Breastfeeding with long nipples
Nipple shape and breastfeeding – Lactation Clinic
Did you know that one of the biggest concerns or obstacles to the successful breastfeeding can be the shape of your nipples? You may have heard about a “misfortune” if one is born with flat or inverted nipples. I’ll try to bring some positivity and sense to this complicated issue.
To latch on and start their breastfeeding journey your newborn needs your breast more than your nipple. They are already born with some reserve calories and fluid resources for those few first days while their main goal is to learn how to latch onto the breast no matter what shape and size of the nipples. First milk (colostrum) is already there and those drops should be enough for your baby to stay hydrated and nourished while learning how to latch. Every healthy and term newborn should be given a chance to perform a so called breast crawl towards the breast, finding the breast and latching onto it with little to no assistance. Usually this is enough for them to get the right idea and to become a competent “latcher”. At this point your baby really does not care if your nipples are small, flat, or inverted.
Here is nice illustration by Jim Cooke, showing how many shapes of nipple are out there. One is missing, though: when there’s no nipple at all, only few openings on a completely flat areola. In my experience I have attended to such a patient and we were still able to figure it out so she could exclusively breastfeed her sweet baby!
If you’re still in the colostrum stage, i.e. your milk has not came in yet, your breast should be soft and “modifiable” in a way your baby needs it in order to have a deep latch. Some major concerns at this point could be: too long nipples or too wide nipples, or too long & too wide at the same time nipples.
Too long nipples can trick you and your healthcare professional into thinking as if the baby is having a great latch, when in reality, baby is staying only on the nipple, doing so called ‘nipple-feeding’ instead of breastfeeding. In such case your nipples quickly become very sore and you don’t see actual baby’s drinking at the breast. You can try to fold your nipple by pressing with your thumb at the base of your nipple, and releasing it the second prior baby is almost done with latching onto your breast.
In such case your nipples quickly become very sore and you don’t see actual baby’s drinking at the breast. You can try to fold your nipple by pressing with your thumb at the base of your nipple, and releasing it the second prior baby is almost done with latching onto your breast.
Too wide nipples could become real obstacle for small babies. Each baby has a very limited space in their mouth, so in case of a tiny baby and a very wide nipple it could be a problem to have enough room in their mouth for your nipple and your breast tissue. Again, try your best in “folding” your still soft breast together with your nipple and maybe this will be enough!
Too long and too wide nipples do exist as well. You’re lucky if your baby is big and can achieve a truly deep latch. Make sure there’s no nipple-feeding happening and you don’t feel any discomfort like sore nipples. Multiple “folding” and shaping can do the trick. Try all possible variations of this, you might find one working for you!
Flat nipples are the least problematic. They get longer when you have a good latch and baby starts to suckle – this is how suction affects them. Just make sure your breast is soft enough so your baby could latch onto it. In other words: flat nipples are as good as normal nipples and you’re lucky if you have them.
They get longer when you have a good latch and baby starts to suckle – this is how suction affects them. Just make sure your breast is soft enough so your baby could latch onto it. In other words: flat nipples are as good as normal nipples and you’re lucky if you have them.
Inverted nipples are one of the biggest challenges for everyone. From my private practice experience I can conclude that mothers have their best chance to have an exclusive breastfeeding just by using bare breast if they reach out for a Lactation Consultant help during the first 24-28 hours postpartum. During this short period, the breast is at its softest and most elastic condition, so one can really shape it as needed, and the baby is not yet used to the silicon shape and texture in their mouth. This is the time when you really must know how to latch a baby onto any possible breast. It requires years of practice and a very specialized training to perform this procedure successfully, and not to avert the baby from the breast. Our team of Lactation Consultants is constantly learning something new from the best professionals in our field, so we could help you in your particular situation. By the way, if by any chance you are not pregnant and not breastfeeding, do yourself a favour and find a trusted Osteopath or a Chiropractor and try to resolve this issue with their help beforehand. We are dealing with some constriction here and gentle bodywork could really help you!
Our team of Lactation Consultants is constantly learning something new from the best professionals in our field, so we could help you in your particular situation. By the way, if by any chance you are not pregnant and not breastfeeding, do yourself a favour and find a trusted Osteopath or a Chiropractor and try to resolve this issue with their help beforehand. We are dealing with some constriction here and gentle bodywork could really help you!
If you have no idea how to do the above mentioned nipple ‘folding’ and breast shaping, our team can help! Sometimes, babies are born with a very sensitive gag reflex and in such case they actually start gagging. An actual deep latch, along with the long nipple, can trigger the gag reflex, or they have no room in their mouth enough to latch onto without damaging the nipple and causing the pain. If this is your case, despite anything you’ve already tried, just start milk expressing to keep your milk supply and use finger-feeding for few days and then try again. Your baby is growing bigger with every passing day, and they will really outgrow this situation! Skilled Osteopath or Chiropractor can help to resolve this problem faster.
Your baby is growing bigger with every passing day, and they will really outgrow this situation! Skilled Osteopath or Chiropractor can help to resolve this problem faster.
What about nipple shields? We can state that we do not judge moms using them, and, moreover, we do not undermine them saying that in such case there’s no breastfeeding happening. It’s happening. You’re still using your breasts and your milk to feed your baby. And we are certain it was not the first thing you’ve grabbed after your baby was born. And our guess is you’d still like to wean from it ASAP! Because it’s an additional burden of your new reality. We are ready to help you! We look at the nipple shield as one of the possible tools at your disposal, and, usually, only as temporary stepping stone on the road to an easier breastfeeding. There are few things to remember when using nipple shields:
- nipple shields do not convert breast to the bottle, i.e. baby still has to latch onto the breast, not only the nipple;
- make sure you use it correctly;
- make sure your baby is actually drinking while using it.

If you did not achieve a good latch prior to your milk coming in, and suddenly you have found yourself in the situation when your breasts are swollen and engorged (sometimes, to a very severe extent), your nipples are already sore and your baby cannot latch and get the milk out – try to resolve your engorgement, express the milk, feed the baby using one of the alternative methods, in other words – it’s about time to call an expert.
Breastfeeding with Large Nipples
Latching Issues • Jan 20, 2021
Have you ever wondered whether big nipples and breastfeeding can ever go hand-in-hand?
If you have very big nipples, and breastfeeding is something you will surely do, it might be better for you to be well-prepared.
Babies are born with the instinct to feed. However, for women with very large nipples, it might be a bit difficult to get the baby to latch on and feed. Instead of a pleasant experience, you might end up with sore nipples from breastfeeding.
Most of the time, a mother's nipples will not be big enough to cause problems while breastfeeding...
So, what are the most common questions about large nipples new mothers have? Let’s look at some of them:
• What are the ways for women with large nipples to breastfeed?
• How to deal with sore nipples from breastfeeding?
• What to do if the infant refuses to drink from your large breasts and nipples?
Big Nipples and Breastfeeding Guidelines
So, what is the right way to do it, even if you think your extremely large nipples will make it all the more challenging? Your baby has nature’s gift of knowing how to feed unless your baby has sucking problems, which could make things a little more complicated.
• Hold your breast with a U hold (thumb or forefinger on top of the breast and other fingers under your breast, as in the picture). Try not to touch the areola (the dark part around your nipple). This works exceptionally well for women with heavy breasts and large puffy nipples.
• Lying down while breastfeeding can also sometimes help. Many mothers with large nipples say that they breastfeed the best while using a football hold position or lying down position.
• If you have large nipples and sore nipples are an additional woe, express some milk the moment your baby has finished feeding. Gently spread this milk all over the areola and nipple. You will find that cracked nipples get immediate relief after breastfeeding.
• Sore nipples due to breastfeeding can be remedied best with a pure lanolin cream.
• For women with very large nipples or large, long nipples, it often helps to squish the nipple down, making it easy for the baby to latch on.
• If all else fails, some mothers have found that using a nipple shield can help a baby latch on easier.
• For those mothers who want to stop breastfeeding, you can continue to give your baby breast milk by pumping exclusively.
• More information about breastfeeding with large breasts.
Most importantly, for women with big nipples and breastfeeding issues, patience and knowledge are always the best answer. Get your facts in place, seek advice from experienced women, and you might just be headed for a beautiful breastfeeding experience!
- Latching Issues
- Sore Nipples
Subscribe to our newsletter
Get the latest posts delivered right to your inbox.
Your email address
Now check your inbox and click the link to confirm your subscription.
Please enter a valid email address
Oops! There was an error sending the email, please try later.
Breastfeeding with pierced, flat or inverted nipples
The shape and size of nipples can vary greatly from woman to woman. Our practical tips will help you make breastfeeding easier, no matter what your nipples are.
Our practical tips will help you make breastfeeding easier, no matter what your nipples are.
Share this information
Most women's nipples protrude, enlarge and swell when touched, but some have flat or even inward nipples. In addition, some women pierce one or both nipples. Usually flat, inverted or pierced nipples do not cause problems when breastfeeding, but in some cases additional help may be needed.
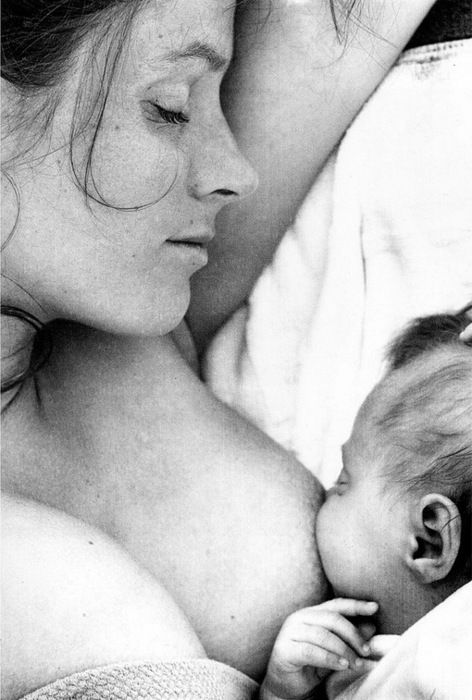
“Don't panic if you have flat or inverted nipples. As a rule, this does not interfere with breastfeeding in any way,” says Shawnad Hilton, a lactation consultant, health visitor and newborn care specialist who has worked with Medela in the UK for more than a decade. “Remember that your baby takes into his mouth not only the nipple, but also part of the breast.”
However, in the early days, when the baby's mouth is still very small and suckling skills have not developed, inverted or flat nipples can make feeding difficult, especially if the baby is unwell or born prematurely.
“Flat or inverted nipples may not reach the baby's palate and therefore not trigger the sucking reflex,” Schoned explains. “That is, the baby may have trouble grasping and holding the breast in the mouth, and the baby will not get enough milk.”
How to tell if you have flat or inverted nipples
Flat nipples 1 do not protrude much from the areola (the darker
area surrounding the nipple) even when stimulated.
Inverted nipples seem to be recessed in the center. They may look like this all the time or only if they are stimulated. Sometimes inverted nipples are on the same level with the areola, and sometimes even sink deep into the breast tissue.
This feature may occur on one or both nipples. It is estimated that approximately 10% of nulliparous women have at least one retracted nipple. 2 If you're not sure what type of nipples you have, try a simple pinch test: Gently squeeze your breast with your thumb and forefinger on both sides of the areola. The nipple should come forward. If your nipple hides inside, creating a depression, then it is retracted.
The nipple should come forward. If your nipple hides inside, creating a depression, then it is retracted.
Preparing inverted and flat nipples during pregnancy
You may have noticed that during pregnancy your breasts have changed and your nipples have become more protruding. If this does not happen and you are worried that the shape of your nipples will make breastfeeding difficult, try using nipple formers* in consultation with your doctor. These are soft and flexible silicone discs that are discreetly placed in the bra and slightly squeeze the nipples, helping to pull them out.
“In a normal pregnancy, nipple formers can be worn from 32 weeks,” advises Schoned. - Start wearing them for an hour a day, gradually increasing the time to eight hours. If you have an incompetent (weakened) cervix or are at risk of preterm labor, check with your healthcare provider about when you can start using shapers, as nipple stimulation can trigger contractions.”
“Nipple formers can continue to be worn after childbirth,” adds Schoned. “Try to put them in a bra 30 to 60 minutes before feeding.”
“Try to put them in a bra 30 to 60 minutes before feeding.”
“I have inverted nipples, and after two or three weeks of constantly trying to latch on, I almost switched to formula,” recalls Nina, a mother from Germany. “I turned to La Leche Liga for help, and one nice woman came to me and supported me to continue to feed. She suggested trying nipple shapers and they really helped me. Somehow my baby began to understand what to do! Breastfeeding went well and I nursed him until he was 21 months old.”
How to help your baby latch on to flat or inverted nipples
If your baby enjoys sucking on your thumb but isn't as interested in your breast, chances are your nipple isn't reaching the palate. The baby may become nervous, push off the breast and cry or even fall asleep on your chest. If this happens, ask a lactation consultant or healthcare professional to check the grip.
There are several tricks you can use before every feed to make your nipples more comfortable to latch on to. Schoned recommends the following:
Schoned recommends the following:
- twist the nipple between thumb and forefinger so that it protrudes better;
- place fingers in a "V" or "C" shape and squeeze the breast just behind the areola to push out the nipple;
- apply a cold compress or ice cube to the nipple to push it forward;
- Express milk manually or with a breast pump for a couple of minutes before feeding so that the nipple comes out more.
“I had a flat nipple, but I only found out about it when I noticed Austin was having trouble suckling on that side,” says Jennifer, mother of two in the UK. “From an anatomical point of view, there is nothing abnormal in this, it’s just that my nipple does not protrude so much, and this requires some skill when feeding. Before giving this breast, I always pinched and squeezed the nipple a little and tried to put it into the baby's mouth. It was a little difficult at first, but over time I learned.”
Using nursing pads
If none of the above work and your baby still has difficulty latch-on, your lactation consultant or healthcare professional may recommend that you breastfeed with a nursing pad*. They are thin and flexible nipple-shaped silicone funnels with holes at the tip through which milk will flow.
They are thin and flexible nipple-shaped silicone funnels with holes at the tip through which milk will flow.
It is easier for the baby to put the feeding pad in his mouth, as it is larger and more rigid. In addition, such an overlay will reach him to the sky, causing a sucking reflex. Do not use nursing pads for a long time. If you experience pain or other problems, contact your lactation consultant or healthcare professional to check that your baby is latching on properly with a breastfeeding pad. You will also need to monitor your baby's weight gain to ensure that milk production is meeting his needs. 3
Over time, as your baby learns to suckle properly and your nipples get used to breastfeeding, you will be able to breastfeed without breast pads.
“My nipples are rather flat. The doctor advised me nursing pads, and I was successfully able to feed my two babies,” says Ann-Sophie, mother of two from Sweden. “My secret is to make them adhere better to the skin, I lightly wet the edges before use. ”
”
Breastfeeding with pierced nipples
Many women with pierced nipples find it does not affect their ability to breastfeed. However, jewelry must be removed before feeding, as the child may choke on them or injure their tongue, gums or palate.
“I had a nipple piercing, but I got it off a year later when I got pregnant because my breasts were very sensitive,” says Kelly, mother of three from the UK. “I breastfed my daughter exclusively, and then her two younger brothers, and never had any problems. And the pierced nipple was my favorite!”
Some women report that milk can leak from piercings, while others believe that piercing scars reduce milk production 4 - but this has not been well researched.
“You can't predict how a piercing will affect breastfeeding until milk production begins,” Schoned explains. - If you are concerned, talk to a lactation consultant or healthcare professional. And remember that one breast may be enough for babies to get the nutrition they need if there are problems with the second. ”
”
What to do if you can't breastfeed with flat or inverted nipples
If you've tried all the options and still can't breastfeed, you still shouldn't deprive your baby of breastmilk.
“Mom and baby's health is the most important thing,” says Schoned. “Maybe you should switch to full pumping and feed your baby only expressed milk. You can also try the supplementary feeding system** where the baby continues to feed at the breast while receiving additional expressed milk through a tube. That is, the baby will still suck on the breast and stimulate the production of milk, which, in turn, will help you pump even more.
“I have inverted nipples. After the disastrous experience of breastfeeding my first son with my second, I decided to get my way after all,” says Babettli, mother-of-two from Italy. - On the advice of experts, I tried nipple formers and nursing pads, but everything was unsuccessful. In the end, pumping with the Medela Symphony*** Double Electronic Clinical Breast Pump proved to be the best solution for us. I fed exclusively on expressed milk for up to four months.”
I fed exclusively on expressed milk for up to four months.”
Care for different types of nipples
Flat or inverted nipples may require extra care as the baby may squeeze them harder and they may become inflamed at first. Tips on how to care for sore nipples can be found in Nursing Nipple Care.
If your nipples become inverted after a feed, any moisture can lead to inflammation and increase the risk of infections, including thrush. Blot your nipples dry after each feed before they have time to hide inside.
With swelling of the mammary glands, when even protruding nipples can become flat, flat or inverted nipples can be difficult. Read the helpful tips in the article on breast swelling.
The good news is that continuous breastfeeding or pumping can change the shape of your nipples and breastfeeding will become easier over time. With the arrival of the next child, you may not have to face this problem at all, as happened with Leanne, a mother of two from the UK.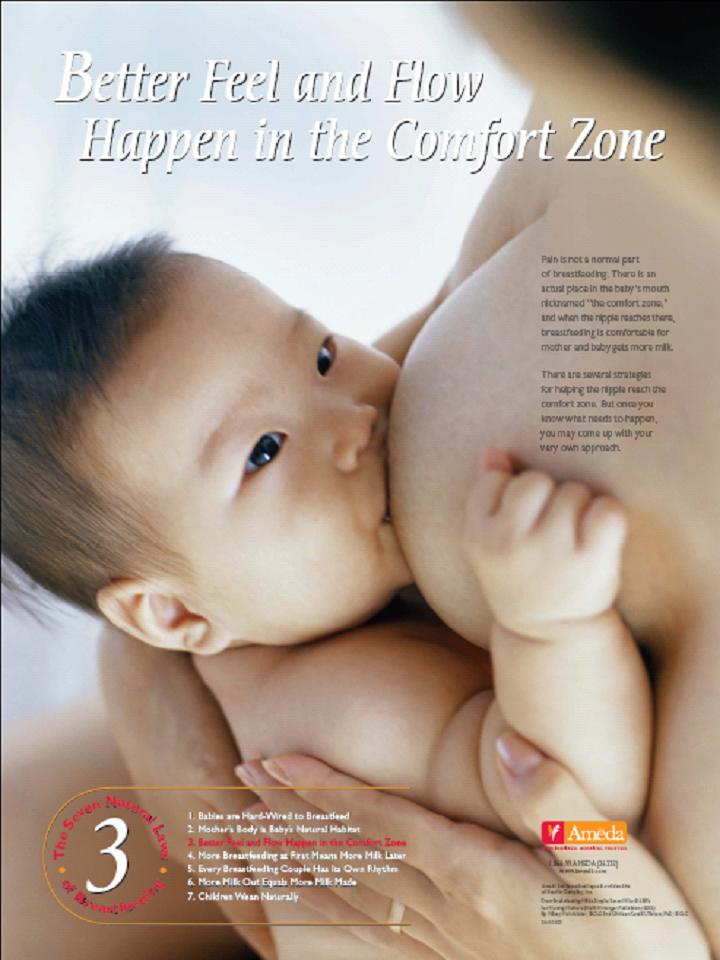
“The second feeding was like a fairy tale,” she says. “After almost four months of pumping for my first son, my flat nipples were so extended that with my second son I no longer had to use breast pads - he was able to suck directly from the breast. The youngest is now nine months old and I still breastfeed him.”
Literature
1 Pluchinotta AM. The Outpatient Breast Clinic. Springer International Publishing ; 2015. - Pluchinotta A.M., "Treatment of breast diseases on an outpatient basis". Springer International Publishing. 2015.
2 Alexander JM, Campbell MJ. Prevalence of inverted and non-protractile nipples in antenatal women who intend to breast-feed. The Breast . 1997;6(2):72-78. — Alexander JM, Campbell MJ, "Prevalence of inverted and intractable nipples in pregnant women who intend to breastfeed." Ze Brest (Chest). 1997;6(2):72-78.
3 McKechnie AC, Eglash A. Nipple shields: a review of the literature.Breastfeeding Medicine. 2010;5(6):309-314. — McKechnie A.S., Eglash A., "Nipple Covers: A Review of the Literature". Brestfeeding Medicine (Breastfeeding Medicine). 2010;5(6):309-314.
Nipple shields: a review of the literature.Breastfeeding Medicine. 2010;5(6):309-314. — McKechnie A.S., Eglash A., "Nipple Covers: A Review of the Literature". Brestfeeding Medicine (Breastfeeding Medicine). 2010;5(6):309-314.
4 Garbin CP0106 , Rowan MK , Hartmann PE , Geddes DT . Association of nipple piercing with abnormal milk production and breastfeeding. JAMA, Journal of the American Medical Association. 2009;301(24):2550-2551. - Garbin S.P., Deacon J.P., Rowan M.C., Hartmann P.I., Geddes D.T., "Nipple piercing and its impact on abnormal milk production and breastfeeding", JAMA (Journal of the American medical association). 2009;301(24):2550-2551.
Read instructions before use. Consult a specialist about possible contraindications.

* RC No. FSZ 2010/07352 dated 07/19/10
** RC No. FSZ 2010/07353 dated 07/19/10
*** RC No. FSZ 2010/06525 dated 17/03/2003 9002 Various feeding positions breastfeeding
Try different breastfeeding positions to find the one that works best for you and your baby. You can see the options in our selection of photos
Share this information
There is no right or wrong way to hold the baby while feeding
, and mom and baby are sure to find their favorite position.
It is important that both you and your child feel comfortable. 1.2 It's good to learn a few different breastfeeding positions and techniques because life's circumstances often require us to be flexible, especially as your baby gets older and you start to leave the house more often.
Whatever position you choose to breastfeed your baby, remember a few simple rules.
- Prepare everything you need before feeding, including drinks, food, mobile phone, TV remote control, book or magazine.
 And do not forget to go to the toilet - the feeding process can take a long time!
And do not forget to go to the toilet - the feeding process can take a long time! - Make sure your baby is comfortable. Whichever position you choose, it's important to keep your baby strong, level, and provide good support for their head, neck, and spine.
- You should also be comfortable. Don't stress. If necessary, use pillows of different sizes or rolls of towels to support your back or arms.
- Make sure your baby is latching on correctly. Proper grip is the key to comfort when breastfeeding.
- If your baby does not latch on well or you experience pain while feeding, contact a lactation consultant for help. The specialist will also be able to show you how to hold your baby more comfortably.
1. Relaxed feeding or reclining position
The relaxed feeding position, also known as biological feeding, 1 is often the first position for most mothers. If, immediately after birth, the baby is placed on the mother’s chest or stomach, normally, he instinctively reaches for the breast and tries to grab the nipple. This phenomenon is known as the breast seeking reflex. Skin-to-skin contact stimulates the infant's feeding instinct, and gravity helps him to latch onto the breast and maintain balance.
This phenomenon is known as the breast seeking reflex. Skin-to-skin contact stimulates the infant's feeding instinct, and gravity helps him to latch onto the breast and maintain balance.
But it's not just newborns that can be fed in the reclining position - this position is great for babies of all ages. It can be especially helpful if your baby does not latch well in other positions or does not like to be touched during feeding, and also if you have too much milk flow or too large breasts. Isabelle, a mother from the UK, shares her experience: “I had large breasts, and the baby was born small - 2.7 kg, so it was not easy to find a comfortable position at first. After a few weeks, it became clear that there was no “correct” posture for me. As a result, I most often fed lying down, putting the baby on my chest. ”
It is more convenient to feed not lying flat on your back, but half-sitting, leaning on pillows. So you will have a back support and you will be able to watch the baby during feeding.
2. Cradle position
This is the classic
first thought of breastfeeding. Mom sits
straight, and the baby lies on her side on her arm, pressing her stomach against her stomach. 3 Although this is a very popular position, it is not always easy to master with newborns because it gives the baby less support. Try putting a pillow under your back, and put a special breastfeeding pillow on your knees and lean on it with your hands. So you can more reliably support the child, without overstraining your back and shoulders. Just make sure that the baby does not lie too high on the pillow for feeding. The breast should remain at a natural level so that the baby can grab it without effort, otherwise sore nipples cannot be avoided.
“I breastfed in the cradle position because it suited me perfectly! It was comfortable and I loved just sitting and looking at my little one,” recalls Rachel, a mother of two from Italy.
3. Cross Cradle
This breastfeeding position looks almost the same as the Cradle, but the baby is on the other arm. 3 This gives your baby support around the neck and shoulders so he can tilt his head to latch on. This position is great for breastfeeding newborns and small babies, as well as for babies who do not latch well. Since the baby lies completely on the other hand, it becomes easier to control his position and you can adjust the chest with your free hand.
3 This gives your baby support around the neck and shoulders so he can tilt his head to latch on. This position is great for breastfeeding newborns and small babies, as well as for babies who do not latch well. Since the baby lies completely on the other hand, it becomes easier to control his position and you can adjust the chest with your free hand.
Julie, a UK mother of two, finds this position very practical: “I usually breastfeed my youngest in the cross cradle position. So I have a free second hand, and I can take care of an older baby at the same time. ”
Do not hold the baby's head at first, otherwise you may inadvertently press his chin against his chest. Because of this, the child will not be able to take the breast deeply, because the nipple will rest against the base of the tongue, and not against the palate, which will lead to inflammation of the nipples. As the child grows, this position becomes more comfortable, and he can rest his head on your palm (as shown in the photo above).
4. Underarm breastfeeding
In this position, also known as the "ball grip", the mother sits and the baby lies along her arm at the side, legs towards the back of the chair (or any other seat). 3 Another comfortable position for newborn breastfeeding, you can give your baby good support, full control of the position and a good view of his face. And the baby feels safe in close contact with the mother's body. This position is especially good for those who have had a caesarean section or a premature birth, as well as mothers of twins and women with large breasts.
“When I breastfed my first daughter, I had very large K-sized breasts—twice the size of her head,” recalls Amy, an Australian mother of two. - I put rolls of towels under each breast, because they were very heavy, and fed my daughter in a pose from under the arm, but only sitting straighter so as not to crush her. This position was also convenient because I had a caesarean section and could not put the baby on my stomach.
5. Side-lying position
The side-lying position is ideal for relaxed
feeding at night in bed or on the couch. If you had a
caesarean section or ruptures during childbirth, this position may be more comfortable than sitting down. 3 In this position, mother and baby lie side by side, tummy to tummy.
“It was difficult for me to sit during endless night feedings, firstly because of the caesarean section, and secondly because of lack of sleep,” recalls Francesca, a mother from the UK. “And then I discovered that you can feed your baby lying on your side and rest at the same time.”
“Because of the short tongue frenulum, Maisie could only properly latch on to her breasts while lying on her side. The lactation consultant showed me how it's done. In this position, the flow of milk was optimal for my daughter, and it was easier for her to keep the nipple in her mouth. As she got older, she became much better at grabbing her breasts in normal positions,” says Sarah, mother of two from Australia.
6. Relaxed breastfeeding after caesarean section
If you can't find a comfortable position for breastfeeding after caesarean section, 3 try to hold the baby on the shoulder while reclining — this does not put pressure on the postoperative suture and allows you to breastfeed the baby comfortably. You can also try side feeding.
7. Sitting upright breastfeeding or “koala pose”
When breastfeeding in an upright position or “koala pose”, the baby sits with a straight back and a raised head on the mother's hip. 4 This position can be tried even with a newborn if it is well supported, but it is especially convenient for feeding an older child who can already sit up by himself. The upright sitting position, or “koala pose,” is great for toddlers who suffer from reflux or ear infections and feel better sitting. In addition, this pose may be suitable for children with a shortened frenulum of the tongue or reduced muscle tone.
“When my daughter got a little older, I would often feed her in an upright position, which was more comfortable for both of us, and I could still hold her close,” recalls Peggy, a mother from Switzerland. “Besides, it was possible to discreetly breastfeed her in public places.”
“Besides, it was possible to discreetly breastfeed her in public places.”
8. Overhanging position
In this position, the baby lies on his back, and the mother bends over him
on all fours so that the nipple falls directly into his mouth. 4 According to some mothers, this breastfeeding position is good to use from time to time for mastitis, when touching the breast is especially unpleasant. Some say that this breastfeeding position helps with blockage of the milk ducts, although there is no scientific evidence for this yet. You can also feed in the “overhanging” position while sitting, kneeling over the baby on a bed or sofa, as well as reclining on your stomach with support on your elbows. Pillows of various sizes that you can lean on will help you avoid back and shoulder strain.
“I have breastfed several times in the 'overhang' position for clogged milk ducts when no other means of dissolving the blockage worked. And this pose seems to have helped. I think it's because of gravity, and also because the breasts were at a completely different angle than with normal feeding, and my daughter sucked her differently, ”says Ellie, a mother of two from the UK.
I think it's because of gravity, and also because the breasts were at a completely different angle than with normal feeding, and my daughter sucked her differently, ”says Ellie, a mother of two from the UK.
Feeding in the "overhanging" position is unlikely to be practiced regularly, but in some cases this position may be useful.
“I used to breastfeed in the overhang position when my baby was having trouble latch-on,” says Lorna, mother of two in the UK. - This, of course, is not the most convenient way, but then I was ready for anything, if only he could capture the chest. We succeeded and have been breastfeeding for eight months now!”
9. Feeding a baby in a sling or "on the fly"
Breastfeeding in a sling takes some practice, but it can be used to go out of the house, look after older children or even do a little household chores.
The sling is also useful if the baby does not like to lie down or is often attached to the breast. Lindsey, a mother of two in the US, notes: “I used the carrier frequently for both of my children. When we were out, I tied the sarong around my neck and covered the carrier with it. Under such a cape, the baby can eat as much as he wants until he falls asleep.
When we were out, I tied the sarong around my neck and covered the carrier with it. Under such a cape, the baby can eat as much as he wants until he falls asleep.
This breastfeeding position is best when the baby is already good at breastfeeding and can hold his head up by himself. Any slings are suitable for breastfeeding, including elastic and rings, as well as carrying bags. Whatever option you choose, the main thing is that you can always see the face of the child, and his chin does not rest against his chest.
10. Double hand-held breastfeeding
Double hand-held breastfeeding (or “double-ball gripping”) is great for mothers of twins—you can breastfeed both at the same time while keeping your arms relatively free. 4 When feeding in this position, it is advisable to use a special pillow for breastfeeding twins, especially at first. It will provide extra support and help keep both babies in the correct position, as well as reduce the burden on the abdomen if you had a caesarean section. In addition, the hands are freer, and if necessary, you can deal with one child without interfering with the second.
In addition, the hands are freer, and if necessary, you can deal with one child without interfering with the second.
“My twins were born very tiny and had to be fed every two hours at any time of the day or night. Very soon it became clear: if I want to do anything besides feeding, I need to feed them both at the same time, - says Emma, mother of two children from the UK. “I breastfed them two by hand using a breastfeeding pillow.”
Other good positions for breastfeeding twins are two criss-cross cradles, one baby in the cradle and the other close at hand, reclining feeding, or sitting upright (one baby on one side, the other on the other).
11. Breastfeeding in the “with breast support” or “dancer's hand” position
muscle tone (which is typical for premature babies, children suffering from various diseases or Down syndrome), try supporting his head and your chest at the same time. 4 Grab your chest with your palm underneath so that your thumb is on one side and all the other fingers are on the other. Move your hand slightly forward so that your thumb and forefinger form a "U" just in front of your chest. With the other three fingers, continue to support the chest. With your thumb and forefinger, hold the baby's head while feeding so that his chin rests on the part of the palm between them, your thumb gently holds the baby on one cheek, and your index finger on the other. So the baby gets excellent support, and you can control his position and see if he is holding his breast.
Move your hand slightly forward so that your thumb and forefinger form a "U" just in front of your chest. With the other three fingers, continue to support the chest. With your thumb and forefinger, hold the baby's head while feeding so that his chin rests on the part of the palm between them, your thumb gently holds the baby on one cheek, and your index finger on the other. So the baby gets excellent support, and you can control his position and see if he is holding his breast.
Literature
1 Colson SD et al. Optimal positions for the release of primitive neonatal reflexes stimulating breastfeeding. Early Hum Dev . 2008;84(7):441-449. - Colson S.D. et al., "Optimal Positions for Provoking Primitive Innate Reflexes to Induce Breastfeeding." Early Hume Dev. 2008;84(7):441-449.
2 UNICEF UK BFHI [ Internet ].