Where is the placenta attached
About the placenta – role and complications
About the placenta – role and complications | Pregnancy Birth and Baby beginning of content7-minute read
Listen
What is the placenta?
The placenta is a temporary organ that develops during pregnancy. It attaches to the lining of your uterus and delivers oxygen and nutrients to your growing baby through the umbilical cord.
If something goes wrong with the placenta, it can be serious and even life-threatening to both mum and baby.
What is the role of the placenta during pregnancy?
The placenta passes oxygen, nutrients and antibodies from your blood to your baby. It also carries waste products from your baby back to your blood, so your body can get rid of them.
The placenta also produces some hormones like oestrogen and progesterone that are needed during pregnancy.
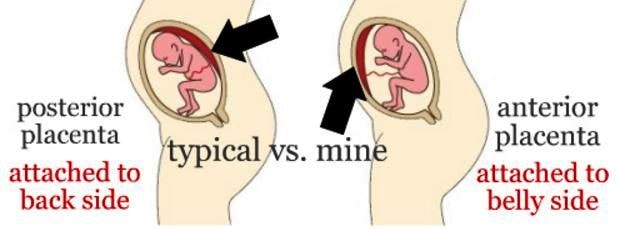
What is the normal position of the placenta during pregnancy?
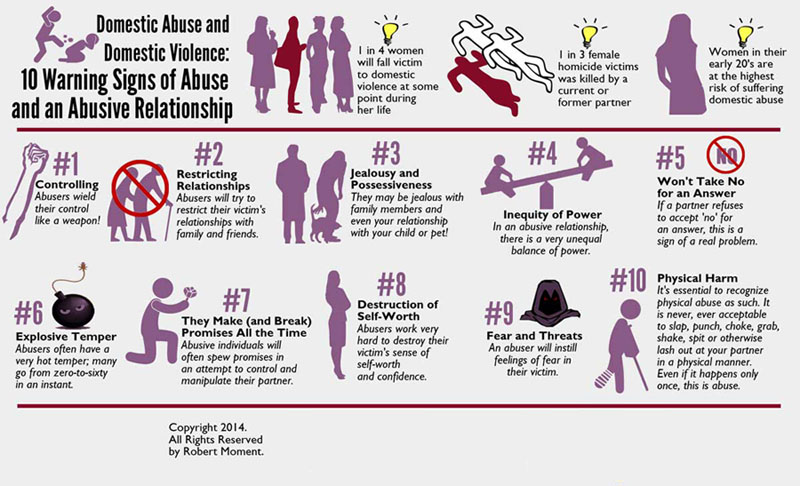
The placenta should attach to the wall of the uterus, usually at the top, side, front or back. The exact location will vary from person to person and in each pregnancy.
The placenta can sometimes develop low in the uterus but will generally move higher as your uterus stretches. The position of the placenta will be checked at your 18-week ultrasound.
This image shows a normal placental location, with the placenta attached at the top of the uterus.How does the placenta work in twin pregnancies?
Fraternal twins come from separate eggs and each have their own placenta. Identical twins come from the same egg that separates, and they may share a placenta or have their own.
Can medicines cross the placenta?
Alcohol, nicotine, medicines and other drugs can cross the placenta and affect your baby’s health.
What should I do to keep my placenta healthy during pregnancy?
It’s important to visit your healthcare provider regularly during pregnancy.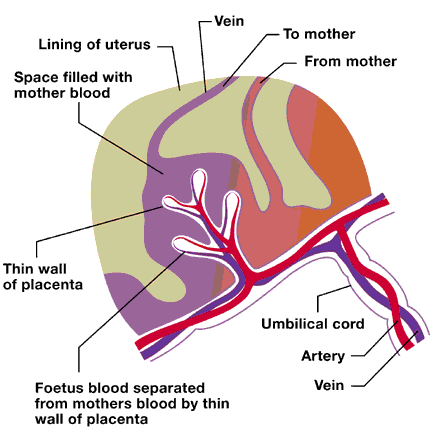 If there are complications, they can be identified during these appointments.
If there are complications, they can be identified during these appointments.
Tell your doctor if you have had problems with the placenta in a previous pregnancy, or if you have had any surgery to your uterus.
If you smoke, drink alcohol or take certain drugs during pregnancy, this increases the likelihood of problems with the placenta.
Always consult your doctor before you take any medicines, including over-the-counter medicines, natural therapies and supplements, while you are pregnant.
Speak with your doctor or midwife if you have any concerns, or if you experience:
- severe abdominal (stomach) pain or back pain
- vaginal bleeding
- contractions
- any trauma to your abdomen, for example from a fall or car accident
What happens to the placenta after my baby is born?
After your baby is born, you will need to birth your placenta. This is called the third stage of labour.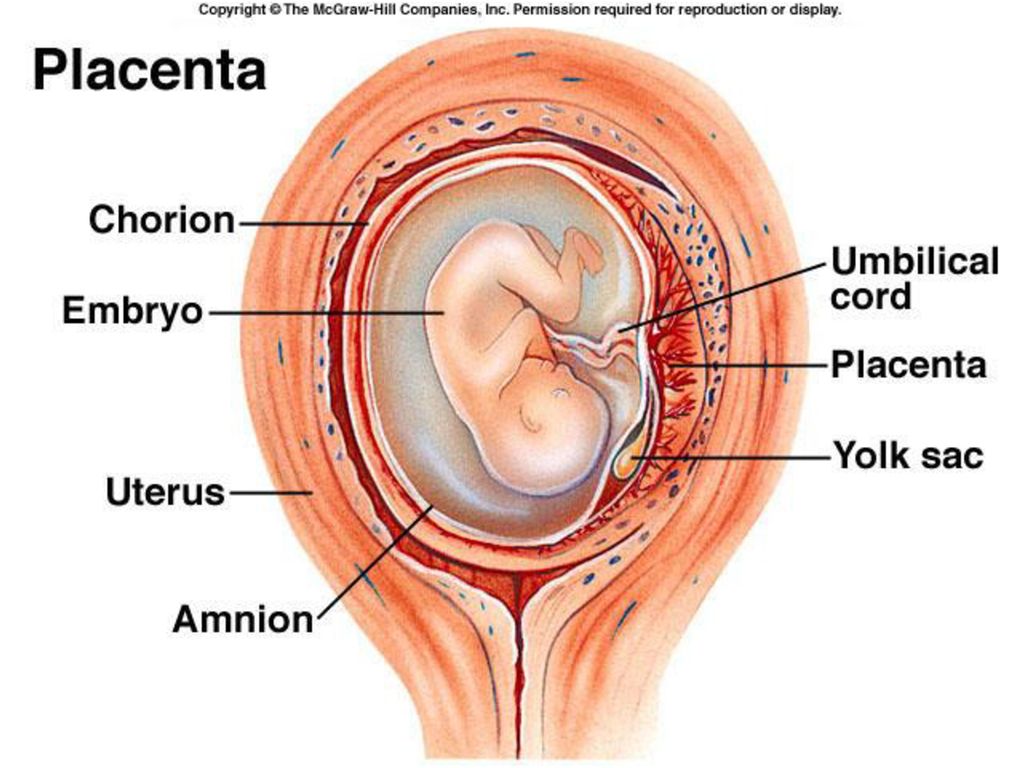 This stage of labour can be managed in different ways.
This stage of labour can be managed in different ways.
If you had a vaginal birth, you will usually have some mild contractions and need to give a few pushes to help your placenta to come out.
If you have a caesarean section, your doctor will remove the placenta at the same time your baby is born.
Once you birth your placenta your doctor or midwife will check that it looks complete. If there is any concern that your placenta isn’t complete, they may suggest further investigations. If any bits of placenta are retained (stay inside you), they may have to be surgically removed to prevent infection.
Can I take my placenta home with me?
It is your choice what you do with your placenta. You may choose to discard it; in which case your hospital or birthing centre will take care of this.
If you wish to take your placenta home, you can speak to your doctor or midwife to arrange this.
In some cultures, people bury the placenta in a special place.
‘Placentophagy’ is a practice where people cook and eat their placenta.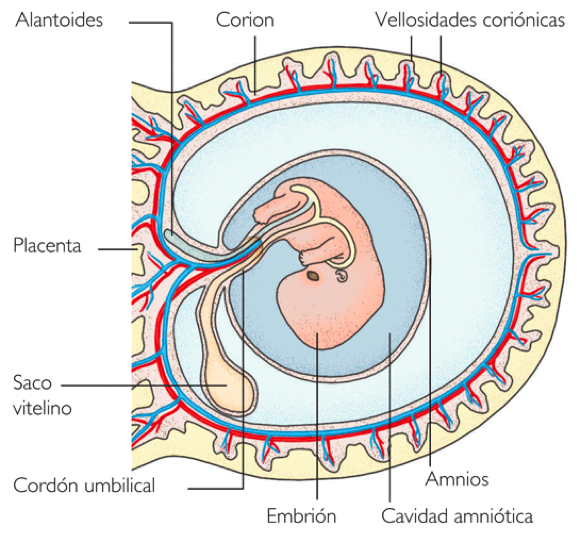 There is no research to support health benefits from this. However, you may choose to do this for cultural, spiritual, or personal reasons.
There is no research to support health benefits from this. However, you may choose to do this for cultural, spiritual, or personal reasons.
Some commercial service providers offer to turn your placenta into capsules for you to swallow. It should be noted that there may be a risk of infection from poor preparation. These practices should be treated with caution.
Can anything go wrong with my placenta?
Problems with your placenta can happen during pregnancy, birth and after birth. These are potentially dangerous for both you and your baby.
If your bleeding is severe and you have significant pain, call triple zero (000) for an ambulance or go to your nearest hospital emergency department.
If you have any vaginal bleeding during pregnancy, it’s important to see your doctor as soon as possible.
Placental abruption is when some or all the placenta comes away from the wall of the uterus before your baby is born.
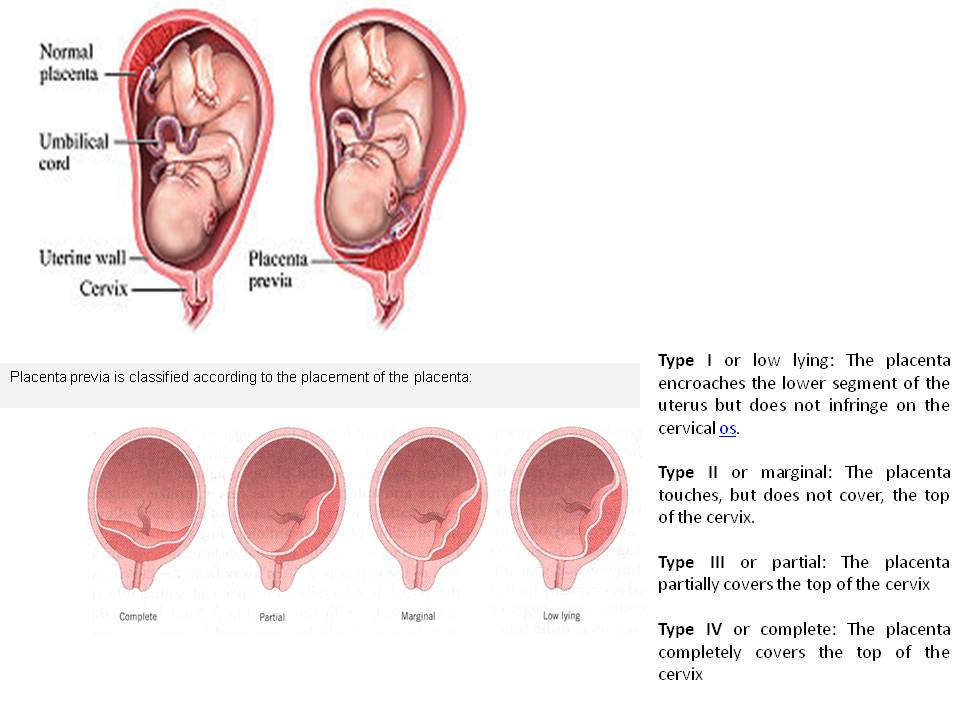
Placenta praevia is when the placenta partially or totally covers the cervix (the narrow opening in the uterus).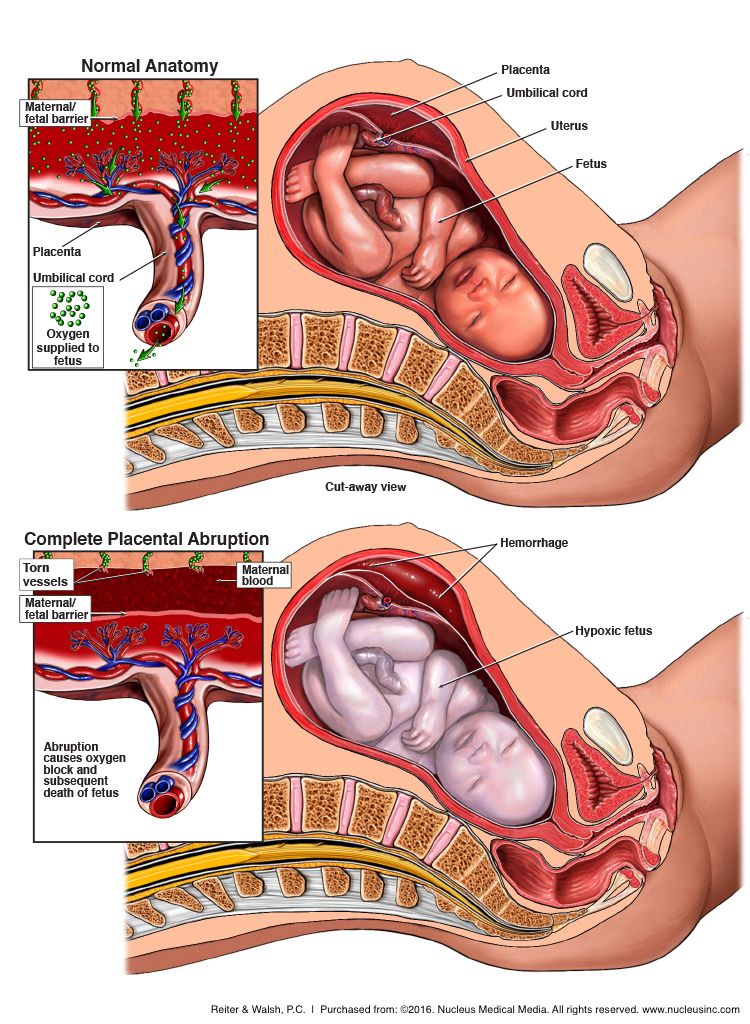
Placental insufficiency is when the placenta doesn’t work properly during pregnancy. It deprives the baby of oxygen and nutrients they need to grow and develop.
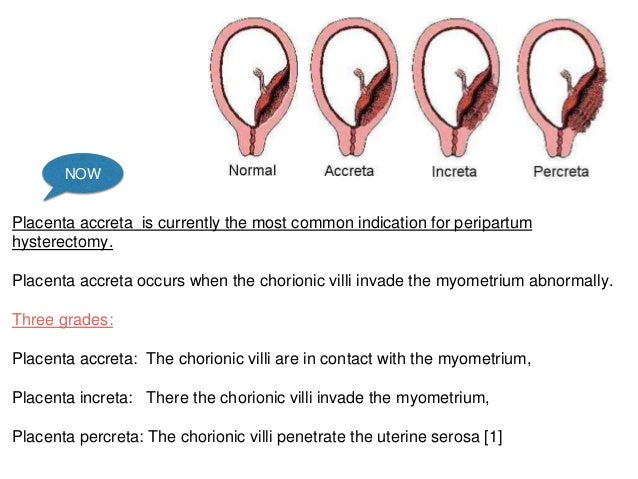
Placenta accreta is when the placenta grows too deeply into the wall of the uterus. This can lead to severe bleeding during or after delivery and can be life-threatening.
Retained placenta is when your placenta does not completely come out after the birth. This might be because it is stopped by your cervix or is still attached to your uterus.
Speak to a maternal child health nurse
Call Pregnancy, Birth and Baby to speak to a maternal child health nurse on 1800 882 436 or video call. Available 7am to midnight (AET), 7 days a week.
Sources:
UNSW Embryology (KA02 Fetus or newborn affected by complications of placenta), Royal Women's Hospital (Placenta problems), RANZCOG (Intrauterine Growth Restriction: Screening, Diagnosis, and Management - Placenta accreta), The Royal Women’s Hospital Victoria Australia (Taking Your Placenta Home For Burial Or Consumption), International Journal of Women’s Health (Retained placenta after vaginal delivery: risk factors and management), NHS UK (What complications can affect the placenta?)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: July 2022
Back To Top
Related pages
- Mum's first 24 hours after birth
- Giving birth - stages of labour
- Placenta complications in pregnancy
Need more information?
Placenta previa - Better Health Channel
Placenta previa means the placenta has implanted at the bottom of the uterus, over the cervix or close by.
Read more on Better Health Channel website
Retained placenta
A retained placenta is when part or all of the placenta is not delivered after the baby is born. It can lead to serious infection or blood loss.
Read more on Pregnancy, Birth & Baby website
Placenta praevia
Placenta praevia is a condition where the placenta lies low and may cover the cervix, blocking the baby's exit during birth.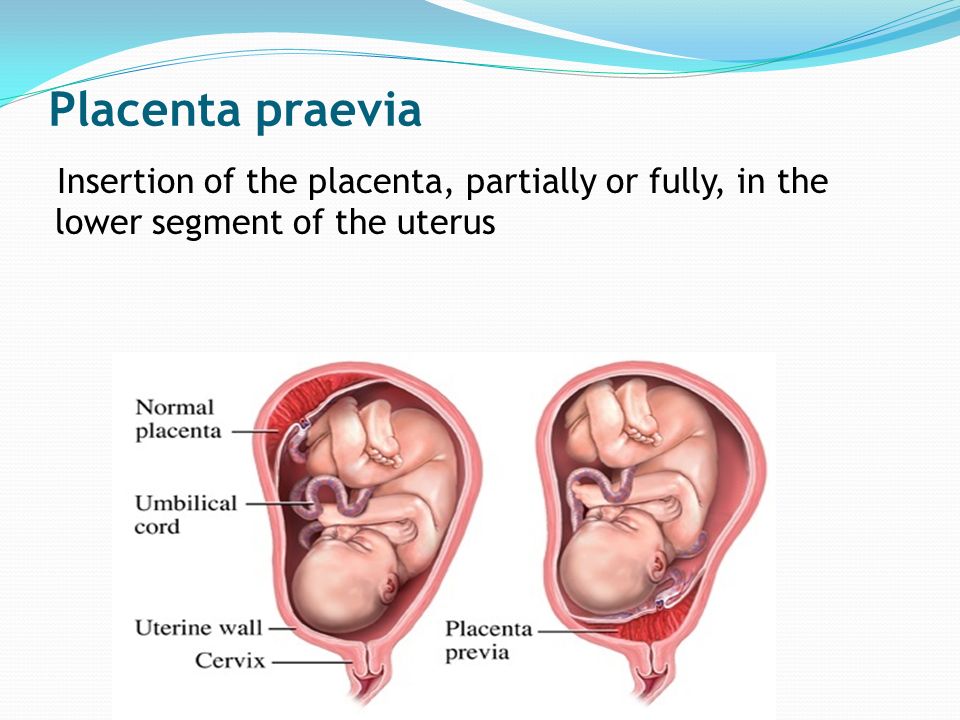
Read more on Pregnancy, Birth & Baby website
Placenta accreta
Placenta accreta is a serious but rare pregnancy complication that causes heavy bleeding. If you have it, you will need special care at the birth.
Read more on Pregnancy, Birth & Baby website
Placental abruption - Better Health Channel
Placental abruption means the placenta has detached from the wall of the uterus, starving the baby of oxygen and nutrients.
Read more on Better Health Channel website
Placental insufficiency
Placental insufficiency occurs when the placenta does not work properly and your baby doesn't get the oxygen and nutrients they need.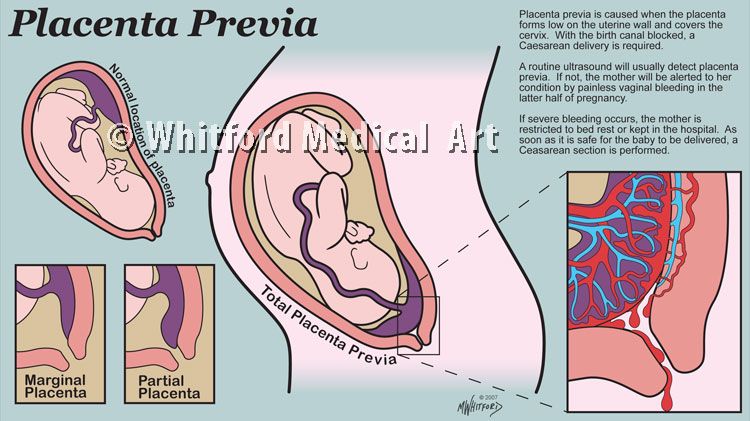
Read more on Pregnancy, Birth & Baby website
It is not just a woman’s issue - Alcohol and Drug Foundation
If a woman drinks during pregnancy the alcohol crosses the placenta to the baby. But what about the effect of alcohol on men?
Read more on Alcohol and Drug Foundation website
Placental abruption
Placental abruption is when some or all of the placenta peels away from the uterus wall before birth. It can deprive the baby of oxygen and nutrients.
Read more on Pregnancy, Birth & Baby website
Pregnancy test - Pathology Tests Explained
Starting approximately two weeks after conception, a hormone called human chorionic gonadatropin (hCG) hormone is produced by the developing placenta and can be detected in urine and in blood
Read more on Pathology Tests Explained website
4 weeks pregnant: Key points
When you are 4 weeks pregnant your body and your new baby are undergoing rapid changes.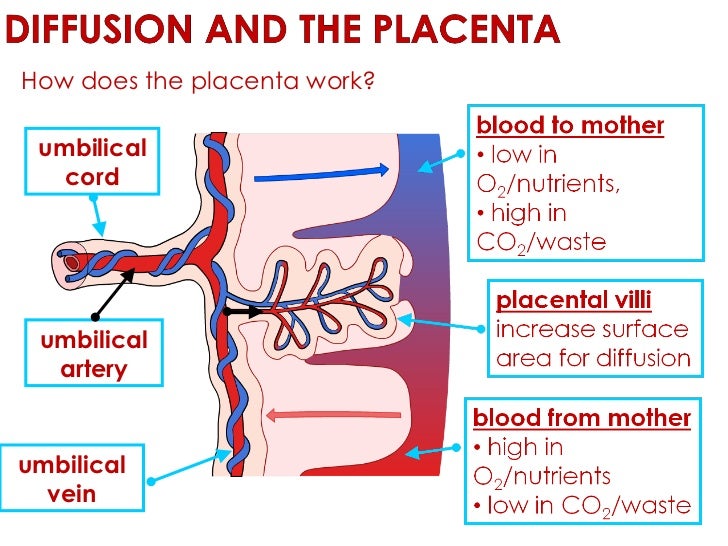 The placenta forms and begins producing a hormone called human chorionic gonadotrophin (hCG), which is the substance a pregnancy test detects to confirm you are pregnant. The cells which are growing into your new baby establish membranes which connect them to the placenta and prepare themselves for differentiation into different types of cells, which will occur next week when you are 5 weeks pregnant. These developments may cause you to experience unusual emotions and also cause changes in your body such as darkening of the areolas of your nipples.
The placenta forms and begins producing a hormone called human chorionic gonadotrophin (hCG), which is the substance a pregnancy test detects to confirm you are pregnant. The cells which are growing into your new baby establish membranes which connect them to the placenta and prepare themselves for differentiation into different types of cells, which will occur next week when you are 5 weeks pregnant. These developments may cause you to experience unusual emotions and also cause changes in your body such as darkening of the areolas of your nipples.
Read more on Parenthub website
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now entering.
OKNeed further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.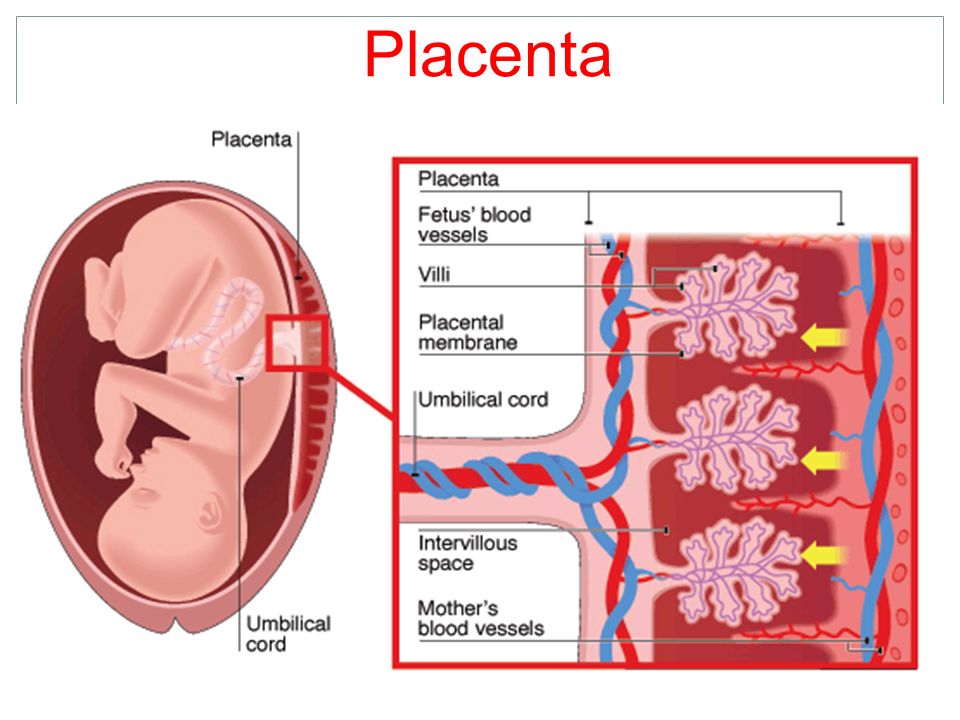
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
Placenta Delivery: What to Expect
The placenta is a unique organ of pregnancy that nourishes your baby. Typically, it attaches to the top or side of the uterus. The baby is attached to the placenta via the umbilical cord.
After your baby is delivered, the placenta follows. This is the case in most births. But there are some exceptions.
Delivery of the placenta is also known as the third stage of labor. Delivery of the entire placenta is vital to your health after giving birth. Retained placenta can cause bleeding and other unwanted side effects.
For this reason, a doctor will examine the placenta after delivery to ensure that it is intact. If a piece of placenta is left in the uterus or the placenta doesn’t deliver, there are other steps a doctor can take.
The placenta is an organ shaped like a pancake or disk. It is attached on one side to your uterus and on the other side to the baby’s umbilical cord.
The placenta is responsible for many important functions when it comes to a baby’s growth. This includes producing hormones, such as:
- estrogen
- human chorionic gonadotropin (hCG)
- progesterone
The placenta has two sides. The parental side is usually dark red in color, while the fetal side is shiny and almost translucent in color. After the baby is born, a doctor will examine the placenta to ensure each side appears as it is expected to.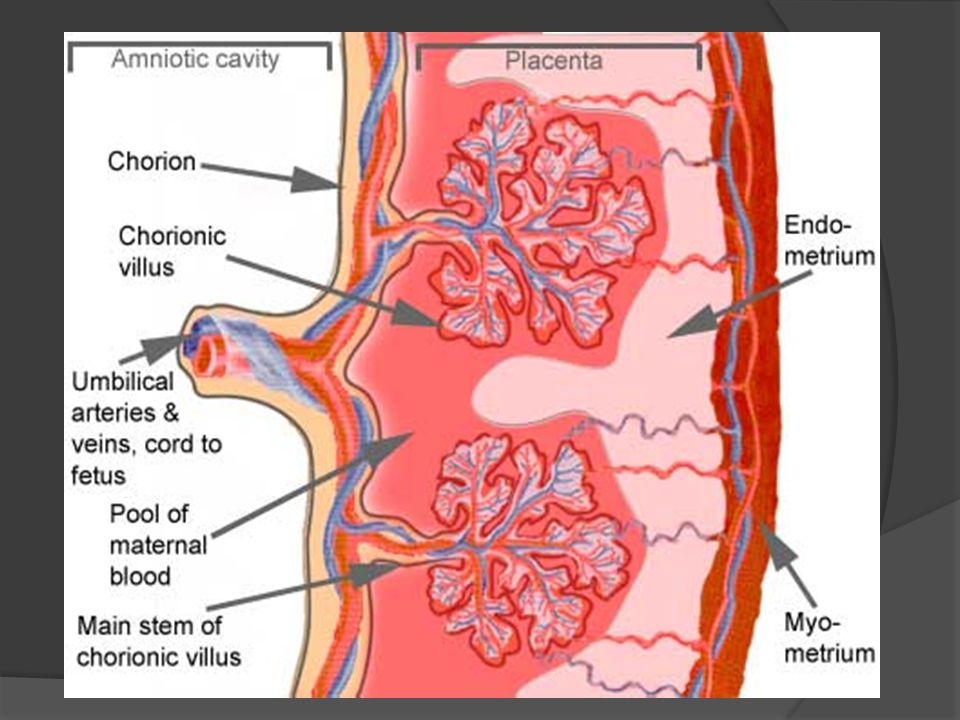
Some people ask to save their placenta and will boil it to eat it or even dehydrate it and encapsulate it into pills. In fact, some people believe that taking the pills will reduce postpartum depression or postpartum anemia. However, scientific studies have not proven these effects.
Other people plant the placenta in the ground as a symbolic gesture of the connection between life and earth.
Some states and hospitals have rules about saving the placenta, so a pregnant person should always check with the facility they’re delivering at to make sure they can save the placenta.
Placenta delivery after a vaginal birth
In a vaginal delivery, after the baby is born, your uterus will continue to contract. These contractions will move the placenta forward for delivery. They aren’t usually as strong as labor contractions.
However, some doctors may ask you to continue to push, or they may press on your stomach as a means to advance the placenta forward. Usually, placenta delivery is quick, within about 5 minutes after having your baby. However, it can take longer for some people.
However, it can take longer for some people.
Often, after you deliver your baby, you’re very focused on seeing them for the first time and may not notice the placenta delivery. However, some people observe an additional gush of blood after delivery that’s usually followed by the placenta.
The placenta is attached to the umbilical cord, which is attached to your baby. Because there aren’t any nerves in the umbilical cord, it doesn’t hurt when the cord is cut.
The American College of Obstetricians and Gynecologists (ACOG) recommends in its 2020 guidelines that unless the cord is wrapped around the baby’s neck, it should not be clamped and cut sooner than at least 30 to 60 seconds after birth. This delay improves your baby’s hemoglobin and iron levels, among other benefits.
Placenta delivery after a cesarean
If you deliver via cesarean delivery (also known as C-section), your doctor will physically remove the placenta from your uterus before closing up the incision in the uterus and stomach.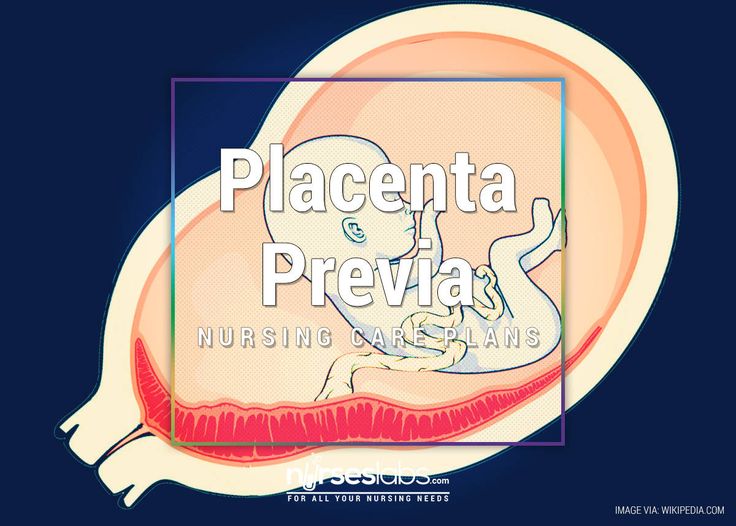
After delivery, your doctor will likely massage the top of your uterus (known as the fundus) to encourage it to contract and start to shrink. If a uterus cannot contract and become firmer, a doctor may give you medication, such as Pitocin, to make the uterus contract.
Breastfeeding or chestfeeding a baby immediately after birth or placing the baby on your skin (known as skin-to-skin contact) can also cause the uterus to contract.
Regardless of how your placenta is delivered, your doctor will inspect it for intactness.
If it appears that a portion of the placenta is missing, your doctor may recommend an ultrasound of the uterus to confirm. Sometimes, excessive bleeding after delivery can indicate that some placenta is still in the uterus.
A birthing person should deliver the placenta within 30 to 60 minutes after having the baby. If the placenta isn’t delivered or doesn’t come out entirely, it’s called retained placenta.
Reasons the placenta may not fully deliver include:
- The cervix has closed and is too small an opening for the placenta to move through.
- The placenta is too tightly attached to the wall of the uterus.
- A portion of the placenta broke off or remained attached during delivery.
Retained placenta is a major concern because the uterus must clamp back down after giving birth. Tightening the uterus helps the blood vessels inside stop bleeding. If the placenta is retained, a person can experience bleeding or infection.
Retained portions of the placenta after delivery can lead to dangerous bleeding and infection. A doctor will typically recommend surgical removal as quickly as possible.
However, sometimes the placenta is so attached to the uterus that it isn’t possible to remove without also removing the uterus (hysterectomy).
A person is at increased risk for retained placenta if they have any of the following:
- previous history of retained placenta
- previous history of cesarean delivery
- history of uterine fibroids
If you are concerned about retained placenta, talk with your doctor prior to delivery. They can discuss your delivery plan with you and notify you when the placenta is delivered.
They can discuss your delivery plan with you and notify you when the placenta is delivered.
The birth process can be an exciting one and one that’s full of emotions. Typically, delivering the placenta isn’t painful.
Often, it occurs so quickly after birth that a new parent may not even notice because they’re so focused on baby (or babies!). But it’s important that the placenta is delivered in its entirety.
If you wish to save your placenta, always notify the facility, doctors, and nurses in advance of delivery to be sure that it can be properly saved or stored.
Maternity hospital №7, Novosibirsk - What is the placenta?
Anna Valentinovna Yakimova, obstetrician-gynecologist, MD talks about the placenta and placental insufficiency.
Picture from the site http://s7ya7.zdorovo-zivi.ru
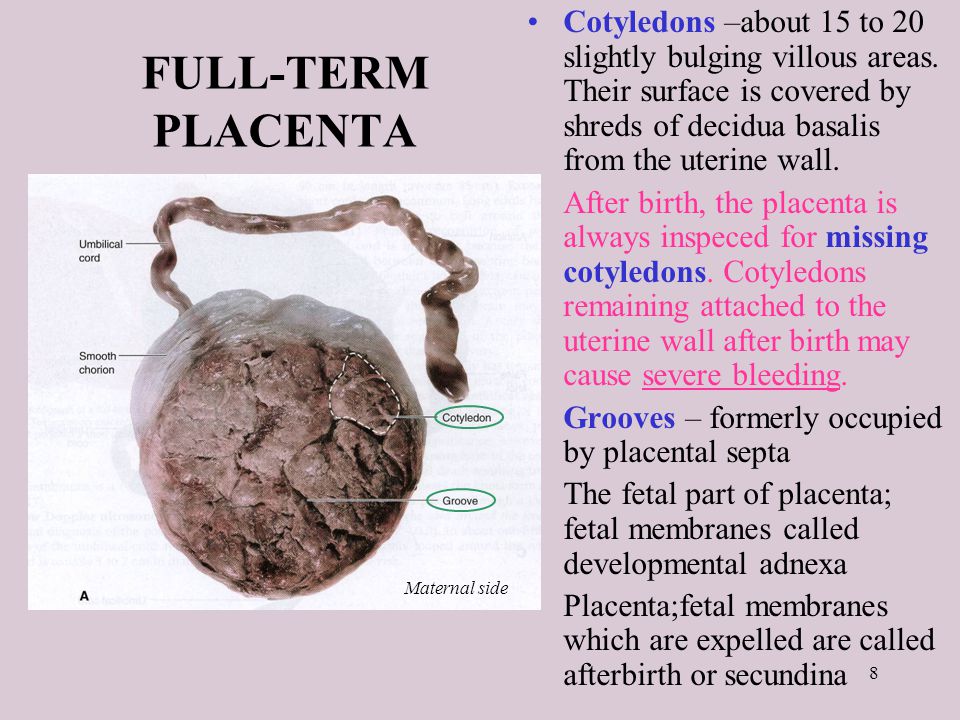
Placenta. The name of the organ comes from lat. placenta - cake, cake, pancake. This is an extra-embryonic organ, consisting of villi, thanks to which the fetus is nourished, respired, and waste products are removed from its blood.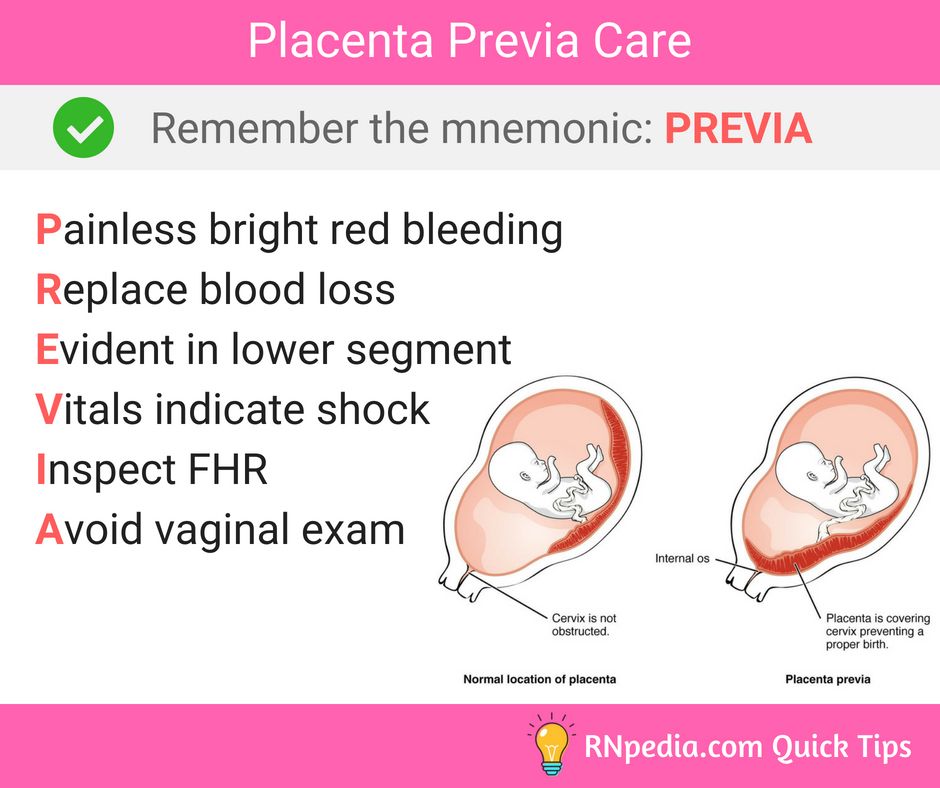 There are free and fixing (anchor) villi. The placenta is formed in the place where the embryo was implanted, arises as a result of the connection of the chorion - extraembryonic tissue with a thickened uterine mucosa (decidual tissue). Despite the fact that the blood of the mother and fetus does not mix, as they are separated by the placental barrier, the fetus receives all the necessary nutrients and oxygen from the mother's blood. In addition, the placenta produces hormones that ensure the preservation of pregnancy. The placenta has two surfaces. The surface that faces the fetus is called the fetal. It is covered with a smooth shell - the amnion, through which large vessels shine through. The one that is attached to the wall of the uterus is called maternal.
There are free and fixing (anchor) villi. The placenta is formed in the place where the embryo was implanted, arises as a result of the connection of the chorion - extraembryonic tissue with a thickened uterine mucosa (decidual tissue). Despite the fact that the blood of the mother and fetus does not mix, as they are separated by the placental barrier, the fetus receives all the necessary nutrients and oxygen from the mother's blood. In addition, the placenta produces hormones that ensure the preservation of pregnancy. The placenta has two surfaces. The surface that faces the fetus is called the fetal. It is covered with a smooth shell - the amnion, through which large vessels shine through. The one that is attached to the wall of the uterus is called maternal.
The main structural unit of the placenta is cotelidone. Cotyledon of the placenta is conditionally comparable to a tree. Each cotyledon is formed by a stem villus, from which, like branches of a tree, villi of the second and third order extend, containing vessels.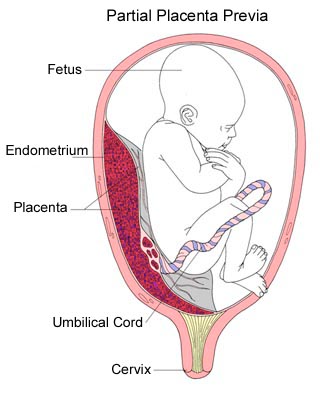 The central part of the cotyledon forms a cavity, which is surrounded by many villi. Between the cotyledons there is a space - mejvirus, which on the maternal side is limited by partitions (septa) extending from the mucous membrane of the uterus. Most of the placental villi are freely immersed in the intervillous space (free villi) and are bathed in maternal blood. The spiral arteries, which are small branches of the arteries that supply the uterus, open into the intervillous space and supply oxygen-rich blood to the intervillous space. Due to the pressure difference, which is higher in the mother's arterial bed compared to the intervillous space, oxygenated blood from the mouths of the spiral arteries is directed through the center of the cotyledon to the villi, washes them, reaches the chorionic plate and returns to the maternal circulation through the venous orifices through the separating septa. . In this case, the blood flow of the mother and fetus are separated from each other. Those.
The central part of the cotyledon forms a cavity, which is surrounded by many villi. Between the cotyledons there is a space - mejvirus, which on the maternal side is limited by partitions (septa) extending from the mucous membrane of the uterus. Most of the placental villi are freely immersed in the intervillous space (free villi) and are bathed in maternal blood. The spiral arteries, which are small branches of the arteries that supply the uterus, open into the intervillous space and supply oxygen-rich blood to the intervillous space. Due to the pressure difference, which is higher in the mother's arterial bed compared to the intervillous space, oxygenated blood from the mouths of the spiral arteries is directed through the center of the cotyledon to the villi, washes them, reaches the chorionic plate and returns to the maternal circulation through the venous orifices through the separating septa. . In this case, the blood flow of the mother and fetus are separated from each other. Those. maternal and fetal blood does not mix. Thus, the concept of the placental barrier appears: the blood of the mother of the fetus does not mix, because they are separated by the wall of the villus, loose connective tissue inside the villus and the wall of the vessel that is inside the villus, and in which the blood of the fetus circulates.
maternal and fetal blood does not mix. Thus, the concept of the placental barrier appears: the blood of the mother of the fetus does not mix, because they are separated by the wall of the villus, loose connective tissue inside the villus and the wall of the vessel that is inside the villus, and in which the blood of the fetus circulates.
At the end of pregnancy, the placenta is a soft disk 15-18 cm in diameter, 2-4 cm thick in the central part, weighing about 500-600 g. their capillaries - 12 m2. The placenta, membranes, and umbilical cord together form the afterbirth, which is expelled from the uterus after the baby is born.
Normally, the placenta is attached to the uterine cavity on its anterior or posterior surface, sometimes in the fundus. If the placenta is attached in the lower part of the uterine cavity, close to the internal opening of the cervix - the internal pharynx, then its blood supply is often insufficient and the fetus may suffer from lack of oxygen and nutrients - a phenomenon called placental insufficiency occurs.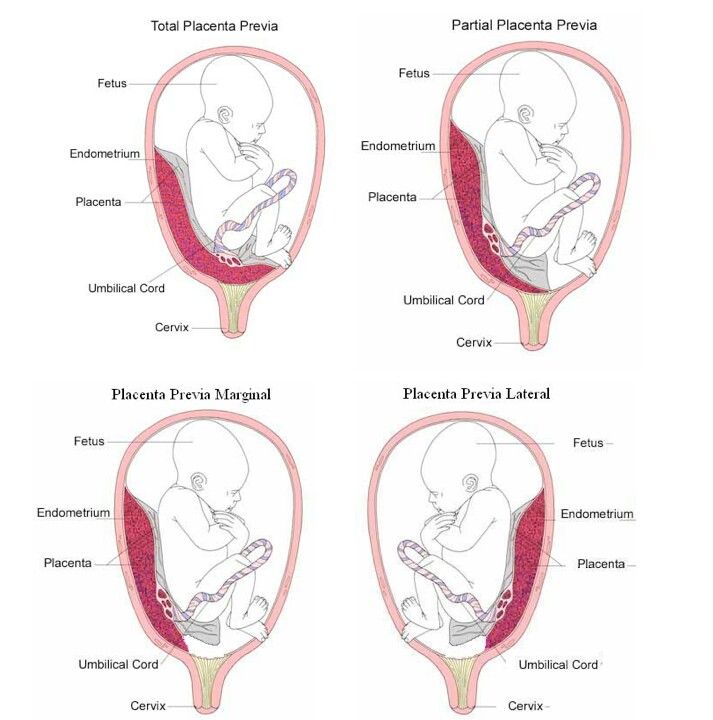
Placental insufficiency is a violation of all or some of the functions of the placenta, ultimately leading to oxygen starvation (hypoxia), fetal growth retardation or death and / or early termination of pregnancy.
Placental insufficiency may occur early in pregnancy due to impaired placental formation, for example, if the spiral arteries that supply blood to the villi do not lose the ability to narrow their lumen in response to exposure to vasoconstrictor substances. It is possible that there is a violation of the development of blood vessels inside the villi, the vessels can form in the central part of the villus, and not close to its wall, then the transfer of nutrients from the mother's blood to the fetal blood and the flow of metabolic products back will be difficult. The process of development of the placenta (in particular, vascular formation) occurs to a greater extent in the first and second trimesters of pregnancy, ending at about 30-32 weeks. After this period, involutive processes predominate ("aging", immuring the villi with fibrinoid). Along with the processes of involution in the placenta during pregnancy, young villi develop, more often avascular, which, however, only partially compensate for the function of mature villi containing vessels that have “fallen out” of the circulation.
In another scenario, placental insufficiency occurs at a later date, as a result of damage to the placenta in inflammatory processes, diabetes in a pregnant woman, or high blood pressure, when blood flow to the uterus is disturbed, which can also occur with increased maternal blood clotting . It is believed that it is the violation of the uteroplacental circulation that plays the main role in the formation of the intrauterine growth retardation syndrome. Before the advent of Doppler ultrasound research methods in obstetric practice, there were no non-invasive methods for studying blood flow in the mother-placenta-fetus system. To date, Doppler is the most preferred instrumental method that provides useful information in relation to the detection of blood flow disorders and the determination of pregnancy management tactics for placental insufficiency.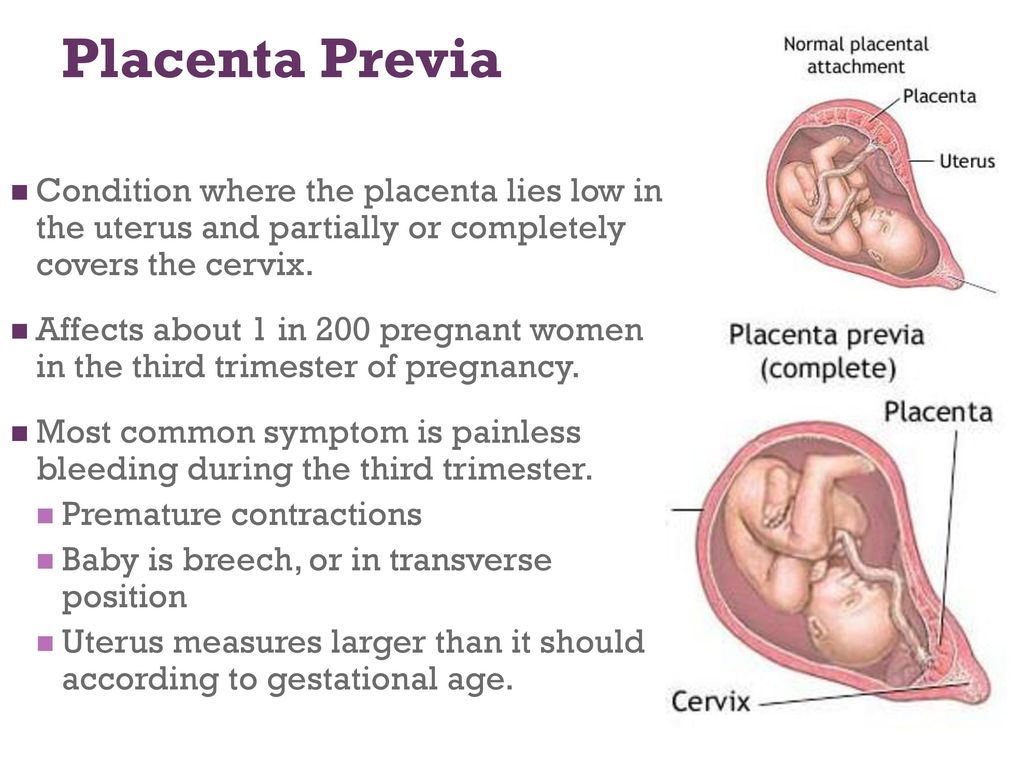 If there are symptoms of placental insufficiency - a mismatch in the height of the uterine fundus, signs of a threat of early termination of pregnancy, rapid or slow fetal heart rate (normal: 120-160 beats per minute), an altered amount of amniotic fluid - it is necessary to conduct an ultrasound examination, Doppler blood flow in the vessels of the uterus, umbilical cord and fetus, and in the third trimester - cardiotocography. The earliest sign of placental dysfunction is a decrease in its production of hormones and proteins, therefore, in pregnant women with a known risk of placental dysfunction (for example, if she has a chronic inflammatory process or often / constantly increased blood pressure, etc.), you can examine the level placental lactogen, progesterone, unconjugated estriol in the blood. And on the basis of the data obtained, predict the further development of pregnancy and take preventive measures.
If there are symptoms of placental insufficiency - a mismatch in the height of the uterine fundus, signs of a threat of early termination of pregnancy, rapid or slow fetal heart rate (normal: 120-160 beats per minute), an altered amount of amniotic fluid - it is necessary to conduct an ultrasound examination, Doppler blood flow in the vessels of the uterus, umbilical cord and fetus, and in the third trimester - cardiotocography. The earliest sign of placental dysfunction is a decrease in its production of hormones and proteins, therefore, in pregnant women with a known risk of placental dysfunction (for example, if she has a chronic inflammatory process or often / constantly increased blood pressure, etc.), you can examine the level placental lactogen, progesterone, unconjugated estriol in the blood. And on the basis of the data obtained, predict the further development of pregnancy and take preventive measures.
Can placental insufficiency be treated? The answer to this question is ambiguous.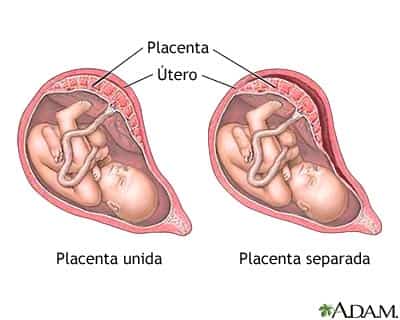 It is possible to influence the development of the placenta when it is incomplete, improving the conditions for development - by eliminating, for example, the inflammatory process, normalizing blood pressure, lowering the tone of the uterus, and normalizing blood clotting. You can influence the metabolism in the cells of the placenta - by doing this, for example, by introducing drugs into the body of a pregnant woman that help improve the utilization of glucose by cells. It is possible to influence the tone of the vessels, reduce the permeability of the wall and, in this way, the swelling of the tissues decreases and the penetration of oxygen into them improves. But we must understand that we do not cure placental insufficiency, we are only trying to influence the compensatory mechanisms that exist in the placenta, if this succeeds, the manifestations of placental insufficiency disappear. But more often, treatment is aimed at prolonging the pregnancy to the term of a viable fetus.
It is possible to influence the development of the placenta when it is incomplete, improving the conditions for development - by eliminating, for example, the inflammatory process, normalizing blood pressure, lowering the tone of the uterus, and normalizing blood clotting. You can influence the metabolism in the cells of the placenta - by doing this, for example, by introducing drugs into the body of a pregnant woman that help improve the utilization of glucose by cells. It is possible to influence the tone of the vessels, reduce the permeability of the wall and, in this way, the swelling of the tissues decreases and the penetration of oxygen into them improves. But we must understand that we do not cure placental insufficiency, we are only trying to influence the compensatory mechanisms that exist in the placenta, if this succeeds, the manifestations of placental insufficiency disappear. But more often, treatment is aimed at prolonging the pregnancy to the term of a viable fetus.
But if the signs of placental insufficiency increase, and the gestation period is more than 32 weeks, when even in a normal placenta it undergoes involution, the placenta initially developed incorrectly, and now it performs its functions worse, the fetus suffers, then it is useless to treat placental insufficiency, it is better to carry out early delivery and to nurse the newborn without the risk of intrauterine death, which is possible if the placenta depletes its reserves.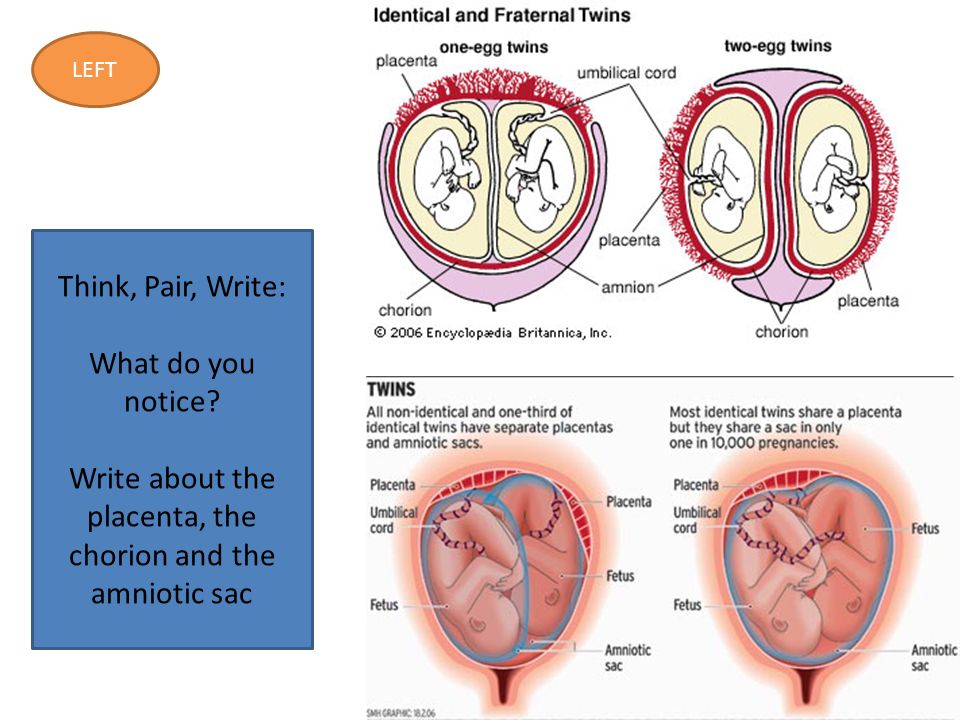 Sometimes it is necessary to make a decision on early delivery and at an earlier date, when the treatment of placental insufficiency is impossible and the delay threatens the life of the fetus.
Sometimes it is necessary to make a decision on early delivery and at an earlier date, when the treatment of placental insufficiency is impossible and the delay threatens the life of the fetus.
What is the placenta
It connects two organisms - the mother and the fetus, providing it with the necessary nutrients.
Where is the placenta located and what does it look like?
In a normal pregnancy, the placenta is located in the body of the uterus along its posterior (more often) or anterior wall. It is fully formed by the 15-16th week of pregnancy, after the 20th week, active exchange begins through the placental vessels. From the 22nd to the 36th week of pregnancy, an increase in the mass of the placenta occurs, and by the 36th week it reaches full functional maturity.
Figure 1. Schematic representation of the location of the placenta in the uterus of a pregnant woman. Photo: Wikipedia (Public Domain) In appearance, the placenta looks like a round flat disk. By the time of delivery, the weight of the placenta is 500-600 g, the diameter is 15-18 cm and the thickness is 2-3 cm.
By the time of delivery, the weight of the placenta is 500-600 g, the diameter is 15-18 cm and the thickness is 2-3 cm.
Functions of the placenta
Photo: zffoto / freepik.com- First, gas exchange occurs through the placenta: oxygen penetrates from the mother's blood to the fetus, and carbon dioxide is transported in the opposite direction.
- Secondly, the fetus receives through the placenta the nutrients necessary for its growth and development. It must be remembered that many substances (alcohol, nicotine, drugs, many drugs, viruses) easily penetrate through it and can have a damaging effect on the fetus. In addition, with its help, the fetus gets rid of the products of its vital activity.
- Thirdly, the placenta provides immunological protection to the fetus, delaying the cells of the mother's immune system, which, having penetrated to the fetus and recognized a foreign object in it, could trigger its rejection reactions. At the same time, the placenta passes maternal antibodies that protect the fetus from infections.
- Fourthly, the placenta plays the role of an endocrine gland and synthesizes hormones (human chorionic gonadotropin (hCG), placental lactogen, prolactin, etc.) necessary to maintain pregnancy, growth and development of the fetus.
Normally, the placenta together with the membranes (afterbirth) is born 10-15 minutes after the birth of the fetus. She is carefully examined and sent for a morphological study. First, it is very important to make sure that the whole placenta was born (that is, there are no damages on its surface and there is no reason to believe that pieces of the placenta remained in the uterine cavity). Secondly, according to the state of the placenta, one can judge the course of pregnancy (whether there was an abruption, infectious processes, etc.).
What do doctors want to know about the placenta?
During pregnancy, it is important to look for signs of placental dysfunction - placental insufficiency. To do this, during an ultrasound study, the structure of the placenta, its location in the uterine cavity, thickness, and the correspondence of the size of the fetus to the gestational age are studied. In addition, the blood flow in the placental vessels is studied.
In addition, the blood flow in the placental vessels is studied.
Degree of maturity
Photo: wavebreakmedia-micro / freepik.comThis parameter, as doctors say, is "ultrasonic", that is, it depends on the density of the structures of the placenta determined by ultrasound.
There are four degrees of placental maturity:
- Normally, zero degree of placental maturity should be determined before 30 weeks of pregnancy.
- The first degree is considered valid from 27 to 34 weeks.
- Second - from 34 to 39.
- Starting from 37 weeks, the third degree of placental maturity can be determined.
At the end of pregnancy, the so-called physiological aging of the placenta occurs, accompanied by a decrease in the area of its exchange surface, the appearance of areas of salt deposition.
Place of attachment
Photo: kuprevich / freepik.com Determined by ultrasound. As mentioned above, during a normal pregnancy, the placenta is located in the body of the uterus.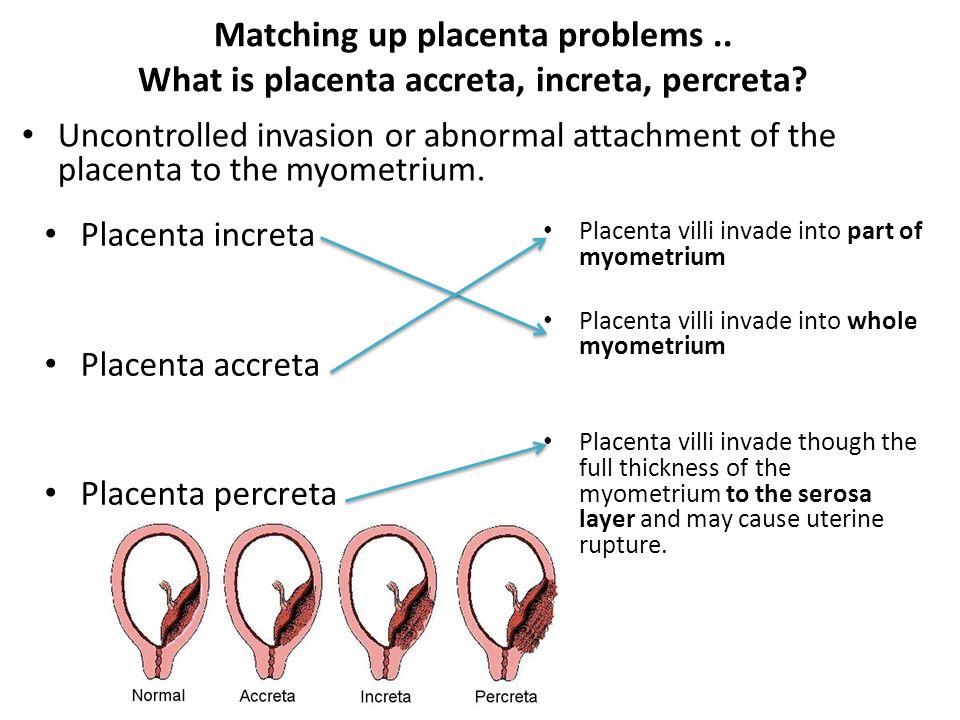 Sometimes, during an ultrasound examination in the first half of pregnancy, it is found that the placenta is located in the lower parts of the uterus, reaching or even overlapping the area of the internal os of the cervix. In the future, as pregnancy progresses, the placenta most often shifts from the lower sections of the uterus to the top. However, if after 32 weeks the placenta still overlaps the area of the internal os, this condition is called *placenta previa**, which is a serious complication of pregnancy.
Sometimes, during an ultrasound examination in the first half of pregnancy, it is found that the placenta is located in the lower parts of the uterus, reaching or even overlapping the area of the internal os of the cervix. In the future, as pregnancy progresses, the placenta most often shifts from the lower sections of the uterus to the top. However, if after 32 weeks the placenta still overlaps the area of the internal os, this condition is called *placenta previa**, which is a serious complication of pregnancy.
Placenta previa can lead to bleeding, which can occur during the second or third trimester of pregnancy or during childbirth.
Ultrasound with placenta previa. Turk J Obstet Gynecol / ResearchGate (Creative Commons Attribution 2.5 Generic license)Thickness
Also determined by ultrasound - placentometry: after establishing the placenta attachment, the area where it has the largest size is found, which is determined. The thickness of the placenta, as already mentioned, continuously increases until 36-37 weeks of pregnancy (by this time it ranges from 20 to 40 mm).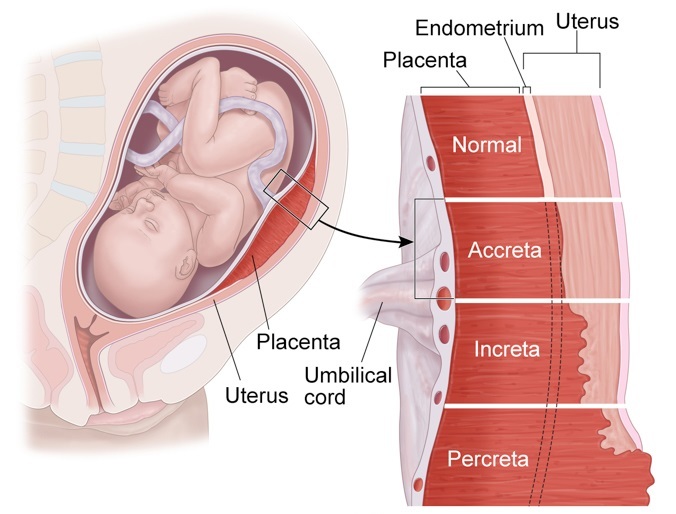 Then its growth stops, and in the future the thickness of the placenta either decreases or remains at the same level.
Then its growth stops, and in the future the thickness of the placenta either decreases or remains at the same level.
Deviation from the norm of at least one of these indicators may indicate trouble during pregnancy.
References
- Tiwari D., Das CR., Sultana R., Kashyap N., Islam M., Bose PD., Saikia AK., Bose S. Increased homocysteine mediated oxidative stress as a key determinant of hepatitis E virus ( HEV) infected pregnancy complication and outcome: A study from Northeast India. // Infect Genet Evol - 2021 - Vol - NNULL - p.104882; PMID:33905889
- Salmanian B., Belfort M.A., Shamshirsaz A.A. The risk of placenta accreta spectrum in women with in vitro fertilization in different populations. // Am J Obstet Gynecol - 2021 - Vol - NNULL - p.; PMID:33905744
- Olmos-Ortiz A., Olivares-Huerta A., García-Quiroz J., Zariñán T., Chavira R., Zaga-Clavellina V., Avila E., Halhali A., Durand M., Larrea F., Díaz L. Placentas associated with female neonates from pregnancies complicated by urinary-tract infections have higher cAMP content and cytokines expression than males.
 // Am J Reprod Immunol - 2021 - Vol - NNULL - p.e13434; PMID:33905581
// Am J Reprod Immunol - 2021 - Vol - NNULL - p.e13434; PMID:33905581 - Tandl V., Hoch D., Bandres-Meriz J., Nikodijevic S., Desoye G., Majali-Martinez A. Different regulation of IRE1α and eIF2α pathways by oxygen and insulin in ACH-3P trophoblast model. // Reproduction - 2021 - Vol - NNULL - p.; PMID:33904834
- Ji S., Gumina D., McPeak K., Moldovan R., Post MD., Su EJ. Human placental villous stromal extracellular matrix regulates fetoplacental angiogenesis in severe fetal growth restriction. // Clin Sci (Lond) - 2021 - Vol - NNULL - p.; PMID:33904582
- Shmeleva EV., Colucci F. Maternal natural killer cells at the intersection between reproduction and mucosal immunity. // Mucosal Immunol - 2021 - Vol - NNULL - p.; PMID:33903735
- Moreno-Sepulveda J., Espinós JJ., Checa MA. Lower risk of adverse perinatal outcomes in natural versus artificial frozen-thawed embryo transfer cycles: a systematic review and meta-analysis. // Reprod Biomed Online - 2021 - Vol - NNULL - p.