When do cleft palates form
Facts about Cleft Lip and Cleft Palate
Cleft lip and cleft palate are birth defects that occur when a baby’s lip or mouth do not form properly during pregnancy. Together, these birth defects commonly are called “orofacial clefts”.
Click here to view a larger image
Click here to view a larger image
What is Cleft Lip?
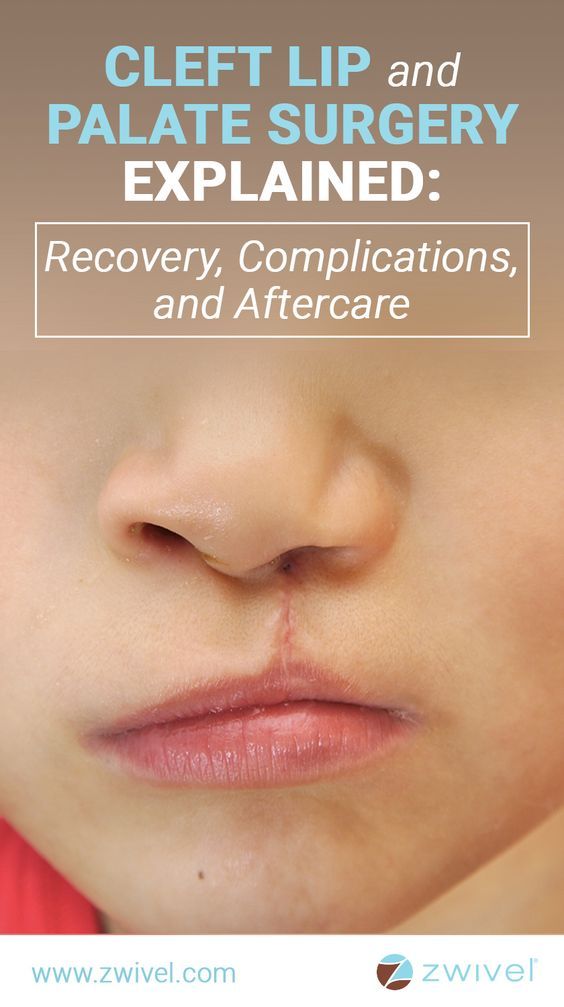
The lip forms between the fourth and seventh weeks of pregnancy. As a baby develops during pregnancy, body tissue and special cells from each side of the head grow toward the center of the face and join together to make the face. This joining of tissue forms the facial features, like the lips and mouth. A cleft lip happens if the tissue that makes up the lip does not join completely before birth. This results in an opening in the upper lip. The opening in the lip can be a small slit or it can be a large opening that goes through the lip into the nose. A cleft lip can be on one or both sides of the lip or in the middle of the lip, which occurs very rarely. Children with a cleft lip also can have a cleft palate.
What is Cleft Palate?
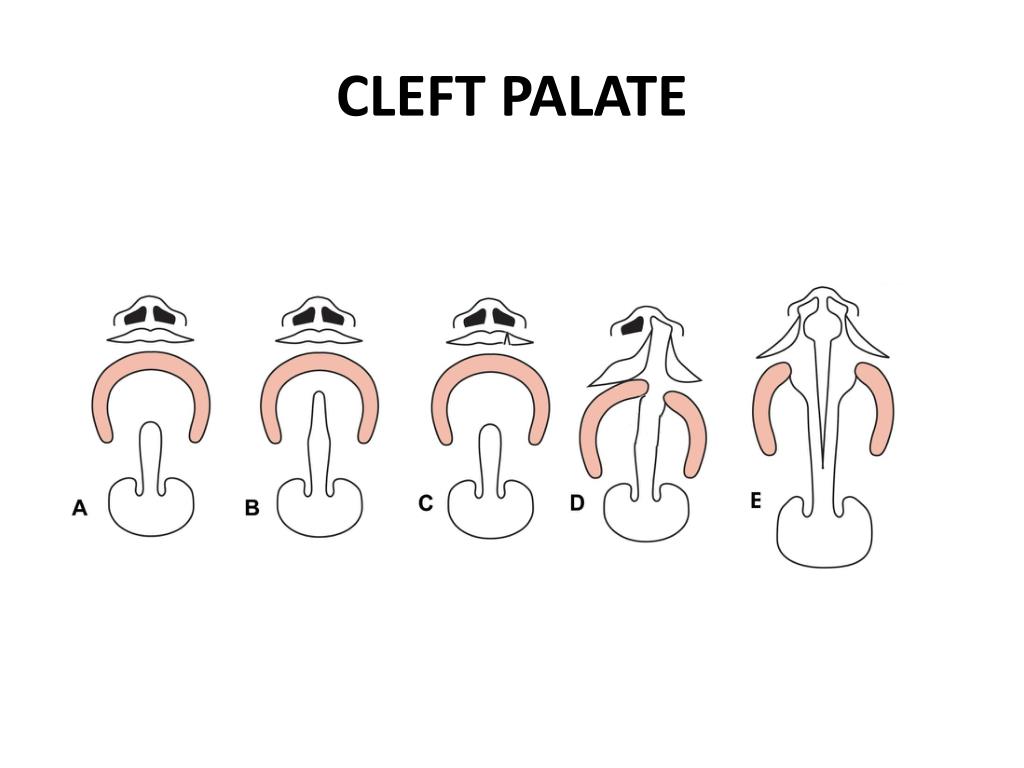
The roof of the mouth (palate) is formed between the sixth and ninth weeks of pregnancy. A cleft palate happens if the tissue that makes up the roof of the mouth does not join together completely during pregnancy. For some babies, both the front and back parts of the palate are open. For other babies, only part of the palate is open.
Other Problems
Children with a cleft lip with or without a cleft palate or a cleft palate alone often have problems with feeding and speaking clearly and can have ear infections. They also might have hearing problems and problems with their teeth.
How Many Babies are Born with Cleft Lip/Cleft Palate?
- About 1 in every 1,600 babies is born with cleft lip with cleft palate in the United States.
- About 1 in every 2,800 babies is born with cleft lip without cleft palate in the United States.
- About 1 in every 1,700 babies is born with cleft palate in the United States.
 1
1
Causes and Risk Factors
The causes of orofacial clefts among most infants are unknown. Some children have a cleft lip or cleft palate because of changes in their genes. Cleft lip and cleft palate are thought to be caused by a combination of genes and other factors, such as things the mother comes in contact with in her environment, or what the mother eats or drinks, or certain medications she uses during pregnancy.
Like the many families of children with birth defects, CDC wants to find out what causes them. Understanding the factors that are more common among babies with a birth defect will help us learn more about the causes. CDC funds the Centers for Birth Defects Research and Prevention, which collaborate on large studies such as the National Birth Defects Prevention Study (NBDPS; births 1997-2011) and the Birth Defects Study To Evaluate Pregnancy exposureS (BD-STEPS; began with births in 2014), to understand the causes of and risks for birth defects, including orofacial clefts.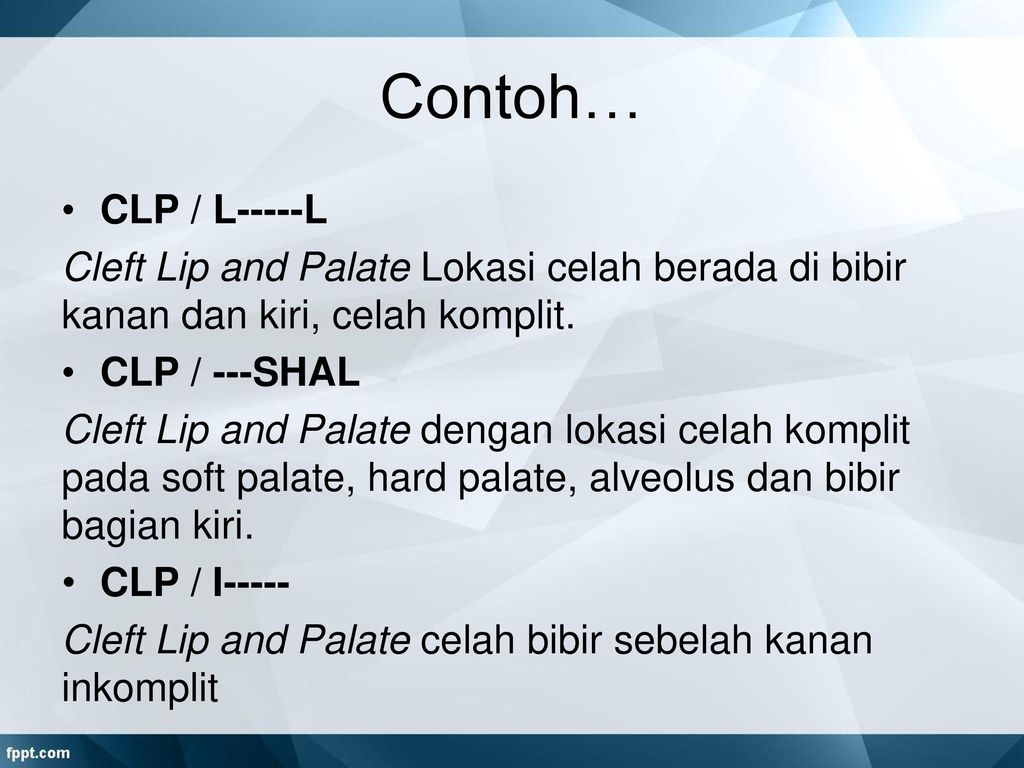
Recently, CDC reported on important findings from research studies about some factors that increase the chance of having a baby with an orofacial cleft:
- Smoking―Women who smoke during pregnancy are more likely to have a baby with an orofacial cleft than women who do not smoke.2-3
- Diabetes―Women with diabetes diagnosed before pregnancy have an increased risk of having a child with a cleft lip with or without cleft palate, compared to women who did not have diabetes.5
- Use of certain medicines―Women who used certain medicines to treat epilepsy, such as topiramate or valproic acid, during the first trimester (the first 3 months) of pregnancy have an increased risk of having a baby with cleft lip with or without cleft palate, compared to women who didn’t take these medicines.6-7
CDC continues to study birth defects, such as cleft lip and cleft palate, and how to prevent them. If you are pregnant or thinking about becoming pregnant, talk with your doctor about ways to increase your chances of having a healthy baby.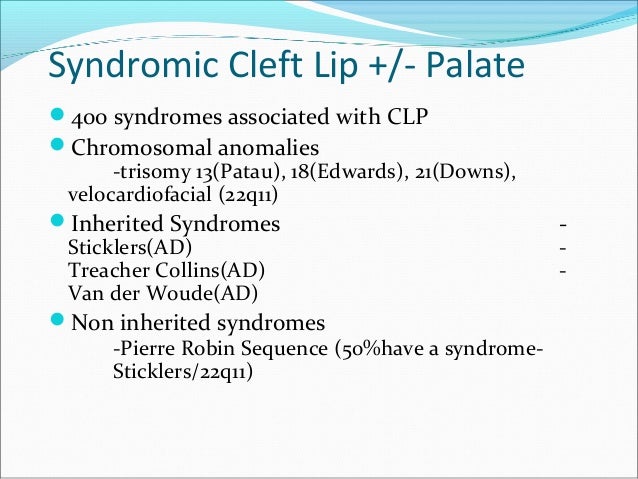
Diagnosis
Orofacial clefts, especially cleft lip with or without cleft palate, can be diagnosed during pregnancy by a routine ultrasound. They can also be diagnosed after the baby is born, especially cleft palate. However, sometimes certain types of cleft palate (for example, submucous cleft palate and bifid uvula) might not be diagnosed until later in life.
Management and Treatment
Services and treatment for children with orofacial clefts can vary depending on the severity of the cleft; the child’s age and needs; and the presence of associated syndromes or other birth defects, or both.
Surgery to repair a cleft lip usually occurs in the first few months of life and is recommended within the first 12 months of life. Surgery to repair a cleft palate is recommended within the first 18 months of life or earlier if possible.8 Many children will need additional surgical procedures as they get older. Surgical repair can improve the look and appearance of a child’s face and might also improve breathing, hearing, and speech and language development.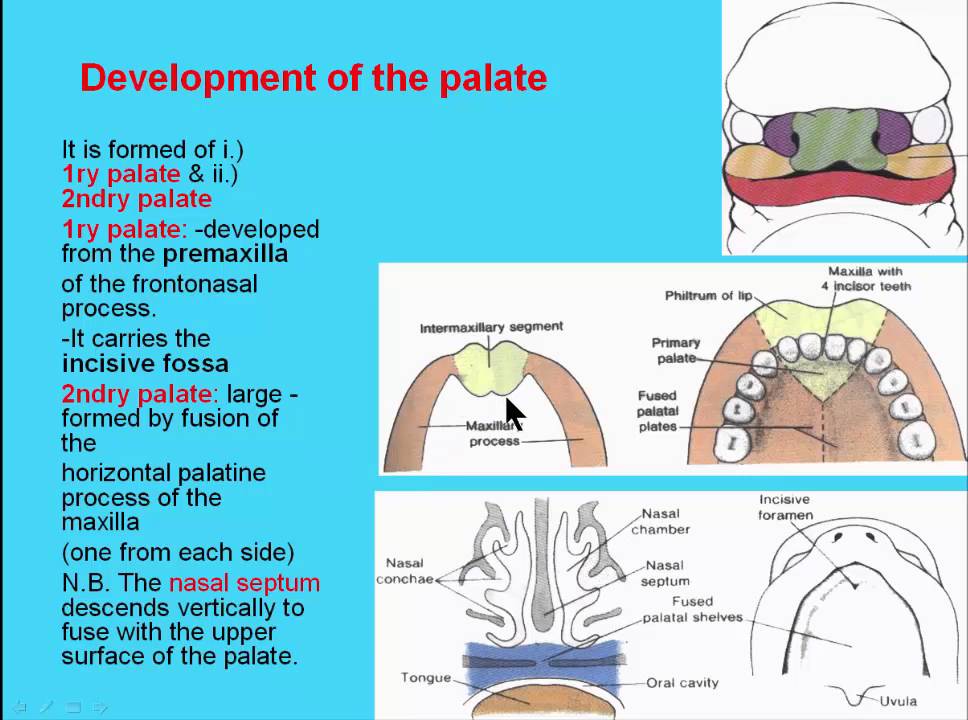 Children born with orofacial clefts might need other types of treatments and services, such as special dental or orthodontic care or speech therapy.4,8
Children born with orofacial clefts might need other types of treatments and services, such as special dental or orthodontic care or speech therapy.4,8
With treatment, most children with orofacial clefts do well and lead a healthy life. Some children with orofacial clefts may have issues with self-esteem if they are concerned with visible differences between themselves and other children. Parent-to-parent support groups can prove to be useful for families of babies with birth defects of the head and face, such as orofacial clefts.
References
- Mai CT, Isenburg JL, Canfield MA, Meyer RE, Correa A, Alverson CJ, Lupo PJ, Riehle‐Colarusso T, Cho SJ, Aggarwal D, Kirby RS. National population‐based estimates for major birth defects, 2010–2014. Birth Defects Research. 2019; 111(18): 1420-1435.
- Little J, Cardy A, Munger RG. Tobacco smoking and oral clefts: a meta-analysis. Bull World Health Organ. 2004;82:213-18.
- Honein MA, Rasmussen SA, Reefhuis J, Romitti P, Lammer EJ, Sun L, Correa A.
 Maternal smoking, environmental tobacco smoke, and the risk of oral clefts. Epidemiology 2007;18:226–33.
Maternal smoking, environmental tobacco smoke, and the risk of oral clefts. Epidemiology 2007;18:226–33. - Yazdy MM, Autry AR, Honein MA, Frias JL. Use of special education services by children with orofacial clefts. Birth Defects Research (Part A): Clinical and Molecular Teratology 2008;82:147-54.
- Correa A, Gilboa SM, Besser LM, Botto LD, Moore CA, Hobbs CA, Cleves MA, Riehle-Colarusso TJ, Waller DK, Reece EA. Diabetes mellitus and birth defects. American Journal of Obstetrics and Gynecology 2008;199:237.e1-9.
- Margulis AV, Mitchell AA, Gilboa SM, Werler MM, Glynn RJ, Hernandez-Diaz S, National Birth Defects Prevention Study. Use of topiramate in pregnancy and risk of oral clefts. American Journal of Obstetrics and Gynecology 2012;207:405.e1-e7.
- Werler MM, Ahrens KA, Bosco JL, Michell AA, Anderka MT, Gilboa SM, Holmes LB, National Birth Defects Prevention Study. Use of antiepileptic medications in pregnancy in relation to risks of birth defects. Annals of Epidemiology 2011;21:842-50.
- American Cleft Palate-Craniofacial Association. Parameters for evaluation and treatment of patients with cleft lip/palate or other craniofacial anomalies. Revised edition, Nov 2009. Chapel Hill, NC. P. 1-34. https://acpa-cpf.org/wp-content/uploads/2017/06/Parameters_Rev_2009_9_.pdf
The images are in the public domain and thus free of any copyright restrictions. As a matter of courtesy we request that the content provider (Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities) be credited and notified in any public or private usage of this image.
The images are in the public domain and thus free of any copyright restrictions. As a matter of courtesy we request that the content provider (Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities) be credited and notified in any public or private usage of this image.
Cleft Palate (for Parents) - Nemours KidsHealth
What Is a Cleft Palate?
A cleft palate (PAL-it) is when a baby is born with an opening (a cleft) in the roof of the mouth.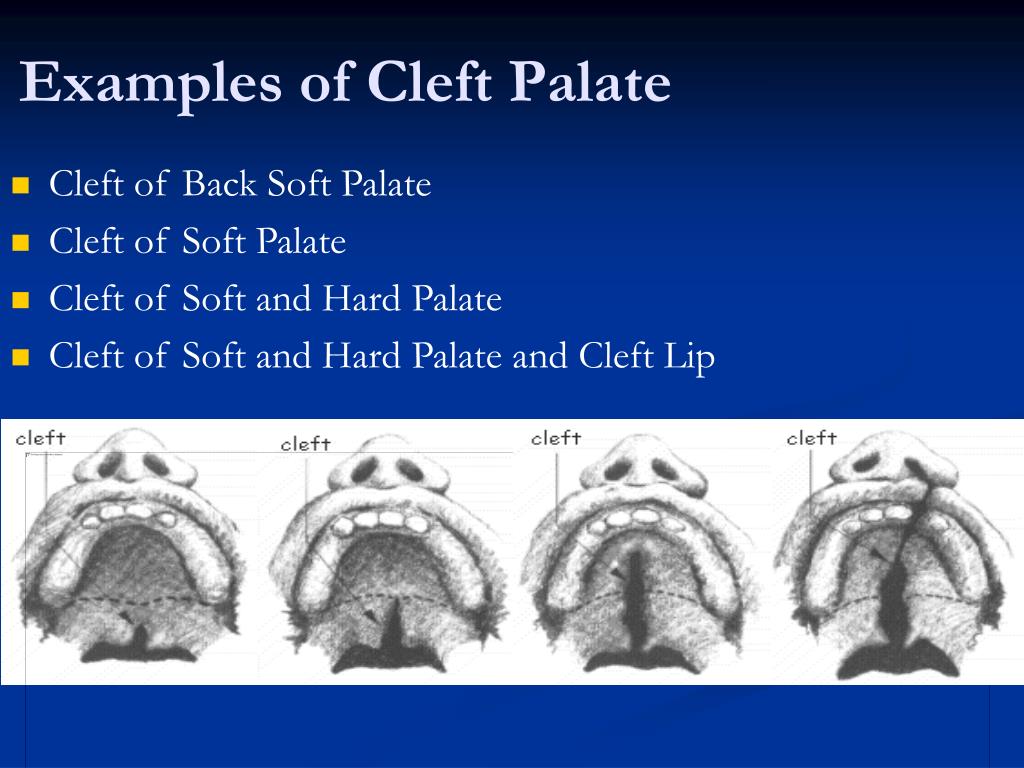 This leaves a hole between the nose and the mouth.
This leaves a hole between the nose and the mouth.
The opening can:
- just be in the back of the palate (the soft palate)
or - extend into the front of the palate behind the gums (the hard palate)
Sometimes the opening in the palate can connect with an opening in the gums and the lip (cleft lip and palate). These orofacial clefts are some of the most common birth defects. Most kids can have surgery to repair them early in life.
A baby with a cleft might have:
- only a cleft palate
- only a cleft lip
- both a cleft lip and a cleft palate
What Causes Cleft Palate?
During the first 6 to 10 weeks of pregnancy, the bones and skin of a baby's upper jaw, nose, and mouth normally come together (fuse) to form the roof of the mouth and the upper lip. A cleft palate happens when parts of the roof of the mouth do not fuse together completely.
Doctors don't always know why a baby develops a cleft, though some clefts may be related to genetic (inherited) factors.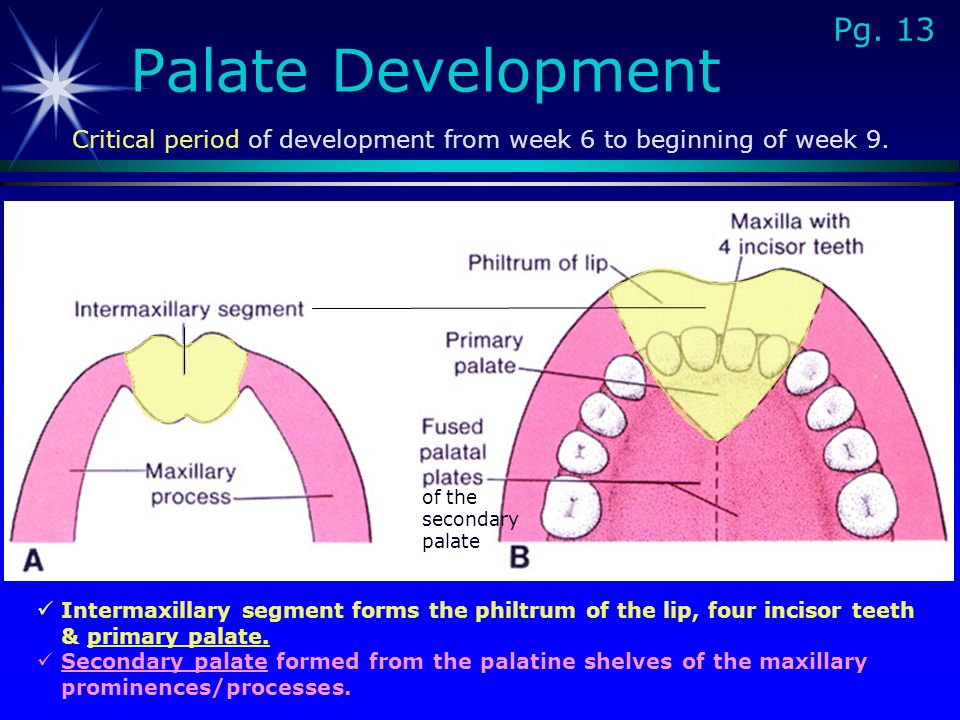 Also, some environmental factors can increase the risk of a birth defect, such as:
Also, some environmental factors can increase the risk of a birth defect, such as:
- taking certain medicines (such as some anti-seizure medicines) during pregnancy
- not getting the right amount of prenatal nutrients
- exposure to some chemicals during pregnancy
- smoking cigarettes, using drugs, and/or drinking alcohol during pregnancy
How Is a Cleft Palate Diagnosed?
Newborns have an oral exam soon after they're born. Doctors usually find a cleft palate when they examine the inside of a baby's mouth during this exam.
How Is a Cleft Palate Treated?
A cleft palate usually is repaired with surgery called palatoplasty (PAL-eh-tuh-plass-tee) when the baby is 10–12 months old. The goals of palatoplasty are to:
- Close the opening between the nose and mouth.
- Help create a palate that works well for speech.
- Prevent food and liquid from leaking out of the nose.
In this surgery, a plastic surgeon will:
- Close the cleft in layers.
- Rearrange and repair the muscles of the soft palate so they work better during speech.
- Make two incisions (cuts) on each side of the palate behind the gums to ease tension on the palate repair.
This surgery requires general anesthesia and takes about 2–3 hours. Most babies can go home after 1 or 2 days in the hospital. The stitches will dissolve on their own.
Your child will need a liquid diet for a week or two, then will eat soft foods for several more weeks before going back to a regular diet. You may be asked to keep your baby in special sleeves ("no-nos") that prevent the elbows from bending. This is so your baby can't put any fingers or hard objects into the mouth, which could make the cleft palate repair come open.
When Should I Call the Doctor?
Cleft palate surgery has greatly improved in recent years. Most kids who undergo it have very good results. There are risks with any surgery, though, so call the doctor if your child:
- has a fever above 101.
 4°F (38.5°C)
4°F (38.5°C) - has lasting pain or discomfort
- has heavy bleeding from the mouth or nose
- won't drink fluids
- isn't making wet diapers
What Else Should I Know?
A child with a cleft palate can sometimes have other health problems, such as:
- trouble breathing
- frequent ear infections
- trouble feeding
- hearing loss
- eye problems
- speech difficulties
It's important to work with a care team experienced in treating children with cleft lip and palate. Besides the pediatrician, a child's treatment team will include:
- plastic surgeon
- ear, nose, and throat (ENT) physician (otolaryngologist)
- orthodontist
- dentist
- speech-language pathologist
- audiologist
You might also work with:
- an oral surgeon
- a social worker
- a psychologist or therapist
- a geneticist
- a team coordinator
Some kids with cleft palate may need other surgeries as they get older.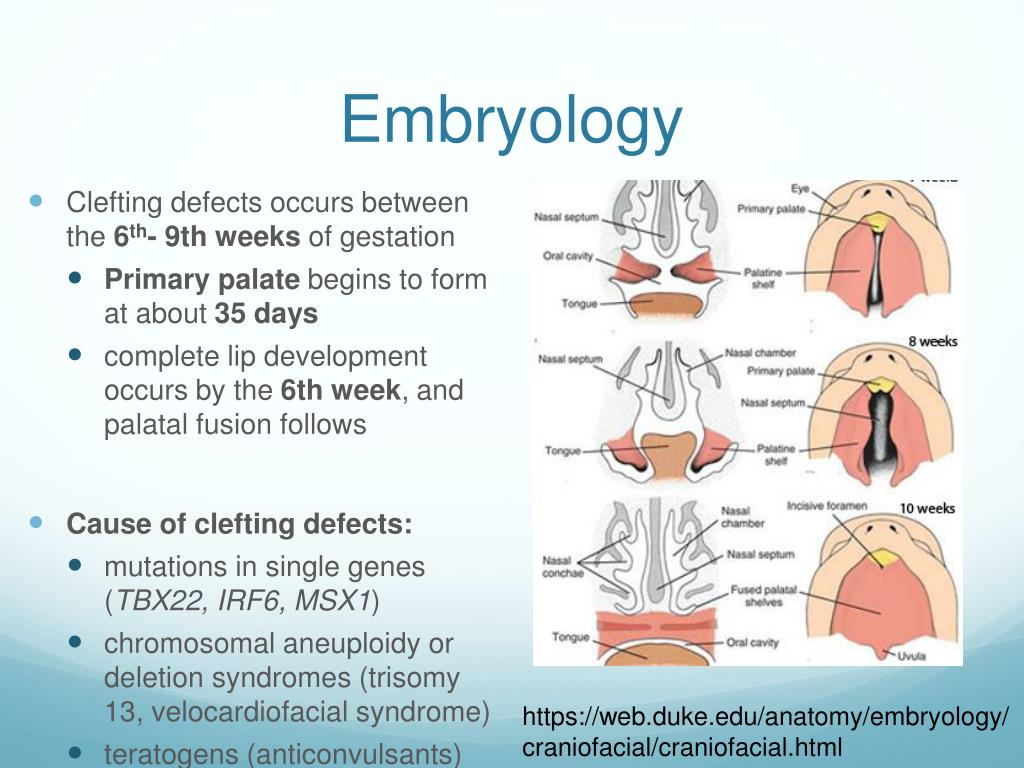 These might include:
These might include:
- Speech surgery: Children can develop speech problems even after the palate has been repaired. At your regular appointments with the cleft team, the speech-language pathologist will carefully listen to your child's speech to help the surgeon decide if another surgery is needed to improve speech.
- Orthognathic (or-thig-NATH-ik) surgery: Some children with cleft palate need this surgery to realign the jaws and teeth when they're older. It's done when the child is finished growing.
Looking Ahead
Most kids with cleft palate are treated successfully with no lasting problems. A team experienced in treating children with cleft lip and palate can create a treatment plan tailored to your child's needs.
The psychologists and social workers on the treatment team are there for you and your child. So turn to them to help guide you through any hard times. You also can find more information and support online:
- American Cleft Palate-Craniofacial Association (ACPA)
- Cleft Lip & Palate Association
- FACES: The National Craniofacial Association
- Smile Train
Reviewed by: Brian C.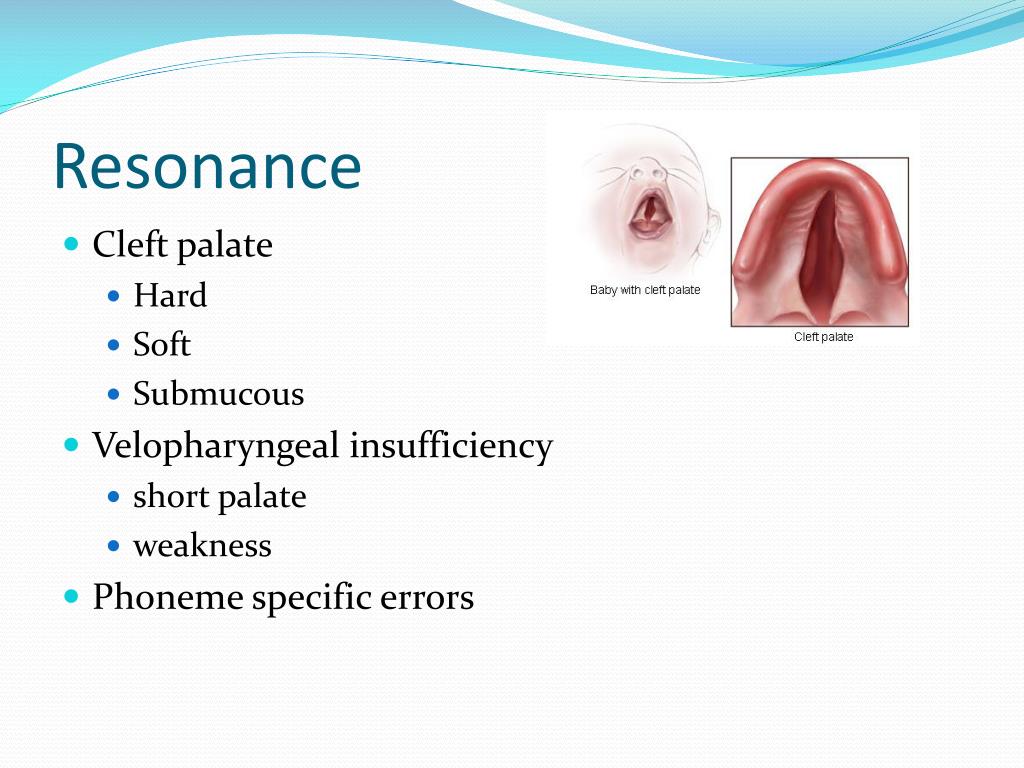 Kellogg, MD
Kellogg, MD
Date reviewed: June 2019
Cleft lip and palate: the defect can be corrected
Cleft lip and palate is one of the most common congenital malformations of the upper jaw: it occurs in a third of patients with congenital developmental anomalies. In Moscow, 1 in 800 babies is born with this malformation.
An anomaly is detected, as a rule, on ultrasound in the 1-2 trimester of pregnancy. Such news is a huge stress for future parents. But in most cases, due to timely and qualified treatment, cosmetic and functional defects in the baby can be eliminated. nine0003
At what age is surgical treatment most effective and how is a complex anomaly treated?
What influences the formation of a defect?
The defect is formed in the first two months of intrauterine development of the child, when the formation of the facial skeleton takes place. The cause of the development of pathology is an anomaly of chromosomes.
Both hereditary factors (7%) and external factors (40%) influence the development of the defect.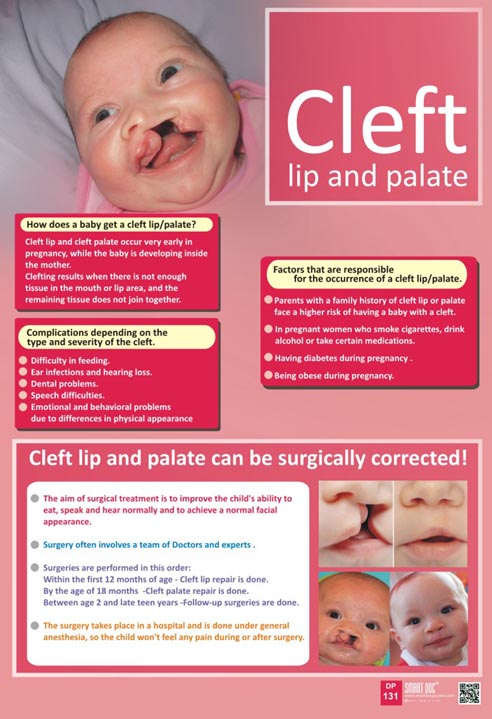 External ones include infectious and viral diseases, smoking, drugs, alcoholism, the use of certain medicinal substances, a lack of vitamin folic acid, poor ecology, and so on. nine0003
External ones include infectious and viral diseases, smoking, drugs, alcoholism, the use of certain medicinal substances, a lack of vitamin folic acid, poor ecology, and so on. nine0003
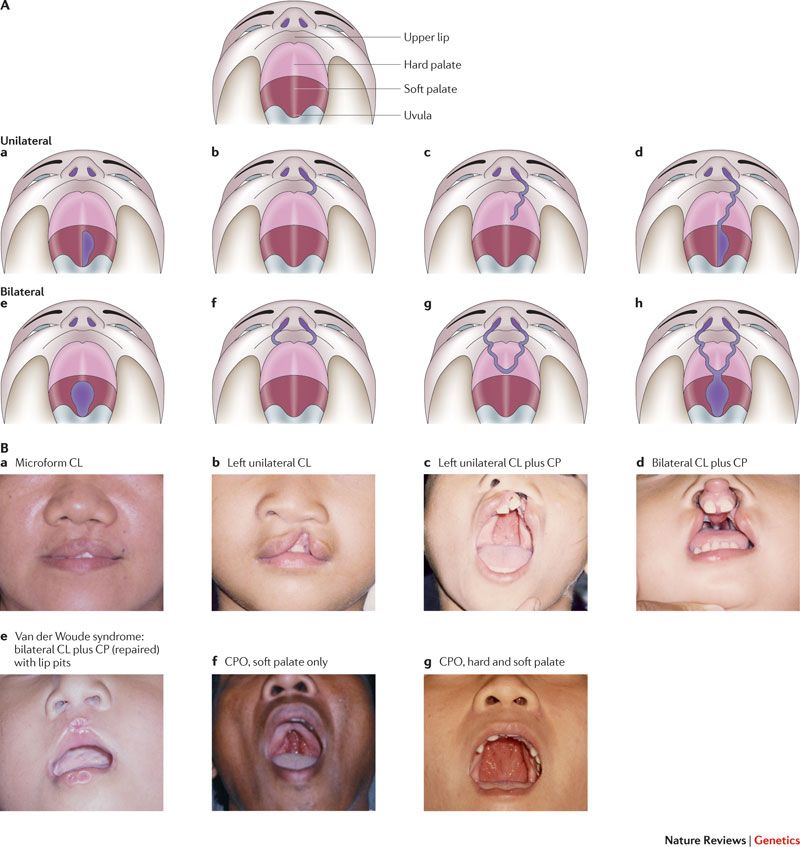
What types of clefts are there?
Clefts can be both lips and palate. They, in turn, are isolated (only the lips or only the palate) and through, when the defect extends to the upper lip, alviolar process and palate. Each of the types has different degrees of severity. In addition, the defect can be both unilateral (often on the left) and bilateral.
With an isolated cleft lip, as a rule, the deformity may be minor, or it may be accompanied by deformity of the nasal septum, alar cartilage and cleft alveolar process, which further leads to problems with the teeth. nine0003
With cleft palate (from a slight splitting of the soft palate only to severe bilateral lesions of the soft and hard palate), children may have problems with eating, breathing, sucking, and later with sound pronunciation.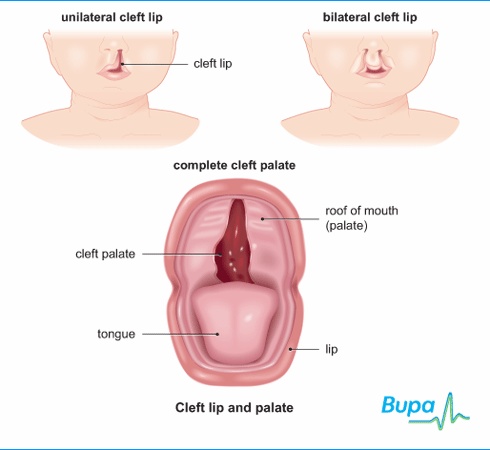 Thanks to timely surgical intervention, it is possible to obtain an ideal result of treatment.
Thanks to timely surgical intervention, it is possible to obtain an ideal result of treatment.
The most severe form is a bilateral penetrating cleft lip and palate. But even in this case, timely treatment and rehabilitation give the baby a chance to recover. nine0003
If a cleft is found in a baby during intrauterine diagnosis, what should parents do?
The most important thing I would like to say to parents who are faced with this problem is not to worry. It is important to immediately seek a consultation with maxillofacial surgeons involved in the treatment of pathology.
We advise future parents even before the baby is born. We tell you how to properly feed a child - it is better to use a spoon or a bottle with special nipples in order to maintain swallowing reflexes, because they can fade with prolonged tube feeding. nine0003
Often this defect can be accompanied by pathology of the bone and cardiovascular systems, kidneys. Therefore, it is important to undergo research immediately after birth and exclude these diseases. If the baby does not have other serious concomitant diseases, we prescribe planned surgical treatment to eliminate the defect.
If the baby does not have other serious concomitant diseases, we prescribe planned surgical treatment to eliminate the defect.
At the request of the parents, after the maternity hospital, the child can be transferred to the neonatology department of our hospital, where the mother will be taught how to feed the child, examined and given recommendations on how to manage it before a planned operation. nine0003
At what age is surgical treatment most effective?
The optimal age for surgery to correct cleft lip and eliminate nasal deformity, if there is no gross pathology among other systems, is 3 months. Earlier plastic surgeries do not provide the best aesthetic result.
If the child has a severe cleft, the correction can be done in two steps. At six months, if it concerns the palate - the soft palate, from one to two years - the hard palate. If surgical treatment is carried out in one stage, then it is performed at the age of 9months to 1.5 years.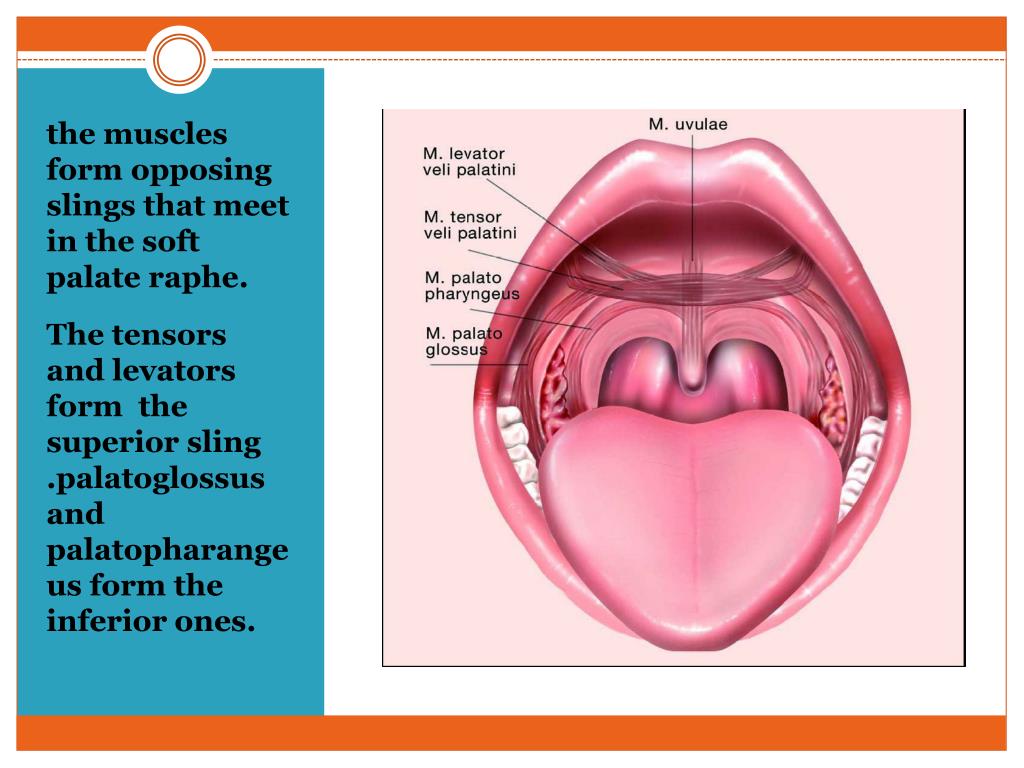 This has a number of advantages: the child endures one rather than two anesthesia, the tissues are more mature, which means that the result of the treatment will be more effective. We advise palatoplasty for children under two years of age, until incorrect speech has formed in the brain - the center of speech.
This has a number of advantages: the child endures one rather than two anesthesia, the tissues are more mature, which means that the result of the treatment will be more effective. We advise palatoplasty for children under two years of age, until incorrect speech has formed in the brain - the center of speech.
If the child has a severe cleft, the correction can be done in two steps. At six months, if it concerns the palate - the soft palate, from one to two years - the hard palate. If surgical treatment is carried out in one stage, then it is performed at the age of 9months to 1.5 years. This has a number of advantages: the child endures one rather than two anesthesia, the tissues are more mature, which means that the result of the treatment will be more effective. We advise palatoplasty for children under two years of age, until incorrect speech has formed in the brain - the center of speech.
What operations are performed for cleft lip and palate?
Correction of a congenital anomaly requires a comprehensive approach.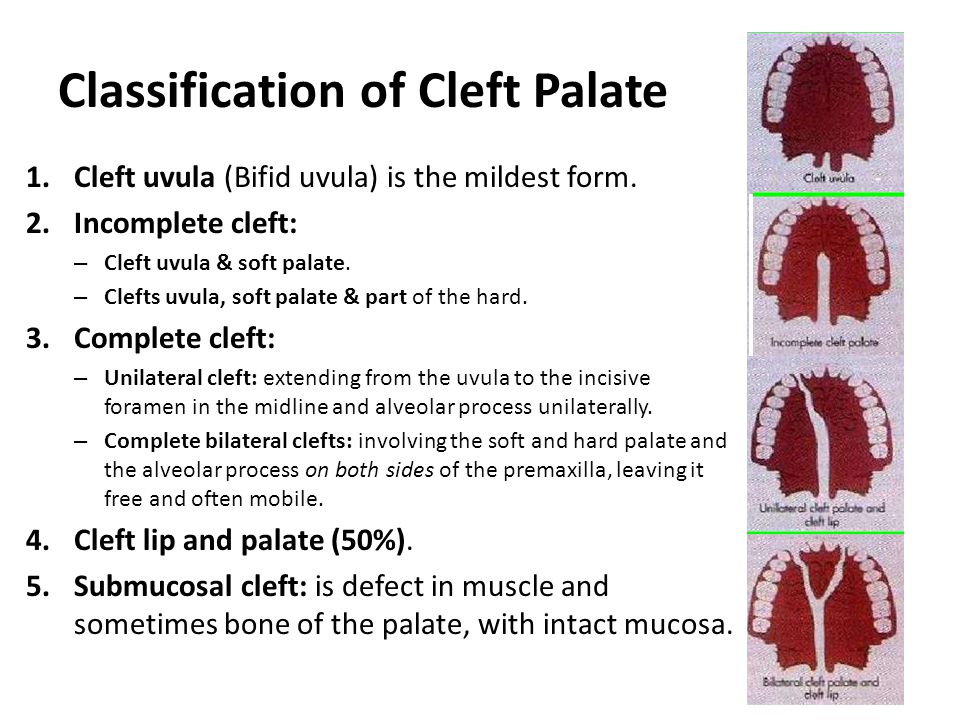 It is aimed not only at eliminating a cosmetic defect, but also at reconstructing functional disorders, eliminating problems with swallowing, breathing and sound pronunciation. The volume and type of operational assistance depends on the characteristics of each child and is selected individually. nine0003
It is aimed not only at eliminating a cosmetic defect, but also at reconstructing functional disorders, eliminating problems with swallowing, breathing and sound pronunciation. The volume and type of operational assistance depends on the characteristics of each child and is selected individually. nine0003
If the cleft appears as an isolated lip or palate, the surgical treatment is performed in one step. In the most difficult cases, the correction is carried out in several stages.
Cheiloplasty is performed for isolated cleft lip without severe nose deformity. The vestibule of the oral cavity is created (the space located under the upper lip), the integrity of the circular muscle of the upper lip is restored, and a red border is formed. If the defect of the upper lip is more severe, then one-stage cheilorhinoplasty (lip and nose plastic surgery) is performed. We perform lip plasty and put the alar cartilages of the nose in a symmetrical position. On the 7th day, postoperative sutures are removed and the children are discharged from the hospital with recommendations for further management of the child.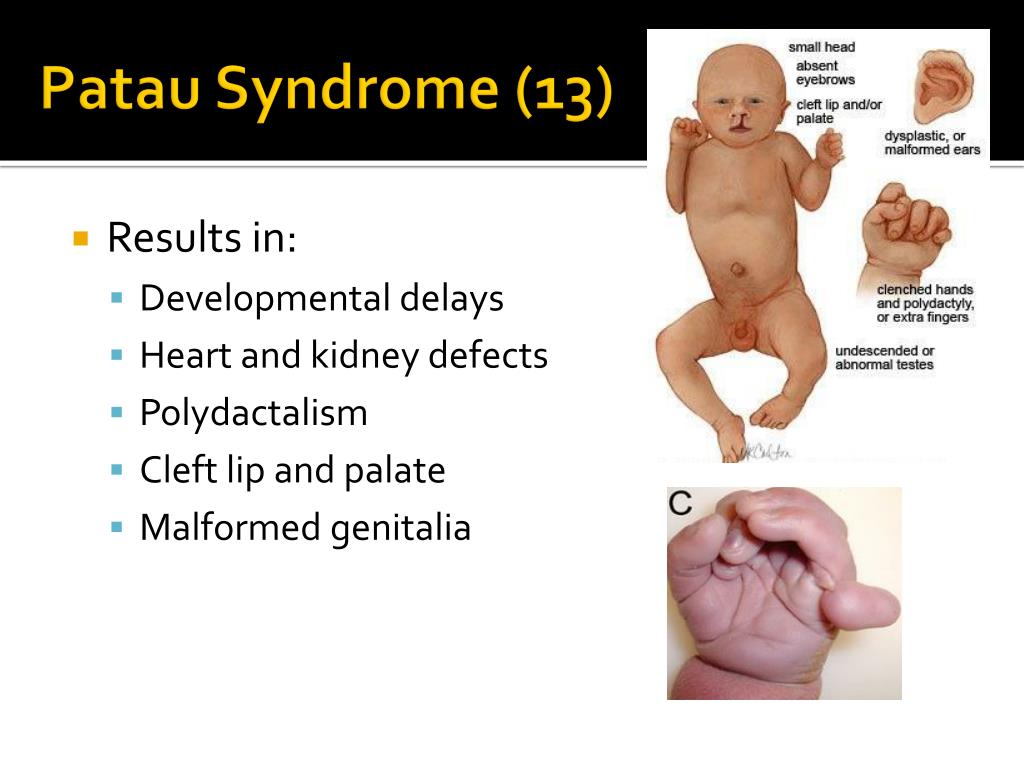 nine0003
nine0003
Isolated cleft palate appears as an anatomical lesion in the soft palate (movable veil of the palate) or soft and hard palate. Pathology is accompanied by a violation of swallowing, breathing and sound pronunciation. The plasty of the palate includes the restoration of the hard palate and soft tissues of the palatine curtain, the closure of the alveolar process. After the operation, when children reach 3 years of age, classes with a speech therapist are recommended to prevent speech disorders, manifested by nasal and illegible speech. nine0003
If speech disorders are not eliminated by the efforts of speech therapists alone, then there is a surgical correction - elimination of palatopharyngeal insufficiency. The operation consists in transplanting flaps on the pedicle in the area of the pharyngeal ring.
From the age of 5, the child is sent for treatment to an orthodontist to eliminate defects in the dentoalveolar system. At the end of orthodontic treatment, the next stage of surgical treatment is performed - bone grafting of the cleft of the alveolar process to eliminate the bone defect of the alveolar process.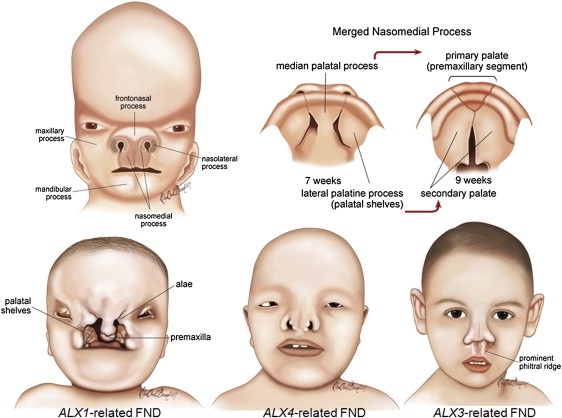 nine0003
nine0003
The Morozov Children's Hospital has accumulated extensive experience in the effective treatment of cleft lip and palate. Every year, doctors perform up to 200 operations to correct these congenital malformations.
Cleft lip and palate | Bebbo
Submitted by sasanchez on Thu, 02/17/2022 - 13:20
Cleft lip ("cleft lip") or palate ("cleft palate") refers to the phenomenon when the lip or palate does not close properly. This creates a cleft or hole in the lip or mouth. Cleft lip and palate can occur separately or together. More common is cleft lip. nine0003
Cleft lip and palate are congenital pathologies - they occur during the development of the fetus in the womb.
It is not exactly known what causes cleft palate and lip. It is believed that they are largely due to genetic factors, although often there are no known cases of such disorders in the genus.
There is some evidence that smoking and drinking during pregnancy, pre-pregnancy diabetes, and obesity during pregnancy may increase the risk of having a baby with or without cleft lip and palate. nine0003
Having a baby with a cleft lip and/or palate can be very distressing, but it is important to remember that these disorders can be corrected.
Cleft lip and palate symptoms
Cleft lip and/or palate can vary in severity. They can range from a small notch in the upper lip to a large gap in the lip and palate.
In the case of a cleft palate, a hole in the palate indicates an abnormal connection between the mouth and nose.
Other cleft lip and palate problems
Babies with cleft palate can be extremely difficult to feed . This is due to the fact that it is difficult or impossible for them to suck, although they do not have problems with swallowing.
Babies with cleft palate can often get ear infections with a risk of hearing loss.
Children with cleft lip and palate may also have problems with teeth and gums . For example, they may be missing teeth, have extra teeth, or teeth that will erupt in the wrong place or in an abnormal direction. This may affect milk and/or molars. nine0003
Cleft lip and palate can cause a nasal (nasal) tone of voice and can also affect the appearance of a child's nose.
Treatment of cleft lip and palate
Treatment of cleft lip and/or palate depends on the severity.
First of all, babies need to be fed with a special cup or an extended nipple. Thanks to them, milk will enter the back of the throat.
All cases require surgery, and the type, complexity, and number of surgeries will depend on the severity of the cleft lip or palate. Repair cleft lip usually at 3–6 months of age, and cleft palate at about 9 months of age.-12 months before babies start talking. Lips usually look much better after surgery.
After surgery, children with cleft lip or palate need regular visits to specialists who will examine them. This is necessary in order to check how they grow, how they look, speak and hear. These check-ups let doctors know if additional surgery is needed.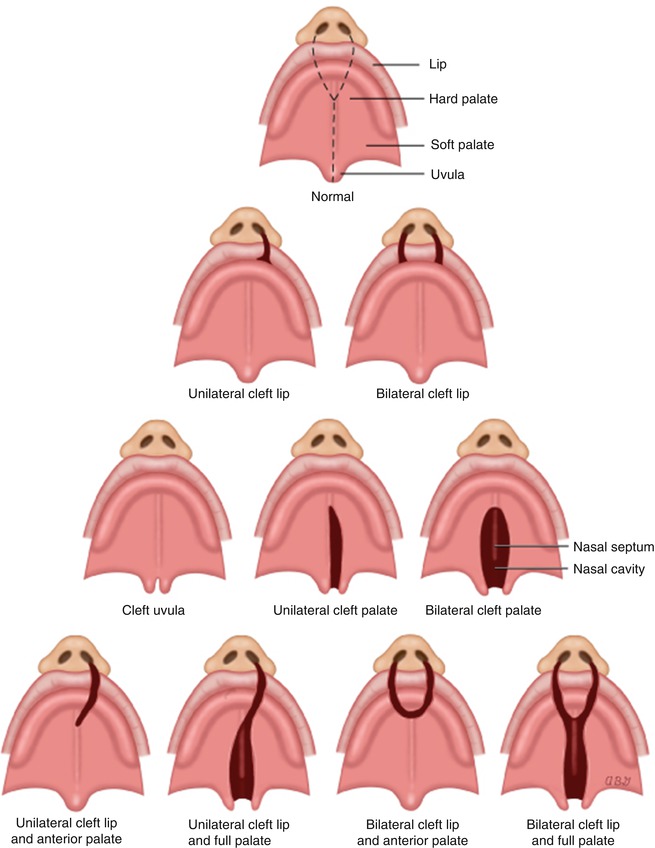
Children with cleft lip and palate often need additional treatment . For example, children with cleft palate need to see a speech therapist to help them learn to speak normally. Children may also need specialized dental care to correct dental problems. nine0003
Cleft lip and palate prevention
- See a genetic counseling specialist. Especially if you have had cases of cleft lip and palate in your family.
- Take your prenatal vitamins. If you are planning to become pregnant soon, ask your doctor if you should take prenatal vitamins.
- Do not smoke or drink alcohol. Drinking alcohol or smoking during pregnancy increases the risk of having a baby with malformations. nine0126
- Gain healthy weight during pregnancy.
.
Australian Article
On
Cover Image
Image
511 - Cleft lip and palate.