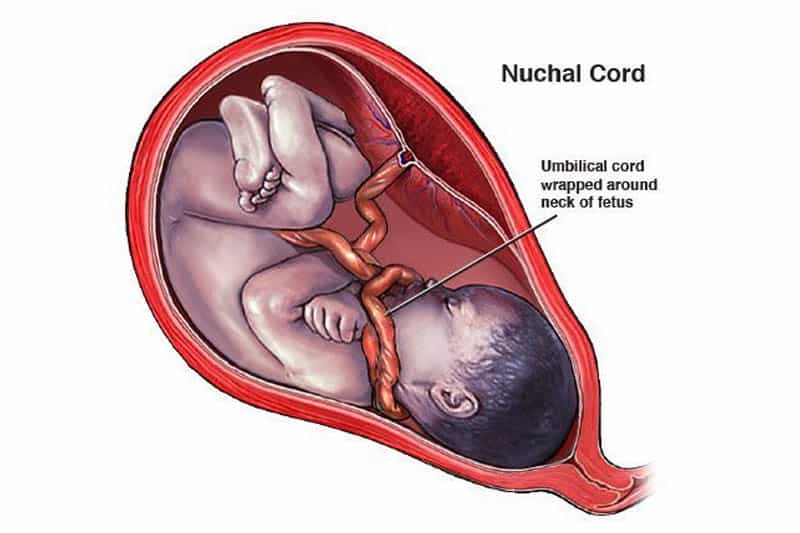
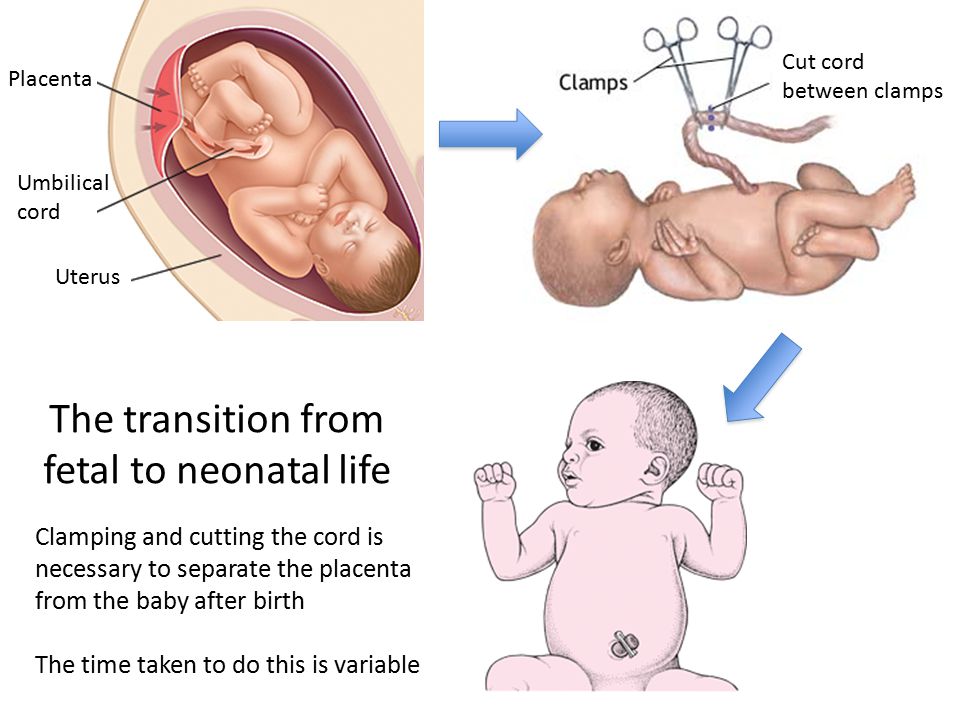
Umbilical cord detaches from placenta
Symptoms, Causes & Effects On Baby
Overview
What is a placental abruption?
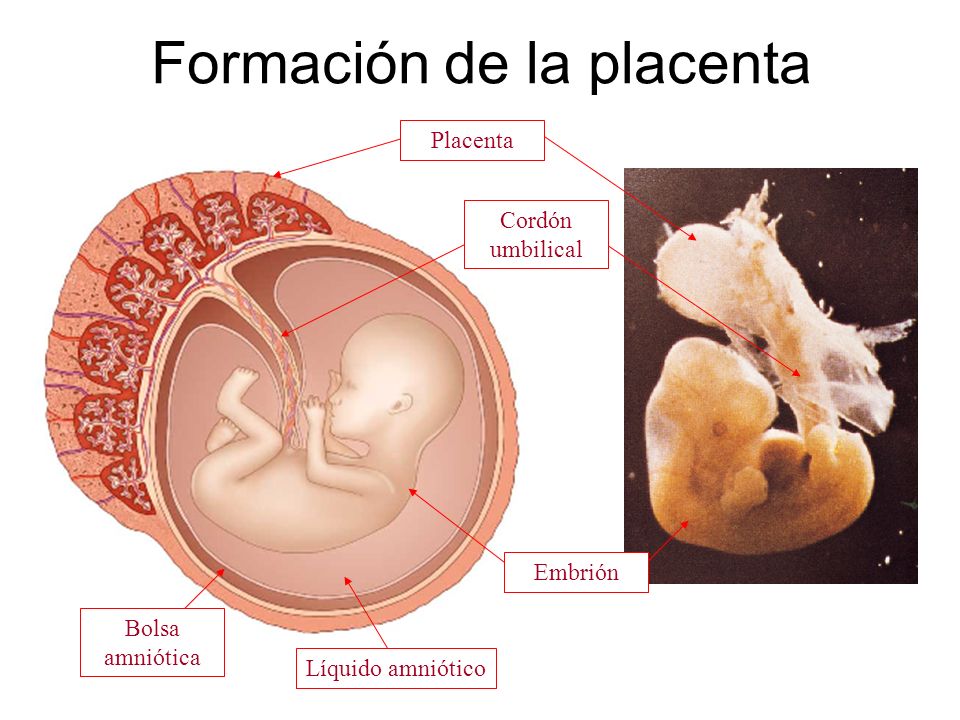
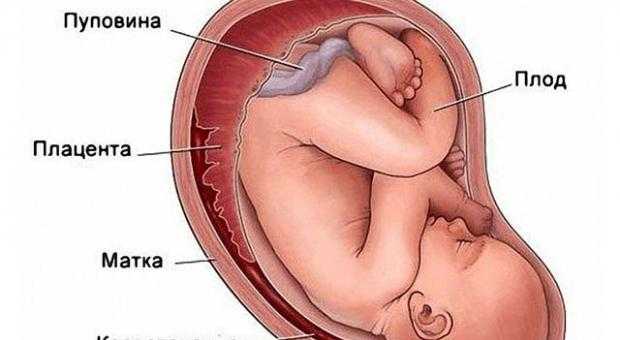
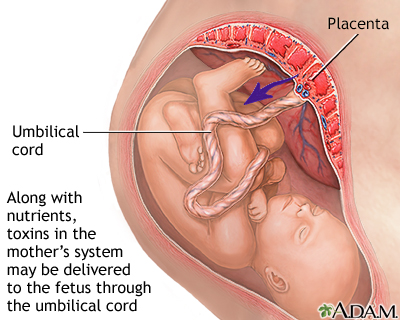
Placental abruption is a complication of pregnancy that happens when the placenta separates from your uterus before delivery. The placenta is a temporary organ that connects a growing fetus to your uterus during pregnancy. It attaches to the wall of your uterus, usually on the top or side and acts as a lifeline that gives nutrients and oxygen to the fetus through the umbilical cord. The placenta also removes waste from the fetus's blood.
In placental abruption, the placenta may completely detach or partially detach. This can decrease the amount of oxygen and nutrients to the fetus and cause heavy bleeding in the birthing parent. Placental abruption is a serious condition that requires medical treatment.
What are the different types of placental abruption?
- A partial placental abruption occurs when the placenta does not completely detach from the uterine wall.
- A complete or total placental abruption occurs when the placenta completely detaches from the uterine wall. There is usually more vaginal bleeding associated with this type of abruption.
- Revealed placental abruptions have moderate to severe vaginal bleeding that you can see.
- Concealed placental abruptions have little or no visible vaginal bleeding. Blood is trapped between the placenta and uterine wall.
What is the difference between placental abruption and placenta previa?
In placenta previa, the placenta is covering all or part of the birthing parent's cervix. It's also called low-lying placenta. Think of it as an obstacle that’s blocking the exit from the uterus. Even though the placenta is in a complicated position, it’s still attached to the uterus. When the placenta detaches from the uterus, this is a placental abruption. Both conditions can cause vaginal bleeding during pregnancy and labor.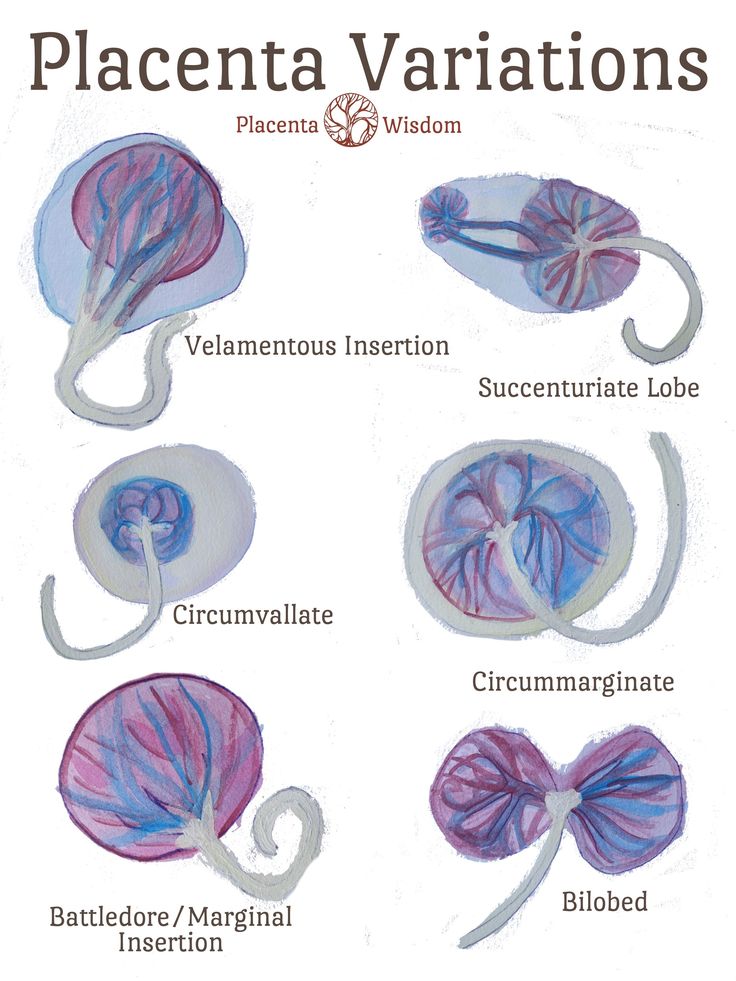
How common is a placental abruption?
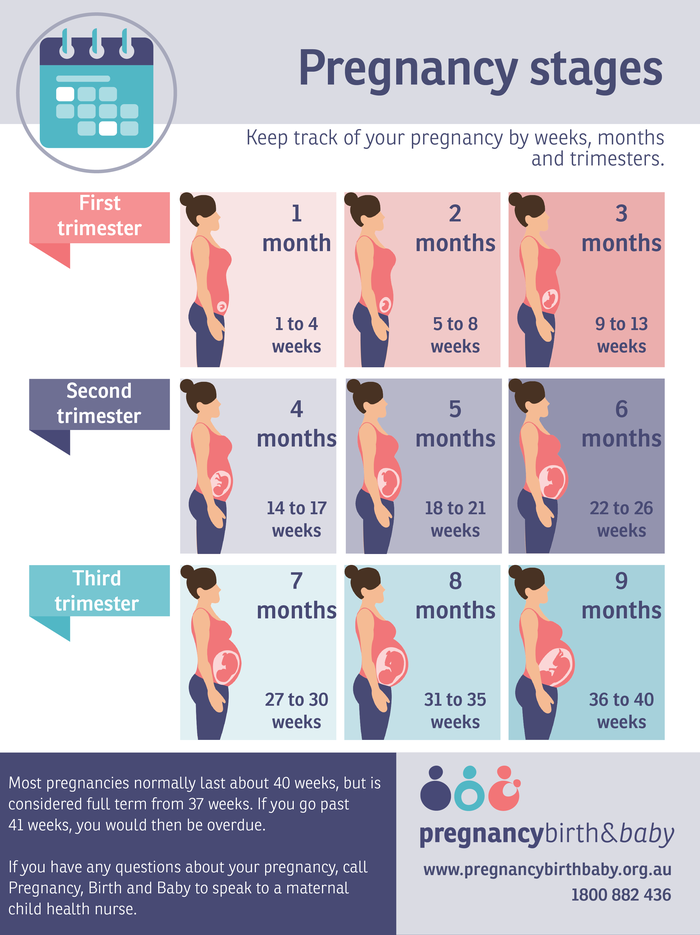
About 1 out of 100 pregnancies has placental abruption. This condition is usually seen in the third trimester, but it can happen any time after 20 weeks of pregnancy up until delivery.
What are the effects of placental abruption?
Placental abruption can be life-threatening to the fetus and sometimes to you. Complications from a placental abruption include:
For baby:
- Premature birth.
- Low birth weight.
- Growth problems.
- Brain injury from lack of oxygen.
- Stillbirth.
For birthing parent:
- Blood loss.
- Blood clotting issues.
- Blood transfusion.
- Hemorrhage.
- Kidney failure.
Symptoms and Causes
What causes placental abruption?
The cause of placental abruption is often unknown. Certain lifestyle choices or abdominal trauma can increase your risk for placental abruption.
What are the risk factors for placental abruption?
You are at higher risk for placental abruptions if you have any of the following:
- Trauma or injury to your uterus (like a car accident, fall or blow to the stomach).
- Previous placental abruption.
- Multiple gestations (twins or triplets).
- High blood pressure (hypertension), gestational diabetes or preeclampsia.
- If you smoke or have a history of drug use.
- Short umbilical cord.
- Maternal age 35 or greater.
- Uterine fibroids.
- Thrombophilia (a blood clotting disorder).
- Premature rupture of membranes (the water breaks before the fetus is full term).
- Rapid loss of the amniotic fluid.
What are the signs and symptoms of placental abruption?
Each person can have different symptoms of placental abruption. However, the most common symptom is vaginal bleeding with cramping during the third trimester of pregnancy. Symptoms or signs can also include:
- Abdominal pain.
- Uterine contractions that are longer and more intense than average labor contractions.
- Uterine tenderness.
- Backache or back pain.
- Decreased fetal movement.

Vaginal bleeding can vary and is not an indication of how much the placenta has separated. In some instances, there could be no visible bleeding because the blood is trapped between the placenta and the uterine wall. Pain can range from mild cramping to strong contractions and often begins suddenly.
These symptoms can resemble other pregnancy conditions. Always consult with your healthcare provider for a diagnosis.
Do you always bleed during a placental abruption?
Most of the time, you will see some blood during a placental abruption. In the event of a concealed abruption, the blood will be behind the placenta. In that case, there will be no bleeding. In other cases, the abruption develops slowly, which can cause occasional, light bleeding.
Talk to your healthcare provider about any vaginal bleeding you experience during your pregnancy.
What does placental abruption feel like?
You may experience sudden or sharp pain, cramping, or tenderness in your lower pelvic region or back during a placental abruption.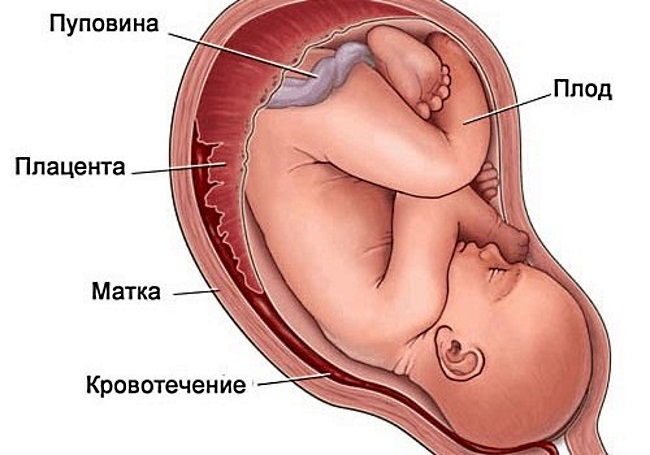 You could also feel less movement from the fetus. You should discuss these symptoms with your healthcare provider immediately.
You could also feel less movement from the fetus. You should discuss these symptoms with your healthcare provider immediately.
What are the first signs of a placental abruption?
The most common symptom of a placental abruption is vaginal bleeding, although you will not always bleed. You may also have sudden, ongoing pain in your abdomen or back.
Diagnosis and Tests
How is a placental abruption diagnosed?
Placental abruption is diagnosed through an exam and monitoring. You may be admitted to the hospital depending on the severity of the abruption or you may be able to rest at home. Your healthcare provider will:
- Ask how much bleeding has occurred.
- Ask where you feel pain and how intense the pain is.
- Ask when symptoms started.
- Monitor your blood pressure.
- Monitor the fetal heart rate and movement.
- Monitor your contractions.
- Use ultrasound to locate the bleeding and to check the fetus.
- Recommend blood or urine tests.
There are typically three grades of placental abruption a healthcare provider will diagnose:
- Grade 1: Small amount of bleeding, some uterine contractions, and no signs of stress to you or the fetus.
- Grade 2: Mild to moderate amount of bleeding, some uterine contractions, and signs of fetal stress.
- Grade 3: Moderate to severe bleeding or concealed bleeding, uterine contractions that do not relax, abdominal pain, low blood pressure, and fetal death.
It is important to discuss any symptoms or changes in symptoms with your healthcare provider.
Management and Treatment
How is a placental abruption treated?
Once the placenta has separated from the uterus, it cannot be reconnected or repaired. A healthcare provider will recommend treatment based on:
- The severity of the abruption.
- How long the pregnancy is/gestational age of the fetus.
- Signs of distress from the fetus.
- Amount of blood you've lost.
Generally, the severity of the abruption and gestational age of the fetus are the two most important factors:
If the fetus isn't close to full term:
- If it's too soon for your baby to be born and your abruption is mild, you will be closely monitored until you reach 34 weeks of pregnancy. If the fetal heart rate is normal and you're not bleeding, your healthcare provider may allow you to go home to rest. They may give you medication to help with fetal lung development.
- If your abruption is severe and the health of you or the fetus are at risk, immediate delivery may be necessary.
If the fetus is near full term:
- If your abruption is mild and the fetal heart rate is stable, a closely monitored vaginal delivery is possible. This is generally determined around 34 weeks of pregnancy.
- If the abruption gets worse or you or the fetus are in danger at any time, the baby will be delivered via emergency Cesarean section.
Prevention
Can I prevent a placental abruption?
Placental abruptions are typically unpreventable. You can reduce your risk by:
- Not smoking or using drugs.
- Keeping your blood pressure at a healthy level.
- Keeping diabetes under control.
- Taking health and safety precautions like wearing a seat belt.
- Reporting any abdominal trauma to your healthcare provider.
- Talking to your healthcare provider about any vaginal bleeding.
Outlook / Prognosis
What can I expect if I have a placental abruption?
This can vary depending on the severity of your symptoms and how far along you are in your pregnancy. You can expect to be monitored closely and often. Watch for any changes in symptoms and discuss them with your healthcare provider immediately.
What is my baby’s survival rate after a placental abruption?
The two factors that affect survival rate are gestational age at birth and the severity of the abruption.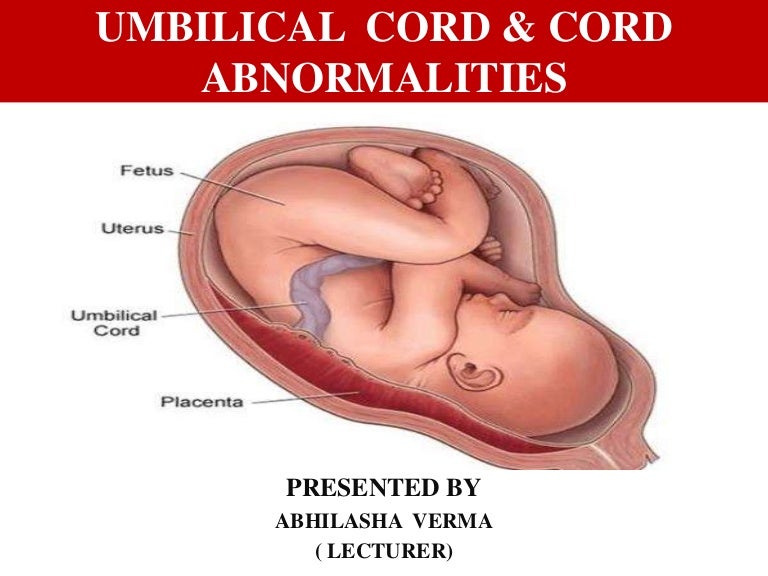 Early detection, close monitoring, and quick treatment can help reduce complications.
Early detection, close monitoring, and quick treatment can help reduce complications.
Can I have another placental abruption?
You have about a 15% chance of having another abruption in a future pregnancy. With two prior abruptions, this chance increases to about 25%. If you have had a previous abruption, please let your healthcare provider know.
What are questions I should ask my healthcare provider?
Your healthcare provider should be able to answer your questions and prepare you for treatment of placental abruption. Here are some questions you might ask:
- Is my baby’s life in danger? Is mine?
- What are my treatment options?
- Can I give birth now?
- How will I know if my abruption is worsening?
- What are potential complications?
- Do I need additional tests?
Frequently Asked Questions
Can sex cause a placental abruption?
Sexual intercourse is not a direct cause of placental abruption.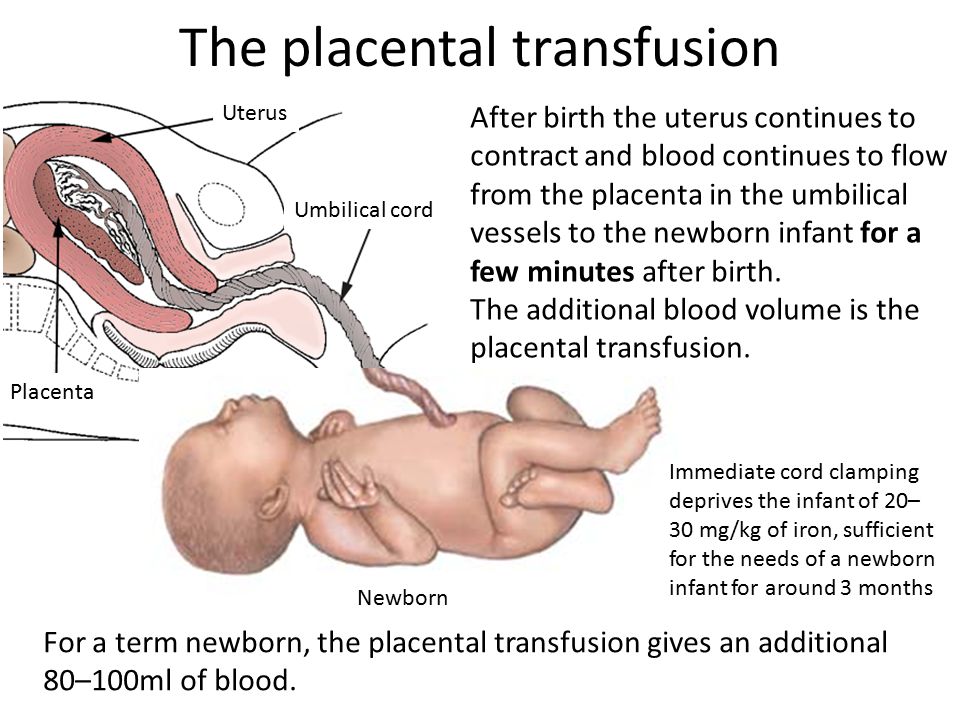 In most cases, it’s perfectly safe to have sex during pregnancy. Activities with a high risk of falling or abdominal trauma should be avoided during pregnancy.
In most cases, it’s perfectly safe to have sex during pregnancy. Activities with a high risk of falling or abdominal trauma should be avoided during pregnancy.
Can sneezing cause a placental abruption?
Sneezing is a normal thing your body does and is not a cause for placental abruption. It can't harm the fetus in any way. If you have any concerns about frequent and forceful sneezing or coughing, reach out to your healthcare provider for guidance.
Can smoking cause a placental abruption?
Smoking can increase your risk of many complications during pregnancy, including placental abruption. Ask your healthcare provider about ways to quit smoking.
When do I call my healthcare provider if I suspect a placental abruption?
Call your healthcare provider immediately if are bleeding, cramping or experience pelvic pain during your pregnancy, especially in the third trimester.
A note from Cleveland Clinic
Placental abruption is an uncommon, yet serious condition people can experience during pregnancy.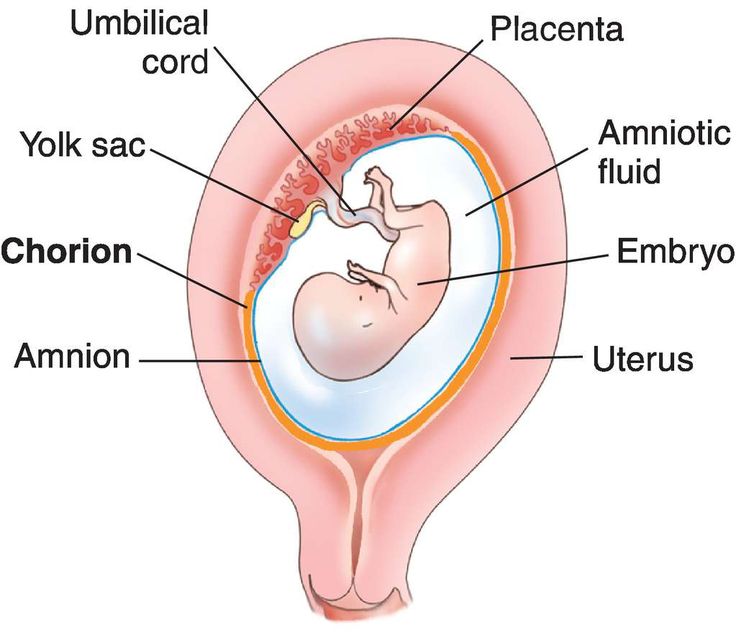 Talk to your healthcare provider if you experience vaginal bleeding, pelvic pain or cramping. Placental abruption should be diagnosed and treated promptly to ensure you and your baby are healthy.
Talk to your healthcare provider if you experience vaginal bleeding, pelvic pain or cramping. Placental abruption should be diagnosed and treated promptly to ensure you and your baby are healthy.
Symptoms, Causes & Effects On Baby
Overview
What is a placental abruption?
Placental abruption is a complication of pregnancy that happens when the placenta separates from your uterus before delivery. The placenta is a temporary organ that connects a growing fetus to your uterus during pregnancy. It attaches to the wall of your uterus, usually on the top or side and acts as a lifeline that gives nutrients and oxygen to the fetus through the umbilical cord. The placenta also removes waste from the fetus's blood.
In placental abruption, the placenta may completely detach or partially detach. This can decrease the amount of oxygen and nutrients to the fetus and cause heavy bleeding in the birthing parent. Placental abruption is a serious condition that requires medical treatment.
What are the different types of placental abruption?
- A partial placental abruption occurs when the placenta does not completely detach from the uterine wall.
- A complete or total placental abruption occurs when the placenta completely detaches from the uterine wall. There is usually more vaginal bleeding associated with this type of abruption.
- Revealed placental abruptions have moderate to severe vaginal bleeding that you can see.
- Concealed placental abruptions have little or no visible vaginal bleeding. Blood is trapped between the placenta and uterine wall.
What is the difference between placental abruption and placenta previa?
In placenta previa, the placenta is covering all or part of the birthing parent's cervix. It's also called low-lying placenta. Think of it as an obstacle that’s blocking the exit from the uterus. Even though the placenta is in a complicated position, it’s still attached to the uterus.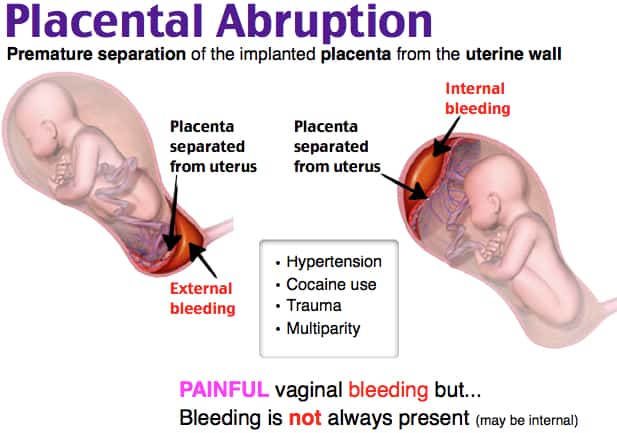 When the placenta detaches from the uterus, this is a placental abruption. Both conditions can cause vaginal bleeding during pregnancy and labor.
When the placenta detaches from the uterus, this is a placental abruption. Both conditions can cause vaginal bleeding during pregnancy and labor.
How common is a placental abruption?
About 1 out of 100 pregnancies has placental abruption. This condition is usually seen in the third trimester, but it can happen any time after 20 weeks of pregnancy up until delivery.
What are the effects of placental abruption?
Placental abruption can be life-threatening to the fetus and sometimes to you. Complications from a placental abruption include:
For baby:
- Premature birth.
- Low birth weight.
- Growth problems.
- Brain injury from lack of oxygen.
- Stillbirth.
For birthing parent:
- Blood loss.
- Blood clotting issues.
- Blood transfusion.
- Hemorrhage.
- Kidney failure.
Symptoms and Causes
What causes placental abruption?
The cause of placental abruption is often unknown. Certain lifestyle choices or abdominal trauma can increase your risk for placental abruption.
Certain lifestyle choices or abdominal trauma can increase your risk for placental abruption.
What are the risk factors for placental abruption?
You are at higher risk for placental abruptions if you have any of the following:
- Trauma or injury to your uterus (like a car accident, fall or blow to the stomach).
- Previous placental abruption.
- Multiple gestations (twins or triplets).
- High blood pressure (hypertension), gestational diabetes or preeclampsia.
- If you smoke or have a history of drug use.
- Short umbilical cord.
- Maternal age 35 or greater.
- Uterine fibroids.
- Thrombophilia (a blood clotting disorder).
- Premature rupture of membranes (the water breaks before the fetus is full term).
- Rapid loss of the amniotic fluid.
What are the signs and symptoms of placental abruption?
Each person can have different symptoms of placental abruption. However, the most common symptom is vaginal bleeding with cramping during the third trimester of pregnancy. Symptoms or signs can also include:
Symptoms or signs can also include:
- Abdominal pain.
- Uterine contractions that are longer and more intense than average labor contractions.
- Uterine tenderness.
- Backache or back pain.
- Decreased fetal movement.
Vaginal bleeding can vary and is not an indication of how much the placenta has separated. In some instances, there could be no visible bleeding because the blood is trapped between the placenta and the uterine wall. Pain can range from mild cramping to strong contractions and often begins suddenly.
These symptoms can resemble other pregnancy conditions. Always consult with your healthcare provider for a diagnosis.
Do you always bleed during a placental abruption?
Most of the time, you will see some blood during a placental abruption. In the event of a concealed abruption, the blood will be behind the placenta. In that case, there will be no bleeding. In other cases, the abruption develops slowly, which can cause occasional, light bleeding.
Talk to your healthcare provider about any vaginal bleeding you experience during your pregnancy.
What does placental abruption feel like?
You may experience sudden or sharp pain, cramping, or tenderness in your lower pelvic region or back during a placental abruption. You could also feel less movement from the fetus. You should discuss these symptoms with your healthcare provider immediately.
What are the first signs of a placental abruption?
The most common symptom of a placental abruption is vaginal bleeding, although you will not always bleed. You may also have sudden, ongoing pain in your abdomen or back.
Diagnosis and Tests
How is a placental abruption diagnosed?
Placental abruption is diagnosed through an exam and monitoring. You may be admitted to the hospital depending on the severity of the abruption or you may be able to rest at home. Your healthcare provider will:
- Ask how much bleeding has occurred.
- Ask where you feel pain and how intense the pain is.
- Ask when symptoms started.
- Monitor your blood pressure.
- Monitor the fetal heart rate and movement.
- Monitor your contractions.
- Use ultrasound to locate the bleeding and to check the fetus.
- Recommend blood or urine tests.
There are typically three grades of placental abruption a healthcare provider will diagnose:
- Grade 1: Small amount of bleeding, some uterine contractions, and no signs of stress to you or the fetus.
- Grade 2: Mild to moderate amount of bleeding, some uterine contractions, and signs of fetal stress.
- Grade 3: Moderate to severe bleeding or concealed bleeding, uterine contractions that do not relax, abdominal pain, low blood pressure, and fetal death.
It is important to discuss any symptoms or changes in symptoms with your healthcare provider.
Management and Treatment
How is a placental abruption treated?
Once the placenta has separated from the uterus, it cannot be reconnected or repaired. A healthcare provider will recommend treatment based on:
A healthcare provider will recommend treatment based on:
- The severity of the abruption.
- How long the pregnancy is/gestational age of the fetus.
- Signs of distress from the fetus.
- Amount of blood you've lost.
Generally, the severity of the abruption and gestational age of the fetus are the two most important factors:
If the fetus isn't close to full term:
- If it's too soon for your baby to be born and your abruption is mild, you will be closely monitored until you reach 34 weeks of pregnancy. If the fetal heart rate is normal and you're not bleeding, your healthcare provider may allow you to go home to rest. They may give you medication to help with fetal lung development.
- If your abruption is severe and the health of you or the fetus are at risk, immediate delivery may be necessary.
If the fetus is near full term:
- If your abruption is mild and the fetal heart rate is stable, a closely monitored vaginal delivery is possible.
 This is generally determined around 34 weeks of pregnancy.
This is generally determined around 34 weeks of pregnancy. - If the abruption gets worse or you or the fetus are in danger at any time, the baby will be delivered via emergency Cesarean section.
Prevention
Can I prevent a placental abruption?
Placental abruptions are typically unpreventable. You can reduce your risk by:
- Not smoking or using drugs.
- Keeping your blood pressure at a healthy level.
- Keeping diabetes under control.
- Taking health and safety precautions like wearing a seat belt.
- Reporting any abdominal trauma to your healthcare provider.
- Talking to your healthcare provider about any vaginal bleeding.
Outlook / Prognosis
What can I expect if I have a placental abruption?
This can vary depending on the severity of your symptoms and how far along you are in your pregnancy. You can expect to be monitored closely and often. Watch for any changes in symptoms and discuss them with your healthcare provider immediately.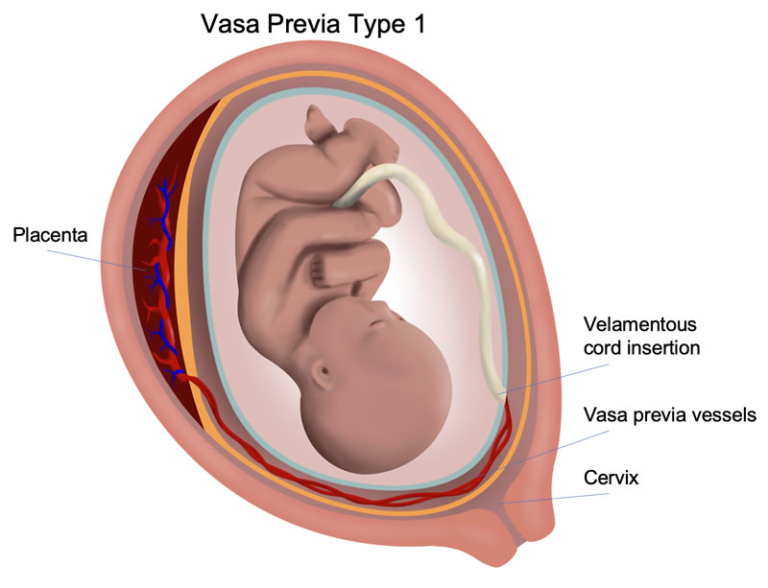
What is my baby’s survival rate after a placental abruption?
The two factors that affect survival rate are gestational age at birth and the severity of the abruption. Early detection, close monitoring, and quick treatment can help reduce complications.
Can I have another placental abruption?
You have about a 15% chance of having another abruption in a future pregnancy. With two prior abruptions, this chance increases to about 25%. If you have had a previous abruption, please let your healthcare provider know.
What are questions I should ask my healthcare provider?
Your healthcare provider should be able to answer your questions and prepare you for treatment of placental abruption. Here are some questions you might ask:
- Is my baby’s life in danger? Is mine?
- What are my treatment options?
- Can I give birth now?
- How will I know if my abruption is worsening?
- What are potential complications?
- Do I need additional tests?
Frequently Asked Questions
Can sex cause a placental abruption?
Sexual intercourse is not a direct cause of placental abruption. In most cases, it’s perfectly safe to have sex during pregnancy. Activities with a high risk of falling or abdominal trauma should be avoided during pregnancy.
In most cases, it’s perfectly safe to have sex during pregnancy. Activities with a high risk of falling or abdominal trauma should be avoided during pregnancy.
Can sneezing cause a placental abruption?
Sneezing is a normal thing your body does and is not a cause for placental abruption. It can't harm the fetus in any way. If you have any concerns about frequent and forceful sneezing or coughing, reach out to your healthcare provider for guidance.
Can smoking cause a placental abruption?
Smoking can increase your risk of many complications during pregnancy, including placental abruption. Ask your healthcare provider about ways to quit smoking.
When do I call my healthcare provider if I suspect a placental abruption?
Call your healthcare provider immediately if are bleeding, cramping or experience pelvic pain during your pregnancy, especially in the third trimester.
A note from Cleveland Clinic
Placental abruption is an uncommon, yet serious condition people can experience during pregnancy.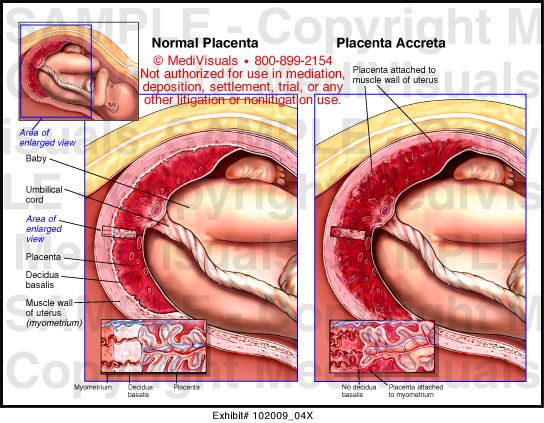 Talk to your healthcare provider if you experience vaginal bleeding, pelvic pain or cramping. Placental abruption should be diagnosed and treated promptly to ensure you and your baby are healthy.
Talk to your healthcare provider if you experience vaginal bleeding, pelvic pain or cramping. Placental abruption should be diagnosed and treated promptly to ensure you and your baby are healthy.
Sitemap
State autonomous professional
educational institution
Republic of Bashkortostan
"Salavat Medical College"
453261 Republic of Bashkortostan
Salavat, st. Furmanova, 4
Phone/fax: (3476)-38-78-83
e-mail: [email protected]
- College information
- Basic information
- Structure and governing bodies of the college
- Documents
- Education
- Educational standards and requirements
- Manual.
 Teaching staff
Teaching staff - Logistics and equipment of the educational process
- Scholarships and other financial support
- Paid educational services
- Financial and business activities
- Vacancies for reception (transfer)
- Personal data processing
- Anti-corruption
- Legal framework for combating extremism and terrorism
- Vacancies
- Information security
- Olympics
- Mentoring
- Available environment
- International cooperation
- Applicant
- Applicant
- Control figures for the reception of citizens
- Admission Rules
- Regulations on Individual Achievements
- Local regulations
- List of specialties
- Document acceptance schedule
- Terms of admission under contracts for the provision of paid educational services
- Information on the need for applicants to undergo a mandatory preliminary medical examination (examination)
- Exemplary entrance tests
- Features of conducting entrance examinations for the disabled and persons with disabilities
- Information about the possibility of filing documents by mail
- Submission of documents by e-mail
- List and deadlines for submission of documents
- Information on the availability of a hostel and the number of places in hostels allocated for nonresident applicants
- Enrollment Orders
- Number of applications submitted
- Filing and hearing appeals
- College Application
- Appeal of citizens on admission issues
- Targeted training
- Consent to the processing of personal data
- Entrance examinations
- Rating of applicants
- student
- Fundamentals
- Regulations
- Culture and sports
- Dormitory
- Student Council
- Life safety
- Teaching materials
- Employment of graduates
- Graduate Accreditation
- Page of educational psychologist
- Student Union
- Scholarship of the Head of the Republic of Bashkortostan
- teacher
- Reference information
- Educational and methodical work
- Additional education
- Republican information and training pedagogical seminars
- Contacts
- Hotline
- Feedback
- Contacts of controlling organizations
This page does not exist.
|
The navel was first discovered in non-avian dinosaurs
Paleontologists studied the integument of a well-preserved specimen of Psittacosaurus and found an umbilical scar (actually a navel) in it, like in some crocodiles and lizards.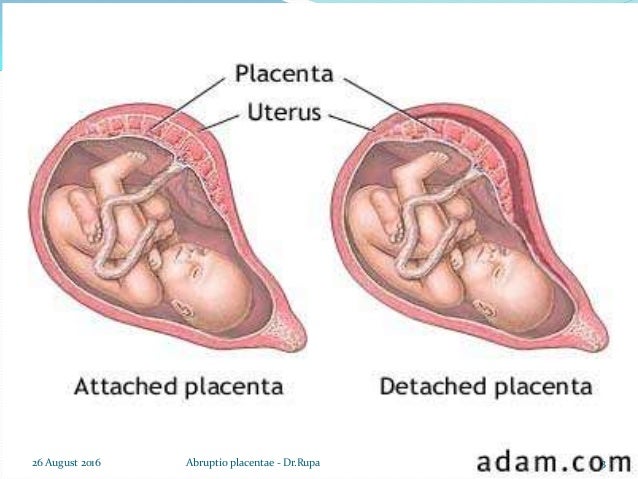 This is the first find of a navel among non-avian dinosaurs - and among all pre-Cenozoic amniotes in general. The study was published in the journal BMC Biology .
This is the first find of a navel among non-avian dinosaurs - and among all pre-Cenozoic amniotes in general. The study was published in the journal BMC Biology .
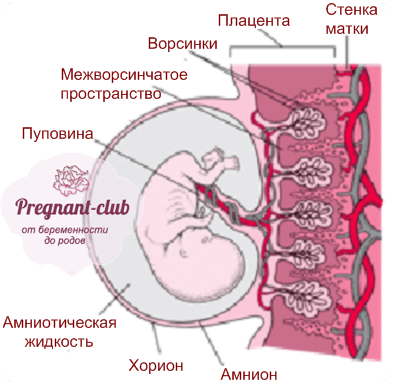
Amniotes (Amniota) include sauropsids (traditional reptiles along with birds) and synapsids (mammals and their relatives). A distinctive feature of this group is the four embryonic membranes (amnion, chorion, allantois and yolk sac), which ensure the development of the embryo out of water. In this they differ from anamnia (Anamnia) - amphibians, fish and jawless ones, which need water for reproduction.
Amnion (the group is actually named after him) provides the aquatic environment that is necessary for the development of the embryo. The chorion (serous membrane) and allantois are responsible for gas exchange, while the latter also serves as a place for the accumulation of nitrogenous waste (which is why it is also called the embryonic bladder). Finally, the yolk sac provides nourishment to the embryo.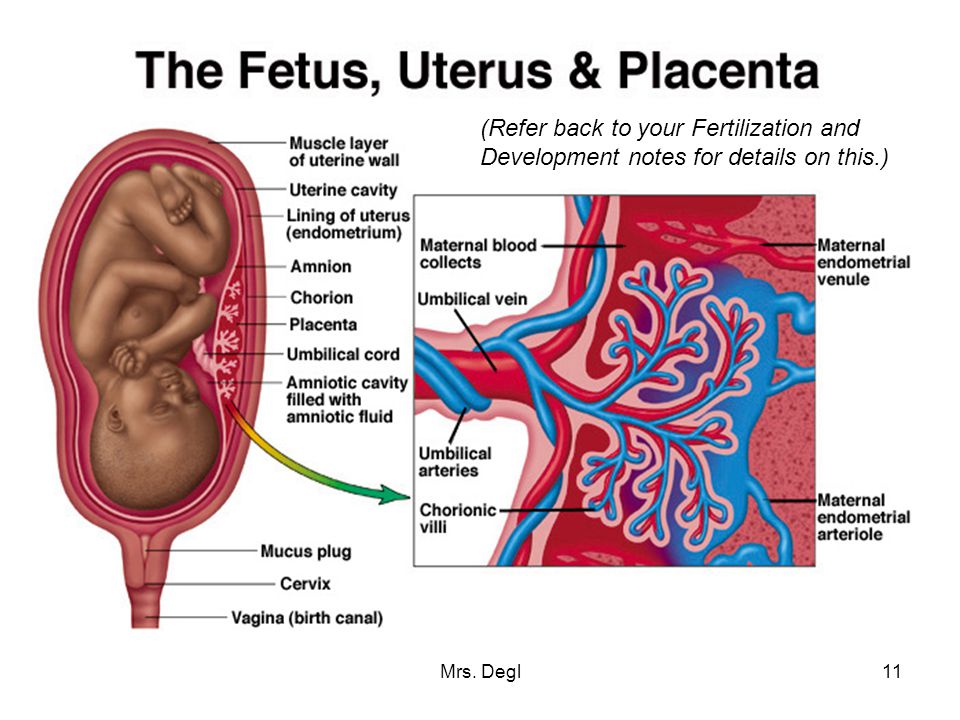
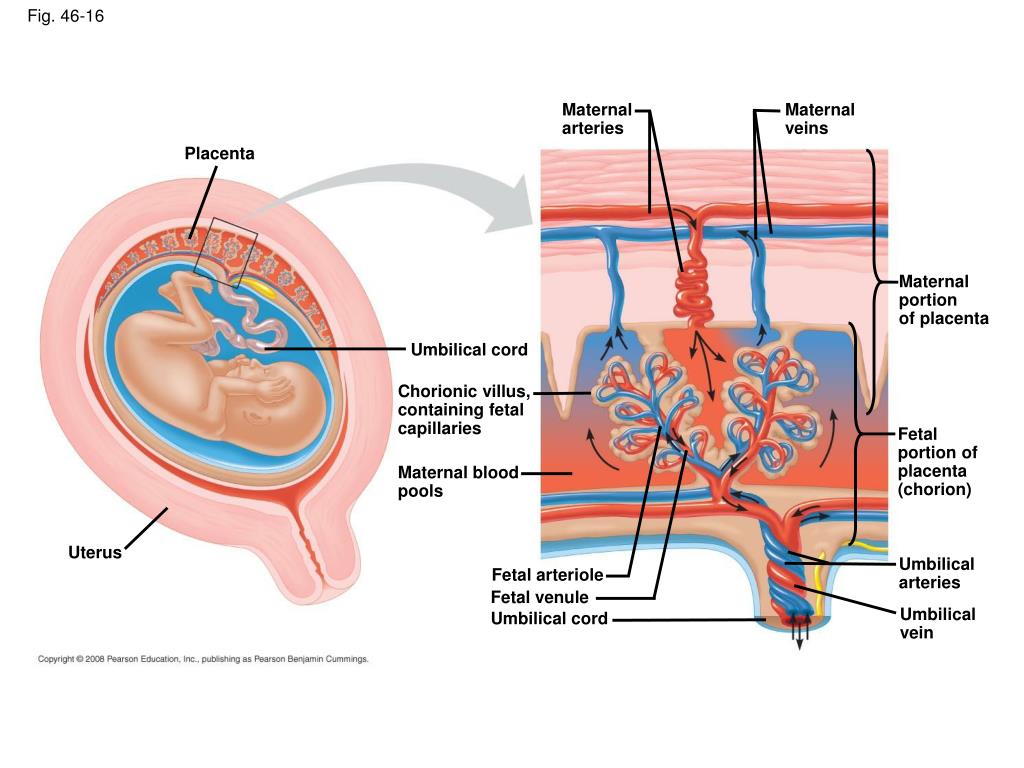
There are various modifications of these structures. For example, chorion and allantois in placental mammals are involved in the formation of the placenta. The embryonic membranes are also part of the umbilical cord, which connects the embryo to the placenta. After birth, the umbilical cord is separated - and a scar remains at the place of its attachment, which is called the navel.
However, not only placental mammals have a similar scar, but also other amniotes, since their embryos have a connection with the yolk sac and allantois. Before hatching, the remnants of the yolk sac are drawn into the body of the embryo through the umbilical opening, which then closes with the formation of a scar. In most sauropsids, the scar disappears a few days or weeks after hatching, but in some species, such as the rock dove ( Columba livia ) or the Mississippi alligator ( Alligator mississippiensis ), it is also preserved in adults.
Soft tissues rarely fossilize, so umbilical scars have not yet been found in pre-Cenozoic amniotes.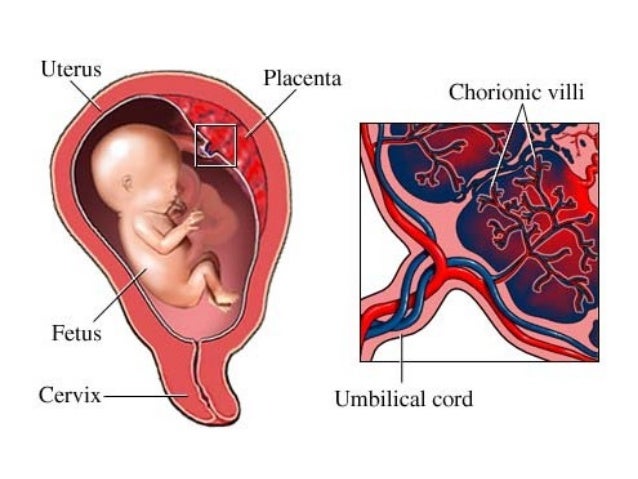 This situation was corrected by Phil R. Bell from the University of New England in Australia and his colleagues from Argentina, China and the USA. Using laser-induced fluorescence, paleontologists studied the integument of a well-preserved specimen of Psittacosaurus ( Psittacosaurus sp. ) is a basal horned dinosaur, a distant relative of Triceratops.
This situation was corrected by Phil R. Bell from the University of New England in Australia and his colleagues from Argentina, China and the USA. Using laser-induced fluorescence, paleontologists studied the integument of a well-preserved specimen of Psittacosaurus ( Psittacosaurus sp. ) is a basal horned dinosaur, a distant relative of Triceratops.
This specimen (SMF R 4970) comes from the Chinese province of Liaoning, most likely from the Lower Cretaceous Yixian Formation, estimated to be between 125.8 and 124.1 million years old. In total, about a dozen species of psittacosaurus are known (one of which, Psittacosaurus sibiricus , was found on the territory of Russia), but SMF R 4970 is not assigned to a specific species.
Previously, other researchers have already studied its integuments and found formations on the tail that look like needles or bristles. This time, paleontologists found two rows of scales on the abdomen with a line of interstitial tissue between them.