0 negative blood type pregnancy
Rh Incompatibility During Pregnancy (for Parents)
One of the first tests a pregnant woman should expect is a blood-type test. This test checks her blood type and Rh factor. Her Rh factor may play a role in her baby's health, so it's important to know this information early in pregnancy.
What's an Rh Factor?
An Rh factor is a protein found on some red blood cells (RBCs). Not everyone carries this protein, though most do. They are Rh-positive. People who don't carry the protein are Rh-negative.
What if Parents Don't Have the Same Rh Factor?
When a mother-to-be and father-to-be are not both positive or negative for Rh factor, it's called Rh incompatibility.
For example:
- If a woman who is Rh negative and a man who is Rh positive conceive a baby, the fetus may have Rh-positive blood, inherited from the father. (About half of the children born to an Rh-negative mother and Rh-positive father will be Rh-positive.
)
Rh incompatibility usually isn't a problem if it's the mother's first pregnancy. That's because the baby's blood does not normally enter the mother's circulatory system during the pregnancy.
During the birth, though, the mother's and baby's blood can mix. If this happens, the mother's body recognizes the Rh protein as a foreign substance. It then might begin making antibodies (proteins that act as protectors if foreign cells enter the body) against the Rh protein.
Rh-negative pregnant women can be exposed to the Rh protein that might cause antibody production in other ways too. These include:
- blood transfusions with Rh-positive blood
- miscarriage
- ectopic pregnancy
When Is a Baby at Risk?
Rh antibodies are harmless until the mother's second or later pregnancies. If she is ever carrying another Rh-positive child, her Rh antibodies will recognize the Rh proteins on the surface of the baby's blood cells as foreign. Her antibodies will pass into the baby's bloodstream and attack those cells.
Her antibodies will pass into the baby's bloodstream and attack those cells.
This can make the baby's red blood cells swell and rupture. This is known as hemolytic or Rh disease of the newborn. It can make a baby's blood count get very low.
How Is Rh Incompatibility Treated?
If a pregnant woman has the potential to develop Rh incompatibility, doctors give her a series of two Rh immune-globulin shots during her first pregnancy. She'll get:
- the first shot around the 28th week of pregnancy
- the second shot within 72 hours of giving birth
Rh immune-globulin acts like a vaccine. It prevents the mother's body from making any Rh antibodies that could cause serious health problems in the newborn or affect a future pregnancy.
A woman also might get a dose of Rh immune-globulin if she has a miscarriage, an amniocentesis, or any bleeding during pregnancy.
If a doctor finds that a woman has already developed Rh antibodies, her pregnancy will be closely watched to make sure that those levels are not too high.
In rare cases, if the incompatibility is severe and a baby is in danger, the baby can get special blood transfusions called exchange transfusions either before birth (intrauterine fetal transfusions) or after delivery. Exchange transfusions replace the baby's blood with blood with Rh-negative blood cells. This stabilizes the level of red blood cells and minimizes damage from Rh antibodies already in the baby's bloodstream.
Thanks to the success rate of Rh immune-globulin shots, exchange transfusions in Rh-incompatible pregnancies are rarely needed in the United States.
What Else Should I Know?
If you're not sure what your Rh factor is and think you're pregnant, it's important to start regular prenatal care as soon as possible — including blood-type testing. With early detection and treatment of Rh incompatibility, you can focus on more important things — like welcoming a new, healthy baby.
Reviewed by: Thinh Phu Nguyen, MD
Date reviewed: July 2022
Blood Types (for Parents) - Nemours KidsHealth
Blood transfusions are a lifesaving treatment for many Americans. Blood transfusions are needed for many reasons, including surgery, after accidents, and for patients with
Blood transfusions are needed for many reasons, including surgery, after accidents, and for patients with
chronicillnesses and cancer. Every 2 seconds, someone needs a blood transfusion.
Blood cannot be artificially made, so doctors rely on volunteer donations. To keep the blood supply safe, every donation is tested for blood type and checked for infectious diseases.
What Are the Components of Blood?
All blood contains these basic components:
- red blood cells that deliver oxygen
- white blood cells that fight infections
- platelets that help blood clot
- plasma, the liquid part of blood
But not everyone has the same blood type.
What Are the Blood Types?
Categorizing blood according to type helps prevent reactions when someone gets a blood transfusion. Red blood cells have markers on their surface that characterize the cell type. These markers (also called antigens) are proteins and sugars that our bodies use to identify the blood cells as belonging in us.
These markers (also called antigens) are proteins and sugars that our bodies use to identify the blood cells as belonging in us.
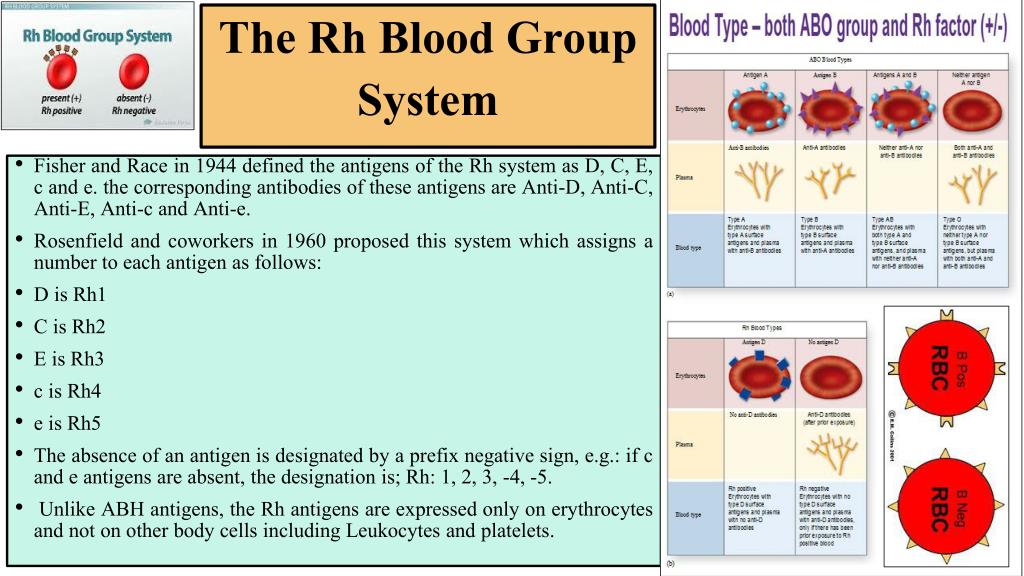
The two main blood groups are ABO and Rh.
The ABO blood system has four main types:
- Type A: This blood type has a marker known as A.
- Type B: This blood type has a marker known as B.
- Type AB: This blood type has both A and B markers.
- Type O: This blood type has neither A nor B markers.
Blood is further classified as being either "Rh positive" (meaning it has Rh factor) or "Rh negative" (without Rh factor).
So, there are eight possible blood types:
- O negative. This blood type doesn't have A or B markers, and it doesn't have Rh factor.
- O positive. This blood type doesn't have A or B markers, but it does have Rh factor. O positive blood is one of the two most common blood types (the other is A positive).
- A negative. This blood type has A marker only.
- A positive. This blood type has A marker and Rh factor, but not B marker. Along with O positive, it's one of the two most common blood types.
- B negative. This blood type has B marker only.
- B positive. This blood type has B marker and Rh factor, but not A marker.
- AB negative. This blood type has A and B markers, but not Rh factor.
- AB positive. This blood type has all three types of markers — A, B, and Rh factor.
Having any of these markers (or none of them) doesn't make a person's blood any healthier or stronger. It's just a genetic difference, like having green eyes instead of blue or straight hair instead of curly.
Why Are Blood Types Important?
The immune system is the body's protection against invaders. It can identify antigens as self or nonself. To get a blood transfusion safely, a person's immune system must recognize the donor cells as a match to his or her own cells. If a match isn't recognized, the cells are rejected.
To get a blood transfusion safely, a person's immune system must recognize the donor cells as a match to his or her own cells. If a match isn't recognized, the cells are rejected.
The immune system makes proteins called antibodies that act as protectors if foreign cells enter the body. Depending on which blood type a person has, the immune system will make antibodies to react against other blood types.
If a patient gets the wrong blood type, the antibodies immediately set out to destroy the invading cells. This aggressive, whole-body response can give someone a fever, chills, and low blood pressure. It can even cause vital body systems — like breathing or the kidneys — to fail.
Here's an example of how the blood type-antibody process works:
- Let's say you have type A blood. Because your blood contains the A marker, it makes B antibodies.
- If B markers (found in type B or type AB blood) enter your body, your type A immune system gets fired up against them.
- This means that you can only get a transfusion from someone with A or O blood, not from someone with B or AB blood.
In the same way, if you have the B marker, your body makes A antibodies. So as a person with type B blood, you could get a transfusion from someone with B or O blood, but not A or AB.
Things are a little different for people with type AB or type O blood:
- If you have both A and B markers on the surface of your cells (type AB blood), your body does not need to fight the presence of either.
- This means that someone with AB blood can get a transfusion from someone with A, B, AB, or O blood.
But if you have type O blood, your red blood cells have no A or B markers. So:
- Your body will have both A and B antibodies and will therefore feel the need to defend itself against A, B, and AB blood.
- A person with O blood can only get a transfusion with O blood.
Blood transfusions are one of the most frequent lifesaving procedures hospitals do. Blood is collected from healthy donors every day, and more blood donors are always needed. One blood donation can save up to three lives.
Blood is collected from healthy donors every day, and more blood donors are always needed. One blood donation can save up to three lives.
Pregnancy in women with Rh-negative blood
The issue of Rhesus conflict during pregnancy is one of the few in medicine, in which all the i's are dotted and not only diagnostic and treatment methods have been developed, but, most importantly, effective prevention.
The history of immunoprophylaxis of Rhesus conflict is a rare example of unconditional success in medicine. Indeed, after the introduction of a set of preventive measures, infant mortality from complications of the Rhesus conflict decreased from 46 to 1.6 per 100 thousand children - that is, almost 30 times.
What is Rh conflict, why does it occur and what can be done to minimize the risk of its occurrence?
The entire population of the planet, depending on the presence or absence on erythrocytes (red blood cells) of the protein, denoted by the letter "D", is divided respectively into Rh-positive and Rh-negative people. According to approximate data, about 15% of Europeans are Rh-negative. When pregnancy occurs in an Rh-negative woman from an Rh-positive man, the probability of having an Rh-positive child is 60%.
According to approximate data, about 15% of Europeans are Rh-negative. When pregnancy occurs in an Rh-negative woman from an Rh-positive man, the probability of having an Rh-positive child is 60%.
In this case, when fetal erythrocytes enter the mother's bloodstream, an immune reaction occurs, as a result of which fetal erythrocytes are damaged, anemia and a number of other serious complications occur.
During physiological pregnancy, fetal erythrocytes cross the placenta in the first trimester in 3% of women, in the second - in 15%, in the third - in 48%. In addition, massive casting occurs in childbirth, after termination of pregnancy (abortion, miscarriage, ectopic pregnancy, hydatidiform mole), invasive procedures (chorionic villus biopsy, amniocentesis), prenatal bleeding with a threat of termination of pregnancy.
The total risk of developing an Rh conflict in Rh-negative women pregnant with an Rh-positive fetus in the absence of prophylaxis is about 16%. In women who have undergone prophylaxis, this risk is reduced to 0.2%.
In women who have undergone prophylaxis, this risk is reduced to 0.2%.
And now the most interesting - what is this very prevention and what needs to be done to keep the situation under control.
All women who applied to a medical institution for pregnancy registration, as well as those who applied to terminate an unwanted pregnancy, are assigned an analysis to determine the blood type and Rh factor. Sexual partners of women who have a negative Rh are also recommended to undergo an examination to establish Rh-affiliation. If, by a happy coincidence, a man also has a negative Rh factor, then there is no risk of an Rh conflict and there is no point in conducting immunoprophylaxis.
Women with Rh-negative blood and Rh-positive partner's blood who wish to terminate an unwanted pregnancy are advised to give an injection of anti-Rh immunoglobulin within 72 hours after the termination. The mechanism of action of this drug is based on the fact that the injected antibodies bind the fetal erythrocytes that have entered the maternal bloodstream and prevent the development of an immune response.
Rh-negative women registered for pregnancy are prescribed a monthly blood test for anti-Rh antibodies. Thus, it is determined whether there was contact between the blood of the mother and the fetus, and whether the woman's immune system reacted to a foreign protein.
If by the 28th week there are no anti-Rh antibodies in the woman's blood, she is sent for prophylactic administration of anti-Rh immunoglobulin. This prophylaxis is carried out from 28 to 30 weeks of pregnancy. After that, the determination of anti-Rhesus antibodies in the mother's blood is not carried out.
If, according to the results of the examination, anti-Rhesus antibodies are detected in a woman before 28 weeks of pregnancy, she is sent for an in-depth examination to determine the severity of the Rh conflict, timely treatment and, if necessary, emergency delivery.
After the birth of an Rh-negative woman, the Rh factor is determined. And, if the baby is Rh-positive, within 72 hours after birth, the woman is also injected with anti-Rh immunoglobulin.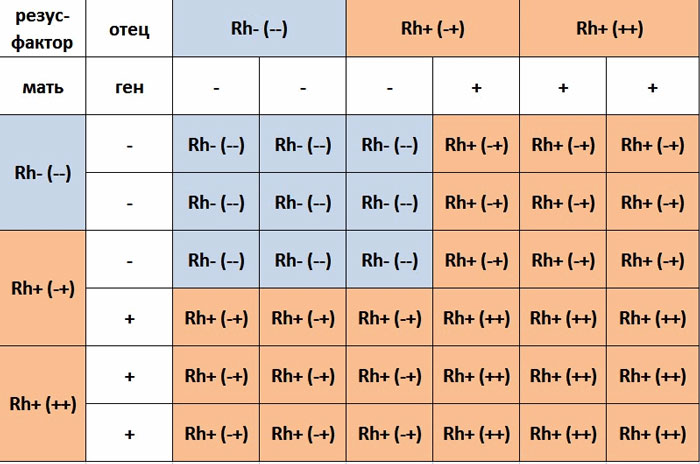
Other situations requiring prophylactic administration of anti-Rhesus immunoglobulin:
- miscarriage or non-progressive pregnancy;
- ectopic pregnancy;
- hydatidiform mole;
- prenatal bleeding with threatened miscarriage;
- invasive intrauterine interventions during pregnancy.
The only controversial issue at the moment is the determination of the Rh factor of the fetus during pregnancy. To do this, starting from the 10th week of pregnancy, a woman’s blood is taken, the genetic material of the fetus is isolated from it, and on the basis of a genetic study, the Rh affiliation of the unborn child is determined.
On the one hand, this study would allow 40% of Rh-negative women carrying an Rh-negative fetus to avoid monthly testing of anti-Rh antibodies and the introduction of anti-Rh immunoglobulin.
On the other hand, this research does not appear in the official order of the Ministry of Health, is not included in the CHI system and is carried out only on a paid basis.
Thus, at the moment, a clear algorithm has been developed for the management of pregnant women with Rh-negative blood. And following this simple algorithm will allow a woman to give birth to one, two or more healthy babies.
Obstetrician-gynecologist
antenatal clinic No. 14
Khivrich E.B.
Pregnancy and Rh conflict. | Tete-a-Tete Medical Center
Every young woman should know her blood type and Rh factor. According to statistics, 15% of people lack the Rh factor - they are called Rh-negative. The remaining 85% who have it are called Rh-positive.
Rh factor is an immunological property of the blood, which depends on the presence of a special type of protein. Because, whether it is on the surface of red blood cells or not, and it will depend on the Rh blood - positive or negative. Rh affiliation is determined simultaneously with the blood group. Although they are completely independent. It is inherited as a stronger trait and never changes throughout life. The Rh-affiliation of the blood cannot speak of any health, immune or metabolic disorders. It's just a genetic trait, an individual trait, like eye or skin color.
It is inherited as a stronger trait and never changes throughout life. The Rh-affiliation of the blood cannot speak of any health, immune or metabolic disorders. It's just a genetic trait, an individual trait, like eye or skin color.
When does Rh conflict occur?
A "positive" mother has no Rh-conflict with the fetus under any circumstances, and the father's Rh does not matter in this case. But if the pregnant woman’s blood turns out to be Rh-negative, the blood group and Rh-affiliation of her husband are also established. If the mother and father of the future baby have a negative Rh, there is nothing to worry about. The baby will also be born Rh-negative. In this case, there simply cannot be any conflicts! But if the parents' Rh is positive, the baby in the vast majority of cases will have a Rh factor protein in the blood (as already mentioned, it is transmitted as a stronger sign). Rh conflict can occur during pregnancy if the mother's Rh factor does not match the Rh factor of the fetus. In the case when the carrier of a positive Rh factor is a baby, the likelihood of an Rh conflict is much higher, and its consequences are much more serious. In addition to the Rh factor, a conflict may develop if the blood of the future mother and child are incompatible in group. Group incompatibility develops if the mother has the first blood group - 0 (I), and the child has the second A (II) or the third B (III).
In the case when the carrier of a positive Rh factor is a baby, the likelihood of an Rh conflict is much higher, and its consequences are much more serious. In addition to the Rh factor, a conflict may develop if the blood of the future mother and child are incompatible in group. Group incompatibility develops if the mother has the first blood group - 0 (I), and the child has the second A (II) or the third B (III).
In most cases, the first pregnancy of a woman with Rh-negative blood - a fetus with Rh-positive blood is normal, however, even with a second similar pregnancy, the likelihood of a Rh conflict increases sharply. At the same time, it is of no small importance how your previous pregnancy ended, which arose with the risk of Rh conflict.
The formation of antibodies usually occurs:
- in 3-4% of cases after a miscarriage
- in 5-6% after an abortion
- in 1% of cases after an ectopic pregnancy
- in 10-15% after normal delivery
The risk of developing antibodies is also increased if you had a caesarean section or if placental abruption occurred. From all this it follows that the risk depends on how many fetal red blood cells enter the mother's blood.
From all this it follows that the risk depends on how many fetal red blood cells enter the mother's blood.
What is the essence of the conflict? The Rh factor of the fetus crosses the placental barrier and enters the mother's blood. Her body, perceiving the fetus as something alien, produces protective antibodies.
The antibodies that the mother produces are completely harmless to her, but in the fetus it causes the destruction of its red blood cells. If all the necessary measures are not taken, this can threaten the unborn child with very serious deviations. A child may be born icteric, mentally handicapped, with damage to the brain and central nervous system.
In these cases, an exchange transfusion can help the baby. Doctors inject him with Rh-negative single-group blood and carry out resuscitation. This operation must be carried out within 36 hours after the birth of the baby.
So, as soon as you are planning a baby, take a blood test to determine the Rh factor.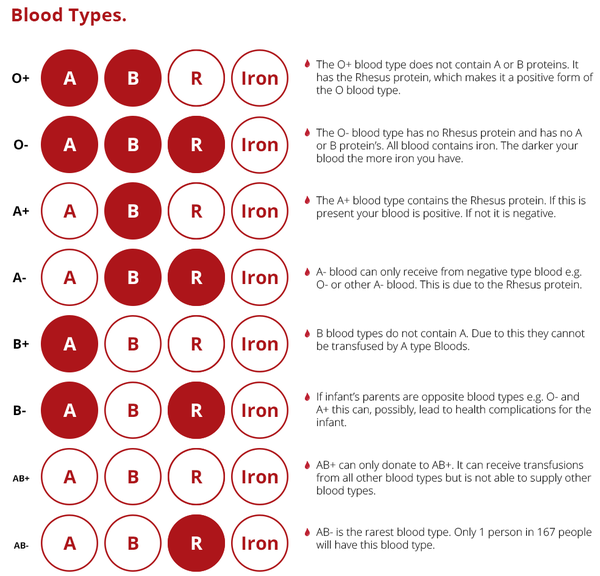 And this should be done not only by you, but also by your partner. The incompatibility of partners for the Rh factor is not a reason for frustration or abandoning the dream of a child. Just do not forget about the most careful and regular monitoring of your health. Such a pregnancy requires a much more responsible and attentive attitude. Try to find a competent specialist whom you completely trust, and clearly follow all his recommendations.
And this should be done not only by you, but also by your partner. The incompatibility of partners for the Rh factor is not a reason for frustration or abandoning the dream of a child. Just do not forget about the most careful and regular monitoring of your health. Such a pregnancy requires a much more responsible and attentive attitude. Try to find a competent specialist whom you completely trust, and clearly follow all his recommendations.
An expectant mother with a negative Rh factor will have to donate blood from a vein quite often for the presence of antibodies. Up to thirty-two weeks of pregnancy, this analysis is carried out once a month, from 32 to 35 weeks - twice a month, and then until childbirth weekly. This procedure, of course, is not the most pleasant, but absolutely necessary. According to the level of antibodies in the blood of a pregnant woman, the doctor can draw conclusions about the alleged Rh factor in the child and determine the beginning of the Rh conflict.![]()
Correct treatment or preventive measures can only be prescribed by a qualified specialist.
In case of a critical increase in the antibody titer, the expectant mother must be hospitalized in a specialized perinatal center, where the condition of the mother and baby will be constantly monitored. Doctors will track:
- The dynamics of the antibody titer in the blood of the expectant mother;
- Ultrasound data: an increase in the size of the fetal liver, thickening of the placenta, the appearance of polyhydramnios and fluid in the pericardium and abdominal cavity of the fetus;
- Data from amniocentesis (test of amniotic fluid) or cordocentesis (test of cord blood).
If antibodies are not detected in the blood of the future mother, at the 28th week of pregnancy, the doctor may recommend the prophylactic administration of anti-Rh immunoglobulin, which is a kind of "Rh-inoculation" - it binds the baby's red blood cells that have entered the mother's blood and thus prevents an immune response (formation antibodies).