What is a caesarean
Cesarean Section | Johns Hopkins Medicine
What is a Cesarean section?
Cesarean section, C-section, or Cesarean birth is the surgical delivery of a baby through a cut (incision) made in the mother's abdomen and uterus. Health care providers use it when they believe it is safer for the mother, the baby, or both.
The incision made in the skin may be:
- Up-and-down (vertical). This incision extends from the belly button to the pubic hairline.
or
- Across from side-to-side (horizontal). This incision extends across the pubic hairline. It is used most often, because it heals well and there is less bleeding.
The type of incision used depends on the health of the mother and the fetus. The incision in the uterus may also be either vertical or horizontal.
Why might I need a C-section?
If you can't deliver vaginally, C-section allows the fetus to be delivered surgically. You may be able to plan and schedule your Cesarean. Or, you may have it done because of problems during labor.
Several conditions make a Cesarean delivery more likely. These include:
- Abnormal fetal heart rate. The fetal heart rate during labor is a good sign of how well the fetus is doing. Your provider will monitor the fetal heart rate during labor. The normal rate varies between 120 to 160 beats per minute. If the fetal heart rate shows there may be a problem, your provider will take immediate action. This may be giving the mother oxygen, increasing fluids, and changing the mother's position. If the heart rate doesn’t improve, he or she may do a Cesarean delivery.
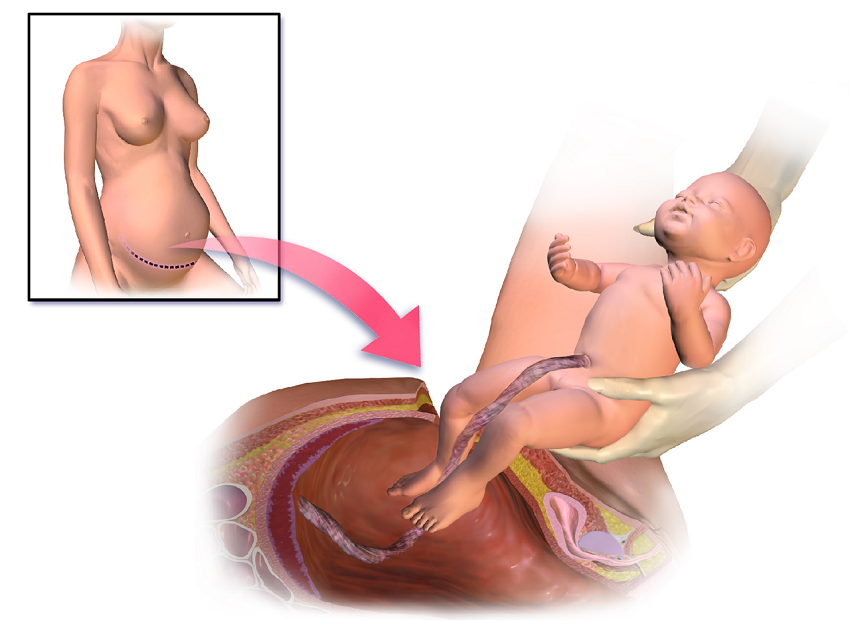
- Abnormal position of the fetus during birth. The normal position for the fetus during birth is head-down, facing the mother's back. Sometimes a fetus is not in the right position. This makes delivery more difficult through the birth canal.

- Problems with labor. Labor that fails to progress or does not progress the way it should.
- Size of the fetus. The baby is too large for your provider to deliver vaginally.
- Placenta problems. This includes placenta previa, in which the placenta blocks the cervix. (Premature detachment from the fetus is known as abruption.)
- Certain conditions in the mother, such as diabetes, high blood pressure, or HIV infection
- Active herpes sores in the mother’s vagina or cervix
- Twins or other multiples
- Previous C-section
Your healthcare provider may have other reasons to recommend a Cesarean delivery.
What are the risks of a C-section?
Some possible complications of a C-section may include:
- Reactions to the medicines used during surgery
- Bleeding
- Abnormal separation of the placenta, especially in women with previous Cesarean delivery
- Injury to the bladder or bowel
- Infection in the uterus
- Wound infection
- Trouble urinating or urinary tract infection
- Delayed return of bowel function
- Blood clots
After a C-section, a woman may not be able to have a vaginal birth in a future pregnancy.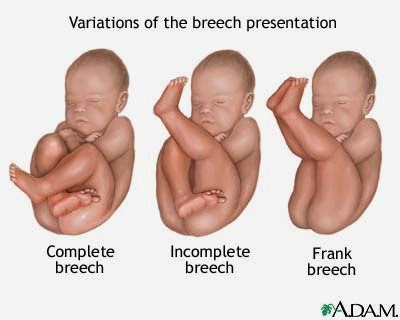 It will depend on the type of uterine incision used. Vertical scars are not strong enough to hold together during labor contractions, so a repeat C-section is necessary.
It will depend on the type of uterine incision used. Vertical scars are not strong enough to hold together during labor contractions, so a repeat C-section is necessary.
You may have other risks that are unique to you. Be sure to discuss any concerns with your healthcare provider before the procedure, if possible.
How do I get ready for a C-section?
- Your healthcare provider will explain the procedure to you and you can ask question.
- You will be asked to sign a consent form that gives your permission to do the procedure. Read the form carefully and ask questions if something is unclear.
- You will be asked when you last had anything to eat or drink. If your C-section is planned and requires general, spinal, or epidural anesthesia, you will be asked to not eat or drink anything for 8 hours before the procedure.
- Tell your healthcare provider if you are sensitive to or are allergic to any medicine, latex, iodine, tape, or anesthesia.
- Tell your healthcare provider of all medicine (prescription and over-the-counter), vitamins, herbs, and supplements that you are taking.
- Tell your healthcare provider if you have a history of bleeding disorders or if you are taking any blood-thinning medicines (anticoagulants), aspirin, or other medicines that affect blood clotting. You may be told to stop these medicines before the procedure.
- You may be given medicine to decrease the acid in your stomach. These also help dry the secretions in your mouth and breathing passages.
- Plan to have someone stay with you after a C-section. You may have pain in the first few days and will need help with the baby.
- Follow any other instructions your provider gives you to get ready.
What happens during a C-section?
A C-section will be done in an operating room or a special delivery room.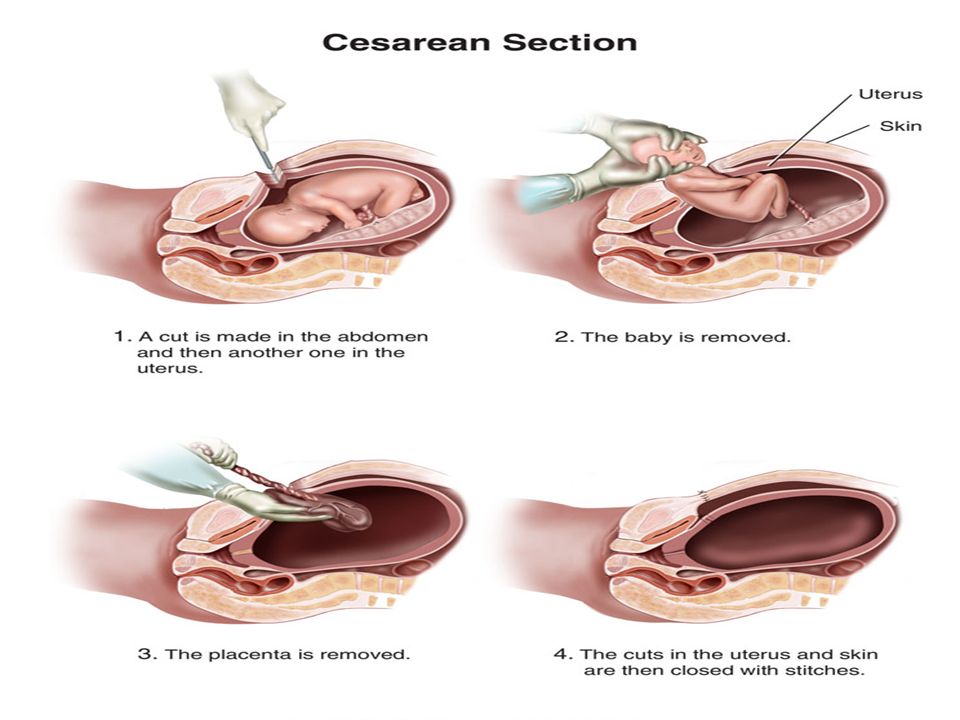 Procedures may vary depending on your condition and your healthcare provider's practices.
Procedures may vary depending on your condition and your healthcare provider's practices.
In most cases, you will be awake for a C-section. Only in rare cases will a mother need medicine that puts you into a deep sleep (general anesthesia). Most C-sections are done with a regional anesthesia such as an epidural or spinal. With these, you will have no feeling from your waist down, but you will be awake and able to hear and see your baby as soon as he or she is born.
Generally, a C-section follows this process:
- You will be asked to undress and put on a hospital gown.
- You will be positioned on an operating or exam table.
- A urinary catheter may be put in if it was not done before coming to the operating room.
- An intravenous (IV) line will be started in your arm or hand.
- For safety reasons, straps will be placed over your legs to hold you on the table.
- Hair around the surgical site may be shaved.
 The skin will be cleaned with an antiseptic solution.
The skin will be cleaned with an antiseptic solution. - Your abdomen (belly) will be draped with sterile material. A drape will also be placed above your chest to screen the surgical site.
- The anesthesiologist will continuously watch your heart rate, blood pressure, breathing, and blood oxygen level during the procedure.
- Once the anesthesia has taken effect, your provider will make an incision above the pubic bone, either transverse or vertical. You may hear the sounds of an electrocautery machine that seals off bleeding.
- Your provider will make deeper incisions through the tissues and separate the muscles until the uterine wall is reached. He or she will make a final incision in the uterus. This incision is also either horizontal or vertical.
- Your provider will open the amniotic sac, and deliver the baby through the opening. You may feel some pressure or a pulling sensation.
- He or she will cut the umbilical cord.
- You will get medicine to help the uterus contract and expel the placenta in your IV.
- Your provider will remove your placenta and examine the uterus for tears or pieces of placenta.
- He or she will use sutures to close the incision in the uterine muscle and reposition the uterus in the pelvic cavity.
- Your provider will close the muscle and tissue layers with sutures. He or she will close the skin incision with sutures or surgical staples.
- Finally, your provider will apply a sterile bandage.
What happens after a C-section?
In the hospital
In the recovery room, nurses will watch your blood pressure, breathing, pulse, bleeding, and the firmness of your uterus.
Usually, you can be with your baby while you are in the recovery area. In some cases, babies born by Cesarean will first need to be monitored in the nursery for a short time. Breastfeeding can start in the recovery area, just as with a vaginal delivery.
Breastfeeding can start in the recovery area, just as with a vaginal delivery.
After an hour or 2 in the recovery area, you will be moved to your room for the rest of your hospital stay.
As the anesthesia wears off, you may get pain medicine as needed. This can be either from the nurse or through a device connected to your intravenous (IV) line called a PCA (Patient Controlled Analgesia) pump. In some cases, pain medicine may be given through the epidural catheter until it is removed.
You may have gas pains as the intestinal tract starts working again after surgery. You will be encouraged to get out of bed. Moving around and walking helps ease gas pains. Your healthcare provider may also give you medicine for this. You may feel some uterine contractions called after-pains for a few days. The uterus continues to contract and get smaller over several weeks.
The urinary catheter is usually removed the day after surgery.
You may be given liquids to drink a few hours after surgery. You can gradually add more solid foods as you can handle them.
You can gradually add more solid foods as you can handle them.
You may be given antibiotics in your IV while in the hospital and a prescription to keep taking the antibiotics at home.
At home
You will need to wear a sanitary pad for bleeding. It is normal to have cramps and vaginal bleeding for several days after birth. You may have discharge that changes from dark red or brown to a lighter color over several weeks.
Do not douche, use tampons, or have sex until your healthcare provider tells you it’s OK. You may also have other limits on your activity, including no strenuous activity, driving, or heavy lifting.
Take a pain reliever as recommended by your healthcare provider. Aspirin or certain other pain medicines may increase bleeding. So, be sure to take only recommended medicines.
Arrange for a follow-up visit with your healthcare provider. This is usually 2 to 3 weeks after the surgery.
Call your healthcare provider right away if any of these occur:
- Heavy vaginal bleeding
- Foul-smelling drainage from your vagina
- Fever or chills
- Severe abdominal (belly) pain
- Increased pain, redness, swelling, or bleeding or other drainage from the incision
- Leg pain
- Trouble breathing, chest pain, or heart palpitations
Your healthcare provider may give you other instructions, depending on your situation.
Next steps
Before you agree to the test or the procedure make sure you know:
- The name of the test or procedure
- The reason you are having the test or procedure
- What results to expect and what they mean
- The risks and benefits of the test or procedure
- What the possible side effects or complications are
- When and where you are to have the test or procedure
- Who will do the test or procedure and what that person’s qualifications are
- What would happen if you did not have the test or procedure
- Any alternative tests or procedures to think about
- When and how will you get the results
- Who to call after the test or procedure if you have questions or problems
- How much will you have to pay for the test or procedure
C-section - Mayo Clinic
Overview
Cesarean delivery (C-section) is used to deliver a baby through surgical incisions made in the abdomen and uterus.
Planning for a C-section might be necessary if there are certain pregnancy complications. Women who have had a C-section might have another C-section. Often, however, the need for a first-time C-section isn' clear until after labor starts.
If you're pregnant, knowing what to expect during and after a C-section can help you prepare.
Products & Services
- Book: Mayo Clinic Family Health Book, 5th Edition
- Book: Mayo Clinic Guide to a Healthy Pregnancy
- Book: Obstetricks
Why it's done
Health care providers might recommend a C-section if:
- Labor isn't progressing normally. Labor that isn't progressing (labor dystocia) is one of the most common reasons for a C-section. Issues with labor progression include prolonged first stage (prolonged dilation or opening of the cervix) or prolonged second stage (prolonged time of pushing after complete cervical dilation).
- The baby is in distress.
 Concern about changes in a baby's heartbeat might make a C-section the safest option.
Concern about changes in a baby's heartbeat might make a C-section the safest option. - The baby or babies are in an unusual position. A C-section is the safest way to deliver babies whose feet or buttocks enter the birth canal first (breech) or babies whose sides or shoulders come first (transverse).
- You're carrying more than one baby. A C-section might be needed for women carrying twins, triplets or more. This is especially true if labor starts too early or the babies are not in a head-down position.
- There's a problem with the placenta. If the placenta covers the opening of the cervix (placenta previa), a C-section is recommended for delivery.
- Prolapsed umbilical cord. A C-section might be recommended if a loop of umbilical cord slips through the cervix in front of the baby.
- There's a health concern. A C-section might be recommended for women with certain health issues, such as a heart or brain condition.
- There's a blockage. A large fibroid blocking the birth canal, a pelvic fracture or a baby who has a condition that can cause the head to be unusually large (severe hydrocephalus) might be reasons for a C-section.
- You've had a previous C-section or other surgery on the uterus. Although it's often possible to have a vaginal birth after a C-section, a health care provider might recommend a repeat C-section.
Some women request C-sections with their first babies. They might want to avoid labor or the possible complications of vaginal birth. Or they might want to plan the time of delivery. However, according to the American College of Obstetricians and Gynecologists, this might not be a good option for women who plan to have several children. The more C-sections a woman has, the greater the risk of problems with future pregnancies.
Request an Appointment at Mayo Clinic
From Mayo Clinic to your inbox
Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health.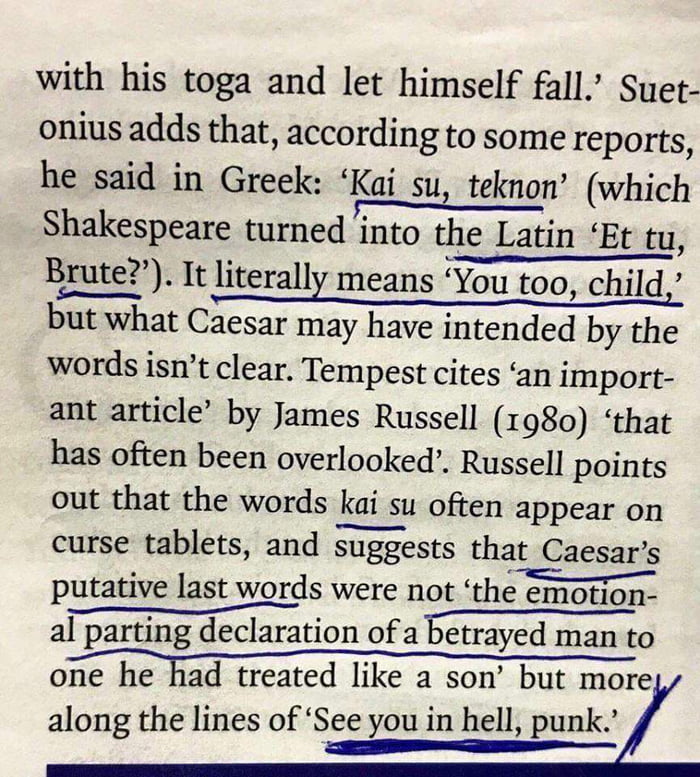
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
Risks
Like other types of major surgery, C-sections carry risks.
Risks to babies include:
- Breathing problems.
 Babies born by scheduled C-section are more likely to develop a breathing issue that causes them to breathe too fast for a few days after birth (transient tachypnea).
Babies born by scheduled C-section are more likely to develop a breathing issue that causes them to breathe too fast for a few days after birth (transient tachypnea). - Surgical injury. Although rare, accidental nicks to the baby's skin can occur during surgery.
Risks to mothers include:
- Infection. After a C-section, there might be a risk of developing an infection of the lining of the uterus (endometritis), in the urinary tract or at the site of the incision.
- Blood loss. A C-section might cause heavy bleeding during and after delivery.
- Reactions to anesthesia. Reactions to any type of anesthesia are possible.
- Blood clots. A C-section might increase the risk of developing a blood clot inside a deep vein, especially in the legs or pelvis (deep vein thrombosis). If a blood clot travels to the lungs and blocks blood flow (pulmonary embolism), the damage can be life-threatening.
- Surgical injury. Although rare, surgical injuries to the bladder or bowel can occur during a C-section.
-
Increased risks during future pregnancies. Having a C-section increases the risk of complications in a later pregnancy and in other surgeries. The more C-sections, the higher the risks of placenta previa and a condition in which the placenta becomes attached to the wall of the uterus (placenta accreta).
A C-section also increases the risk of the uterus tearing along the scar line (uterine rupture) for women who attempt a vaginal delivery in a later pregnancy.
How you prepare
For a planned C-section, a health care provider might suggest talking with an anesthesiologist if there are medical conditions that might increase the risk of anesthesia complications.
A health care provider might also recommend certain blood tests before a C-section. These tests provide information about blood type and the level of the main component of red blood cells (hemoglobin). The test results can be helpful in case you need a blood transfusion during the C-section.
The test results can be helpful in case you need a blood transfusion during the C-section.
Even for a planned vaginal birth, it's important to prepare for the unexpected. Discuss the possibility of a C-section with your health care provider well before your due date.
If you don't plan to have more children, you might talk to your health care provider about long-acting reversible birth control or permanent birth control. A permanent birth control procedure might be performed at the time of the C-section.
What you can expect
Before the procedure
Abdominal incisions used during C-sections
Abdominal incisions used during C-sections
A C-section includes an abdominal incision and a uterine incision. The abdominal incision is made first. It's either a vertical incision between your navel and pubic hair (left) or, more commonly, a horizontal incision lower on your abdomen (right).
Uterine incisions used during C-sections
Uterine incisions used during C-sections
A C-section includes an abdominal incision and a uterine incision. After the abdominal incision, the health care provider will make an incision in the uterus. Low transverse incisions are the most common (top left).
After the abdominal incision, the health care provider will make an incision in the uterus. Low transverse incisions are the most common (top left).
A C-section can be done in various ways. But most C-sections involve these steps:
- At home. Your health care provider might ask you to shower at home with an antiseptic soap the night before and the morning of your C-section. Don't shave your pubic hair within 24 hours of your C-section. This can increase the risk of a surgical site infection. If your pubic hair needs to be removed, it will be trimmed by the surgical staff just before surgery.
- At the hospital. Your abdomen will be cleansed. A thin tube (catheter) will likely be placed into your bladder to collect urine. An intravenous line will be placed in a vein in your hand or arm to provide fluid and drugs, including antibiotics to prevent infection.
-
Anesthesia. Most C-sections are done under regional anesthesia, which numbs only the lower part of your body.
 This allows you to be awake during the procedure. Common choices include a spinal block and an epidural block.
This allows you to be awake during the procedure. Common choices include a spinal block and an epidural block.Some C-sections might require general anesthesia. With general anesthesia, you won't be awake during the birth.
During the procedure
A doctor makes surgical incisions in the abdomen and the uterus to deliver the baby.
- Abdominal incision. The doctor makes an incision in the abdominal wall. It's usually done horizontally near the pubic hairline. Or the doctor might make a vertical incision from just below the navel to just above the pubic bone.
- Uterine incision. The uterine incision is then made — usually horizontally across the lower part of the uterus (low transverse incision). Other types of uterine incisions might be used depending on the baby's position within the uterus and whether there are complications, such as placenta previa or preterm delivery.
- Delivery.
 The baby will be delivered through the incisions. The doctor clears the baby's mouth and nose of fluids, then clamps and cuts the umbilical cord. The placenta is then removed from the uterus, and the incisions are closed with sutures.
The baby will be delivered through the incisions. The doctor clears the baby's mouth and nose of fluids, then clamps and cuts the umbilical cord. The placenta is then removed from the uterus, and the incisions are closed with sutures.
If you have regional anesthesia, you're likely to be able to hold the baby shortly after delivery.
After the procedure
A C-section usually requires a hospital stay for 2 to 3 days. Your health care provider will discuss pain relief options with you.
Once the anesthesia begins to wear off, you'll be encouraged to drink fluids and walk. This helps prevent constipation and deep vein thrombosis. Your health care team will monitor your incision for signs of infection. The bladder catheter will likely be removed as soon as possible.
You can start breastfeeding as soon as you're ready, even in the delivery room. Ask your nurse or a lactation consultant to teach you how to position yourself and support your baby so that you're comfortable. Your health care team will select medications for your post-surgical pain with breastfeeding in mind.
Your health care team will select medications for your post-surgical pain with breastfeeding in mind.
When you go home
During the C-section recovery process, discomfort and fatigue are common. To promote healing:
- Take it easy. Rest when possible. Try to keep everything that you and your baby need within reach. For the first few weeks, don't lift more than 25 pounds.
- Use recommended pain relief. To soothe incision soreness, your health care provider might recommend a heating pad and pain medications that are safe for breastfeeding women and their babies. These include ibuprofen (Advil, Motrin IB, others) and acetaminophen (Tylenol, others).
- Wait to have sex. To prevent infection, wait at least six weeks to have sex and don't put anything in your vagina after your C-section.
- Wait to drive. If you're taking narcotics for pain relief, it might take 1 to 2 weeks before you can comfortably apply brakes and twist to check blind spots.

Check your C-section incision for signs of infection. Pay attention to any symptoms. Contact your health care provider if:
- Your incision is red, swollen or leaking discharge
- You have a fever
- You have heavy bleeding
- You have worsening pain
If you have severe mood swings, loss of appetite, overwhelming fatigue and lack of joy in life shortly after childbirth, you might have postpartum depression. Contact your health care provider if you think you might be depressed, especially if your symptoms don't go away, you have trouble caring for your baby or completing daily tasks, or you have thoughts of harming yourself or your baby.
The American College of Obstetricians and Gynecologists recommends that postpartum care be ongoing. Have contact with your health care provider within three weeks after delivery. Within 12 weeks after delivery, see your health care provider for a postpartum evaluation.
During this appointment your health care provider likely will check your mood and emotional well-being, discuss contraception and birth spacing, review information about infant care and feeding, talk about your sleep habits and issues related to fatigue and do a physical exam, including a pap smear if it's due.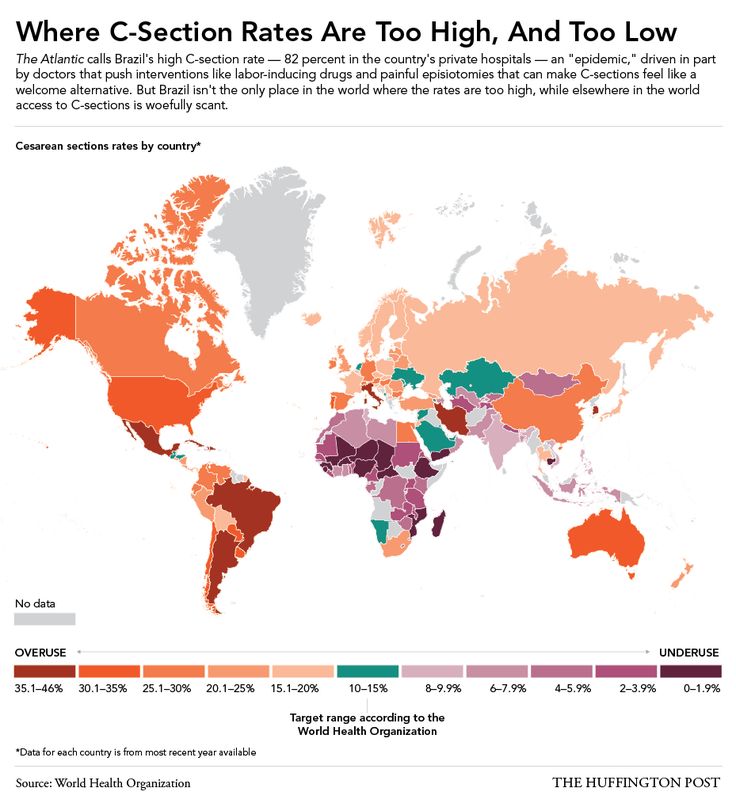 This might include a check of your abdomen, vagina, cervix and uterus to make sure you're healing well.
This might include a check of your abdomen, vagina, cervix and uterus to make sure you're healing well.
Clinical trials
Explore Mayo Clinic studies of tests and procedures to help prevent, detect, treat or manage conditions.
By Mayo Clinic Staff
Related
Products & Services
indications, how they do it, for how long they do it, and how it differs from emergency
In 2016, I had an emergency caesarean section.
Veronika Vysotina
went through a caesarean section
All five days before the discharge, doctors called me and other women who needed an operation “cesareans”, and our babies were called “cesareans”.
I was not at all ready for the operation: the pregnancy was going great. For almost half a year after the cesarean, I struggled with various thoughts, went through the stages of "I'm not a real mother" and "I'm ashamed in front of the child", I envied my friends who gave birth themselves.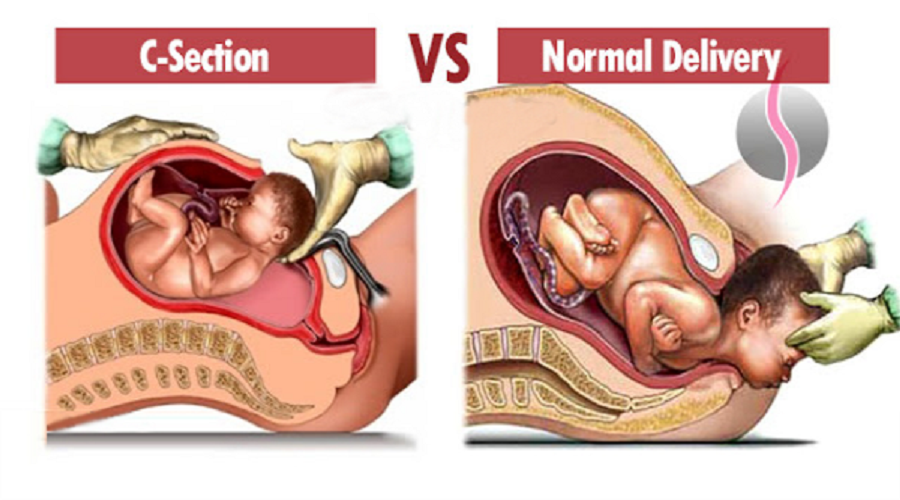 Fortunately, now all this is behind us. nine0003
Fortunately, now all this is behind us. nine0003
In the article I will tell you what a caesarean section is, how it is done and how the recovery goes.
What is a caesarean section
What is it. Caesarean section is also childbirth, only operational. And efficiency here is not about time, but about surgical intervention. Unlike natural childbirth, when a woman gives birth to a child herself through attempts, during a cesarean, the doctor makes an incision in the abdomen with a scalpel and takes the child out of the uterus through it.
Caesarean section - Medscape
Initially, a caesarean section was performed to save the baby if the mother died in childbirth. This operation is mentioned even in Greek and Roman myths - even the name itself came, according to one version, from the Roman law, according to which a pregnant woman could be buried only after the child was taken out of her stomach.
Caesarean section - Britannica
In the 17th century, caesarean sections were performed on living women, but almost always the patient died due to blood loss or infection. mid 19For centuries, doctors came up with the idea of removing the uterus, and a little later they began to put stitches on it, leaving a chance for the next pregnancy.
mid 19For centuries, doctors came up with the idea of removing the uterus, and a little later they began to put stitches on it, leaving a chance for the next pregnancy.
Methodical letter of the Ministry of Health of the Russian Federation on the classification of caesarean sectionPDF, 2.98 MB
Nowadays, caesarean section has become a fairly common situation: in Russia, about every third birth ends like this.
This is a medieval engraving depicting a caesarean section. It is believed that almost the birth of Gaius Julius Caesar is depicted here. But this is a historical myth: Caesar's mother survived after giving birth. Source: The History Blog Which is better: caesarean or natural childbirth. The term "natural birth" is a little outdated: childbirth cannot be unnatural. A caesarean section is carried out according to indications from the mother or fetus - often otherwise the woman cannot give birth or there is a risk to the health and even the life of the child.
It cannot be said that some way to give birth is definitely better: doctors recommend the method of delivery that will be the safest in a particular situation.
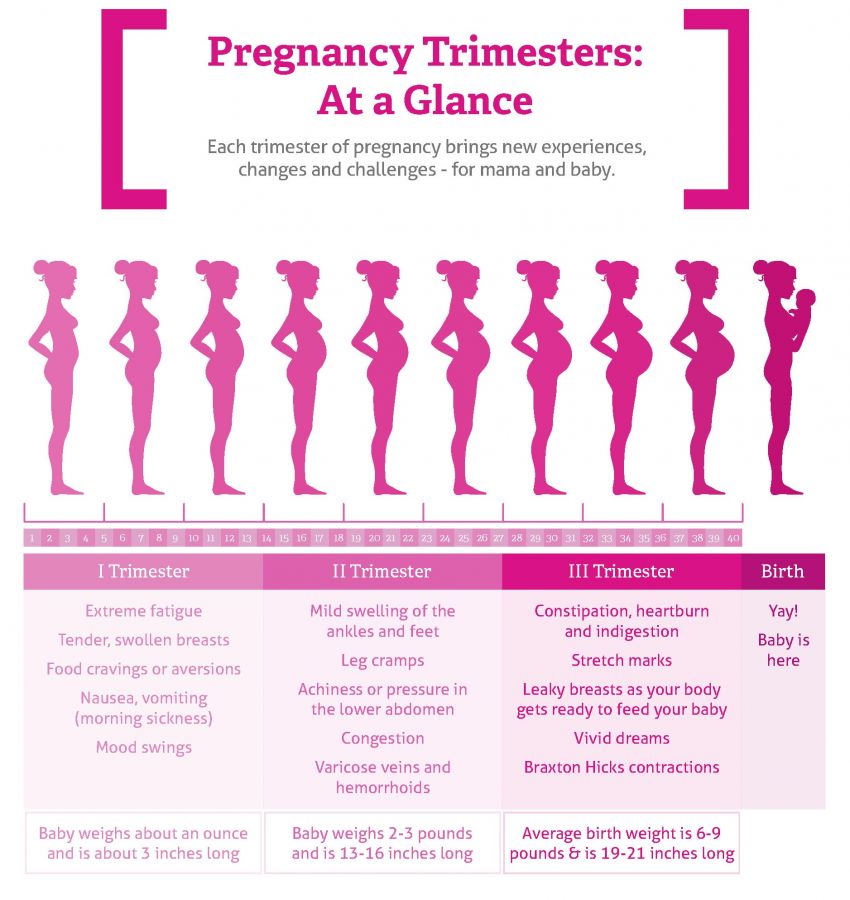
What week is the caesarean section. nine0018 If a caesarean section was planned in advance, then it is usually done starting from the 39th week of pregnancy.
Types of cesarean section
Elective. It is so called because the woman and the doctor know about it in advance, while agreeing on a specific date for the operation.
Caesarean section - NHS
Emergency. This is when the need for operative delivery arises unexpectedly, usually already in the process of childbirth. For example, when a woman suddenly stops labor and this creates a danger to the child, or heavy bleeding begins. nine0003
In addition, there are several types of operations in obstetrics, but in general they can be divided into two large types.
Transverse or horizontal.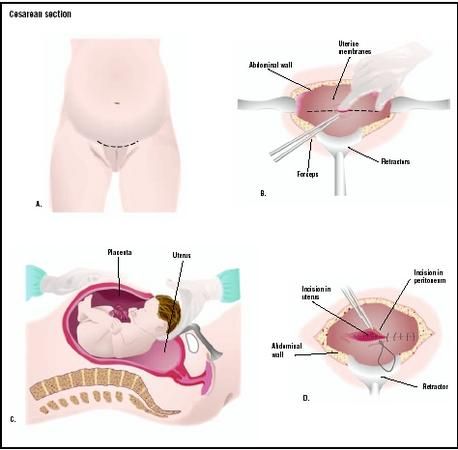 In this case, the incision is made horizontally across the lower abdomen. Doctors prefer this method if the caesarean section is planned and the patient's life is not in danger. Such an incision takes a little longer, but it is less dangerous in terms of infections. The scar from the horizontal incision is subsequently less noticeable. nine0003
In this case, the incision is made horizontally across the lower abdomen. Doctors prefer this method if the caesarean section is planned and the patient's life is not in danger. Such an incision takes a little longer, but it is less dangerous in terms of infections. The scar from the horizontal incision is subsequently less noticeable. nine0003
Longitudinal or vertical. In this case, a large vertical incision is made almost from the navel to the pelvic bone. This allows you to quickly remove the child in an emergency.
A horizontal incision for caesarean section is better at least cosmetically: it can be hidden under underwearWho is having a caesarean section
A caesarean section can be elective or emergency. Planned is so called because the woman and the doctor know about it in advance, while agreeing on a specific date. nine0003
Clinical guidelines for caesarean section in Russia
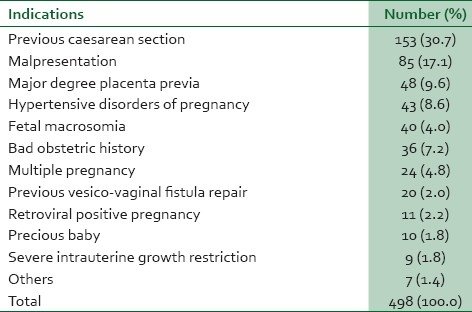
There are many reasons for surgery. Here is some of them.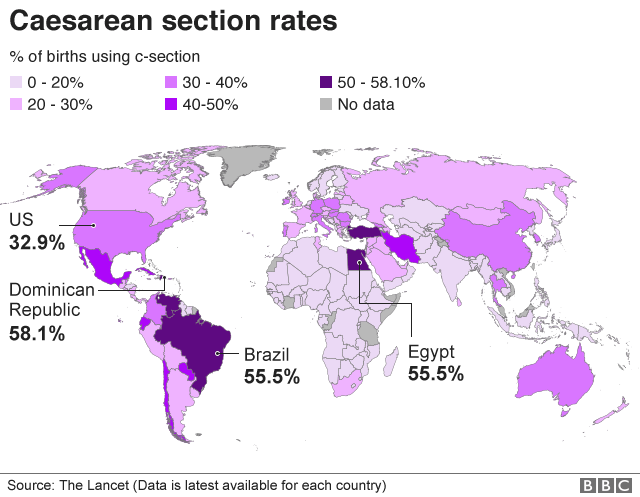
Breech presentation of the child. This is a situation where the fetus in the mother's abdomen lies with its legs or buttocks down and cannot roll over in any way. The Russian clinical guidelines state that breech presentation of a fetus weighing more than 3600 g is a direct indication for caesarean section.
Of course, natural childbirth in such cases is possible, but the risks for mother and child are too great, so doctors prefer to do caesarean. There are other incorrect positions of the fetus, which serve as indications for surgery. nine0003
Mother's health problems. These include, for example, cardiovascular disease or spinal problems. In such situations, the period of attempts can become deadly for a woman. Also, an indication for caesarean section may be fibroids, a neoplasm on the cervix or its deformation after plastic surgery - for example, after suturing severe tears during previous births.
Anatomically narrow pelvis. This is a situation where the size of the pelvic bones in a woman is smaller than necessary for a normal birth. In ordinary life, this does not cause inconvenience, but in childbirth it can become a serious problem: the baby's head will not go through a strong narrowing. That is why, already when registering pregnant women, gynecologists must measure the external dimensions of the pelvis and calculate the internal ones using a special formula. nine0003
This is a situation where the size of the pelvic bones in a woman is smaller than necessary for a normal birth. In ordinary life, this does not cause inconvenience, but in childbirth it can become a serious problem: the baby's head will not go through a strong narrowing. That is why, already when registering pregnant women, gynecologists must measure the external dimensions of the pelvis and calculate the internal ones using a special formula. nine0003
This also includes other situations that are called “fetal-pelvic disproportions” in the clinical guidelines: for example, deformity of the pelvic bones or a mismatch between the size of the pelvis of the mother and fetus.
/life/kontrakt-beremennost/
How much does pregnancy management cost?
Placenta previa. In some women, the placenta is located in the lower part of the uterus and covers the internal os - in other words, blocks the "exit" for the child.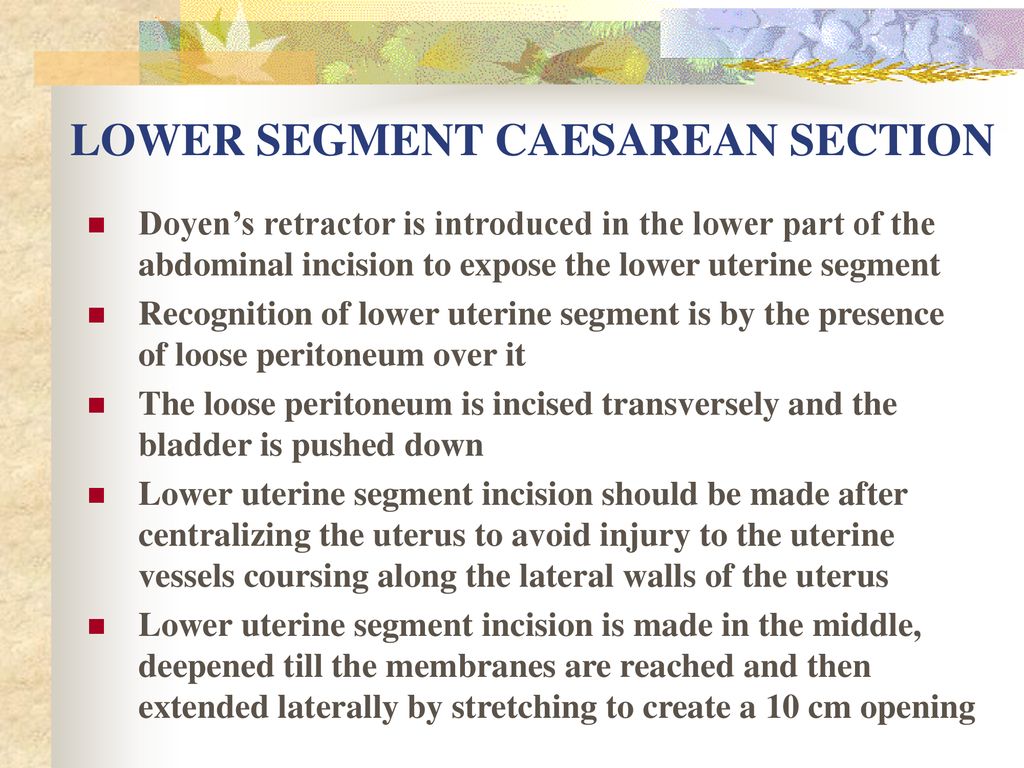 nine0003
nine0003
Previous cesarean. In general, there are quite a lot of situations when, after a caesarean section, a woman gives birth to a child in a natural way. However, this may not always be the case.
With regard to emergency caesarean section, everything that threatens the life of a woman and a child serves as a reason. These are, for example, placental abruption, car and other accidents, lack of oxygen in a child, stopping labor after it begins.
My experience. I had an emergency caesarean at 41 weeks pregnant, at that time I had already been a week and a half past the planned date of delivery. The reason for the operation was a clinically narrow pelvis: its dimensions were normal, but the child still could not pass. As the doctor later explained, my son decided to rest his forehead against the bones of the pelvis, while usually children are born with the back of the head forward, while pressing the chin to the chest. nine0003
My friend had an emergency c-section at 37 weeks due to eclampsia, a serious complication that often presents with swelling and very high blood pressure, threatening two lives at once. The reasons for this condition are still poorly understood - in Germany, where my friend lives, eclampsia is even called "pregnancy poisoning".
The reasons for this condition are still poorly understood - in Germany, where my friend lives, eclampsia is even called "pregnancy poisoning".
/german-birth/
How much does it cost to give birth in Germany
Can a woman have a caesarean at her request?
Oksana Bogdashevskaya
gynecologist of the Fomina Clinic network
In some countries, for example in the USA, operative delivery can be performed without taking into account medical indications - simply at the request of the woman. The local association of obstetricians and gynecologists asks that decisions be made carefully, but such births account for about 2.5% of all cases of caesarean sections.
As with any operation, risks and complications must be considered. A caesarean section requires a longer hospital stay and has its own risks associated with pain relief, bleeding, thrombosis, bowel or bladder injury. A scar on the uterus complicates the course of the next pregnancy, creating a threat of uterine rupture during pregnancy and childbirth. nine0003
nine0003
Although vaginal delivery after a previous cesarean is possible, in practice there is a “domino effect”: a cesarean gives rise to a cesarean, and two cesareans lead to a third cesarean. Each time, the risks increase more and more, so "caesarean at will" is not the best option for women who want to have many children.
In Russia, you can't officially have a cesarean just because you want to. The list of indications for it is strictly defined by federal clinical guidelines. nine0003
How to prepare for surgery
Caesarean section, like any other abdominal surgery, is performed on an empty stomach. With a planned caesarean, at least eight hours must pass after eating and two hours after drinking water. In Russia, they still often give an enema to cleanse the intestines, although I found a study that this is not necessary before a planned caesarean.
On the eve of the operation, a general blood test is performed, its group, Rh factor and coagulation are assessed. It is imperative to get tested for HIV, syphilis, and hepatitis B. Also the day before, an anesthesiologist comes to the woman's room. He asks the patient in detail about injuries, illnesses, allergies to drugs and more. This information is needed by a specialist in order to choose the safest type of anesthesia. nine0003
It is imperative to get tested for HIV, syphilis, and hepatitis B. Also the day before, an anesthesiologist comes to the woman's room. He asks the patient in detail about injuries, illnesses, allergies to drugs and more. This information is needed by a specialist in order to choose the safest type of anesthesia. nine0003
/analyz/
You have the right to free analyzes under compulsory health insurance
After the conversation, the doctor signs a voluntary informed consent for medical intervention with the patient. This document does not relieve doctors of responsibility, but only confirms that the patient understood the essence of the procedures - anesthesia and the operation itself - and agrees with them.
In my emergency caesarean situation, there was no preparation at all. When my water broke at ten in the evening, the nurse took blood tests and gave me an enema. During the contractions, the doctor examined him several times and put CTG sensors. Either the problems were not visible, or they were not reported to me, but until seven in the morning I was still preparing for a natural birth. Then the head of the department came, conducted an examination, studied the CTG data and, as a result, announced: “I give the child three hours. If it doesn’t turn around as it should, we will have a Caesarean.” nine0003
Either the problems were not visible, or they were not reported to me, but until seven in the morning I was still preparing for a natural birth. Then the head of the department came, conducted an examination, studied the CTG data and, as a result, announced: “I give the child three hours. If it doesn’t turn around as it should, we will have a Caesarean.” nine0003
How to be healthy and rich
We tell you how to choose a good doctor and not pay for unnecessary tests. Twice a week - in your mail along with other articles about money. Subscribe, it's free
What anesthesia is used for caesarean section
There are two types of anesthesia for caesarean section: general and regional. The doctor is obliged to find out the presence of contraindications to both: if the patient has contraindications to the general one, they make a regional one - and vice versa.
Labor pain relief - Medscape
Anesthesia. At the same time, the patient is asleep and does not know what is happening. And the effect of regional anesthesia extends only to part of the body, that is, the woman is conscious during the operation and can immediately see the child. General anesthesia is usually used in emergencies or when the patient is unconscious. There are almost no contraindications to anesthesia, but recovery from it can be long and difficult, it is often accompanied by nausea, muscle pain and confusion. nine0003
And the effect of regional anesthesia extends only to part of the body, that is, the woman is conscious during the operation and can immediately see the child. General anesthesia is usually used in emergencies or when the patient is unconscious. There are almost no contraindications to anesthesia, but recovery from it can be long and difficult, it is often accompanied by nausea, muscle pain and confusion. nine0003
Regional anesthesia. It is divided into two subtypes - epidural and spinal. In both cases, the doctor uses a thin needle to make an injection in the area of the spine. They differ in where exactly the needle goes: into the epidural space or into the cerebrospinal fluid. Epidural anesthesia begins to work within about 20 minutes, spinal anesthetic works faster.
Regional anesthesia has more contraindications than general anesthesia: these include spinal injuries or pressure problems in the mother, oxygen starvation of the fetus. Nevertheless, it is used much more often for cesarean delivery: local anesthesia is safer for the patient and is recommended by numerous protocols around the world. For example, only in the USA at 95% of births use this option.
For example, only in the USA at 95% of births use this option.
/american-girl/
How to go to give birth in the USA
In epidural anesthesia, the doctor leaves a catheter at the injection site through which the anesthetic can be added. Spinal anesthesia is a one-time procedure, its effect cannot be extended. Sometimes doctors combine both optionsCan a woman choose the type of anesthesia herself
Alexander Ronenson
Head of the Department of Anesthesiology and Resuscitation of the Perinatal Center named after E. M. Bakunina
In short, maybe. However, if there are no contraindications, the doctor will first of all recommend spinal anesthesia to the patient - she has the lowest risks of complications.
If a patient, for some personal reasons, refuses spinal anesthesia and chooses general anesthesia, she has every right to do so in accordance with Art. 20 of the Federal Law of the Russian Federation "On the fundamentals of protecting the health of citizens" (No.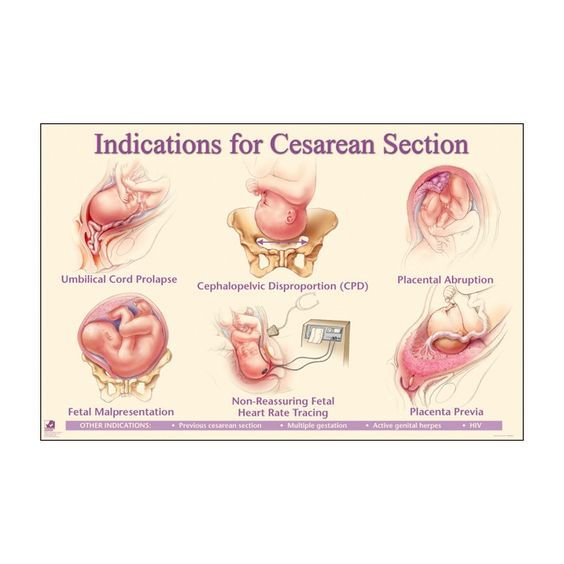 323). At the same time, a woman must understand all possible risks and complications, and is also obliged to sign an informed voluntary consent for general anesthesia and refusal of spinal anesthesia. nine0003
323). At the same time, a woman must understand all possible risks and complications, and is also obliged to sign an informed voluntary consent for general anesthesia and refusal of spinal anesthesia. nine0003
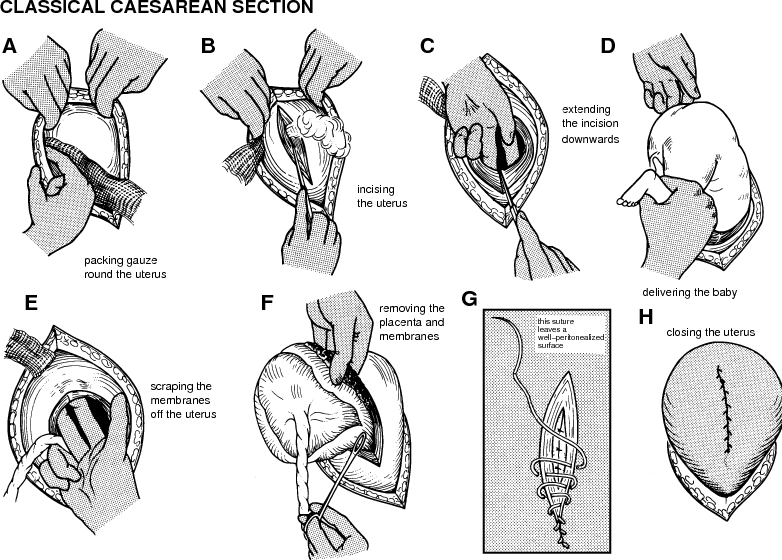
How is a cesarean performed and how long does the operation take?
The operation usually takes about 40 minutes. It involves several obstetrician-gynecologists with assistants, a team of anesthesiologists, a pediatrician or neonatologist - a doctor who assesses the condition of the newborn.
The nurse inserts a urinary catheter, a special bag with a hose that prevents fluid from accumulating in the bladder. A full bladder can interfere with surgeons during surgery, and if accidentally cut, creates a high risk of infection in the abdominal cavity. nine0003
The anesthesiologist performs anesthesia, after which the operating team can start working. The skin is treated with an antiseptic and the first external incision is made along the abdominal wall.
Then the skin and all layers of the tissues of the abdomen under it are pulled apart and an incision is made on the uterus. The child is removed, the umbilical cord is cut off and transferred to a neonatologist for examination.
The child is removed, the umbilical cord is cut off and transferred to a neonatologist for examination.
Surgeons continue their work during this time. If during natural childbirth the placenta is born on its own after a while, then during caesarean delivery it has to be removed by doctors. If even a small piece of the placenta remains inside the uterus, there is a high probability of postpartum hemorrhage and inflammation. nine0003
/platnie-rodi/
How much does it cost to give birth in Moscow
After successful removal of the baby and placenta, the uterus and all subsequent layers up to the skin are sutured in reverse order, using self-absorbable threads or special surgical glue. Sometimes the skin can be held together with metal staples or non-absorbable threads, but then they will have to be removed separately. And some studies say that the use of staples is sometimes fraught with the risk of wound complications. nine0003
/where-babies-born/
5 Moscow maternity hospitals where it is not scary to give birth to a child
Sometimes a woman is only shown a baby, sometimes she is allowed to hold or attach to her breast right in the operating room: it all depends on the internal rules of a particular maternity hospital.
Is it safe for a child to have a caesarean? For example, premature babies are removed from the uterus in the whole fetal bladder - this is a very complex and delicate procedure. nine0003
In other cases, it is important for a baby to go through birth stress: this increases his adaptive abilities. That is why it is now recommended to carry out planned operations only after the onset of labor activity - in order to allow the baby to "be born".
When passing through the birth canal of the mother, the child's body is colonized with maternal lactoflora. Research is even being carried out now: is it worth lubricating newborns born via caesarean with the mother's vaginal secretions, how adequate this imitation is. nine0003
Are children born after caesarean different from those born vaginally? There is an opinion that the heads of children who were born in different ways are different. It's not exactly like that. In newborns born naturally, at first a really characteristic shape of the head is called a birth tumor. However, these changes pass quickly, and in the future, the heads of babies do not differ.
However, these changes pass quickly, and in the future, the heads of babies do not differ.
How I had a caesarean section
I had an emergency caesarean section that was not warned about in advance. Although even so, the preparation stage turned out to be the same as during a planned operation. Blood tests, ultrasound and CTG were standard. Dinner the day before was at 5:00 pm, then around 9:00 pm I drank a cup of tea with a small cookie — by the time of the operation I had not eaten anything for 13 hours. nine0003
The anesthetist, who came to see me on the day of delivery, quickly interviewed me and said that the anesthesia would be spinal. He immediately gave me some paper to sign - apparently, consent to the operation and anesthesia. I honestly don’t remember what happened there: after ten hours of contractions, it seemed to me that I was ready to sign a donation for an apartment, if only all this would end soon.
In the operating room, I had to completely undress and climb onto the table. The anesthesiologist ordered me to lie on my side and drew something on my spine - apparently, he marked the place of the future injection. I did not feel the injection itself, there was only a slight tingling sensation. nine0003
The anesthesiologist ordered me to lie on my side and drew something on my spine - apparently, he marked the place of the future injection. I did not feel the injection itself, there was only a slight tingling sensation. nine0003
Then I was allowed to lie on my back, and my hands were fixed on special stands on the left and right. The anesthetist connected a pulse oximeter to my finger, put a blood pressure cuff on my arm, and put oxygen tubes in my nose to make it easier for me to breathe. The nurse inserted a urinary catheter into the urethra.
I was very scared, most of all I did not want to watch how the operation would go. She closed her eyes and immediately received a scolding from the anesthesiologist: "I must see your condition." At this time, the nurse put a curtain in the chest area - just so that I could not see anything. nine0003
The legs became very warm - the anesthesiologist said that the anesthesia had begun to take effect, and gave the command to the surgeons that "we are ready. " Now, when I am writing this article, I read that they can check the readiness with a piece of ice or with clamps that lightly pinch the skin.
" Now, when I am writing this article, I read that they can check the readiness with a piece of ice or with clamps that lightly pinch the skin.
During the operation, for some reason I really wanted to talk-talk-talk. It seems that I told the anesthesiologist my entire biography. The doctor at that time looked at the values of the devices and told me about the actions of the surgeons: “Now, now they will get the baby. Now scream. You have a boy!" nine0003
Now I don't remember the baby's first cry. But I clearly remembered him outwardly: they carried my son past - for some reason, his skin was blue-violet. Later, the baby was washed, shown to me and given a kiss on the forehead. They didn’t offer to put it on the chest, and then I didn’t know that it was possible at all.
In 2016 I had a transverse incision and it was sutured with absorbable sutures. This is how the suture looks four years after the operation. Usually it is hidden under underwear or a swimsuit - it does not cause any concern, I even forget about itHow was the day in the intensive care unit
Immediately after the operation, I was taken to the intensive care unit. My son was taken to the neonatal unit - I already found out a few hours later, when a neonatologist came to me and asked for consent to vaccinations.
My son was taken to the neonatal unit - I already found out a few hours later, when a neonatologist came to me and asked for consent to vaccinations.
I remember that my head was very foggy: apparently, fatigue from ten-hour contractions and the effect of anesthesia had an effect. I did not ask where my child was and where they took him. It was important for me to know only one thing: did I forget my slippers in the antenatal ward. Now it seems funny and scary at the same time. nine0003
/life/sumka-v-roddom/
How much does it cost to pack a bag for the maternity hospital? I didn't argue. Or did not have time - fell asleep.
Waking up in intensive care, I took this photo and sent it to my husband with the caption: “No stomach! I lie down and see my feet!”What can I eat after a caesarean section
When I woke up after the operation, I realized that I was terribly hungry, but the doctor did not allow me to. You could only drink low-fat chicken broth with white meat, and even then only a few sips. My husband unknowingly gave me a two-liter jar filled to the neck. The nurse then laughed: “Is this what they brought for the whole resuscitation, or what?” nine0003
My husband unknowingly gave me a two-liter jar filled to the neck. The nurse then laughed: “Is this what they brought for the whole resuscitation, or what?” nine0003
I also had to drink a lot of water, probably to make up for the loss of blood. My relatives also gave me water. The doctor advised me to buy bottles of 0.25 liters: it is difficult and uncomfortable to drink lying down from a "one and a half" bottle. The resuscitation nurse approached each patient in the ward every 40 minutes and reminded them to drink. At the end of the day, she wrote down in a notebook how much she drank and how full the urinal bag was.
Later doctors allow solid food. It is important to eat so that there is no constipation, in particular, eat vegetables and drink plenty of water. nine0003
How was the recovery
On the first day after the operation, the lights out was announced at about ten in the evening. I clearly remembered that the thought then flashed through my head: “This is my last good night for the coming year. You need to sleep." The next morning, I was already transferred to the postpartum ward. I felt great, I was ready to jump around the ward.
You need to sleep." The next morning, I was already transferred to the postpartum ward. I felt great, I was ready to jump around the ward.
I spent five days in the maternity hospital after the caesarean: I was operated on on Friday and discharged on Tuesday. Starting on Saturday, they gave injections of oxytocin, a hormone that helps the uterus contract and at the same time stimulates milk production. The injections were very painful - the buttock then hurt for another three weeks. nine0003
Back in the maternity hospital, I had a dressing done once. In the operating room, of course, they put a bandage on the wound, but after all, the caesarean was an emergency, so I didn’t have good postoperative plasters. The bandage was a gauze soaked in something pink. It was not very pleasant to remove such a seam: the fabric stuck to the seam.
I had all the sutures made with self-absorbable threads, they did not need to be removed. On the day of discharge, only an ultrasound was done to make sure everything was healing well and not bleeding. nine0003
nine0003
How to recover quickly after a caesarean section
Suture after caesarean section. As a rule, a bandage is applied to the suture after a caesarean section for 24-48 hours. After its removal, the wound is treated. If the sutures need to be removed, this is usually done on the sixth, seventh or eighth day after the operation.
C-section Recovery - NHS
How and how to treat a stitch. It is enough to gently clean and dry the wound every day, and also monitor the appearance of signs of infection - this is redness, swelling, increased soreness, a feeling of heat in the suture area, a change in the color of the discharge. The maternity hospital will give recommendations on the treatment of seams, which should be followed at home. nine0003
C-section recovery - Mayo Clinic
How long does the uterus and suture heal after cesarean. Recovery after surgery takes four to six weeks. A scar gradually forms on the skin: at first it will be bright and noticeable, but after a few months it will brighten and will not stand out so much.
How much does the uterus shrink after cesarean. Uterine contractions may be felt during the first few days after surgery. They remind menstrual cramps. nine0003
These contractions may be uncomfortable, but they help prevent excessive bleeding by constricting the blood vessels in the uterus. An over-the-counter pain reliever, such as ibuprofen, can be taken to relieve pain.
Exercise after caesarean section. After the operation, you should start moving as soon as possible, but the physical activity should be moderate. Any exercises can be done only after the permission of the doctor.
Usually they can be started three to four weeks after the caesarean if everything went without complications. It is important not to do exercises that lead to abdominal tension: abdominal exercises, squats, straight leg raises from a prone position, and others. nine0003
Massage after caesarean section. Body massage can be done after complete healing of postoperative sutures. Massage of the hands and feet is allowed, and there is evidence that it can alleviate the discomfort associated with the operation.
Massage of the hands and feet is allowed, and there is evidence that it can alleviate the discomfort associated with the operation.
Period after caesarean section. The operation does not affect the restoration of the menstrual cycle after pregnancy. When breastfeeding, menstruation will return after it stops or when the woman becomes less likely to put the baby to the breast. If a woman is not breastfeeding, then her periods will return on average two months after the birth of the baby. nine0003
Bandage is an elastic bandage that is worn over the waistband to support fabrics. It is believed that the bandage helps to relieve pain after surgery, especially during movement. There is evidence to support this, although other studies show that wearing a brace has little effect on discomfort.
How to wear a bandage after a caesarean section. The bandage must fit snugly enough to the body, but not squeeze. It needs to be fastened so that support is felt, but the bandage does not interfere with breathing and does not cause discomfort. nine0003
nine0003
Before using the bandage, you should consult your doctor. Also, it should not be worn if there are signs of infection or inflammation in the suture area.
How long to wear a bandage after a caesarean section. It should not be worn all the time without taking it off. The brace is usually worn four to eight hours a day. You can’t sleep in it, as it is uncomfortable, it can make breathing and blood circulation difficult.
Wear a brace, as a rule, from six to twelve weeks after childbirth - after this time the body will recover sufficiently. nine0003 Postpartum bandage costs an average of 1000 R. Sometimes it helps to relieve pain after surgery. Source: Yandex Market
What are the restrictions on sexual life and subsequent pregnancy
Oksana Bogdashevskaya
gynecologist of the Fomina Clinic network
The first postpartum visit to the antenatal clinic should be planned within two weeks after discharge. nine0003
Sex after cesarean. Sexual activity can be resumed four to six weeks after the operation, but it is better to see a doctor again before that and discuss contraceptive issues.
Sexual activity can be resumed four to six weeks after the operation, but it is better to see a doctor again before that and discuss contraceptive issues.
If you are planning a new pregnancy, then do not forget about the safe interval. The optimal interval between births should be about two and a half years - different protocols give slightly different numbers. However, these data are similar to recommendations for natural childbirth.
If less than six months have elapsed from delivery by caesarean to a new conception, then the next pregnancy is at risk of uterine rupture. If less than 12 months, there are high chances of placenta previa and abruption. nine0003
When can I exercise after a caesarean section
For at least four weeks after surgery, you should avoid exercises that directly affect the abs, and during the recovery period, you should not lift weights, run, do weight training. The load should only be light.
Sports activities are usually not possible until eight weeks after surgery. From that point on, it's usually safe to return to swimming, Pilates, yoga, light jogging, and low-resistance gym activities. nine0003
From that point on, it's usually safe to return to swimming, Pilates, yoga, light jogging, and low-resistance gym activities. nine0003
Aerobics, running, strength training are usually possible 12 weeks after surgery. In any case, you should consult a doctor before resuming sports.
When does milk come after caesarean and is it possible to breastfeed
After caesarean section, you can immediately breastfeed, just like after a normal birth. Sometimes breastfeeding takes longer after surgery. For example, milk production may start a little slower. nine0003
Breastfeeding after a caesarean section - Australian Breastfeeding Association
Babies born by caesarean section may not breastfeed as actively. This can be solved by trying to feed the baby more often.
Complications after caesarean
Although caesarean has become commonplace, it is wrong to think that this is just an “easy way to give birth”. This is a real abdominal operation, which is much more dangerous than natural childbirth.
It happens that after a caesarean section, a woman develops complications. One of them is endomyometritis, an inflammation of the lining of the uterus.
Women after cesarean have a high risk of leg thrombosis. This is due to the fact that anesthesia weakens and expands the vascular walls, the blood flow slows down. That is why doctors recommend wearing special compression stockings for a planned caesarean, they maintain the desired level of blood flow.
Sometimes, after a caesarean, women have problems with the onset of lactation - this is due to the fact that hormones in such a situation begin to work a little differently than during natural childbirth. Fortunately, I didn’t have such a problem: the milk came already on the third day. nine0003
Babies delivered by cesarean may have slightly different gut microflora. When a child is born naturally, he receives some of the microorganisms from the mother's birth canal. This does not happen with a caesarean, so these babies may develop colic earlier.
/colic/
How to help a newborn with colic
Even after a normal birth, a woman is not recommended to lift weights of more than five to six kilograms for the first few months - the approximate weight of a baby in winter overalls. In the postpartum period, this can lead to bleeding, and in the case of a caesarean, even to rupture of the sutures. nine0003
A month and a half after giving birth, I noticed that three red pustules appeared near the suture. Wildly frightened, I made an appointment with the first gynecologist I came across. Ultrasound of the soft tissues showed that everything was in order with the suture, and later small pieces of threads came out of the pustules, which had not yet had time to resolve. The doctor said that this sometimes happens and you should not be afraid - the seam will not open. And so it happened, everything quickly healed.
But I had enough worries. The fact is that during the operation, my son accidentally made a large cut a centimeter from his eye and another one on his head. Fortunately, they healed within a month and a half and are now completely invisible. nine0003 I'm afraid to imagine what would have happened if the cut was closer to my eye
Fortunately, they healed within a month and a half and are now completely invisible. nine0003 I'm afraid to imagine what would have happened if the cut was closer to my eye
Psychological pressure and depression after a caesarean
Somehow I came across a comparison of women who gave birth by caesarean with those who leave children in maternity hospitals. Some people stigmatize such mothers as “not a real mother” and reproach them: “I couldn’t even give birth, how are you going to educate?”
"No, it's okay: don't feel guilty about a caesarean birth" - NEN
Such words, to put it mildly, do not add self-confidence. Some women are already feeling ashamed that they allegedly "lost control" and that they "got the child already ready." nine0003
Not far from postpartum depression. Here are its main signs: depressed state, lack of interest in the child or too strong feelings for him, inability and unwillingness to enjoy life, tearfulness, impaired appetite. Postpartum depression is extremely dangerous and should not be ignored, especially if the symptoms recur regularly.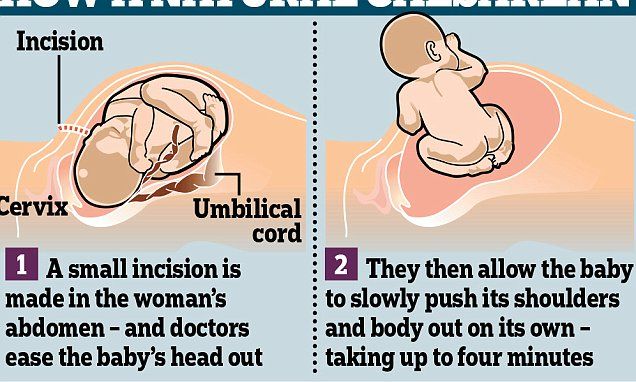
Postpartum Depression - Medscape
If you notice these signs in yourself or a woman you know who has recently given birth, it is important to see a psychologist or psychotherapist. The specialist will do tests to determine the level of depression, possibly send them for tests, and in emergency cases even offer medical treatment in a hospital setting. Alas, there are stories on the Internet about the suicide of women who have recently given birth. nine0003
/psychotherapy-search/
How to choose a psychotherapist
Fortunately, I was able to cope with my feelings on my own, even though they came to me periodically for six months. The switch was the idea that the birth went well and that it is not clear how the situation would have developed if the doctors had not performed a caesarean. My son got an Apgar score of 8/8, which is a good and high number.
Apgar score - Medscape
How to apply for sick leave after cesarean
Caesarean section is considered a complication of childbirth.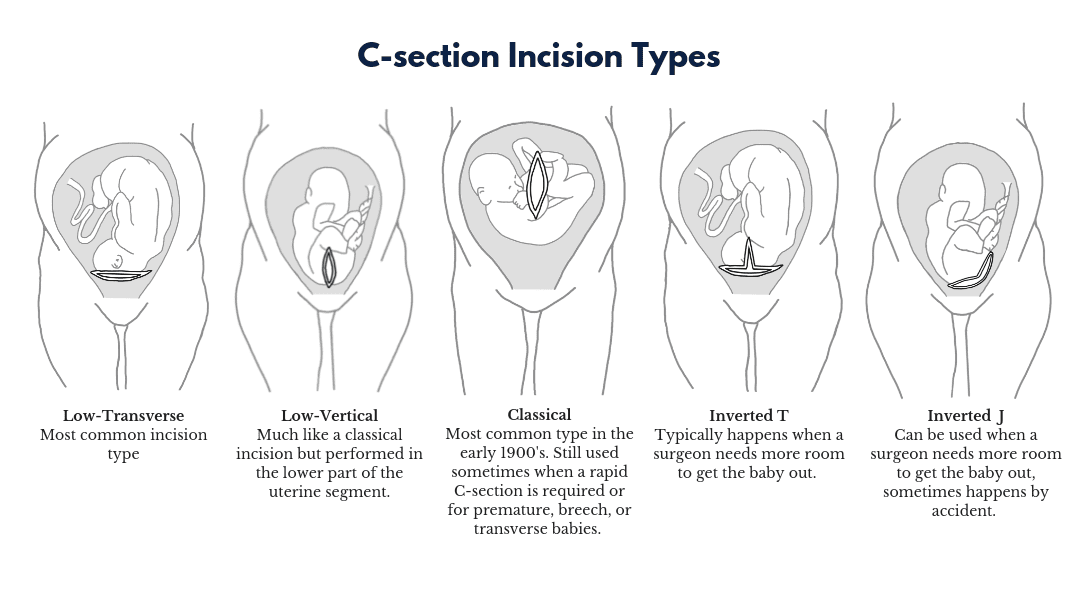 Because of it, maternity leave is extended by two weeks. At the same time, an additional code 020 is put on the sick leave.
Because of it, maternity leave is extended by two weeks. At the same time, an additional code 020 is put on the sick leave.
I was issued a sick leave at the maternity hospital before discharge. It indicated this additional code and a new deadline for starting work. On the new sick leave they wrote that it was a continuation of the previous one.
This is my first sick leave. Code 05 is simply written here - maternity leave. Theoretically, I was supposed to go to work on September 13. This sick leave was issued at the maternity hospital. They wrote the number of the first sheet in the header, put an additional code 020. Now I had to go to work on 29September The statement for the newborn also indicated about the caesarean sectionHow much does a caesarean section cost
I didn’t pay anything for a caesarean section. This operation is included in the list of those that are performed under compulsory health insurance. However, if a woman enters into a paid contract for childbirth, surgery is paid separately, such programs are more expensive.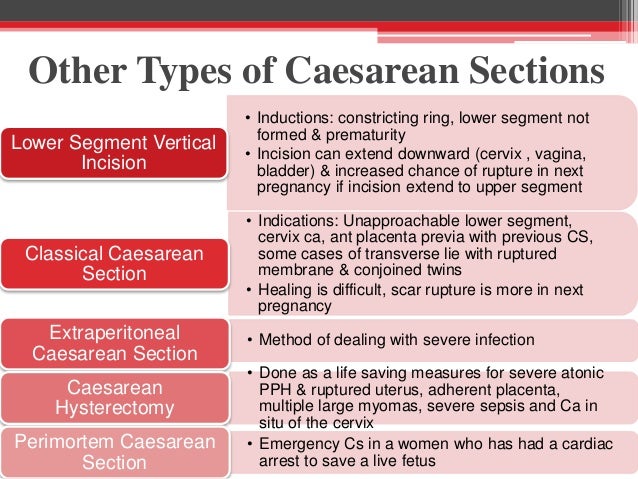 Here are some examples.
Here are some examples.
How much does a contract for operative delivery cost in different clinics
| Clinic | Contract price for operative delivery |
|---|---|
| Mother and Child | From 222 000 R |
| Maternity hospital No. 25 | 135 000 R |
| Maternity hospital No. 8 | Complicated childbirth program - 120,000 R |
| Center. V. I. Kulakova | From 85 000 R |
| Regional Clinical Perinatal Center. E. M. Bakunin | From 27 600 R |
"Mother and Child"
From 222 000 R
Maternity hospital No. 25
135,000 R
Maternity hospital No. 8
Complicated childbirth program — 120,000 R
V. I. Kulakova
From 85,000 R
Regional Clinical Perinatal Center named after V.I. E. M. Bakunina
From 27,600 R
Remember
- Caesarean section is a real operation with real incisions, numerous sutures, anesthesia and possible complications.
- Whenever possible, doctors choose local anesthesia, most often spinal anesthesia: it is safer. nine0468
- It is better to wear special compression stockings during the operation: they maintain blood flow at the desired level and prevent thrombosis.
- A woman after a caesarean section needs additional support and assistance. At least she can't lift anything heavy. It is especially important to monitor the mental state.
- A caesarean delivery extends maternity leave.
Caesarean section - Clinic 29
Modern technology Caesarean section consists in the fact that the incision of the skin and subcutaneous tissue is made along the lower fold of the abdomen in the transverse direction (according to Pfannenstiel) up to 15 cm long, or a transverse incision is made (according to Joel-Kohan) 2-3 cm below the middle of the distance between the womb and the navel 10-12 cm long. This is a convenient and fast enough operative access for caesarean section.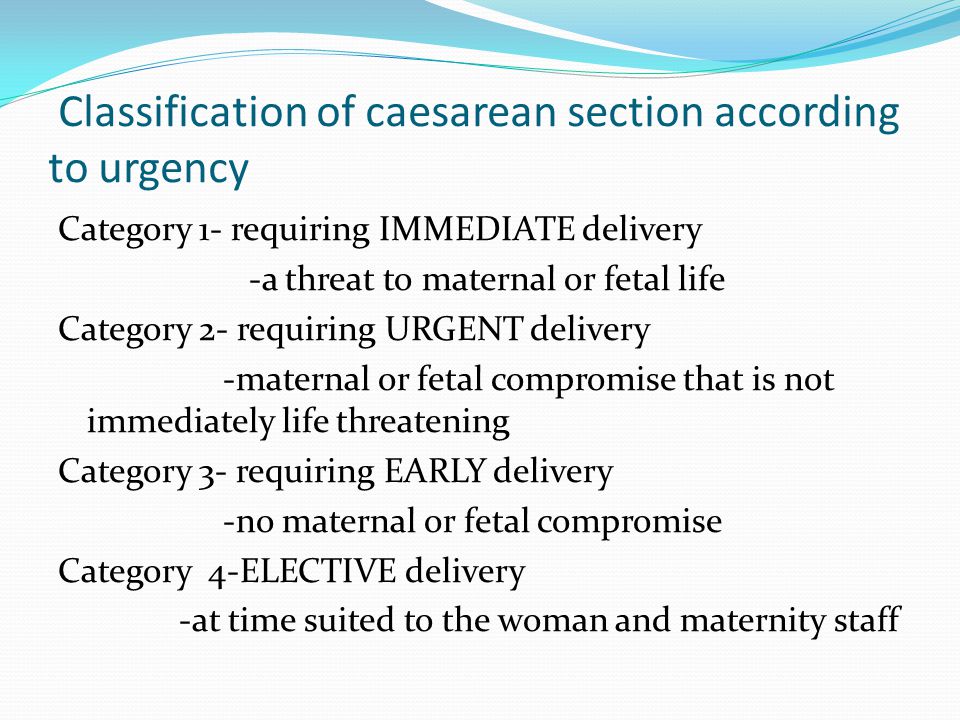 Such an incision has its advantages: it has a good cosmetic effect, which explains the widespread use of this type of intervention, because both of these incisions create favorable conditions for intradermal suture. It is noteworthy that during a repeated caesarean section, an incision on the skin is made at the site of the previous scar with excision of the latter. Such an incision of the anterior abdominal wall allows for a more active postoperative period compared to a longitudinal (lower median) incision. The puerperal woman is allowed to get out of bed during the first day after the operation, which is the prevention of subinvolution of the uterus, intestinal paresis, the formation of adhesions and reduces the risk of thrombosis in the postoperative period. nine0003
Such an incision has its advantages: it has a good cosmetic effect, which explains the widespread use of this type of intervention, because both of these incisions create favorable conditions for intradermal suture. It is noteworthy that during a repeated caesarean section, an incision on the skin is made at the site of the previous scar with excision of the latter. Such an incision of the anterior abdominal wall allows for a more active postoperative period compared to a longitudinal (lower median) incision. The puerperal woman is allowed to get out of bed during the first day after the operation, which is the prevention of subinvolution of the uterus, intestinal paresis, the formation of adhesions and reduces the risk of thrombosis in the postoperative period. nine0003
Over the past 10 years, the technique of caesarean section has progressively changed. A prerequisite for this was the work proving that the unsutured visceral and parietal peritoneum does not entail any additional postoperative complications and even significantly reduces the likelihood of adhesions in the abdominal cavity. Another prerequisite was the widespread use in surgical practice of synthetic (vicryl, polyglycolide) absorbable suture material, and therefore, when suturing an incision on the uterus, a single-row continuous suture is more often used. In patients with a single-row suture on the uterus (according to ultrasound data), edema in the area of the postoperative suture is observed 4 times less often than with a double-row suture. The suture on the uterus and aponeurosis is treated using argon plasma coagulation (APC). A feature of the APC is that the active electrode is blown with argon, ionized, and a torch is formed between the electrode and the tissue. In an environment of inert argon gas at a temperature of 120°C, tissue coagulation occurs to a depth of no more than 3 mm. In this case, there is no effect of carbonization-charring, since there is no direct combustion of the tissue, and there is also a direct thermal effect on the microbial agent. Due to APC, the healing processes are activated - as a result of deep tissue heating: myometrium in the suture area (to a depth of 10-15 mm) and reduction of collagen fibers due to tissue heat treatment.
Another prerequisite was the widespread use in surgical practice of synthetic (vicryl, polyglycolide) absorbable suture material, and therefore, when suturing an incision on the uterus, a single-row continuous suture is more often used. In patients with a single-row suture on the uterus (according to ultrasound data), edema in the area of the postoperative suture is observed 4 times less often than with a double-row suture. The suture on the uterus and aponeurosis is treated using argon plasma coagulation (APC). A feature of the APC is that the active electrode is blown with argon, ionized, and a torch is formed between the electrode and the tissue. In an environment of inert argon gas at a temperature of 120°C, tissue coagulation occurs to a depth of no more than 3 mm. In this case, there is no effect of carbonization-charring, since there is no direct combustion of the tissue, and there is also a direct thermal effect on the microbial agent. Due to APC, the healing processes are activated - as a result of deep tissue heating: myometrium in the suture area (to a depth of 10-15 mm) and reduction of collagen fibers due to tissue heat treatment. The use of APC for caesarean section can reduce blood loss during surgery, improve the quality of life in the postoperative period by reducing pain and reducing the length of stay in the hospital. Direct antibacterial action makes it possible to refuse preventive course antibiotic therapy, promotes the healing of the surgical wound, and reduces the risk of purulent-inflammatory diseases in the postoperative period. In addition, the consistency of the scar on the uterus is achieved, which allows you to increase the percentage of subsequent spontaneous births. nine0003
The use of APC for caesarean section can reduce blood loss during surgery, improve the quality of life in the postoperative period by reducing pain and reducing the length of stay in the hospital. Direct antibacterial action makes it possible to refuse preventive course antibiotic therapy, promotes the healing of the surgical wound, and reduces the risk of purulent-inflammatory diseases in the postoperative period. In addition, the consistency of the scar on the uterus is achieved, which allows you to increase the percentage of subsequent spontaneous births. nine0003
The combination of several well-known techniques and the elimination of a number of optional steps make it possible to speak of Stark caesarean section as a new modification that has a number of advantages over conventional methods. These include rapid retrieval; a significant reduction in the duration of the operation; reduction of blood loss; reducing the need for postoperative use of painkillers; reduction in the incidence of intestinal paresis and other postoperative complications; earlier discharge for 3-4 days after birth. nine0478 The duration of a traditional surgical intervention is on average 40 minutes, and in the Stark modification - 22 minutes. Due to these advantages, as well as the simplicity of the method itself, this operation is quickly gaining popularity. Babies removed after a cesarean section according to Stark have a more stable adaptation, which allows them to be breastfed during the first minutes of life.
nine0478 The duration of a traditional surgical intervention is on average 40 minutes, and in the Stark modification - 22 minutes. Due to these advantages, as well as the simplicity of the method itself, this operation is quickly gaining popularity. Babies removed after a cesarean section according to Stark have a more stable adaptation, which allows them to be breastfed during the first minutes of life.
Our Maternity Hospital uses a new technique of "slow" caesarean section. A unique, gentle way of delivery "slow" caesarean section at 29maternity hospital! The method of "natural" or "slow" caesarean section, for patients with a contraindication for natural childbirth, was developed by English specialists in elite clinics in London. Its essence is as follows: the woman in labor is conscious, as in a conventional cesarean, the doctor makes a small incision and removes the baby's head. Unlike a standard cesarean section, when the baby is quickly taken out, not giving the opportunity to adapt to environmental conditions, with a “slow” cesarean section, the child is given the opportunity to get out of the uterus on his own.