2 month old baby skull
Your Baby's Head - HealthyChildren.org
Log in | Register
Ages & Stages
Ages & Stages
Listen
Español
Text Size
By Laura Jana, MD, FAAP & Jennifer Shu, MD, FAAP
Many parents have been mistakenly led to believe that all newborns are born picture-perfect, with pretty little round heads. Let us just say that for anyone who has gone through or will experience vaginal delivery, it is nothing short of a blessing that a baby’s skull is made up of soft bony plates that are capable of compressing and overlapping to fit through the narrow birth canal—a process referred to as molding.
Shaping up
For some babies—such as those who "drop" well in advance of being born (in other words, settle themselves head first deep into their mother’s pelvis well in advance of delivery), or those who must endure long labors and narrow birth canals—the result is often a newborn head shape that more closely resembles a cone than a nice round ball.
If you run your fingers over your newborn’s skull, you may also find that you can feel ridges along the areas where the bony plates of the skull have overlapped. In short, slightly misshapen heads are quite common right after birth.
Fortunately, over the next several weeks the bones of your baby’s skull will almost assuredly round out and the ridges will disappear—assuming, that is, that your baby doesn’t spend too much time on their back with his head in any one position. This is a common but easily avoidable cause for the development of a flat back or side of the head known as plagiocephaly.
The soft spot
You will notice one to two areas on your baby’s head that seem to be lacking bony protection. These soft spots, referred to as fontanelles (anterior for the larger one in the front, posterior for the smaller and typically less noticeable one in the back), are normal gaps in a newborn’s skull that will allow your baby’s brain to grow rapidly throughout the next year.
Many parents are afraid to touch these soft spots, but you can rest assured that, despite their lack of a bony layer, they are well protected from typical day-to-day baby handling. Other things to know about the soft spot(s) include:
- In young infants, a sunken soft spot (when combined with poor feeding and dry diapers) can suggest dehydration. Our advice to you: Don’t read too much into this because it can be a subtle finding or sometimes be present in normal babies. Instead, make sure you have a good grasp on how to recognize dehydration and check with your doctor if you have any concerns—with or without a sunken soft spot.
- In some instances, the soft spot on the top of your baby’s head may seem to be pulsating. There is no need to worry—this movement is quite normal and simply reflects the visible pulsing of blood that corresponds to your baby’s heartbeat.
Bumps & bruises
In addition to molding, a bit of swelling or bruising of the scalp immediately following delivery is not uncommon for newborns. The swelling usually is most noticeable at the top back part of the head and is medically referred to as a caput (short for caput succedaneum). When bruising of the head occurs during delivery, the result can be a boggy-feeling area, called a cephalohematoma.
The swelling usually is most noticeable at the top back part of the head and is medically referred to as a caput (short for caput succedaneum). When bruising of the head occurs during delivery, the result can be a boggy-feeling area, called a cephalohematoma.
Bruising and swelling are usually harmless and go away on their own over the first days and weeks, but can be a contributing factor for jaundice.
Gone today, but hair tomorrow
Sure, babies are sometimes born with full heads of hair, but it’s far more likely for them to be born with little to none. And those with hair today are likely to find it gone tomorrow. That’s because any hair your baby is born with is likely to thin out significantly over the next few months before ultimately being replaced with "real" hair. It is also entirely possible that whatever hair your newborn does have will change color by several shades and several times over their lifetime.
More information
- How Your Newborn Looks
- Uneven Head Shape in Babies: Causes and Treatment of Craniosynostosis
About Dr.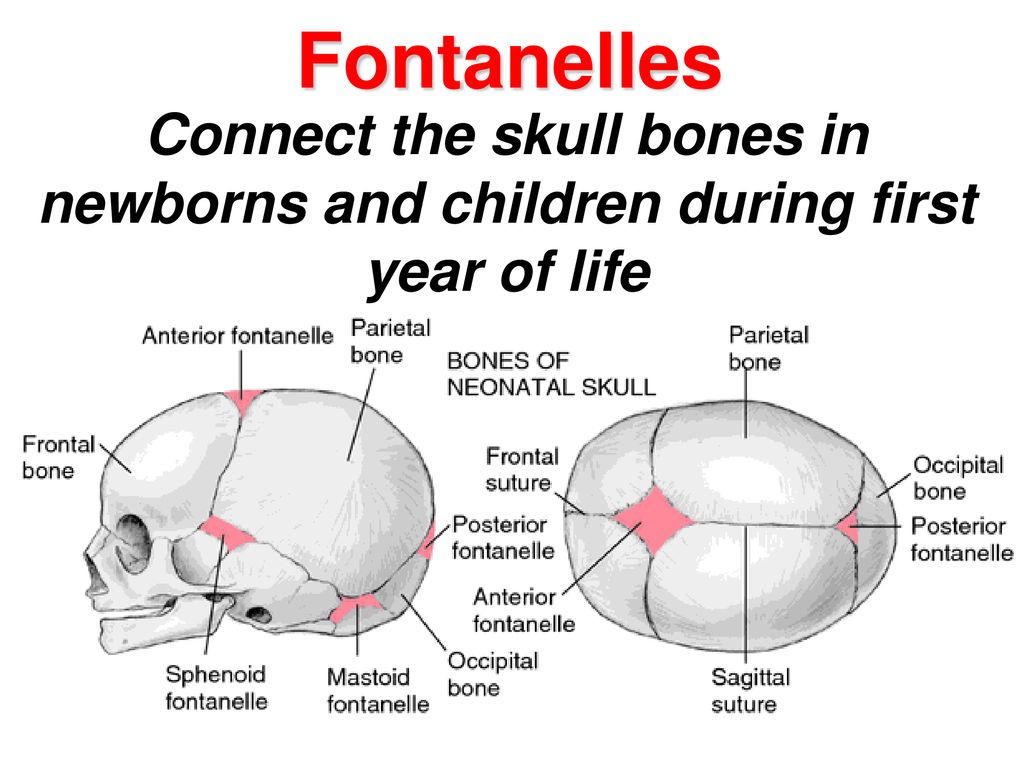 Jana JanaLaura A. Jana, MD, FAAP, is a pediatrician and mother of 3 with a faculty appointment at the Penn State University Edna Bennett Pierce Prevention Research Center. She is the author of more than 30 parenting and children's books and serves as an early childhood expert/contributor for organizations including the Maternal and Child Health Bureau, Primrose Schools, and US News & World Report. She lives in Omaha, NE. |
About Dr. ShuJennifer Shu, MD, FAAP serves as the medical editor of HealthyChildren.org and provides oversight and direction for the site in conjunction with the staff editor. Dr. Shu is a practicing pediatrician at Children's Medical Group in Atlanta, Georgia, and she is also a mom. She earned her medical degree at the Medical College of Virginia in Richmond and specialized in pediatrics at the University of California, San Francisco. Her experience includes working in private practice, as well as working in an academic medical center. |
 She served as director of the normal newborn nursery at Dartmouth-Hitchcock Medical Center in New Hampshire. Dr. Shu is also co-author of Food Fights and Heading Home with Your Newborn published by the American Academy of Pediatrics.
She served as director of the normal newborn nursery at Dartmouth-Hitchcock Medical Center in New Hampshire. Dr. Shu is also co-author of Food Fights and Heading Home with Your Newborn published by the American Academy of Pediatrics.- Last Updated
- 12/31/2021
- Source
- Heading Home With Your Newborn, 4th Edition (Copyright 2020 American Academy of Pediatrics)
The information contained on this Web site should not be used as a substitute for the medical care and advice of your pediatrician. There may be variations in treatment that your pediatrician may recommend based on individual facts and circumstances.
About the fontanelle | Pregnancy Birth and Baby
About the fontanelle | Pregnancy Birth and Baby beginning of content5-minute read
Listen
What is a fontanelle?
A fontanelle is a ‘soft spot’ of a newborn baby’s skull. It is a unique feature that is important for the normal growth and development of your baby’s brain and skull. Your health team will check your baby’s fontanelles during routine visits.
It is a unique feature that is important for the normal growth and development of your baby’s brain and skull. Your health team will check your baby’s fontanelles during routine visits.
If you touch the top of your baby’s head you can feel a soft spot in between the bones — this is a fontanelle.
A newborn baby’s skull is made up of sections of bone known as plates that are joined together by fibrous joints called sutures. The sutures provide some flexibility and allow your baby’s head to narrow slightly as it travels through the birth canal. The sutures also enable your baby’s head to grow in the first years of life.
There are 2 fontanelles on your baby’s skull. These are the skin-covered gaps where the skull plates meet. The anterior fontanelle is at the top of your baby’s head, and the posterior fontanelle is located at the back of your baby’s head.
Illustration showing the anterior and posterior (front and back) fontanelles of a baby's skull.When will my baby’s fontanelles close?
The posterior fontanelle usually closes by the time your baby is 2 months old. The anterior fontanelle can close any time between 4 and 26 months of age. Around 1 in every 2 babies will have a closed fontanelle by the time they are 14 months old.
The anterior fontanelle can close any time between 4 and 26 months of age. Around 1 in every 2 babies will have a closed fontanelle by the time they are 14 months old.
Can I touch my baby’s fontanelles?
Yes, you can gently touch your baby’s fontanelles. If you run your fingers softly along your baby’s head you are can probably feel them. Your doctor will touch your baby’s fontanelles as part of their routine medical examination. There is no need to be concerned or worried about touching your baby’s fontanelles as long as you are gentle.
What does a normal fontanelle look like?
Your baby’s fontanelle should feel soft and flat. If you softly touch a fontanelle, you may at times feel a slight pulsation — this is normal. If a fontanelle changes, or feels different to how it usually does, show your doctor or midwife as it may be a sign that your baby’s health may need to be checked.
Sunken fontanelle
If you notice that your baby’s fontanelles are low or sunken, your baby may be dehydrated.
However, you may notice other signs of dehydration in your baby before their fontanelles becomes sunken.
Other signs of dehydration include:
- having fewer wet nappies
- not feeding well
- loosing fluids from vomiting or diarrhoea
- perspiration (or sweating) in very hot weather
- being less alert or floppy
Bulging fontanelle
A bulging or swollen fontanelle may be a sign of a number of serious but rare conditions including meningitis or encephalitis (infections in the brain), cerebral haemorrhage (bleeding in the brain), hydrocephalus, an abscess or another cause of increased pressure in the brain.
If you think that your baby’s fontanelles are bulging or sunken, seek medical advice immediately.
What if a fontanelle closes too soon?
Your baby’s fontanelles may close early. This can happen for several reasons. Your baby may have hyperthyroidism (high levels of the thyroid hormone) or hyperparathyroidism (high levels of parathyroid hormone). Another cause of early fontanelle closure is a condition known as craniosynostosis. Craniosynostosis occurs when one or more of the fibrous joints (sutures) between the bone plates in a baby’s skull fuse too early, before the brain has finished growing. As the brain continues to grow, it pushes on the skull from the inside but cannot expand into the closed over area. This causes the skull to have an unusual shape.
Another cause of early fontanelle closure is a condition known as craniosynostosis. Craniosynostosis occurs when one or more of the fibrous joints (sutures) between the bone plates in a baby’s skull fuse too early, before the brain has finished growing. As the brain continues to grow, it pushes on the skull from the inside but cannot expand into the closed over area. This causes the skull to have an unusual shape.
If you notice that your baby’s fontanelles seem to have closed early, if you can feel a ridge along your baby’s skull, or if you think that your baby’s head has an unusual shape, take your baby to see their GP or paediatrician.
What if a fontanelle doesn’t close?
Your baby’s fontanelles may not close on time for several reasons. Common reasons for delayed fontanelle closure include congenital hypothyroidism (low thyroid hormones from birth), Down syndrome, increased pressure inside the brain, rickets and familial macrocephaly (a genetic tendency to have a large head).
If one or both of your baby’s fontanelles haves not closed by the time they are 2 years old, speak to your GP or paediatrician.
If you have any concerns about your baby’s fontanelles you should make an appointment to see your child health nurse, GP or paediatrician.
Speak to a maternal child health nurse
Call Pregnancy, Birth and Baby to speak to a maternal child health nurse on 1800 882 436 or video call. Available 7am to midnight (AET), 7 days a week.
Sources:
Children’s Health Queensland Hospital and Health Service (Craniosynostosis), American Family Physician (The Abnormal Fontanel), Australian Family Physician (The 6 week check - An opportunity for continuity of care), WA Health (Bulging Anterior Fontanelle), The Royal Children's Hospital Melbourne (Clinical Practice Guidelines: Dehydration)Learn more here about the development and quality assurance of healthdirect content.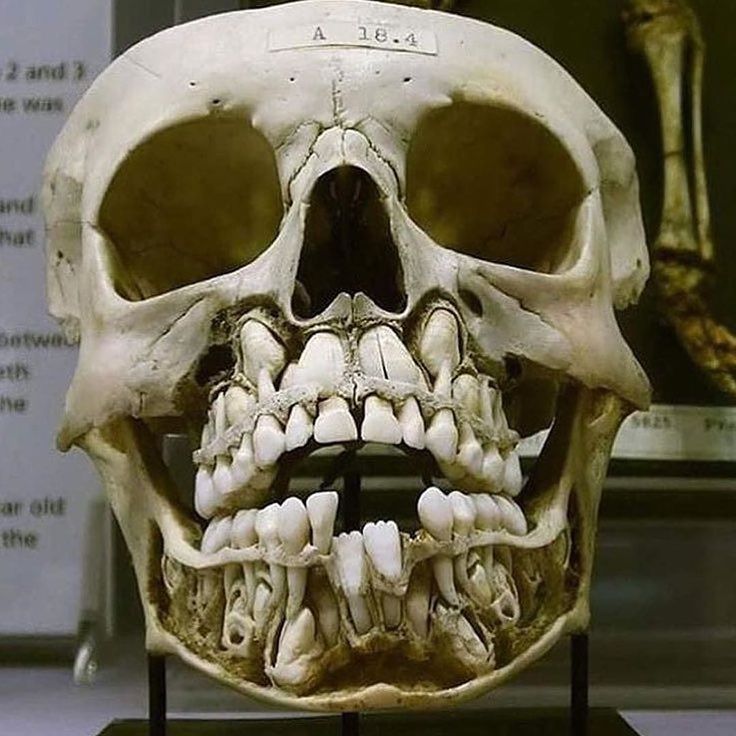
Last reviewed: February 2022
Back To Top
Related pages
- Regular health checks for babies
- Knowing your baby is well - podcast
- How to know when your baby is well - video
- How your baby’s brain develops
Need more information?
Newborn baby essentials
Find out some of the essentials for looking after your newborn. Find out when your baby will need to have health checkups and immunisations. There is also lots of information on nappies, giving your baby a bath and teeth development.
Read more on Pregnancy, Birth & Baby website
Colic in infants - MyDr.com.au
Colic is a pattern of unexplained, excessive crying in an otherwise healthy and well-fed baby and happens to 1 in 5 Australian babies.
Read more on myDr website
Knowing your baby is well - podcast
Listen to Dianne Zalitis, midwife and Clinical Lead at Pregnancy, Birth and Baby, talk to Feed Play Love with Shevonne Hunt about signs your baby is well.
Read more on Pregnancy, Birth & Baby website
Common worries and fears for parents
New parents often worry that they don't know what to do. However, there are practical ways to deal with the challenges so you can enjoy your baby more.
Read more on Pregnancy, Birth & Baby website
Flattened head
Plagiocephaly (flattened or misshapen head) means an uneven or asymmetrical head shape. Plagiocephaly won't affect your baby's brain development but it should be treated.
Read more on Pregnancy, Birth & Baby website
Glossary of pregnancy and labour
Glossary of common terms and abbreviations used in pregnancy and labour.
Read more on Pregnancy, Birth & Baby website
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now entering.
OKNeed further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
Head shape in a newborn: what options are considered normal loose (they will have to completely harden in the first year), and the seams between them have not yet had time to overgrow. During childbirth, the bones overlap each other, allowing the baby to move out more easily. That is why, after natural childbirth, the shape of the head is slightly elongated, while in small "caesareans" it is even and rounded.
 Due to the ups and downs of traveling through the birth canal, a baby may be born with an asymmetrical head, and sometimes also with a bump (cephalohematoma) or edema (the so-called generic). nine0003
Due to the ups and downs of traveling through the birth canal, a baby may be born with an asymmetrical head, and sometimes also with a bump (cephalohematoma) or edema (the so-called generic). nine0003 Mothers often wonder: why do babies have such a large head? Relative to the size of the body, it is indeed much larger than in adults - at birth, the baby's head in a circumference is about 2 cm larger than the chest. But it happens that these dimensions increase even more: this happens if cerebrospinal fluid accumulates in the cranial cavity. Then doctors talk about hydrocephalus. This problem can occur if a woman has a severe infection during pregnancy. And it happens the other way around - the head of the newborn is too small (microcephaly). Fortunately, in many cases, the reason for its unusual shape or size is much simpler: a child can inherit all these features from their parents. nine0003
In newborns, the following head shapes are considered normal:
-
Dolichocephalic - in this case, the skull is slightly flattened, elongated from the chin to the back of the head, and has an elongated diagonal shape.

-
Bracheocephalic - the transverse diameter of the head is greater than the longitudinal one, the skull is elongated from the forehead to the back of the head, slightly flattened.
-
Tower - the skull is elongated vertically, the reason is the rapid healing of the sutures of the skull bones. nine0003
When will the baby's head become the correct shape? It begins to level off already in the first days after childbirth, and in total this process can last up to a year. How can you help your baby get back to normal?
-
Caring care. If the baby lies on his back in one position for a long time, his head may become flat. That is why the child's head must be turned from time to time to the left, then to the right, lay the baby on its side, and if necessary, put a roller. nine0003
-
Proper nutrition. The shape of the child's head may change due to rickets, in which calcium metabolism is disturbed in the body.
 In this situation, the baby will need the help of a doctor; he will advise the mother to monitor her diet (for example, eat more dairy products) if she is breastfeeding the baby, and he will prescribe a suitable mixture for the little “artist”.
In this situation, the baby will need the help of a doctor; he will advise the mother to monitor her diet (for example, eat more dairy products) if she is breastfeeding the baby, and he will prescribe a suitable mixture for the little “artist”. -
Orthopedic pillows for newborns. These pillows are prescribed by a doctor to correct the shape of the baby's head and prevent deformities in the back of the head and neck. nine0003
More interesting and useful materials for expectant mothers - in our channel on Yandex.Zen.
Lyubov Prishlaya
Today they are reading
Very personal: Harry and Meghan showed 15 exclusive wedding pictures movie premiere
0003How the children of the host of “Good night, kids!” look like Oksana Fedorova - rare shots
Plagiocephaly in a child - an irregular shape of the skull in an infant
The disease is cured by:
Children's osteopath
Article content
- Causes of
- Types of plagiocephaly in children
- Signs of disease
- Diagnostics of plagiocephaly in children
Plagiocephaly is an abnormally shaped skull, or flat head syndrome, in infants. Its signs are detected to some extent in every fifth child, and only every tenth of them needs specific treatment. Deformation becomes distinct noticeable by 2 months (sometimes earlier). Treatment started on time is usually effective.
Its signs are detected to some extent in every fifth child, and only every tenth of them needs specific treatment. Deformation becomes distinct noticeable by 2 months (sometimes earlier). Treatment started on time is usually effective.
Causes
- Postpartum - permanent position with emphasis on the bones of the skull (mainly lying on the back) or premature fusion of the sutures of the skull.
- Intrauterine - in most cases caused by the anatomical position during gestation - with twin pregnancy and / or pressing the fetus to the mother's ribs, large fetus or uterine abnormalities, premature prolapse during childbirth. nine0024
- Pathological conditions - torticollis, or torticollis - shortening of the muscles of the neck on one side, other neuromuscular diseases.
Previously, the disease was diagnosed less frequently - due to the fact that pediatricians recommended laying newborns on their side. To date, it has been proven that this position increases the risk of sudden infant death syndrome in a dream, therefore, since 1992, it has been recommended to lay children on their backs during sleep, which becomes a frequent cause of deformation of the skull bones that have not yet been fully formed. nine0003
To date, it has been proven that this position increases the risk of sudden infant death syndrome in a dream, therefore, since 1992, it has been recommended to lay children on their backs during sleep, which becomes a frequent cause of deformation of the skull bones that have not yet been fully formed. nine0003
Types of plagiocephaly in children
According to etiological types, plagiocephaly is distinguished:
- Positional - acquired, caused by mechanical deformations - intrauterine or perinatal. Occurs in the vast majority of cases. Source:
https://www.ncbi.nlm.nih.gov/pubmed/25382999
Mawji A, Vollman AR, Fung T, Hatfield J, McNeil DA, Sauvé R
Risk factors for positional plagiocephaly and appropriate time frames for prevention messaging
// Pediatric Child Health. 2014 Oct;19(8):423-7 - Deformation - due to congenital diseases - progressive deformity due to early fusion of the cranial bones.
 It occurs extremely rarely - in 1 out of 2,000 patients. Source:
It occurs extremely rarely - in 1 out of 2,000 patients. Source:
https://www.ncbi.nlm.nih.gov/pubmed/30151193
Renz-Polster H, De Bock
Deformational plagiocephaly: The case for an evolutionary mismatch
// Evol Med Public Health. 2018 Aug 8;2018(1):180-185. doi: 10.1093/emph/eoy019. eCollection 2018
By localization it happens:
- frontal;
- occipital;
- side.
Signs of disease
Atypical skull shape - flattened in the occipital region. Rarely - elongated in the frontal direction or squeezed from the sides. Characteristic frontal or temporal bulges, protrusions of the parietal region are possible. nine0003
If the asymmetry of the head is caused by congenital anomalies, then without treatment, the pathology progresses. Over time, it can cause negative consequences in a child - increased intracranial pressure and the symptoms caused by it . Source:
Source:
E.V. Mammadov
Plagiocephaly. II. Synostotic, deformation and compensatory
// Children's surgery, 2003, No. 5, p. 45-50
Diagnosis of plagiocephaly in a child
In accordance with modern recommendations, the diagnosis is made on the basis of a clinical examination. For differential diagnosis - identifying the cause of the pathology - ultrasound, radiography or CT of the skull are optionally prescribed. nine0003
Methods of treatment
The main treatment for positional plagiocephaly in infants is the reposition method : multiple changes in body position during the day. The child should lie on his back as little as possible when he is awake. Minimize wearing in a sling and carrier, transport in a car seat. An effective technique is to change the position of the child relative to the light source (stimulates turning over).
Children older than 7 weeks also indicated exercise therapy. It is aimed at:
It is aimed at:
- stimulation of motor development and correction of positional preferences;
- stretching of the neck muscles with torticollis - an increase in the range of motion in the cervical spine.
Includes laying out the child on the stomach during wakefulness under the supervision of adults.
With moderate and severe deformities, as well as with the ineffectiveness of conservative treatment, orthotics are indicated - helmet therapy. The orthosis is made according to individual measurements in an orthopedic workshop. The child wears it 23 hours a day until it heals or needs to change the size of the helmet. nine0003
Conservative treatment and orthotics last for several months. The bones of the skull gradually assume a physiological position, while no damage is done to the brain, and neurological diseases do not develop.
If the deformity is due to a congenital anomaly, surgery is indicated. As a rule, it is done at the age of ~7-9 years. The use of orthopedic pillows for newborns is contraindicated, as they sometimes cause infant death.
The use of orthopedic pillows for newborns is contraindicated, as they sometimes cause infant death.
nine0003
Sources:
- https://www.ncbi.nlm.nih.gov/pubmed/25382999 Mawji A, Vollman AR, Fung T, Hatfield J, McNeil DA, Sauvé R. Risk factors for positional plagiocephaly and appropriate time frames for prevention messaging // Paediatr child health. 2014 Oct;19(8):423-7.
- https://www.ncbi.nlm.nih.gov/pubmed/30151193 Renz-Polster H, De Bock. Deformational plagiocephaly: The case for an evolutionary mismatch // Evol Med Public Health. 2018 Aug 8;2018(1):180-185. doi: 10.1093/emph/eoy019. eCollection 2018.
- E.V. Mammadov. Plagiocephaly. II. Synostotic, deformation and compensatory // Children's surgery, 2003, No. 5, pp. 45-50.
The information in this article is provided for reference only and does not replace the advice of a qualified professional. Do not self-medicate! At the first signs of the disease, you should consult a doctor.