged 3-6 months, although you can keep your baby this way almost from birth. He rests his head on your shoulder, you hold his feet with your hand, and your arms with your forearm. With your other hand, you support the baby under the buttocks. At the same time, the child's legs should be bent at the knee and hip joints and bred. Don't forget to alternate hands.
In front of the bust . Starting from 6 months, this way of holding the baby provides him with the same position as in the position on the back. The baby leans back against your chest, his legs are bent and divorced, the soles are in contact. Hold the baby's shins with your thumbs, the feet with the index, middle and ring fingers, and the buttocks with the little fingers. This position is useful for the development of the child: as well as on the back, he can play with his legs, improving movements, mastering his body and gaining an idea of \u200b\u200bspace.
This position is useful for the development of the child: as well as on the back, he can play with his legs, improving movements, mastering his body and gaining an idea of \u200b\u200bspace.
In front of the stomach . In children from 7 months old, this method allows you to reproduce crawling in a plastunsky way - a motor skill that they just need to master at this age. With one hand, take the child under the chest, and pass the other between the legs, supporting the stomach. Don't forget to switch hands.
On the side. Suitable for babies from 10 months, when they are already sitting confidently. Take the child so that he wraps his legs around your side, and rests his back on your forearm. You should support the baby's knee with your hand, giving it a slightly bent position. One arm of the child is on your chest, the other is free. Please note: you need to wear a child in this position alternately from one side to the other.
And, finally, a universal and completely international way to carry children of any age. Holding the palm of your right hand under the breast of the baby, firmly press his back to your chest. With your left hand, grasp the child's right thigh, bending his legs at the hip joints. Please note: the weight of a child under 6 months should not fall on your hand supporting the baby's pelvis - this is harmful to his spine and can ruin his posture in the future.
The baby grows, his body weight increases, and it becomes difficult to carry the baby in his arms for a long time (especially after 3 months of age, when the weight of the child reaches an average of 7 kg). Here, assistive devices for carrying children, such as a baby sling and a kangaroo backpack, can help out for a while. A baby sling is a modern modification of a piece of fabric that provides close physical contact between mother and child. In addition, with it, if necessary, it is easier to breastfeed a child while on the street or in another public place. You can use a baby sling from birth to a year and a half. It all depends on the weight of the baby and your physical capabilities. It is also very important to find the optimal position for the child and for the mother, which would provide both with maximum comfort. The basic positions of the baby in a baby sling are horizontal, with support for the spine, and (for older children) raised vertical or sitting, when the baby is tightly pulled by the fabric. A kangaroo backpack can be used only after the baby learns to hold his head confidently and his back muscles get stronger. Preference should be given to backpacks with a rigid back. But, nevertheless, you should not get too carried away with a baby sling and a kangaroo backpack. Firstly, it is still more useful for the baby to lie on the hard mattress of the crib or stroller. Secondly, it is unlikely that the child will like to sleep while sitting in a backpack. And, thirdly, a long stay of a child in the same position, which causes an uneven load on different parts of the spine, can provoke a pathology of the musculoskeletal system.
You can use a baby sling from birth to a year and a half. It all depends on the weight of the baby and your physical capabilities. It is also very important to find the optimal position for the child and for the mother, which would provide both with maximum comfort. The basic positions of the baby in a baby sling are horizontal, with support for the spine, and (for older children) raised vertical or sitting, when the baby is tightly pulled by the fabric. A kangaroo backpack can be used only after the baby learns to hold his head confidently and his back muscles get stronger. Preference should be given to backpacks with a rigid back. But, nevertheless, you should not get too carried away with a baby sling and a kangaroo backpack. Firstly, it is still more useful for the baby to lie on the hard mattress of the crib or stroller. Secondly, it is unlikely that the child will like to sleep while sitting in a backpack. And, thirdly, a long stay of a child in the same position, which causes an uneven load on different parts of the spine, can provoke a pathology of the musculoskeletal system. Therefore, it is not recommended to keep the baby in a baby sling and "kangaroo" for more than 40 minutes a day. When the child grows up a little, you can practice the pose when the baby sits on his mother's side, facing her. The advantages of this position: the mother has one hand free, and the child has an excellent view. If the mother, for health reasons, is not recommended to take the baby in her arms, then you can often put him on her stomach, put him on her knees.
Therefore, it is not recommended to keep the baby in a baby sling and "kangaroo" for more than 40 minutes a day. When the child grows up a little, you can practice the pose when the baby sits on his mother's side, facing her. The advantages of this position: the mother has one hand free, and the child has an excellent view. If the mother, for health reasons, is not recommended to take the baby in her arms, then you can often put him on her stomach, put him on her knees.
And, finally, many parents are concerned about the question, is it possible to spoil him by often taking the baby in his arms? If the needs of the child are not ignored, they are not denied affection and tactile contact, then this does not mean at all that he is spoiled and poorly educated. Love is not a synonym for bad parenting, especially if we are talking about a baby who is only a few weeks or months old. There is an opinion that it is impossible to spoil a child up to 12 months - until this age, all his "whims" are justified by needs, so an adult should indulge the baby in everything. And only when the baby reaches the year, parents should selectively treat his requests - based on what they are caused by. From this age, it is already possible to instill in the baby the concept that not only he, but also the people around him have needs.
And only when the baby reaches the year, parents should selectively treat his requests - based on what they are caused by. From this age, it is already possible to instill in the baby the concept that not only he, but also the people around him have needs.
Harsh parenting methods, according to which taking a child in your arms means pampering him, ignore the natural need of the baby for the constant presence of the mother (or the one who cares for him). While promoting the principle of early formation of "independence", they have significant negative features. Firstly, a child who is deliberately separated from his mother does not develop a trusting, kind attitude towards the world, and this will certainly have a negative impact in his adult life. Secondly, the restriction of bodily contact between mother and baby does not contribute to the emergence of mutual feelings between them. It is not surprising that the child in such cases is perceived as a hindrance to the usual way of life and ordinary affairs.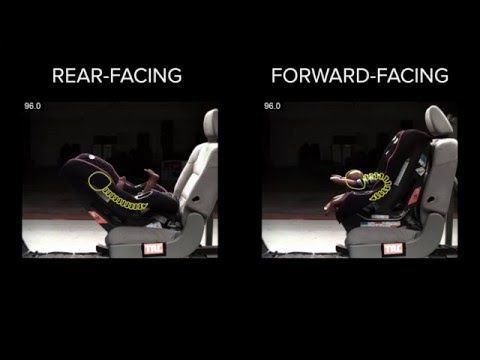 And the baby constantly needs communication and his crying is a call to everyone, and first of all to his mother. Indeed, even in those cases when, it would seem, there are no reasons for tears, the baby may burst into offended or angry crying - because he is not yet ready for loneliness, his biological connection with his mother is still too strong. Thirdly, it should be borne in mind that a strict attitude towards a child, when adults try not to show their feelings and emotions in relation to a child, is not a guarantee of a good upbringing of a child and his further success. Most often, a young mother has a lot of chores around the house. Therefore, if she often takes the baby in her arms, she will have to sacrifice some things. In addition, carrying a child in her arms is also physically not very easy. In general, if desired, there are many reasons for minimizing physical contact with a child. Here you need to prioritize and decide what is more important for you - the daily routine or the development of the child.
And the baby constantly needs communication and his crying is a call to everyone, and first of all to his mother. Indeed, even in those cases when, it would seem, there are no reasons for tears, the baby may burst into offended or angry crying - because he is not yet ready for loneliness, his biological connection with his mother is still too strong. Thirdly, it should be borne in mind that a strict attitude towards a child, when adults try not to show their feelings and emotions in relation to a child, is not a guarantee of a good upbringing of a child and his further success. Most often, a young mother has a lot of chores around the house. Therefore, if she often takes the baby in her arms, she will have to sacrifice some things. In addition, carrying a child in her arms is also physically not very easy. In general, if desired, there are many reasons for minimizing physical contact with a child. Here you need to prioritize and decide what is more important for you - the daily routine or the development of the child. If you want to properly take care of the child and at the same time not start life, look for helpers-allies with whom you can do everything.
If you want to properly take care of the child and at the same time not start life, look for helpers-allies with whom you can do everything.
Make an appointment
to the doctor - Bagdasaryan Kristina Genrihovna
Clinic "Mother and Child" St. Petersburg
PregnancyManagement of pregnancyManagement of pregnancy after IVFManagement of pregnancy in Rh-conflictGynecologyDiary of pregnancyImmunological causes of miscarriageConservative gynecologyConservative treatment of cervical pathologyContracts for the management of pregnancyTreatment of miscarriagePlanning pregnancyHLA compatibility
By clicking on the send button, I consent to the processing of personal data
Attention! Prices for services in different clinics may vary. To clarify the current cost, select a clinic
All areasSpecialist consultations (children)Therapeutic research
01.
Specialist consultations (children)
02.
Therapeutic research
Nothing found
The administration of the clinic takes all measures to timely update the price list posted on the website, however, in order to avoid possible misunderstandings, we advise you to clarify the cost of services and the timing of the tests by calling
Important! About wearing “Facing the world”
I will tell you about wearing the baby facing from the mother, “Facing the world”, why it is not necessary, and how to teach the baby to the correct position.
Sling is a physiological carrier. In the sling, the baby is positioned like a mother in her arms. In the sling there is no position facing away from the mother. We carry the baby on the hip, behind the back in the cradle position, BUT always facing the mother.
Consider the position of mother and child from the point of view of physiology.
At birth, our baby's spine has the shape of the Russian letter "C" - the back is rounded.
Between the vertebrae are intervertebral discs that act as connecting pads and shock absorbers. In a baby, the spine straightens and forms up to a year old, bends are also formed gradually and therefore it is best to cushion the intervertebral discs in a rounded position. When we carry the baby facing us, he leans on his mother with his upper body, his back is rounded, the intervertebral discs work at full strength and absorb our steps. If you turn the child to face away from you, then the child's back straightens or arches back. In this case, the intervertebral discs are displaced, they are additionally compressed and can cause pain to the child. Any damage to the intervertebral discs can lead to the development of inflammation and pain.
If we carry a baby facing away from us in any carrier, then his legs will hang down. We cannot give the legs the correct physiological position, the child hangs on the perineum, which bears the entire load, which is naturally harmful, uncomfortable and painful. If we carry a child in a sling facing away from us, then all its advantages are immediately lost, it will not be better than the same kangaroo.
If we carry a child in a sling facing away from us, then all its advantages are immediately lost, it will not be better than the same kangaroo.
And most importantly, the entire body weight of the child is loaded precisely by the lower spine - the sacral, which is not recommended to be loaded at all until the baby is completely seated. The child's knees should be higher than the priests, only in this case the load is transferred from the child's sacrum to the hips. The upper part of the body of the baby, when worn facing the mother, lies on the mother. The load is evenly distributed. We support the child's hips with a sling or hands. If the baby is facing away from us, we cannot give such a position of the legs in the carrier. The position in which the child hangs on the perineum can be an impetus for the development of hip dysplasia. Hip dysplasia is the most common type of deformity of the musculoskeletal system in children. Knowledgeable physicians recommend slings to prevent dysplasia or to aid in treatment.
In the position facing away from the mother on the shoulders and cervical spine of the baby, an unacceptable load also occurs. The kid has to constantly hold his head, straighten his shoulders, the spine does not absorb well. The baby gets tired, he has no one to lean on, his head hangs down, his chin is pressed to his chest - the child’s breathing is difficult or, on the contrary, his head is thrown back. When the baby is facing his mother, he can put his head on his mother's chest, like on a pillow, and have a sweet sleep, relax.
Now let's look a little at the physiology of the carrier - usually the mother.
The spine of an already formed adult is similar to the Latin letter S - it has four bends that cushion our steps. When the baby is located facing the mother, then its weight is evenly distributed over the mother, as if smeared, and it is easy to carry the baby. If we turn the baby over to face away from us, then it becomes difficult to carry him. Feeling as if we are carrying a separate bag - the center of gravity is shifting. The greater the weight of the baby, the more mother's shoulders and back are rounded forward, and the lower back bends. Over time, mom's posture takes on the shape of a question mark. Also, the shift in the center of gravity puts additional stress on the hip joints and feet of the parent.
If we turn the baby over to face away from us, then it becomes difficult to carry him. Feeling as if we are carrying a separate bag - the center of gravity is shifting. The greater the weight of the baby, the more mother's shoulders and back are rounded forward, and the lower back bends. Over time, mom's posture takes on the shape of a question mark. Also, the shift in the center of gravity puts additional stress on the hip joints and feet of the parent.
Psychology.
Facing away from mother is harmful from the point of view of psychology. The kid constantly sees movement, flashing images, a lot of new and incomprehensible information. And most importantly, information cannot run out at the moment when the baby is tired of it. He cannot turn away, he cannot hide into his mother, he can only close his eyes. Therefore, when the child is overexcited, the brain turns on a protective reflex - the child falls asleep with his head hanging down, and this is a stressful and uncomfortable dream. And, unfortunately, I often see such a picture on the streets of the city.
And, unfortunately, I often see such a picture on the streets of the city.
Very good research in 2008 was done in the UK. More than 2500 couples took part in them: mother-child. The research was aimed at studying the interaction between the baby and parents, at determining the level of stress in the child's body, when the baby was taken in a stroller to his mother and facing the world.
So, for the harmonious growth and development of a child, it is very important that parents notice and instantly respond to his needs and requirements, to his feelings and emotions.
Children from birth to three years of age took part in the study, this is the period in which a baby is usually carried in her arms, in a sling and carried in a stroller.
60% of children out of 100% were silent during the walk. Children up to a year old mostly slept. The children who were carried facing the world asked for 5 times more hands than those who were traveling facing their mother.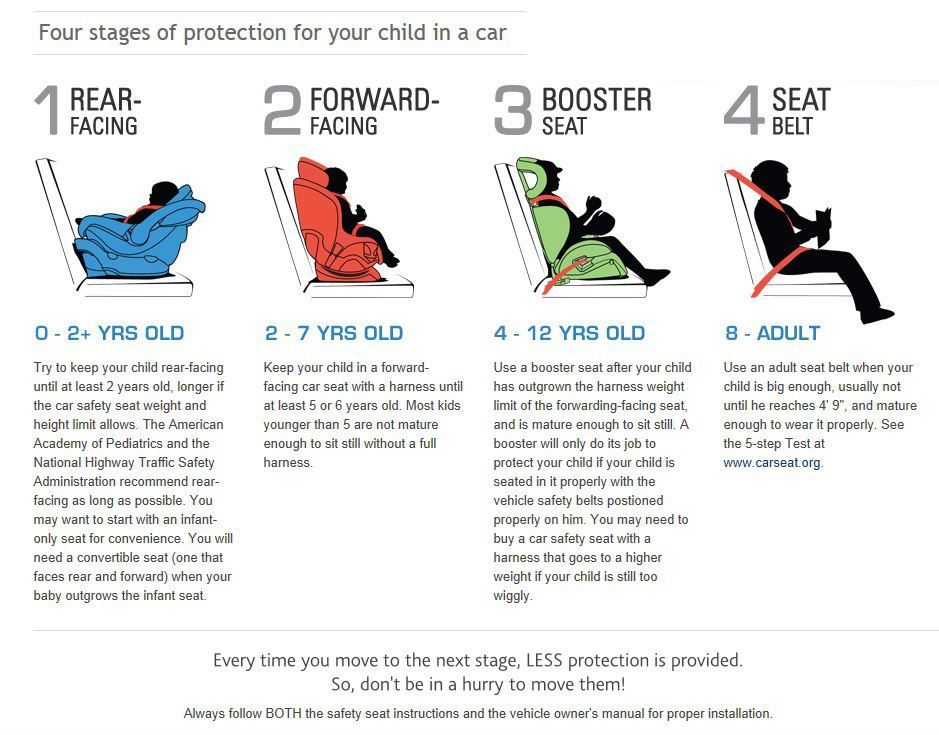 The mother communicated much more actively with the children, who were carried face to face, and they felt safer than the child who was carried facing away from him. Mother and child need communication, contact is necessary, if the child is turned away from the mother, then she communicates less with him, does not see the baby's facial expressions. When the baby is turned to face the parent, communication always happens, and it is much brighter and more colorful. She often calls the baby by name, even talks to him about nature and weather as with an adult. This moment was tested on me when I carried the baby in a sling, I constantly wanted to communicate with him, and the child reciprocated.
The mother communicated much more actively with the children, who were carried face to face, and they felt safer than the child who was carried facing away from him. Mother and child need communication, contact is necessary, if the child is turned away from the mother, then she communicates less with him, does not see the baby's facial expressions. When the baby is turned to face the parent, communication always happens, and it is much brighter and more colorful. She often calls the baby by name, even talks to him about nature and weather as with an adult. This moment was tested on me when I carried the baby in a sling, I constantly wanted to communicate with him, and the child reciprocated.
Children also sleep better when they feel safe. Security, according to Maslow's pyramid, is one of the basic needs of any person.
Contact with a parent allows children to feel calm and secure, unlike children who are being carried or carried facing away from themselves. During the study, such children experienced emotional stress and overexcitation, it was more difficult for them to fall asleep.
During the study, such children experienced emotional stress and overexcitation, it was more difficult for them to fall asleep.
The psyche of our kids is still being formed. They have yet to learn to distinguish important from insignificant details, to ignore unnecessary information and to respond to it correctly. If the baby is facing away from the mother, he feels lonely and unprotected. He needs to explore the world, but he needs to do this with his mother. Being facing his mother, he also looks around and sees everything perfectly. But the baby still does not know how to respond to him in certain situations. In this, first of all, his mother helps him - with her voice, her facial expressions. The child may be frightened by the approaching person, but when he sees that his mother is smiling, he will calm down and smile too. If there is no mother in front of the eyes, the child has to constantly make decisions for himself: how to react to this or that event. This overworks him and overloads the child's psyche.
During my consultations I talk, explain to my mother, change my intonation and always smile))) I help children make decisions and be in a good mood.
I'll tell you a very good anecdote on the subject)))
— Let's determine the cause of your neurosis, the psychiatrist suggests to the patient. - Tell me, what is your job?
– I sort oranges.
- Well, what's so difficult about that?!
– I need to sort the oranges: big ones into one basket, smaller ones into a medium one and small ones into a small one.
– So why are you nervous at such a quiet job?
– Calm?! Yes, you finally understand that all day long I have to make decisions, decisions, decisions !!
Likewise, our child has to constantly make decisions, and, as we understand, they will not always be made correctly.
Carrying a baby facing away from you causes the baby not pleasant sensations, but stress. The second part of the research showed that the heart rate in a child quickens when he is turned away from himself, and decreases when he is taken facing his mother, that is, the child calms down.
The second part of the research showed that the heart rate in a child quickens when he is turned away from himself, and decreases when he is taken facing his mother, that is, the child calms down.
When the baby is facing the mother, he has an excellent view to the left, and to the right, and back (for older children). Seeing a stranger or being frightened by a car, the baby can always hide in mommy, snuggle up to her face and ... look again. He will feel protected and explore the world with you.
He can kiss his mother's breast at any moment, which a child who is turned away from his mother cannot do.
Skin-to-skin contact between baby and mother allows premature babies to catch up with their birth peers (kangaroo method). The vibration of the mother's voice and her heartbeat act as a sedative. The baby's tummy warmed by your warmth helps to cope with colic.
Now about vision.
A child's vision is formed before school age. In the first month of life, the baby reacts to light, then begins to distinguish between the chest, this is also helped by touch and smell. By 4-6 months, the baby begins to distinguish the face of the mother, the faces of those who communicate with him and whom he often sees. Further, he begins to distinguish between such figures as a cube, a ball, and others. Why then turn the baby to face away from you? He doesn't see what you see. He will be nervous, worried, overexcited, and not explore the world with his mother. Many say - and he likes it so much. If a child likes sweets, we will not feed him only sweets, will we? Mom knows that the baby should be breastfed, and the eldest needs proper, balanced nutrition. Also here, the baby may like the fact that everything floats and flickers before his eyes, but he does not understand how harmful it can be. Mom understands!
In the first month of life, the baby reacts to light, then begins to distinguish between the chest, this is also helped by touch and smell. By 4-6 months, the baby begins to distinguish the face of the mother, the faces of those who communicate with him and whom he often sees. Further, he begins to distinguish between such figures as a cube, a ball, and others. Why then turn the baby to face away from you? He doesn't see what you see. He will be nervous, worried, overexcited, and not explore the world with his mother. Many say - and he likes it so much. If a child likes sweets, we will not feed him only sweets, will we? Mom knows that the baby should be breastfed, and the eldest needs proper, balanced nutrition. Also here, the baby may like the fact that everything floats and flickers before his eyes, but he does not understand how harmful it can be. Mom understands!
_______________________________________________________________
How to teach a baby who is accustomed to “facing the world” to face his mother in order to properly carry him in his arms and in a sling.
Standard situation: a mother wants to carry her baby in a sling, but he starts to act up and dodge. We temporarily put the sling aside, we can use it as a blanket, so that the baby is already used to it. Now we begin to teach the baby to the correct position on his hands without a sling. From the moment the mother decided to carry the baby in the correct position - facing herself, the child is no longer turned away from us. If you turn the baby facing away from you, you will have to start all over again. Mom gave slack, and the kids understand this very well. Since the mother decided to wear it this way, and she is confident in her decision, then it will be so, and this must be passed on and instilled in the baby.
You can carry your baby in any position, but only facing you. The most comfortable is the position on the shoulder and on the hip for children who hold their heads.
These positions offer the greatest scope for viewing.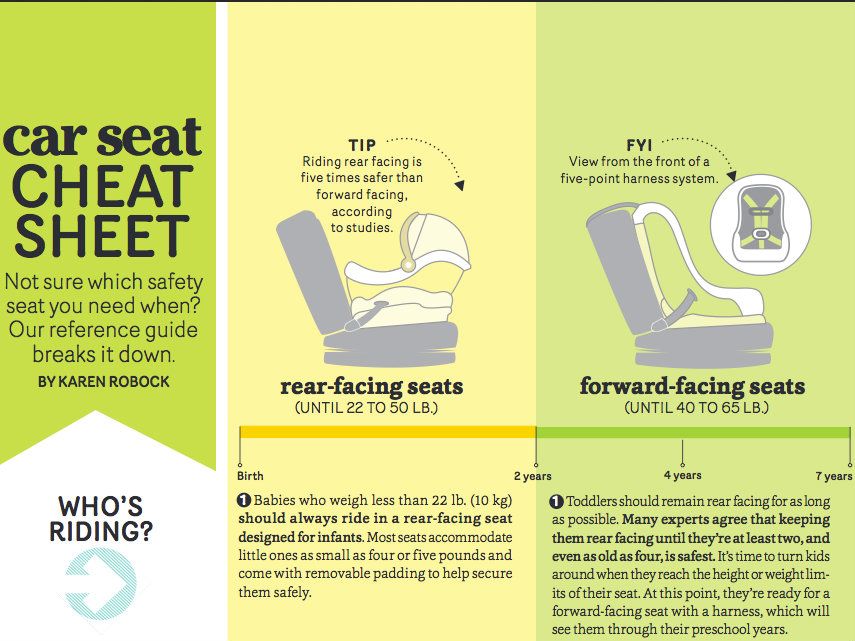 If the baby wants to roll over, is naughty and cries, mom needs to talk to him, you need to be completely calm. The mood of the mother is transmitted to the child. Chat and talk with your baby. Wear it on your hip and be an actress. Talk to him teeth - tell him that now mom will wear you like this and only like this: “No, my dear! I will not turn you over again, no matter how you ask! ”Sing your favorite song to him, show him something interesting, change intonation to distract the baby. Hang slingobus and toys around your neck, give them to him in his hands, at the same time fine motor skills of the child's hands will develop.
If the baby wants to roll over, is naughty and cries, mom needs to talk to him, you need to be completely calm. The mood of the mother is transmitted to the child. Chat and talk with your baby. Wear it on your hip and be an actress. Talk to him teeth - tell him that now mom will wear you like this and only like this: “No, my dear! I will not turn you over again, no matter how you ask! ”Sing your favorite song to him, show him something interesting, change intonation to distract the baby. Hang slingobus and toys around your neck, give them to him in his hands, at the same time fine motor skills of the child's hands will develop.
Be sure to offer breasts. The baby should form the mother-arms-breast association, and later - the sling. Change position from one hip to the other, on the stomach, in a cradle. Sing a song, dance with him, put on a sling, let the baby get used to it.
If you are tired, and the baby continues to be naughty - put him on the bed, but do not give in to crying, do not carry him away from you. Later, you can try to place the baby in a sling. It is better to do this in the morning, when the baby slept, ate and did all the necessary morning procedures, when he is satisfied. You can go outside or a balcony, but again, talk with the baby - he will hear and listen to you, and the fresh air has a calming effect on the children. We take our time and confidently put on the sling. I had a May-sling when I was retraining my nephews (the mothers did not express much desire and entrusted them to me). I went out into the yard, lifted the back of the sling, we, walking, looked at the grapes in the yard, I told how tasty and beautiful it was. Then, imperceptibly for the baby, I threw on one strap, and then the second, continuing to hug the baby, sway and walk. Don't stop and don't worry. The child was capricious, we remove the straps back, with the words: “No, no baby! Everything is fine, look at the sun!”)))) I hope everything will work out for you, because after winding the sling and swaying a little, my nephew immediately fell asleep in it, and this was our victory.
Later, you can try to place the baby in a sling. It is better to do this in the morning, when the baby slept, ate and did all the necessary morning procedures, when he is satisfied. You can go outside or a balcony, but again, talk with the baby - he will hear and listen to you, and the fresh air has a calming effect on the children. We take our time and confidently put on the sling. I had a May-sling when I was retraining my nephews (the mothers did not express much desire and entrusted them to me). I went out into the yard, lifted the back of the sling, we, walking, looked at the grapes in the yard, I told how tasty and beautiful it was. Then, imperceptibly for the baby, I threw on one strap, and then the second, continuing to hug the baby, sway and walk. Don't stop and don't worry. The child was capricious, we remove the straps back, with the words: “No, no baby! Everything is fine, look at the sun!”)))) I hope everything will work out for you, because after winding the sling and swaying a little, my nephew immediately fell asleep in it, and this was our victory.