Baby with severe jaundice
Infant jaundice - Symptoms and causes
Overview
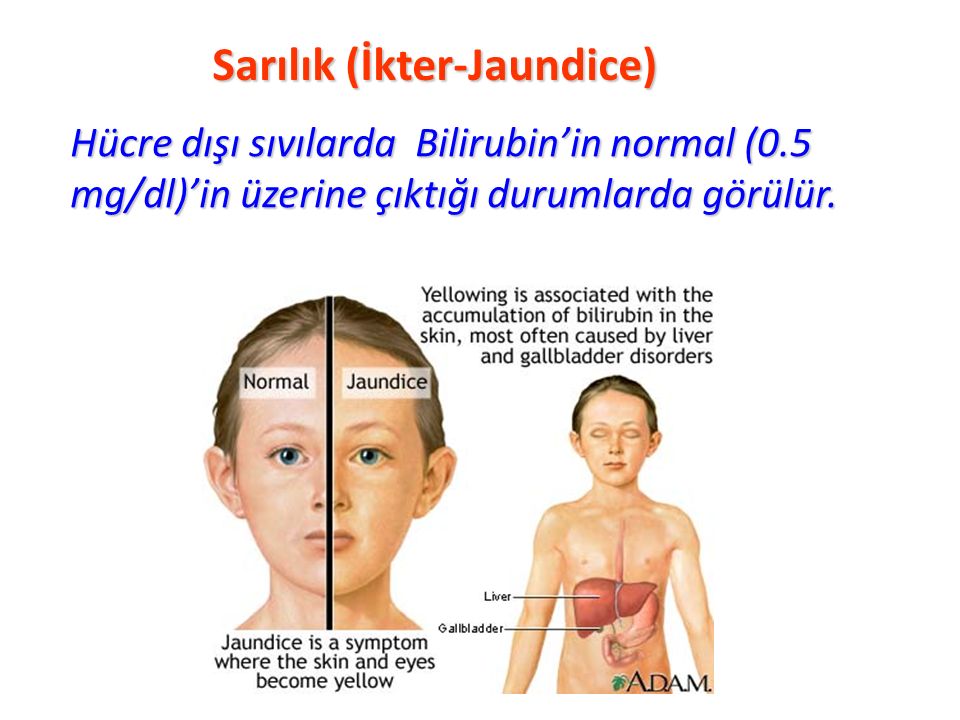
Infant jaundice is yellow discoloration of a newborn baby's skin and eyes. Infant jaundice occurs because the baby's blood contains an excess of bilirubin (bil-ih-ROO-bin), a yellow pigment of red blood cells.
Infant jaundice is a common condition, particularly in babies born before 38 weeks' gestation (preterm babies) and some breast-fed babies. Infant jaundice usually occurs because a baby's liver isn't mature enough to get rid of bilirubin in the bloodstream. In some babies, an underlying disease may cause infant jaundice.
Most infants born between 35 weeks' gestation and full term need no treatment for jaundice. Rarely, an unusually high blood level of bilirubin can place a newborn at risk of brain damage, particularly in the presence of certain risk factors for severe jaundice.
Products & Services
- Book: Mayo Clinic Family Health Book, 5th Edition
- Newsletter: Mayo Clinic Health Letter — Digital Edition
Symptoms
Yellowing of the skin and the whites of the eyes — the main sign of infant jaundice — usually appears between the second and fourth day after birth.
To check for infant jaundice, press gently on your baby's forehead or nose. If the skin looks yellow where you pressed, it's likely your baby has mild jaundice. If your baby doesn't have jaundice, the skin color should simply look slightly lighter than its normal color for a moment.
Examine your baby in good lighting conditions, preferably in natural daylight.
When to see a doctor
Most hospitals have a policy of examining babies for jaundice before discharge. The American Academy of Pediatrics recommends that newborns be examined for jaundice during routine medical checks and at least every eight to 12 hours while in the hospital.
Your baby should be examined for jaundice between the third and seventh day after birth, when bilirubin levels usually peak. If your baby is discharged earlier than 72 hours after birth, make a follow-up appointment to look for jaundice within two days of discharge.
The following signs or symptoms may indicate severe jaundice or complications from excess bilirubin. Call your doctor if:
Call your doctor if:
- Your baby's skin becomes more yellow
- The skin on your baby's the abdomen, arms or legs looks yellow
- The whites of your baby's eyes look yellow
- Your baby seems listless or sick or is difficult to awaken
- Your baby isn't gaining weight or is feeding poorly
- Your baby makes high-pitched cries
- Your baby develops any other signs or symptoms that concern you
Request an Appointment at Mayo Clinic
From Mayo Clinic to your inbox
Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health. Click here for an email preview.
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
Causes
Excess bilirubin (hyperbilirubinemia) is the main cause of jaundice. Bilirubin, which is responsible for the yellow color of jaundice, is a normal part of the pigment released from the breakdown of "used" red blood cells.
Newborns produce more bilirubin than adults do because of greater production and faster breakdown of red blood cells in the first few days of life. Normally, the liver filters bilirubin from the bloodstream and releases it into the intestinal tract. A newborn's immature liver often can't remove bilirubin quickly enough, causing an excess of bilirubin. Jaundice due to these normal newborn conditions is called physiologic jaundice, and it typically appears on the second or third day of life.
A newborn's immature liver often can't remove bilirubin quickly enough, causing an excess of bilirubin. Jaundice due to these normal newborn conditions is called physiologic jaundice, and it typically appears on the second or third day of life.
Other causes
An underlying disorder may cause infant jaundice. In these cases, jaundice often appears much earlier or much later than does the more common form of infant jaundice. Diseases or conditions that can cause jaundice include:
- Internal bleeding (hemorrhage)
- An infection in your baby's blood (sepsis)
- Other viral or bacterial infections
- An incompatibility between the mother's blood and the baby's blood
- A liver malfunction
- Biliary atresia, a condition in which the baby's bile ducts are blocked or scarred
- An enzyme deficiency
- An abnormality of your baby's red blood cells that causes them to break down rapidly
Risk factors
Major risk factors for jaundice, particularly severe jaundice that can cause complications, include:
- Premature birth.
 A baby born before 38 weeks of gestation may not be able to process bilirubin as quickly as full-term babies do. Premature babies also may feed less and have fewer bowel movements, resulting in less bilirubin eliminated through stool.
A baby born before 38 weeks of gestation may not be able to process bilirubin as quickly as full-term babies do. Premature babies also may feed less and have fewer bowel movements, resulting in less bilirubin eliminated through stool. - Significant bruising during birth. Newborns who become bruised during delivery gets bruises from the delivery may have higher levels of bilirubin from the breakdown of more red blood cells.
- Blood type. If the mother's blood type is different from her baby's, the baby may have received antibodies through the placenta that cause abnormally rapid breakdown of red blood cells.
- Breast-feeding. Breast-fed babies, particularly those who have difficulty nursing or getting enough nutrition from breast-feeding, are at higher risk of jaundice. Dehydration or a low caloric intake may contribute to the onset of jaundice. However, because of the benefits of breast-feeding, experts still recommend it.
 It's important to make sure your baby gets enough to eat and is adequately hydrated.
It's important to make sure your baby gets enough to eat and is adequately hydrated. - Race. Studies show that babies of East Asian ancestry have an increased risk of developing jaundice.
Complications
High levels of bilirubin that cause severe jaundice can result in serious complications if not treated.
Acute bilirubin encephalopathy
Bilirubin is toxic to cells of the brain. If a baby has severe jaundice, there's a risk of bilirubin passing into the brain, a condition called acute bilirubin encephalopathy. Prompt treatment may prevent significant lasting damage.
Signs of acute bilirubin encephalopathy in a baby with jaundice include:
- Listlessness
- Difficulty waking
- High-pitched crying
- Poor sucking or feeding
- Backward arching of the neck and body
- Fever
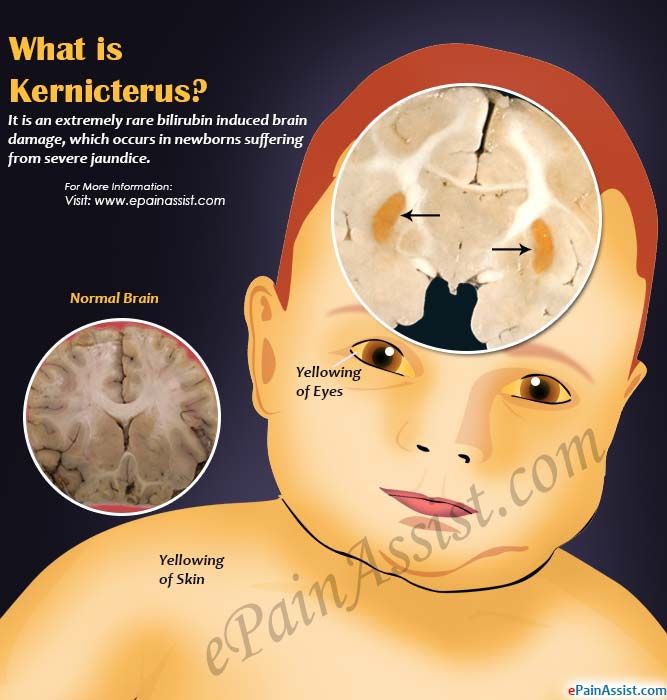
Kernicterus
Kernicterus is the syndrome that occurs if acute bilirubin encephalopathy causes permanent damage to the brain. Kernicterus may result in:
Kernicterus may result in:
- Involuntary and uncontrolled movements (athetoid cerebral palsy)
- Permanent upward gaze
- Hearing loss
- Improper development of tooth enamel
Prevention
The best preventive of infant jaundice is adequate feeding. Breast-fed infants should have eight to 12 feedings a day for the first several days of life. Formula-fed infants usually should have 1 to 2 ounces (about 30 to 60 milliliters) of formula every two to three hours for the first week.
By Mayo Clinic Staff
Related
Associated Procedures
Products & Services
What are Jaundice and Kernicterus?
Jaundice is the yellow color seen in the skin of many newborns. Jaundice happens when a chemical called bilirubin builds up in the baby’s blood. During pregnancy, the mother’s liver removes bilirubin for the baby, but after birth the baby’s liver must remove the bilirubin. In some babies, the liver might not be developed enough to efficiently get rid of bilirubin. When too much bilirubin builds up in a new baby’s body, the skin and whites of the eyes might look yellow. This yellow coloring is called jaundice.
When too much bilirubin builds up in a new baby’s body, the skin and whites of the eyes might look yellow. This yellow coloring is called jaundice.
When severe jaundice goes untreated for too long, it can cause a condition called kernicterus. Kernicterus is a type of brain damage that can result from high levels of bilirubin in a baby’s blood. It can cause athetoid cerebral palsy and hearing loss. Kernicterus also causes problems with vision and teeth and sometimes can cause intellectual disabilities. Early detection and management of jaundice can prevent kernicterus.
Signs and Symptoms
Jaundice usually appears first on the face and then moves to the chest, belly, arms, and legs as bilirubin levels get higher. The whites of the eyes can also look yellow. Jaundice can be harder to see in babies with darker skin color. The baby’s doctor or nurse can test how much bilirubin is in the baby’s blood.
See your baby’s doctor the same day if your baby:
- Is very yellow or orange (skin color changes start from the head and spread to the toes).
- Is hard to wake up or will not sleep at all.
- Is not breastfeeding or sucking from a bottle well.
- Is very fussy.
- Does not have enough wet or dirty diapers (at least 4-6 thoroughly wet diapers in 24 hours and 3 to 4 stools per day by the fourth day).
Get emergency medical help if your baby:
- Is crying inconsolably or with a high pitch.
- Is arched like a bow (the head or neck and heels are bent backward and the body forward).
- Has a stiff, limp, or floppy body.
- Has strange eye movements.
Diagnosis
At a minimum, babies should be checked for jaundice every 8 to 12 hours in the first 48 hours of life. It is important for your baby to be seen by a nurse or doctor when the baby is between 3 and 5 days old, because this is usually when a baby’s bilirubin level is highest. This is why, if your baby is discharged before age 72 hours, your baby should be seen within 2 days of discharge. The timing of this visit may vary depending on your baby’s age when released from the hospital and other factors.
The timing of this visit may vary depending on your baby’s age when released from the hospital and other factors.
A doctor or nurse may check the baby’s bilirubin using a light meter that is placed on the baby’s head. This results in a transcutaneous bilirubin (TcB) level. If it is high, a blood test will likely be ordered.
The best way to accurately measure bilirubin is with a small blood sample from the baby’s heel. This results in a total serum bilirubin (TSB) level. If the level is high, based upon the baby’s age in hours and other risk factors, treatment will likely follow. Repeat blood samples will also likely be taken to ensure that the TSB decreases with the prescribed treatment.
Treatment
No baby should develop brain damage from untreated jaundice.
When being treated for high bilirubin levels, the baby will be undressed and put under special lights. The lights will not hurt the baby. This can be done in the hospital or even at home. The baby’s milk intake may also need to be increased. In some cases, if the baby has very high bilirubin levels, the doctor will do a blood exchange transfusion. Jaundice is generally treated before brain damage is a concern.
In some cases, if the baby has very high bilirubin levels, the doctor will do a blood exchange transfusion. Jaundice is generally treated before brain damage is a concern.
Putting the baby in sunlight is not recommended as a safe way of treating jaundice.
Risk Factors
About 60% of all babies have jaundice. Some babies are more likely to have severe jaundice and higher bilirubin levels than others. Babies with any of the following risk factors need close monitoring and early jaundice management:
Preterm Babies
Babies born before 37 weeks, or 8.5 months, of pregnancy might have jaundice because their liver is not fully developed. The young liver might not be able to get rid of so much bilirubin.
Babies with Darker Skin Color
Jaundice may be missed or not recognized in a baby with darker skin color. Checking the gums and inner lips may detect jaundice. If there is any doubt, a bilirubin test should be done.
East Asian or Mediterranean Descent
A baby born to an East Asian or Mediterranean family is at a higher risk of becoming jaundiced. Also, some families inherit conditions (such as G6PD deficiency), and their babies are more likely to get jaundice.
Also, some families inherit conditions (such as G6PD deficiency), and their babies are more likely to get jaundice.
Feeding Difficulties
A baby who is not eating, wetting, or stooling well in the first few days of life is more likely to get jaundice.
Sibling with Jaundice
A baby with a sister or brother that had jaundice is more likely to develop jaundice.
Bruising
A baby with bruises at birth is more likely to get jaundice. A bruise forms when blood leaks out of a blood vessel and causes the skin to look black and blue. The healing of large bruises can cause high levels of bilirubin and your baby might get jaundice.
Blood Type
Women with an O blood type or Rh negative blood factor might have babies with higher bilirubin levels. A mother with Rh incompatibility should be given Rhogam.
- When severe jaundice goes untreated for too long, it can cause brain damage and a condition called kernicterus.
- Early diagnosis and treatment of jaundice can prevent kernicterus.
- If you’re concerned that your baby might have jaundice visit your baby’s doctor right away. Ask for a jaundice bilirubin test.
If You’re Concerned
If you think your baby has jaundice you should call and visit your baby’s doctor right away. Ask your baby’s doctor or nurse about a jaundice bilirubin test.
If your baby does have jaundice, it is important to take jaundice seriously and stick to the follow-up plan for appointments and recommended care.
Make sure your baby is getting enough to eat. The process of removing waste also removes bilirubin in your baby’s blood. If you are breastfeeding, you should nurse the baby at least 8 to 12 times a day for the first few days. This will help you make enough milk for the baby and will help keep the baby’s bilirubin level down. Support and advice for breastfeeding mothers may increase the chances of successful breastfeeding. If you are having trouble breastfeeding, ask your doctor, nurse, or a lactation coach for help.
Jaundice of newborns. What is Neonatal Jaundice?
IMPORTANT
The information in this section should not be used for self-diagnosis or self-treatment. In case of pain or other exacerbation of the disease, only the attending physician should prescribe diagnostic tests. For diagnosis and proper treatment, you should contact your doctor.
Neonatal jaundice is a physiological or pathological condition caused by hyperbilirubinemia and manifested by icteric staining of the skin and visible mucous membranes in children in the first days of their life. Jaundice of newborns is characterized by an increase in the concentration of bilirubin in the blood, anemia, icterus of the skin, mucous membranes and sclera of the eyes, hepato- and splenomegaly, in severe cases - bilirubin encephalopathy. Diagnosis of neonatal jaundice is based on a visual assessment of the degree of jaundice on the Cramer scale; determination of the level of erythrocytes, bilirubin, liver enzymes, blood groups of mother and child, etc.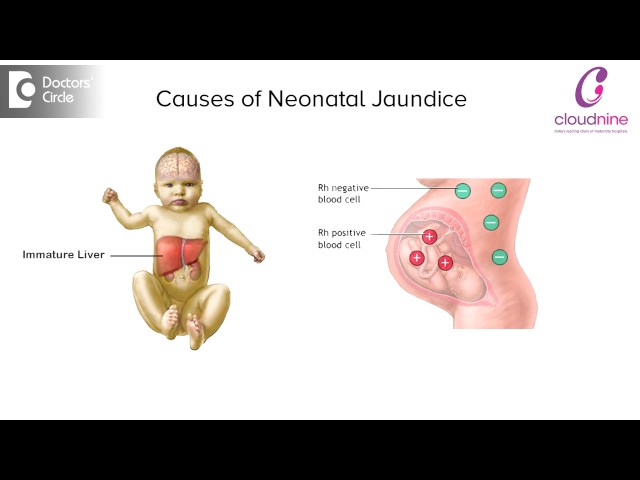 Treatment of jaundice in newborns includes breastfeeding, infusion therapy, phototherapy, exchange transfusion.
Treatment of jaundice in newborns includes breastfeeding, infusion therapy, phototherapy, exchange transfusion.
- Classification and causes of neonatal jaundice
- Symptoms of jaundice in newborns
- Physiological neonatal jaundice
- Hereditary jaundices
- Jaundice in endocrine pathology
- Jaundice in neonates with asphyxia and birth trauma
- Pregnane jaundice
- Kernic jaundice and bilirubin encephalopathy
- Diagnosis of neonatal jaundice
- Treatment of neonatal jaundice
- Prognosis of neonatal jaundice
- Prices for treatment
General
Neonatal jaundice is a neonatal syndrome characterized by a visible icteric coloration of the skin, sclera and mucous membranes due to an increase in the level of bilirubin in the child's blood. According to observations, in the first week of life, neonatal jaundice develops in 60% of full-term and 80% of premature babies. In pediatrics, physiological neonatal jaundice is the most common, accounting for 60–70% of all cases of the syndrome. Newborn jaundice develops when the level of bilirubin rises above 80-90 µmol/l in term infants and more than 120 µmol/l in preterm infants. Prolonged or severe hyperbilirubinemia has a neurotoxic effect, i.e. causes brain damage. The degree of toxic effects of bilirubin depends mainly on its concentration in the blood and the duration of hyperbilirubinemia.
In pediatrics, physiological neonatal jaundice is the most common, accounting for 60–70% of all cases of the syndrome. Newborn jaundice develops when the level of bilirubin rises above 80-90 µmol/l in term infants and more than 120 µmol/l in preterm infants. Prolonged or severe hyperbilirubinemia has a neurotoxic effect, i.e. causes brain damage. The degree of toxic effects of bilirubin depends mainly on its concentration in the blood and the duration of hyperbilirubinemia.
Newborn jaundice
Classification and causes of neonatal jaundice
First of all, neonatal jaundice can be physiological and pathological. By origin, jaundice in newborns is divided into hereditary and acquired. Based on laboratory criteria, i.e., an increase in one or another fraction of bilirubin, hyperbilirubinemia is distinguished with a predominance of direct (bound) bilirubin and hyperbilirubinemia with a predominance of indirect (unbound) bilirubin.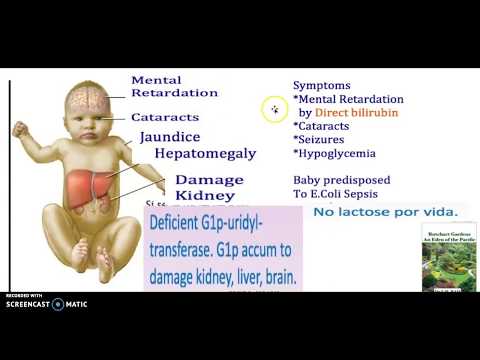
Conjugational jaundice in newborns includes cases of hyperbilirubinemia resulting from reduced clearance of bilirubin by hepatocytes:
- Physiological (transient) jaundice of full-term newborns
- Jaundice in premature newborns
- Hereditary jaundice associated with Gilbert syndrome, Crigler-Najjar type I and II, etc.
- Jaundice due to endocrine pathology (hypothyroidism in children, diabetes mellitus in the mother)
- Jaundice in newborns with asphyxia and birth trauma
- Pregnane jaundice in breastfed children
- Drug-induced jaundice of newborns due to the prescription of chloramphenicol, salicylates, sulfonamides, quinine, large doses of vitamin K, etc.
Hemolytic jaundice of newborns is characterized by an increase in the level of bilirubin due to increased destruction (hemolysis) of the child's red blood cells. These types of hyperbilirubinemia include:
- Hemolytic disease of the fetus and newborn
- Erythrocyte enzyme and membranopathies
- Hemoglobinopathy (sickle cell anemia, thalassemia)
- Polycythemia
Obstructive jaundice in newborns is caused by a violation of the removal of bilirubin with bile through the biliary tract and intestines. They can occur with defects (atresia, hypoplasia) of the intrahepatic and extrahepatic ducts, intrauterine cholelithiasis, compression of the bile ducts from the outside by an infiltrate or tumor, blockage of the bile ducts from the inside, bile thickening syndrome, pyloric stenosis, intestinal obstruction, etc.
They can occur with defects (atresia, hypoplasia) of the intrahepatic and extrahepatic ducts, intrauterine cholelithiasis, compression of the bile ducts from the outside by an infiltrate or tumor, blockage of the bile ducts from the inside, bile thickening syndrome, pyloric stenosis, intestinal obstruction, etc.
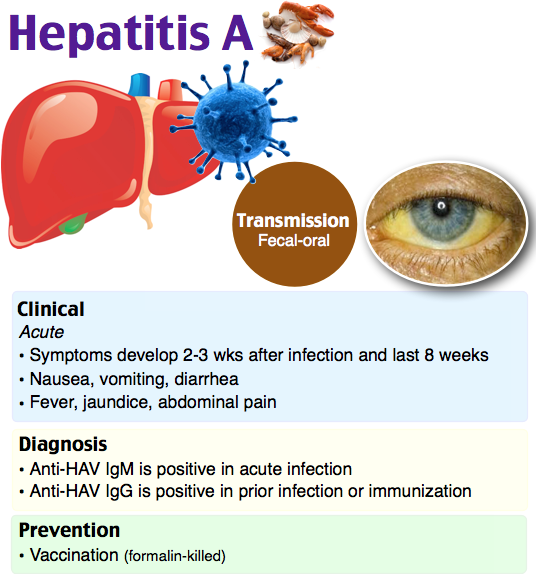
Jaundice of mixed origin (parenchymal) occurs in newborns with fetal hepatitis caused by intrauterine infections (toxoplasmosis, cytomegaly, listeriosis, herpes, viral hepatitis A, B, D), toxic-septic liver damage with sepsis, hereditary metabolic diseases (cystic fibrosis, galactosemia ).
Symptoms of neonatal jaundice
Physiological neonatal jaundice
Transient jaundice is a borderline condition of the neonatal period. Immediately after the birth of a child, excess red blood cells, in which fetal hemoglobin is present, is destroyed with the formation of free bilirubin. Due to the temporary immaturity of the liver enzyme glucuronyltransferase and intestinal sterility, the binding of free bilirubin and its excretion from the body of the newborn with feces and urine is reduced. This leads to the accumulation of excess bilirubin in the subcutaneous fat and staining of the skin and mucous membranes in yellow.
This leads to the accumulation of excess bilirubin in the subcutaneous fat and staining of the skin and mucous membranes in yellow.
Physiological jaundice of newborns develops 2-3 days after birth, reaches its maximum at 4-5 days. The peak concentration of indirect bilirubin averages 77-120 µmol/l; urine and feces are of normal color; the liver and spleen are not enlarged.
With transient jaundice of newborns, a mild degree of yellowness of the skin does not extend below the umbilical line and is detected only with sufficient natural light. With physiological jaundice, the health of the newborn is usually not disturbed, however, with significant hyperbilirubinemia, sluggish sucking, lethargy, drowsiness, and vomiting may be noted.
In healthy newborns, the occurrence of physiological jaundice is associated with a temporary immaturity of the liver enzyme systems, therefore it is not considered a pathological condition. When observing the child, organizing proper feeding and care, the manifestations of jaundice subside on their own by the age of 2 weeks.
When observing the child, organizing proper feeding and care, the manifestations of jaundice subside on their own by the age of 2 weeks.
Jaundice in premature newborns is characterized by an earlier onset (1–2 days), reaching a peak of manifestations by 7 days and subsiding by three weeks of a child's life. The concentration of indirect bilirubin in the blood of premature babies is higher (137-171 µmol/l), its increase and decrease is slower. Due to the longer maturation of liver enzyme systems in premature babies, there is a threat of developing nuclear jaundice and bilirubin intoxication.
Hereditary jaundice
The most common form of hereditary conjugative jaundice in newborns is constitutional hyperbilirubinemia (Gilbert's syndrome). This syndrome occurs in the population with a frequency of 2-6%; inherited in an autosomal dominant manner. Gilbert's syndrome is based on a defect in the activity of liver enzyme systems (glucuronyl transferase) and, as a result, a violation of the uptake of bilirubin by hepatocytes.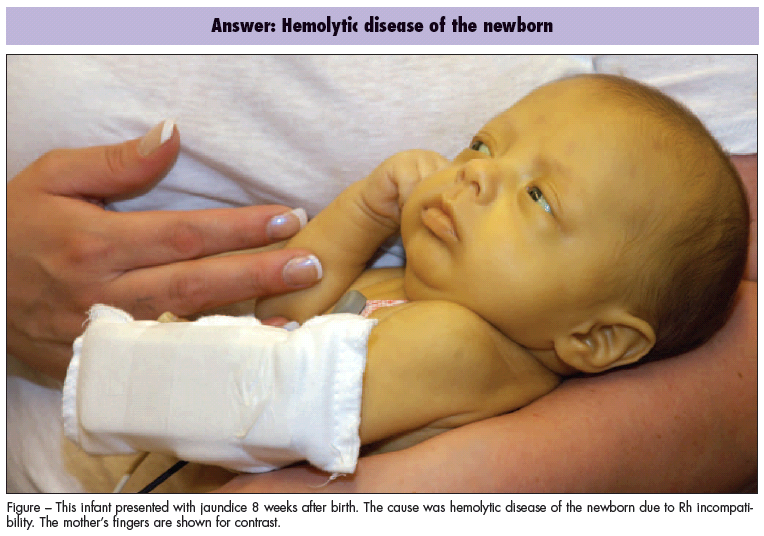 Jaundice of newborns with constitutional hyperbilirubinemia proceeds without anemia and splenomegaly, with a slight rise in indirect bilirubin.
Jaundice of newborns with constitutional hyperbilirubinemia proceeds without anemia and splenomegaly, with a slight rise in indirect bilirubin.
Hereditary neonatal jaundice in Crigler-Najjar syndrome is associated with very low activity of glucuronyl transferase (type II) or its absence (type I). In type I syndrome, neonatal jaundice develops already in the first days of life and steadily increases; hyperbilirubinemia reaches 428 µmol/l and above. The development of nuclear jaundice is typical, a fatal outcome is possible. Type II syndrome, as a rule, has a benign course: neonatal hyperbilirubinemia is 257-376 µmol/l; nuclear jaundice rarely develops.
Jaundice due to endocrine pathology
It usually occurs in children with congenital hypothyroidism due to a deficiency of thyroid hormones that disrupts the maturation of the glucuronosyltransferase enzyme, the processes of conjugation and excretion of bilirubin. Jaundice with hypothyroidism is detected in 50-70% of newborns; manifests itself on the 2-3rd day of life and lasts up to 3-5 months. In addition to jaundice, newborns have lethargy, pastosity, arterial hypotension, bradycardia, a rough voice, and constipation.
In addition to jaundice, newborns have lethargy, pastosity, arterial hypotension, bradycardia, a rough voice, and constipation.
Early jaundice can occur in newborns whose mothers have diabetes mellitus due to hypoglycemia and acidosis. It is manifested by a protracted icteric syndrome and indirect hyperbilirubinemia.
Jaundice in newborns with asphyxia and birth trauma
Fetal hypoxia and neonatal asphyxia delay the formation of enzyme systems, resulting in hyperbilirubinemia and kernicterus. Various birth injuries (cephalohematomas, intraventricular hemorrhages) can be sources of formation of indirect bilirubin and its increased penetration into the bloodstream with the development of icteric staining of the skin and mucous membranes. The severity of neonatal jaundice depends on the severity of the hypoxic-asphyxic syndrome and the level of hyperbilirubinemia.
Pregnane jaundice
Aries syndrome, or jaundice in breastfed babies, develops in 1-2% of newborns. It can occur in the first week of a child's life (early jaundice) or on days 7-14 (late neonatal jaundice) and persist for 4-6 weeks. Among the possible causes of pregnane jaundice in newborns are the presence in the milk of maternal estrogens that prevent the binding of bilirubin; unsteady lactation in the mother and relative malnutrition of the child, causing reabsorption of bilirubin in the intestine and its entry into the bloodstream, etc. It is believed that the risk factors for jaundice in newborns who are breastfed are later (after 12 hours of life) meconium discharge, delayed clamping umbilical cord, labor induction. The course of this type of neonatal jaundice is always benign.
It can occur in the first week of a child's life (early jaundice) or on days 7-14 (late neonatal jaundice) and persist for 4-6 weeks. Among the possible causes of pregnane jaundice in newborns are the presence in the milk of maternal estrogens that prevent the binding of bilirubin; unsteady lactation in the mother and relative malnutrition of the child, causing reabsorption of bilirubin in the intestine and its entry into the bloodstream, etc. It is believed that the risk factors for jaundice in newborns who are breastfed are later (after 12 hours of life) meconium discharge, delayed clamping umbilical cord, labor induction. The course of this type of neonatal jaundice is always benign.
Kernic jaundice and bilirubin encephalopathy
With a progressive increase in the concentration of indirect bilirubin in the blood, it can penetrate the blood-brain barrier and deposit in the basal nuclei of the brain (kernicterus of the newborn), causing the development of a dangerous condition - bilirubin encephalopathy.
At the first stage, the clinic is dominated by signs of bilirubin intoxication: lethargy, apathy, drowsiness of the child, monotonous cry, wandering eyes, regurgitation, vomiting. Soon, newborns develop classic signs of nuclear jaundice, accompanied by stiff neck, spasticity of the muscles of the body, periodic excitation, bulging of the large fontanel, extinction of sucking and other reflexes, nystagmus, bradycardia, convulsions. During this period, which lasts from several days to several weeks, irreversible damage to the central nervous system occurs. Over the next 2-3 months of life, a deceptive improvement is observed in the condition of children, however, already at 3-5 months of life, neurological complications are diagnosed: cerebral palsy, mental retardation, deafness, etc.
Diagnosis of neonatal jaundice
Jaundice is detected even at the stage of the child's stay in the maternity hospital by a neonatologist or pediatrician when visiting a newborn shortly after discharge.
The Kramer scale is used to visually assess the degree of neonatal jaundice.
- I degree - jaundice of the face and neck (bilirubin 80 µmol/l)
- II degree - jaundice extends to the level of the navel (bilirubin 150 µmol/l)
- III degree - jaundice extends to the level of the knees (bilirubin 200 µmol/l)
- IV degree - jaundice extends to the face, trunk, limbs, except for the palms and soles (bilirubin 300 µmol/l)
- V - total jaundice (bilirubin 400 µmol/l)
The necessary laboratory tests for the primary diagnosis of neonatal jaundice are: bilirubin and its fractions, complete blood count, blood group of the child and mother, Coombs test, PTI, urinalysis, liver tests. If hypothyroidism is suspected, it is necessary to determine the thyroid hormones T3, T4, TSH in the blood. Identification of intrauterine infections is carried out by ELISA and PCR.
As part of the diagnosis of mechanical jaundice, newborns undergo ultrasound of the liver and bile ducts, MR cholangiography, FGDS, plain radiography of the abdominal cavity, consultation of a pediatric surgeon and a pediatric gastroenterologist.
Treatment of neonatal jaundice
To prevent jaundice and reduce the degree of hyperbilirubinemia, all newborns need early onset (from the first hour of life) and regular breastfeeding. In newborns with neonatal jaundice, the frequency of recommended breastfeeding is 8–12 times a day without a night break. It is necessary to increase the daily volume of fluid by 10-20% compared with the physiological need of the child, the intake of enterosorbents. If oral hydration is impossible, infusion therapy is performed: glucose drip, physical. solution, ascorbic acid, cocarboxylase, vitamins of group B. In order to increase the conjugation of bilirubin, a newborn with jaundice may be prescribed phenobarbital.
The most effective treatment for indirect hyperbilirubinemia is continuous or intermittent phototherapy, which converts indirect bilirubin into a water-soluble form. Complications of phototherapy can be hyperthermia, dehydration, burns, allergic reactions.
With hemolytic jaundice of newborns, exchange transfusion, hemosorption, and plasmapheresis are indicated. All pathological neonatal jaundices require immediate treatment of the underlying disease.
Prognosis of neonatal jaundice
Transient jaundice in newborns in the vast majority of cases resolves without complications. However, a violation of the mechanisms of adaptation can lead to the transition of physiological jaundice of newborns into a pathological state. Observations and evidence base indicate that there is no relationship between hepatitis B vaccination and neonatal jaundice. Critical hyperbilirubinemia can lead to the development of kernicterus and its complications.
Children with pathological forms of neonatal jaundice are subject to dispensary observation of a district pediatrician and a pediatric neurologist.
Sources
- In case of pain or other exacerbation of the disease, only the attending physician should prescribe diagnostic tests.
 For diagnosis and proper treatment, you should contact your doctor.
For diagnosis and proper treatment, you should contact your doctor. Newborn jaundice: causes, treatment, consequences, prevention
Newborn jaundice is experienced by many parents. This is especially true for premature babies, but in babies who were born at term, this is also a common occurrence.
Jaundice develops in the first few days after the birth of the baby, and the change in skin color usually becomes noticeable on the 3rd-4th day, just when the mother and baby return home from the hospital.
Why does this happen and what is the difference between physiological neonatal jaundice, which does not require treatment, and dangerous pathological neonatal jaundice? We deal with doctors.
What you need to know about jaundice in newborns
Bilirubin is formed during the breakdown of red blood cells (blood cells that are responsible for transporting oxygen) throughout life and is excreted from the body without problems with the help of the liver.
 All body systems in a newborn do not work well enough, for example, the liver may not have enough enzymes to break it down and excrete it. Because of this, bilirubin accumulates in the blood, and the skin color becomes yellow. It happens that the whites of the eyes acquire the same shade.
All body systems in a newborn do not work well enough, for example, the liver may not have enough enzymes to break it down and excrete it. Because of this, bilirubin accumulates in the blood, and the skin color becomes yellow. It happens that the whites of the eyes acquire the same shade. Physiological jaundice differs from pathological jaundice in that the former does not require treatment and resolves on its own. This usually happens after the first month of a baby's life. But the pathological condition is important and needs to be tracked in time. It affects the general well-being, has negative consequences, but with a competent approach, it is treated by a pediatrician or neonatologist.
Physiological jaundice - a variant of the norm In the first days of life, many parents experience yellowing of the baby's skin. At the same time, nothing threatens the condition of children, and the shade of the skin is normalized after 7-10 days. The only thing that can overshadow the first days of a baby’s life is vomiting.  Occurs against the background of a bunch of bilirubin with albumin to prevent the toxic effects of the first (1). But such a phenomenon is rare.
Occurs against the background of a bunch of bilirubin with albumin to prevent the toxic effects of the first (1). But such a phenomenon is rare. There are several types of pathological jaundice Conjugative jaundice develops due to liver enzyme deficiency. Hemolytic jaundice is associated with a change in the structure of red blood cells. And the problem of obstructive jaundice is a violation of the outflow of bile. Things to pay attention to when treating jaundice (in addition to the general condition) The doctor first of all specifies whether the child has prematurity and other factors that can complicate the course of the disease, whether there is a hereditary predisposition to this disease. It is worth paying attention to the appetite of the baby, and his mother, the level of lactation is also important. There is a "bilirubin encephalopathy" In this condition, bilirubin enters the nervous system of the child due to the fact that there is not enough albumin to neutralize it.  The baby shows symptoms such as drowsiness, convulsions, and a weakened grasping reflex.
The baby shows symptoms such as drowsiness, convulsions, and a weakened grasping reflex. Jaundice is not contagious It cannot be transmitted through droplets. The cause of the disease is the increased breakdown of red blood cells and the insufficient functionality of the liver, which does not have time to process bilirubin secreted in large quantities. When phototherapy is used for jaundice At risk of hyperbilirubinemia, with physiological jaundice, if the baby's blood type is incompatible with the mother's blood type, if the bilirubin level rises above 5 µmol/l per hour. How long does jaundice last in newborns
The duration of jaundice in a newborn depends on the characteristics of the organism. Physiological jaundice usually reaches its maximum on the 3-4th day of the baby's life. Gradual fading begins on days 4-5, and on days 7-14, the child's body completely copes with this condition.

- Parents are not always able to reliably determine whether the baby's jaundice is normal or not. Therefore, this condition is given maximum attention by the medical staff (first in the maternity hospital, then on patronage), - explains Albina Yusupova, pediatric neonatologist Lahta Clinic . - Before discharge in the maternity hospital, doctors examine the child, determine the presence of jaundice, evaluate the skin color in dynamics, whether the yellowness of the skin / sclera increases or not. Often they resort to using a percutaneous method for measuring the level of bilirubin (it is he who gives such staining of the skin) or take blood for analysis. With high numbers, phototherapy is prescribed (a special lamp or mattress). There are no exact numbers for this, it depends on many factors: gestational age (term baby or not), the presence of cephalohematoma or bruising at birth, the color of feces / urine, whether there are concomitant pathologies or not, the blood type of the mother and child, how the mother eats and gains weight Baby.
In most cases, pathological jaundice develops on the first day of a newborn's life. The duration may vary depending on the reason why the child suffers from this disease: sometimes the treatment takes 2 months, and in complex cases where enhanced therapy is required, jaundice can last up to a month.
Higher bilirubin levels have been reported in breastfed neonates with large postpartum weight loss (≥8%), diabetic mothers, low gestational age, and drug induction of labor with oxytocin (2).
Causes of jaundice in newborns
Jaundice can appear in a baby for various reasons. Most often it is the accumulation of bilirubin in the blood. But there are other conditions that newborns face in the first weeks of life.
Bilirubin
Signs of pathology:
- deviations from the normal course of physiological jaundice (earlier or later appearance, prolonged persistence, undulating course),
- appearance of pallor or a greenish tinge of the skin,
- increase in the concentration of total bilirubin in the blood serum,
- relative increase in the level of the direct fraction of bilirubin (3).
Unlike physiological, pathological jaundice, as a rule, develops in the first hours after the baby is born. There may be dark urine and discoloration of feces, anemia, and pale skin. At the same time, the level of bilirubin is very high:
- above 256 µmol/l in children born at term,
- above 171 µmol/l in premature babies.
This condition is called hyperbilirubinemia. The most common cause of its development is hemolysis due to the incompatibility of the blood of the mother and child for erythrocyte antigens.
Other causes
“Pathological jaundice can be caused by several reasons,” says pediatrician Anna Levadnaya, Ph.D., author of the blog about pediatrics . - The most common is an increased breakdown of hemoglobin due to an Rhesus conflict or a blood type conflict between mother and child. Also, the cause of jaundice can be a pathology of the liver or a pathology of excretion of bile into the intestines.
In addition, jaundice can be a sign of an infection, hypothyroidism (due to a decrease in thyroid function), polycythemia (an increased level of red blood cells in the blood), intestinal obstruction, or pyloric stenosis (this is a congenital narrowing of the stomach before entering the intestines, which makes it difficult for food to pass through). into it). It can occur with certain medications and for other reasons.
Hepatic jaundice occurs when a child's liver is exposed to viruses or bacteria. It can also develop with hepatitis B and hepatitis C, blood sepsis. At this time, the liver and spleen increase in size, the baby's urine acquires a more pronounced color. Hepatic jaundice is treated comprehensively, primarily by acting on the cause.
Violation of the outflow of bile can cause obstructive jaundice. This happens when the patency of the bile ducts worsens due to malformations, underdevelopment, or the appearance of neoplasms. Here, all attention should be paid to the place where bile accumulates and the reason why it accumulates.
After all, it is because of her that the baby may show symptoms of jaundice.
Another cause is neonatal cholestasis. To confirm the diagnosis, it is necessary to make sure that the content of the direct fraction of bilirubin in the blood is more than 15-20% of the total level, an increase in the concentration of cholesterol, beta-lipoproteins, bile acids, as well as alkaline phosphatase and gamma-glutamyltransferase enzymes (3). This pathology occurs due to an increased level of bile acid synthesis, for which the newborn's liver is not ready. It happens that neonatal cholestasis occurs for reasons not related to the work of the liver. For example, against the background of hypoxia or the development of cardiovascular insufficiency.
There is also the so-called breastfeeding jaundice. There are studies that show that in healthy full-term infants who are bottle-fed, the level of bilirubin reaches a peak on the 5th day of life and becomes completely normal, on average, on the 13th day, while with natural feeding, two peaks of bilirubin rise are possible ( 3–5 and 10–15 days of life) with a gradual slow decrease (4).
Jaundice from breast milk (from which certain hormones that increase bilirubin levels enter the baby's body) can last up to 6 weeks.
If the doctor makes this diagnosis, he must exclude the presence of hyperbilirubinemia. Because breastfeeding jaundice cannot cause it. If, when HB is canceled for 1-2 days, bilirubin begins to decrease, and yellowness disappears, the diagnosis is confirmed. But with positive dynamics, the abolition of breastfeeding is not required: it is resumed after 1-2 days. During the pause, the mother must definitely express herself in order to maintain lactation at the required level.
Treatment of neonatal jaundice
Physiological neonatal jaundice, as we have already said, does not require treatment. Sometimes pediatricians recommend supplementing such children with water, but only if lactation is established and using a spoon, not a bottle.
As for the pathological jaundice of a newborn, it requires mandatory treatment, which is prescribed by a doctor.
The most effective treatment for this condition is phototherapy. For this, a special lamp with blue light is used: under the influence of ultraviolet radiation, bilirubin breaks down and is excreted from the body of the newborn with urine and feces. The intensity and duration of phototherapy depends on the baby's body weight at birth and the level of bilirubin, which is constantly monitored. As a rule, three-hour sessions under the lamp are prescribed with a break of 2-3 hours. The newborn must be undressed, but the eyes must be protected, the boys also have the genitals.
In severe cases of neonatal jaundice, when the life of the baby is at risk, a blood transfusion may be indicated.
Physicians have almost abandoned the use of drugs to treat neonatal jaundice. Some of them, for example, ascorbic acid and albumin, negatively affect the functioning of the nervous system, the effectiveness of allochol and B vitamins has not been proven, and Karsil and Essentiale have not been sufficiently tested specifically for newborns (3).
- It is important to note that most experts now agree that the appointment of sorbents, drugs such as phenobarbital, Essentiale, LIV-52, the abolition of breastfeeding, UV (ultraviolet blood enrichment), electrophoresis or excessive infusion therapy for jaundice is ineffective ( and it’s not safe for phenobarbital), says Anna Levadnaya.
Consequences of jaundice in newborns
Physiological jaundice in newborns, as we have already noted, goes away on its own and does not bear negative consequences for the health of the baby. But the consequences of pathological jaundice in a newborn can be extremely serious, especially if treatment is not started on time.
— Excessively high levels of bilirubin in the blood can lead to brain damage, — notes Anna Levadnaya. - As a rule, this occurs in children with hemolytic disease according to the Rh factor, with an increase in the level of bilirubin above 298-342 µmol/l. And the higher the level of bilirubin, the higher the risk of encephalopathy.
Prevention of jaundice in newborns
The best prevention of jaundice in newborns is a healthy lifestyle for mothers during pregnancy, giving up bad habits, good nutrition.
In addition, the expectant mother must be tested to detect Rh-negative blood factor. Children born to mothers with Rh-negative blood are at risk for jaundice. After the birth of such babies, they carefully examine and monitor the content of bilirubin in the blood, and also determine the blood group.
- Women who may have a child with hemolytic jaundice are treated already during pregnancy. They are injected with anti-rhesus gamma globulin, and at birth, the child is immediately clamped on the umbilical cord and tested for bilirubin. If there are indications according to the tests, then the child is immediately put on phototherapy, - adds neonatologist Nadezhda Shurtakova . - The mother of the baby can also influence the fact that the child does not have jaundice. She needs to feed the baby more on the first day, try to get milk so that the baby does not lose weight.
Jaundice often occurs with a large loss of initial weight. Bilirubin is a fat-soluble substance, and if the body of a newborn does not have enough fats, proteins and carbohydrates, then jaundice occurs at certain values of body weight loss.
Mother's milk is the best food for a newborn, it is easily digested, the intestines are stimulated faster, it is populated with beneficial microflora, the necessary enzymes are produced. All this helps the body of the newborn to cope with jaundice faster and more efficiently.
Frequently asked questions and answers
Nadezhda Shurtakova, neonatologist, head of the neonatal department at Maternity Hospital No. 4 (Moscow) answered frequently asked questions.
When is jaundice in newborns considered normal?
There are physiological and pathological jaundice. Physiological jaundice, which appears at the end of the second or third day of life, does not require treatment. Such jaundice is not pronounced and disappears on its own in 7-10 days.
Physiological jaundice is present in 80% of children. Such children are discharged home without any additional examinations and treatment.
In what case is the child placed under the lamp and how long does the child need to stay there?
The child is placed under a lamp, for phototherapy, with pathological jaundice. The duration of therapy depends on what causes it.
Hemolytic jaundice of the newborn due to the Rh factor may appear already in the prenatal period, the child may be born with it and need an exchange transfusion. Such children are laid out under the lamp immediately at birth.
Jaundice caused by AB0 incompatibility (blood group incompatibility) appears at the age of 1.5 days. It is necessary to look at a biochemical blood test, and if there are indications, also put the child on phototherapy.
There is also conjugative jaundice, it, like physiological, also appears on the third day, but with it the amount of bilirubin (yellow substance) in the blood is significantly increased.
Such children are also subject to phototherapy.
In different situations, phototherapy lasts from 1 to 4 days, usually 2-3 days, it is carried out under the control of biochemical and clinical blood tests. When the indicators are normal, the child is removed from phototherapy.
How long does it take to stay in the hospital if a newborn has jaundice?
Hemolytic jaundice lasts 5-7 days. We stabilize such children, wait for the end of the increase in bilirubin and then transfer them to another hospital. However, if treatment is started on time, the indicators return to normal faster, and the mother and child are already discharged from the hospital.
In case of conjugative jaundice, which may appear on the 4th day, after discharge from the maternity hospital, children are admitted to hospitals from the districts.
Sources
- E.I. Yulish. Jaundice syndrome in newborns: approaches to therapy // Health of the child.