Down syndrome chances in pregnancy
Facts about Down Syndrome | CDC
Down syndrome is a condition in which a person has an extra chromosome.
What is Down Syndrome?
Down syndrome is a condition in which a person has an extra chromosome. Chromosomes are small “packages” of genes in the body. They determine how a baby’s body forms and functions as it grows during pregnancy and after birth. Typically, a baby is born with 46 chromosomes. Babies with Down syndrome have an extra copy of one of these chromosomes, chromosome 21. A medical term for having an extra copy of a chromosome is ‘trisomy.’ Down syndrome is also referred to as Trisomy 21. This extra copy changes how the baby’s body and brain develop, which can cause both mental and physical challenges for the baby.
Even though people with Down syndrome might act and look similar, each person has different abilities. People with Down syndrome usually have an IQ (a measure of intelligence) in the mildly-to-moderately low range and are slower to speak than other children.
Some common physical features of Down syndrome include:
- A flattened face, especially the bridge of the nose
- Almond-shaped eyes that slant up
- A short neck
- Small ears
- A tongue that tends to stick out of the mouth
- Tiny white spots on the iris (colored part) of the eye
- Small hands and feet
- A single line across the palm of the hand (palmar crease)
- Small pinky fingers that sometimes curve toward the thumb
- Poor muscle tone or loose joints
- Shorter in height as children and adults
How Many Babies are Born with Down Syndrome?
Down syndrome remains the most common chromosomal condition diagnosed in the United States. Each year, about 6,000 babies born in the United States have Down syndrome. This means that Down syndrome occurs in about 1 in every 700 babies.1
Types of Down Syndrome
There are three types of Down syndrome. People often can’t tell the difference between each type without looking at the chromosomes because the physical features and behaviors are similar.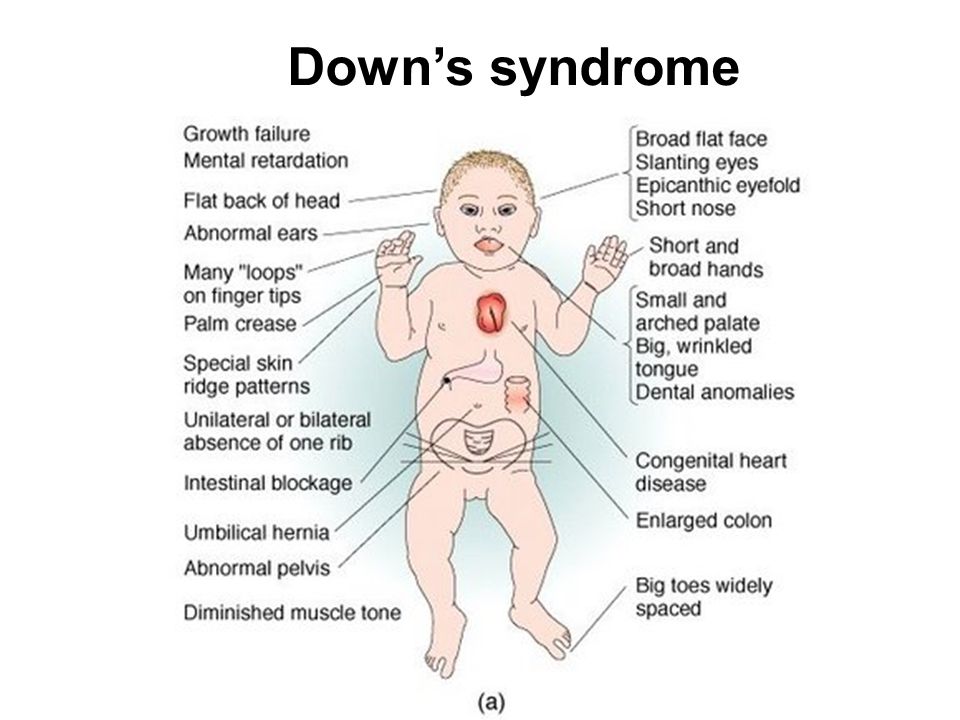
- Trisomy 21: About 95% of people with Down syndrome have Trisomy 21.2 With this type of Down syndrome, each cell in the body has 3 separate copies of chromosome 21 instead of the usual 2 copies.
- Translocation Down syndrome: This type accounts for a small percentage of people with Down syndrome (about 3%).2 This occurs when an extra part or a whole extra chromosome 21 is present, but it is attached or “trans-located” to a different chromosome rather than being a separate chromosome 21.
- Mosaic Down syndrome: This type affects about 2% of the people with Down syndrome.2 Mosaic means mixture or combination. For children with mosaic Down syndrome, some of their cells have 3 copies of chromosome 21, but other cells have the typical two copies of chromosome 21. Children with mosaic Down syndrome may have the same features as other children with Down syndrome. However, they may have fewer features of the condition due to the presence of some (or many) cells with a typical number of chromosomes.

Causes and Risk Factors
- The extra chromosome 21 leads to the physical features and developmental challenges that can occur among people with Down syndrome. Researchers know that Down syndrome is caused by an extra chromosome, but no one knows for sure why Down syndrome occurs or how many different factors play a role.
- One factor that increases the risk for having a baby with Down syndrome is the mother’s age. Women who are 35 years or older when they become pregnant are more likely to have a pregnancy affected by Down syndrome than women who become pregnant at a younger age.3-5However, the majority of babies with Down syndrome are born to mothers less than 35 years old, because there are many more births among younger women.6,7
Diagnosis
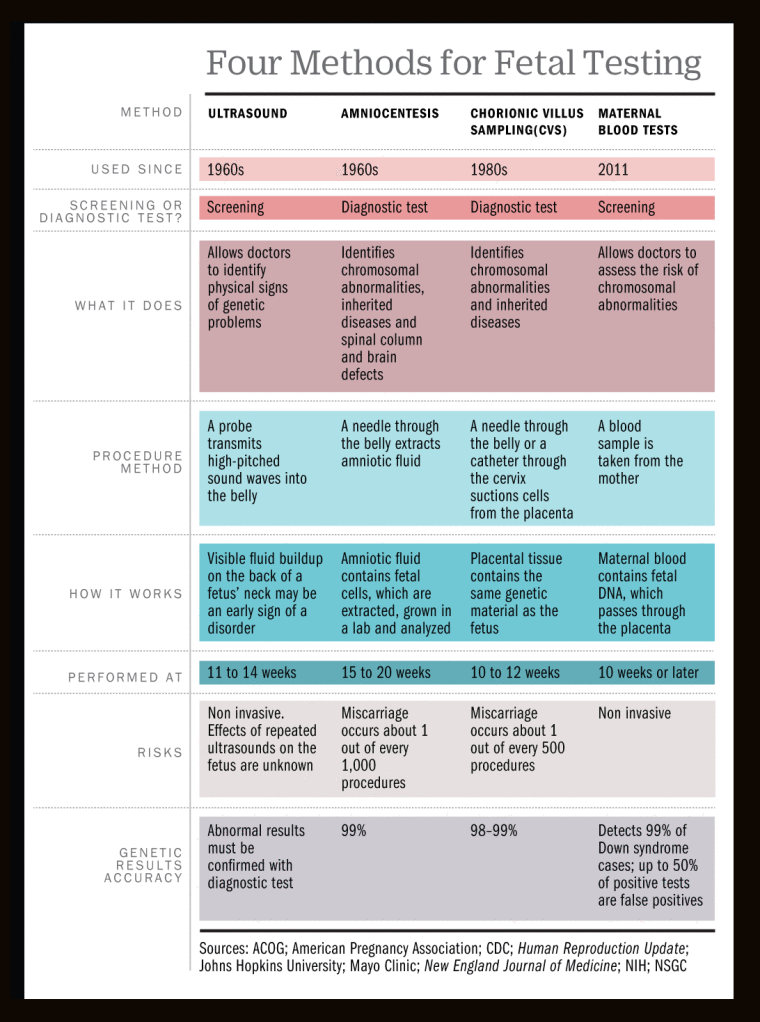
There are two basic types of tests available to detect Down syndrome during pregnancy: screening tests and diagnostic tests. A screening test can tell a woman and her healthcare provider whether her pregnancy has a lower or higher chance of having Down syndrome.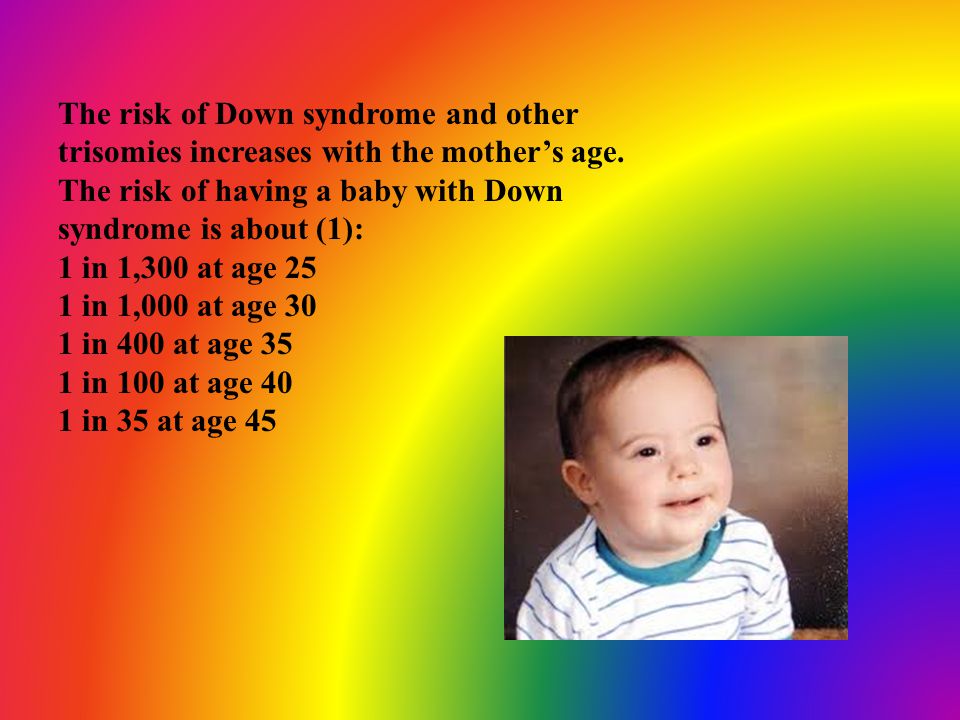 Screening tests do not provide an absolute diagnosis, but they are safer for the mother and the developing baby. Diagnostic tests can typically detect whether or not a baby will have Down syndrome, but they can be more risky for the mother and developing baby. Neither screening nor diagnostic tests can predict the full impact of Down syndrome on a baby; no one can predict this.
Screening tests do not provide an absolute diagnosis, but they are safer for the mother and the developing baby. Diagnostic tests can typically detect whether or not a baby will have Down syndrome, but they can be more risky for the mother and developing baby. Neither screening nor diagnostic tests can predict the full impact of Down syndrome on a baby; no one can predict this.
Screening Tests
Screening tests often include a combination of a blood test, which measures the amount of various substances in the mother’s blood (e.g., MS-AFP, Triple Screen, Quad-screen), and an ultrasound, which creates a picture of the baby. During an ultrasound, one of the things the technician looks at is the fluid behind the baby’s neck. Extra fluid in this region could indicate a genetic problem. These screening tests can help determine the baby’s risk of Down syndrome. Rarely, screening tests can give an abnormal result even when there is nothing wrong with the baby. Sometimes, the test results are normal and yet they miss a problem that does exist.
Diagnostic Tests
Diagnostic tests are usually performed after a positive screening test in order to confirm a Down syndrome diagnosis. Types of diagnostic tests include:
- Chorionic villus sampling (CVS)—examines material from the placenta
- Amniocentesis—examines the amniotic fluid (the fluid from the sac surrounding the baby)
- Percutaneous umbilical blood sampling (PUBS)—examines blood from the umbilical cord
These tests look for changes in the chromosomes that would indicate a Down syndrome diagnosis.
Other Health Problems
Many people with Down syndrome have the common facial features and no other major birth defects. However, some people with Down syndrome might have one or more major birth defects or other medical problems. Some of the more common health problems among children with Down syndrome are listed below.8
- Hearing loss
- Obstructive sleep apnea, which is a condition where the person’s breathing temporarily stops while asleep
- Ear infections
- Eye diseases
- Heart defects present at birth
Health care providers routinely monitor children with Down syndrome for these conditions.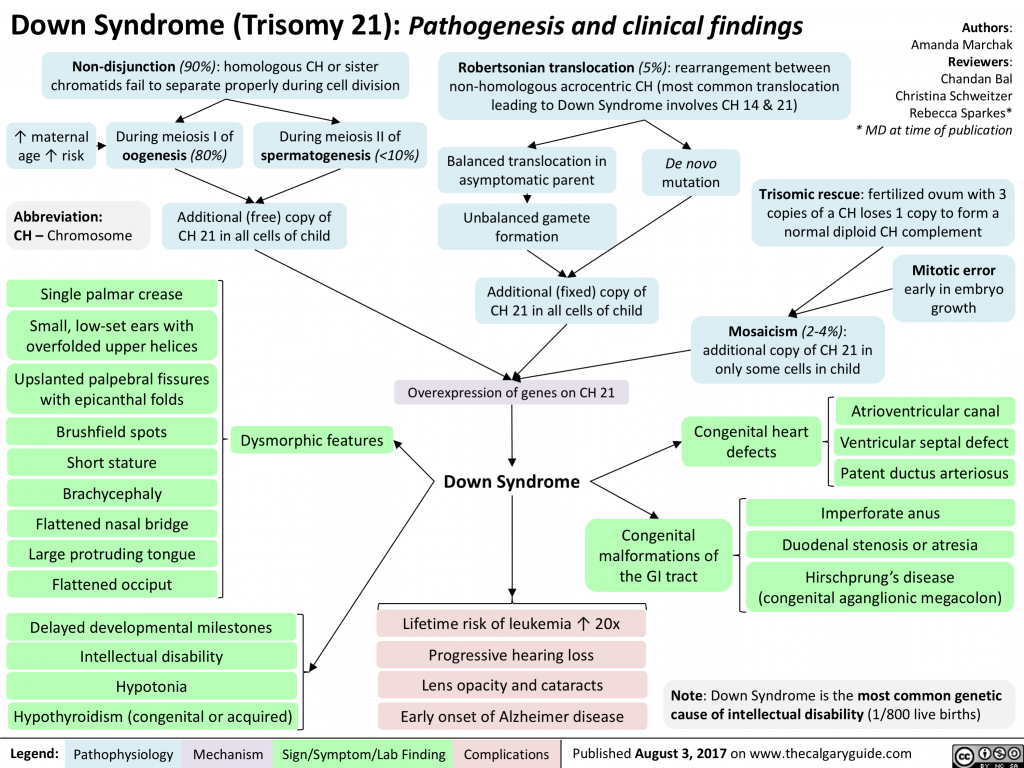
Treatments
Down syndrome is a lifelong condition. Services early in life will often help babies and children with Down syndrome to improve their physical and intellectual abilities. Most of these services focus on helping children with Down syndrome develop to their full potential. These services include speech, occupational, and physical therapy, and they are typically offered through early intervention programs in each state. Children with Down syndrome may also need extra help or attention in school, although many children are included in regular classes.
Other Resources
The views of these organizations are their own and do not reflect the official position of CDC.
- Down Syndrome Research Foundation (DSRF)external icon
DSRF initiates research studies to better understand the learning styles of those with Down syndrome. - Global Down Syndrome Foundationexternal icon
This foundation is dedicated to significantly improving the lives of people with Down syndrome through research, medical care, education and advocacy.
- National Association for Down Syndromeexternal icon
The National Association for Down Syndrome supports all persons with Down syndrome in achieving their full potential. They seek to help families, educate the public, address social issues and challenges, and facilitate active participation. - National Down Syndrome Society (NDSS)external icon
NDSS seeks to increase awareness and acceptance of those with Down syndrome.
References
- Mai CT, Isenburg JL, Canfield MA, Meyer RE, Correa A, Alverson CJ, Lupo PJ, Riehle‐Colarusso T, Cho SJ, Aggarwal D, Kirby RS. National population‐based estimates for major birth defects, 2010–2014. Birth Defects Research. 2019; 111(18): 1420-1435.
- Shin M, Siffel C, Correa A. Survival of children with mosaic Down syndrome. Am J Med Genet A. 2010;152A:800-1.
- Allen EG, Freeman SB, Druschel C, et al. Maternal age and risk for trisomy 21 assessed by the origin of chromosome nondisjunction: a report from the Atlanta and National Down Syndrome Projects.
 Hum Genet. 2009 Feb;125(1):41-52.
Hum Genet. 2009 Feb;125(1):41-52. - Ghosh S, Feingold E, Dey SK. Etiology of Down syndrome: Evidence for consistent association among altered meiotic recombination, nondisjunction, and maternal age across populations. Am J Med Genet A. 2009 Jul;149A(7):1415-20.
- Sherman SL, Allen EG, Bean LH, Freeman SB. Epidemiology of Down syndrome. Ment Retard Dev Disabil Res Rev. 2007;13(3):221-7.
- Adams MM, Erickson JD, Layde PM, Oakley GP. Down’s syndrome. Recent trends in the United States. JAMA. 1981 Aug 14;246(7):758-60.
- Olsen CL, Cross PK, Gensburg LJ, Hughes JP. The effects of prenatal diagnosis, population ageing, and changing fertility rates on the live birth prevalence of Down syndrome in New York State, 1983-1992. Prenat Diagn. 1996 Nov;16(11):991-1002.
- Bull MJ, the Committee on Genetics. Health supervision for children with Down syndrome. Pediatrics. 2011;128:393-406.
Prenatal Testing for Down Syndrome | Patient Education
Down syndrome is a genetic condition caused by extra genes from the 21st chromosome. It results in certain characteristics, including some degree of cognitive disability and other developmental delays. Common physical traits include an upward slant of the eyes; flattened bridge of the nose; single, deep crease on the palm of the hand; and decreased muscle tone. A child with Down syndrome, however, may not have all these traits.
It results in certain characteristics, including some degree of cognitive disability and other developmental delays. Common physical traits include an upward slant of the eyes; flattened bridge of the nose; single, deep crease on the palm of the hand; and decreased muscle tone. A child with Down syndrome, however, may not have all these traits.
The incidence of Down syndrome in the United States is about 1 in 1,000 births. There is no association between Down syndrome and culture, ethnic group, socioeconomic status or geographic region.
Age-Related Risks
Generally, the chance of having a Down syndrome birth is related to the mother's age. Under age 25, the odds of having a child with Down syndrome are about 1 in 1,400. At age 35, the odds are about 1 in 350. At age 40, the odds are about 1 in 100.
Causes of Down Syndrome
There are three causes of Down syndrome:
Trisomy 21
An estimated 95 percent of people with Down syndrome have trisomy 21, meaning they have three number 21 chromosomes instead of two. We normally have 23 pairs of chromosomes, each made up of genes. During the formation of the egg and the sperm, a woman's or a man's pair of chromosomes normally split so that only one chromosome is in each egg or sperm. In trisomy 21, the 21st chromosome pair does not split and a double dose goes to the egg or sperm. An estimated 95 to 97 percent of the extra chromosome is of maternal origin.
We normally have 23 pairs of chromosomes, each made up of genes. During the formation of the egg and the sperm, a woman's or a man's pair of chromosomes normally split so that only one chromosome is in each egg or sperm. In trisomy 21, the 21st chromosome pair does not split and a double dose goes to the egg or sperm. An estimated 95 to 97 percent of the extra chromosome is of maternal origin.
Translocation
Translocation occurs in about 3 to 4 percent of people with Down syndrome. In this type, an extra part of the 21st chromosome gets stuck onto another chromosome. In about half of these situations, one parent carries the extra 21st chromosome material in a "balanced" or hidden form.
Mosaicism
In mosaicism, the person with Down syndrome has an extra 21st chromosome in some of the cells but not all of them. The other cells have the usual pair of 21st chromosomes. About 1 to 2 percent of people with Down syndrome have this type.
Prenatal Testing
Screening tests can identify women at increased risk of having a baby with Down syndrome. These tests have no risks of miscarriage, but can't determine with certainty whether a fetus is affected. Diagnostic tests, on the other hand, are extremely accurate at identifying certain abnormalities in the fetus, but carry a small — generally less than 1 percent — risk of miscarriage. We offer options for both screening and diagnostic testing.
These tests have no risks of miscarriage, but can't determine with certainty whether a fetus is affected. Diagnostic tests, on the other hand, are extremely accurate at identifying certain abnormalities in the fetus, but carry a small — generally less than 1 percent — risk of miscarriage. We offer options for both screening and diagnostic testing.
Continue reading
Screening Tests
Sequential Integrated Screening — Sequential integrated screening is offered to all pregnant women by the state of California. This non-invasive screening is performed in two steps.
In the first step, which is performed between 10 and 14 weeks of pregnancy, a blood sample is taken from the mother and a nuchal translucency ultrasound is performed to measure the amount of fluid at the back of the baby's neck. If the blood test is scheduled prior to the ultrasound, we can provide the results at the end of the ultrasound appointment. The results of the blood test, the nuchal translucency measurement and the mother's age are used to estimate the risk for Down syndrome and trisomy 18.
The second step is a maternal blood test between 15 to 20 weeks of pregnancy. When the results of this blood test are combined with the results from the first trimester blood test and nuchal translucency ultrasound, the detection rate for Down syndrome increases. This test also provides a personal risk assessment for having a fetus with trisomy 18, Smith-Lemli-Opitz syndrome, an open neural tube defect or an abdominal wall defect.
Diagnostic Tests
Amniocentesis, chorionic villus sampling (CVS) and ultrasound are the three primary procedures for diagnostic testing.
Amniocentesis — Amniocentesis is used most commonly to identify chromosomal problems such as Down syndrome. When the fetus is known to be at risk, it can detect other genetic diseases like cystic fibrosis, Tay-Sachs disease and sickle cell disease.
An amniocentesis procedure for genetic testing is typically performed between 15 and 20 weeks of pregnancy. Under ultrasound guidance, a needle is inserted through the abdomen to remove a small amount of amniotic fluid.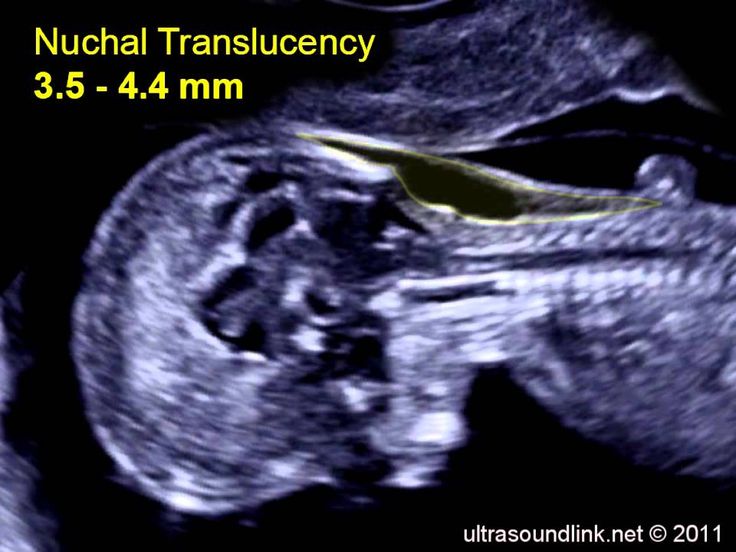 The cells from the fluid are then cultured and a karyotype analysis — an analysis of the chromosomal make-up of the cells — is performed. It takes about two weeks to receive the results of the test.
The cells from the fluid are then cultured and a karyotype analysis — an analysis of the chromosomal make-up of the cells — is performed. It takes about two weeks to receive the results of the test.
Amniocentesis detects most chromosomal disorders, such as Down syndrome, with a high degree of accuracy. Testing for other genetic diseases, such as Tay-Sachs disease, is not routinely performed but can be detected through specialized testing if your fetus is known to be at risk. Testing for neural tube defects, such as spina bifida, also can be performed.
There is a small risk of miscarriage as a result of amniocentesis — about 1 in 100 or less. Miscarriage rates for procedures performed at UCSF Medical Center are less than 1 in 350.
Chorionic Villus Sampling (CVS) — Like amniocentesis, chorionic villus sampling is used most commonly to identify chromosomal problems such as Down syndrome. It can detect other genetic diseases like cystic fibrosis, Tay-Sachs disease and sickle cell disease in at-risk fetuses.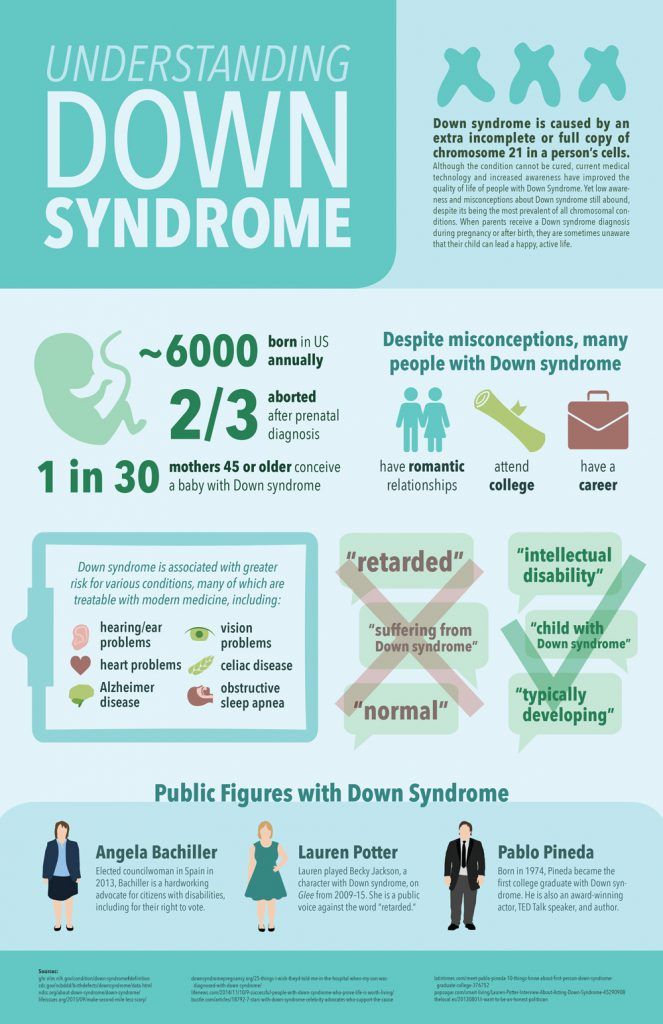 The main advantage of CVS over amniocentesis is that it is done much earlier in pregnancy, at 10 to 12 weeks rather than 15 to 20 weeks.
The main advantage of CVS over amniocentesis is that it is done much earlier in pregnancy, at 10 to 12 weeks rather than 15 to 20 weeks.
CVS involves removing a tiny piece of tissue from the placenta. Under ultrasound guidance, the tissue is obtained either with a needle inserted through the abdomen or a catheter inserted through the cervix. The tissue is then cultured and a karyotype analysis of the chromosomal make-up of the cells is performed. It takes about two weeks to receive the results.
The advantage of CVS over amniocentesis is that the test is performed much earlier in pregnancy, so results are typically available by the end of the third month. A disadvantage is that spinal cord defects cannot be detected. Expanded alpha fetoprotein (AFP) blood testing or ultrasound can be performed later in the pregnancy to screen for spinal cord defects.
There is a small risk of miscarriage as a result of CVS — 1 in 100 or less. Miscarriage rates for procedures performed at UCSF Medical Center are less than 1 in 350.
Ultrasound — The primary purpose of ultrasound is to determine the status of a pregnancy — the due date, size of the fetus and if the mother is carrying multiples. Ultrasound also can provide some information about possible birth defects in a fetus. All patients at UCSF Medical Center undergo a comprehensive ultrasound examination before any invasive tests are performed. Results of the ultrasound are explained at the time of the visit.
In some patients, an ultrasound raises concern of a possible abnormality in the fetus. We have extensive experience in performing and interpreting ultrasounds in pregnancy.
If You Receive a Positive Result
If you receive positive results on a screening test, we recommend that you discuss this with your doctor and a genetic counselor. Options for further diagnostic testing will be explained. The decision as to whether to have invasive genetic testing is up to you.
If a diagnostic test finds a genetic abnormality, the significance of such results should be discussed with experts familiar with the condition, including a medical geneticist and a genetic counselor, as well as your own doctor.
Screening for Down syndrome during pregnancy in Moscow, prices
Down syndrome - human trisomy on the 21st chromosome - the most common of this group of diseases, occurs in about 1 in 700-800 newborns. The probability of having a child with Down syndrome increases with the age of the expectant mother. However, taking into account the birth rate in different age groups, 80% of children with Down syndrome are born to mothers under the age of 30 years.
After the birth of one child with Down syndrome, the mother's risk of relapse for each subsequent child is approximately 1% higher than her age risk. This fact is especially important for young mothers, whose age-related risks are small.
Prenatal screening, recommended for all pregnant women, regardless of risk group, to detect chromosomal pathology, includes the study of serum markers (alpha-fetoprotein, free estriol, human chorionic gonadotropin) and ultrasound, performed routinely in the first trimester of pregnancy. The most characteristic ultrasound findings in Down's syndrome include heart defects, shortened long bones, underdeveloped fetal nasal bone, malformations of the small intestine, etc. If the results show an increased risk of the presence of chromosomal abnormalities, a diagnostic invasive intervention is performed to take fetal biomaterial for confirmatory research. Depending on the duration of pregnancy, this can be a chorionic villus biopsy (10-12 weeks) or amniocentesis (from the 15th week). According to the results of genetic diagnosis of the obtained fetal material, a prenatal diagnosis is made, and when the syndrome is confirmed in the fetus, the issue of maintaining pregnancy is decided.
The most characteristic ultrasound findings in Down's syndrome include heart defects, shortened long bones, underdeveloped fetal nasal bone, malformations of the small intestine, etc. If the results show an increased risk of the presence of chromosomal abnormalities, a diagnostic invasive intervention is performed to take fetal biomaterial for confirmatory research. Depending on the duration of pregnancy, this can be a chorionic villus biopsy (10-12 weeks) or amniocentesis (from the 15th week). According to the results of genetic diagnosis of the obtained fetal material, a prenatal diagnosis is made, and when the syndrome is confirmed in the fetus, the issue of maintaining pregnancy is decided.
Most patients with Down syndrome, unless diagnosed prenatally, are usually recognized at birth due to typical phenotypic features, but in some cases prematurity or ethnic differences may make clinical diagnosis less straightforward. In addition to the characteristic external features, malformations of many organs and systems are described in Down syndrome. The most common of these are congenital heart defects (observed in approximately 50% of cases), often requiring surgical intervention. Malformations of the gastrointestinal tract are also noted, especially duodenal atresia (2-5% of cases), Hirschsprung's disease, esophageal atresia and other serious disorders.
The most common of these are congenital heart defects (observed in approximately 50% of cases), often requiring surgical intervention. Malformations of the gastrointestinal tract are also noted, especially duodenal atresia (2-5% of cases), Hirschsprung's disease, esophageal atresia and other serious disorders.
Ophthalmic diseases - strabismus, cataracts, myopia and glaucoma - are more common in children with Down syndrome. There may also be hearing loss of heterogeneous origin, spinal cord compression, myopathic symptoms associated with spinal cord compression (weakness, abnormal reflexes, urinary incontinence, etc.).
For all the problems associated with their mental development, Down syndrome patients show a wide range of developmental abilities, with high variability in personality and behavioral phenotypes. The most common causes of death in patients with Down syndrome are associated with congenital heart defects, infections (such as pneumonia), and malignant neoplasms of the blood system. Surgical correction of associated congenital malformations is usually successful, and long-term survival is good. However, less than half of patients survive to age 60, and less than 15% survive past age 68. Neurodegenerative diseases with features of Alzheimer's disease occur in most patients over 40 years of age.
Surgical correction of associated congenital malformations is usually successful, and long-term survival is good. However, less than half of patients survive to age 60, and less than 15% survive past age 68. Neurodegenerative diseases with features of Alzheimer's disease occur in most patients over 40 years of age.
The development of laboratory and ultrasound diagnostics has made it possible to develop and introduce into the practice of practical healthcare, including in our country, a number of comprehensive measures that solve many problems of monitoring the condition of the fetus and the course of pregnancy, including prenatal detection of Down syndrome in the fetus in the early stages pregnancy. These tasks can be solved by traditional screening of the first trimester, which combines the study of serum hormonal markers and ultrasound.
Non-invasive prenatal testing (NIPT) complements the data of traditional screening, because due to its higher sensitivity and specificity, it allows you to refine the results.
The use of Prenetix NIPT as an expert-level screening reduces the number of invasive interventions that verify chromosomal diseases, and thereby avoids potential complications of invasion and reduces the risk of miscarriage as a result of diagnostic measures.
Screening tests for Down syndrome in the first 24 weeks of pregnancy
Relevance
Down's syndrome (also known as Down's disease or Trisomy 21) is an incurable genetic disorder that causes significant physical and mental health problems and disability. However, Down syndrome affects people in completely different ways. Some have significant symptoms, while others have minor health problems and are able to lead relatively normal lives. There is no way to predict how badly a child might be affected.
Parents-to-be during pregnancy are given the opportunity to have a screening test for Down's Syndrome in their baby to help them make a decision. If a mother is carrying a child with Down syndrome, then a decision should be made whether to terminate the pregnancy or keep it. The information gives parents the opportunity to plan life with a child with Down syndrome.
The information gives parents the opportunity to plan life with a child with Down syndrome.
The most accurate screening tests for Down syndrome include amniotic fluid (amniocentesis) or placental tissue (chorionic villus biopsy (CVS)) to look for abnormal chromosomes associated with Down syndrome. Both of these tests involve inserting a needle into the mother's abdomen, which is known to increase the risk of miscarriage. Thus, screening tests are not suitable for all pregnant women. Therefore, more often take blood and urine tests of the mother, and also conduct an ultrasound examination of the child. These screening tests are not perfect because they can miss cases of Down syndrome and are also at high risk of being positive when the child does not have Down syndrome. Thus, if a high risk is identified using these screening tests, further amniocentesis or CVS is required to confirm the diagnosis of Down syndrome.
What we did
We analyzed combinations of serum screening tests in the first (up to 14 weeks) and second (up to 24 weeks) trimesters of pregnancy with or without ultrasound screening in the first trimester. Our goal was to identify the most accurate tests for predicting the risk of Down syndrome during pregnancy. One ultrasound index (neckfold thickness) and seven different serological indexes (PAPP-A, total hCG, free beta-hCG, unbound estriol, alpha-fetoprotein, inhibin A, ADAM 12) were studied, which can be used separately, in ratios or in combination with each other, obtained before 24 weeks of gestation, thereby obtaining 32 screening tests for the detection of Down's syndrome. We found 22 studies involving 228615 pregnant women (including 1067 fetuses with Down syndrome).
Our goal was to identify the most accurate tests for predicting the risk of Down syndrome during pregnancy. One ultrasound index (neckfold thickness) and seven different serological indexes (PAPP-A, total hCG, free beta-hCG, unbound estriol, alpha-fetoprotein, inhibin A, ADAM 12) were studied, which can be used separately, in ratios or in combination with each other, obtained before 24 weeks of gestation, thereby obtaining 32 screening tests for the detection of Down's syndrome. We found 22 studies involving 228615 pregnant women (including 1067 fetuses with Down syndrome).
What we found
During Down Syndrome screening, which included tests during the first and second trimesters that combined to determine overall risk, we found that a test that included neckfold measurement and PAPP- A in the first trimester, as well as the determination of total hCG, unbound estriol, alpha-fetoprotein and inhibin A in the second trimester, turned out to be the most sensitive, as it allowed to determine 9out of 10 pregnancies associated with Down syndrome.![]()