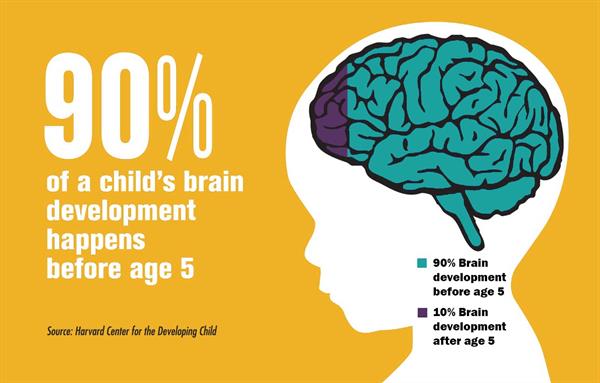
First part of brain to develop
Child Development 101: Early Brain Development
The human brain, that magnificent organ that gives us the potential to run marathons, compose symphonies and launch satellites, begins forming about three weeks after conception. Although much of what occurs during early brain development is genetically determined, some evidence suggests that children’s earliest experiences can affect how their brain develops.
According to Christine Dobson, director of programs and research at ChildTrauma Academy, a Houston-based organization dedicated to improving the lives of maltreated children, “It’s in the context of a safe, protective environment that healthy development occurs.”
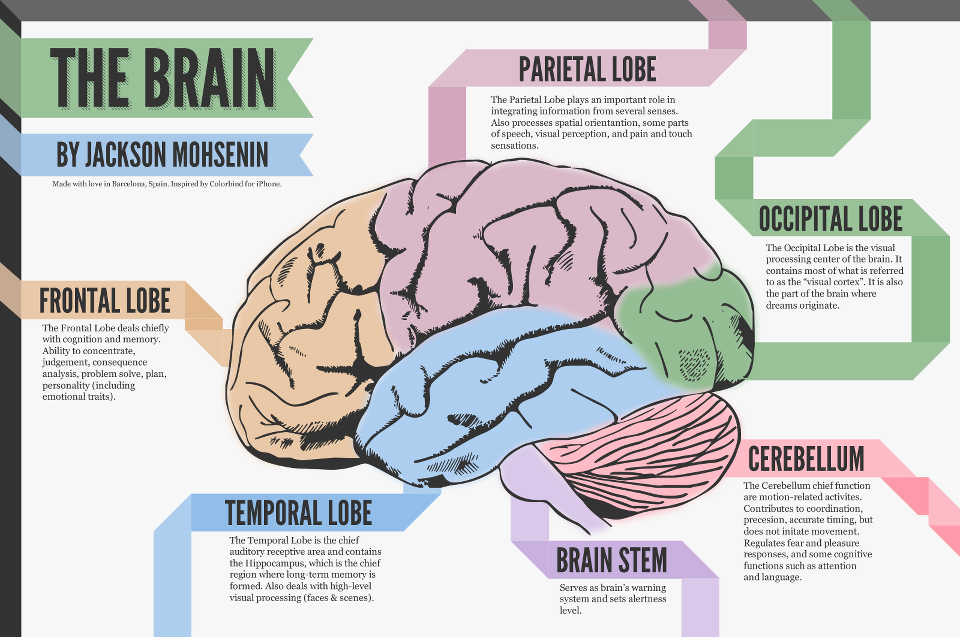
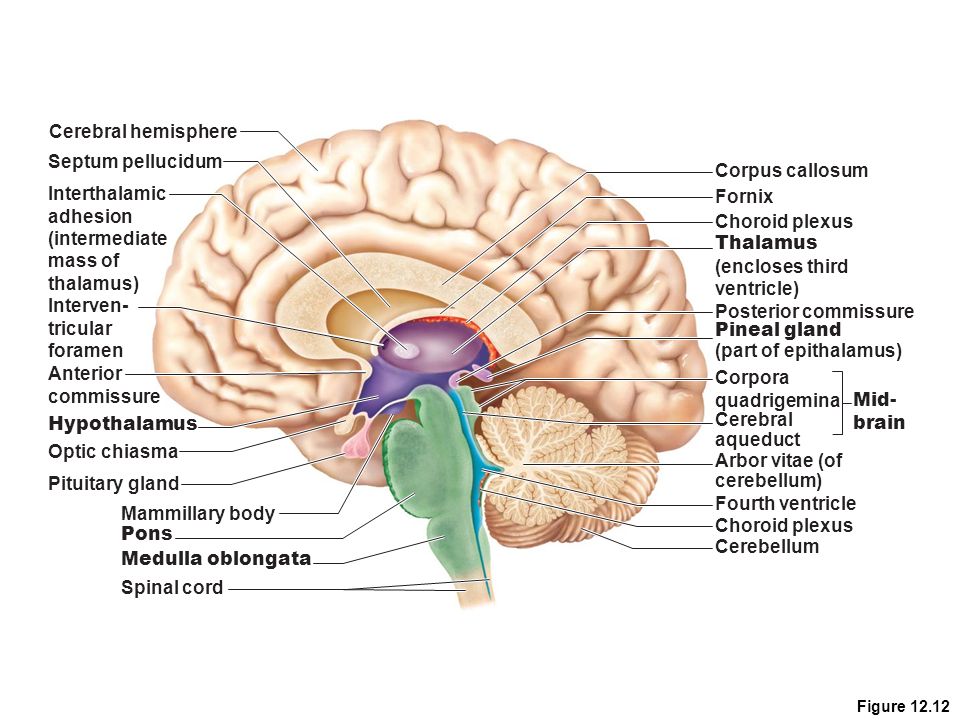
Although the brainstem is the first part of the brain to develop, the higher parts are evolving simultaneously but at different rates. The cerebral cortex – the part of the brain that controls thought, feeling, language and the senses – is the last to mature and begins functioning shortly before a baby is born.
To illustrate, take Elisa, a healthy little girl. As a newborn, Elisa’s brain is 25 percent the size of an adult brain. During what scientists call the “exuberant period,” the brain cells in Elisa’s cerebral cortex are forming the connections necessary for early milestones such as color vision, emotional attachments and voluntary actions like grasping. By age 2, her brain has produced more than a hundred trillion of these connections, also known as synapses.
Ideally, children born into supportive environments will have caregivers who regularly interact with them as the brain continues forming synapses. This interaction enables a toddler’s brain to develop in the areas needed for acquiring language and bonding emotionally.
“Within the brain, attachment and reward are interrelated,” Dobson said. “When a caregiver responds to the needs of a crying baby, the brain makes a connection between the relief of distress and responsive human interaction. This creates a template of humans as nurturing and safe that children will carry into their future relationships.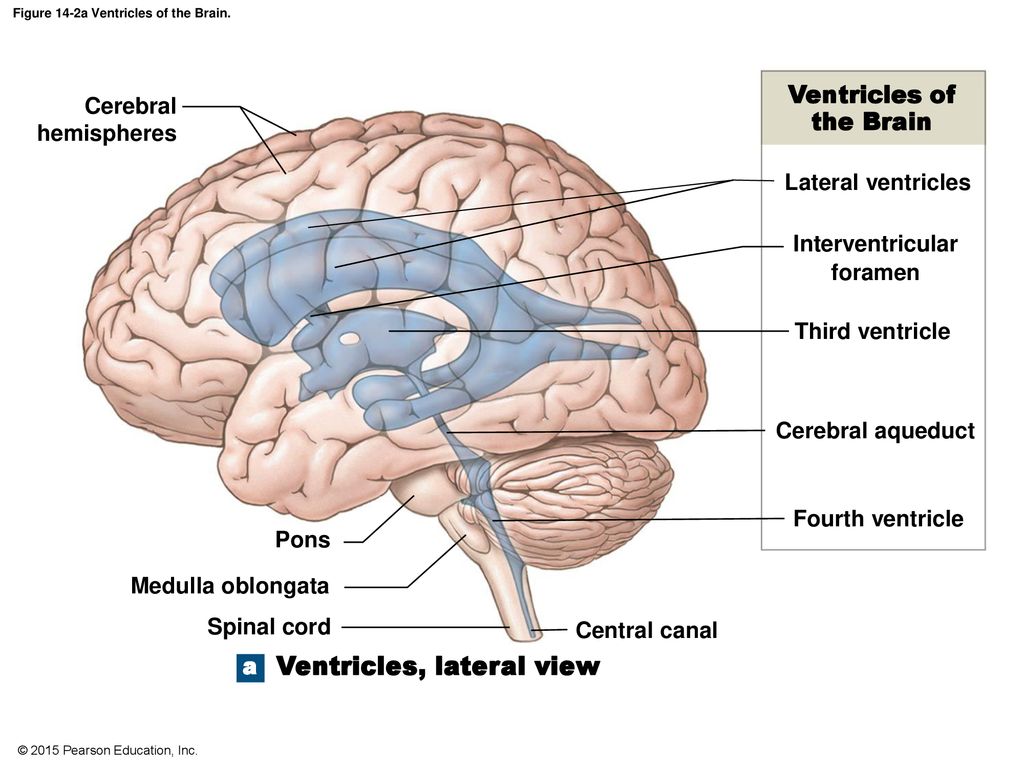 ”
”
By the time she’s 5, Elisa’s brain enables her to express opinions, form friendships and ride a bicycle. Her brain will continue developing into early adulthood, at which point marathoner, songwriter and engineer are only some of the options she will be equipped to consider.
Additional Resources
- ZERO TO THREE on Brain Development
Oct 7, 2021 | Articles, Parents
Celebrating Indigenous Peoples' Day Indigenous Peoples' Day — while not a federal holiday — is recognized on the second Monday in October by many cities and states in the United States, including the City of Los Angeles, Los Angeles County and California. The day...
Sep 29, 2021 | Articles, Parents
Celebrating Filipino American History Month Each year, the United States recognizes Filipino American History during the month of October. As the second-largest Asian American group in the country and the third-largest ethnic group in California, Filipino Americans...
Sep 14, 2021 | Articles, News & Resources, Parents
Celebrating National Hispanic Heritage Month 2021: September 15th – October 15th Hispanic communities — the largest ethnic minority group in the United States, according to Pew Research Center — have made enormous contributions to the history, culture and achievements. ..
..
Aug 23, 2021 | Parents
For This New Mom, a Doula was the Key to Joyous Childbirth When Terika Hameth found out she was pregnant last year, her initial joy was soon overwhelmed by anxiety. “I thought, ‘What if I die?’” she said. Her fear was not misplaced. Black women in Los Angeles County...
Aug 19, 2021 | Parents
Get Out & Play: How Often do Preschoolers Play Outside with Their Parents? Just more than half of preschool-aged children go outside to play with their parents daily, and whether or not they do often depends on factors like the child's gender, the mother's...
Aug 16, 2021 | Literacy, Parents, Ready for School
Raising Biliterate, Bilingual Kids Equals Double the Benefits My jaw dropped when I heard my little ones rattle off Spanish for the first time. Had all of that reading in Spanish finally paid off? The answer: yes. (Along with a little help from Dora.) In our house, we...
Aug 3, 2021 | Parents, Race Equity
Black Breastfeeding Week is August 25-31! When it comes to breastfeeding, racial equity is an issue.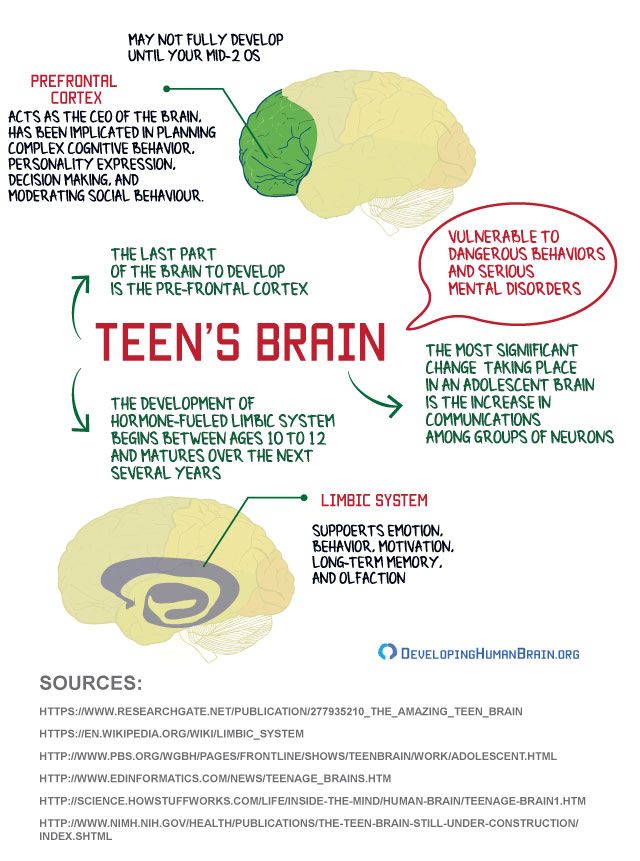 According to the Centers for Disease Control, fewer than 60% of Black mothers have ever breastfed compared to 75% of white mothers. Breastfeeding builds immunities, is...
According to the Centers for Disease Control, fewer than 60% of Black mothers have ever breastfed compared to 75% of white mothers. Breastfeeding builds immunities, is...
Aug 3, 2021 | Parents, Physical Health, Ready for School
August is Immunization Awareness Month Thanks to immunizations over the last three generations, many serious diseases are now a thing of the past. But recent outbreaks of measles — infecting more than 1,000 people nationwide — have prompted discussion and legislative...
Aug 3, 2021 | Parents, Ready for School
Child Development 101: Teaching Dual-Language Learners According to child development experts, newborns have the capacity to learn many languages at once without getting confused because, as their brain develops, so too does the ability to separate one language from...
Jun 11, 2021 | Parents, Race Equity
Celebrating Juneteenth: Freedom Day While Americans traditionally celebrate July 4th as the anniversary of the signing of the Declaration of Independence which declared the original colonies to be free from British rule, the reality of the matter is that not everyone. ..
..
A Practical Guide to Developing Resilient Learners
What we have learned about the process of brain development helps us understand more about the roles both genetics and the environment play in our development. It appears that genetics predispose us to develop in certain ways, but our experiences, including our interactions with other people, have a significant impact on how our predispositions are expressed. Research now shows that many capacities thought to be fixed at birth are actually dependent on a sequence of experiences combined with heredity. Both factors are essential for optimum development of the human brain (Shonkoff & Phillips, 2000).
Early brain development
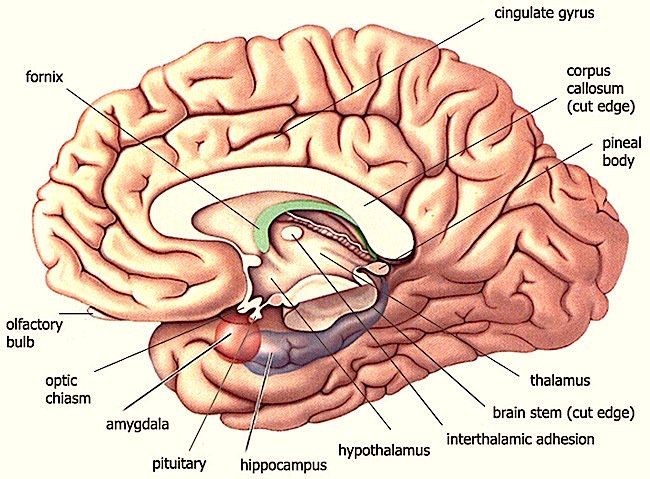
The raw material of the brain is the nerve cell, called the neuron. During fetal development, neurons are created and migrate to form the various parts of the brain. As neurons migrate, they also differentiate, or specialise, to govern specific functions in the body in response to chemical signals (Perry, 2002). This process of development occurs sequentially from the ‘bottom up,’ that is, from areas of the brain controlling the most primitive functions of the body (e.g., heart rate, breathing) to the most sophisticated functions (e.g., complex thought) (Perry, 2000). The first areas of the brain to fully develop are the brainstem and midbrain; they govern the bodily functions necessary for life, called the autonomic functions. At birth, these lower portions of the nervous system are very well developed, whereas the higher regions (the limbic system and cerebral cortex) are still rather primitive. Higher function brain regions involved in regulating emotions, language, and abstract thought grow rapidly in the first three years of life (Zero to Three, 2012).
This process of development occurs sequentially from the ‘bottom up,’ that is, from areas of the brain controlling the most primitive functions of the body (e.g., heart rate, breathing) to the most sophisticated functions (e.g., complex thought) (Perry, 2000). The first areas of the brain to fully develop are the brainstem and midbrain; they govern the bodily functions necessary for life, called the autonomic functions. At birth, these lower portions of the nervous system are very well developed, whereas the higher regions (the limbic system and cerebral cortex) are still rather primitive. Higher function brain regions involved in regulating emotions, language, and abstract thought grow rapidly in the first three years of life (Zero to Three, 2012).
Figure 3.1: Image courtesy of Beacon House Therapeutic Services & Trauma Team | 2020 | www.beaconhouse.org.uk This diagram cannot be reproduced without prior perimission from Beacon House.
Brain development in childhood
Brain development or learning, is actually the process of creating, strengthening, and discarding connections among the neurons. These connections are called synapses. Synapses organise the brain by forming pathways that connect the parts of the brain governing everything we do—from breathing and sleeping to thinking and feeling. This is the essence of postnatal brain development, because at birth, very few synapses have been formed. The synapses present at birth are primarily those that govern our bodily functions such as heart rate, breathing, eating, and sleeping. The development of synapses occurs at an astounding rate during a child’s early years in response to that child’s experiences. At its peak, the cerebral cortex of a healthy toddler may create two million synapses per second (Zero to Three, 2012). By the time children are two years old, their brains have approximately 100 trillion synapses, many more than they will ever need. Based on the child’s experiences, some synapses are strengthened and remain intact, but many are gradually discarded. This process of synapse elimination—or pruning—is a normal part of development (Shonkoff & Phillips, 2000).
These connections are called synapses. Synapses organise the brain by forming pathways that connect the parts of the brain governing everything we do—from breathing and sleeping to thinking and feeling. This is the essence of postnatal brain development, because at birth, very few synapses have been formed. The synapses present at birth are primarily those that govern our bodily functions such as heart rate, breathing, eating, and sleeping. The development of synapses occurs at an astounding rate during a child’s early years in response to that child’s experiences. At its peak, the cerebral cortex of a healthy toddler may create two million synapses per second (Zero to Three, 2012). By the time children are two years old, their brains have approximately 100 trillion synapses, many more than they will ever need. Based on the child’s experiences, some synapses are strengthened and remain intact, but many are gradually discarded. This process of synapse elimination—or pruning—is a normal part of development (Shonkoff & Phillips, 2000). By the time children reach adolescence, about half of their synapses have been discarded, leaving the number they will have for most of the rest of their lives.
By the time children reach adolescence, about half of their synapses have been discarded, leaving the number they will have for most of the rest of their lives.
Another important process that takes place in the developing brain is myelination. Myelin is the white fatty tissue that forms a sheath to insulate mature brain cells, thus ensuring clear transmission of neurotransmitters across synapses. Young children process information slowly because their brain cells lack the myelin necessary for fast, clear nerve impulse transmission (Zero to Three, 2012). Like other neuronal growth processes, myelination begins in the primary motor and sensory areas (the brain-stem and cortex) and gradually progresses to the higher-order regions that control thought, memories, and feelings. Also, like other neuronal growth processes, a child’s experiences affect the rate and growth of myelination, which continues into young adulthood (Shonkoff & Phillips, 2000). By three years of age, a baby’s brain has reached almost 90% of its adult size. The growth in each region of the brain largely depends on receiving stimulation, which spurs activity in that region. This stimulation provides the foundation for learning.
The growth in each region of the brain largely depends on receiving stimulation, which spurs activity in that region. This stimulation provides the foundation for learning.
Brain Development in Adolescence
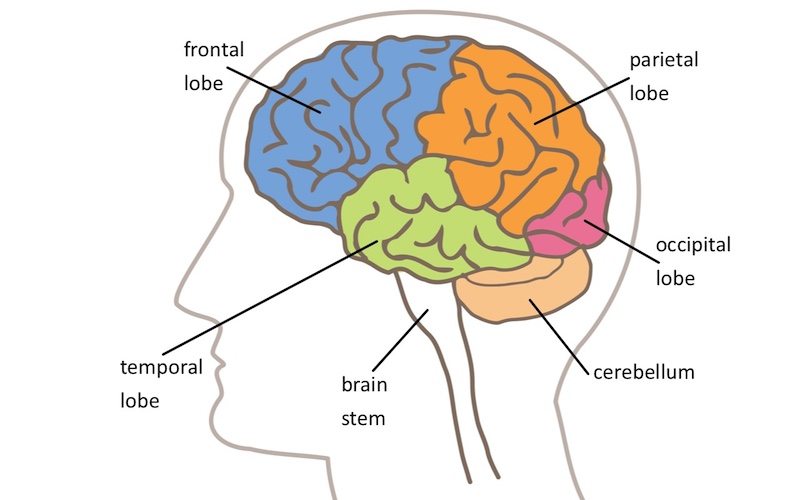
Brain imaging technologies have provided evidence of the brain continuing to grow and develop into young adulthood – with current research pointing to the brain continuing grow and develop into the thirties (Lebel & Beaulieu, 2011). Right before puberty, adolescent brains experience a growth spurt that occurs mainly in the frontal lobe, which is the area that governs planning, impulse control, and reasoning. During the teenage years, the brain goes through a process of pruning synapses—somewhat like the infant and toddler brain— and also sees an increase in white matter and changes to neurotransmitter systems (Konrad, Firk, & Uhlhaas, 2013).
As the teenager grows into a young adult, the brain develops more myelin to insulate the nerve fibres and speed neural processing, and this myelination occurs last in the frontal lobe. Brain imaging comparisons between the brains of teenagers and the brains of young adults have shown that most of the brain areas were the same—that is, the teenage brain had reached maturity in the areas that govern such abilities as speech and sensory capabilities. The major difference was the immaturity of the teenage brain in the frontal lobe and in the myelination of that area (National Institute of Mental Health, 2001). Normal puberty and adolescence lead to the maturation of a physical body, but the brain lags behind in development, especially in the areas that allow teenagers to reason and think logically. Most teenagers act impulsively at times, using a lower area of their brains—their ‘gut reaction’—because their frontal lobes are not yet mature. Impulsive behaviour, poor decisions, and increased risk-taking are all part of the normal teenage experience. Given the dynamic nature of brain development in the teenage years, decision making during this developmental stage appears to be heavily influenced by heightened emotions, with limitations in the capacity for cognitive processes linked to the prefrontal cortex (Chamberlain, 2009).
Brain imaging comparisons between the brains of teenagers and the brains of young adults have shown that most of the brain areas were the same—that is, the teenage brain had reached maturity in the areas that govern such abilities as speech and sensory capabilities. The major difference was the immaturity of the teenage brain in the frontal lobe and in the myelination of that area (National Institute of Mental Health, 2001). Normal puberty and adolescence lead to the maturation of a physical body, but the brain lags behind in development, especially in the areas that allow teenagers to reason and think logically. Most teenagers act impulsively at times, using a lower area of their brains—their ‘gut reaction’—because their frontal lobes are not yet mature. Impulsive behaviour, poor decisions, and increased risk-taking are all part of the normal teenage experience. Given the dynamic nature of brain development in the teenage years, decision making during this developmental stage appears to be heavily influenced by heightened emotions, with limitations in the capacity for cognitive processes linked to the prefrontal cortex (Chamberlain, 2009).
Plasticity—The Influence of Environment
Researchers have coined the term ‘plasticity’ to describe the changes in the brain in response to changes in the environment, and its related patterns of activation in the brain (Perry, 2006). The rate and types of changes in neuronal pathways has been found to be different in each stage of development (Perry, 2006). For example, the lower parts of the brain – controlling basic functions such as breathing and heart rate – have been found to be less flexible, or plastic, than the higher functioning cortex, that control higher level cognitions. While the plasticity of the areas of brain like prefrontal cortex decreases as a child gets older, some degree of plasticity remains in the brain (Perry, 2006). Research continues to inform our understanding of lifelong learning, coping and resilience in the face of adverse events. The developing brain’s ongoing adaptations are the result of both genetics and experience. Our brains prepare us to expect certain experiences by forming the pathways needed to respond to those experiences. For example, our brains are ‘wired’ to respond to the sound of speech; when babies hear people speaking, the neural systems in their brains responsible for speech and language receive the necessary stimulation to organise and function (Perry, 2006).
For example, our brains are ‘wired’ to respond to the sound of speech; when babies hear people speaking, the neural systems in their brains responsible for speech and language receive the necessary stimulation to organise and function (Perry, 2006).
The activation of appropriate pathways in development has been found to be important. For example, research has found that the more babies are exposed to language in the form of caregivers and adults speaking, the stronger their neural pathways related to speech and language. This principle of neurodevelopment has been referred to as ‘use it or lose it’ (Shore, 2015) where through processes of creating, strengthening, and discarding synapses that our brains adapt to the challenges and opportunities of their developmental environment. Regardless, all children need stimulation and nurturance for healthy development. When these are lacking in cases of maltreatment or deprivation, the child’s brain development may be impacted. The brain’s plasticity to its environment means that it changes in response to a negative environment just as readily as it will adapt to a positive one.
Regardless of the general environment, though, all children need stimulation and nurturance for healthy development. If these are lacking (e.g., if a child’s caretakers are indifferent, hostile, depressed, or cognitively impaired), the child’s brain development may be impaired. Because the brain adapts to its environment, it will adapt to a negative environment just as readily as it will adapt to a positive one.
Sensitive Periods
Current research on brain development suggests that there are sensitive periods for development of certain capabilities. These are referred to as ‘windows of proximal development’ – a time in the developmental process when certain parts of the brain may be most susceptible to particular experiences (Siegal, 2015). Animal studies have shed light on sensitive periods, showing, for example, that animals that are artificially blinded during the sensitive period for developing vision may never develop the capability to see, even if the blinding mechanism is later removed.
It is more difficult to study human sensitive periods, but we know that, if certain synapses and neuronal pathways are not repeatedly activated, they may be discarded, and their capabilities may diminish. For example, infants have a genetic predisposition to form strong attachments to their primary caregivers, but they may not be able to achieve strong attachments, or trusting, durable bonds if they are in a severely neglectful situation with little one-on-one caregiver contact. Children from Romanian institutions who had been severely neglected had a much better attachment response if they were placed in foster care—and thus received more stable parenting—before they were 24 months old (Smyke, Zeanah, Fox, Nelson, & Guthrie, 2010). This indicates that there is a sensitive period for attachment, but it is likely that there is a general sensitive period rather than a true cut-off point for recovery (Zeanah, Gunnar, McCall, Kreppner, & Fox, 2011).
While sensitive periods exist for development and learning, we also know that the plasticity of the brain often allows children to recover from missing certain experiences.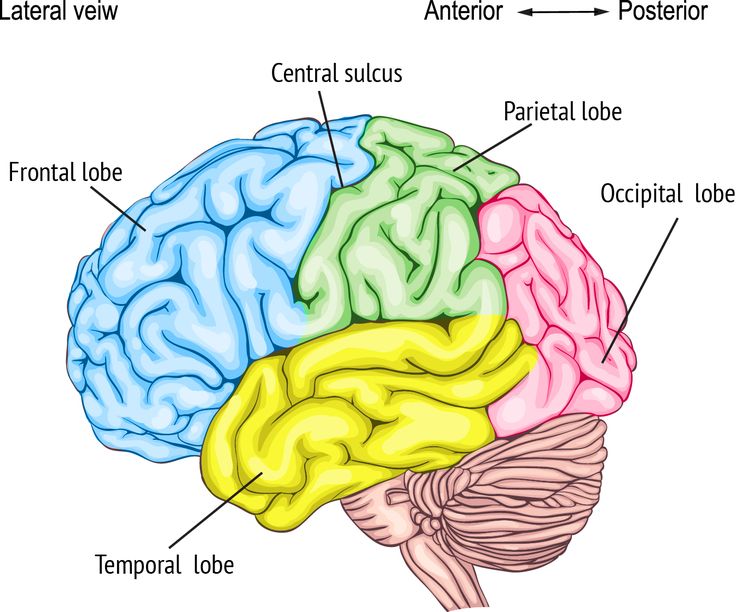 Both children and adults may be able to make up for missed experiences later in life, but it is likely to be more difficult. This is especially true if a young child was deprived of certain stimulation, which resulted in the pruning of synapses (neuronal connections) relevant to that stimulation and the loss of neuronal pathways. As children progress through each developmental stage, they will learn and master each step more easily if their brains have built an efficient network of pathways to support optimal functioning.
Both children and adults may be able to make up for missed experiences later in life, but it is likely to be more difficult. This is especially true if a young child was deprived of certain stimulation, which resulted in the pruning of synapses (neuronal connections) relevant to that stimulation and the loss of neuronal pathways. As children progress through each developmental stage, they will learn and master each step more easily if their brains have built an efficient network of pathways to support optimal functioning.
Memories
The organising framework for children’s development is based on the creation of memories. When repeated experiences strengthen a neuronal pathway, the pathway becomes encoded, and it eventually becomes a memory. Children learn to put one foot in front of the other to walk. They learn words to express themselves. And they learn that a smile usually brings a smile in return. At
some point, they no longer have to think much about these processes—their brains manage these experiences with little effort because the memories that have been created allow for a smooth, efficient flow of information.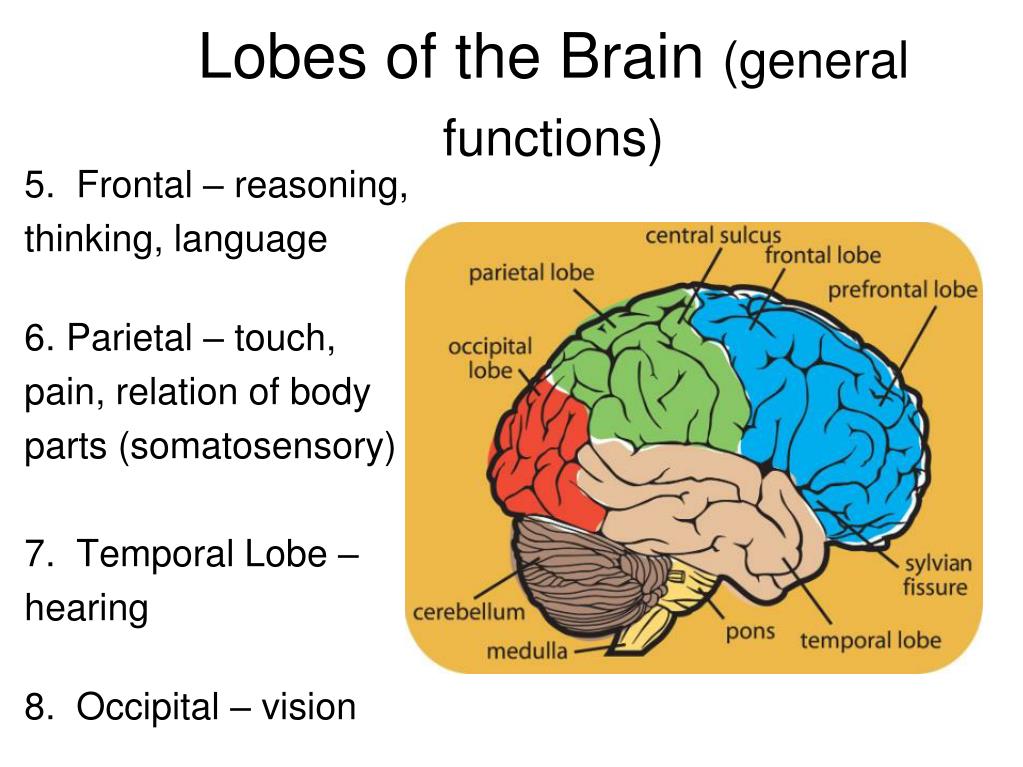
The creation of memories is part of our adaptation to our environment. Our brains attempt to understand the world around us and fashion our interactions with that world in a way that promotes our survival and, hopefully, our growth, but if the early environment is abusive or neglectful, our brains may create memories of these experiences that adversely colour our view of the world throughout our life.
Babies are born with the capacity for implicit memory, which means that they can perceive their environment and recall it in certain unconscious ways (Applegate & Shapiro, 2005). For instance, they recognise their mother’s voice from an unconscious memory. These early implicit memories may have a significant impact on a child’s subsequent attachment relationships. In contrast, explicit memory, which develops around age two, refers to conscious memories and is tied to language development. Explicit memory allows children to talk about themselves in the past and future or in different places or circumstances through the process of conscious recollection (Applegate & Shapiro, 2005).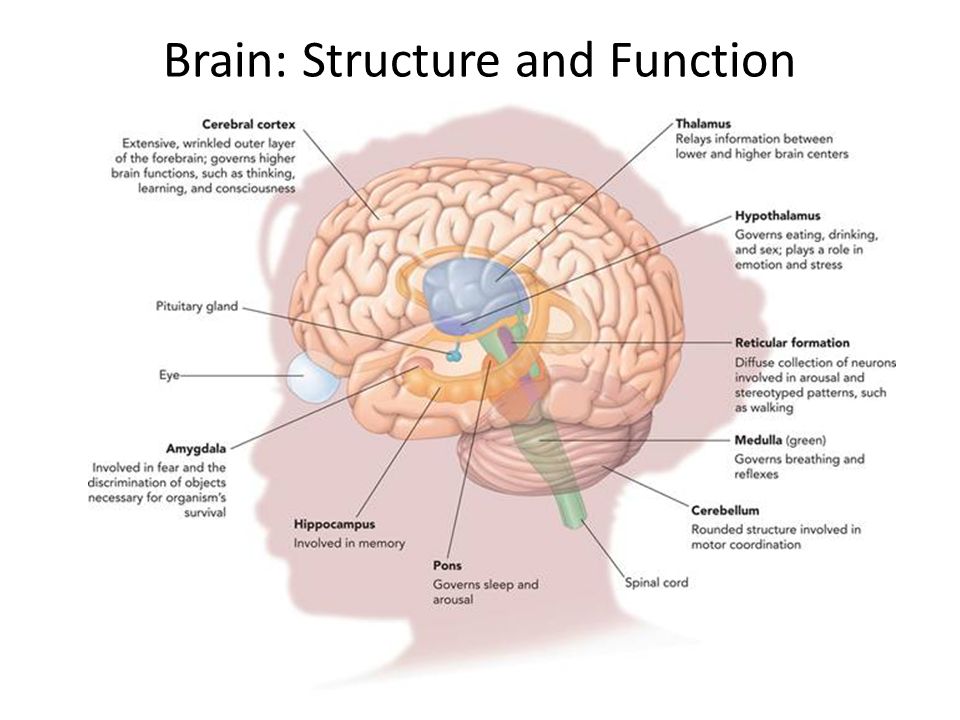
Sometimes, children who have been abused or suffered other trauma may not retain or be able to access explicit memories of their experiences. However, they may retain implicit memories of the physical or emotional sensations, and these implicit memories may produce flashbacks, nightmares, or other uncontrollable reactions (Applegate & Shapiro, 2005). This may be the case with young children or infants who suffer abuse or neglect.
Responding to Stress
We all experience different types of stress throughout our lives. The type of stress and the timing of that stress determine whether and how there is an impact on the brain. The National Scientific Council on the Developing Child (2014) outlines three classifications of stress:
- Positive stress is moderate, brief, and generally a normal part of life (e.g., entering a new child care setting). Learning to adjust to this type of stress is an essential component of healthy development.
- Tolerable stress includes events that have the potential to alter the developing brain negatively, but which occur infrequently and give the brain time to recover (e.
 g., the death of a loved one).
g., the death of a loved one). - Toxic stress includes strong, frequent, and prolonged activation of the body’s stress response system (e.g., chronic neglect).
Healthy responses to typical life stressors (i.e., positive and tolerable stress events) are complex and may change depending on individual and environmental characteristics, such as genetics, the presence of a sensitive and responsive caregiver, and past experiences. A healthy stress response involves a variety of hormone and neurochemical systems throughout the body, including the sympathetic-adrenomedullary (SAM) system, which produces adrenaline, and the hypothalamic pituitary-adrenocortical (HPA) system, which produces cortisol (National Council on the Developing Child, 2014). Increases in adrenaline help the body engage energy stores and alter blood flow. Increases in cortisol also help the body engage energy stores and also can enhance certain types of memory and activate immune responses.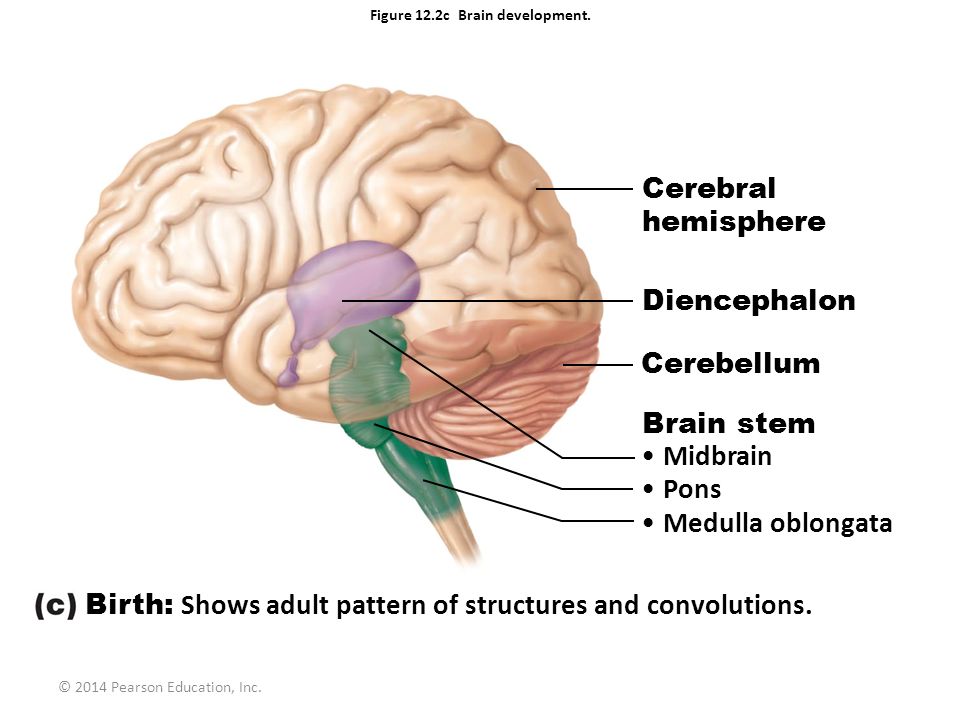 In a healthy stress response, the hormonal levels will return to normal after the stressful experience has passed.
In a healthy stress response, the hormonal levels will return to normal after the stressful experience has passed.
Please note that the above information on the three types of stress is reproduced with permission from the National Scientific Council on the Developing Child. (2014). Excessive stress disrupts the architecture of the developing brain (Working Paper 3). Retrieved from http://developingchild.harvard.edu/resources/reports_and_working_papers/working_papers/w p3/. Additional reproduction of this information is not permitted without prior permission from the National Scientific Council on the Developing Child.
Applegate, J. S., & Shapiro, J. R. (2005). Neurobiology for clinical social work theory and practice. New York: W. W. Norton & Company.
Chamberlain, L. B. (2009). The amazing teen brain: What every child advocate needs to know. Child Law Practice, 28(2), 1-2, 22–24.
Konrad, K., Firk, C., & Uhlhaas, P. J. (2013). Brain development during adolescence: Neuroscientific insights into this developmental period. Deutsches Arzteblatt International, 110(25), 425–431.
J. (2013). Brain development during adolescence: Neuroscientific insights into this developmental period. Deutsches Arzteblatt International, 110(25), 425–431.
Lebel, C., & Beaulieu, C. (2011). Longitudinal development of human brain wiring continues from childhood into adulthood. Journal of Neuroscience, 31, 10937–10947.
National Institute of Mental Health. (2001). Teenage brain: A work in progress. Retrieved from
https://public.health.oregon.gov/HealthyPeopleFamilies/Youth/AdolescentGrowthDevelopment/Documents/teenbrain.pdf
National Scientific Council on the Developing Child. (2014). Excessive stress disrupts the architecture of the developing brain (Working Paper 3). Retrieved from http://developingchild.harvard.edu/resources/reports_and_working_papers/working_papers/w
p3/
Perry, B. D. (2000). The neuroarcheology of childhood maltreatment: The neurodevelopmental costs of adverse childhood events. Child Trauma Academy. Retrieved from http://www.juconicomparte.org/recursos/Neuroarcheology%20of%20childhood%20maltreatm
Child Trauma Academy. Retrieved from http://www.juconicomparte.org/recursos/Neuroarcheology%20of%20childhood%20maltreatm
ent_zmH8.pdf
Perry, B. D. (2002). Childhood experience and the expression of genetic potential: What childhood neglect tells us about nature and nurture. Brain and Mind, 3, 79–100.
Perry, B. D. (2006). Applying principles of neurodevelopment to clinical work with maltreated and traumatized children: The neurosequential model of therapeutics. In N. B. Webb (Ed.), Working with traumatized youth in child welfare (pp. 27–52). New York: The Guilford Press.
Siegel, D. (1999). The developing mind- How relationships and the brain interact to shape who we are. New York: Guilford.
Shonkoff, J. P., & Phillips, D. A. (2000). From neurons to neighborhoods: The science of early childhood development. Washington, D.C.: National Academy Press.
Smyke, A. T., Zeanah, C. H., Fox, N. A., Nelson, C. A., & Guthrie, D. (2010). Placement in foster care enhances attachment among young children in institutions. Child Development, 81, 212–223.
A., & Guthrie, D. (2010). Placement in foster care enhances attachment among young children in institutions. Child Development, 81, 212–223.
Zeanah, C. H., Gunnar, M. R., McCall, R. B., Kreppner, J. A., & Fox, N. A. (2011). VI. Sensitive periods. Monographs of the Society for Research in Child Development, 76, 147–162.
Zero to three. (2012). FAQ’s on the brain. Retrieved from http://www.zerotothree.org/childdevelopment/ brain-development/faqs-on-the-brain.html
Brain development and executive functioning
Kati Knapp, MSc, J. Bruce Morton, PhD
Western University, Canada
(English). Translation: August 2015
Introduction
Executive functions are processes that enable many daily activities, including planning, flexible thinking, focused attention, and behavior inhibition, and continue to develop into early adulthood.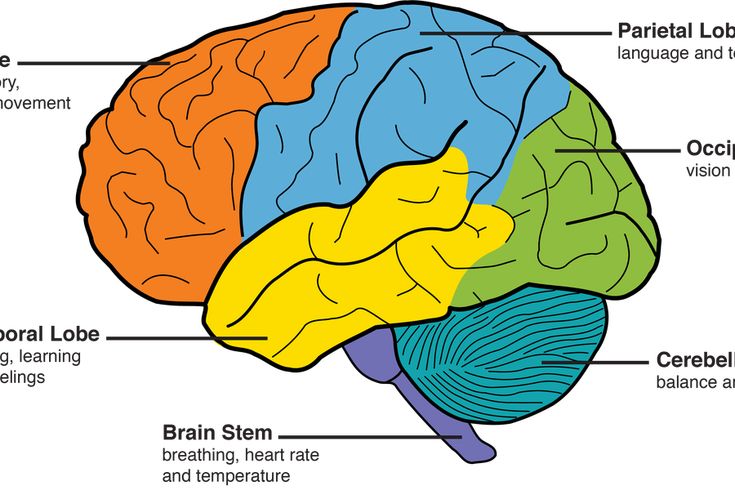 1.2 An important condition for the development of these psychological abilities is the structural and functional development of the brain. 3,4,5,6 One of the slowest developing regions of the brain is the prefrontal cortex, a large area of the cerebral cortex located in the anterior lobe. Remarkably, this area of the brain continues to develop over three decades of life. 7.8 Neuroimaging studies 9.10 and surveys of patients with brain injuries 11,12,13 suggest that the prefrontal cortex is vital for controlling attention, thinking, and behavior, in part because it connects the perceptual, emotional and motor centers located in other areas of the brain. The fact that the prefrontal cortex, 14.15 , which is important for executive control, is slowly developing, has led to the suggestion that the development of executive functioning is closely related to the maturation of the prefrontal cortex. 16,17,18 One of the consequences of this is the difficulty in dealing with such everyday tasks as not playing with a forbidden toy, which will be difficult for even normally developing children to overcome.
1.2 An important condition for the development of these psychological abilities is the structural and functional development of the brain. 3,4,5,6 One of the slowest developing regions of the brain is the prefrontal cortex, a large area of the cerebral cortex located in the anterior lobe. Remarkably, this area of the brain continues to develop over three decades of life. 7.8 Neuroimaging studies 9.10 and surveys of patients with brain injuries 11,12,13 suggest that the prefrontal cortex is vital for controlling attention, thinking, and behavior, in part because it connects the perceptual, emotional and motor centers located in other areas of the brain. The fact that the prefrontal cortex, 14.15 , which is important for executive control, is slowly developing, has led to the suggestion that the development of executive functioning is closely related to the maturation of the prefrontal cortex. 16,17,18 One of the consequences of this is the difficulty in dealing with such everyday tasks as not playing with a forbidden toy, which will be difficult for even normally developing children to overcome.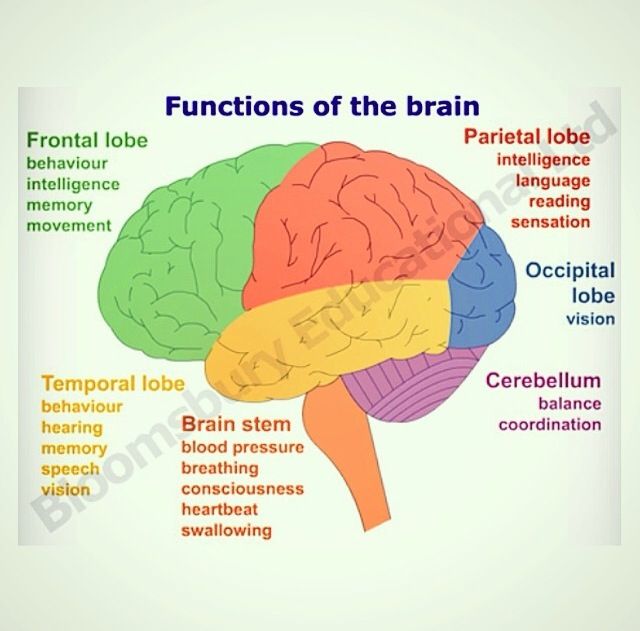
Subject
Understanding that the prefrontal cortex is important for behavioral self-regulation and that it develops gradually may explain why, for example, children find it difficult to: (a) stop one activity and switch to a new one; (b) plan ahead; (c) do more than one thing at once; (d) concentrate for a long period of time; and (e) refuse immediate remuneration. Findings from developmental cognitive neuroscience confirm that these behaviors are a normal part of growing up, and are to some extent rooted in how the brain works at this stage of life.
Issues
Understanding exactly how the development of the prefrontal cortex contributes to the development of executive processes is extremely difficult. First, executive functions are difficult to accurately define and measure, partly because basic concepts like inhibition or cognitive flexibility actually describe rather than explain behavior. Second, it is unclear whether the processes involved in controlling one type of behavior, such as language, are the same as those involved in controlling other types of behavior, such as emotions. Third, items suitable for testing executive functioning at a certain age will generally not be suitable for testing executive functioning in older children. All this complicates the comparison of executive functioning in children of different ages. Ultimately, developmental cognitive neuroscientists are interested in establishing relationships between age-related changes in executive functioning and age-related changes in brain function. To achieve this, it is necessary not only to properly define and measure executive functioning, but also to obtain direct measurements of brain functioning. One approach is functional magnetic resonance imaging (fMRI), a safe and relatively non-invasive way to study changes in brain activity that occur when people perform certain tasks. Being effective and safe to use even in newborn babies, 19.20 fMRI relies on participants remaining still for at least 5 to 10 minutes while the images are taken. A small movement of just 5-10 mm can result in images that are very fuzzy (with a high level of noise) and are virtually unanalysable.
Third, items suitable for testing executive functioning at a certain age will generally not be suitable for testing executive functioning in older children. All this complicates the comparison of executive functioning in children of different ages. Ultimately, developmental cognitive neuroscientists are interested in establishing relationships between age-related changes in executive functioning and age-related changes in brain function. To achieve this, it is necessary not only to properly define and measure executive functioning, but also to obtain direct measurements of brain functioning. One approach is functional magnetic resonance imaging (fMRI), a safe and relatively non-invasive way to study changes in brain activity that occur when people perform certain tasks. Being effective and safe to use even in newborn babies, 19.20 fMRI relies on participants remaining still for at least 5 to 10 minutes while the images are taken. A small movement of just 5-10 mm can result in images that are very fuzzy (with a high level of noise) and are virtually unanalysable.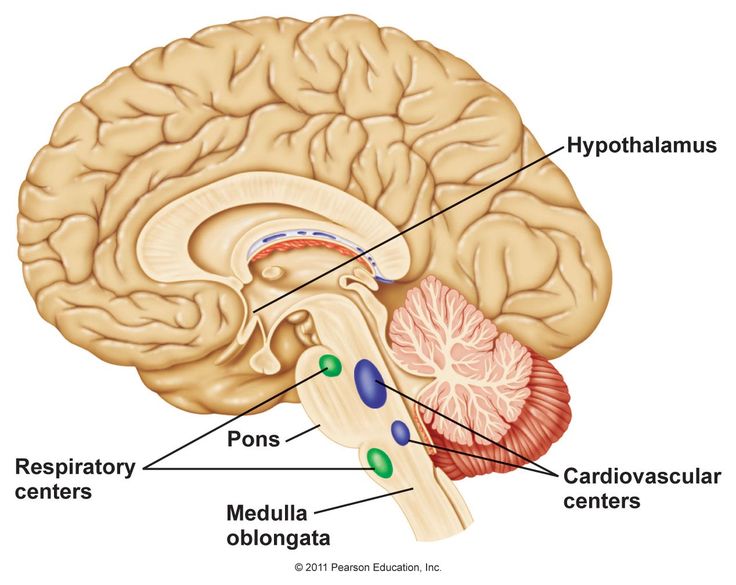 Things can get even more complicated if young children perform prescribed tasks differently from older children, so it becomes impossible to find out whether age-related differences in brain activity patterns are due solely to age differences in participants, or whether they arise in addition to differences associated with how younger and older children perform tasks. Simply put, if we instruct seven-year-olds to solve a problem in a way that four-year-olds might solve, this could, in principle, make the brain activity patterns of seven-year-olds look indistinguishable from those observed in four-year-olds. To mitigate these problems, researchers are developing new neuroimaging protocols that can be performed quickly and that do not require children to complete a task. In these so-called "resting shots," the children simply lie still for only five minutes with their eyes open. 21 The resulting images are used to study age-related changes in "intrinsic" patterns of cortical connectivity, which can then be compared to the measures of executive functions collected outside the MRI scan.
Things can get even more complicated if young children perform prescribed tasks differently from older children, so it becomes impossible to find out whether age-related differences in brain activity patterns are due solely to age differences in participants, or whether they arise in addition to differences associated with how younger and older children perform tasks. Simply put, if we instruct seven-year-olds to solve a problem in a way that four-year-olds might solve, this could, in principle, make the brain activity patterns of seven-year-olds look indistinguishable from those observed in four-year-olds. To mitigate these problems, researchers are developing new neuroimaging protocols that can be performed quickly and that do not require children to complete a task. In these so-called "resting shots," the children simply lie still for only five minutes with their eyes open. 21 The resulting images are used to study age-related changes in "intrinsic" patterns of cortical connectivity, which can then be compared to the measures of executive functions collected outside the MRI scan.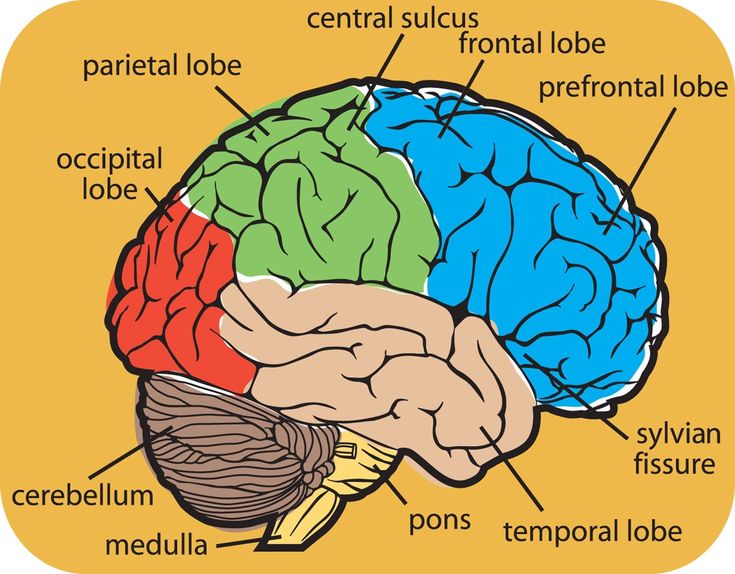
Scientific context
The results of MRI studies of developmental executive functioning paint a fascinating but complex picture. Some studies, for example, report that younger children show less activity in the prefrontal cortex (PFC) in the situation of executive function tasks than older participants, findings that are similar to the intuition that as functional development areas of the brain, it shows more stable activity, and executive functioning improves. 22.23 Other results suggest a slightly more complex story, as some areas of the PFC show increased activity with increasing age, while others show decreasing activity with increasing age. 24,25,26 One explanation for this pattern of behavior is that, early in life, executive functioning is associated with weak but diffuse PFC activity, while later in life executive functioning is associated with strong but focal PFC activity. 26 Thus, in the center of the developing area of the brain, activity increases with age, while in the surrounding areas it decreases with age. Another explanation is that certain areas within the PFC become more productive as we get older. Thus, in the early stages of development, these areas need to work very hard to maintain a certain level of activation of executive functioning. However, with further development, when these areas function more efficiently, they can maintain a relative level of activation of executive functioning with less energy expenditure. Clearly, more research is needed to elucidate this complex picture.
Another explanation is that certain areas within the PFC become more productive as we get older. Thus, in the early stages of development, these areas need to work very hard to maintain a certain level of activation of executive functioning. However, with further development, when these areas function more efficiently, they can maintain a relative level of activation of executive functioning with less energy expenditure. Clearly, more research is needed to elucidate this complex picture.
One of the strong findings of the fMRI study of the development of executive functioning activity is that there are many additional areas outside the PFC associated with the development of executive functioning activity, including the anterior cingulate, anterior insular, parietal, and motor cortex. 27.28 One explanation for these data is that executive performance tasks are very complex and involve many different sub-processes, such as keeping instructions in mind, 27,29,30 response to some stimuli and ignoring others, 22 planning and execution of a motor response, 26 evaluation of feedback. Therefore, it is possible that executive functioning tasks are associated with activity in many areas of the brain, since the tasks themselves involve many different subprocesses, each of which is associated with the activity of different areas of the brain. If this is the case, then the next challenge for future research will be to determine which subprocesses are affected by age-related changes and link these changes to changes in the functioning of specific areas of the brain. The second interpretation is that the PFC does not function independently, but is part of a larger, functionally homogeneous network. According to this view, whether the participant is keeping instructions in mind, planning a response, or evaluating feedback, there will be stable activity throughout the network. If this is true, then the next research challenge will be to determine how the organization of the larger network changes as it evolves. Opportunities include changes in areas spanning larger networks, as well as changes in the number and strength of links between their constituent areas.
Therefore, it is possible that executive functioning tasks are associated with activity in many areas of the brain, since the tasks themselves involve many different subprocesses, each of which is associated with the activity of different areas of the brain. If this is the case, then the next challenge for future research will be to determine which subprocesses are affected by age-related changes and link these changes to changes in the functioning of specific areas of the brain. The second interpretation is that the PFC does not function independently, but is part of a larger, functionally homogeneous network. According to this view, whether the participant is keeping instructions in mind, planning a response, or evaluating feedback, there will be stable activity throughout the network. If this is true, then the next research challenge will be to determine how the organization of the larger network changes as it evolves. Opportunities include changes in areas spanning larger networks, as well as changes in the number and strength of links between their constituent areas.
Key questions
- What are the constituent processes that underlie the execution of assignments for executive functions?
- Are the various executive functions associated with each individual area of the brain?
- How do changes in brain function affect changes in executive functions?
Recent research findings
Recently, researchers have begun to study age-related changes in brain networks believed to be important for executive functioning by examining changes in the connections between the PFC and other areas commonly associated with executive functioning, such as parietal cortex, anterior cingulate cortex, and insular cortex. 28 Because these networks can be observed and measured even when test subjects are at rest, many studies have recently used so-called resting-state fMRI to investigate the organization of cognitive control networks at different ages. 31.32 Initial results indicated a branching age-related transformation of networks, with new long-term associations being formed and previous short-term associations being eliminated as children get older.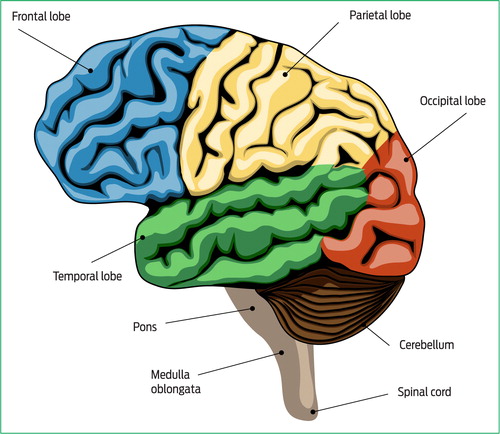 33 Recent data have challenged these initial findings and suggested that the age-related transformation of executive functioning networks may be less clear-cut than originally thought. 34 However, despite these initial errors, the study of networking continues to attract attention as researchers develop, as researchers increasingly recognize that regions of the brain work together to bring high-level thought and action to life.
33 Recent data have challenged these initial findings and suggested that the age-related transformation of executive functioning networks may be less clear-cut than originally thought. 34 However, despite these initial errors, the study of networking continues to attract attention as researchers develop, as researchers increasingly recognize that regions of the brain work together to bring high-level thought and action to life.
Unexplored areas
The most significant gap in fMRI research on developmental executive functioning is probably the lack of longitudinal studies. Unlike cross-sectional studies, in which one group of children is compared with another group of older children, longitudinal studies compare the same group of children at different ages. Needless to say, longitudinal studies are very expensive, time consuming, and can be very risky, which is the reason for the low volume of longitudinal studies to date. However, longitudinal projects have a number of important advantages over slice projects. Firstly, when comparing two groups of children of different ages, there are many factors that can potentially differ from group to group, in addition to age, differences in intellectual development, temperament / personality traits, as well as socio-economic status, not to mention others . Given that each of these factors is associated with executive functioning, conclusions regarding the importance of age in explaining group differences in brain activation patterns become irrelevant. Second, an important goal of age-related cognitive neuroscience is to discover early patterns of psychological and nervous system organization that determine future states, both positive (eg, intellectual and social well-being) and negative (eg, psychopathology). Identification of such patterns is best achieved when the same group of children is systematically observed over time until some of the children show any tendencies (e.g., giftedness, addictions, risky sexual behavior, and etc.). Only then can one go back and see which indicators of behavioral or brain studies collected earlier are successfully predicting future outcomes.
Firstly, when comparing two groups of children of different ages, there are many factors that can potentially differ from group to group, in addition to age, differences in intellectual development, temperament / personality traits, as well as socio-economic status, not to mention others . Given that each of these factors is associated with executive functioning, conclusions regarding the importance of age in explaining group differences in brain activation patterns become irrelevant. Second, an important goal of age-related cognitive neuroscience is to discover early patterns of psychological and nervous system organization that determine future states, both positive (eg, intellectual and social well-being) and negative (eg, psychopathology). Identification of such patterns is best achieved when the same group of children is systematically observed over time until some of the children show any tendencies (e.g., giftedness, addictions, risky sexual behavior, and etc.). Only then can one go back and see which indicators of behavioral or brain studies collected earlier are successfully predicting future outcomes.
Conclusions
The brain takes the first two decades of life to develop into adulthood. During this time, different areas of the brain develop at different rates. Along with the development of regions, connections between brain regions also develop gradually during childhood and adolescence. In combination with this development of brain structure and function comes an improvement in the ability to solve problems of executive functioning. Children show gradual improvement in their ability to plan ahead, switch from task to task, and slow down when asked to do so. The study of brain networks and their development may provide a practical way to quantify the relationship between brain development and executive maturation. The frontal cortex and the parietal cortex need to interact in order to effectively perform tasks for executive functioning. Effective interaction between these areas is not fully developed until late adolescence, and this may explain why the abilities of executive functioning are not formed until the second decade of life.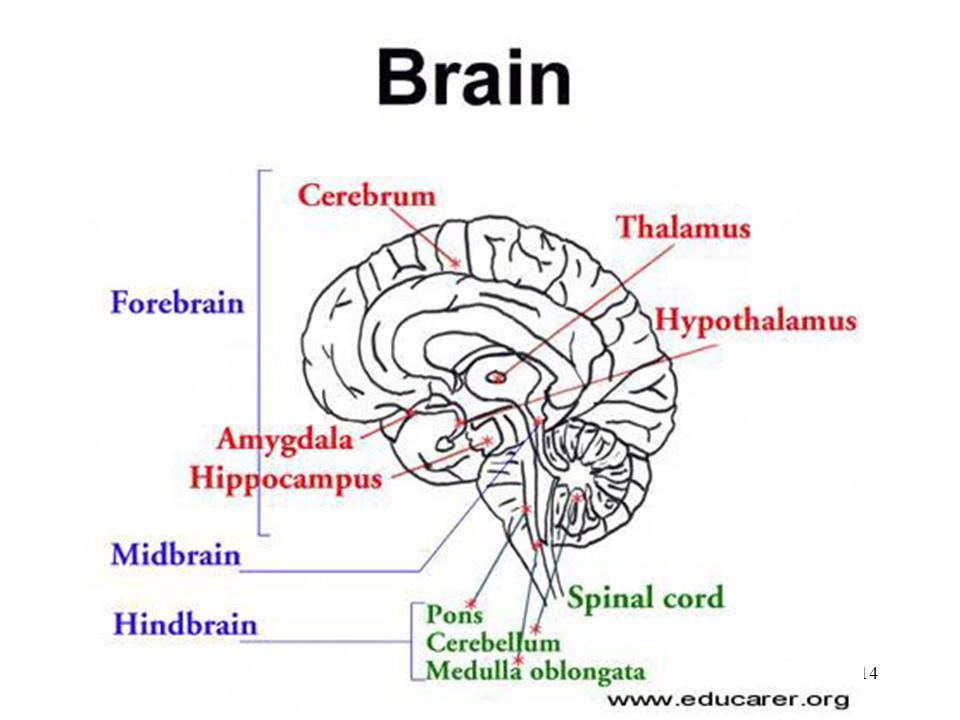
Advice for Parents, Services and Policy
We need to remember that children's brains are constantly evolving. Whether we measure gray matter consistency, white matter volume, synaptic density, or any other anatomical feature of the brain, we will see continuous changes occurring until adulthood. It is clear that these changes will have an impact on the child's cognitive functioning, and the same will be especially true for executive functioning, given the complexity of the processes involved. Given the importance of executive functioning for academic achievement and social well-being, identifying problems in cognitive and behavioral self-regulation at an early stage is clearly important. At the same time, all young children will have trouble planning ahead, overcoming temptations, regulating emotions, and focusing on a task: that's how the brain works at this age.
Literature
- Best JR, Miller PH, Jones LL. Executive functions after age 5: Changes and correlates .
 Dev Rev . 2009;29(3):180-200.
Dev Rev . 2009;29(3):180-200. - Luna B, Garver KR, Urban TA, Lazar, NA, Sweeney JA.Maturation of cognitive processes from late childhood to adulthood. Child Dev . 2004;75(5):1357-1372.
- Shaw P, Kabani, NJ, Lerch JP, et al. Neurodevelopmental trajectories of the human cerebral cortex. J Neurosci . 2008;28(14):3586-3594.
- Huttenlocher PR, de Courten C, Garey LJ, Van der Loos H. Synaptogenesis in human visual cortex – evidence for synapse elimination during normal development. Neurosci Lett . 1982;33(3):247-252.
- Giedd JN, Blumenthal J, Jeffries NO, et al. Brain development during childhood and adolescence: A longitudinal MRI study. Nat Neurosci . 1999;2(10):861-863.
- Sowell ER, Peterson BS, Thompson PM, Welcome SE, Henkenius AL, Toga AW. Mapping cortical change across the human life span. Nat Neurosci . 2003;6(3):309-315.
- Gogtay N, Giedd JN, Lusk L, et al.
 Dynamic mapping of human cortical development during childhood through early adulthood. P Natl Acad Sci USA . 2004;101(21):8174-8179.
Dynamic mapping of human cortical development during childhood through early adulthood. P Natl Acad Sci USA . 2004;101(21):8174-8179. - Huttenlocher PR. Dendritic and synaptic development in human cerebral cortex: Time course and critical periods. Dev Neuropsychol . 1999;16(3):347-349.
- Lie C, Specht K, Marshall JC, Fink GR. Using fMRI to decompose the neural processes underlying the Wisconsin Card Sorting Test. Neuroimage . 2006;30(3):1038-1049.
- Aarts E, Roelofs A, van Turennout M. Attentional control of task and response in lateral and medial frontal cortex: Brain activity and reaction time distributions. Neuropsychologia . 2009;47(10):2089-2099.
- Perrett E. The left frontal lobe of man and the suppression of habitual responses in verbal categorical behavior. Neuropsychologia . 1974;12(3):323-330.
- Aron AR, Fletcher PC, Bullmore ET, Sahakian BJ, Robbins TW. Stop-signal inhibition disrupted by damage to right inferior frontal gyrus in humans.
 Nat Neurosci . 2003;6(2):115-116.
Nat Neurosci . 2003;6(2):115-116. - Milner B. Effects of different brain lesions on card sorting: The role of the frontal lobes. Arch Neurol . 1963;9(1):90-100.
- Huttenlocher PR. Synaptic density in human frontal cortex – developmental changes and effects of aging. Brain Res . 1979;163(2):195-205.
- Sowell ER, Thompson PM, Tessner KD, Toga AW. Mapping continued brain growth and gray matter density reduction in dorsal frontal cortex: Inverse relationships during postadolescent brain maturation. J Neurosci . 2001;21(22):8819-8829.
- Bunge SA, Zelazo PD. A brain-based account of the development of rule use in childhood. Curr Dir Psychol Sci . 2006;15(3):118-121.
- Dempster FN. The rise and fall of the inhibitory mechanism: Toward a unified theory of cognitive development and aging. Dev Rev . 1992;12(2):45-75.
- Diamond A. Normal development of prefrontal cortex from birth to young adulthood: Cognitive functions, anatomy, and biochemistry.
 In: Stuss DT, Knight RT, eds. Principles of Frontal Lobe Function . Oxford: Oxford University Press; 1992:466-503.
In: Stuss DT, Knight RT, eds. Principles of Frontal Lobe Function . Oxford: Oxford University Press; 1992:466-503. - Smyser CD, Inder TE, Shimony JS, et al. Longitudinal analysis of neural network development in preterm infants. Cereb Cortex . 2010;20(12):2852-2862.
- Davidson MC, Thomas KM, Casey BJ. Imaging the developing brain with fMRI. Ment Retard Dev D R . 2003;9(3):161-167.
- Kelly AMC, Di Martino A, Uddin LQ, et al. Development of anterior cingulate functional connectivity from late childhood to early adulthood. Cereb Cortex . 2009;19(3):640-657.
- Adleman NE, Menon V, Blasey CM, et al. A developmental fMRI study of the Stroop color-word task. Neuroimage . 2002;16(1):61-75.
- Luna B, Thulborn KR, Munoz DP, et al. Maturation of widely distributed brain function subserves cognitive development. Neuroimage . 2001;13(5):786-793.
- Morton JB, Bosma R, Ansari D.
 Age-related changes in brain activation associated with dimensional shifts of attention: An fMRI study. Neuroimage , 2009;46(1):249-256.
Age-related changes in brain activation associated with dimensional shifts of attention: An fMRI study. Neuroimage , 2009;46(1):249-256. - Bunge SA, Dudukovic NM, Thomason ME, Vaidya CJ, Gabrieli JDE. Immature frontal lobe contributions to cognitive control in children: Evidence from fMRI. Neuron . 2002;33(2):301-311.
- Casey BJ, Trainor RJ, Orendi JL, et al. A developmental functional MRI study of prefrontal activation during performance of a go-no-go task. J Cognitive Neurosci . 1997;9(6):835-847.
- Braver TS, Cohen JD, Nystrom LE, Jonides J, Smith EE, Noll DC. A parametric study of prefrontal cortex involvement in human working memory. Neuroimage . 1997;5(1):49-62.
- Cole MW, Schneider W. The cognitive control network: Integrated cortical regions with dissociable functions. Neuroimage . 2007;37(1):343-360.
- Bunge SA, Wright SB. Neurodevelopmental changes in working memory and cognitive control.
 Curr Opin Neurobiol . 2007;17(2):243-250.
Curr Opin Neurobiol . 2007;17(2):243-250. - Kwon H, Reiss AL, Menon V. Neural basis of protracted developmental changes in visuo-spatial working memory. P Natl Acad Sci USA . 2002;99(20):13336-13341.
- Biswal B, Yetkin FZ, Haughton VM, Hyde JS. Functional connectivity in the motor cortex of resting human brain using echo-planar MRI. Magn Reson Med . 1995;34(4):537-541.
- Vogel AC, Power JD, Petersen SE, Schlagger BL. Development of the brain's functional network architecture. Neuropsychol Rev . 2010;20(4):362-375.
- Fair DA, Dosenbach NUF, Church JA, et al. Development of distinct control networks through segregation and integration. P Natl Acad Sci USA . 2007;104(33):13507-13512.
- Power JD, Barnes KA, Snyder AZ, Schlaggar BL, Petersen SE. Spurious but systematic correlations in functional connectivity MRI networks arise from subject motion. NeuroImage . 2012;59(3):2142-2154.
For citation:
Knapp K, Bruce MJ. Brain development and executive functioning. In: Tremblay RE, Buavan M, Peters RDeV, eds. Morton DB, eds. Topics. Encyclopedia of Early Childhood Development [online]. https://www.encyclopedia-deti.com/upravlyayushchie-funkcii/ot-ekspertov/razvitie-mozga-i-upravlyayushchee-funkcionirovanie. Published: January 2013 (English). Viewed on November 6, 2022
Text copied to clipboard ✓
Stroke: symptoms, first aid, prevention.
The human brain depends on a constant and sufficient supply of oxygenated blood. When blood circulation is disturbed, severe disorders of the brain activity occur.
Stroke is a violation of blood circulation in the brain, caused by blockage or rupture of blood vessels. This is a condition where a blood clot - a blood clot - or blood from a ruptured vessel disrupts blood flow in the brain.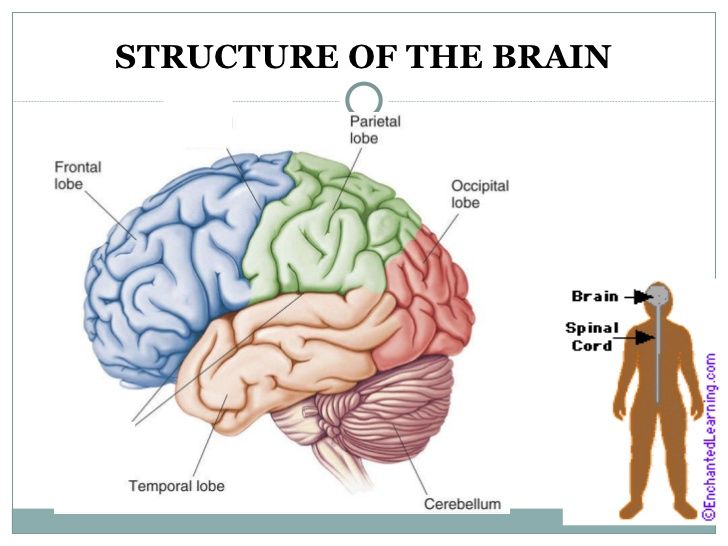 The lack of oxygen and glucose leads to the death of brain cells and impaired motor functions, speech or memory.
The lack of oxygen and glucose leads to the death of brain cells and impaired motor functions, speech or memory.
According to WHO, stroke causes 6.7 million deaths per year worldwide, second only to coronary heart disease. In most countries of the world, doctors consider stroke to be the most common cause of neurological disorders, leading to varying degrees of disability, and hence disability. In Russia, no more than 20% of patients return to work after a stroke, and one-third of stroke patients are people of working age. Recently, stroke in Russia is no longer a diagnosis of only the elderly, doctors are increasingly fixing this disease not only in 25-30-year-old Russians, but also in children.
A stroke can affect anyone. Stroke prevention is about reducing risk factors. The disease is easier to prevent. Simple measures to help avoid a stroke will extend your life by 15-20 years. Some risk factors, such as the development of an aneurysm or the development of a blood clot as a result of an injury, are difficult to control. However, a significant number of factors are mainly due to lifestyle.
However, a significant number of factors are mainly due to lifestyle.
These factors include:
- high blood pressure;
- high cholesterol;
- diabetes mellitus;
- obesity and overweight;
- cardiovascular diseases;
- smoking;
- drug use;
- drinking alcohol.
In addition, stroke is more likely to develop in people over 55 years of age and those whose close relatives have already suffered a stroke. Between the ages of 45 and 55, stroke is twice as common in men as in women,
Three-quarters of all cases are ischemic stroke. This term refers to a condition in which a blood clot clogs a vessel and blocks blood flow to a specific part of the brain. Usually, a blood clot forms somewhere in the peripheral vessels of the body, breaks off and reaches the brain through the bloodstream. There, it gets stuck in the small vessels of the brain and blocks the blood flow in them.
The second type of stroke - hemorrhagic - is much less common. It occurs when a blood vessel ruptures in the brain. If the vessel is on the surface of the brain, the leaked blood fills the space between the brain and the skull. This is called subarachnoid bleeding. And if the vessel bursts in the deeper structures of the brain, the blood from it fills the surrounding tissues.
It occurs when a blood vessel ruptures in the brain. If the vessel is on the surface of the brain, the leaked blood fills the space between the brain and the skull. This is called subarachnoid bleeding. And if the vessel bursts in the deeper structures of the brain, the blood from it fills the surrounding tissues.
Damage to a small area of the brain leads to minor disorders - weakness of the limbs. Violation of blood circulation in large areas of the brain causes paralysis and even death: the degree of damage depends not only on the extent, but also on the location of the stroke.
Many people who have had a stroke remain partially or completely paralyzed on one side of the body, have problems with speech and control of urination and defecation. Intellectual abilities also suffer - memory, cognitive functions.
The onset of a stroke is usually asymptomatic. But after a few minutes, the brain cells, deprived of nutrition, begin to die, and the effects of a stroke become noticeable.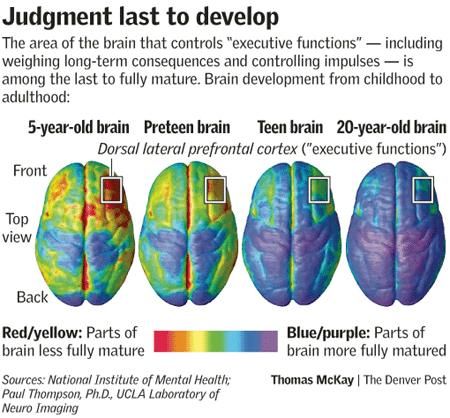
Common symptoms of a stroke:
- sudden weakness in the face, arm or leg, usually on one side of the body;
- sudden clouding of consciousness, problems with speech or with understanding speech;
- sudden vision problems in one or both eyes;
- sudden disturbance of gait, dizziness, loss of balance or coordination;
- sudden severe headache of unknown cause.
It is very important to immediately recognize its symptoms in order to call an ambulance as soon as possible. After all, the sooner treatment is started, the better a person recovers from a stroke. Untimely seeking help leads to severe complications and disability.
Stroke first aid is not just important, it is vital. And if suddenly you are near a person who has shown clear signs of a stroke, you should immediately take several actions. The life of this person depends on them.
- As soon as you realize that a person has all the signs of a stroke, call an ambulance immediately.
 This must be done immediately so as not to miss time. Violation of cerebral circulation is most effectively treated in the first 3 hours. So don't waste your time.
This must be done immediately so as not to miss time. Violation of cerebral circulation is most effectively treated in the first 3 hours. So don't waste your time. - Remove extra people from the room if it is indoors. If outside, ask everyone to step aside and not interfere with the flow of fresh air. Only those who can help should stay nearby.
- Do not stir the person under any circumstances. This is dangerous. The patient must be left where the attack occurred. Do not transfer to bed.
- Elevate the patient's upper body and head (approximately 30 degrees). It is best to put a few pillows. Unfasten or remove all clothing that is constricting and interferes with breathing (belt, collar, belt, etc.).
- Supply fresh air.
- If vomiting occurs, turn victim's head to one side and thoroughly clean out vomit, otherwise person may suffocate.
- It sometimes happens that a stroke is accompanied by epileptic seizures. Moreover, they can follow one after another.
 In this case, turn the person to one side, insert a spoon wrapped in a handkerchief, a comb, a stick into the mouth and, lightly holding the patient’s head with your hands, wipe the foam. The most important thing in this case is not to crush the person. You just need to hold it a little and that's it. And even more so, you can not bring ammonia. The consequences can be terrible - cessation of breathing and death.
In this case, turn the person to one side, insert a spoon wrapped in a handkerchief, a comb, a stick into the mouth and, lightly holding the patient’s head with your hands, wipe the foam. The most important thing in this case is not to crush the person. You just need to hold it a little and that's it. And even more so, you can not bring ammonia. The consequences can be terrible - cessation of breathing and death. - It may happen that the victim's heart stops and breathing stops. In this case, you will have to immediately start an indirect heart massage and a session of artificial respiration.
Stroke prevention is based on the basic principles of a healthy lifestyle.
- Know and control your blood pressure - it should not be more than 140/90 mmHg.
- Do not start smoking or stop smoking as early as possible.
- Add as little salt as possible to your food and avoid canned and processed foods that contain it in excess.
- Control the level of cholesterol in the blood - the maximum allowable level is 5 mmol / l.