Aversion breech baby
External cephalic version (ECV) | Pregnancy Birth and Baby
External cephalic version (ECV) | Pregnancy Birth and Baby beginning of content4-minute read
Listen
Giving birth is more challenging for babies who are bottom-down, or breech, when labour starts. This page explains external cephalic version (ECV), which tries to turn breech babies to the head-down position ready for a normal vaginal birth.
The breech position
Throughout your pregnancy, your baby repeatedly turns around and changes position. Most babies will settle into a head-down, or 'cephalic', position by 36 weeks of pregnancy. But about 3 in 100 babies are in a breech position at 36 weeks. For these babies, birth would be more difficult than if they were in the cephalic position.
Some breech babies turn naturally in the last month of pregnancy. If this is your first baby, the chance of the baby turning itself after 36 weeks is about 1 in 8. If this is your second or subsequent baby, the chance is about 1 in 3.
If your baby is still in a breech position at 36 weeks, your doctor or midwife might suggest you consider an external cephalic version, or ECV. The aim is to turn your baby so that it is head-down when labour starts.
An ECV is performed after 37 weeks of pregnancy.
Can anyone have an ECV?
Most women can have an ECV if they have a healthy pregnancy with a normal amount of amniotic fluid. However, an ECV is not recommended if:
- you need a caesarean for other reasons
- you have had vaginal bleeding in the previous 7 days
- the baby's heart rate is not normal
- a complicated pregnancy
- you are having twins or triplets
- you have an unusually shaped uterus
- you recently had vaginal bleeding
- you have placenta praevia (your placenta is growing close to, or on, your cervix)
- other health conditions, like high blood pressure or diabetes
ECV might also not be recommended if your unborn baby is unwell or not growing well.
If you have had a caesarean section before, an ECV can still be performed but there are special considerations that need to be discussed with your doctor.
How is an ECV performed?
A health professional with appropriate expertise, usually an obstetrician, puts their hands on your abdomen to try to turn your baby into a head-down position.
A cardiotocograph, or CTG, will monitor your baby’s wellbeing for 20 to 30 minutes before the procedure.
A small needle will be inserted into your hand so that medication to relax your uterus can be administered directly into your vein.
An obstetrician will then perform an ultrasound to confirm the position of the baby, and then attempt to turn the baby by pressing their hands firmly on your abdomen. Some women find this uncomfortable, while others don’t. The pressure on your abdomen lasts a few minutes. If the first attempt is unsuccessful, the obstetrician might try again.
The CTG might be applied again after the procedure to assess your baby’s wellbeing before you leave.
It usually takes about 3 hours from start to finish.
Where would I have an ECV?
Although complications from an ECV are rare, it is recommended that the procedure is done by an experienced health professional, in a hospital where there are facilities for emergency caesarean section. About 1 in 1,000 women go into labour after an ECV. About 1 in 200 women need an immediate caesarean section.
Will ECV work?
ECV can work, although there is no guarantee of success. If it does work, there is a small chance the baby will turn again to the breech position. But overall, ECV improves a woman’s chances of having a vaginal birth.
What happens if ECV doesn’t work?
A vaginal birth may still be possible, depending on your individual clinical circumstances and the type of breech position your baby is in. Talk to your doctor or midwife about your options.
What other methods are there to potentially turn my baby from a breech position?
Some people think that you might be able to encourage your baby to turn by holding yourself in certain positions, such as kneeling with your bottom in the air and your head and shoulders flat to the ground. Other options you might hear include acupuncture, a Chinese herb called moxibustion and chiropractic treatment. There is no good evidence that these work. Discuss with your doctor or midwife before having any treatment during pregnancy.
Other options you might hear include acupuncture, a Chinese herb called moxibustion and chiropractic treatment. There is no good evidence that these work. Discuss with your doctor or midwife before having any treatment during pregnancy.
Sources:
Mater Hospital Brisbane (Pregnancy: External Cephalic Version), Royal Australian and New Zealand College of Obstetricians and Gynaecologists (Breech Presentation at the End of your Pregnancy), BioMed Central (Does moxibustion work? An overview of systematic reviews (BMC Research Notes 20103:284)), Department of Health (Clinical practice guidelines: Pregnancy care), SA Department for Health and Ageing (Perinatal practice guideline: Breech presentation), NSW Health (External Cephalic Version (ECV) for Breech Presentation)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: April 2020
Back To Top
Related pages
- Breech birth
- Breech pregnancy
Need more information?
External Cephalic Version for Breech Presentation - Maternal, child and family health
This information brochure provides information about an External Cephalic Version (ECV) for breech presentation
Read more on NSW Health website
Breech presentation and turning the baby
In preparation for a safe birth, your health team will need to turn your baby if it is in a bottom first ‘breech’ position.
Read more on WA Health website
Breech pregnancy
When a baby is positioned bottom-down late in pregnancy, this is called the breech position.
Read more on Pregnancy, Birth & Baby website
Labour complications
Even if you’re healthy and well prepared for childbirth, there’s always a chance of unexpected problems. Learn more about labour complications.
Read more on Pregnancy, Birth & Baby website
Malpresentation
Malpresentation is when your baby is in an unusual position as the birth approaches. Sometimes it’s possible to move the baby, but a caesarean maybe safer.
Read more on Pregnancy, Birth & Baby website
Pregnancy at week 35
You'll probably be having lots of Braxton Hicks contractions by now. It's your body's way of preparing for the birth. They should stop if you move position.
They should stop if you move position.
Read more on Pregnancy, Birth & Baby website
Anatomy of pregnancy and birth - pelvis
The pelvis helps carry your growing baby and is especially tailored for vaginal births. Learn more about the structure and function of the female pelvis.
Read more on Pregnancy, Birth & Baby website
Rhesus D negative in pregnancy
Find out what being Rhesus D negative could mean for your baby and how it is treated.
Read more on Pregnancy, Birth & Baby website
Placental abruption - Better Health Channel
Placental abruption means the placenta has detached from the wall of the uterus, starving the baby of oxygen and nutrients.
Read more on Better Health Channel website
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now entering.
OKNeed further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.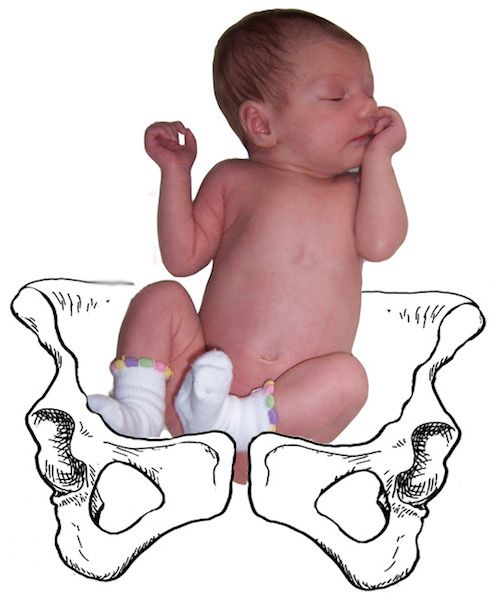
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
What Is External Cephalic Version (ECV)?
Written by Danny Bonvissuto
Reviewed by Nivin Todd, MD on August 25, 2022
In this Article
- What Is External Cephalic Version?
- External Cephalic Version Procedure
- Does ECV Hurt?
- External Cephalic Version Risks
- External Cephalic Version Success
- Are There Possible Complications From an ECV?
- External Cephalic Version Alternatives
What Is External Cephalic Version?
External cephalic version, or ECV, is a maneuver your doctor may use when your unborn baby is set up to come out bottom first or feet first. Those positions are called a breech birth, and they can make a vaginal birth more difficult. With an ECV, your doctor turns the baby into a headfirst, or cephalic, position toward the opening of the birth canal.
Those positions are called a breech birth, and they can make a vaginal birth more difficult. With an ECV, your doctor turns the baby into a headfirst, or cephalic, position toward the opening of the birth canal.
External Cephalic Version Procedure
It’s usually done by your obstetrician. Your baby's heartbeat will be monitored for about a half-hour before the ECV. In some cases, you may get medicine through an IV to relax your uterus. This won't affect your baby.
Then, by pressing their hands on the outside of your belly, your doctor will try to turn your baby. The goal is to get your baby to do a little flip in your womb and finish up head-down. This can take several hours.
Your doctor may use an ultrasound to check your baby's position and guide the process.
Does ECV Hurt?
To turn your baby, your doctor will use firm pressure. Everyone reacts differently, so you might feel discomfort or pain. Many women go through an ECV without any painkillers. But your doctor may give you an epidural or other pain medication or even put you to sleep during the procedure.
But your doctor may give you an epidural or other pain medication or even put you to sleep during the procedure.
External Cephalic Version Risks
An ECV isn't right for you if you're expecting more than one baby or you need a C-section.
It also works best on women with a pear-shaped womb and not those with a heart-shaped womb, called a bicornuate uterus.
Other reasons your doctor might tell you not to get an ECV are:
- You have vaginal bleeding within 7 days of the procedure.
- Your baby has an abnormal heartbeat or health problems.
- Your water has broken.
- Your baby is larger than average.
- Your amniotic fluid levels are too low or too high.
- Your baby’s head is hyperextended, meaning it’s straight instead of bending forward.
- You have a heart problem or a placenta previa, which can cause severe bleeding during pregnancy and delivery.
ECVs are usually safe, but there are some risks. In rare cases, it can cause changes in your baby's heart rate, tearing of the placenta, and preterm labor.
The procedure is usually done near a delivery room in case you need an emergency C-section.
External Cephalic Version Success
ECVs work about half the time. If your doctor can't get your baby to flip after the first attempt, they may try again after a week or so.
The odds of success are higher if:
- The ECV is attempted soon after 36 weeks of pregnancy, before the baby grows too large.
- You’ve given birth before.
- There is enough amniotic fluid surrounding the baby.
Things that can lower the chances that an ECV will work include:
- The baby has dropped to your pelvis.
- Your uterus is tense or hard.
- Your doctor has trouble touching and feeling your baby’s head.
After a successful ECV, babies flip to the headfirst position, then flip back to breech. And sometimes breech babies flip on their own before birth, though the bigger they get, the less room there is to move.
Doctors deliver most breech babies by C-section. A vaginal birth may still be possible, depending on your health, your baby's health, and their position. Ask your doctor about your options.
A vaginal birth may still be possible, depending on your health, your baby's health, and their position. Ask your doctor about your options.
Are There Possible Complications From an ECV?
After a successful ECV, most women go on to have normal vaginal births. But call your doctor right away if you have contractions, bleeding, or you don't feel your baby moving the way you did before the procedure.
External Cephalic Version Alternatives
If an ECV can’t get your baby into a headfirst position, you have other options for giving birth. They may include:
- Deliver the baby vaginally in breech position
- Have your baby by C-section (this is less risky than a vaginal birth)
The problem of breech presentation of the fetus. External obstetric rotation of the fetus on the head.
Breech presentation of the fetus occurs in 3% -5% of cases at full-term pregnancy. Vaginal delivery with breech presentation is associated with high risks both on the mother's side and on the fetus's side. Thus, breech presentation is currently considered pathological, even if the conditions necessary for childbirth through the birth canal are ideally met, and the fetus is relatively small relative to the size of the mother's pelvis. During vaginal delivery, the arms and head of the fetus may tilt back, which can lead to injury.
Thus, breech presentation is currently considered pathological, even if the conditions necessary for childbirth through the birth canal are ideally met, and the fetus is relatively small relative to the size of the mother's pelvis. During vaginal delivery, the arms and head of the fetus may tilt back, which can lead to injury.
Currently the most common method of delivery in breech presentation is a caesarean section (90%). Among the indications for the use of caesarean section, breech presentation ranks third among others in the world. However, this the operation does not make it possible to completely eliminate the risk of trauma to the fetus, since when it is removed, it is also possible to tilt the arms and head of the fetus, and their release requires the use of complex manipulations.
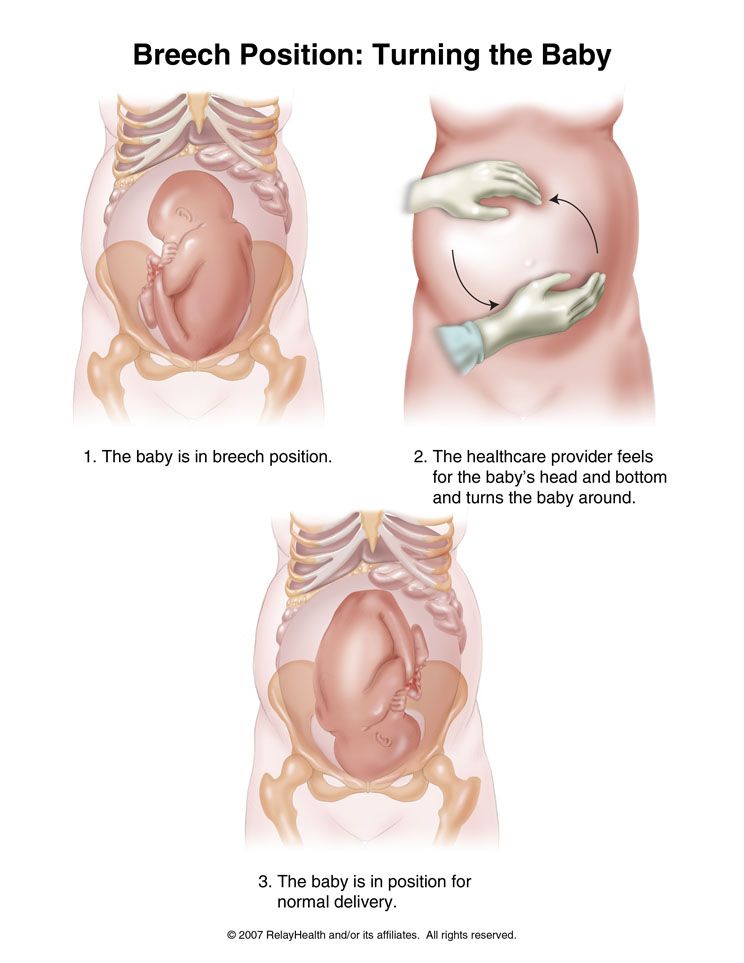
To correct breech presentation today, the world is using EXTERNAL OBTETAL TURNING OF THE FETUS ON THE HEAD proposed at the end the century before last by the Russian obstetrician Arkhangelsky B. A.
A.
External obstetric cephalic rotation (EFRT) is a procedure during which the doctor turns the fetus from the outside through the wall of the uterus breech presentation in the head. A successful attempt at NAPP allows women to give birth on their own, avoiding a caesarean section.
What is required for external cephalic fetal rotation?
External obstetric rotation of the fetus on the head is performed before the onset of labor, usually starting from 36 weeks of pregnancy.
It is necessary to consult a doctor and conduct an ultrasound examination to confirm the fact breech presentation of the fetus and determine the conditions for NAPP, starting from 34-35 weeks of pregnancy.
| The operation of external rotation of the fetus on the head in breech presentation |
When NAPP is possible:
- From 36 to 37 weeks, since with earlier use, it is likely that it will return to the breech presentation.

- In the presence of a singleton pregnancy.
- Subject to the mobility of the buttocks of the fetus (if they are tightly pressed against the entrance to the mother's pelvis, it will be extremely difficult to change the position of the fetus).
- Sufficient amount of amniotic fluid. With oligohydramnios, this manipulation can be traumatic for the fetus, while with polyhydramnios there is a high probability of a reverse rotation of the fetus in a breech presentation.
- Sufficient amount of amniotic fluid. With oligohydramnios, this manipulation can be traumatic for the fetus, while with polyhydramnios there is a high probability of a reverse rotation of the fetus in a breech presentation.
- Fetal head flexed
When NAPP is not possible:
- With the outflow of amniotic fluid.
- If the patient has contraindications to the use of drugs used to relax the uterus (tocolysis).
- In the presence of obstetric indications or indications from the health of the mother for delivery by caesarean section.
- With the extensor position of the fetal head.
- If the fetus has congenital developmental features.
- With multiple pregnancy.
- In the presence of structural features of the uterus in a pregnant woman
However, in addition to this, there are a number of factors that may favor or, on the contrary, serve as a contraindication to external obstetric turning the fetus on the head, and which can only be determined by a doctor during a direct examination of a pregnant woman.
How NAPP is conducted
For manipulation, hospitalization in the maternity hospital is necessary. Preliminarily, an additional examination of the pregnant woman is carried out in the required volume, including ultrasound.
During the NAPP:
Immediately before the start of the manipulation, a CTG is recorded to assess the condition of the fetus.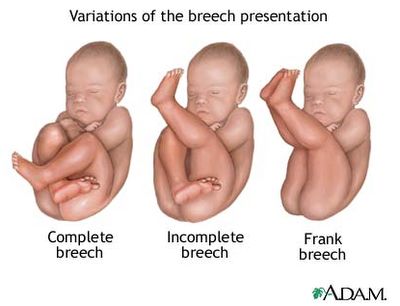
Drugs are administered to prevent uterine contractions (tocolytics).
Further, under constant ultrasound and KGT control, as well as the continued administration of drugs that relax the uterus, the doctor performs a turn.
Holding both hands on the surface of the pregnant woman's abdomen, one on the head of the fetus, and the other on the buttocks of the fetus, the doctor pushes and rotates the fetus to the upside down position. A pregnant woman may feel some discomfort during the procedure. The degree of discomfort depends on the individual sensitivity of each patient.
After the procedure is successfully completed, the CTG is recorded again, to make sure that the fetus feels well and has successfully undergone the procedure. Usually during the day, the condition of the mother and fetus is monitored, after which the patient is discharged and continues the pregnancy until spontaneous delivery occurs.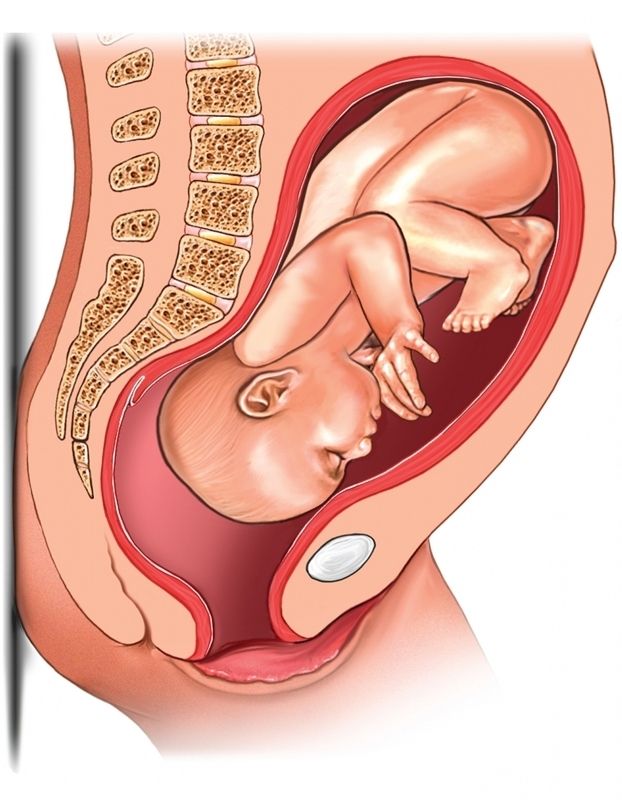
If the doctor notices a deterioration in the condition of the fetus according to the monitoring data, then the procedure is immediately stopped.
If the first attempt was not successful, your doctor may suggest another attempt if the fetus is in good health.
APP is performed ONLY in a maternity ward where there is an opportunity for an emergency delivery, if necessary.
Risks associated with NAPP
Subject to constant monitoring of the condition of the fetus, constant tocolysis (administration of drugs that relax the uterus) The risks associated with this procedure are minimal. Complications from its use occur in less than 1-2% of cases.
Complications of NAPP include:
- compression or "twisting" of the umbilical cord. In this case, constant monitoring of the condition of the fetus allows you to immediately fix its deterioration and stop the procedure.
- discharge of amniotic fluid or the development of labor. This complication can be considered relative, since the rotation in most cases is carried out at full-term pregnancy.
This complication can be considered relative, since the rotation in most cases is carried out at full-term pregnancy.
Any deviation from the normal course of the procedure serves as a reason to stop the manipulation and decide on the choice of further management tactics.
Carrying out NAPP with Rh-negative mother's blood.
The presence of Rh isoimmunization (that is, the presence of anti-Rh antibodies in the mother's blood) is a contraindication to this procedure, as it increases the risk of anemia in the fetus.
In the absence of isoimmunization (absence of anti-Rhesus antibodies) it is possible to carry out NAPP with prophylaxis by introducing anti-Rhesus immunoglobulin.
If you have a breech presentation of the fetus and you want to know about further options for pregnancy management, delivery, external obstetric rotation of the fetus on the head, the presence of indications and contraindications for its implementation, please consult our specialists.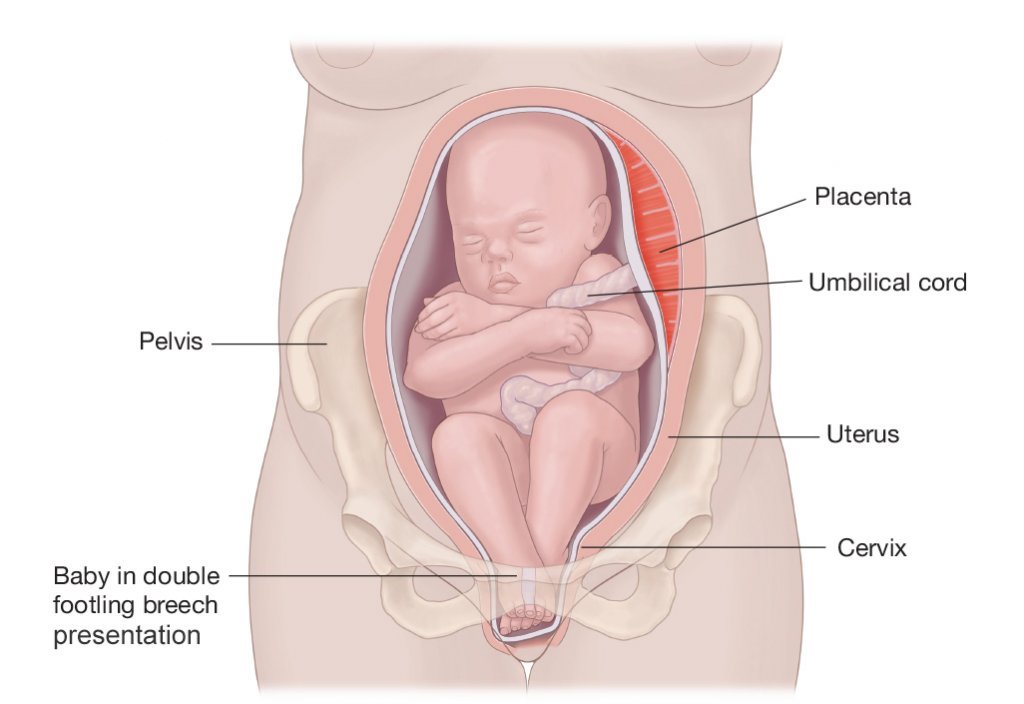
Breech presentation of the fetus: signs, diagnosis
Consultation with a specialist:
Breech presentation of the fetus is one of the options for the location of the child in the womb. In this case, the fetus, as it were, "sits" in the uterus, and its head is directed upwards. Normally, breech presentation is observed up to 32 weeks, after this period such an arrangement of the fetus is considered pathological.
Only a gynecologist can determine the breech presentation during an examination or according to the results of an ultrasound scan. If the baby is positioned incorrectly, the doctor may prescribe special exercises or manipulations to correctly position the fetus.
To determine whether the baby has taken the correct position for childbirth, it is necessary to undergo an examination by a gynecologist and ultrasound at 32-34 weeks.
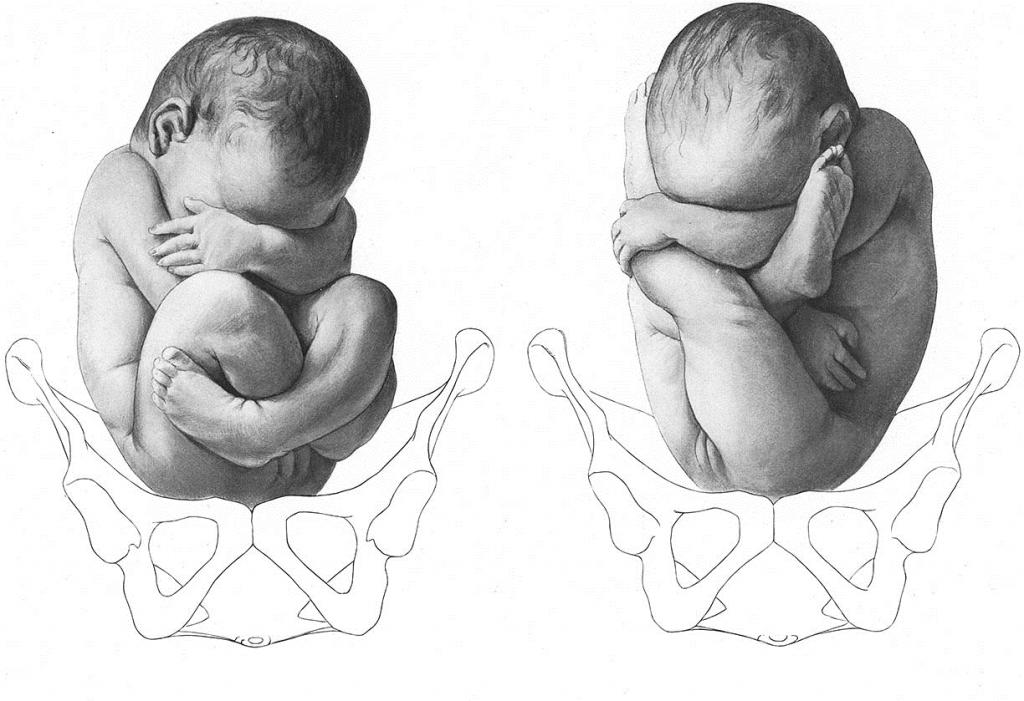
Types of breech presentation of the fetus
Breech presentation of the fetus is divided into types:
- gluteal;
- foot.
In breech presentation of the fetus during childbirth, the baby's buttocks are the first to appear. At the same time, its legs are located along the body and straightened at the knees. In such a situation, we can say that the woman is lucky, since in this case she practically does not need additional help, and the risk of complications is reduced to a minimum. With a mixed breech presentation, the legs and pelvis may appear at the same time.
Foot presentation is considered more unfavorable. According to statistics, up to 15% of children with breech presentation are born this way. In the foot position, the first of the birth canals are the legs, not the pelvis. Usually in the case of a foot presentation, a caesarean section is performed.
Call now
+7 (495) 215-56-90
Make an appointment
Causes of breech presentation
The reasons that caused the pelvic presentation of the fetus can be quite a lot, but the most common are:
- polyhydramnios - usually in this case, the baby is highly mobile and simply does not have time to take the desired position by the time of birth;
- oligohydramnios - in this case, the child's ability to change his position is limited, as a result of which the baby simply cannot take a physiological position;
- twin pregnancy - in this case, it is very difficult for babies to move due to lack of space, it is worth noting that the "traditional" head presentation of the fetus in multiple pregnancy is rare regardless of the week of pregnancy;
- entanglement with the umbilical cord - sometimes a very active baby can wrap the umbilical cord around himself so much that it becomes completely impossible for him to take the correct position for childbirth;
- pathology of the uterus - some diseases of the uterus (for example, fibroids) can directly affect the position of the fetus.

In some cases, in the presence of the problems described above, the breech presentation of the fetus can threaten the following dangers:
- premature birth;
- hypoxia - if the child in the gluteal position pinched the umbilical cord;
- difficult delivery with the risk of injury to both mother and child..
Breech diagnosis
It is almost impossible to independently suspect a breech presentation of the fetus without understanding obstetrics and gynecology. In addition, such a situation before a certain period should not bother the expectant mother at all. Usually, the first symptoms of breech presentation in the uterus are determined by the obstetrician at the examination at 32-34 weeks. In this case, the doctor pays attention to the area where the child's heartbeat is heard and palpates the abdomen. In the event that the symptoms indicate a breech presentation of the fetus, the specialist will prescribe an additional examination that will either confirm or refute his conclusion.
There are several ways that experienced obstetricians resort to in order to determine the presence of a breech presentation in a fetus.
- First, it is a visual inspection and palpation of the abdomen. Usually, it is not difficult for a specialist to determine the position where the child's head is and where his feet are. In addition, the obstetrician may resort to listening to the heart. If his sounds are heard above the navel, then the child is in a breech presentation. This is the simplest and most affordable method of research and diagnosis.
- Secondly, the obstetrician can determine the presentation of the fetus and the location of the head at the time of the onset of labor. Usually, this method is resorted to if a woman goes into labor urgently and she has no data on previous examinations, and on the position of the fetus - pelvic or head. In this case, the specialist probes the position of the child through the vagina.
- Thirdly, ultrasound is considered the surest and most reliable way.
 It is best to perform an ultrasound scan in breech presentation at 32-34 weeks, when the baby takes its final position.
It is best to perform an ultrasound scan in breech presentation at 32-34 weeks, when the baby takes its final position.
Treatment
In fact, in the absence of pathology, breech presentation of the fetus is not some kind of terrible diagnosis that needs to be feared. In addition, in some cases, correcting such a situation can be quite simple.
Remember that any exercises and manipulations aimed at giving the child the desired position must be fully coordinated with the specialist. Otherwise, you risk causing irreparable harm to the unborn baby.
- Exercise "Turns". To turn, lie on your back and bend your knees slightly. After that, you need to smoothly turn on your side and lie down in this position for about 2 minutes. Then the manipulation must be repeated, but on the other side. The number of repetitions in such an exercise should not exceed 8-10.
- Butt lift exercise. This exercise is contraindicated in women with placenta previa or with a scar on the uterus.