Baby's soft spot closing too early
Facts about Craniosynostosis | CDC
Craniosynostosis is a birth defect in which the bones in a baby’s skull join together too early. This happens before the baby’s brain is fully formed. As the baby’s brain grows, the skull can become more misshapen.
Click here to view a larger image
Click here to view a larger image
What is Craniosynostosis?
Craniosynostosis is a birth defect in which the bones in a baby’s skull join together too early. This happens before the baby’s brain is fully formed. As the baby’s brain grows, the skull can become more misshapen. The spaces between a typical baby’s skull bones are filled with flexible material and called sutures. These sutures allow the skull to grow as the baby’s brain grows. Around two years of age, a child’s skull bones begin to join together because the sutures become bone. When this occurs, the suture is said to “close.” In a baby with craniosynostosis, one or more of the sutures closes too early. This can limit or slow the growth of the baby’s brain.
When a suture closes and the skull bones join together too soon, the baby’s head will stop growing in only that part of the skull. In the other parts of the skull where the sutures have not joined together, the baby’s head will continue to grow. When that happens, the skull will have an abnormal shape, although the brain inside the skull has grown to its usual size. Sometimes, though, more than one suture closes too early. In these instances, the brain might not have enough room to grow to its usual size. This can lead to a build-up of pressure inside the skull.
Types of Craniosynostosis
The types of craniosynostosis depend on what sutures join together early.
- Sagittal synostosis– The sagittal suture runs along the top of the head, from the baby’s soft spot near the front of the head to the back of the head. When this suture closes too early, the baby’s head will grow long and narrow (scaphocephaly).
 It is the most common type of craniosynostosis.
It is the most common type of craniosynostosis. - Coronal synostosis – The right and left coronal sutures run from each ear to the sagittal suture at the top of the head. When one of these sutures closes too early, the baby may have a flattened forehead on the side of the skull that closed early (anterior plagiocephaly). The baby’s eye socket on that side might also be raised up and his or her nose could be pulled toward that side. This is the second most common type of craniosynostosis.
- Bicoronal synostosis – This type of craniosynostosis occurs when the coronal sutures on both sides of the baby’s head close too early. In this case, the baby’s head will grow broad and short (brachycephaly).
- Lambdoid synostosis – The lambdoid suture runs along the backside of the head. If this suture closes too early, the baby’s head may be flattened on the back side (posterior plagiocephaly). This is one of the rarest types of craniosynostosis.
- Metopic synostosis – The metopic suture runs from the baby’s nose to the sagittal suture at the top of the head. If this suture closes too early, the top of the baby’s head shape may look triangular, meaning narrow in the front and broad in the back (trigonocephaly). This is one of the rarest types of craniosynostosis.
Other Problems
Many of the problems a baby can have depend on:
- Which sutures closed early
- When the sutures closed (was it before or after birth and at what age)
- Whether or not the brain has room to grow
Sometimes, if the condition is not treated, the build-up of pressure in the baby’s skull can lead to problems, such as blindness, seizures, or brain damage.
How Many Babies are Born with Craniosynostosis?
Researchers estimate that about 1 in every 2,500 babies is born with craniosynostosis in the United States.1
Causes and Risk Factors
The causes of craniosynostosis in most infants are unknown. Some babies have a craniosynostosis because of changes in their genes. In some cases, craniosynostosis occurs because of an abnormality in a single gene, which can cause a genetic syndrome. However, in most cases, craniosynostosis is thought to be caused by a combination of genes and other factors, such as things the mother comes in contact with in her environment, or what the mother eats or drinks, or certain medications she uses during pregnancy.
Some babies have a craniosynostosis because of changes in their genes. In some cases, craniosynostosis occurs because of an abnormality in a single gene, which can cause a genetic syndrome. However, in most cases, craniosynostosis is thought to be caused by a combination of genes and other factors, such as things the mother comes in contact with in her environment, or what the mother eats or drinks, or certain medications she uses during pregnancy.
CDC, like the many families of children with birth defects, wants to find out what causes these conditions. Understanding the factors that are more common among babies with a birth defect will help us learn more about the causes. CDC funds the Centers for Birth Defects Research and Prevention, which collaborate on large studies such as the National Birth Defects Prevention Study (NBDPS; births 1997-2011), to understand the causes of and risks for birth defects, such as craniosynostosis.
Recently, CDC reported on important findings from research studies about some factors that increase the chance of having a baby with craniosynostosis:
- Maternal thyroid disease ― Women with thyroid disease or who are treated for thyroid disease while they are pregnant have a higher chance of having an infant with craniosynostosis, compared to women who don’t have thyroid disease.
 2
2 - Certain medications ― Women who report using clomiphene citrate (a fertility medication) just before or early in pregnancy are more likely to have a baby with craniosynostosis, compared to women who didn’t take this medicine.3
CDC continues to study birth defects, such as craniosynostosis, and how to prevent them. If you are pregnant or thinking about becoming pregnant, talk with your doctor about ways to increase your chances of having a healthy baby.
Diagnosis
Craniosynostosis usually is diagnosed soon after a baby is born. Sometimes, it is diagnosed later in life.
Usually, the first sign of craniosynostosis is an abnormally shaped skull. Other signs may include:
- No “soft spot” on the baby’s skull
- A raised firm edge where the sutures closed early
- Slow growth or no growth in the baby’s head size over time
Doctors can identify craniosynostosis during a physical exam. A doctor will feel the baby’s head for hard edges along the sutures and unusual soft spots. The doctor also will look for any problems with the shape of the baby’s face. If he or she suspects the baby might have craniosynostosis, the doctor usually requests one or more tests to help confirm the diagnosis. For example, a special x-ray test, such as a CT or CAT scan, can show the details of the skull and brain, whether certain sutures are closed, and how the brain is growing.
The doctor also will look for any problems with the shape of the baby’s face. If he or she suspects the baby might have craniosynostosis, the doctor usually requests one or more tests to help confirm the diagnosis. For example, a special x-ray test, such as a CT or CAT scan, can show the details of the skull and brain, whether certain sutures are closed, and how the brain is growing.
Treatments
Many types of craniosynostosis require surgery. The surgical procedure is meant to relieve pressure on the brain, correct the craniosynostosis, and allow the brain to grow properly. When needed, a surgical procedure is usually performed during the first year of life. But, the timing of surgery depends on which sutures are closed and whether the baby has one of the genetic syndromes that can cause craniosynostosis.
Babies with very mild craniosynostosis might not need surgery. As the baby gets older and grows hair, the shape of the skull can become less noticeable. Sometimes, special medical helmets can be used to help mold the baby’s skull into a more regular shape.
Each baby born with craniosynostosis is different, and the condition can range from mild to severe. Most babies with craniosynostosis are otherwise healthy. Some children, however, have developmental delays or intellectual disabilities, because either the craniosynostosis has kept the baby’s brain from growing and working normally, or because the baby has a genetic syndrome that caused both craniosynostosis and problems with how the brain works. A baby with craniosynostosis will need to see a healthcare provider regularly to make sure that the brain and skull are developing properly. Babies with craniosynostosis can often benefit from early intervention services to help with any developmental delays or intellectual problems. Some children with craniosynostosis may have issues with self-esteem if they are concerned with visible differences between themselves and other children. Parent-to-parent support groups also can be useful for new families of babies with birth defects of the head and face, including craniosynostosis.
Other Resources
The views of these organizations are their own and do not reflect the official position of CDC.
- Children’s Craniofacial Association (CCA)
CCA addresses the medical, financial, psychosocial, emotional, and educational concerns relating to craniofacial conditions. - The National Craniofacial Association (FACES)
FACES is dedicated to assisting children and adults who have craniofacial disorders resulting from disease, accident, or birth.
References
- Boulet SL, Rasmussen SA, Honein MA. A population-based study of craniosynostosis in metropolitan Atlanta, 1989-2003. Am J Med Genet Part A. 2008;146A:984–991.
- Rasmussen SA, Yazdy MM, Carmichael SL, Jamieson DJ, Canfield MA, Honein MA. Maternal thyroid disease as a risk factor for craniosynostosis. Obstet Gynecol. 2007;110:369-377.
- Reefhuis J, Honein MA, Schieve LA, Rasmussen SA, and the National Birth Defects Prevention Study. Use of clomiphene citrate and birth defects, National Birth Defects Prevention Study, 1997–2005.
 Hum Reprod. 2011;26:451–457.
Hum Reprod. 2011;26:451–457.
The images are in the public domain and thus free of any copyright restrictions. As a matter of courtesy we request that the content provider (Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities) be credited and notified in any public or private usage of this image.
The images are in the public domain and thus free of any copyright restrictions. As a matter of courtesy we request that the content provider (Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities) be credited and notified in any public or private usage of this image.
Craniosynostosis | Johns Hopkins Medicine
What You Need to Know
- Craniosynostosis is common and occurs in one out of 2,200 live births.

- The condition affects males slightly more often than females.
- Craniosynostosis is most often sporadic (occurs by chance) but can be inherited in some families.
What is craniosynostosis?
In fetuses and newborns, the skull consists of several plates of bone that are separated by flexible, fibrous joints called sutures. As infants grow and develop, the sutures close, forming a solid piece of bone.
Craniosynostosis is a condition in which the sutures close too early, causing problems with normal brain and skull growth. Premature closure of the sutures may also cause pressure inside the head to increase and the skull or facial bones to change from a normal, symmetrical appearance.
What causes craniosynostosis?
Craniosynostosis is a feature of many different genetic syndromes that have a variety of inheritance patterns and chances for recurrence, depending on the specific syndrome present.
It is important for the child with craniosynostosis and his/her family members to be examined carefully for signs of an inherited genetic disorder, such as limb defects, ear abnormalities or heart defects.
Craniosynostosis Symptoms
In infants with this condition, the most common signs are changes in the shape of the head and face. One side of your child’s face may look markedly different from the other side. Other, much less common signs may include:
- A full or bulging fontanelle (soft spot located on the top of the head)
- Sleepiness (or less alert than usual)
- Very noticeable scalp veins
- Increased irritability
- High-pitched cry
- Poor feeding
- Projectile vomiting
- Increasing head circumference
- Developmental delays
The symptoms of craniosynostosis may resemble other conditions or medical problems, so always work with your child’s physician to clarify a diagnosis.
Different Types of Craniosynostosis
Brachycephaly
Anterior brachycephaly involves fusion of either the right or left side of the coronal suture that runs across the top of the baby’s head from ear to ear.
This is called coronal synostosis, and it causes the normal forehead and brow to stop growing. The result is a flattening of the forehead and the brow on the affected side, with the forehead tending to be excessively prominent on the opposite side. The eye on the affected side may also have a different shape, and there may be flattening of the back of the head (occipital). When the suture fusion is all the way across the back of the child’s skull, the result is posterior plagiocephaly.
Trigonocephaly
Trigonocephaly is a fusion of the metopic (forehead) suture. This suture runs from the top of the head down the middle of the forehead, toward the nose.
Early closure of this suture may result in a prominent ridge running down the forehead. Sometimes, the forehead looks quite pointed, like a triangle, with closely placed eyes (hypotelorism).
Sometimes, the forehead looks quite pointed, like a triangle, with closely placed eyes (hypotelorism).
Scaphocephaly
Scaphocephaly is an early closure or fusion of the sagittal suture. This suture runs front to back, down the middle of the top of the head. This fusion causes a long, narrow skull. The skull is long from front to back and narrow from ear to ear.
Craniosynostosis Diagnosis
Craniosynostosis may be congenital (present at birth) or observed later, often during a physical examination in the first year of life.
The diagnosis involves thorough physical examination and diagnostic testing. Your child’s doctor will start with a complete prenatal and birth history, asking about any family history of craniosynostosis or other head or face abnormalities.
The doctor may also ask about developmental milestones, since craniosynostosis can be associated with other neuromuscular disorders. Developmental delays may require further medical follow-up for underlying problems.
During the examination, the doctor will measure the circumference of your child’s head to identify normal and abnormal ranges. Craniosynostosis can be diagnosed by physical exam. If needed, your neurosurgeon may recommend imaging tests.
Craniosynostosis: Fitz’s Story
When Fitz was born, it was obvious that his skull was misshapen. By 5 weeks old, Fitz had been diagnosed with craniosynostosis. His skull had fused early and was constricting his brain growth.
See Fitz's story
Craniosynostosis Treatment
The key to treating craniosynostosis is early detection and treatment. Specific therapy for craniosynostosis will be determined by your child’s physician based on:
- Your child’s age, overall health and medical history
- Extent of the craniosynostosis
- Type of craniosynostosis (which sutures are involved)
- Your child’s tolerance for specific medications, procedures or therapies
- Expectations for the course of the craniosynostosis
- Your opinion or preference
Surgery is typically the recommended treatment, since it can reduce pressure in the head and correct the deformities of the face and skull bones.
Early diagnosis and consultation with a specialist are important. In general, the best time to operate is before the child is 1 year old, since the bones are still very soft and easy to work with. If your child’s condition is severe, the doctor may recommend surgery as early as 1 month of age.
Before surgery, your child’s physician will explain the operation and may review before-and-after photographs of children who have had a similar type of surgery.
Calvarial Vault Remodeling
In this procedure, the surgeon makes an incision in the infant’s scalp and corrects the shape of the head by moving the area of the skull that is abnormally or prematurely fused, and then reshapes the skull so it can take more of a round contour. Surgery can last up to six hours. Your baby will likely spend one night in the intensive care unit, plus an additional few days in the hospital for monitoring.
Even if your child’s deformity is seen early on, this surgery is best suited for babies 5-6 months of age or older to ensure the bone is thick enough to perform the needed reshaping. This surgery may commonly involve a blood transfusion.
This surgery may commonly involve a blood transfusion.
After surgery, there may be temporary facial swelling. Unlike other surgical options, there are no additional steps post-surgery unless a recurrence of craniosynostosis is found. You can expect to follow up with your surgery team one month post-surgery to check on the surgery incision site, and again at six and 12 months after the procedure to ensure healing is progressing.
Endoscopic Craniosynostosis Surgery
Some hospitals may offer the option of this minimally invasive surgery, which may be performed when the baby is 2–3 months old, depending on the type and degree of craniosynostosis.
The procedure involves the use of an endoscope, a small tube that the surgeon can look through and see immediately inside and outside the skull through very small incisions in the scalp. The surgeon opens the prematurely fused suture to enable the baby’s brain to grow normally.
The surgery itself takes approximately one hour and involves less blood loss compared with cranial vault remodeling, so there is less chance of requiring a blood transfusion. Your baby will stay in the hospital overnight for monitoring before being released to go home.
Your baby will stay in the hospital overnight for monitoring before being released to go home.
This type of surgery is followed by the use of a molding helmet to reshape the skull. Additional appointments with the helmet provider (orthotist) will be necessary for fitting the helmet to your child. You can expect to follow up with your surgery team every three months for the first year post-surgery to check progress of the skull reshaping.
After Craniosynostosis Surgery
Following craniosynostosis surgery, your child will likely have a turbanlike dressing around his or her head, and may experience swelling in the face and eyelids. Your child will spend the period after surgery in an intensive care unit for close monitoring.
The care team will watch closely for any problems after surgery, such as:
- Fever (greater than 101 degrees Fahrenheit)
- Vomiting
- Irritability
- Redness and swelling along the incision areas
- Decreased alertness
These complications require prompt evaluation by your child’s surgeon.
Follow-Up Care
The recovery process is different for each child. Your child’s health care team will work with your family, giving you instructions on how to care for your child at home and outlining specific problems that require immediate medical attention.
Craniosynostosis can affect a child’s brain and development. The degree of the problems depends on the severity of the craniosynostosis, the number of sutures that are fused, and the presence of brain or other organ system problems that could affect the child.
The physician may recommend genetic counseling to evaluate the child’s parents for any disorders that may run in families.
A child with craniosynostosis requires frequent medical evaluations to ensure that the skull, facial bones, jaw alignment and brain are developing normally. The medical team will provide education and guidance to help you make the most of your child’s health and well-being.
The Johns Hopkins Cleft and Craniofacial Center
Each year, the Johns Hopkins Cleft and Craniofacial Center treats approximately 650 babies and children with cleft lip and palate or other craniofacial conditions. Our goal is to help our patients achieve their full potential, without being defined or limited by facial differences.
Our goal is to help our patients achieve their full potential, without being defined or limited by facial differences.
Learn More about the Cleft and Craniofacial Center
Large fontanel in newborns. Examination IPM Clinic for Children Krasnoyarsk
The birth of a baby is a very important and joyful event in the life of young parents. After birth, there are a lot of questions about the health, care and proper development of the baby. The very first questions are often asked about the fontanel.
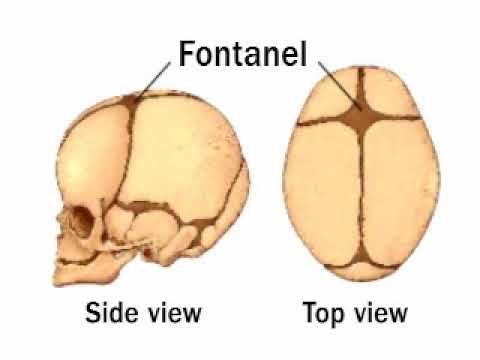
Fontanelle - soft, non-ossified area of the cranial vault of newborn babies, consisting of the remnants of the membranous skeleton and connecting the bones of the skull. In the area of the fontanelles, a pulsation of the arteries of the brain and membranes is felt, which is why these areas are called pulsating, gushing. Fontanelles allow you to “compress” the cranial vault during childbirth for a better passage of the baby through the birth canal. Four of them close in the first days of a child's life, the fifth in the second month of life, and the sixth, the largest (anterior), closes from 3 to 24 or more months. Very often, fontanelles and the pace of their closure cause great concern to parents.
Four of them close in the first days of a child's life, the fifth in the second month of life, and the sixth, the largest (anterior), closes from 3 to 24 or more months. Very often, fontanelles and the pace of their closure cause great concern to parents.
Role of the fontanel:
- The growth of the skull bones depends on the growth of the brain. The fontanelles provide elasticity to the skull during the most rapid growth. This period is from birth to two years of a child's life.
- Fontanelles also protect the baby's skull from injury: upon impact, the possibility of elastic deformation of the skull remains, which extinguishes all the kinetic energy of the impact and protects the child.
- The brain of a newborn baby is very sensitive to overheating, and a kind of natural “window” brings excess heat out and naturally cools the meninges, thereby playing an important role in the processes of heat transfer and thermoregulation of the body.
The size of the anterior (large) fontanel varies greatly.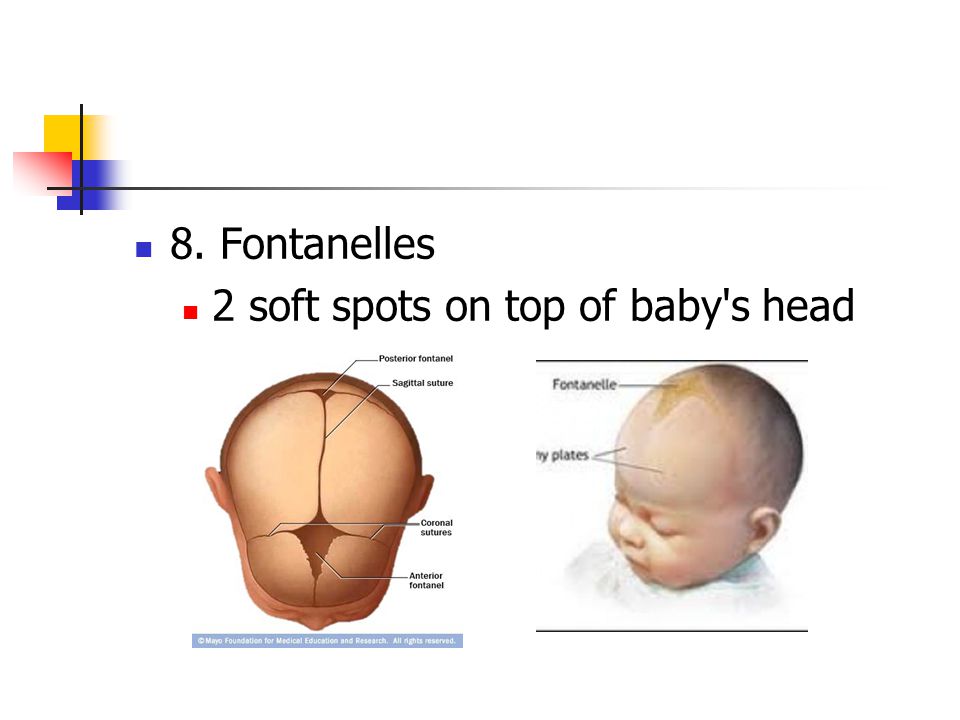 On average, the normal size of the fontanel at birth is 3.0 * 2.5 cm, it has a diamond shape.
On average, the normal size of the fontanel at birth is 3.0 * 2.5 cm, it has a diamond shape.
With active growth and constant development of the baby, the free space between the bones gradually hardens and decreases in size, the pulsation becomes almost imperceptible.
Timing of fontanel closure may vary. On average, complete closure occurs by the year (normally also up to two years).
When the fontanel closes too slowly, the parents start to worry. But premature closure also does not speak well.
reasons for the “big” fontanel:
- Achondroplasia (hereditary disease)
- Down Syndrome
- Hydrocephalus
- Premature birth
- Neonatal Hypoteriosis
- RACHITS
RACHITS is one of the most common rickets slow closure of the fontanel. Most often, rickets develops in premature babies and in children who do not receive preventive treatment with vitamin D. In a child with rickets, the edges of a large fontanel are flexible, the back of the head flattens, and characteristic bone thickenings form on both sides of the sternum.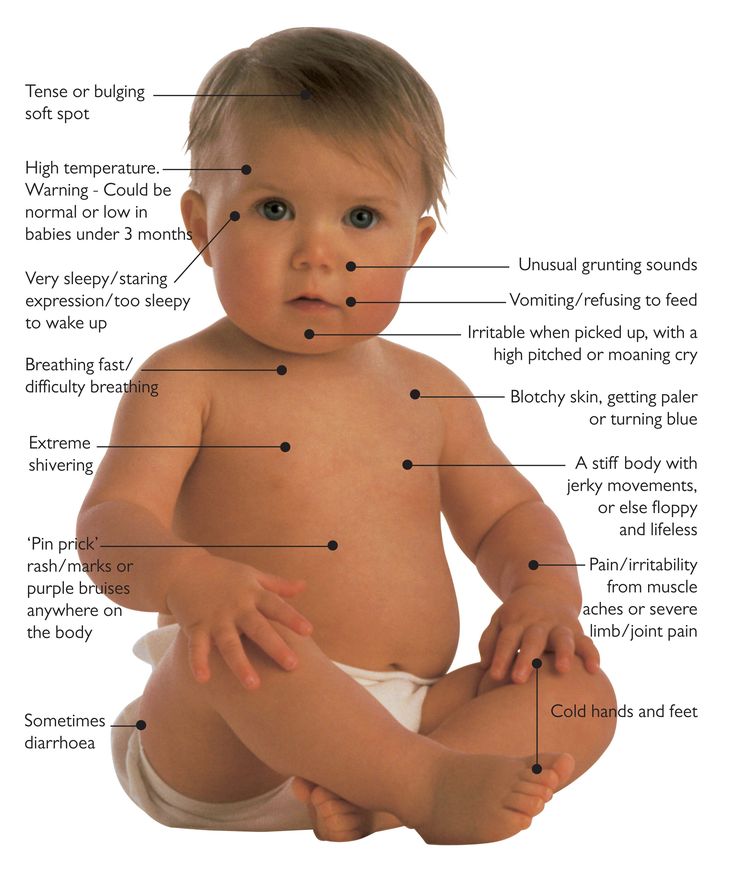
The change in the appearance of the fontanel also indicates a number of certain problems:
- Furious fontanel occurs against the background of
- an increase in temperature to febrile numbers
- multiple vomiting
- diarrhea
- Brutcher
- meningitis
- encephalitis
- intracranial bleeding
- increased intracranial pressure
Many factors are affected on the pace of ossification:
- for mom:
- a balanced diet
- sufficient intake of calcium in the body
- polyvitamin complexes
- for the child:
- the appointment of vitamin Ditamin D
— sunbathing
Dispensary examination of a child under one year old allows the pediatrician to examine the baby every month. During the examination, a complete examination of the child is carried out, weighing, measuring height, head and chest circumference. The size of the large fontanel is also measured.
The size of the large fontanel is also measured.
Be healthy!
Phone number for making an appointment with a pediatrician (391) 200-50-03
everything you need to know about fontanelles in newborns and children - Children - tsn.ua
they are a little worried: how to do everything correctly and accurately, without injuring the fragile bones of the baby? They are especially afraid of washing the head of the baby and combing the hair because of the fontanel. Maya Smolyar, head of the department of post-intensive nursing of premature newborns of the Zhytomyr Regional Perinatal Center, spoke about whether special care is needed for the fontanel and what changes in it should alert.
What is the fontanelle and what is it for
The fontanel is that part of the child's head where there is temporarily no complete ossification. The largest fontanel is on the crown, where the bones do not converge together, leaving a diamond-shaped area. Physiologically, the child is designed so that during childbirth, these bones of the skull are slightly deformed, allowing the fetal head to pass through the birth canal. In addition, the fontanel is a kind of reserve, due to which the brain of a newborn child will then grow.
Physiologically, the child is designed so that during childbirth, these bones of the skull are slightly deformed, allowing the fetal head to pass through the birth canal. In addition, the fontanel is a kind of reserve, due to which the brain of a newborn child will then grow.
Normally, a child has 6 fontanelles. The largest is located on the crown, the second largest is the occipital, it is typical for premature babies. The smallest are located on the sides of the cranium.
When do fontanelles overgrow?
At the time of birth, a full-term baby has only one large fontanel on the crown of the head. All others must be closed. In extreme cases, traces of the occipital fontanel may remain, which should close during the first month. And the lateral fontanelles must be overgrown by the time of birth.
When does the parietal fontanel close?
Normally, a large fontanel closes in the period from one to 1.5 years. If the closure occurs earlier, for example, at 6-8 months, then this may be a normal variant or a family predisposition, but this should be paid attention to and consulted with a pediatrician.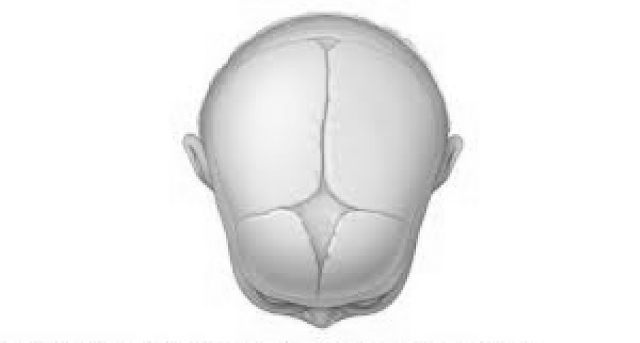 Premature closure of the fontanel may indicate the manifestation of certain problems.
Premature closure of the fontanel may indicate the manifestation of certain problems.
What should I do if the fontanel actively pulsates or sinks?
If the child's parietal fontanel pulsates when crying, you should not pay attention to it, but if the pulsation is noticeable in the child's calm state or during sleep, then you need to contact a pediatrician, who will refer you to a pediatric neurologist. Most likely, the child has increased intracranial pressure, or the so-called hydrocephalic syndrome.
Sometimes, the fontanel, on the contrary, sinks inward. This can only happen in children of the first month of life. And if it sinks after the first month, then this indicates that the child has lost fluid with diarrhea or is not eating enough. Parents should know that a normal fontanel should be at the level of the skull bones. In a calm state, it should neither bulge and pulsate, nor sink.
Is it normal to have crusts on the child's head in the fontanel area?
Parents should understand that the fontanel does not require special care.