Is induced labor more painful
Inducing labour - NHS
An induced labour is one that's started artificially. Every year, 1 in 5 labours are induced in the UK.
Sometimes labour can be induced if your baby is overdue or there's any risk to you or your baby's health.
This risk could be if you have a health condition such as high blood pressure, for example, or your baby is not growing.
Induction will usually be planned in advance. You'll be able to discuss the advantages and disadvantages with your doctor and midwife, and find out why they think your labour should be induced.
It's your choice whether to have your labour induced or not.
If your pregnancy lasts longer than 42 weeks and you decide not to have your labour induced, you should be offered increased monitoring to check your baby's wellbeing.
Why you might be induced
- if you're overdue
- if your waters have broken
- if you or your baby have a health problem
If you're overdue
Induction will be offered if you do not go into labour naturally by 42 weeks, as there will be a higher risk of stillbirth or problems for the baby.
If your waters break early
If your waters break more than 24 hours before labour starts, there's an increased risk of infection to you and your baby.
If your waters break after 34 weeks, you'll have the choice of induction or expectant management.
Expectant management is when your healthcare professionals monitor your condition and your baby's wellbeing, and your pregnancy can progress naturally as long as it's safe for both of you.
Your midwife or doctor should discuss your options with you before you make a decision.
They should also let you know about the newborn (neonatal) special care hospital facilities in your area.
If your baby is born earlier than 37 weeks, they may be vulnerable to problems related to being premature.
If your waters break before 34 weeks, you'll only be offered induction if there are other factors that suggest it's the best thing for you and your baby.
If you have a health condition or your baby is not thriving
You may be offered an induction if you have a condition that means it'll be safer to have your baby sooner, such as diabetes, high blood pressure or intrahepatic cholestasis of pregnancy.
If this is the case, your doctor and midwife will explain your options to you so you can decide whether or not to have your labour induced.
Membrane sweep
Before inducing labour, you'll be offered a membrane sweep, also known as a cervical sweep, to bring on labour.
To carry out a membrane sweep, your midwife or doctor sweeps their finger around your cervix during an internal examination.
This action should separate the membranes of the amniotic sac surrounding your baby from your cervix. This separation releases hormones (prostaglandins), which may start your labour.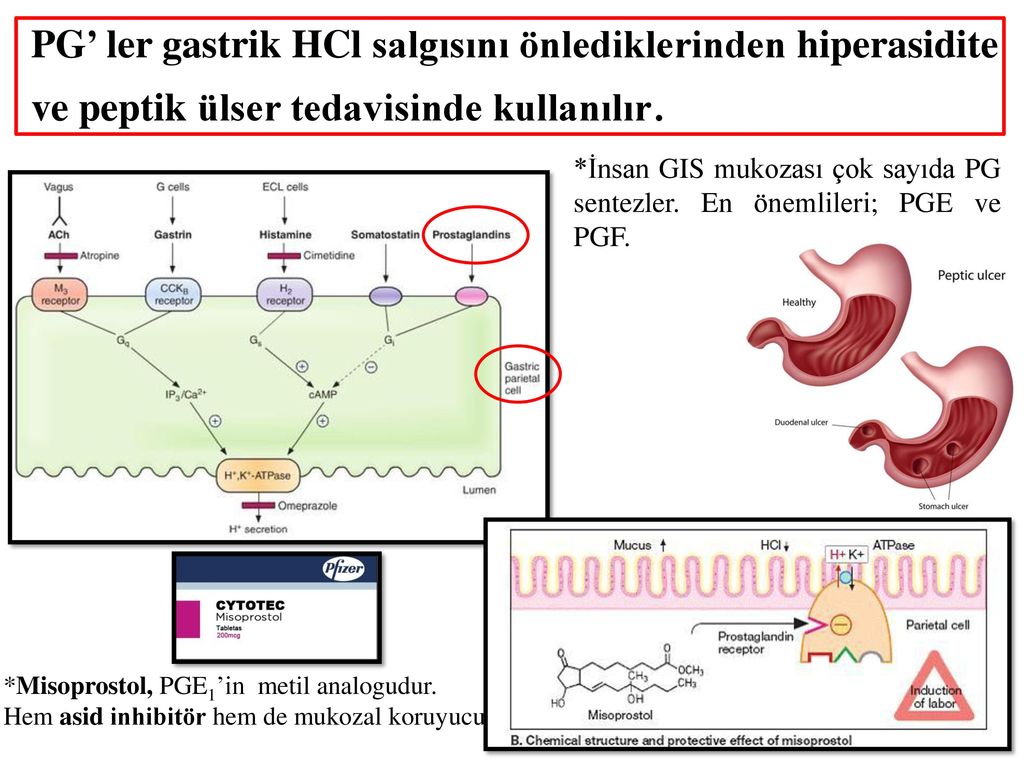
Having a membrane sweep does not hurt, but expect some discomfort or slight bleeding afterwards.
If labour does not start after a membrane sweep, you'll be offered induction of labour.
Induction is always carried out in a hospital maternity unit. You'll be looked after by midwives and doctors will be available if you need their help.
How labour is induced
If you're being induced, you'll go into the hospital maternity unit.
Contractions can be started by inserting a tablet (pessary) or gel into your vagina.
Induction of labour may take a while, particularly if the cervix (the neck of the uterus) needs to be softened with pessaries or gels.
You will usually stay in the hospital maternity unit while you wait for it to work.
If you've had no contractions after 6 hours, you may be offered another tablet or gel.
If you have a controlled-release pessary inserted into your vagina, it can take 24 hours to work. If you are not having contractions after 24 hours, you may be offered another dose.
Sometimes a hormone drip is needed to speed up the labour. Once labour starts, it should proceed normally, but it can sometimes take 24 to 48 hours to get you into labour.
What induced labour feels like
Induced labour is usually more painful than labour that starts on its own, and you may want to ask for an epidural.
Your pain relief options during labour are not restricted by being induced. You should have access to all the pain relief options usually available in the maternity unit.
If you are induced you'll be more likely to have an assisted delivery, where forceps or ventouse suction are used to help the baby out.
If induction of labour does not work
Induction is not always successful, and labour may not start.
Your obstetrician and midwife will assess your condition and your baby's wellbeing, and you may be offered another induction or a caesarean section.
Your midwife and doctor will discuss all your options with you.
Natural ways to start labour
There are no proven ways of starting your labour yourself at home.
You may have heard that certain things can trigger labour, such as herbal supplements and having sex, but there's no evidence that these work.
Other methods that are not supported by scientific evidence include acupuncture, homeopathy, hot baths, castor oil and enemas.
Having sex will not cause harm, but you should avoid having sex if your waters have broken as there's an increased risk of infection.
For more information on induction, you can read the NICE information for the public on induction of labour.
Video: When would I be induced and what's involved?
In this video, a midwife describes what an induction of labour is and what is involved.
Media last reviewed: 20 March 2020
Media review due: 20 March 2023
Induced labour | Pregnancy Birth and Baby
What is an induced labour?
Labour normally starts naturally any time between 37 and 42 weeks of pregnancy. The cervix softens and starts to open, you will get contractions, and your waters break.
In an induced labour, or induction, these labour processes are started artificially. It might involve mechanically opening your cervix, breaking your waters, or using medicine to start off your contractions — or a combination of these methods.
In Australia, about 1 in 3 women has an induced labour.
What are the differences between an induced and a natural labour?
An induced labour can be more painful than a natural labour. In natural labour, the contractions build up slowly, but in induced labour they can start more quickly and be stronger. Because the labour can be more painful, you are more likely to want some type of pain relief.
If your labour is induced, you are also more likely to need other interventions, such as the use of forceps or ventouse (vacuum) to assist with the birth of your baby. You will not be able to move around as much because the baby will be monitored more closely than during a natural labour.
You will only be offered induced labour if there is a risk to you or your baby's health. Your doctor might recommend induced labour if:
- you are overdue (more than 41 weeks pregnant)
- there is a concern the placenta is not working as it should
- you have a health condition, such as diabetes, kidney problems, high blood pressure or pre-eclampsia
- the baby is making fewer movements, showing changes in its heart rate, or not growing well
- your waters have broken, but the contractions have not started naturally
- you are giving birth to more than one baby (twins or multiple birth)
Not everyone can have an induced labour. It is not usually an option if you have had a caesarean section or major abdominal surgery before, if you have placenta praevia, or if your baby is breech or lying sideways.
It is not usually an option if you have had a caesarean section or major abdominal surgery before, if you have placenta praevia, or if your baby is breech or lying sideways.
Can I decide whether to have an induced labour?
If you are overdue, you might decide to wait and see if labour will start naturally. However, if there is a chance you or your baby are at risk of complications, you might need to consider induced labour before your due date.
When making your decision, discuss the risks and benefits with your doctor. Do not be afraid to ask lots of questions, such as:
- Why do I need an induction?
- How will it affect me and my baby?
- What will happen if I do not have the induction?
- What procedures are involved and how will you care for me and my baby?
You might need to consider several other health concerns. For example, there is a higher risk of stillbirth or other problems if your baby is not born before 42 weeks, and an increased risk of infection if your waters break more than 24 hours before labour starts.
What can I expect with an induced labour?
During the late stages of your pregnancy, your healthcare team will carry out regular checks on your health and your baby's heath. These checks help them decide whether it is better to induce labour or to keep the baby inside. Always tell your doctor or midwife if you notice your baby is moving less than normal.
If they decide it is medically necessary to induce labour, first your doctor or midwife will do an internal examination by feeling inside your vagina. They will feel your cervix to see if it is ready for labour. This examination will also help them decide on the best method for you.
It can take from a few hours to as long as 2 to 3 days to induce labour. It depends how your body responds to the treatment. It is likely to take longer if this is your first pregnancy or you are less than 37 weeks pregnant.
What options are there to induce labour?
There are different ways to induce labour. Your doctor or midwife will recommend the best method for you when they examine your cervix. You may need a combination of different strategies. You will need to provide written consent for the procedure.
You may need a combination of different strategies. You will need to provide written consent for the procedure.
Sweeping the membranes
During a vaginal examination, the midwife or doctor makes circular movements around your cervix with their finger. This action should release a hormone called prostaglandins. You do not need to be admitted to hospital for this procedure and it is often done in the doctor's room. This can be enough to get labour started, meaning you will not need any other methods.
Risks: This is a simple and easy procedure; however, it does not always work. It can be a bit uncomfortable, but it does not hurt.
Oxytocin
A synthetic version of the hormone oxytocin is given to you via a drip in your arm to start your contractions. When the contractions start, the amount of oxytocin is adjusted so you keep on having regular contractions until the baby is born. This whole process can take several hours.
Risks: Oxytocin can make contractions stronger, more frequent and more painful than in natural labour, so you are more likely to need pain relief. You will not be able to move around much because of the drip in your arm and you will also have a fetal monitor around your abdomen to monitor your baby.
You will not be able to move around much because of the drip in your arm and you will also have a fetal monitor around your abdomen to monitor your baby.
Sometimes the contractions can come too quickly, which can affect the baby's heart rate. This can be controlled by slowing down the drip or giving you another medicine.
Artificial rupture of membranes ('breaking your waters')
Artificial rupture of membranes (ARM) is used when your waters do not break naturally. Your doctor or midwife inserts a small hook-like instrument through your vagina to make a hole in the membrane sac that is holding the amniotic fluid. This will increase the pressure of your baby's head on your cervix, which may be enough to get labour started. Many women will also need oxytocin to start their contractions.
Risks: ARM can be a bit uncomfortable but not painful. There is a small increased risk of a prolapsed umbilical cord, bleeding or infection.
Prostaglandins
A synthetic version of the hormone prostaglandins is inserted into your vagina to soften your cervix and prepare your body for labour. It can be in the form of a gel, which may be given in several doses (usually every 6 to 8 hours), or a pessary and tape (similar to a tampon), which slowly releases the hormone over 12 to 24 hours. You will need to lie down and stay in hospital after the prostaglandins is inserted. You may also then need ARM if your waters have not broken, or oxytocin to bring on the contractions.
It can be in the form of a gel, which may be given in several doses (usually every 6 to 8 hours), or a pessary and tape (similar to a tampon), which slowly releases the hormone over 12 to 24 hours. You will need to lie down and stay in hospital after the prostaglandins is inserted. You may also then need ARM if your waters have not broken, or oxytocin to bring on the contractions.
Prostaglandins gel is often the preferred method of inducing labour since it is the closest to natural labour. Tell your midwife or doctor straight away if you start to experience painful, regular contractions 5 minutes apart for your first baby, or 10 minutes apart for subsequent babies, or if your waters break, because these are both signs that your labour is beginning.
Risks: Some women find their vagina is sore after the prostaglandin gel, or they might experience nausea, vomiting or diarrhoea. These side effects are rare and there is no evidence that induction using prostaglandin is any more painful than a natural labour.
Very rarely, the contractions can come too strongly, which can affect the baby's heart rate. This can be controlled by giving you another medicine or removing the pessary.
You need to let your doctor or midwife know immediately if you start bleeding, or if your baby is moving less, because this could be a sign that something is wrong.
Cervical ripening balloon catheter
A cervical ripening balloon catheter is a small tube attached to a balloon that is inserted into your cervix. The balloon is inflated with saline, which usually puts enough pressure on your cervix for it to open. It stays in place for up to 15 hours, and then you will be examined again.
Tell your midwife or doctor straight away if you start to experience painful, regular contractions 5 minutes apart for your first baby, or 10 minutes apart for subsequent babies, or if your waters break, because these are both signs that your labour is beginning.
You may also need ARM or oxytocin if you are using a cervical ripening balloon catheter.
Risks: Inserting the catheter can be a bit uncomfortable but not painful.
You also need to let your doctor or midwife know immediately if you start bleeding, or your baby is moving less, because this could be a sign that something is wrong.
Can I have pain relief during induced labour?
Induced labour is usually more painful than natural labour. Depending on the type of induction you are having, this could range from discomfort with the procedure or more intense and longer lasting contractions as a result of the medication you have been given. Women who have induced labour are more likely to ask for an epidural for relief.
Because inductions are almost always done in hospital, the full range of pain relief should be available to you. There is usually no restriction on the type of pain relief you can have if your labour is induced.
Are there any risks with inducing labour?
There are some increased risks if you have an induced labour.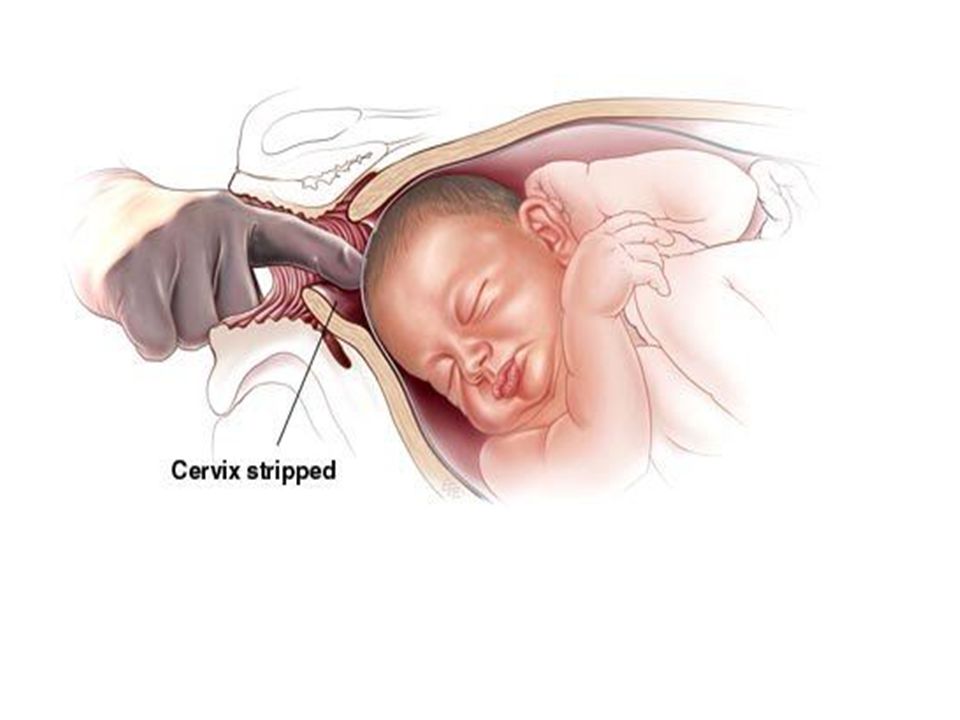 These include that:
These include that:
- it will not work — in about 1 of 4 cases, women go on to have a caesarean
- your baby will not get enough oxygen and their heart rate is affected
- you or your baby get an infection
- your uterus tears
- you bleed a lot after the birth
What happens if the induction does not work?
Not all induction methods will work for everyone. Your doctor may try another method, or you might need to have a caesarean. Your doctor will discuss all of these options with you.
Learn more here about the development and quality assurance of healthdirect content.
Article about natural childbirth
Natural childbirth is a magical combination of words that everyone understands in their own way. Some say that this is childbirth without medical intervention, others - that this is childbirth "according to science." Recently, however, it seems that the disputing parties have come to a common definition of natural childbirth. We can say that natural childbirth is a process that is perceived as natural and normal by a trained woman in labor, a doctor and an obstetrician. These are births in which any medical interventions are carried out only according to strict indications, and the woman has the freedom to give birth in the way that suits her.
We can say that natural childbirth is a process that is perceived as natural and normal by a trained woman in labor, a doctor and an obstetrician. These are births in which any medical interventions are carried out only according to strict indications, and the woman has the freedom to give birth in the way that suits her.
Why is there so much talk about the inadmissibility of unnecessary medical intervention in the course of natural childbirth?
Every woman is different, so every pregnancy and every birth is different. When childbirth begins on its own and lasts as long as nature intended for them, then, as a rule, they end in a successful resolution. Of course, we are not talking about cases where the child's heartbeat is disturbed, he does not have enough oxygen, or the mother's labor activity is disturbed. No one says that medical intervention in childbirth is not necessary at all. We are talking about the fact that it is unacceptable to interfere in the normal course of childbirth. And the fact that the child feels normal, and childbirth, even long ones, proceed correctly, can be determined by listening to the child's heart sounds.
And the fact that the child feels normal, and childbirth, even long ones, proceed correctly, can be determined by listening to the child's heart sounds.
However, in the maternity hospital, labor is often stimulated and then artificially accelerated in order to make labor go faster. Of course, this interferes with a truly natural process. Therefore, the definition of natural childbirth as childbirth without artificial stimulation without clear indications for it is not without foundation. Induced labor is usually more painful than spontaneous labor, so labor induction also involves pain relief.
The fact is that the woman's body does not have time to produce the hormones necessary for natural pain relief, and is left alone with contractions, much stronger than those that should be at the beginning of childbirth. And anesthesia in childbirth is always harmful to the child. The safest for him epidural anesthesia does not allow the mother to push properly, because she does not feel her body - which means that the likelihood that the child will be pulled with forceps or vacuum increases, which guarantees injuries, usually cephalohematomas. We repeat that there are cases when anesthesia is necessary, but not as often as it is carried out, not for everyone! The same applies to the notorious episiotomy - an incision in the perineum, which until recently was done to almost all women in labor during the period of attempts.
We repeat that there are cases when anesthesia is necessary, but not as often as it is carried out, not for everyone! The same applies to the notorious episiotomy - an incision in the perineum, which until recently was done to almost all women in labor during the period of attempts.
There are times when a perineal incision is necessary, for example, if the child's heartbeat indicates a state of hypoxia. If there is no need to speed up labor, then episiotomy is not needed. As a rule, with extremely rare exceptions, the size of the woman's vagina corresponds to the size of the baby's head.
In addition, perineal tears heal more easily and faster than cut tissues. Not to mention the fact that during normal, calm childbirth, perineal tears are quite rare - the tissues of the perineum have time to stretch, they are quite elastic, but this takes time. In addition, there are special techniques for protecting the perineum from ruptures that midwives must master. As a result, unnecessary medical intervention during childbirth can create many problems for both mother and child. When these are side effects of the necessary medical care - this is one thing, and when the birth would have gone better without such "help" - this makes one think about the need for such "help". As the saying goes, "don't take care of me so fiercely."
When these are side effects of the necessary medical care - this is one thing, and when the birth would have gone better without such "help" - this makes one think about the need for such "help". As the saying goes, "don't take care of me so fiercely."
So, natural childbirth is childbirth without unnecessary and unnecessary medical intervention. We repeat that all these medical procedures may be necessary for a woman in labor or a fetus - and then their use will be evaluated in a completely different way. The point now is that healthy childbirth takes place at such a speed as planned by nature, and not at the speed the doctor wants. And only such childbirth can be called natural. Another important point. During such childbirth, a woman should be able to take a comfortable body position for her at any stage of childbirth.
This does not mean that we should put an equal sign between natural and vertical births. Yes, the vertical position of the woman in labor most often turns out to be optimal - but it happens differently. It is better for someone to walk, someone to sit, someone to lie on their side. And lifting a woman who needs to lie down is a restriction of her freedom, which means that it is the same deviation from the natural course of childbirth, as is the position lying on her back, which is mandatory for everyone. However, as a rule, childbirth goes better in an upright position - but it should be chosen by the woman herself with the help of a doctor or midwife. If the position is chosen correctly both in contractions and in attempts, anesthesia is almost never required.
It is better for someone to walk, someone to sit, someone to lie on their side. And lifting a woman who needs to lie down is a restriction of her freedom, which means that it is the same deviation from the natural course of childbirth, as is the position lying on her back, which is mandatory for everyone. However, as a rule, childbirth goes better in an upright position - but it should be chosen by the woman herself with the help of a doctor or midwife. If the position is chosen correctly both in contractions and in attempts, anesthesia is almost never required.
Childbirth involves maximum psychological comfort for the woman in labor. As a rule, to achieve it, it is necessary that a close person is next to the woman during childbirth - most often this is the father of the child, but maybe it will be the mother of the woman in labor or her close friend. Even if a woman does not want her partner to see the process of childbirth directly, it is unlikely that at least one woman will refuse the help of her husband at the stage of contractions - the most difficult and longest stage of childbirth.
The psychological mood of a woman is very important for the natural course of childbirth. If a woman in labor perceives herself as a patient who needs medical attention, then it is hardly possible to talk about natural childbirth. And vice versa, when a woman is prepared - physically, psychologically, knows what is happening to her and her child, knows how she can help herself, childbirth will go easier. On the other hand, the opposite point is important: during childbirth, the head with all its knowledge should be turned off as much as possible. The woman in labor must surrender herself to the flow of labor, completely relax and not think about how she looks, or about how far the cervix has dilated - about anything other than her baby.
No one is saying that natural childbirth is childbirth without pain. No, but the pain does not start suddenly and does not exceed the limit that a woman can endure without the use of painkillers. The role of anesthesia is played by hormones that are produced by the body during childbirth, the correct breathing of a woman, relaxation, a well-formed sound - not a heart-rending cry, but rather singing. All this comes by itself, if the woman in labor is not in a panic, if she is relaxed. Therefore, to relax, completely and completely, you need to learn before giving birth. Many, unfortunately, believe that natural childbirth flows by itself, and there is no need to prepare for it in any way. This is a gross and harmful mistake for a woman in labor.
All this comes by itself, if the woman in labor is not in a panic, if she is relaxed. Therefore, to relax, completely and completely, you need to learn before giving birth. Many, unfortunately, believe that natural childbirth flows by itself, and there is no need to prepare for it in any way. This is a gross and harmful mistake for a woman in labor.
If a woman knows what happens to her and the baby during childbirth, knows the techniques of breathing, relaxation, imagines in detail what she will do and in what case, then it will be much easier for her to calm down and surrender to the process of giving birth to a new life. Therefore, natural childbirth must begin with a healthy pregnancy, during which the woman, alone or with her husband, attends special courses or childbirth preparation schools. Many of these courses target pregnant couples specifically for a gentle birth.
Natural childbirth should also end naturally. This means that immediately after the birth of the child, it is placed on the mother's stomach so that the skin-to-skin contact necessary for both occurs, then the mother puts the baby to the breast.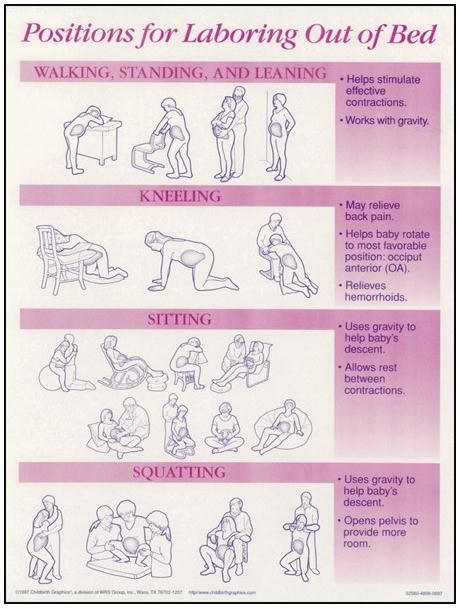 The umbilical cord is also not cut immediately, but only after it stops pulsing - this is necessary so that all the blood that circulates between the baby and the placenta passes into the baby's body. Natural childbirth also implies that after childbirth and postpartum treatment, mother and baby are together and may not part even for the night. Most often, a baby born as a result of natural childbirth also receives natural feeding from the very first hours of life.
The umbilical cord is also not cut immediately, but only after it stops pulsing - this is necessary so that all the blood that circulates between the baby and the placenta passes into the baby's body. Natural childbirth also implies that after childbirth and postpartum treatment, mother and baby are together and may not part even for the night. Most often, a baby born as a result of natural childbirth also receives natural feeding from the very first hours of life.
Therefore, speaking of such childbirth, we repeat that this is not just a childbirth without medical manipulations. This is a fundamentally different attitude to childbirth - as a natural process that should lead to the birth of a healthy baby.
Natural childbirth is not an end in itself, it is the next step after a healthy and proper pregnancy to ensure that the baby, who has long been loved and desired, is healthy and happy.
Source: Maternity hospitals in Moscow and the region
Stimulation of labor activity or induction of labor
The purpose of this information material is to familiarize the patient with the induction of labor procedure and to provide information on how and why it is performed.
In most cases, labor begins between the 37th and 42nd weeks of pregnancy. Such births are called spontaneous. If drugs or medical devices are used before the onset of spontaneous labor, then the terms "stimulated" or "induced" labor are used in this case.
Labor should be induced when further pregnancy is for some reason unsafe for the mother or baby, and it is not possible to wait for the onset of spontaneous labor.
The purpose of stimulation is to start labor by stimulating uterine contractions.
When inducing labor, the patient must be in the hospital so that both mother and baby can be closely monitored.
Labor induction methods
The choice of labor induction method depends on the maturity of the cervix in the patient, which is assessed using the Bishop scale (when viewed through the vagina, the position of the cervix, the degree of its dilatation, consistency, length, and the position of the presenting part of the fetus in the pelvic area are assessed). Also important is the medical history (medical history) of the patient, for example, a past caesarean section or operations on the uterus.
Also important is the medical history (medical history) of the patient, for example, a past caesarean section or operations on the uterus.
The following methods are used to induce (stimulate) labor:
- Oral misoprostol is a drug that is a synthetic analogue of prostaglandins found in the body. It prepares the body for childbirth, under its action the cervix becomes softer and begins to open.
- Balloon Catheter – A small tube is placed in the cervix and the balloon attached to the end of the tube is filled with fluid to apply mechanical pressure to the cervix. When using this method, the cervix becomes softer and begins to open. The balloon catheter is kept inside until it spontaneously exits or until the next gynecological examination.
- Amniotomy or opening of the fetal bladder - in this case, during a gynecological examination, when the cervix has already sufficiently dilated, the fetal bladder is artificially opened. When the amniotic fluid breaks, spontaneous uterine contractions will begin, or intravenous medication may be used to stimulate them.
- Intravenously injected synthetic oxytocin - acts similarly to the hormone of the same name produced in the body. The drug is given by intravenous infusion when the cervix has already dilated (to support uterine contractions). The dose of the drug can be increased as needed to achieve regular uterine contractions.
When is it necessary to induce labor?
Labor induction is recommended when the benefits outweigh the risks.
Induction of labor may be indicated in the following cases:
- The patient has a comorbid condition complicating pregnancy (eg, high blood pressure, diabetes mellitus, preeclampsia, or some other condition).
- The duration of pregnancy is already exceeding the norm - the probability of intrauterine fetal death increases after the 42nd week of pregnancy.
- Problems related to the fetus, for example, problems with the development of the fetus, abnormal amount of amniotic fluid, changes in the condition of the fetus, various diseases in the fetus.

- If the amniotic fluid has broken and uterine contractions have not started within the next 24 hours, there is an increased risk of inflammation in both the mother and the fetus. This indication does not apply in case of preterm labor, when preparation of the baby's lungs with a special medicine is necessary before delivery.
- Intrauterine fetal death.
What are the risks associated with labor induction?
Labor induction is not usually associated with significant complications.
Occasionally, after receiving misoprostol, a patient may develop fever, chills, vomiting, diarrhea, and too frequent uterine contractions (tachysystole). In case of too frequent contractions to relax the uterus, the patient is injected intravenously relaxing muscles uterus medicine. It is not safe to use misoprostol if you have had a previous caesarean section as there is a risk of rupture of the uterine scar.