What is percentile in pregnancy
Understanding baby growth charts | Pregnancy Birth and Baby
Understanding baby growth charts | Pregnancy Birth and Baby beginning of content6-minute read
Listen
Baby or infant growth charts show how your child is growing. It's important not to compare your baby's size with that of other babies since this may be misleading. The most important thing is that your baby is healthy, happy, and growing appropriately.
What is an infant growth chart?
An infant growth chart helps you, your doctor and other health professionals keep track of how your baby is growing.
Your baby’s growth is a good indicator of their overall health and nutrition. This is done by comparing your baby's growth with that of other babies of the same age. There are different charts for:
- males and females
- infants and older children
Growth charts record changes in your baby's measurements, including their:
- length (height)
- weight
- head circumference
These measurements are recorded on the chart so you can see how they change over time. On the vertical (up-and-down) axis is the measurement; on the horizontal (side-to-side) axis is the baby's age.
There will probably be a growth chart in your child's personal health record. Depending on where you live, this record is known by different names. In New South Wales, it is the Blue Book. In Queensland, it is the Red Book. Your child and family health nurse or doctor may also keep a growth chart.
Infant growth (aged 0 to 2 years) is usually calculated using the World Health Organization's (WHO) growth standards.
Most states and territories use growth charts based on those from the US Centers for Disease Control.
What are percentiles?
Like adults, babies come in all shapes and sizes. The growth charts show this by using 'percentiles'. Below are some examples:
- A baby on the 50th percentile for weight is right in the middle of the normal weight range: 50% of babies their age are lighter, and 50% are heavier.
- A baby on the 5th percentile weighs less than 95% of other babies of that age.
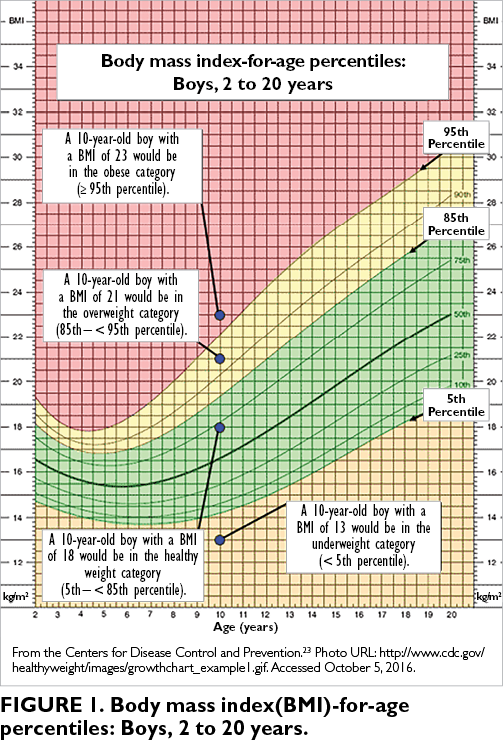
- A baby on the 90th percentile weights more than 90% of other babies that age.
Some babies will always be small. Others will always be large.
All babies grow at different rates, and 'normal' growth varies a lot. The important thing is that your baby continues to grow at a similar rate.
The WHO's infant growth chart for girls aged 0 to 2. The WHO's infant growth chart for boys aged 0 to 2.How are the growth charts used?
Growth charts will help you track how your baby is growing by showing normal growth curves (i.e., always increasing). You can plot your baby’s growth to see if it follows a similar pattern to other babies on that percentile.
Your baby is weighed and measured at birth and then when they are 2 weeks old. After that, their growth is best tracked by measuring them every month until they are 6 months old. Don't worry if their weight goes up and down a bit from day to day — this is normal.
Growth charts are used until your child turns 18.
You can talk to your child health nurse or doctor about other health checks to make sure your child is growing and developing normally.
How will my baby be measured?
Special infant scales are used to weigh babies under 2 years old. Newborns lie down on these scales. It’s more exact to weigh babies with no clothes on until they are 12 months.
After they turn 2, they are measured standing up in light clothes. You baby's head circumference is measured using a tape measure.
If your child was born prematurely, their age is 'corrected'. This means their age is adjusted to account for the number weeks that they were born prematurely. This is done by taking the number of weeks early they were away from their birth age. This corrected age is recorded on all their growth charts. This will continue until they turn 2 years old.
When should I be worried?
It’s important to measure a baby’s growth to see if they are healthy and developing properly. Parents are often worried that their baby isn't growing fast enough. However, it's not the only way to tell if they're healthy.
However, it's not the only way to tell if they're healthy.
All babies lose some weight in the week after birth. They usually regain this weight by 2 weeks. Most babies double their birth weight by 4 months.
Male babies usually triple their weight by 13 months. Female babies usually triple their weight by 15 months.
There is unlikely to be anything wrong if your baby:
- has at least 5 very wet nappies each day
- has pale urine (wee)
- does well-sized, soft poos
- has good skin colour and muscle tone
- is meeting other developmental milestones
Weight gain can be affected by an infection or vomiting. If you are ever worried, talk to your child and family health nurse or doctor.
If your baby’s growth percentile changes a lot – by 2 major percentile lines - talk to your child and family health nurse or doctor. They will assess the child's growth trend to see if there is any reason to be worried.
Remember, don't compare your baby’s growth to that of other baby’s. The important thing is that they continue growing following the same percentile.
The important thing is that they continue growing following the same percentile.
Where can I get more information about baby growth charts?
If you have any questions about your baby's growth or development, you can call Pregnancy, Birth and Baby on 1800 882 436. Or see your child's doctor or early childhood nurse.
Speak to a maternal child health nurse
Call Pregnancy, Birth and Baby to speak to a maternal child health nurse on 1800 882 436 or video call. Available 7am to midnight (AET), 7 days a week.
Sources:
Australian Breastfeeding Association (Baby weight losses and weight gains), World Health Organization (Child growth standards), National Children’s Digital Health Collaborative (Child Digital Health Record Digital Baby Books), Healthy Kids for Professionals (Guide to accurately weighing children using infant scales), Healthy Kids for Professionals (Guide to accurately weighing children using standing scales), Child and Adolescent Health Service (Growth – birth to 18 years), The Royal Children's Hospital Melbourne (Clinical Practice Guidelines: Slow Weight Gain)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: July 2022
Back To Top
Need more information?
Growth charts for babies & children | Raising Children Network
Child growth charts give a guide to how well children are growing. Growth usually follows a typical pattern, which is influenced by genes and environment.
Read more on raisingchildren.net.au website
Baby weight losses and weight gains | Australian Breastfeeding Association
One of the common concerns for parents is if their baby is gaining enough weight. What is the normal growth rate for babies? How can you weigh a baby accurately? What is a growth chart and how can you read one? This article answers all your questions about baby weight gains or if you think your baby is not gaining enough weight.
Read more on Australian Breastfeeding Association website
Your baby's growth and development - 10 months old
A 10-month-old will be very active. As a parent, you’ll probably be chasing them around as they crawl, and be learning more about their developing personality.
Read more on Pregnancy, Birth & Baby website
Tooth arrival chart
Babies are usually born with 20 baby teeth. Use this chart to see when you can expect their teeth to come through.
Read more on Pregnancy, Birth & Baby website
Your baby's growth and development - 1 month old
Your baby starts developing from the moment they are born. At 1 month, cuddling, sleeping and feeding are all that really matters to your baby.
At 1 month, cuddling, sleeping and feeding are all that really matters to your baby.
Read more on Pregnancy, Birth & Baby website
Your baby's growth and development - 11 months old
At 11 months old, your baby is almost a toddler – you’ll probably be surprised at how quickly they can move around your home and how independent they are becoming.
Read more on Pregnancy, Birth & Baby website
Your baby's growth and development - 3 months old
By 3 months, your baby will have formed a strong attachment to you. They will respond with lots of smiles, and you can really enjoy your baby as they develop.
Read more on Pregnancy, Birth & Baby website
Your baby's growth and development - 5 months old
At 5 months, your baby is quickly growing and developing. They may soon be sitting up on their own, preparing for solid foods and learning new language skills.
They may soon be sitting up on their own, preparing for solid foods and learning new language skills.
Read more on Pregnancy, Birth & Baby website
Your baby's growth and development - 7 months old
Your 7-month-old baby is growing fast and may even be sitting up on their own and eating solid foods. Learn more here about how your baby is developing when they reach 7 months.
Read more on Pregnancy, Birth & Baby website
Your baby's growth and development - 2 months old
At 2 months, your baby is growing fast and becoming more alert. They will also be making more sounds and getting better at moving their little bodies.
Read more on Pregnancy, Birth & Baby website
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now entering.
Need further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
Small to Large Get Closer Look in Third Trimester
Main Takeaways:
- In certain pregnancies, such as premature or preterm babies, the size and growth of the fetus matters.
- Obstetricians use their experience, the fundal height of the mother, and an ultrasound to determine the fetal size.
- A term pregnancy of at least 37 weeks or more has an average weight of 6 pounds 6 ounces. At 40 weeks gestation, the average weight is 7 pounds 12 ounces.
One of the rituals of pregnancy is estimating the size of the baby. Everyone has an opinion. Does fetal size matter? The answer is that in some situations size or, perhaps more accurately, growth does matter.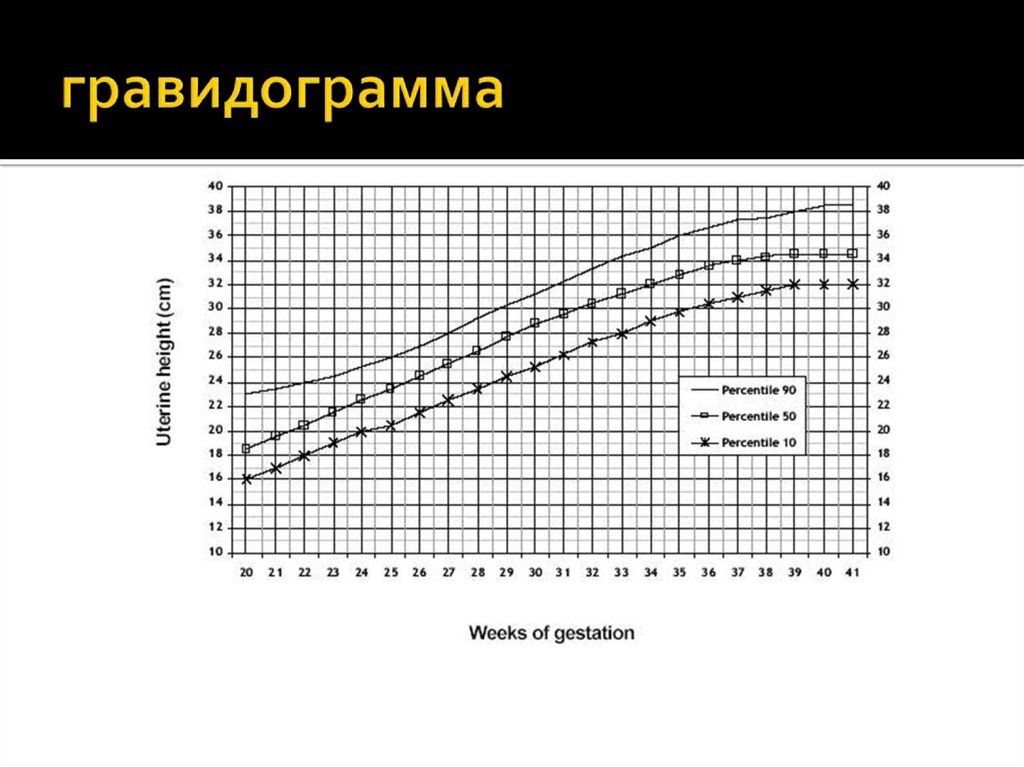 This article will review why size and fetal growth in a full-term pregnancy are important. The topic of small babies born preterm or prematurely will be addressed in other articles on this website.
This article will review why size and fetal growth in a full-term pregnancy are important. The topic of small babies born preterm or prematurely will be addressed in other articles on this website.
The accurate estimation of fetal size is actually quite difficult.
An obstetrician has three tools he/she can use:
1. Experience
Some obstetricians deliver up to 600 babies a year and with each delivery, they are estimating the size of the baby and comparing their estimates with the actual birth weight. The experience gained with so many deliveries usually results in an obstetrician’s estimate being quite accurate.
2. Fundal Height
With each prenatal visit in the third trimester, the doctor or nurse will measure the mother’s fundus, from her pubic bone to the top of her abdomen. This measurement, in centimeters, is referred to as the fundal height.
The general rule of thumb is that the number of centimeters of fundal height should equal the gestational age of the baby. Therefore, for a pregnancy at 34 weeks gestation, a fundal measurement of 32 cm would suggest a small baby as opposed to a fundal measurement of 36 cm which would suggest a larger baby.
Therefore, for a pregnancy at 34 weeks gestation, a fundal measurement of 32 cm would suggest a small baby as opposed to a fundal measurement of 36 cm which would suggest a larger baby.
3. Obstetrical Ultrasound
On occasion, a healthcare professional may order an obstetrical ultrasound in the third trimester. The ultrasound technician will measure the size of the baby’s head circumference, abdominal circumference, femur length, and the diameter of the fetal skull. Those measurements can then be used to calculate a rough estimate of the size of the baby.
Why Does Fetal Size Matter?A term pregnancy refers to a birth of at least 37 weeks or more. The average weight of a baby born at 37 weeks is 2,900 grams (6 pounds 6 ounces). Three weeks later, at 40 weeks gestation, the average weight is 3,550 grams (7 pounds 12 ounces).
For the vast majority of babies, whether they weigh above or below average has no effect on their health and well-being.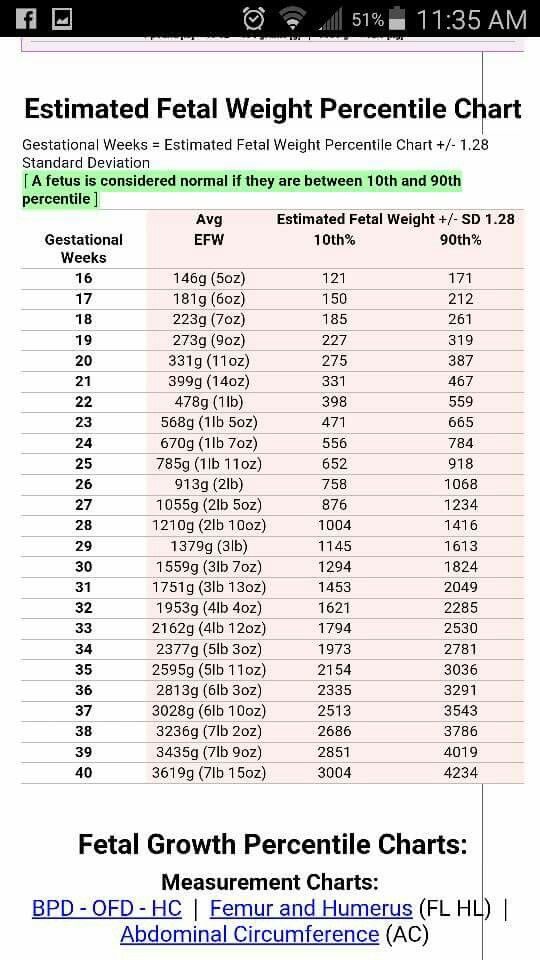 In some fetal size cases, however, a fetus that is small or very big can give rise to some concerns.
In some fetal size cases, however, a fetus that is small or very big can give rise to some concerns.
Small Babies
A baby that weighs less than the 10th percentile for that gestational age is called a “small for gestational age” baby. The 10th percentile for a baby born at 40 weeks gestation is 2,900 grams (6 pounds 6 ounces).
Small for gestational age babies can be diagnosed prior to birth based initially upon fundal measurements and the obstetrician’s experience and then confirmed through ultrasound examinations, sometimes repeated every 2 – 3 weeks during the pregnancy. The fact that a fetus is small for gestational age may mean that the fetus is developing appropriately and is simply going to be a small baby.
Intrauterine Growth Restriction (IUGR)
One area of concern is when the baby is not growing at the expected rate. This is a condition referred to as intrauterine growth restriction. Intrauterine growth restriction, or IUGR, is caused by the fetus not receiving the appropriate nutrients in utero for proper growth.
This can occur during the course of the pregnancy or can first become apparent in the third trimester. The diagnosis of IUGR is made by way of ultrasound examination (usually serial ultrasound examinations) or by Doppler flow studies. Doppler flow studies are a type of ultrasound examination that measures the blood flow in the umbilical artery.
The general rule of thumb is that a fetus diagnosed with IUGR should be delivered if the gestational age is 37 weeks or more on the theory that the fetus can receive better nutrition outside of the womb rather than inside the womb. A fetus with IUGR is less able to tolerate the stress of labor.
Studies have shown that the highest risk factor, by far, for neonatal brain injury is IUGR where the baby weighed less than the third percentile. A diagnosis of IUGR, which is known by the healthcare providers, allows them to more safely manage the labor, recognizing the reduced tolerance of the fetus.
Large Babies
A large for gestational age baby is a baby that weighs more than the 90th percentile for his or her gestational age. A baby born at 40 weeks that weighs more than 4,200 grams (9 pounds 4 ounces) is large for gestational age baby. The 97th percentile is 4,550 grams (10 pounds).
A baby born at 40 weeks that weighs more than 4,200 grams (9 pounds 4 ounces) is large for gestational age baby. The 97th percentile is 4,550 grams (10 pounds).
It is reported that the largest baby ever born was a baby weighing 22 pounds. This baby was born in Ohio in 1879.
The medical term that is sometimes used to refer to a large for gestational age baby is macrosomia. A large for gestational age baby can be diagnosed by the obstetrician’s experience, fundal measurements, and ultrasound.
The major fetal size concern that arises when a fetus is diagnosed as being large for gestational age is the possibility that the shoulder of the fetus may become stuck in the birth canal during a natural delivery. This is an obstetrical emergency called shoulder dystocia. It makes sense that the larger the fetus, the more likely the possibility that he or she will become stuck during the delivery.
There are many reasons why a baby may be large for gestational age.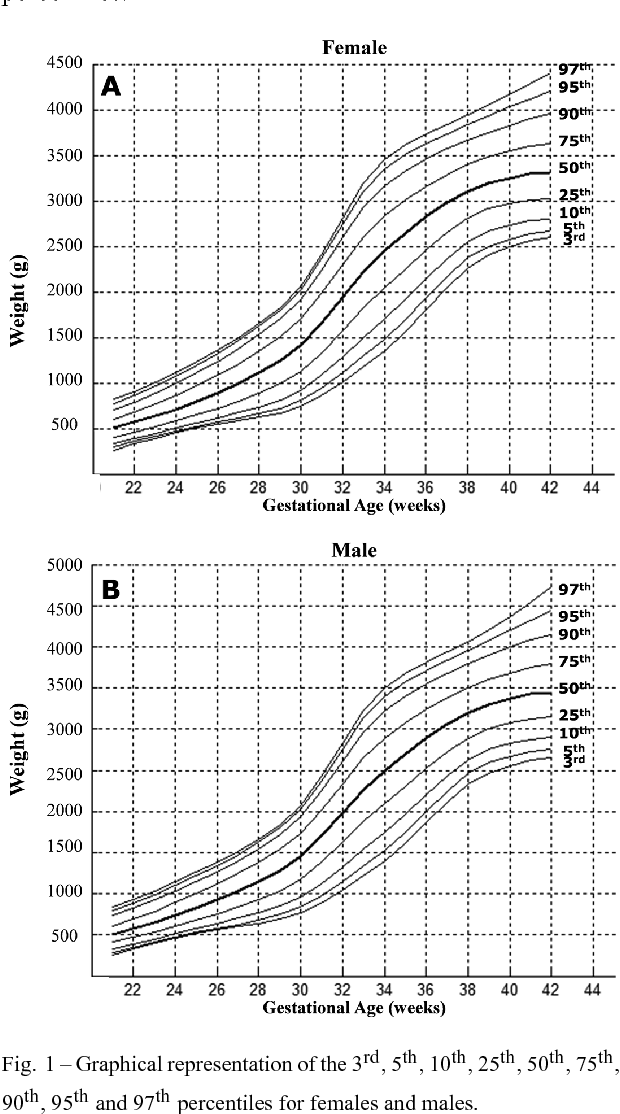 Genetics play a significant role, as do such things as the mother having diabetes before pregnancy or developing diabetes during pregnancy. Further, as pregnancies go beyond 40 weeks, the fetus continues to grow.
Genetics play a significant role, as do such things as the mother having diabetes before pregnancy or developing diabetes during pregnancy. Further, as pregnancies go beyond 40 weeks, the fetus continues to grow.
An important part of the care provided by family physicians, midwives, and obstetricians in the third trimester is to monitor fetal size and, if necessary, take steps to minimize those risks to the fetus resulting from being too small or too big.
If your child was injured during birth and you believe that the injuries were due to a medical professional’s negligence, contact us today.
Susanne Raab
Susanne Raab is a lawyer at Pacific Medical Law, and an advocate for people living with disabilities. She has been selected for inclusion by her peers in Best Lawyers in Canada in the area of Medical Negligence and is recognized as a leading practitioner in the Canadian Legal Lexpert® Directory in medical malpractice. Susanne is also a Fellow of the Litigation Counsel of America, an honorary trial lawyer society whose membership is limited to less than one-half of one percent of North American lawyers, judges and scholars.
Susanne is also a Fellow of the Litigation Counsel of America, an honorary trial lawyer society whose membership is limited to less than one-half of one percent of North American lawyers, judges and scholars.
Fetal growth retardation, the fetus is not gaining weight, what to expect? Part 2 – Family Clinic
In one of the previous articles, we discussed the topic of fetal growth retardation. We got acquainted with some competent terms, and came to the conclusion that the diagnosis is made on the basis of ultrasound parameters, when certain indicators are less than normal.
In this article, we will consider the norms for the size of the fetus, what are they?
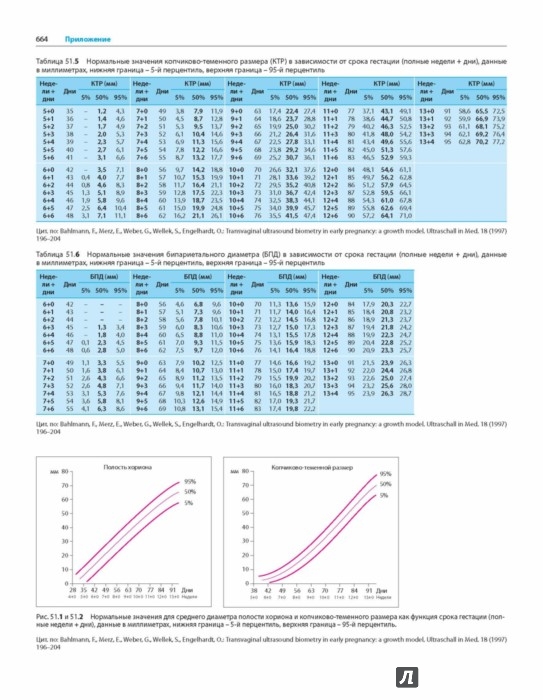
Each doctor who performs ultrasound during pregnancy has a special table (it can be in paper or electronic form) that indicates the parameters, weeks of gestation, and percentiles: namely the 10th percentile, 50th percentile and 9th percentile0th percentile. A percentile is a statistic. The number of percentiles can change, as well as the number of parameters. It is important to understand that the fetus does not grow according to a textbook, but according to its genetic program, and the tasks of an obstetrician-gynecologist with an ultrasound doctor should be understood in dynamics: is it an individual feature of the baby of such intrauterine growth or, indeed, due to placental insufficiency, he lags behind in growth. There are a number of malformations and chromosomal diseases, due to which the fetus is stunted, but then the doctor will suspect this on an ultrasound scan and send it for additional examination.
So, an example of a table of indicators of intrauterine fetal dimensions. Let's take the example of 33 weeks pregnant. This line is highlighted in red. Percentiles indicate the relative position of an individual in the standardization sample. These are some average statistical indicators that help, first of all, doctors navigate between the norm and pathology.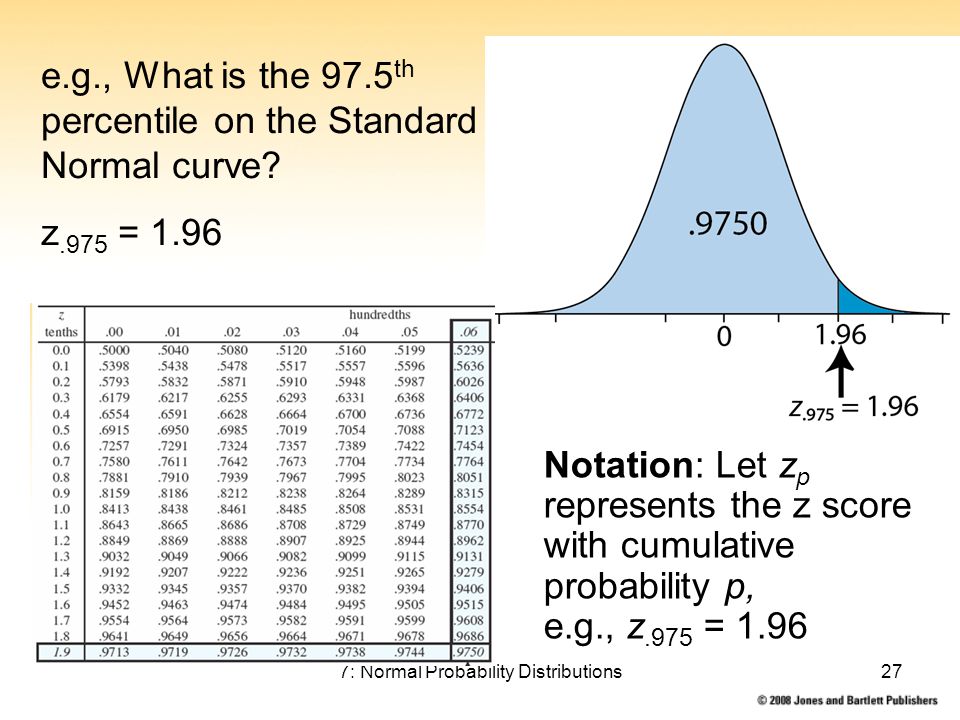 If your gestational age is 33 weeks, and all indicators of fetometry (sizes of different parts of the fetal body) fit into this line, highlighted in red, then there is no cause for alarm. "According to the textbook" is the 50th percentile (the most common indicator of the norm in the population). But the fetus can be larger or smaller. Remember how at school age you lined up in physical education classes, who is taller, who is lower, but all the good guys turned out to be. In percentiles, the same logic, someone is larger (then the doctor will say the phrase: the biparietal size corresponds to 90 percentile for 33 weeks gestation), someone smaller (then the doctor will say the phrase: the size of the femur corresponds to the 10 percentile for 33 weeks gestation). Both of these are normal, and there is no cause for alarm.
If your gestational age is 33 weeks, and all indicators of fetometry (sizes of different parts of the fetal body) fit into this line, highlighted in red, then there is no cause for alarm. "According to the textbook" is the 50th percentile (the most common indicator of the norm in the population). But the fetus can be larger or smaller. Remember how at school age you lined up in physical education classes, who is taller, who is lower, but all the good guys turned out to be. In percentiles, the same logic, someone is larger (then the doctor will say the phrase: the biparietal size corresponds to 90 percentile for 33 weeks gestation), someone smaller (then the doctor will say the phrase: the size of the femur corresponds to the 10 percentile for 33 weeks gestation). Both of these are normal, and there is no cause for alarm.
As in the previous article on fetal growth retardation, let's repeat the main fetometric indicators that guide the assessment of intrauterine growth of the fetus: biparietal size, head circumference, abdominal circumference, femur length.![]() These indicators are highlighted in the table with multi-colored columns. The estimated fetal weight is calculated using a mathematical formula based on these figures.
These indicators are highlighted in the table with multi-colored columns. The estimated fetal weight is calculated using a mathematical formula based on these figures.
In this article, we tried to get acquainted with the principles of assessing intrauterine fetal growth, we saw percentiles and their spread. If you are diagnosed with fetal growth retardation, consult this plate with your doctor to find out if this is true, ask your doctor for an ultrasound. And remember, your baby is individual, the best and most beautiful, let him also grow individually in utero, according to his genetic program.
Obstetrician-gynecologists and ultrasound doctors of the FAMILY CLINIC are ready to answer all questions about the development of the fetus and the course of pregnancy, as well as take care of your pregnancy so that you have a healthy baby.
Ultrasound imaging of intrauterine growth retardation (IUGR)
★ ★ ★ ★ ☆
//=get_the_title()?>
//=round($sum/count($reviewsRating), 2)?>
//=count($reviewsRating)?>
08/08/2019 "Articles"
Author: Vikram S Dogra
Overview
The term “intrauterine growth restriction” has largely replaced the term “intrauterine growth retardation” (IUGR). The definition of IUGR is problematic because we do not know the innate growth potential of the fetus. The most common indicator of this pathology is a fetal weight below the 10th percentile for gestational age. Ultrasound is the preferred method for assessing IUGR.
The definition of IUGR is problematic because we do not know the innate growth potential of the fetus. The most common indicator of this pathology is a fetal weight below the 10th percentile for gestational age. Ultrasound is the preferred method for assessing IUGR.
Brief description
In most cases of IUGR, transcerebellar diameter is taken into account, which can be used as an objective indicator of gestational age. The transcerebellar diameter in millimeters is equal to the gestational age from 1 to 22 weeks of pregnancy. With this definition, IUGR and "small, for gestational age, fetus" are synonymous.
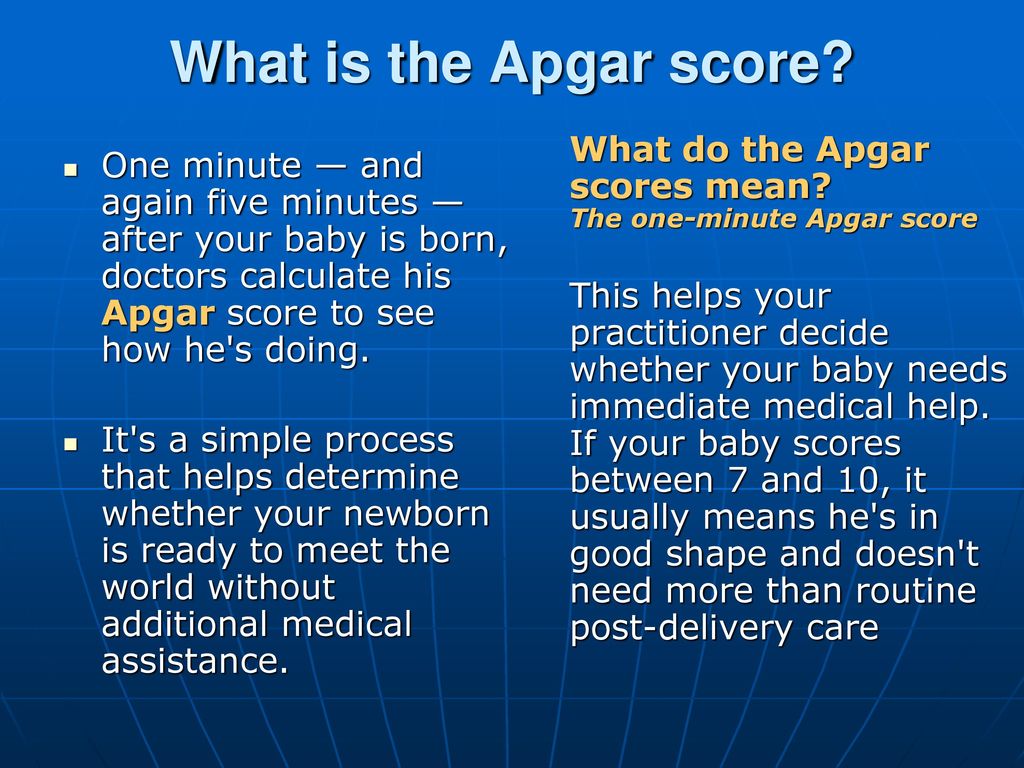
Growth restriction has a prevalence of 10% of all pregnancies. However, this figure varies between patient groups: 3-5% for healthy mothers and 25% or more for some high-risk groups, such as mothers with hypertension. Pregnancy with IUGR is often complicated by a high incidence of intrauterine and birth distress of the fetus and the need for caesarean section. Premature infants are prone to low APGAR scores, low cord pH, intraventricular hemorrhage, necrotizing enterocolitis, hypoglycemia, hypocalcemia, and polycythemia.
Premature infants are prone to low APGAR scores, low cord pH, intraventricular hemorrhage, necrotizing enterocolitis, hypoglycemia, hypocalcemia, and polycythemia.
Melchior et al found that there was a significant association between first trimester uterine artery resistance index (RI) scores and subsequent development of infants who are small for gestational age or have IUGR. However, they argue that uterine artery Doppler sensitivity is higher for small fetuses in preeclamptic mothers than for IUGR, and noted that this difference may be the result of various underlying placental abnormalities that are differently detected in the first trimester.
Skeefers et al found that oligohydramniosis (amniotic fluid index <5) and abnormal umbilical artery Doppler (absent or reversed diastolic blood flow) were of moderate predictive value for perinatal mortality. The authors assessed whether maternal demographic and ultrasound parameters predict perinatal mortality (in utero or neonatal death within the first 28 days of life) for IUGR <35 weeks gestation and birth weight <10th percentile.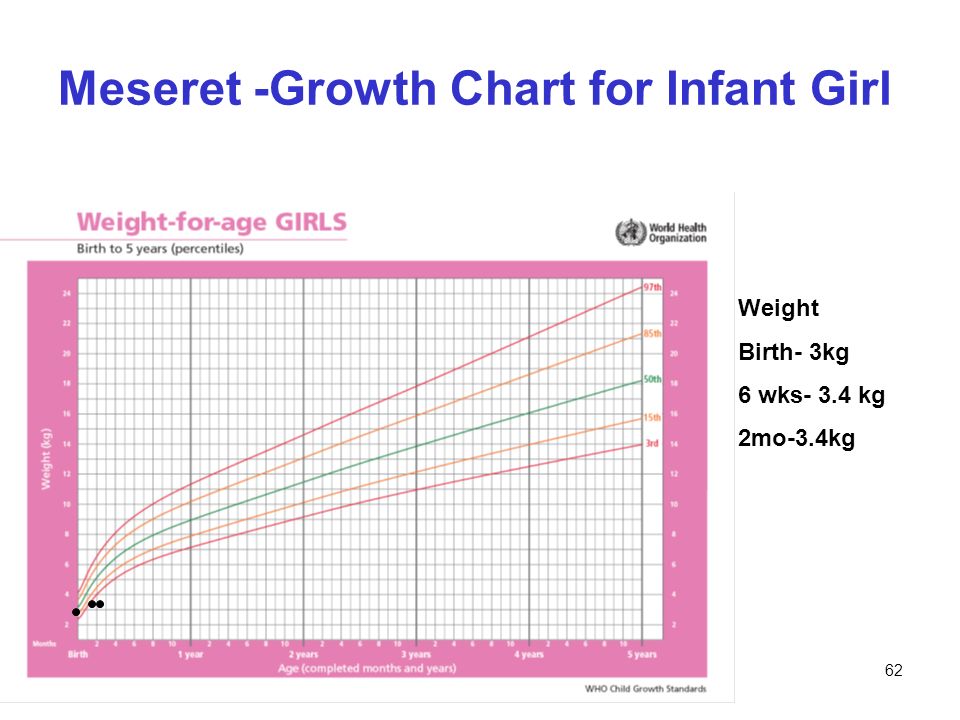 We identified 230 single pregnancies with early IUGR that met the criteria included in the study.
We identified 230 single pregnancies with early IUGR that met the criteria included in the study.
Ultrasound diagnostics
Umbilical artery Doppler can be performed anywhere along the entire length of the umbilical artery. An attempt should be made to obtain as vertical a view of the umbilical artery as possible. Blood in the main uterine arteries flows in the opposite direction to that in the iliac arteries. A typical waveform shows a deep groove in relation to aortic valve closure. The groove, which is present before pregnancy, gradually disappears during pregnancy, and diastolic flow increases as pregnancy progresses (i.e., vessel resistance decreases).
Figure 1 : Normal Doppler waveform of the fetal umbilical artery and vein.
Figure 2: Doppler waveform of the umbilical artery in intrauterine growth retardation shows loss of diastolic flow. Pulsation of the umbilical vein may also be visible. Both of these findings indicate severe IUGR.
Both of these findings indicate severe IUGR.
Fetal weight below the 10th percentile has a negative predictive value of 99%, sensitivity 89% and specificity 88% for the detection of IUGR. An elevated OH-OB ratio has a negative predictive value of 98%, a sensitivity of 82%, and a specificity of 94% for the detection of IUGR. Weight loss with decreased amniotic fluid and the presence of hypertension are predictors of IUGR.
Triplex mode is used to assess venous blood flow in the umbilical cord. This mode includes umbilical vein color Doppler, pulsed Doppler velocimetry, and real-time ultrasound to measure the diameter of the umbilical vein.
Several clinical and sonographic parameters can be used in combination to establish a diagnosis of intrauterine growth retardation with greater certainty:
- Estimated fetal weight;
- Volume of amniotic fluid;
- Maternal pressure indicator.
DO YOU CARE THE ULTRASONIC MACHINE CORRECTLY?
Download the care guide now
IUGR ultrasound criteria
Sonographic criteria for IUGR include the following:
- Increased thigh to abdominal circumference ratio;
- Increased ratio of head circumference to abdominal circumference;
- Unexplained oligohydramnios.
The measurement of body fat is the best measurement for evaluating fetal growth because hepatic damage almost always occurs when growth is shortened. Headlock charts can be used to calculate fetal weight. Most ultrasound machines also use a fetal weight calculation method.
Oligohydramnios is an indicator of IUGR. An amniotic fluid level of less than 5 cm measured in 4 quadrants is suggestive of oligohydramnia. Other causes of oligohydramnios include death in utero, renal agenesis, and premature rupture of membranes.
Figure 3 : Transabdominal ultrasound image of a pregnancy with severe oligohydramnios associated with intrauterine growth retardation. Assessing the anatomy of the fetus is difficult.
The rationale for Doppler studies in the diagnosis of IUGR is that many cases of growth restriction are associated with small vessel disease in the fetoplacental or uteroplacental circulation. Numerous Doppler criteria have been proposed for the diagnosis of IUGR. They include at least 3 of the following indices:
They include at least 3 of the following indices:
- Systolo/diastolic ratio;
- Ripple index;
- Resistance index;
- Spectral waveform of the umbilical, uterine and intrauterine carotid arteries of the fetus and the descending thoracic aorta of the fetus;
- Spectral waveform of the venous duct and inferior vena cava.
Abnormal findings include the following:
- Highest to lowest uterine artery PI ratio greater than 1.1;
- Persistence of the protodiastolic groove, unilateral or bilateral, after 23 weeks is indicative of IUGR or preeclampsia;
- MI greater than 0.55 with double-sided grooves;
- MI greater than 0.65 with one-sided groove;
- MI greater than 0.70 with or without slots;
- IR greater than 90th percentile for gestational age regardless of grooves.
A systolic-diastolic ratio greater than 3 after 30 weeks of gestation is abnormal.
Reversal of blood flow in the ductus venosus is suggestive of a severely malformed fetus and reflects fetal metabolic acidemia.