Forcep assisted birth
Assisted delivery with forceps: MedlinePlus Medical Encyclopedia
In an assisted vaginal delivery, the doctor will use special tools called forceps to help move the baby through the birth canal.
Forceps look like 2 large salad spoons. The doctor uses them to guide the baby's head out of the birth canal. The mother will push the baby the rest of the way out.
Another technique your doctor may use to deliver the baby is called vacuum assisted delivery.
Even after your cervix is fully dilated (open) and you have been pushing, you may still need help getting the baby out. Reasons include:
- After pushing for several hours, the baby may be close to coming out, but needs help to get through the last part of the birth canal.
- You may be too tired to push any longer.
- A medical problem may make it risky for you to push.
- The baby may be showing signs of stress and need to come out faster than you can push it out on your own
Before forceps can be used, your baby needs to be far enough down the birth canal. The baby's head and face must also be in the right position. Your doctor will check carefully to make sure it is safe to use forceps.
Most women will not need forceps to help them deliver. You may feel tired and tempted to ask for a little help. But if there is not a true need for assisted delivery, it is safer for you and your baby to deliver on your own.
You will be given medicine to block pain. This may be an epidural block or a numbing medicine placed in the vagina.
The forceps will be carefully placed on the baby's head. Then, during a contraction, you will be asked to push again. At the same time, the doctor will gently pull to help deliver your baby.
After the doctor delivers the baby's head, you will push the baby the rest of the way out. After delivery, you can hold your baby on your tummy if they are doing well.
If the forceps do not help move your baby, you may need to have a cesarean birth (C-section).
Most forceps-assisted vaginal births are safe when they are done correctly by an experienced doctor. They may decrease the need for a C-section.
They may decrease the need for a C-section.
However, there are some risks with forceps delivery.
Risks for the mother are:
- More severe tears to the vagina which may require prolonged healing time and (rarely) surgery to correct
- Problems with urinating or moving your bowels after delivery
Risks for the baby are:
- Bumps, bruises or marks on the baby's head or face. They will heal in a few days or weeks.
- The head may swell or be cone-shaped. It should return to normal usually within a day or two.
- The baby's nerves may be injured by pressure from the forceps. The baby's face muscles may droop if the nerves are injured, but they will go back to normal when the nerves heal.
- The baby may be cut from the forceps and bleed. This rarely happens.
- There may be bleeding inside the baby's head. This is more serious, but very rare.
Most of these risks are not severe. When properly used, forceps rarely cause lasting problems.
Pregnancy - forceps; Labor - forceps
Foglia LM, Nielsen PE, Deering SH, Galan HL. Operative vaginal delivery. In:Landon MB, Galan HL, Jauniaux ERM, et al, eds. Gabbe's Obstetrics: Normal and Problem Pregnancies. 8th ed. Philadelphia, PA: Elsevier; 2021:chap 13.
Thorp JM, Laughon SK. Clinical aspects of normal and abnormal labor. In: Resnik R, Iams JD,Lockwood CJ, Moore TR, Greene MF, Copel JA, Silver RM, eds. Creasy and Resnik's Maternal-Fetal Medicine: Principles and Practice. 8th ed. Philadelphia, PA: Elsevier; 2019:chap 43.
Updated by: John D. Jacobson, MD, Department of Obstetrics and Gynecology, Loma Linda University School of Medicine, Loma Linda, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
Browse the Encyclopedia
Forceps or vacuum delivery - NHS
Assisted delivery
An assisted birth (also known as an instrumental delivery) is when forceps or a ventouse suction cup are used to help deliver the baby.
Ventouse and forceps are safe and only used when necessary for you and your baby. Assisted delivery is less common in women who've had a spontaneous vaginal birth before.
What happens during a ventouse or forceps delivery?
Your obstetrician or midwife should discuss with you the reasons for having an assisted birth, the choice of instrument and how it will be carried out. Your consent will be needed before the procedure can be carried out.
Find out more about consent to treatment.
You'll usually have a local anaesthetic to numb your vagina and the skin between your vagina and anus (perineum) if you have not already had an epidural.
If your obstetrician has any concerns, you may be moved to an operating theatre so a caesarean section can be carried out if needed.
It is likely a cut (episiotomy) will be needed to make the vaginal opening bigger. Any tear or cut will be repaired with stitches. Depending on the circumstances, your baby can be delivered and placed on your tummy, and your birth partner may still be able to cut the cord if they want to.
Ventouse
A ventouse (vacuum cup) is attached to the baby's head by suction. A soft or hard plastic or metal cup is attached by a tube to a suction device. The cup fits firmly on to your baby's head.
During a contraction and with the help of your pushing, the obstetrician or midwife gently pulls to help deliver your baby.
If you need an assisted birth and you are giving birth at less than 36 weeks pregnant, then forceps may be recommended over ventouse. This is because forceps are less likely to cause damage to your baby's head, which is softer at this point in your pregnancy.
Forceps
Forceps are smooth metal instruments that look like large spoons or tongs. They're curved to fit around the baby's head. The forceps are carefully positioned around your baby's head and joined together at the handles.
With a contraction and your pushing, an obstetrician gently pulls to help deliver your baby.
There are different types of forceps. Some are specifically designed to turn the baby to the right position to be born, such as if your baby is lying facing upwards (occipito-posterior position) or to one side (occipito-lateral position).
Why might I need ventouse or forceps?
An assisted delivery is used in about 1 in 8 births, and may be needed if:
- you have been advised not to try to push out your baby because of an underlying health condition (such as having very high blood pressure)
- there are concerns about your baby's heart rate
- your baby is in an awkward position
- your baby is getting tired and there are concerns that they may be in distress
- you're having a vaginal delivery of a premature baby – forceps can help protect your baby's head from your perineum
A children's doctor (paediatrician) is usually present to check your baby's condition after the birth. After the birth you may be given antibiotics through a drip to reduce your risk of getting an infection.
What are the risks of a ventouse or forceps birth?
Ventouse and forceps are safe ways to deliver a baby, but there are some risks that should be discussed with you.
Vaginal tearing or episiotomy
This will be repaired with dissolvable stitches.
3rd or 4th degree vaginal tear
There's a higher chance of having a vaginal tear that involves the muscle or wall of the anus or rectum, known as a 3rd- or 4th-degree tear.
This kind of tear affects:
- 3 in every 100 women having a vaginal birth
- 4 in every 100 women having a ventouse delivery
- 8 to 12 in every 100 women having a forceps delivery
Higher risk of blood clots
After an assisted birth, there's a higher chance of blood clots forming in the veins in your legs or pelvis. You can help prevent this by moving around as much as you can after the birth.
You may also be advised to wear special anti-clot stockings and have injections of heparin, which makes the blood less likely to clot.
Urinary incontinence
Urinary incontinence (leaking pee) is not unusual after childbirth. It's more common after a ventouse or forceps delivery. You should be offered physiotherapy to help prevent this happening, including advice on pelvic floor exercises.
You should be offered physiotherapy to help prevent this happening, including advice on pelvic floor exercises.
Anal incontinence
Anal incontinence (involuntary farting or leaking poo) can happen after birth, particularly if there's been a 3rd or 4th degree tear. Because there's a higher risk of these tears happening with an assisted delivery, anal incontinence is more likely.
Are there any risks to the baby?
The risks to your baby include:
- a mark on your baby's head (chignon) being made by the ventouse cup – this usually disappears within 48 hours
- a bruise on your baby's head (cephalohaematoma) – this happens to around 1 to 12 of all 100 babies during a ventouse assisted delivery – the bruise is usually nothing to worry about and should disappear with time
- marks from forceps on your baby's face – these usually disappear within 48 hours
- small cuts on your baby's face or scalp – these affect 1 in 10 babies born using assisted delivery and heal quickly
- yellowing of your baby's skin and eyes – this is known as jaundice, and should pass in a few days
Afterwards
You'll sometimes need a small tube that drains your bladder (a catheter) for up to 24 hours.
You're more likely to need this if you've had an epidural as you may not have fully regained sensation in your bladder and therefore do not know when it's full.
The Royal College of Obstretricians and Gynaecologists (RCOG) has further information about assisted delivery.
healthtalk.org has videos and written interviews of women talking about their experiences of vaginal birth, including forceps and ventouse.
Find out more about what happens in labour and pain relief in labour.
Video: what is involved in an assisted birth?
In this video, a midwife explains what an assisted birth is and what is involved.
Media last reviewed: 20 March 2020
Media review due: 20 March 2023
Page last reviewed: 9 June 2020
Next review due: 9 June 2023
Vaginal delivery with forceps and vacuum. Dangerous?
Usually during natural childbirth, your baby goes out into this world on his own. But babies are not always in a hurry to be born according to the plan, in such cases, a little help may be required to transfer the baby to mother's hands. The doctor uses certain methods to deliver the baby, which we will discuss in this article.
But babies are not always in a hurry to be born according to the plan, in such cases, a little help may be required to transfer the baby to mother's hands. The doctor uses certain methods to deliver the baby, which we will discuss in this article.
Vaginal delivery
Assisting and stimulating vaginal delivery is essential when the natural birth process does not move forward. In these cases, the medical team will use certain devices, such as forceps and a vacuum extractor, to safely reach the child.
These methods are usually used when there is a prolonged labor with more than 2-3 hours of unsuccessful efforts by the woman. Instruments may also become necessary when the doctor sees that the child's heart rate is dropping. These methods are not used until the cervix is fully dilated with the baby's head no more than 5 centimeters above the vaginal opening.
Use of forceps
Forceps are a metal device that is used to grasp the baby's head through the birth canal during prolonged labor. Tongs are like long spoons or tongs. Forceps are also used if the baby's condition worsens or if the position is incorrect. Forceps may be used when the doctor sees that the baby's face is in the wrong direction or is not moving down the birth canal. The reason for this may be uterine atony, which means that the uterus is not contracting enough. Before you get the baby with forceps, anesthesia is done in the area around the vagina. In addition, the doctor will perform an episiotomy (an incision between the vagina and anus) prior to delivery.
Benefits of using forceps
Forceps have higher success rates compared to vacuums, according to the health organization. Trained doctors who have been practicing for many years would prefer to use forceps as the ideal approach to childbirth. Second, the use of forceps poses a lower risk of developing a cephalematoma versus a vacuum extractor. A cephalematoma is a condition in which blood accumulates in the area between the bones of the skull and the tissues of the child's head.
A cephalematoma is a condition in which blood accumulates in the area between the bones of the skull and the tissues of the child's head.
Disadvantages of using forceps
The use of forceps increases the chance of vaginal tears compared to a vacuum extractor. The perineum is recovering, but this takes time. Forceps-assisted births are also associated with a risk of damage to the facial nerve. Although these complications are rare, they are more common as a result of the use of forceps.
Vacuum Birth Extractor
Doctors can also use an instrument called a vacuum extractor. The doctor attaches the cup-shaped extractor to the top of the child's head and directs him to the birth canal. The device pulls the baby's head and does not let him go back into the birth canal.
Vacuum extractor advantage
The vacuum extractor has become more commonly used because the method requires less anesthesia and pain medication compared to forceps, thus less risk.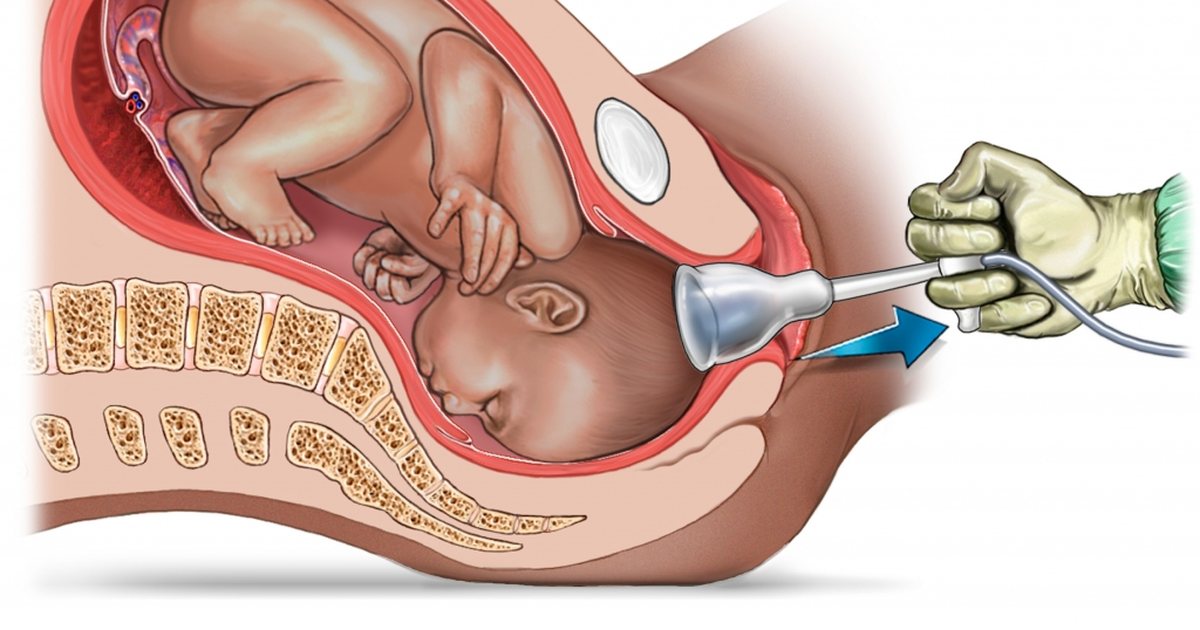
Disadvantages of using a vacuum extractor in
Although the vacuum extractor poses less of a risk, slipping off the top of the instrument makes a caesarean section unavoidable. This increases the chances of complications for both mother and baby. The vacuum extractor can also contribute to other complications such as retinal bleeding, a condition in which bleeding occurs in the blood vessels of a child's retina. The vacuum extractor also poses a risk of developing a cephalematoma. All of these complications can occur due to trauma during childbirth. In some cases, vacuum extraction can result in swelling or bruising of the baby's scalp.
Physicians should be well versed in the specific cases where these methods are applied. If you have any doubts, worries, questions about the use of forceps and a vacuum extractor, be sure to ask your gynecologist. You should be aware of the risks that arise when using these tools!!!
Measures taken during childbirth | Elite Clinic
- Preparing for childbirth
- Painkillers
- Laughing gas and other inhalable gases
- Anesthetic injections
- Pathological childbirth
- Breech presentation
- Caesarean section
- Pneumatic childbirth
- Forceps delivery
- Determination of the condition of the newborn
- Neonatal replacement excluded
- Premature baby
- Postterm baby
When deciding on possible medical pain relief, the obstetrician always assesses the situation from the point of view of two persons - mother and child.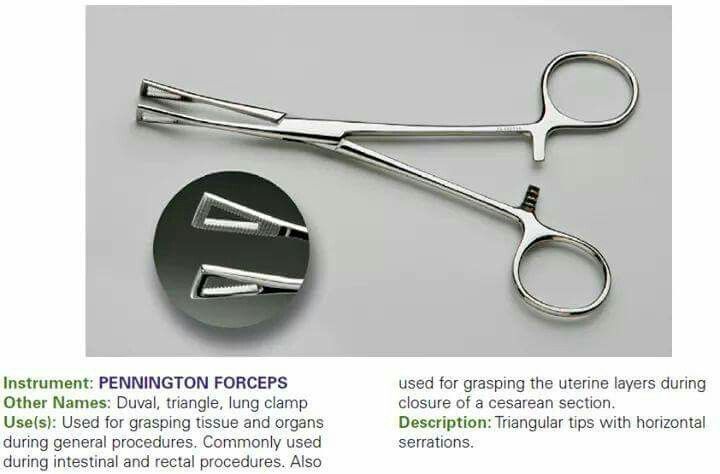 Childbirth requires a lot of mental and physical energy from both the mother and the child.
Childbirth requires a lot of mental and physical energy from both the mother and the child.
Preparation for childbirth
Psychophysical preparation for childbirth is the basis of any method of pain relief. When a woman in labor receives
sufficient information about childbirth, she can treat them appropriately. After all, a person is afraid of everything that is unknown to him and that he has not experienced before, and, seized with fear, he feels pain with greater force. The most important thing is to learn how to relax and breathe correctly at each stage of labor, which, in turn, contributes to the contraction of the uterus. From the point of view of the child being born, this method is the best, since then the possibility of a better supply of oxygen to the child is always ensured. The child's vitality is not reduced, while many painkillers adversely affect it.
Painkillers
Labor pains are not only not dangerous, but they are also positive in a certain sense. However, about 15-20% of women in labor feel such severe pain that their situation requires special measures. If necessary, every woman in labor has the opportunity to receive an effective pain reliever. The negative side of the use of painkillers is that they quickly penetrate the placenta into the fetal circulation and this can paralyze the breath of the newborn if the birth occurs within 2-3 hours after the last dose of medication. Therefore, at the end of childbirth, they try not to give painkillers.
However, about 15-20% of women in labor feel such severe pain that their situation requires special measures. If necessary, every woman in labor has the opportunity to receive an effective pain reliever. The negative side of the use of painkillers is that they quickly penetrate the placenta into the fetal circulation and this can paralyze the breath of the newborn if the birth occurs within 2-3 hours after the last dose of medication. Therefore, at the end of childbirth, they try not to give painkillers.
back to index
Laughing gas and other inhaled gases
A mixture of laughing gas and oxygen can be given without risk during the entire period of cervical dilatation, as the gases are removed from the circulation very quickly. The mixture is inhaled through the mask periodically as the onset of contractions. The gas acts so slowly that inhalation must be started even before the onset of contractions. The same applies to other inhaled gases.
back to index
Anesthetic shots
Also, anesthetic drugs pass through the placenta and can slow the fetal heart rate. They can also temporarily impair blood circulation in the uterus and placenta, and at the same time, the fetus may undergo oxygen starvation. In view of this risk, the condition of the fetus must be flawless before the anesthetic injection, which can be checked by the fetal heart curve.
They can also temporarily impair blood circulation in the uterus and placenta, and at the same time, the fetus may undergo oxygen starvation. In view of this risk, the condition of the fetus must be flawless before the anesthetic injection, which can be checked by the fetal heart curve.
The most effective and safe conduction anesthesia is epidural, in which pain almost completely or completely subsides during the opening period. In this case, an anesthetic injection is injected into the so-called. epidural site located near the spinal canal. Doses may be repeated periodically during labor. Only an anesthetist can perform this procedure. Therefore, an anesthetic injection cannot be obtained in all maternity hospitals.
back to index
Pathological childbirth
Approximately 15% of births are complicated when exceptional measures are taken, such as caesarean section, breech delivery with pneumatic apparatus, forceps.
Breech presentation
During labor, about 3% of fetuses are positioned buttocks or legs down. Usually, in the antenatal clinic, an abnormal position of the fetus is established and in the maternity hospital they try to turn it into the correct position by pressing on the stomach from above. If the fetus cannot be rotated, and it remains in the same position, even before the onset of childbirth, taking into account the size of the fetus and pelvis, the method of delivery is determined. If the fetus is in a breech presentation, childbirth is usually carried out by caesarean section, especially when it comes to first or premature births.
Usually, in the antenatal clinic, an abnormal position of the fetus is established and in the maternity hospital they try to turn it into the correct position by pressing on the stomach from above. If the fetus cannot be rotated, and it remains in the same position, even before the onset of childbirth, taking into account the size of the fetus and pelvis, the method of delivery is determined. If the fetus is in a breech presentation, childbirth is usually carried out by caesarean section, especially when it comes to first or premature births.
back to index
Caesarean section
In Finland, about every eighth woman in labor is given a caesarean section. Most often, this decision is made when, during childbirth, the fetus experiences oxygen starvation, when the placenta has descended too low or it has separated prematurely, or if measurements have shown that the pelvis is too narrow.
During the operation, the tissues of the abdomen and the anterior wall of the uterus are opened, and thus the child will be born. At the same time, the placenta and amniotic membranes are removed. Correction after surgery lasts longer than with normal childbirth. Usually, a woman in labor is discharged 8-10 days after the operation.
At the same time, the placenta and amniotic membranes are removed. Correction after surgery lasts longer than with normal childbirth. Usually, a woman in labor is discharged 8-10 days after the operation.
Caesarean section can be performed under general anesthesia or spinal cord epidural anesthesia. With
this, the mother may not sleep, and feel the birth of her child. The operation itself usually lasts 30 to 40 minutes.
Even though the mother had a caesarean section, she can give birth to her next child naturally. However, after repeated caesarean sections, normal delivery is not considered possible.
back to index
Pneumatic childbirth
When the fetus is at risk of oxygen starvation, or uterine contractions have subsided and the pushing period is delayed, the baby may be assisted to be born with a pneumatic device. The doctor puts a plastic or metal cup on the fetal head, which, under the influence of lower pressure, sticks to the fetal head. Thus, the presenting part of the fetus is firmly captured.
Thus, the presenting part of the fetus is firmly captured.
The mother is pushing as usual, and the pneumatic apparatus is used as an auxiliary tool during the period of pushing. Of all births, births with the help of a pneumatic device account for 2-3%. The method is safe for mother and child. The bump that appears on the head of the child disappears within a few days.
back to index
Forceps delivery
Forceps delivery used to be as common as pneumatic delivery is now. Then forceps were also used in complicated childbirth instead of caesarean section. Therefore, the use of forceps is still avoided during childbirth. In recent years, the use of forceps during childbirth has again become more frequent. Today, forceps are used especially when the heartbeat slows down towards the end of labor and the fetus is at risk of oxygen starvation. In this case, the child can be taken out much faster with forceps than with a pneumatic device and thus avoid the risk of oxygen starvation. In such cases, forceps can be considered a quick, good and safe tool.
In such cases, forceps can be considered a quick, good and safe tool.
back to contents
Determining the state of the newborn
Immediately after birth, the mouth, pharynx and nostrils of the baby are cleaned from mucus and amniotic fluid. The condition of the newborn is assessed according to the so-called. Apgar scale. Points are given for the work of the heart, skin color, breathing, elasticity and irritability.
Most points 10. As a rule, one point is reduced due to skin color. However, do not give too much importance to points.
back to index
Replacement of newborns excluded
Even before the cord is cut, the newborn is identified to rule out the possibility of replacement. Usually, a plastic identification bracelet is used for this. and even in the delivery room they put a plate with a number on a chain around the neck of a newborn. The mother is identified by the same number as the child.
back to index
Premature baby
A premature baby is one who was born more than four weeks before the due date.












