Baby head soft
Baby Soft Spot: How to Care for Your Baby’s Head
As you spend hours gazing at your newborn and stroking his face, you’ll no doubt notice a couple of soft spots on his head. These soft spots, called fontanelles, are perfectly normal and actually play an important role in your baby’s development.
Learn more about these soft spots, including how to protect them, when the bones of the skull will harden, and which warning signs to look out for by reading on.
What Are Baby Soft Spots and Where Are They?
All babies are born with two soft spots (fontanelles) on their heads: The larger soft spot (anterior fontanelle) is toward the front of the head, and the smaller soft spot (posterior fontanelle) is toward the back.
These softer areas are made up of immature skull bones that are still forming and expanding as your baby’s brain grows.
Why Do Babies Have Soft Spots?
The soft spots on babies' heads have two main functions:
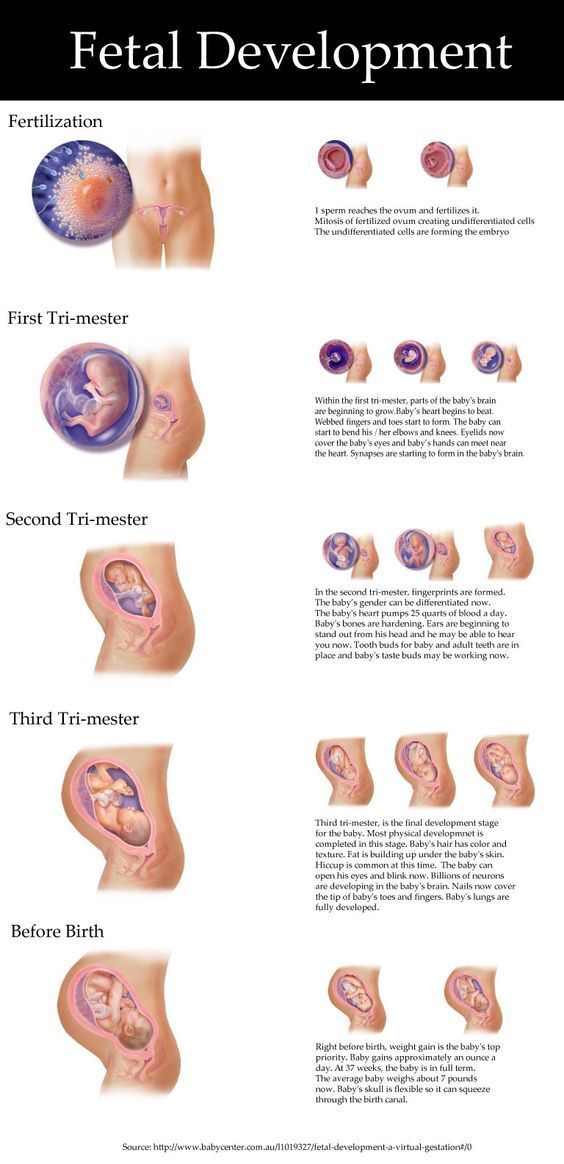
They make it possible for the bony plates of the skull to compress and overlap as the head passes through the narrow birth canal during a vaginal delivery
They allow a baby’s skull to expand, making room for the rapid brain growth that happens in the first year.
related baby tool
Keep an eye on your baby’s average growth by tracking height, weight, and head circumference with our simple tool.
Fill out your baby's details*:
What is your child*
Boy Girl
This is a mandatory field.
Age (between 0 and 24 months)
This is a mandatory field.
Weight (lbs.)
This is a mandatory field.
Height (in.)
This is a mandatory field.
Head circumference (in.)
This is a mandatory field.
*Input details of your baby’s last measurements. **Source: World Health Organization
When Does a Baby's Soft Spot Close or Go Away?
In your baby’s first few months, both soft spots should be open and flat. At about 2 to 3 months of age the soft spot at the back of your baby’s head may close. The soft spot at the front may close around the time your toddler turns 18 months old.
At about 2 to 3 months of age the soft spot at the back of your baby’s head may close. The soft spot at the front may close around the time your toddler turns 18 months old.
What Happens If You Touch the Soft Spot on Your Baby's Head?
As long as you touch your baby’s soft spots gently — for example, when you’re holding your baby and supporting his head and neck or when you’re washing your baby’s hair — you shouldn’t be afraid of hurting him.
There is a thick and durable membrane just under your baby’s scalp that protects her brain, so gently touching the fontanelles won’t hurt her.
To help ensure your baby’s head is protected, it’s a good idea to remind friends, family members, and caregivers to be careful and gentle with your baby’s head.
What Does It Mean When a Baby's Soft Spot Is Pulsating?
Sometimes it may appear that your baby’s soft spot is pulsating. This is completely normal — blood is pulsing through your baby’s body, and this movement can sometimes be visible where the soft spot is. There’s no need to worry if you see your baby’s soft spot pulsing.
This is completely normal — blood is pulsing through your baby’s body, and this movement can sometimes be visible where the soft spot is. There’s no need to worry if you see your baby’s soft spot pulsing.
What Causes a Sunken Soft Spot on Your Baby’s Head?
A sunken soft spot may be due to dehydration, which can happen if your baby does not get enough breast milk or formula. Your baby may also be more likely to be dehydrated if she has a fever, has been vomiting, or has diarrhea.
Beyond a sunken soft spot, these are some of the other signs of dehydration:
Fewer wet diapers
Sunken eyes
A dry mouth
Cool skin
Drowsiness
Irritability.
Contact your baby’s healthcare provider right away if you’re concerned your newborn may be dehydrated.
Keep in mind, a sunken soft spot can sometimes occur in babies who are not dehydrated. It’s safest for your baby’s healthcare provider to make a diagnosis.
It’s safest for your baby’s healthcare provider to make a diagnosis.
What Should You Do If Your Baby Hits His Soft Spot?
Contact your baby’s healthcare provider if your baby hits his soft spot.
If you notice swelling/bulging of the soft spot and/or bruising around her eyes or behind her ears, it may be due to a concussion. Call 911 immediately.
Other signs of a head injury or trauma requiring immediate medical attention include:
Nonstop crying
Your baby being unwilling to feed
Vomiting
Seizures
Discharge or blood from ears or nose
Difficulty waking after sleep.
When Should You Be Concerned About Your Baby's Soft Spot?
The lack of soft spots on your baby’s head may be a sign of very rare condition called craniosynostosis, a birth defect in which your baby’s skull bones fuse together earlier than normal, resulting in a misshapen head. Contact your baby’s healthcare provider if
Contact your baby’s healthcare provider if
your baby seems to lack soft spots
there are raised, firm edges where the skull plates meet
your baby’s skull shape seems misshapen and is not growing over time.
The Bottom Line
Although it might seem a little odd that your baby would have soft spots on her head, they actually serve two important purposes: to make it easier for your baby to pass through the birth canal during a vaginal delivery, and to ensure your baby’s skull can expand to make room for her growing brain.
By around 18 months, your baby’s fontanelles will have closed. In the meantime, be gentle with your baby’s head when holding her.
If your baby accidentally bumps or hits a soft spot, or if you’re concerned that one of the soft spots may be sunken or injured, contact your child’s healthcare provider right away.
When it comes to the shape of your little one’s head, if you’ve noticed flatter spots, it could be because your little one is spending too much time lying on his back looking the same way. Prolonged pressure on the softer skull bones can flatten out the area. Find out more about flat head syndrome and what you can do to treat or prevent it.
Prolonged pressure on the softer skull bones can flatten out the area. Find out more about flat head syndrome and what you can do to treat or prevent it.
About the fontanelle | Pregnancy Birth and Baby
About the fontanelle | Pregnancy Birth and Baby beginning of content5-minute read
Listen
What is a fontanelle?
A fontanelle is a ‘soft spot’ of a newborn baby’s skull. It is a unique feature that is important for the normal growth and development of your baby’s brain and skull. Your health team will check your baby’s fontanelles during routine visits.
If you touch the top of your baby’s head you can feel a soft spot in between the bones — this is a fontanelle.
A newborn baby’s skull is made up of sections of bone known as plates that are joined together by fibrous joints called sutures. The sutures provide some flexibility and allow your baby’s head to narrow slightly as it travels through the birth canal. The sutures also enable your baby’s head to grow in the first years of life.
The sutures provide some flexibility and allow your baby’s head to narrow slightly as it travels through the birth canal. The sutures also enable your baby’s head to grow in the first years of life.
There are 2 fontanelles on your baby’s skull. These are the skin-covered gaps where the skull plates meet. The anterior fontanelle is at the top of your baby’s head, and the posterior fontanelle is located at the back of your baby’s head.
Illustration showing the anterior and posterior (front and back) fontanelles of a baby's skull.When will my baby’s fontanelles close?
The posterior fontanelle usually closes by the time your baby is 2 months old. The anterior fontanelle can close any time between 4 and 26 months of age. Around 1 in every 2 babies will have a closed fontanelle by the time they are 14 months old.
Can I touch my baby’s fontanelles?
Yes, you can gently touch your baby’s fontanelles. If you run your fingers softly along your baby’s head you are can probably feel them. Your doctor will touch your baby’s fontanelles as part of their routine medical examination. There is no need to be concerned or worried about touching your baby’s fontanelles as long as you are gentle.
Your doctor will touch your baby’s fontanelles as part of their routine medical examination. There is no need to be concerned or worried about touching your baby’s fontanelles as long as you are gentle.
What does a normal fontanelle look like?
Your baby’s fontanelle should feel soft and flat. If you softly touch a fontanelle, you may at times feel a slight pulsation — this is normal. If a fontanelle changes, or feels different to how it usually does, show your doctor or midwife as it may be a sign that your baby’s health may need to be checked.
Sunken fontanelle
If you notice that your baby’s fontanelles are low or sunken, your baby may be dehydrated.
However, you may notice other signs of dehydration in your baby before their fontanelles becomes sunken.
Other signs of dehydration include:
- having fewer wet nappies
- not feeding well
- loosing fluids from vomiting or diarrhoea
- perspiration (or sweating) in very hot weather
- being less alert or floppy
Bulging fontanelle
A bulging or swollen fontanelle may be a sign of a number of serious but rare conditions including meningitis or encephalitis (infections in the brain), cerebral haemorrhage (bleeding in the brain), hydrocephalus, an abscess or another cause of increased pressure in the brain.
If you think that your baby’s fontanelles are bulging or sunken, seek medical advice immediately.
What if a fontanelle closes too soon?
Your baby’s fontanelles may close early. This can happen for several reasons. Your baby may have hyperthyroidism (high levels of the thyroid hormone) or hyperparathyroidism (high levels of parathyroid hormone). Another cause of early fontanelle closure is a condition known as craniosynostosis. Craniosynostosis occurs when one or more of the fibrous joints (sutures) between the bone plates in a baby’s skull fuse too early, before the brain has finished growing. As the brain continues to grow, it pushes on the skull from the inside but cannot expand into the closed over area. This causes the skull to have an unusual shape.
If you notice that your baby’s fontanelles seem to have closed early, if you can feel a ridge along your baby’s skull, or if you think that your baby’s head has an unusual shape, take your baby to see their GP or paediatrician.
What if a fontanelle doesn’t close?
Your baby’s fontanelles may not close on time for several reasons. Common reasons for delayed fontanelle closure include congenital hypothyroidism (low thyroid hormones from birth), Down syndrome, increased pressure inside the brain, rickets and familial macrocephaly (a genetic tendency to have a large head).
If one or both of your baby’s fontanelles haves not closed by the time they are 2 years old, speak to your GP or paediatrician.
If you have any concerns about your baby’s fontanelles you should make an appointment to see your child health nurse, GP or paediatrician.
Speak to a maternal child health nurse
Call Pregnancy, Birth and Baby to speak to a maternal child health nurse on 1800 882 436 or video call. Available 7am to midnight (AET), 7 days a week.
Sources:
Children’s Health Queensland Hospital and Health Service (Craniosynostosis), American Family Physician (The Abnormal Fontanel), Australian Family Physician (The 6 week check - An opportunity for continuity of care), WA Health (Bulging Anterior Fontanelle), The Royal Children's Hospital Melbourne (Clinical Practice Guidelines: Dehydration)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: February 2022
Back To Top
Related pages
- Regular health checks for babies
- Knowing your baby is well - podcast
- How to know when your baby is well - video
- How your baby’s brain develops
Need more information?
Newborn baby essentials
Find out some of the essentials for looking after your newborn. Find out when your baby will need to have health checkups and immunisations. There is also lots of information on nappies, giving your baby a bath and teeth development.
Read more on Pregnancy, Birth & Baby website
Colic in infants - MyDr.com.au
Colic is a pattern of unexplained, excessive crying in an otherwise healthy and well-fed baby and happens to 1 in 5 Australian babies.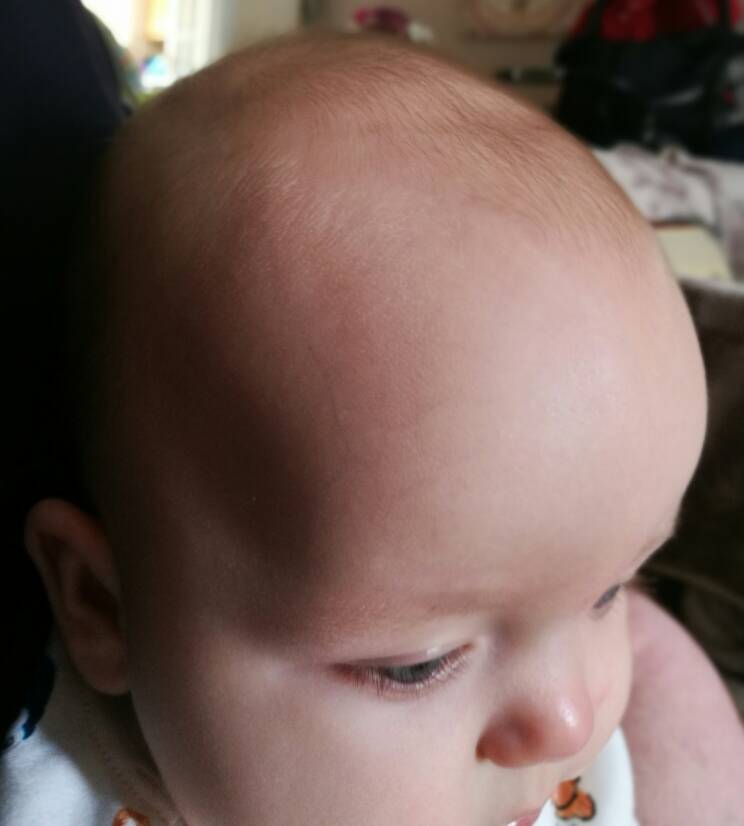
Read more on myDr website
Knowing your baby is well - podcast
Listen to Dianne Zalitis, midwife and Clinical Lead at Pregnancy, Birth and Baby, talk to Feed Play Love with Shevonne Hunt about signs your baby is well.
Read more on Pregnancy, Birth & Baby website
Common worries and fears for parents
New parents often worry that they don't know what to do. However, there are practical ways to deal with the challenges so you can enjoy your baby more.
Read more on Pregnancy, Birth & Baby website
Flattened head
Plagiocephaly (flattened or misshapen head) means an uneven or asymmetrical head shape. Plagiocephaly won't affect your baby's brain development but it should be treated.
Read more on Pregnancy, Birth & Baby website
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now entering.
OKNeed further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
Children's head injuries | Kaplan Medical Center
Head injuries are very common in children, but 60% of them are mild and do not cause any damage. In most cases, the infant or child will cry out of surprise from the pain resulting from the impact, but very soon the crying will stop and the child will continue to act normally. Thus, most cases do not require special treatment or any checks, other than the observation of parents at home.
Thus, most cases do not require special treatment or any checks, other than the observation of parents at home.
Is a hematoma (bruise) in the area of impact dangerous?
Bumps usually show no outward signs other than some redness or superficial abrasions. Sometimes a red-blue swelling may occur at the site of impact, which means subcutaneous hematoma in the area of impact. The occurrence of a hematoma is not surprising, because the scalp area is abundantly covered with blood vessels. Therefore, if an external injury occurs, the bleeding from it will be relatively large compared to similar injuries in other parts of the body, and the internal injury will be a subcutaneous hematoma.
How to treat a hematoma?
Attach something cold wrapped in cloth.
How to stop bleeding?
If there is external bleeding from the wound, apply pressure to the impact site with a piece of a stamp or other tissue.
When can you calm down and understand that we are talking about a slight bruise?
In the following cases, you can understand that this is a minor injury and that you can monitor the child at home:
- This refers to a fall from a small height (large height - more than a meter in infants under two years of age).
- Injury not the result of a traffic accident
- No significant penetrating injury
- Injury not the result of bullying (in any case of suspicion of intentional injury, fundus examination should be performed and reported to a social worker)
- No signs of loss of consciousness or seizures
- Child behaves normally again after a few minutes
- The child did not vomit more than twice after the injury
- The injury did not develop a prolonged or significant headache
When can a child be allowed to sleep after a head injury?
A child can sleep after a head injury, sleep will not hurt him. However, if it seems to parents that drowsiness is significantly increased, so much so that it is difficult to wake the child, you should go to the emergency room.
However, if it seems to parents that drowsiness is significantly increased, so much so that it is difficult to wake the child, you should go to the emergency room.
When should I arrive for an examination in the emergency room?
It is important to come to the emergency room in the following cases:
- The injury was serious or the fall was from a significant height (more than a meter), even if the child looks perfectly healthy
- The child suffers from severe prolonged headaches
- The child suffers from nausea / vomiting for a long time
- The child is restless or indifferent
- There is a cut at the site of the injury that requires sutures or gluing
- The injury occurred to an infant under the age of one year
Please note that there is a fee for visiting the emergency room.
How to recognize a concussion?
In more serious cases, signs of concussion may develop: persistent vomiting, significant dizziness without anatomical disturbances. A child who shows signs of a concussion will usually be hospitalized to monitor the progress of the problem. In most cases, after 24 hours of observation, the child will be discharged home.
A child who shows signs of a concussion will usually be hospitalized to monitor the progress of the problem. In most cases, after 24 hours of observation, the child will be discharged home.
How to make sure that there is no skull fracture?
In more severe cases, a skull fracture may occur. In most cases, we are talking about a "linear" fracture, that is, a crack. Diagnosis is by CT, in which case hospitalization is required for observation for several days to ensure that there are no signs of internal trauma.
When can a head injury be life-threatening?
Internal bleeding can be very dangerous and cause permanent damage or even death. The reason for this is the accumulation of blood in the intracranial box and its pressure on the soft tissues of the brain. Diagnosis of internal bleeding is done by CT of the brain. Bleeding inside the skull can be managed with emergency neurosurgery to drain blood and relieve pressure.
How to avoid such injuries?
It goes without saying that prevention is the most important thing. Falls from a bicycle, scooter or roller skates can be very dangerous if the child is not wearing a helmet. Therefore, it is very important to choose a helmet according to the size.
The head circumference of an adult is from 51 to 62 cm on average; in children from the age of 8 years, the head circumference reaches about 80 percent of its final size. On the packaging of the helmet, its girth in centimeters is indicated, as well as information about the size - small, medium, large.
When cycling, scootering or roller-skating, carefully fasten the helmet straps under the chin and turn your head to make sure that the helmet does not fall off. A helmet that is too large can be very dangerous and cause more damage in the event of an accident.
It is very important that the helmet be made of two types of material, or fused together, to make it resistant. A quality helmet will also be made of shock-absorbing material, such as whipped polyurethane, which is resistant in the event of a fall to protect the head. So even if the bottom layer splits during the first impact of a fall, the top layer of the helmet will hold it and protect it from the next blow. It is very important to purchase a helmet with a rear size adjuster, which will allow the helmet to fit more tightly on the skull. Of course, you should make sure that the helmet meets all the required standards.
A quality helmet will also be made of shock-absorbing material, such as whipped polyurethane, which is resistant in the event of a fall to protect the head. So even if the bottom layer splits during the first impact of a fall, the top layer of the helmet will hold it and protect it from the next blow. It is very important to purchase a helmet with a rear size adjuster, which will allow the helmet to fit more tightly on the skull. Of course, you should make sure that the helmet meets all the required standards.
We wish you well,
ICU staff
"For your information
Microcephaly
Microcephaly- Popular Topics
- Air pollution
- Coronavirus disease (COVID-19)
- Hepatitis
- Data and statistics »
- News bulletin
- The facts are clear
- Publications
- Find the country »
- A
- B
- B
- G
- D
- E
- YOU
- K
- and
- l
- L
- 900 N
- O
- P
- R
- S
- T
- U
- F
- x
- h
- Sh
- Sh.

- K.
- S
- B
- E
- S
- I
- WHO in countries »
- Reporting
- Regions »
- Africa
- America
- Southeast Asia
- Europe
- Eastern Mediterranean
- Western Pacific
- Media Center
- Press releases
- Statements
- Media messages
- Comments
- Reporting
- Online Q&A
- Developments
- Photo reports
- Questions and answers
- Latest information
- Emergencies "
- News "
- Disease Outbreak News
- WHO Data »
- Dashboards »
- COVID-19 Monitoring Dashboard
- Basic moments "
- About WHO »
- CEO
- About WHO
- WHO activities
- Where does WHO work?
- Governing Bodies »
- World Health Assembly
- Executive committee
- Main page/
- Media Center /
- Newsletters/
- Read more/
- Microcephaly
\n
Magnitude of the problem
\n
\nMicrocephaly is a rare condition. The prevalence of microcephaly is estimated to vary considerably due to different definitions and depending on target populations. Scientists are investigating a potential, though unproven, link between an increase in microcephaly cases and Zika virus infection.
The prevalence of microcephaly is estimated to vary considerably due to different definitions and depending on target populations. Scientists are investigating a potential, though unproven, link between an increase in microcephaly cases and Zika virus infection.
\n
Diagnosis
\n
\nMicrocephaly can sometimes be diagnosed by fetal ultrasound. The most appropriate period for diagnosis is the end of the second trimester (about 28 weeks) or the third trimester of pregnancy.
\n
\nChild circumference of newborns should be measured at least 24 hours after birth and compared with the WHO standard child development indicators. The results are interpreted taking into account the gestational age of the child, as well as his height and weight. If there is suspicion, the child is sent for examination to the pediatrician and for a brain scan, the circumference of his head is measured once a month in early infancy and compared with standard indicators. Doctors should also test for known causes of microcephaly.
Doctors should also test for known causes of microcephaly.
\n
Causes of microcephaly
\n
\nMicrocephaly has many potential causes, but often the cause remains unknown. The most common causes include:
\n
- \n
- intrauterine infections: toxoplasmosis (caused by a parasite found in meat that has not been properly cooked), rubella, herpes, syphilis, cytomegalovirus, and HIV; \n
- exposure to toxic chemicals: maternal exposure to heavy metals such as arsenic and mercury, alcohol, radiation, and smoking; \n
- genetic pathologies such as Down syndrome; and \n
- severe malnutrition during fetal development. \n
\n
Signs and symptoms
\n
\nMany babies born with microcephaly may have no other symptoms at birth, but may later develop epilepsy, cerebral palsy, learning disabilities, hearing loss, and problems with vision. Some children with microcephaly develop quite normally.
Some children with microcephaly develop quite normally.
\n
Treatment and care
\n
\nThere is no specific treatment for microcephaly. A multidisciplinary team is needed to evaluate and treat newborns and children with microcephaly. Early promotional activities and play programs can have a positive impact on development. Family counseling and parental support are also very important.
\n
WHO activities
\n
\nSince mid-2015, WHO has been working closely with the Americas to investigate and respond to the outbreak.
\n
\nThe Strategic Response Program and Joint Action Plan outlines steps being taken by WHO and partners in response to Zika virus and potential complications:
\n
- \n
- Working closely with affected countries to conduct outbreak investigations caused by the Zika virus and responding to an unusual rise in microcephaly cases.
 \n
\n - Engage with local communities to communicate the risks of Zika virus disease and how they can protect themselves. \n
- Provide advice and mitigate the potential impact on women of childbearing age and pregnant women and families affected by the Zika virus. \n
- Assist affected countries to improve care for pregnant women and families with children born with microcephaly. \n
- Investigation of the reported increase in microcephaly cases and possible association with Zika virus infection, with the participation of experts and partners. \n
\n
","datePublished":"2018-02-16T09:06:00.0000000+00:00","image":"https://cdn.who.int/media/images/default -source/imported/measure-microcephaly475-jpg.jpg?sfvrsn=7be7eab_0","publisher":{"@type":"Organization","name":"World Health Organization: WHO","logo":{" @type":"ImageObject","url":"https://www.who.int/Images/SchemaOrg/schemaOrgLogo. jpg","width":250,"height":60}},"dateModified": "2018-02-16T09:06:00.0000000+00:00","mainEntityOfPage":"https://www.who.int/ru/news-room/fact-sheets/detail/microcephaly","@context" :"http://schema.org","@type":"Article"};
jpg","width":250,"height":60}},"dateModified": "2018-02-16T09:06:00.0000000+00:00","mainEntityOfPage":"https://www.who.int/ru/news-room/fact-sheets/detail/microcephaly","@context" :"http://schema.org","@type":"Article"};
Basic Facts
- Microcephaly is a condition in which a baby is born with a small head or the head stops growing after birth.
- Microcephaly is a rare condition. One child out of several thousand children is born with microcephaly.
- The most reliable way to detect microcephaly in a baby is to measure the circumference of the baby's head 24 hours after birth, compare it with the WHO standard child development indicators, and then measure the head growth in early infancy.
- Children born with microcephaly may suffer from seizures as they grow, as well as physical and learning disabilities.
- There is no specific test to detect microcephaly in a fetus, but an ultrasound scan in the third trimester of pregnancy can sometimes reveal the problem.

- There is no specific treatment for microcephaly.
Microcephaly is a neonatal malformation in which the baby's head is much smaller than other babies of the same age and sex. Combined with improper brain development, children with microcephaly may develop developmental disabilities. The severity of microcephaly varies from mild to severe.
Magnitude of the problem
Microcephaly is a rare condition. The prevalence of microcephaly is estimated to vary considerably due to different definitions and depending on target populations. Scientists are investigating a potential, though unproven, link between an increase in microcephaly cases and Zika virus infection.
Diagnostics
Microcephaly can sometimes be diagnosed with a fetal ultrasound. The most appropriate period for diagnosis is the end of the second trimester (about 28 weeks) or the third trimester of pregnancy.
Head circumference of newborns should be measured at least 24 hours after birth and compared with WHO standard child development indicators. The results are interpreted taking into account the gestational age of the child, as well as his height and weight. If there is suspicion, the child is sent for examination to the pediatrician and for a brain scan, the circumference of his head is measured once a month in early infancy and compared with standard indicators. Doctors should also test for known causes of microcephaly.
The results are interpreted taking into account the gestational age of the child, as well as his height and weight. If there is suspicion, the child is sent for examination to the pediatrician and for a brain scan, the circumference of his head is measured once a month in early infancy and compared with standard indicators. Doctors should also test for known causes of microcephaly.
Causes of microcephaly
Microcephaly has many potential causes, but often the cause remains unknown. The most common causes include:
- intrauterine infections: toxoplasmosis (caused by a parasite found in undercooked meat), rubella, herpes, syphilis, cytomegalovirus and HIV;
- exposure to toxic chemicals: maternal exposure to heavy metals such as arsenic and mercury, alcohol, radiation and smoking;
- genetic pathologies such as Down syndrome; and
- severe malnutrition during fetal development.
Signs and symptoms
Many babies born with microcephaly may have no other symptoms at birth, but may later develop epilepsy, cerebral palsy, learning disabilities, hearing loss, and vision problems. Some children with microcephaly develop quite normally.
Some children with microcephaly develop quite normally.
Treatment and care
There is no specific treatment for microcephaly. A multidisciplinary team is needed to evaluate and treat newborns and children with microcephaly. Early promotional activities and play programs can have a positive impact on development. Family counseling and parental support are also very important.
WHO activities
Since mid-2015, WHO has been working closely with the Americas to investigate and respond to the outbreak.
The Strategic Response Program and Joint Action Plan outlines steps being taken by WHO and partners in response to Zika virus and potential complications:
- Working closely with affected countries to investigate the Zika virus outbreak and respond to unusual an increase in the incidence of microcephaly.
- Engage with local communities to communicate the risks of Zika virus disease and how they can protect themselves.
- Provide advice and mitigate the potential impact on women of childbearing age and pregnant women, and on families affected by the Zika virus.