Can women give men chlamydia
Detailed STD Facts - Chlamydia
What is chlamydia?
Chlamydia is a common STD caused by infection with Chlamydia trachomatis. It can cause cervicitis, urethritis, and proctitis.
In women, these infections can lead to:
- pelvic inflammatory disease (PID),
- tubal factor infertility,
- ectopic pregnancy, and
- chronic pelvic pain.
Lymphogranuloma venereum (LGV) is another type of STD caused by C. trachomatis. LGV is the cause of recent proctitis outbreaks among gay, bisexual, and other men who have sex with men (MSM) worldwide.1,2
How common is chlamydia?
CDC estimates that there were four million chlamydial infections in 2018.3 Chlamydia is also the most frequently reported bacterial sexually transmitted infection in the United States.4 It is difficult to account for many cases of chlamydia. Most people with the infection have no symptoms and do not seek testing. Chlamydia is most common among young people. Two-thirds of new chlamydial infections occur among youth aged 15-24 years.3 Estimates show that 1 in 20 sexually active young women aged 14-24 years has chlamydia.5
Disparities persist among racial and ethnic minority groups. In 2020, chlamydia rates for African Americans/Blacks were six times that of Whites.4 Chlamydia is also common among MSM. Among MSM screened for rectal chlamydial infection, positivity ranges from 3.0% to 10.5%.6,7 Among MSM screened for pharyngeal chlamydial infection, positivity has ranges from 0.5% to 2.3%.7.8
How do people get chlamydia?
Chlamydia spreads through vaginal, anal, or oral sex with someone with the infection. Semen does not have to be present to get or spread the infection.
Pregnant people can give chlamydia to their baby during childbirth. This can cause ophthalmia neonatorum (conjunctivitis) or pneumonia in some infants. 9-12 Rectal or genital infection can persist one year or longer in infants infected at birth.13 However, sexual abuse should be a consideration among young children with vaginal, urethral, or rectal infection beyond the neonatal period.
9-12 Rectal or genital infection can persist one year or longer in infants infected at birth.13 However, sexual abuse should be a consideration among young children with vaginal, urethral, or rectal infection beyond the neonatal period.
People treated for chlamydia can get the infection again if they have sex with a person with chlamydia.14
Who is at risk for chlamydia?
Sexually active people can get chlamydia through vaginal, anal, or oral sex without a condom with a partner who has chlamydia. It is a very common STD, especially among young people.3
Sexually active young people are at high risk of getting chlamydia for behavioral, biological, and cultural reasons. Some don’t always use condoms.15 Some may move from one monogamous relationship to another during the likely infectivity period of chlamydia. This can increase the risk of transmission.16 Teenage girls and young women may have cervical ectopy (where cells from the endocervix are present on the ectocervix). 17 Cervical ectopy may increase susceptibility to chlamydial infection. High chlamydia prevalence among young people also may reflect barriers to accessing STD prevention services. These barriers can include lack of transportation, cost, and perceived stigma.16-20
17 Cervical ectopy may increase susceptibility to chlamydial infection. High chlamydia prevalence among young people also may reflect barriers to accessing STD prevention services. These barriers can include lack of transportation, cost, and perceived stigma.16-20
MSM are also at risk for infection since chlamydia can spread by oral or anal sex. Among MSM screened for rectal infection, positivity ranges from 3.0% to 10.5%.6.7 Among MSM screened for pharyngeal infection, positivity ranges from 0.5% to 2.3%.7.8
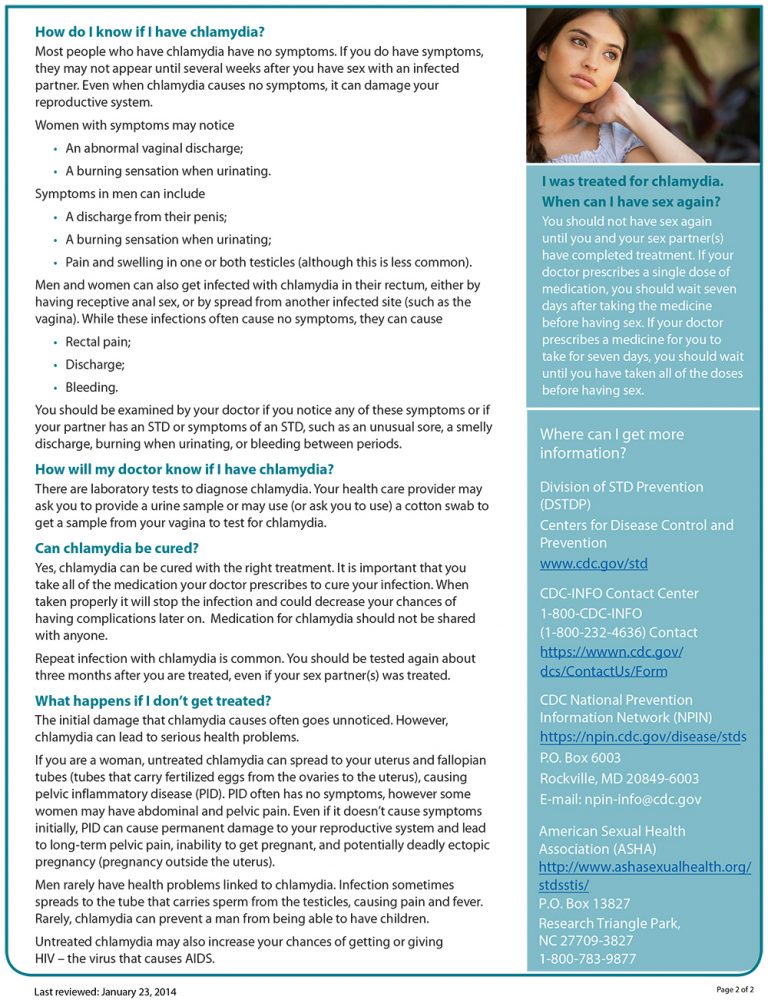
What are the symptoms of chlamydia?
Some refer to chlamydia as a “silent” infection. This is because most people with the infection have no symptoms or abnormal physical exam findings. Studies find that the proportion of people with chlamydia who develop symptoms vary by setting and study methodology. Two modeling studies estimate that about 10% of men and 5-30% of women with a confirmed infection develop symptoms.21. 22 The incubation period of chlamydia is unclear. Given the relatively slow replication cycle of the organism, symptoms may not appear until several weeks after exposure in people who develop symptoms.
22 The incubation period of chlamydia is unclear. Given the relatively slow replication cycle of the organism, symptoms may not appear until several weeks after exposure in people who develop symptoms.
In women, the bacteria initially infect the cervix. This may cause signs and symptoms of cervicitis (e.g., mucopurulent endocervical discharge, easily induced endocervical bleeding). It also can infect the urethra. This may cause signs and symptoms of urethritis (e.g., pyuria, dysuria, urinary frequency). Infection can spread from the cervix to the upper reproductive tract (i.e., uterus, fallopian tubes), causing PID. PID may be asymptomatic (“subclinical PID”)23 or acute, with typical symptoms of abdominal and/or pelvic pain. Signs of cervical motion tenderness and uterine or adnexal tenderness also may occur during examination.
Men with symptoms typically have urethritis, with a mucoid or watery urethral discharge and dysuria. Some men develop epididymitis (with or without symptomatic urethritis) with unilateral testicular pain, tenderness, and swelling. 24
24
Chlamydia can infect the rectum in men and women. This can happen either directly (through receptive anal sex), or via spread from the cervix and vagina in a woman.25, 26 While these infections often have no symptoms, they can cause symptoms of proctitis (e.g., rectal pain, discharge, and/or bleeding).26-28
Conjunctivitis can occur in both men and women through contact with infected genital secretions.29
While chlamydia can also spread to the throat by having oral sex, there are typically no symptoms. It also does not appear to be an important cause of pharyngitis.26
What health problems can result from chlamydia?
The initial damage that chlamydia causes is often unnoticed. However, infections can lead to serious health problems with both short- and long-term effects.
If a woman does not receive treatment, chlamydia can spread into the uterus or fallopian tubes, causing PID. Symptomatic PID occurs in about 10-15% of women who do not receive treatment. 30,31 However, chlamydia can also cause subclinical inflammation of the upper genital tract (“subclinical PID”). Both acute and subclinical PID can cause long-term damage to the fallopian tubes, uterus, and surrounding tissues. The damage can lead to chronic pelvic pain, tubal factor infertility, and potentially fatal ectopic pregnancy.32,33
30,31 However, chlamydia can also cause subclinical inflammation of the upper genital tract (“subclinical PID”). Both acute and subclinical PID can cause long-term damage to the fallopian tubes, uterus, and surrounding tissues. The damage can lead to chronic pelvic pain, tubal factor infertility, and potentially fatal ectopic pregnancy.32,33
Some patients with PID develop perihepatitis, or “Fitz-Hugh-Curtis Syndrome”. This syndrome includes inflammation of the liver capsule and surrounding peritoneum, which can cause right upper quadrant pain.
In pregnant people, untreated chlamydia can lead to pre-term delivery,34 ophthalmia neonatorum (conjunctivitis), and pneumonia in the newborn.
Reactive arthritis can occur in men and women, following infection with or without symptoms. This is sometimes part of a triad of symptoms (with urethritis and conjunctivitis) formerly referred to as Reiter’s Syndrome.35
What about chlamydia and HIV?
Untreated chlamydia may increase a person’s chances of getting or transmitting HIV.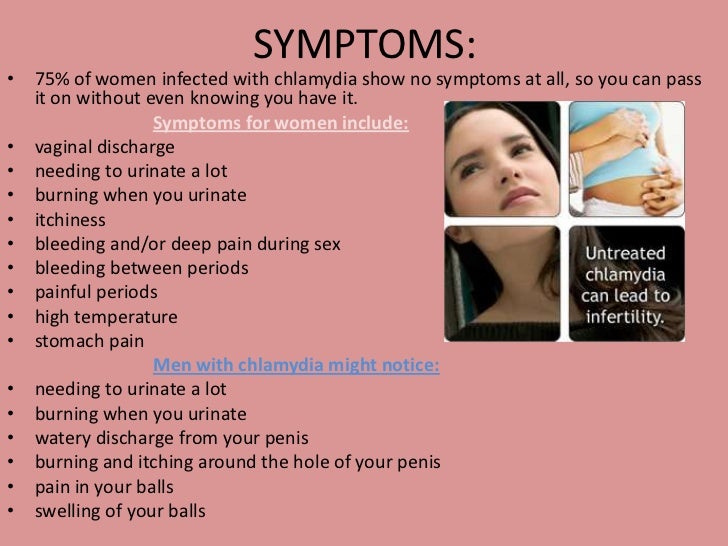 36
36
How does chlamydia affect a pregnant person and their baby?
In newborns, untreated chlamydia can cause:
- pre-term delivery,34
- ophthalmia neonatorum (conjunctivitis),
- and pneumonia.
Prospective studies show that chlamydial conjunctivitis and pneumonia occur in 18-44% and 3-16%, respectively, of infants born to those with chlamydia. 9-12 Neonatal prophylaxis against gonococcal conjunctivitis routinely performed at birth does not effectively prevent chlamydial conjunctivitis.37-39
Screening for and treating chlamydia in pregnant people is the best way to prevent disease in infants. At the first prenatal visit and during the third trimester, screen:
- All pregnant people under age 25; and
- All pregnant people 25 years and older at increased risk for chlamydia (e.g., those who have a new or more than one sex partner).
Retest those with infection four weeks and three months after they complete treatment. 40
40
Who to test for chlamydia?
Anyone with the following genital symptoms should not have sex until they see a healthcare provider:
- A discharge
- A burning sensation when peeing
- Unusual sores, or a rash
Anyone having oral, anal, or vaginal sex with a partner recently diagnosed with an STD should see a healthcare provider.
Because chlamydia usually has no symptoms, screening is necessary to identify most infections. Screening programs can reduce rates of adverse sequelae in women.31,41 CDC recommends yearly chlamydia screening of all sexually active women younger than 25. CDC also recommends screening for older women with risk factors, such as new or multiple partners, or a sex partner who has a sexually transmitted infection.40 Screen and treat those who are pregnant as noted in “How does chlamydia affect a pregnant person and their baby?” Women who are sexually active should discuss their risk factors with a healthcare provider to determine if more frequent screening is necessary.![]()
Routine screening is not necessary for men. However, consider screening sexually active young men in clinical settings with a high prevalence of chlamydia. This can include adolescent clinics, correctional facilities, and STD clinics. Consider this when resources permit and do not hinder screening efforts in women.40
Screen sexually active MSM who have insertive intercourse for urethral chlamydial infection. Also screen MSM who have receptive anal intercourse for rectal infection at least yearly. Screening for pharyngeal infection is not recommended. MSM, including those with HIV, should receive more frequent chlamydia screening at 3- to 6-month intervals, if risk behaviors persist or if they or their sexual partners have multiple partners.40
At the initial HIV care visit, providers should test all sexually active people for chlamydia. Test at least each year during HIV care. A patient’s healthcare provider might determine more frequent screening is necessary, based on the patient’s risk factors.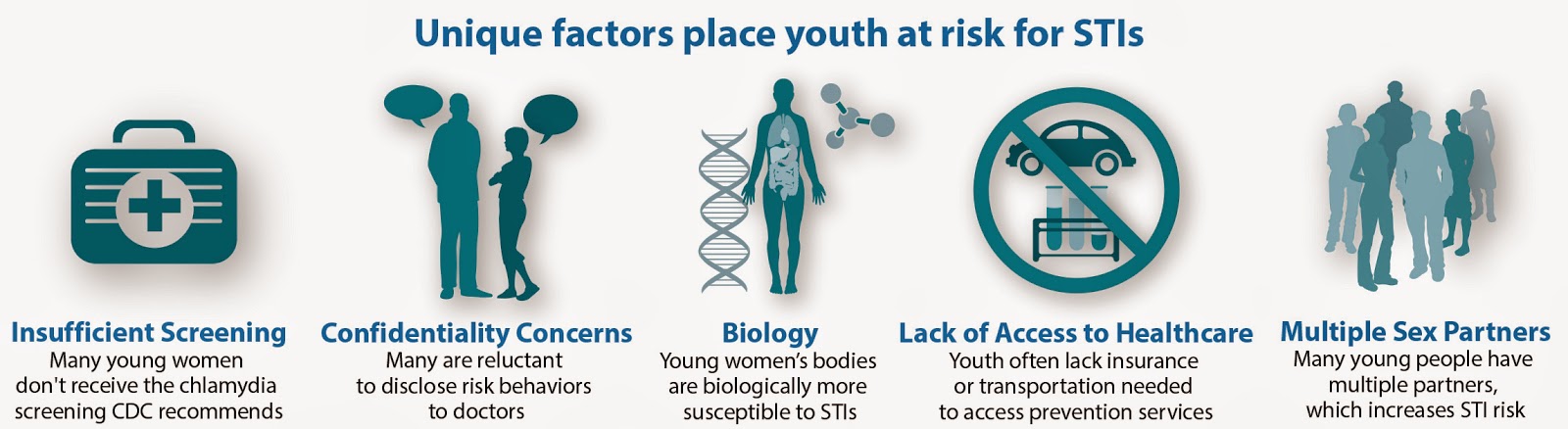 42
42
How is chlamydia diagnosed?
Diagnose chlamydia with nucleic acid amplification tests (NAATs), cell culture, and other types of tests. NAATs are the most sensitive tests to use on easy-to-obtain specimens. This includes vaginal swabs (either clinician- or patient-collected) or urine.43
To diagnose genital chlamydia in women using a NAAT, vaginal swabs are the optimal specimen. Urine is the specimen of choice for men. Urine is an effective alternative specimen type for women.43 Self-collected vaginal swab specimens perform as well as other approved specimens using NAATs.44 Patients may prefer self-collected vaginal swabs or urine-based screening to more invasive specimen collection.45 Adolescent girls may be good candidates for self-collected vaginal swab- or urine-based screening.
Diagnose rectal or pharyngeal infection by testing at the anatomic exposure site. While useful for these specimens, culture is not widely available. Additionally, NAATs have better sensitivity and specificity compared with culture for detecting C. trachomatis at non-genital sites.46-48 Most tests, including NAATs, are not FDA-cleared for use with rectal or pharyngeal swab specimens. NAATs have better sensitivity and specificity compared with culture for the detection of C. trachomatis at rectal sites.46-48 However, some laboratories have met set requirements and have validated NAAT testing on rectal and pharyngeal swab specimens.
Additionally, NAATs have better sensitivity and specificity compared with culture for detecting C. trachomatis at non-genital sites.46-48 Most tests, including NAATs, are not FDA-cleared for use with rectal or pharyngeal swab specimens. NAATs have better sensitivity and specificity compared with culture for the detection of C. trachomatis at rectal sites.46-48 However, some laboratories have met set requirements and have validated NAAT testing on rectal and pharyngeal swab specimens.
What is the treatment for chlamydia?
Antibiotics can easily cure chlamydia. Treatment options are the same, whether a person also has HIV or not.
Patients treated with single-dose antibiotics should not have sex for seven days. Patients treated with a seven-day course of antibiotics should not have sex until they complete treatment, and their symptoms are gone. This helps prevent spreading the infection to sex partners. It is important to take all medicine prescribed to cure chlamydia. Medicine should not be shared with anyone. Although treatment will cure the infection, it will not repair any long-term damage done by the disease. If a person’s symptoms continue for more than a few days after receiving treatment, a healthcare provider should reevaluate them.
Medicine should not be shared with anyone. Although treatment will cure the infection, it will not repair any long-term damage done by the disease. If a person’s symptoms continue for more than a few days after receiving treatment, a healthcare provider should reevaluate them.
Repeat infection with chlamydia is common.49 Women whose sex partners do not receive appropriate treatment are at high risk for re-infection. Having multiple chlamydial infections increases a woman’s risk of serious reproductive health problems (e.g., PID and ectopic pregnancy).50,51 A healthcare provider should retest those with chlamydia about three months after treatment of an initial infection. Retesting is necessary even if their partners receive successful treatment.40
Infants with chlamydia may develop conjunctivitis and/or pneumonia.10 Healthcare providers can treat infection in infants with antibiotics.
What about partners?
People treated for chlamydia should tell their recent sex partners so the partner can see a healthcare provider. “Recent” partners include anyone the patient had anal, vaginal, or oral sex with in the 60 days before symptom onset or diagnosis. This will help protect the partner from health problems and prevent re-infection.
“Recent” partners include anyone the patient had anal, vaginal, or oral sex with in the 60 days before symptom onset or diagnosis. This will help protect the partner from health problems and prevent re-infection.
Patients treated with single-dose antibiotics should not have sex for seven days. Patients treated with a seven-day course of antibiotics should not have sex until they complete treatment, and their symptoms go away.
For tips on talking to partners about sex and STD testing, visit www.gytnow.org/talking-to-your-partner/
In some states, healthcare providers may give people with chlamydia extra medicine or prescriptions to give to their sex partner(s). This is called “expedited partner therapy”, or “EPT.” Clinical trials comparing EPT to asking the patient to refer their partners in for treatment find that EPT leads to fewer re-infections in the index patient and more partner treatment.52 EPT is another strategy providers use to manage the partners of people with chlamydial infection. Partners should still seek medical care, regardless of whether they receive EPT. For more information about EPT, including the legal status in a specific area, see Legal Status of Expedited Partner Therapy.
Partners should still seek medical care, regardless of whether they receive EPT. For more information about EPT, including the legal status in a specific area, see Legal Status of Expedited Partner Therapy.
How can chlamydia be prevented?
Condoms, when used correctly, every time someone has sex can reduce the risk of getting or giving chlamydia.53 The only way to completely avoid chlamydia is to not have vaginal, anal, and oral sex. Another option is being in a long-term, mutually monogamous relationship with a partner who has been tested and does not have chlamydia.
References
1. O’Farrell N, Morison L, Moodley P, et al. Genital ulcers and concomitant complaints in men attending a sexually transmitted infections clinic: implications for sexually transmitted infections management. Sexually transmitted diseases 2008;35:545-9.
2. White JA. Manifestations and management of lymphogranuloma venereum. Current opinion in infectious diseases 2009;22:57-66.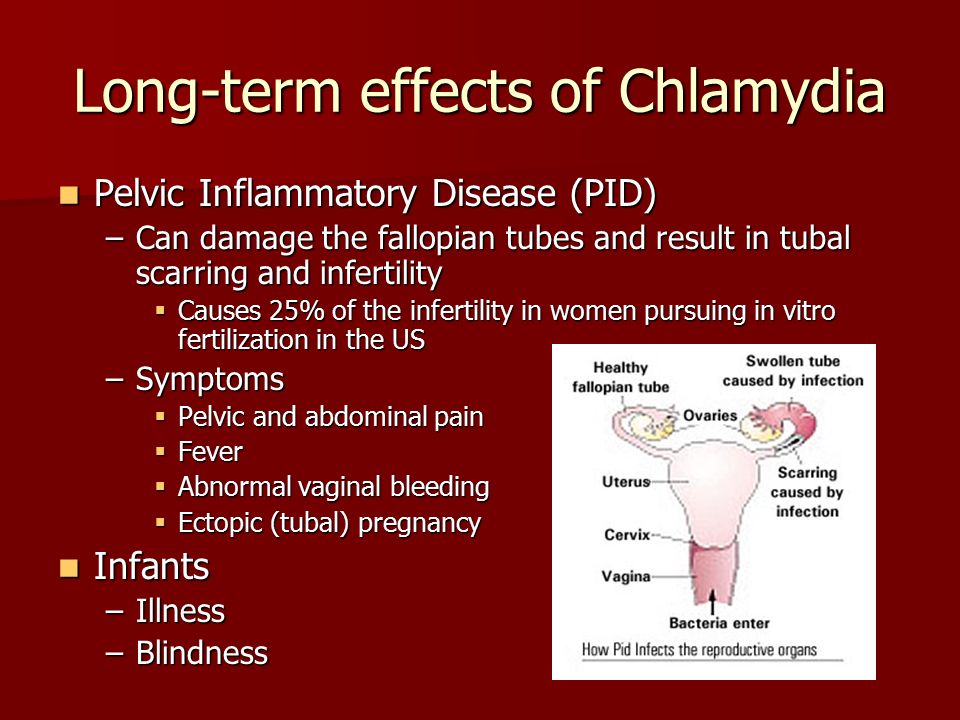
3. Kreisel KM, Spicknall IH, Gargano JW, Lewis FM, Lewis RM, Markowitz LE, Roberts H, Satcher Johnson A, Song R, St. Cyr SB, Weston EJ, Torrone EA, Weinstock HS. Sexually transmitted infections among US women and men: Prevalence and incidence estimates, 2018. Sex Transm Dis 2021; in press.
4. CDC. Sexually Transmitted Disease Surveillance, 2020. Atlanta, GA: Department of Health and Human Services; April 2022.
5. Torrone E, Papp J, Weinstock H. Prevalence of Chlamydia trachomatis Genital Infection Among Persons Aged 14–39 Years — United States, 2007–2012. MMWR 2014;63:834-8.
6. Marcus JL, Bernstein KT, Stephens SC, et al. Sentinel surveillance of rectal chlamydia and gonorrhea among males–San Francisco, 2005-2008. Sexually transmitted diseases 2010;37:59-61.
7. Pinsky L, Chiarilli DB, Klausner JD, et al. Rates of asymptomatic nonurethral gonorrhea and chlamydia in a population of university men who have sex with men. Journal of American college health : J of ACH 2012;60:481-4.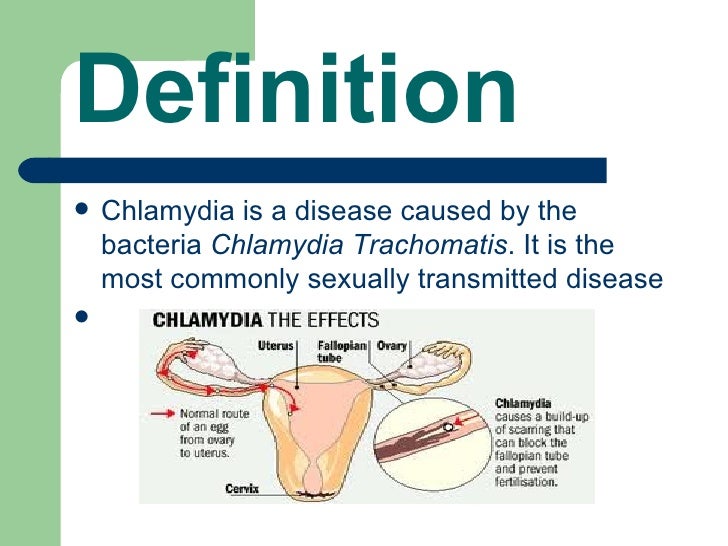
8. Park J, Marcus JL, Pandori M, Snell A, Philip SS, Bernstein KT. Sentinel surveillance for pharyngeal chlamydia and gonorrhea among men who have sex with men–San Francisco, 2010. Sexually transmitted diseases 2012;39:482-4.
9. Frommell GT, Rothenberg R, Wang S, McIntosh K. Chlamydial infection of mothers and their infants. The Journal of pediatrics 1979;95:28-32.
10. Hammerschlag MR, Chandler JW, Alexander ER, English M, Koutsky L. Longitudinal studies on chlamydial infections in the first year of life. Pediatric infectious disease 1982;1:395-401.
11. Heggie AD, Lumicao GG, Stuart LA, Gyves MT. Chlamydia trachomatis infection in mothers and infants. A prospective study. American journal of diseases of children (1960) 1981;135:507-11.
12. Schachter J, Grossman M, Sweet RL, Holt J, Jordan C, Bishop E. Prospective study of perinatal transmission of Chlamydia trachomatis. JAMA : the journal of the American Medical Association 1986;255:3374-7.
13. Bell TA, Stamm WE, Wang SP, Kuo CC, Holmes KK, Grayston JT. Chronic Chlamydia trachomatis infections in infants. JAMA : the journal of the American Medical Association 1992;267:400-2.
14. Batteiger BE, Tu W, Ofner S, et al. Repeated Chlamydia trachomatis genital infections in adolescent women. The Journal of infectious diseases 2010;201:42-51.
15. Eaton DK, Kann L, Kinchen S, et al. Youth risk behavior surveillance – United States, 2011. Morbidity and mortality weekly report Surveillance summaries (Washington, DC : 2002) 2012;61:1-162.
16. Kraut-Becher JR, Aral SO. Gap length: an important factor in sexually transmitted disease transmission. Sexually transmitted diseases 2003;30:221-5.
17. Singer A. The uterine cervix from adolescence to the menopause. British journal of obstetrics and gynaecology 1975;82:81-99.
18. Cunningham SD, Kerrigan DL, Jennings JM, Ellen JM. Relationships between perceived STD-related stigma, STD-related shame and STD screening among a household sample of adolescents.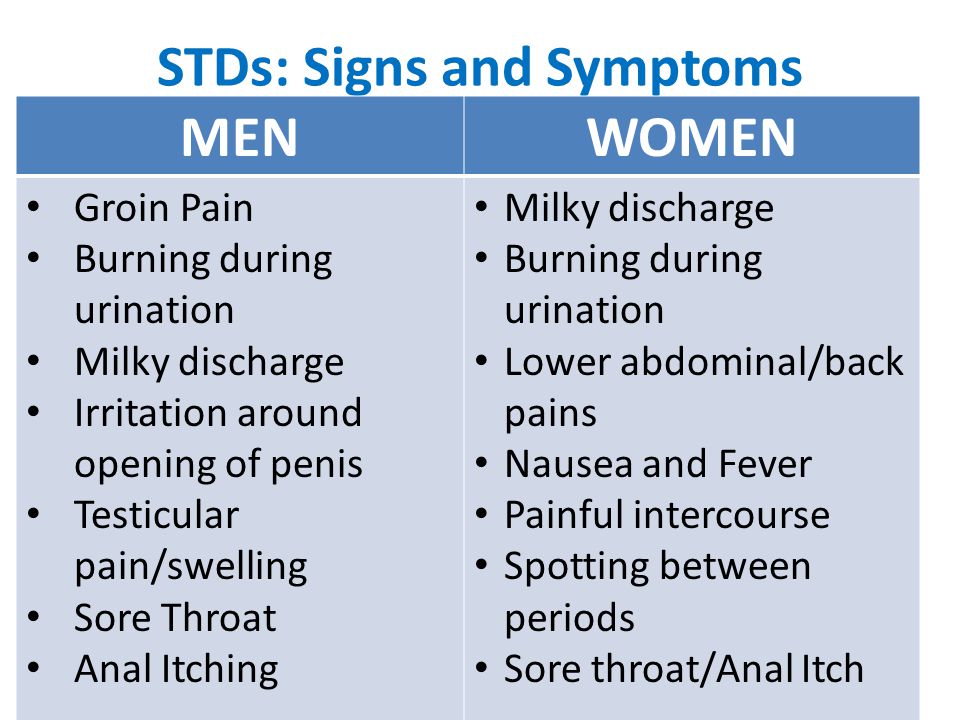 Perspectives on sexual and reproductive health 2009;41:225-30.
Perspectives on sexual and reproductive health 2009;41:225-30.
19. Elliott BA, Larson JT. Adolescents in mid-sized and rural communities: foregone care, perceived barriers, and risk factors. The Journal of adolescent health : official publication of the Society for Adolescent Medicine 2004;35:303-9.
20. Tilson EC, Sanchez V, Ford CL, et al. Barriers to asymptomatic screening and other STD services for adolescents and young adults: focus group discussions. BMC public health 2004;4:21.
21. Farley TA, Cohen DA, Elkins W. Asymptomatic sexually transmitted diseases: the case for screening. Preventive medicine 2003;36:502-9.
22. Korenromp EL, Sudaryo MK, de Vlas SJ, et al. What proportion of episodes of gonorrhoea and chlamydia becomes symptomatic? International journal of STD & AIDS 2002;13:91-101.
23. Wiesenfeld HC, Sweet RL, Ness RB, Krohn MA, Amortegui AJ, Hillier SL. Comparison of acute and subclinical pelvic inflammatory disease. Sexually transmitted diseases 2005;32:400-5.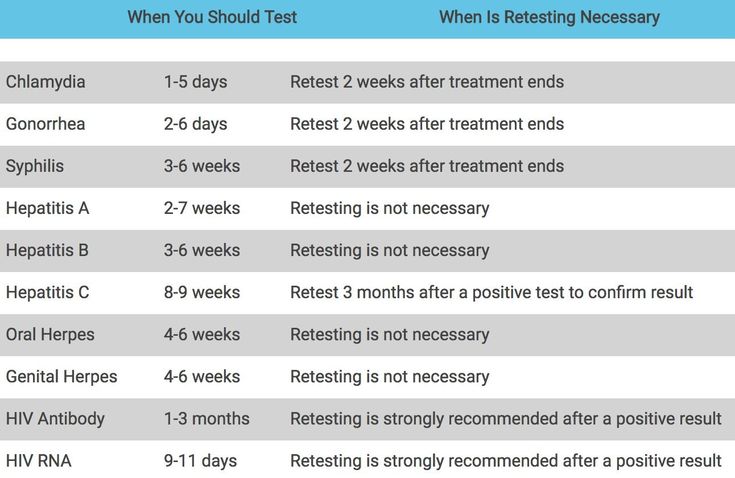
24. Berger RE, Alexander ER, Monda GD, Ansell J, McCormick G, Holmes KK. Chlamydia trachomatis as a cause of acute “idiopathic” epididymitis. The New England journal of medicine 1978;298:301-4.
25. Barry PM, Kent CK, Philip SS, Klausner JD. Results of a program to test women for rectal chlamydia and gonorrhea. Obstetrics and gynecology 2010;115:753-9.
26. Jones RB, Rabinovitch RA, Katz BP, et al. Chlamydia trachomatis in the pharynx and rectum of heterosexual patients at risk for genital infection. Annals of internal medicine 1985;102:757-62.
27. Quinn TC, Goodell SE, Mkrtichian E, et al. Chlamydia trachomatis proctitis. The New England journal of medicine 1981;305:195-200.
28. Thompson CI, MacAulay AJ, Smith IW. Chlamydia trachomatis infections in the female rectums. Genitourinary medicine 1989;65:269-73.
29. Kalayoglu MV. Ocular chlamydial infections: pathogenesis and emerging treatment strategies. Current drug targets Infectious disorders 2002;2:85-91.
30. Haggerty CL, Gottlieb SL, Taylor BD, Low N, Xu F, Ness RB. Risk of sequelae after Chlamydia trachomatis genital infection in women. The Journal of infectious diseases 2010;201 Suppl 2:S134-55.
31. Oakeshott P, Kerry S, Aghaizu A, et al. Randomized controlled trial of screening for Chlamydia trachomatis to prevent pelvic inflammatory disease: the POPI (prevention of pelvic infection) trial. BMJ (Clinical research ed) 2010;340:c1642.
32. Cates W, Jr., Wasserheit JN. Genital chlamydial infections: epidemiology and reproductive sequelae. American journal of obstetrics and gynecology 1991;164:1771-81.
33. Westrom L, Joesoef R, Reynolds G, Hagdu A, Thompson SE. Pelvic inflammatory disease and fertility. A cohort study of 1,844 women with laparoscopically verified disease and 657 control women with normal laparoscopic results. Sexually transmitted diseases 1992;19:185-92.
34. Rours GI, Duijts L, Moll HA, et al. Chlamydia trachomatis infection during pregnancy associated with preterm delivery: a population-based prospective cohort study. European journal of epidemiology 2011;26:493-502.
European journal of epidemiology 2011;26:493-502.
35. Carter JD, Inman RD. Chlamydia-induced reactive arthritis: hidden in plain sight? Best practice & research Clinical rheumatology 2011;25:359-74.
36. Fleming DT, Wasserheit JN. From epidemiological synergy to public health policy and practice: the contribution of other sexually transmitted diseases to sexual transmission of HIV infection. Sexually transmitted infections 1999;75:3-17.
37. Bell TA, Sandstrom KI, Gravett MG, et al. Comparison of ophthalmic silver nitrate solution and erythromycin ointment for prevention of natally acquired Chlamydia trachomatis. Sexually transmitted diseases 1987;14:195-200.
38. Chen JY. Prophylaxis of ophthalmia neonatorum: comparison of silver nitrate, tetracycline, erythromycin and no prophylaxis. The Pediatric infectious disease journal 1992;11:1026-30.
39. Isenberg SJ, Apt L, Wood M. A controlled trial of povidone-iodine as prophylaxis against ophthalmia neonatorum.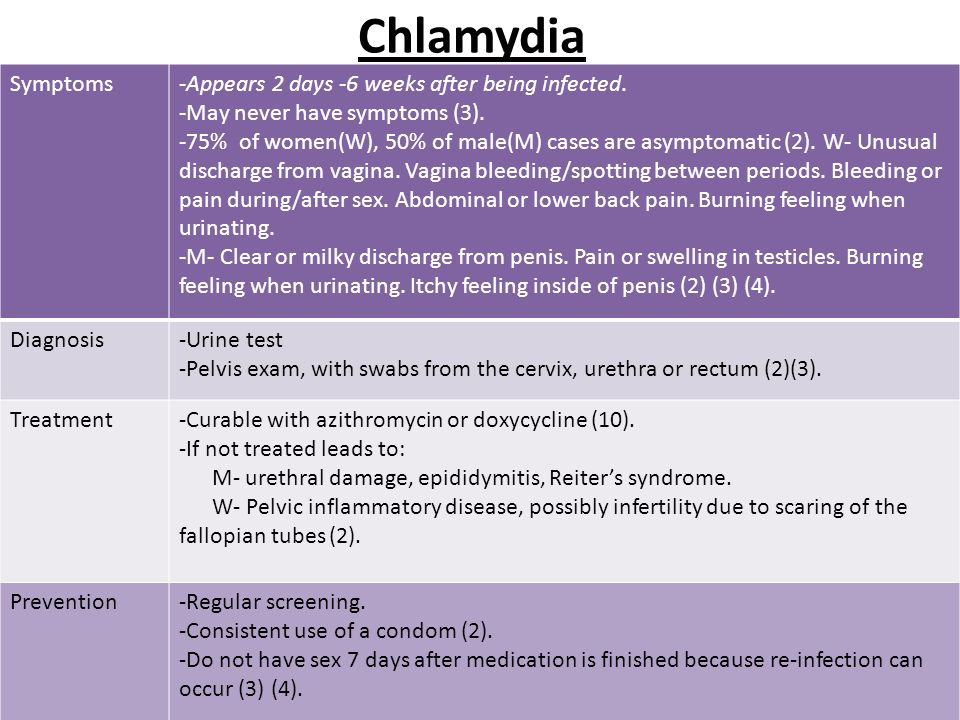 The New England journal of medicine 1995;332:562-6.
The New England journal of medicine 1995;332:562-6.
40. Workowski, KA, Bachmann, LH, Chang, PA, et. al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep 2021; 70(No. 4): 1-187.
41. Scholes D, Stergachis A, Heidrich FE, Andrilla H, Holmes KK, Stamm WE. Prevention of pelvic inflammatory disease by screening for cervical chlamydial infection. The New England journal of medicine 1996;334:1362-6.
42. CDC. Incorporating HIV prevention into the medical care of persons living with HIV. Recommendations of CDC, the Health Resources and Services Administration, the National Institutes of Health, and the HIV Medicine Association of the Infectious Diseases Society of America. MMWR Recommendations and reports : Morbidity and mortality weekly report Recommendations and reports / Centers for Disease Control 2003;52:1-24.
43. APHL. Laboratory Diagnostic Testing for Chlamydia trachomatis and Neisseria gonorrhoeae. Expert Consultation Meeting Summary Report.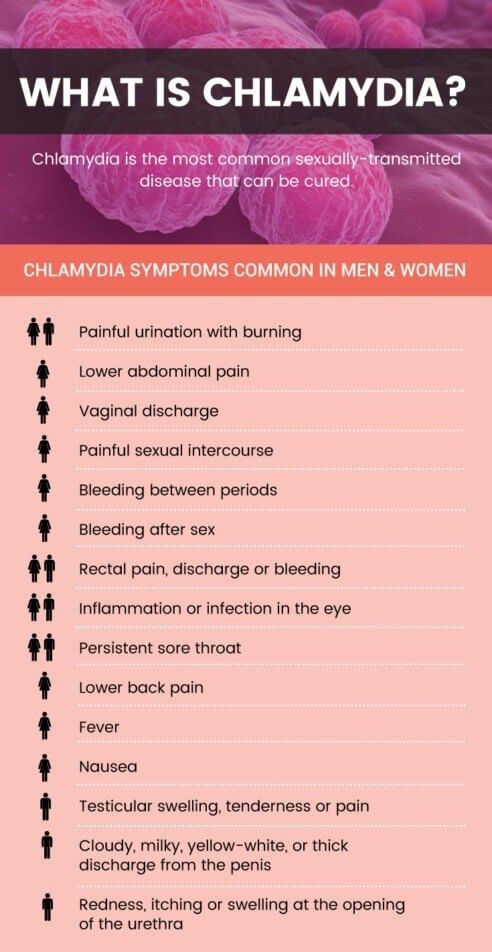 January 13-15, 2009. Atlanta, GA.
January 13-15, 2009. Atlanta, GA.
44. Schachter J, Chernesky MA, Willis DE, et al. Vaginal swabs are the specimens of choice when screening for Chlamydia trachomatis and Neisseria gonorrhoeae: results from a multicenter evaluation of the APTIMA assays for both infections. Sexually transmitted diseases 2005;32:725-8.
45. Doshi JS, Power J, Allen E. Acceptability of chlamydia screening using self-taken vaginal swabs. International journal of STD & AIDS 2008;19:507-9.
46. Bachmann LH, Johnson RE, Cheng H, et al. Nucleic acid amplification tests for diagnosis of Neisseria gonorrhoeae and Chlamydia trachomatis rectal infections. Journal of clinical microbiology 2010;48:1827-32.
47. Mimiaga MJ, Mayer KH, Reisner SL, et al. Asymptomatic gonorrhea and chlamydial infections detected by nucleic acid amplification tests among Boston area men who have sex with men. Sexually transmitted diseases 2008;35:495-8.
48. Schachter J, Moncada J, Liska S, Shayevich C, Klausner JD. Nucleic acid amplification tests in the diagnosis of chlamydial and gonococcal infections of the oropharynx and rectum in men who have sex with men. Sexually transmitted diseases 2008;35:637-42.
Nucleic acid amplification tests in the diagnosis of chlamydial and gonococcal infections of the oropharynx and rectum in men who have sex with men. Sexually transmitted diseases 2008;35:637-42.
49. Hosenfeld CB, Workowski KA, Berman S, et al. Repeat infection with Chlamydia and gonorrhea among females: a systematic review of the literature. Sexually transmitted diseases 2009;36:478-89.
50. Hillis SD, Owens LM, Marchbanks PA, Amsterdam LF, Mac Kenzie WR. Recurrent chlamydial infections increase the risks of hospitalization for ectopic pregnancy and pelvic inflammatory disease. American journal of obstetrics and gynecology 1997;176:103-7.
51. Bakken IJ, Skjeldestad FE, Lydersen S, Nordbo SA. Births and ectopic pregnancies in a large cohort of women tested for Chlamydia trachomatis. Sexually transmitted diseases 2007;34:739-43.
52. Trelle S, Shang A, Nartey L, Cassell JA, Low N. Improved effectiveness of partner notification for patients with sexually transmitted infections: systematic review.![]() BMJ (Clinical research ed) 2007;334:354.
BMJ (Clinical research ed) 2007;334:354.
53. Holmes KK, Levine R, Weaver M. Effectiveness of condoms in preventing sexually transmitted infections. Bulletin of the World Health Organization 2004;82:454-61.
Chlamydia Transmission | How Can You Get Chlamydia?
Medically reviewed by Rosanna Sutherby, PharmD on March 27, 2020. Written by Jordana White. To give you technically accurate, evidence-based information, content published on the Everlywell blog is reviewed by credentialed professionals with expertise in medical and bioscience fields.
Read more: How is chlamydia transmitted? | Can you develop a chlamydia infection on your own? | How easily is chlamydia transmitted? | How can you tell if you have chlamydia? | How can you get rid of chlamydia?
If you’re a sexually active woman, you probably already know at least something about sexually transmitted diseases (STDs). You’re likely aware that it’s important to protect yourself from STDs like chlamydia and gonorrhea, and know that engaging in unprotected sexual contact of any kind elevates your risk for these infections. But to stay safe, you also need to know about all other infection risk factors—so keep reading to learn more about the causes for chlamydia, how to get rid of chlamydia if you’re infected, and more.
But to stay safe, you also need to know about all other infection risk factors—so keep reading to learn more about the causes for chlamydia, how to get rid of chlamydia if you’re infected, and more.
Everlywell at-home STD testing for women can tell you whether you have chlamydia or other common STDs without having to go to a clinic.
Buy At-home STD Testing
How is chlamydia transmitted?
Chlamydia is a bacterial infection caused by Chlamydia trachomatis. It’s also considered a sexually transmitted infection (or STI), which means that it can spread between sex partners through any kind of sexual contact. This contact is not limited to vaginal intercourse; you can also contract oral chlamydia through oral sex, although it is a less common cause of Chlamydia trachomatis infections. Because sexual contact increases your risk, it’s a good idea to know if you have an STD before you have intercourse with a new partner.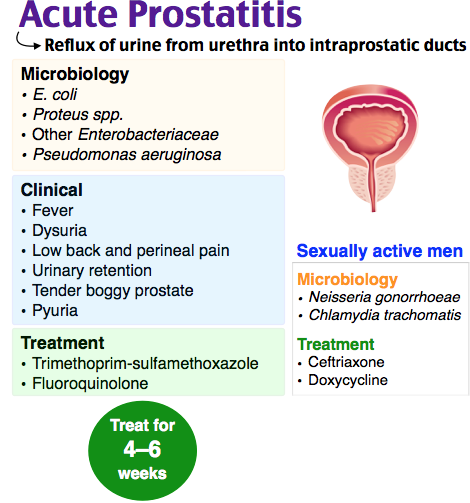
You can also spread chlamydia to different parts of your body without sexual contact. If you have a chlamydia infection in your vagina, you could spread it to your anus just by the act of wiping after you use the bathroom. You could also transmit a chlamydia infection to your eye, simply with hand-to-eye contact. Keep in mind that this form of eye infection is rare, but can still occur if your hands come in contact with the bacteria that causes chlamydia infections. And if you’re pregnant, you can give the infection to your unborn baby passing through your cervix.
In short, there are many different ways you can contract or spread chlamydia. To protect your sexual health and the health of your sexual partner, get tested for chlamydia before beginning any new relationship.
Check For Common STDs Today!
Can you develop a chlamydia infection on your own?
Fortunately, you can’t contract chlamydia on your own because it spreads through sexual contact with other people.
Chlamydia bacteria does, however, thrive in vaginal fluid, semen, and pre-ejaculate (the fluids that the penis may release before sexual climax). For that reason, using a latex condom properly during sexual intercourse and avoiding any kind of unprotected sex is the best way to protect yourself from developing or passing on a chlamydia infection. Caution is important, but fear is unnecessary: you don’t need to worry about contracting chlamydia from kissing someone or sitting on a public toilet seat.
How easily is chlamydia transmitted during sexual intercourse?
Unfortunately, chlamydia is very easily transmitted through unprotected sexual contact. This is especially true because chlamydia infections are sometimes asymptomatic—meaning they don’t cause noticeable symptoms.
In fact, any time you come in contact with the bacteria—even if your sex partner doesn’t ejaculate or you aren’t fully penetrated—you could become infected or pass along the chlamydial infection.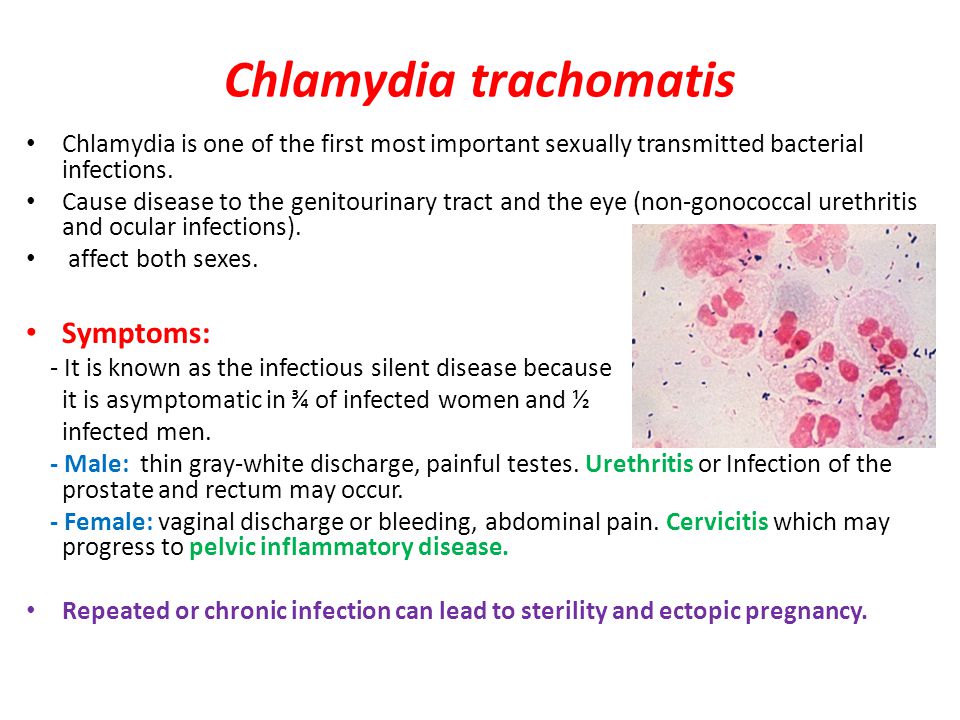 This being the case, men and women should get tested for STIs before beginning any new sexual relationship.
This being the case, men and women should get tested for STIs before beginning any new sexual relationship.
How can you tell if you have chlamydia?
You can have chlamydia without experiencing any symptoms. In fact, many women—approximately 70% of those who are infected—are completely asymptomatic, which means that they are also unaware that they are carrying Chlamydia trachomatis bacteria.
The lack of symptoms can cause health problems over time because an untreated chlamydia infection can lead to complications such as pelvic inflammatory disease (PID). Also, if you become pregnant and have chlamydia, you may develop an ectopic pregnancy (when a fertilized egg implants in your fallopian tubes instead of in your uterus). Some people with untreated chlamydia may develop reactive arthritis, a form of joint inflammation that’s caused by the chlamydia bacterium (as well as other kinds of bacteria). Untreated chlamydia can also damage your reproductive organs, which could potentially lead to infertility.
Thankfully, effective treatments exist for chlamydial infections. But to get treatment, you first need to determine if you have chlamydia in the first place. As mentioned above, you could have chlamydia without any symptoms. But there are certain telltale symptoms you may experience that can help identify it.
Chlamydia symptoms look very different in men and women. If your male partner experiences urethritis (itching or burning when urinating), or has discharge from his penis, he may have chlamydia. If that’s the case, you should both test for sexually transmitted infections.
Chlamydia symptoms in women look different. You may develop abnormal vaginal discharge, and you may experience a burning sensation when urinating. You might also experience pelvic pain, which could manifest as lower abdominal pain. Occasionally, you can develop spotting (bleeding between your periods).
If you notice any of these symptoms, or if you’ve been told by a partner that they have chlamydia, you should talk to your healthcare provider and consider getting tested for chlamydia.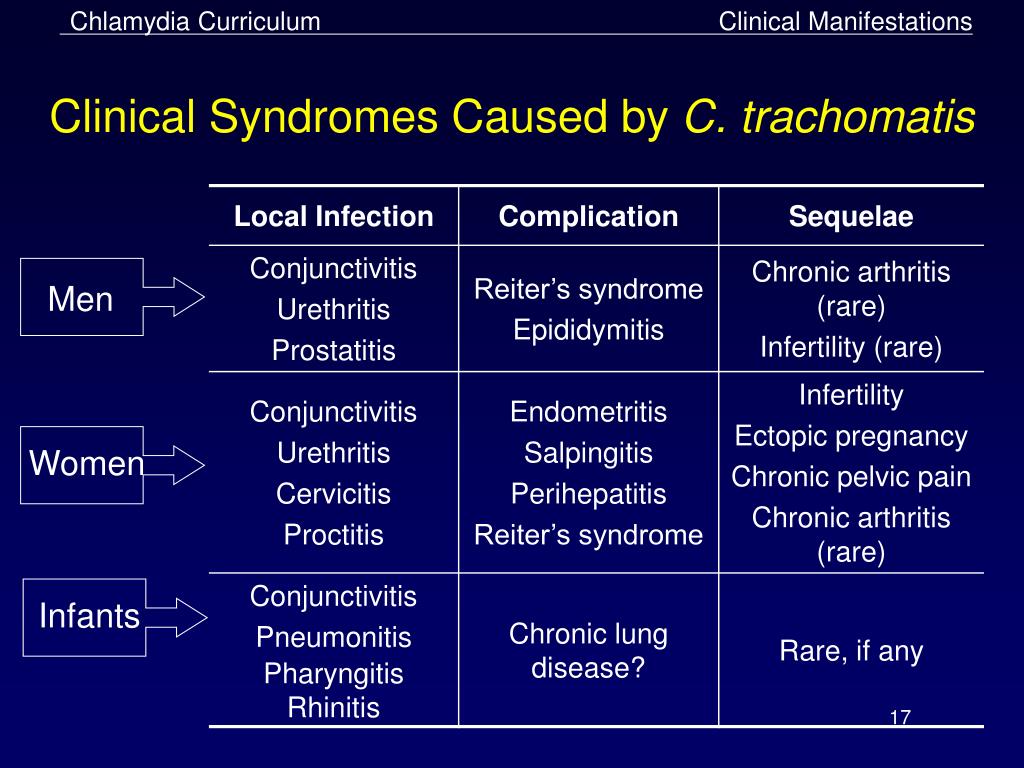 Fortunately, you can easily take a chlamydia test at home. And if you test positive for a chlamydial infection, getting treated is relatively easy.
Fortunately, you can easily take a chlamydia test at home. And if you test positive for a chlamydial infection, getting treated is relatively easy.
Test For STDs From Home
How can you get rid of chlamydia?
If your chlamydia test comes back positive, you may be wondering how to get chlamydia treated. It’s important to discuss treatment options with your healthcare provider. Most likely, you will be treated for chlamydia with oral antibiotics. With treatment, infections often clear up in one to two weeks.
Even if your symptoms resolve sooner, however, it’s very important to complete your healthcare provider’s entire course of prescribed antibiotics. Otherwise, the infection may not be completely eliminated and you could be at risk for reinfection. You could also still pass chlamydia to a partner if you don’t complete the recommended course of antibiotics.
Finally, as part of your treatment for chlamydia, connect with any sexual partners you may have unintentionally exposed to this infection.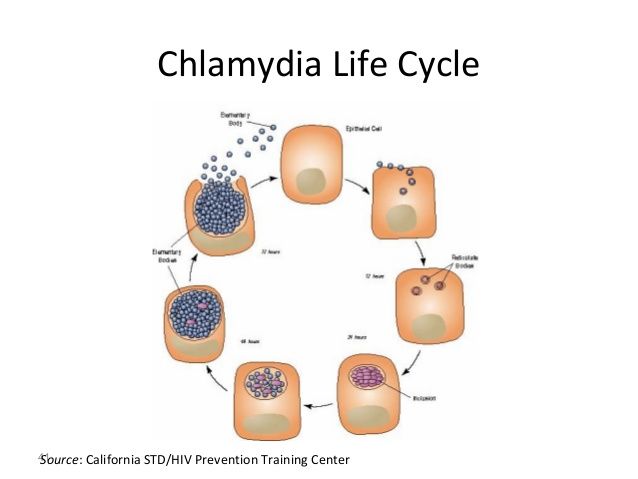 Your healthcare provider may also recommend antibiotics for your partner(s). This is a key part of chlamydia treatment, since it can help prevent reinfection when you resume sexual intercourse.
Your healthcare provider may also recommend antibiotics for your partner(s). This is a key part of chlamydia treatment, since it can help prevent reinfection when you resume sexual intercourse.
Chlamydia is a potentially harmful infection, but fortunately, it’s easy to test for. It’s also simple to treat when you have a confirmed diagnosis. The important thing is stay informed and know your status—something you can do from the privacy and comfort of home with our STD Test for women.
Check For STDs At Home!
Related content
STDs in Women: A Comprehensive Guide
What are the different types of STDs that men and women can get?
How do you know if you have an STD?
What Do STD Discharges Look Like?
7 Health Tips For Women’s Health Week
References
1. Overview: Chlamydia. National Health Service. URL. Accessed March 27, 2020.
2. Chlamydia - CDC Fact Sheet. Centers for Disease Control and Prevention. URL. Accessed March 27, 2020.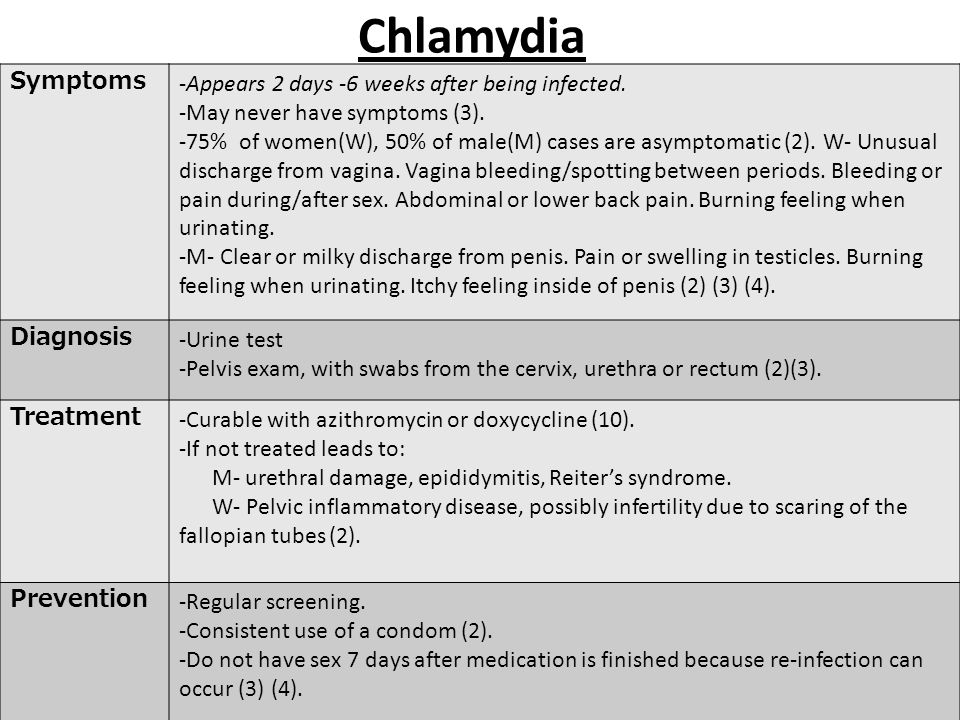
3. Symptoms: Chlamydia. National Health Service. UR. Accessed March 27, 2020.
4. Chlamydia (chlamydia trachomatis genital infection). New York State Department of Health. URL. Accessed March 27, 2020.
5. Chlamydia trachomatis. Mayo Clinic. URL. Accessed March 27, 2020.
6. Chlamydia Treatment and Care. Centers for Disease Control and Prevention. URL. Accessed March 27, 2020.
7. Chlamydia trachomatis. Mayo Clinic. URL. Accessed March 27, 2020.
CHLAMYDIOSIS
CHLAMYDIOSIS
What is chlamydia?
Chlamydia is a predominantly sexually transmitted infectious disease caused by chlamydia (Chlamydia trachomatis) that can infect both men and women. It can cause serious harm to the female reproductive system, which can subsequently make it difficult or impossible for a woman to become pregnant. According to WHO, urogenital chlamydia is one of the most common diseases among STIs.
The causative agent of the disease is chlamydia, an intracellular parasite that, in its cycle of development, resembles both a virus and a bacterium.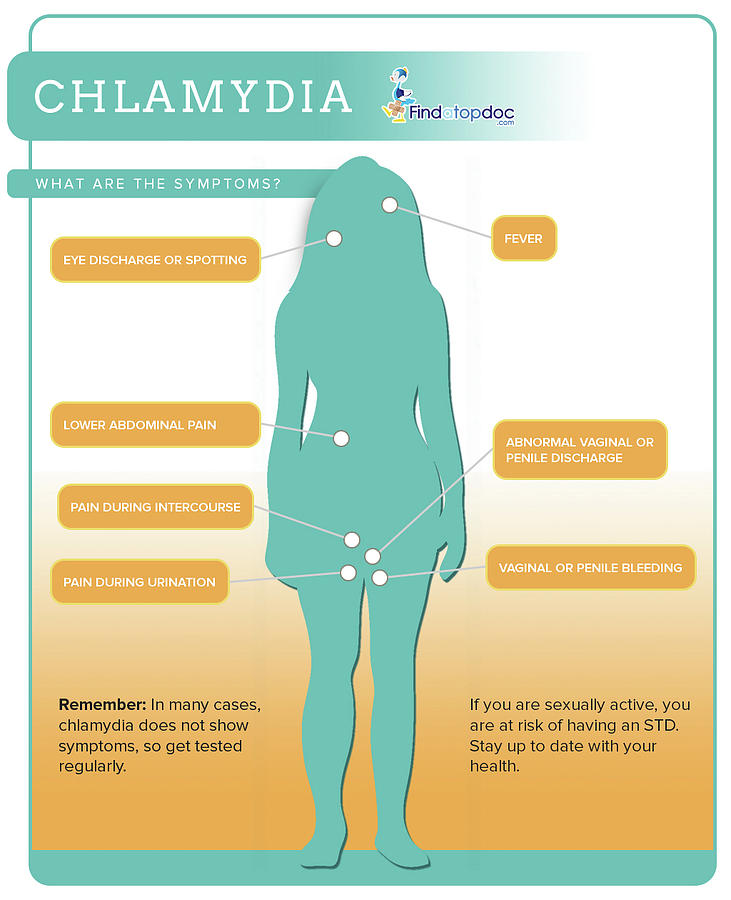 The incubation period for the development of chlamydia is from 5-7 days to 3-6 weeks (average 20-30 days)
The incubation period for the development of chlamydia is from 5-7 days to 3-6 weeks (average 20-30 days)
How is chlamydia transmitted?
1. Sexual contact, including vaginal, anal and oral sex. The probability of transmission during a single sexual intercourse is 68% from an infected woman to a man and 25% from an infected man to a woman.
2. Vertical - infection of newborns (conjunctivitis or pneumonia) during childbirth from a sick mother while passing through the birth canal.
3. The contact-household route of infection with chlamydia is noted much less frequently, through bedding and toiletries, linen, etc. Cases of infection of the mucous membrane of the conjunctiva of the eye are described when transferring secretions from the genital organs with the hands.
What are the manifestations of chlamydial infection?
Most people with chlamydia have no symptoms and many are unaware they have the infection.
Women with symptoms may notice unusual vaginal discharge, burning during urination. In addition, periodic aching pains in the lower abdomen and during intercourse, as well as post-contact spotting, are possible.
In addition, periodic aching pains in the lower abdomen and during intercourse, as well as post-contact spotting, are possible.
Symptoms in men may include: discharge from the penis; burning sensation when urinating; pain and swelling in one or both testicles (although this is less common).
Men and women can also get chlamydia in the rectum. It occurs during anal sex, or by spread from another infected site (such as the vagina). Although these infections often cause no symptoms, they can cause rectal pain, discharge, and bleeding.
How to find out about infection with chlamydia?
Laboratory tests are available to diagnose chlamydia. The most accurate and sensitive is PCR, which makes it possible to detect even a small amount of the pathogen in the test material. For research, scrapings are taken from the cervix and from the urethra, blood, semen, urine.
What are the complications of chlamydial infection?
The initial harm caused by chlamydia often goes unnoticed.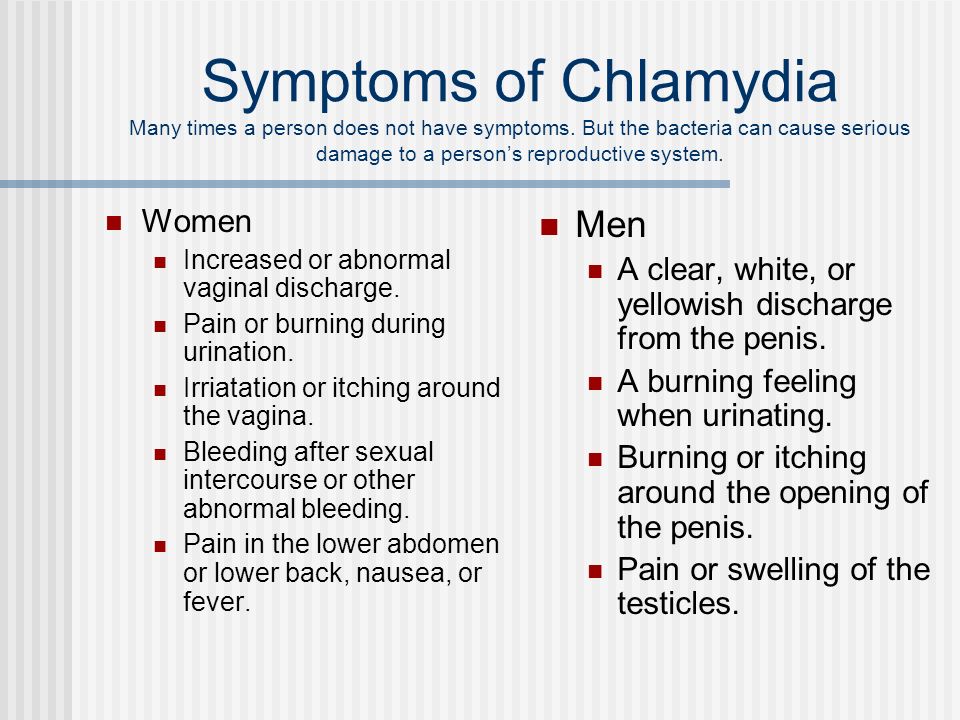 However, chlamydia can lead to serious health problems. Urogenital complications of chlamydia in men are chlamydial prostatitis, urethritis, epididymitis.
However, chlamydia can lead to serious health problems. Urogenital complications of chlamydia in men are chlamydial prostatitis, urethritis, epididymitis.
In women, if untreated, chlamydia causes the development of adhesions, which further leads to the development of infertility, or may cause a potentially life-threatening ectopic pregnancy. One of the serious complications of chlamydia is urethro-oculo-synovial syndrome, characterized by a triad of clinical manifestations: conjunctivitis, urethritis, arthritis.
Can chlamydia be cured?
Yes, chlamydia can be cured with the right treatment. It is important that you take all the medicines your doctor has prescribed to help you heal your infection. Proper medication will cure the infection and may reduce the chance of complications in the future.
Re-infection with chlamydia often occurs. You should not have sex until you and your partner have completed your treatment. You should be rechecked about a month after the end of treatment, even if your partner has also been treated.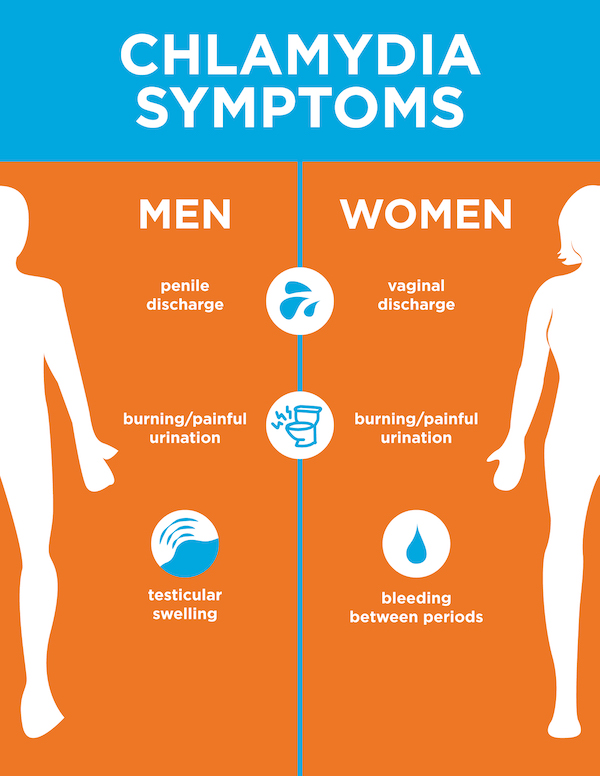
Dermatovenereologist Islyamova R.M.
Chlamydia - KVD №2
What is chlamydia?
Chlamydia is a common sexually transmitted infection (STI). The disease is caused by the bacterium Chlamydia trachomatis (Chlamydia trachomatis), which affects the female genital area and is the cause of non-gonococcal urethritis in men. Manifestations of chlamydia are usually minor or absent, but serious complications develop. Complications can cause irreparable damage to the body, including infertility - all this proceeds very secretly.
Chlamydia also causes penile discharge in infected men.
Ways of contracting chlamydia
Chlamydia can be transmitted through:
- vaginal or anal contact with an infected partner;
- less common with oral sex;
- use of sex toys with an infected partner;
- infection of a newborn during childbirth from a sick mother.
Absolutely all sexually active people can get chlamydia. The greater the number of sexual partners, the greater the risk of infection. The risk of infection is especially high in girls, because their cervix is not fully formed. About 75% of new cases occur in women under 25 years of age. By the age of 30, approximately 50% of sexually active women have had chlamydia. In sexually active men, the risk of infection is highest between the ages of 20 and 24.
The greater the number of sexual partners, the greater the risk of infection. The risk of infection is especially high in girls, because their cervix is not fully formed. About 75% of new cases occur in women under 25 years of age. By the age of 30, approximately 50% of sexually active women have had chlamydia. In sexually active men, the risk of infection is highest between the ages of 20 and 24.
You cannot get chlamydia through kisses, hugs, dishes, baths, towels.
Manifestations of chlamydia
Chlamydia is very secretive. About 75% of infected women and 50% of infected men are asymptomatic. If manifestations of the disease develop, then this occurs approximately 1 to 3 weeks after infection.
In women, chlamydia first affects the cervix and urethra (urinary canal).
Manifestations:
- unusual vaginal discharge;
- pain or discomfort when urinating;
If the infection penetrates to the appendages, manifestations are possible:
- pain in the lower abdomen;
- pain in the lumbar region;
- nausea;
- slight increase in temperature;
- pain during intercourse or bleeding after it;
- bleeding between periods.

Symptoms in men:
- clear or cloudy discharge from the penis;
- pain or discomfort when urinating;
- there may be burning and itching in the area of the outlet of the urethra;
- rarely pain and/or swelling of the testicles.
Men or women who have anal sex with an infected partner can infect the rectum, resulting in inflammation, pain, discharge, or bleeding from the rectum.
Chlamydia can cause sore throat (pharyngitis) in men and women who have oral contact with an infected partner.
What complications can develop if chlamydia is not treated?
If the disease is not treated, serious short-term and persistent complications develop. Like the disease itself, complications often occur insidiously.
In women with untreated chlamydia, infection can spread from the urethra to the fallopian tubes (tubes that carry eggs from the ovaries to the uterus) - this causes (in 40% of cases) the development of pelvic inflammatory disease (PID). PID causes permanent damage to the fallopian tubes, uterus, and surrounding tissues. Chronic pelvic pain, infertility and ectopic pregnancy are the result of PID.
PID causes permanent damage to the fallopian tubes, uterus, and surrounding tissues. Chronic pelvic pain, infertility and ectopic pregnancy are the result of PID.
Women with chlamydia are more susceptible to HIV infection, the risk increases by almost 5 times.
To prevent serious consequences of chlamydia, annual chlamydia screening is required for all sexually active women 25 years of age and younger. An annual examination is necessary for women over 25 who are at risk (new sexual partner, multiple sexual partners). All pregnant women should be screened for chlamydia.
Complications of chlamydia are rare in men. The infection sometimes extends to the epididymis and causes pain, fever, and, rarely, male infertility (sterility).
Rarely, chlamydial infection can cause inflammation of the joints in combination with skin lesions, inflammation of the eyes and urinary tract - this is the so-called Reiter's syndrome.
The effect of chlamydia on a pregnant woman and her child
Chlamydia in pregnant women increases the risk of miscarriage, premature detachment of the placenta. Newborns from infected mothers can get eye and lung infections. A lung infection (pneumonia) can be fatal to a newborn.
Newborns from infected mothers can get eye and lung infections. A lung infection (pneumonia) can be fatal to a newborn.
Diagnosis of chlamydia
Diagnosis includes observation of the patient's clinical symptoms, examination for chlamydia of smears from the cervix, scraping from the urinary canal, the first morning portion of urine. Most often, the study is carried out by PCR (polymerase chain reaction). Swabs and scrapings may cause minor discomfort.
In addition, a blood test is performed by ELISA (enzyme-linked immunosorbent assay) for the presence of immunity to chlamydia, this auxiliary test often helps to establish an accurate diagnosis.
Chlamydia treatment
Chlamydia treatment is with oral antibiotics. To prevent re-infection, all sexual partners must be found, examined and treated. Patients with chlamydia should refrain from unprotected sex during treatment, otherwise it is possible to re-infect the sexual partner. Unfortunately, after successful treatment, re-infection with chlamydia is possible, since a strong immunity to this microorganism does not develop. Repeated infection of women with chlamydia leads to a significant increase in the risk of serious complications, including infertility. A re-examination is carried out 4 weeks after treatment.
Repeated infection of women with chlamydia leads to a significant increase in the risk of serious complications, including infertility. A re-examination is carried out 4 weeks after treatment.
Prevention of chlamydia
The best way to prevent sexually transmitted infections is through long-term sexual contact with one healthy sexual partner. Latex male condoms, when used correctly, drastically reduce the risk of transmission.
Annual chlamydia screening required for all sexually active women aged 25 and under. An annual examination is also necessary for women over 25 who are at risk (new sexual partner, multiple sexual partners). All pregnant women should be screened for chlamydia.
Any manifestations, such as pain or discomfort when urinating, unusual rash, discharge are a signal to stop sexual intercourse and immediately examine in a specialized clinic - KVD. If the patient is found to have chlamydia (or any other STI), he must inform his sexual partners so that they also undergo a full examination and appropriate treatment.