Signs premature labour
Premature labour and birth - NHS
Premature labour is labour that happens before the 37th week of pregnancy. About 8 out of 100 babies will be born prematurely.
Urgent advice: Call your midwife or maternity unit if you're less than 37 weeks pregnant and you have:
- regular contractions or tightenings
- period-type pains
- a gush or trickle of fluid from your vagina – this could be your waters breaking
- backache that's not usual for you
The midwife or hospital will offer checks, tests and monitoring to find out whether:
- your waters have broken
- you're in labour
- you have an infection
These may include a vaginal examination, blood test, urine test and cardiotocography to record contractions and the baby's heartbeat.
They'll need to check you and your baby to find out whether you're in labour and discuss your care choices with you.
Planned premature labour
In some cases, pre-term labour is planned and induced because it's safer for the baby to be born sooner rather than later.
This could be because of a health condition in the mother (such as pre-eclampsia) or in the baby. Your midwife and doctor will discuss with you the benefits and risks of continuing with the pregnancy versus your baby being born premature.
You can still make a birth plan and discuss your wishes with your birth partner, midwife and doctor.
If your waters have broken
If your waters have broken (called preterm pre-labour rupture of membranes, P-PROM), there's an increased risk of infection for you and your baby.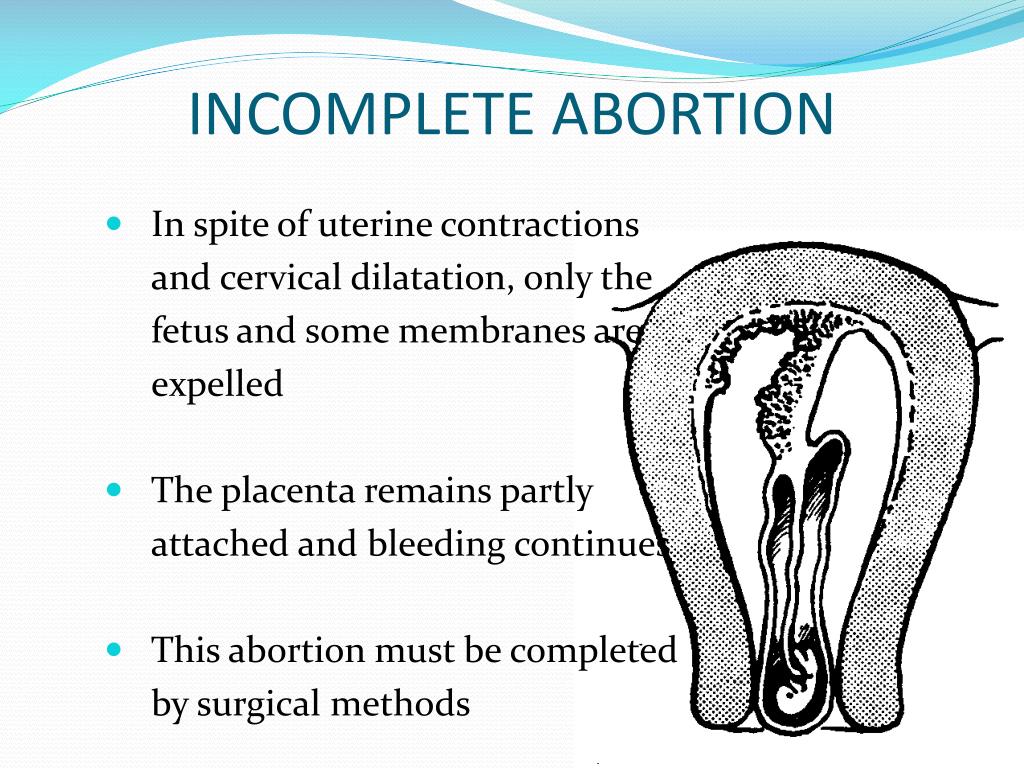 You'll be offered:
You'll be offered:
- antibiotics to take
- tests for infection
P-PROM does not definitely mean you're going into labour but you may be advised to stay in hospital for a few days. When you go home, you'll be advised to call your midwife or maternity unit immediately if:
- your temperature is raised
- you feel hot and shivery
- any fluid coming from your vagina is greenish or smelly
- you bleed from your vagina
- you have pain in your tummy or back
- you have contractions
- your baby's movements slow down or stop or there is a change to their usual pattern of movements
If your pre-term labour is planned or unplanned or if your waters have broken prematurely, you may be offered steroid injections.
If your waters have not broken
Your midwife or doctor should discuss with you the symptoms of pre-term labour and offer checks to see if you're in labour. These checks can include asking you about your medical and pregnancy history, and about possible labour signs, such as:
- contractions – how long, how strong and how far apart they are
- any pain
- any fluid coming from your vagina
You may be offered a vaginal examination, and your pulse, blood pressure and temperature may also be checked.
Your midwife or doctor will also check your baby. They'll probably feel your bump to find out the baby's position and how far into your pelvis the baby's head is.
They should also ask about your baby's movements in the last 24 hours. If they do not ask, tell them about the baby's movements.
If they do not ask, tell them about the baby's movements.
If you're in premature labour
The midwife or doctor may offer:
- medicine to try to slow down or stop your labour
- steroid injections, which can help your baby's lungs
Slowing down labour or stopping it is not appropriate in all circumstances – your midwife or doctor can discuss your situation with you. They will consider:
- how many weeks pregnant you are
- whether it might be safer for the baby to be born – for example, if you have an infection or you're bleeding
- local neonatal (newborn) care facilities and whether you might need to be moved to another hospital
- your wishes
You may be offered a course of steroid injections to help your baby's lungs get ready for breathing if they're born prematurely.
Steroids may not be offered after 36 weeks as your baby's lungs are likely to be ready for breathing on their own.
If you're in premature labour and you're 24 to 29 weeks pregnant you should be offered magnesium sulphate. This can help protect your baby's brain development.
You may also be offered it if you're in labour and 30 to 33 weeks pregnant. This is to protect your baby against problems linked to being born too soon, such as cerebral palsy.
If you take magnesium sulphate for more than 5 to 7 days or several times during your pregnancy, your newborn baby may be offered extra checks. This is because prolonged use of magnesium sulphate in pregnancy has in rare cases been linked to bone problems in newborn babies.
Treatment to prevent early labour
You may be offered treatment to prevent early labour if:
- you've given birth at less than 34 weeks pregnant before
- you've had a miscarriage from 16 weeks pregnant before
- your waters have broken before 37 weeks, in this pregnancy or before
- your cervix has been injured in the past, for example through surgery
- you have a short cervix
There are 2 treatments:
- a small tablet of hormone medicine that you put into your vagina
- an operation to put a stitch in your cervix to help support it
Your midwife or doctor will offer the choice of 2 treatments and they should discuss the risks and benefits with you.
What are the risks to my baby of being born early?
Babies born before full term (before 37 weeks) are vulnerable to problems associated with being born premature. The earlier in the pregnancy a baby is born, the more vulnerable they are.
It's possible for a baby to survive if born at around 24 weeks of pregnancy.
Babies born this early need special care in a hospital with specialist facilities for premature babies. This is called a neonatal unit. They may have health and development problems because they have not fully developed in the womb.
If your baby is likely to be delivered early, you should be admitted to a hospital with a neonatal unit.
Not all hospitals have facilities for the care of very premature babies, so it may be necessary to transfer you and your baby to another unit.
Find out about babies who need special intensive care
Twins and multiples
Twins and triplets are often born prematurely. Find out about giving birth to twins.
Find out about giving birth to twins.
If you have any reason to think that your labour may be starting early, contact your hospital straight away.
Signs and symptoms of premature labour
Early labour means going into labour before 37 weeks. After this point, your pregnancy is classed as full term.
If you think you may be going into early labour, call the hospital or your midwife straight away for advice. They will usually tell you to go straight to hospital, and they may send an ambulance for you.
It’s very difficult, but try not to panic. In 7 out of 10 cases, the symptoms go away and women give birth at term. More than 9 out of 10 women do not give birth within 14 days of having these symptoms.
What are the signs of premature labour?
If you have any of the following symptoms, call the hospital or midwife straight away, because you could be in labour:
- regular contractions or tightenings
- period-type pains or pressure in your vaginal area
- a "show" – when the plug of mucus that has sealed the cervix during pregnancy comes away and out of the vagina
- a gush or trickle of fluid from your vagina – this could be your waters breaking
- backache.

Tell your midwife or hospital staff immediately if:
- you are bleeding
- your baby is moving less than usual
- your waters have broken and they are smelly or coloured.
Braxton Hicks
You may have some signs labour has started, but not others. For example, your waters may have broken but with no contractions, or you may have contractions but your waters haven’t broken.
Many women experience Braxton Hicks, sometimes known as practice contractions. These can become quite strong during the third trimester, and it's easy to mistake them for the real thing. They are usually not painful, so it is important to get checked in hospital if you are having painful contractions.
Find out what contractions really feel like.
What happens at the hospital?
The doctor or midwife at the hospital will examine you and offer you tests to find out if:
- your waters have broken
- you’re in labour
- you have an infection.

These tests may include:
- a vaginal examination to check if your cervix is opening
- blood tests to check for infection
- urine tests to check for infection (or protein for pre-eclampsia)
- a check of your pulse, blood pressure and temperature
- feeling your bump to check the baby’s position
- swabs for infections such as bacterial vaginosis and group B strep
- monitoring and recording any contractions
- a check of your baby’s heartbeat
- a vaginal swab (such as a fetal fibronectin test) to see if your body is preparing to give birth.
Your baby’s movements
Your healthcare team should also ask you about your baby’s movements in the last 24 hours. If they don’t, tell them about your baby’s movements. You should continue to feel your baby move in a normal pattern right up to the time you go into labour and during labour. Tell your healthcare professional immediately if you think your baby’s movements have slowed down, stopped or changed.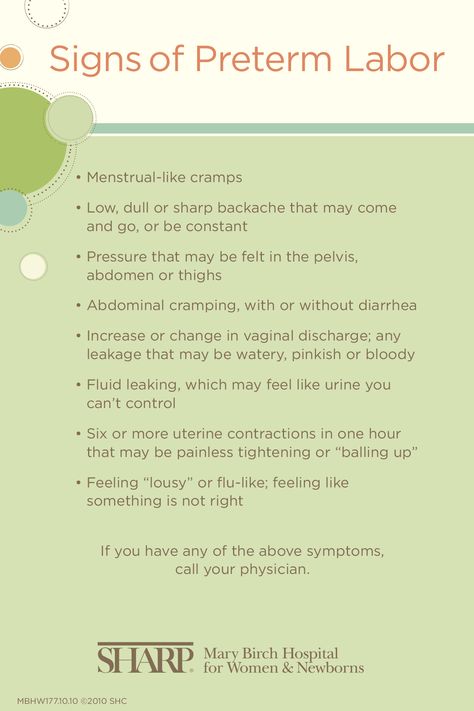
If your waters have broken early (preterm premature rupture of the membranes – PPROM)
Normally your waters break shortly before or during labour. If your waters break before labour at less than 37 weeks of pregnancy, this is known as preterm prelabour rupture of membranes or PPROM. If this happens, it can (but does not always) trigger early labour.
Find out more about PPROM.
How will I know if my waters have broken?
This may feel like a mild popping sensation and/or a trickle or gush of fluid that you can’t stop, unlike when you wee. You may not have any sensation of the actual ‘breaking’, and then the only sign that your waters have broken is the trickle of fluid.
Find out more about what to expect when your waters break.
What happens if I am in preterm labour?
The midwife or doctor will talk to you about whether it’s best to birth your baby now (either by vaginal delivery or caesarean section) or try to slow down labour using medication. They will consider:
They will consider:
- how many weeks pregnant you are
- you and your baby’s health
- what neonatal facilities are available and whether you need to be moved to another hospital
- what you want to do.
You may need to be moved to a hospital that has facilities for premature deliveries. Find out more about in utero transfer.
Removing a stitch (cerclage) if you have one
If you are going to give birth and have had a transvaginal cervical stitch, you will need to have it removed before your baby is born. This is because there is a risk of it tearing if it is still in place while you are having contractions.
If you had a transabdominal stitch, the healthcare team will prepare for a caesarean section. This is because this type of stitch will prevent the cervix from opening so you will not be able to have a vaginal birth.
Medications
Sadly, babies that are born prematurely are more likely to have some health problems. To help reduce the risks you may be offered medication either to delay the birth, or to improve the baby’s health before they are born. Find out more about preparing your baby for a premature birth and giving birth to a premature baby.
To help reduce the risks you may be offered medication either to delay the birth, or to improve the baby’s health before they are born. Find out more about preparing your baby for a premature birth and giving birth to a premature baby.
What happens if I’m not in labour?
If labour hasn't started, your healthcare professional will investigate what may be causing your symptoms and if you and your baby would benefit from further treatment.
They may sometimes recommend that you stay in hospital so they can monitor you and your baby.
Find out what to pack for labour
Premature birth. What do you need to know about them?
According to the recommendations of the World Health Organization, preterm births are considered to occur between the 22nd and 38th weeks of pregnancy.
If we talk about the prevalence of this pathology, then its frequency ranges from 4 to 8% in countries with a developed healthcare system and up to 10-12% in countries that are somewhat lagging behind in terms of the level of medicine. Specifically, in the city of Minsk, the frequency of preterm birth is approximately 3-4%. nine0003
Specifically, in the city of Minsk, the frequency of preterm birth is approximately 3-4%. nine0003
Where is the problem?
Of course, the etiology of triggering the mechanism of preterm labor has not been fully studied. The nature of this phenomenon is very diverse and many-sided. However, experts identify a number of factors that play a leading role in the occurrence of this pathology.
The most common cause of preterm labor is infectious factor . That is, any, even the most banal, for example, a respiratory infection, can trigger the mechanism of premature birth. How does this happen? As a result of the infection in the body, a large amount of biologically active substances are released, which trigger a cascade of various reactions leading to contractile activity of the uterus. Also, the infection can lead to chorioamnionitis (inflammation of the membranes), which provokes premature opening of the membranes and the outflow of amniotic fluid. nine0003
nine0003
Against the background of intrauterine infection, polyhydramnios often occurs, which also provokes premature outflow of water.
The next most common cause of preterm birth is endocrine disorders . The most common is the pathology of the thyroid gland (especially hypofunction), then the pancreas. Also recently there has been an increase in the incidence of gestational diabetes (diabetes that first occurs during pregnancy). In addition, dysfunction of the placenta can be associated with a violation of its structure, improper attachment, and even more often with extragenital pathologies of the mother, leading to feto-placental insufficiency. nine0003
The so-called uterine factors occupy a separate niche in the causes of premature birth. These include fibroids (the myomatous node prevents the normal growth of the uterus), intrauterine synechia, anomalies in the development of the uterus, etc. Often, the cause of premature birth is isthmic-cervical insufficiency. Normally, the muscular ring of the cervix (internal and external os) holds the fetus in the uterine cavity during the gestation period. However, with the development of isthmic-cervical insufficiency (ICI), the muscular ring does not cope with this important function, resulting in the opening of the cervix. The dilated cervix, in turn, cannot hold a growing fetal egg, which poses a threat of miscarriage or premature birth. nine0003
Normally, the muscular ring of the cervix (internal and external os) holds the fetus in the uterine cavity during the gestation period. However, with the development of isthmic-cervical insufficiency (ICI), the muscular ring does not cope with this important function, resulting in the opening of the cervix. The dilated cervix, in turn, cannot hold a growing fetal egg, which poses a threat of miscarriage or premature birth. nine0003
Other causes include central placenta previa, pelvic or incorrect (transverse or oblique) position of the fetus, intoxication of the woman's body, immunological factors that are currently least studied. In rare cases, premature birth can be caused by genetic abnormalities, severe extragenital pathologies of the mother.
The social factor also plays an important role: alcohol, smoking, unhealthy lifestyle are very often the cause of premature birth. nine0003
It is worth noting that in most cases you have to deal with a combination of the above reasons.
When the need arises
In some cases, for medical reasons, doctors have to decide on early delivery. This can be caused by both indications from the mother and from the fetus. The indications on the part of the woman in labor are the conditions in which the further continuation of the pregnancy may pose a threat to her life and health. Such situations may arise in connection with severe preeclampsia, arterial hypertension, long-term treatment-resistant pyelonephritis, retinal detachment, etc.
As for indications from the fetus, these will be all situations in which it is in a state of acute or decompensated chronic hypoxia.
Very often, early delivery is used in multiple pregnancies: in about 40-45% of cases of twins and 100% of cases of triplets. However, here we are talking about planned medical intervention.
Symptoms and course of preterm labor
Clinical symptoms of preterm labor are usually pain in the lower abdomen and in the lumbar region, which can be both permanent and cramping. A sign of the onset of labor can also be abundant mucous discharge from the vagina, which can sometimes be slightly stained with blood. nine0003
A sign of the onset of labor can also be abundant mucous discharge from the vagina, which can sometimes be slightly stained with blood. nine0003
On palpation, the uterus may be toned or excitable. During vaginal examination, the cervix may be shortened, softened. The cervical canal can be either closed or open.
When childbirth is already in progress, a woman feels cramping pains in the lower abdomen, the intensity and duration of which is constantly increasing. The cervix gradually shortens, softens and opens.
Premature rupture of amniotic fluid occurs with or without cervical dilatation. Often it precedes the development of contractions. nine0003
As a rule, preterm labor lasts longer than usual, which is due to the unpreparedness of the internal mechanisms of the female body that regulate labor forces and determine the normal course of urgent labor.
In preterm labor, weakness and incoordination of labor activity are often observed. The rapid course of preterm labor is less common, usually with intrauterine infection of the fetus.
Complications also occur more frequently in the postpartum period than in urgent deliveries. The most common are hypotonic bleeding (impaired uterine contractility), retention of parts of the placenta in the uterus, complications of an infectious nature (metroendometritis, thrombophlebitis). nine0003
Important to know! At the onset of preterm labor, it is very important to be in the hospital as soon as possible, as doctors need to prevent the respiratory distress syndrome of the newborn - intrauterine prevention of respiratory disorders.
Management of preterm labor
Management of preterm labor turns out to be more gentle to the fetus and the mother's birth canal.
During childbirth, all violations of labor activity are regulated. Anesthetization of childbirth, including medical sleep, is often used. With signs of chronic infection, prevention of intrauterine infection is carried out. There is also continuous monitoring of laboratory tests and dynamic cardiomonitoring of the fetus. nine0003
nine0003
Why is preterm birth dangerous?
The main danger of preterm birth is that babies are born prematurely. That is, further we are faced with the problem of premature babies, the risk of dying or acquiring any disease is higher in them than in full-term ones.
All organs and systems of such babies: brain, respiratory organs, liver, etc. still immature. The digestive tract is not yet able to fully absorb the necessary nutrients. Premature babies are very susceptible to infections, their blood vessels are characterized by increased fragility, their thermoregulatory function does not work at all, and immunity is not fully formed. nine0003
Naturally, the earlier a child is born, the more he is unfit for life in the outside world.
It is most difficult for children who were born with extremely low body weight: from 500 g to 1 kg. These are births from the 22nd to the 28th week of pregnancy. Most of these babies may suffer from disorders of the musculoskeletal system, diseases of the psycho-neurological profile.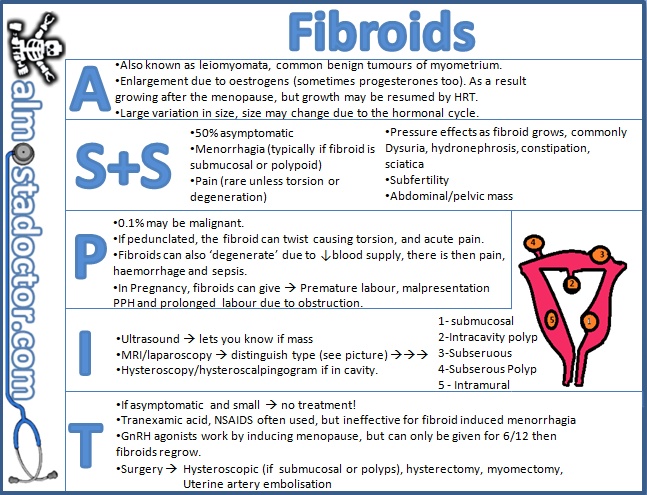 In addition, premature babies are at risk for developing blindness and deafness.
In addition, premature babies are at risk for developing blindness and deafness.
Better prospects for babies born with low birth weight: 1 to 1.5 kg (delivery after 28 weeks of gestation). With a developed healthcare system and proper care, such children almost always survive, and health problems rarely occur. nine0003
After childbirth
After preterm birth, it is necessary to find out their cause, for this various additional examinations are carried out: microbiological studies, histological examination of the placenta, genetic examination, etc.
family planning center. Specialists examine both spouses, advise them, and, if necessary, prepare them for further pregnancy. nine0003
A few words about prevention
Is it possible to avoid preterm birth? In any case, the expectant mother can do what depends on her. Ideally, you need to prepare for pregnancy in advance, fully engaging in pregravid preparation: undergo all the necessary examinations, if there are any diseases, then cure them, or at least carry out the necessary correction so that the pregnancy proceeds with the least complications. It is very important to sanitize all foci of infection, including carious teeth. Strengthen immunity. And of course a healthy lifestyle in general. nine0003
It is very important to sanitize all foci of infection, including carious teeth. Strengthen immunity. And of course a healthy lifestyle in general. nine0003
Obstetrician-gynecologist Pekareva E.P.
Preterm birth | Shchelkovsky perinatal center
What is preterm birth?
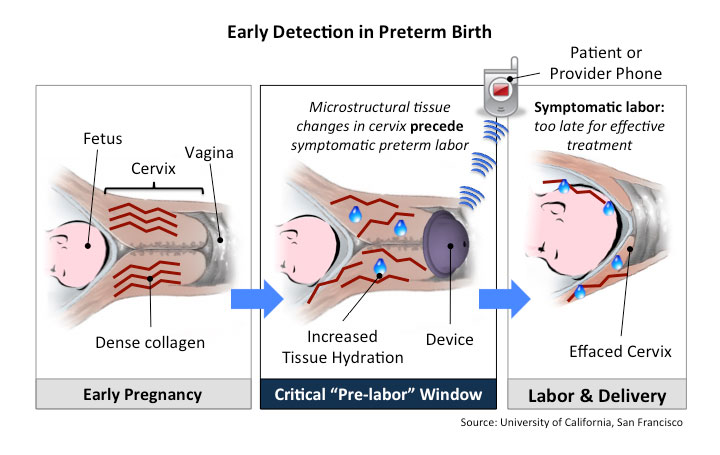
Prematurity is defined as regular uterine contractions resulting in changes in the cervix that begin before 37 weeks of gestation. Changes in the cervix include flattening (the cervix shortens) and dilatation (the cervix opens, allowing the fetus to enter the birth canal). nine0003
Why is preterm birth a concern?
Preterm birth is a major medical and social problem because babies who are born “too early” are not developed enough for extrauterine life. They may be born with serious health problems. Some health problems, such as cerebral palsy, can last a lifetime. Other problems, such as learning disabilities, may appear later in childhood or even into adulthood. nine0003
nine0003
Which premature babies are most at risk of health problems?
The risk of health problems is greatest for babies born before 34 weeks of gestation. However, babies born between 34 and 37 weeks of gestation are also at risk.
What are the risk factors for preterm birth?
Factors that increase the risk of preterm birth include the following: having an early preterm birth, a short cervix, a short interval between pregnancies, a history of certain types of uterine or cervical surgery, some pregnancy complications such as multiple pregnancies, and having history of bleeding, lifestyle factors such as low body weight before pregnancy, smoking during pregnancy, and substance abuse during pregnancy
Is there anything I can do to prevent preterm labor if I am at high risk?
If you have had a preterm birth and are planning another pregnancy, preconception examination (before conception). When you become pregnant, from the earliest dates it is necessary to be observed by an obstetrician-gynecologist.