Risks of ecv
What Is It, Procedure, Risks, Labor, & More
External Cephalic Version: What Is It, Procedure, Risks, Labor, & MoreMedically reviewed by Holly Ernst, PA-C — By Becky Young on April 12, 2018
What is external cephalic version?
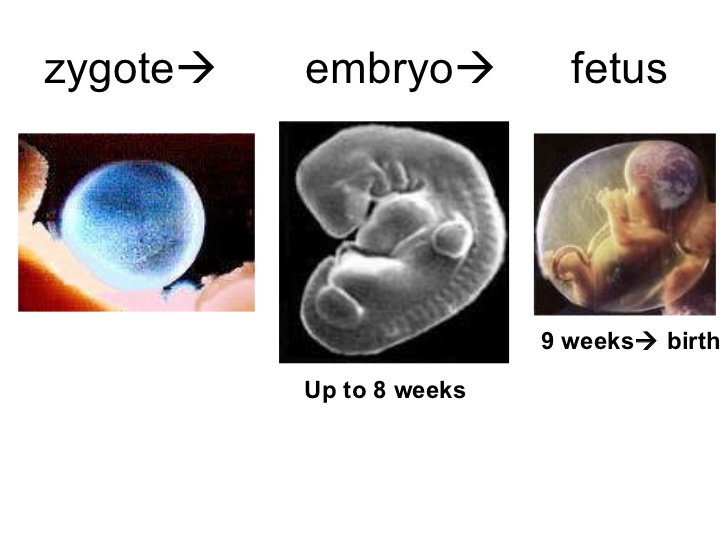
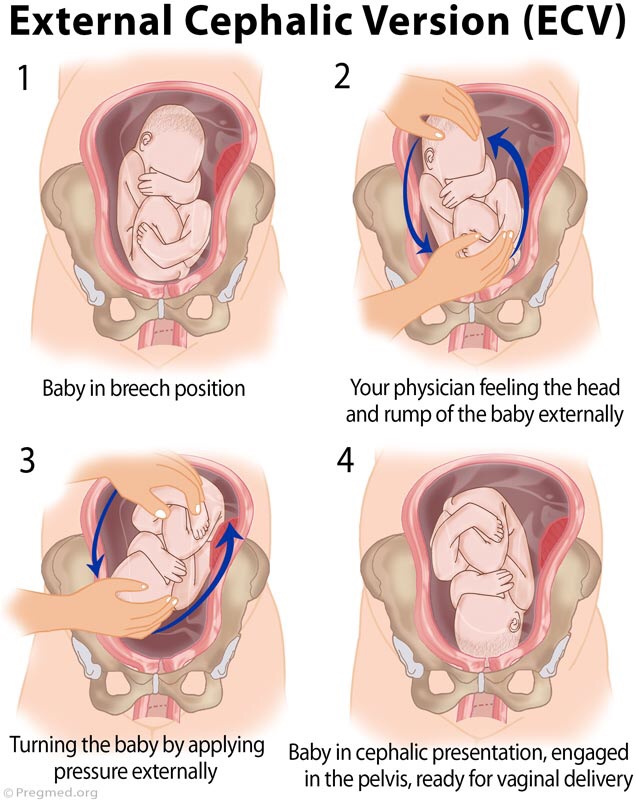
An external cephalic version is a procedure used to help turn a baby in the womb before delivery. During the procedure, your healthcare provider places their hands on the outside of your belly and attempts to manually turn the baby.
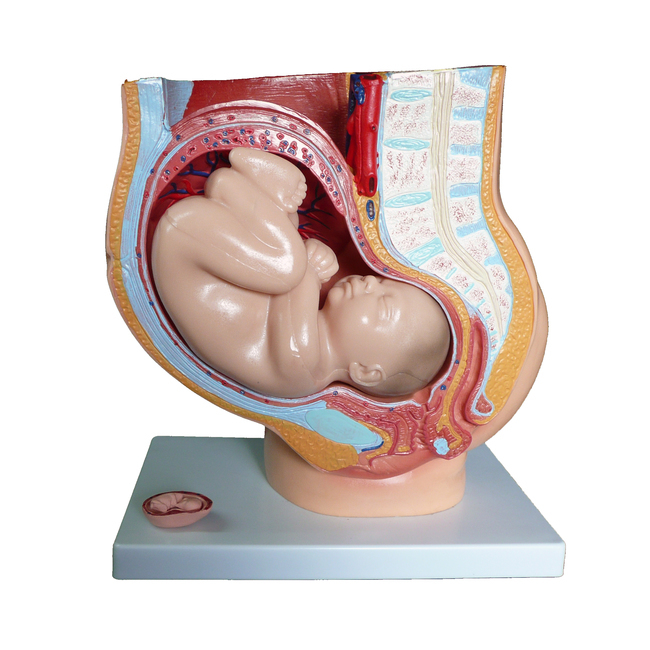
This procedure may be recommended if your baby is in a breech position. This means that their bottom or feet are pointing down toward the vagina, and their head is at the top of your uterus, near your rib cage. A vaginal breech birth is more complicated than a birth where the baby is head down, so it’s preferable that baby is head down before labor starts.
Some women opt to birth their babies via cesarean delivery (C-section) rather than attempt a vaginal breech birth if they’re near or past their estimated due date and the baby still hasn’t turned.
Is it safe?
Most women who are 37 weeks pregnant with a baby in the breech position are candidates for an external cephalic version. The procedure has been found to be successful in turning these babies into a head-down position in around 50 percent of cases. Since breech babies often result in C-sections, a successful external cephalic version may reduce your need for this type of delivery, which is considered an abdominal surgery.
There are some situations in which your healthcare providers may suggest an external cephalic version isn’t right for you. This procedure may not be right for you if:
- you’re already in labor or experiencing any vaginal bleeding
- you’ve had any issues with your placenta during the pregnancy
- there are signs of or concerns for fetal distress
- you are pregnant with more than one baby, such as twins or triplets
- you have any structural abnormalities in your uterus, like large fibroids
Your healthcare provider may also advise against the procedure if you’ve had a previous C-section, your baby is suspected to be larger than average, or you have low or high levels of amniotic fluid. These risk factors are based upon clinical opinion, so you should talk with your healthcare provider to see what they recommend based on your individual pregnancy.
These risk factors are based upon clinical opinion, so you should talk with your healthcare provider to see what they recommend based on your individual pregnancy.
You discuss external cephalic version between 34 and 37 weeks of pregnancy with your doctor if your baby is noted to be breech. Babies often turn on their own before 34 weeks, so there is no need to attempt the procedure earlier in the pregnancy.
The procedure does increase your risk for premature labor and fetal distress. For that reason, most healthcare providers recommend waiting until you’re at term, or 37 weeks pregnant, to attempt this procedure. That reduces risk for complications in your baby if you do need to deliver shortly following the procedure.
You can also talk with your doctor about waiting past 37 weeks, as the baby may spontaneously turn to a head-down position.
The most common risk with an external cephalic version is a temporary change in your baby’s heart rate, which occurs in about 5 percent of cases. Serious complications are extremely rare but can include the need for emergency C-section, vaginal bleeding, loss of amniotic fluid, and umbilical cord prolapse.
Serious complications are extremely rare but can include the need for emergency C-section, vaginal bleeding, loss of amniotic fluid, and umbilical cord prolapse.
What to expect during the procedure
The procedure will normally be performed by an obstetrician. During an external cephalic version, your doctor will place their hand on your belly to physically push the baby into the optimal position. The procedure usually takes around 5 minutes and your baby’s heart rate will be monitored before, during, and after the procedure. If your doctor suspects your baby isn’t responding well to the procedure, it will be stopped.
Many women report that the procedure is uncomfortable, but medications can be used to reduce the amount of pain felt. Using certain medications during the procedure may also increase the chances of successfully turning the baby. This may be because the medication helps your muscles and uterus relax, allowing the healthcare provider to successfully turn the baby more easily.
How will this procedure affect labor and delivery?
If an external cephalic version is successful, then most of the time labor progresses in a regular way following the procedure. The procedure doesn’t generally affect the length of your labor.
There is a small risk that the procedure will rupture membranes e. This can mean that you will begin labor earlier than you might otherwise have done, and your contractions may be more intense from the beginning of labor instead of building in intensity as the labor progresses.
If the procedure is unsuccessful and your baby remains in the breech position, you could opt for a C-section or choose to attempt a vaginal breech delivery.
One of the main risks involved with a vaginal breech delivery is that your baby’s head could become trapped in the birth canal. The other serious concern is umbilical cord prolapse. With umbilical cord prolapse, the umbilical cord leaves your body before your baby. That increases the risk of the cord becoming compressed during delivery, which cuts off the baby’s supply of oxygen and nutrients.
Both of these complications are a medical emergency. Evidence does show an increased risk of perinatal mortality in planned vaginal breech birth as opposed to a C-section with breech presentation.
Are there other ways to turn the baby?
There are a number of different exercises you can try to attempt to turn your baby from the breech position, though these haven’t been proven in studies to be effective in spontaneously turning the breech baby. Always talk to your healthcare provider before trying these exercises to make sure that they are safe for your pregnancy.
Hip tilt
- Lie on the floor in front of a sofa or chair, with your feet on the sofa or chair. Place cushions under your hips to offer additional support. Your hips should be elevated about 1.5 feet above your head, and your body should be at a 45-degree angle.
- Hold this position for 10 to 15 minutes, three times a day. It’s best to do this when your baby is active.
Pelvic rotations
- Stand or sit on an exercise or birthing ball.

- Once you are in position, gently rotate your hips clockwise in a circular movement. Repeat 10 rotations.
- Switch directions, rotating your hips counterclockwise for 10 rotations.
- Repeated three times a day
Rocking back and forth
- Place your hands and knees on the floor.
- Keeping your hands and knees in place, gently rock your body back and forth.
- Do this for 15 minutes. Repeat up to three times a day.
Walk or swim
- Walk, swim, or engage in another low-impact exercise.
- Do this for 30 minutes a day. Staying active may help your baby move out of the breech position.
The takeaway
It’s recommended that an external cephalic version be offered to all women who have a baby in breech position at or close to term, where there are no other complications. The procedure has been shown to be successful in around half of all cases and may lower the likelihood that a C-section will be needed. There are some possible risks, so be sure to discuss the risks and benefits with your healthcare provider before moving forward with this procedure.
There are some possible risks, so be sure to discuss the risks and benefits with your healthcare provider before moving forward with this procedure.
Last medically reviewed on April 12, 2018
- Parenthood
- Pregnancy
- 3rd Trimester
How we reviewed this article:
Healthline has strict sourcing guidelines and relies on peer-reviewed studies, academic research institutions, and medical associations. We avoid using tertiary references. You can learn more about how we ensure our content is accurate and current by reading our editorial policy.
- Berhan Y, et al. (2015). The risks of planned vaginal breech delivery versus planned caesarean section for term breech birth: A meta-analysis including observational studies. DOI:
10.1111/1471-0528.13524 - Grootscholten K, et al. (2008). External cephalic version-related risks: A meta-analysis [Abstract]. DOI:
10. 1097/AOG.0b013e31818b4ade
1097/AOG.0b013e31818b4ade - Kathpalia BSK, et al. (2012). Outcome of external cephalic version in breech presentation. DOI:
10.1016/S0377-1237(12)60036-7 - Kuppens SM, et al. (2017). Fetal heart rate abnormalities during and after external cephalic version: Which fetuses are at risk and how are they delivered? DOI:
10.1186/s12884-017-1547-6 - Lim PS, et al. (2014). Successful external cephalic version: Factors predicting vaginal birth. DOI:
10.1155/2014/860107 - Wang Z-H, et al. (2017). Remifentanil analgesia during external cephalic version for breech presentation in nulliparous women at term: A randomized controlled trial. DOI:
10.1097/MD.0000000000006256 - What happens if your baby is breech? (2017).
nhs.uk/conditions/pregnancy-and-baby/breech-birth/
Share this article
Medically reviewed by Holly Ernst, PA-C — By Becky Young on April 12, 2018
related stories
What Is Back Labor and What Causes It?
Can You Turn a Transverse Baby?
What You Need to Know If Your Baby Is in an Oblique Lie
Is It Safe to Use Exercise to Induce Labor?
How Early Can You Safely Give Birth?
Read this next
What Is Back Labor and What Causes It?
Medically reviewed by Valinda Riggins Nwadike, MD, MPH
Back labor can happen when your baby's head is against your cervix.
 We'll tell you what it's like and how to manage it.
We'll tell you what it's like and how to manage it.READ MORE
Can You Turn a Transverse Baby?
Medically reviewed by Valinda Riggins Nwadike, MD, MPH
As you near the end of your pregnancy, you may worry that your baby's transverse position will cause issues during delivery. Learn more about possible…
READ MORE
What You Need to Know If Your Baby Is in an Oblique Lie
Medically reviewed by Valinda Riggins Nwadike, MD, MPH
An oblique lie is a fetal position in which baby's head is just to the side of the pelvic inlet. It presents some challenges, but there are ways to…
READ MORE
Is It Safe to Use Exercise to Induce Labor?
Medically reviewed by Michael Weber, MD
If you’re pregnant and past your due date, you might wonder if exercising will help induce labor.
 Here’s the truth.
Here’s the truth. READ MORE
How Early Can You Safely Give Birth?
Medically reviewed by Meredith Wallis, MS, APRN, CNM, IBCLC
Not all babies arrive on their due dates — in fact, most don't. So how many weeks early is safe to give birth? Learn more about why certain weeks are…
READ MORE
Can Ectopic Pregnancy Be Diagnosed With Ultrasound?
Medically reviewed by Valinda Riggins Nwadike, MD, MPH
Ectopic pregnancy is a serious condition that requires accurate and swift diagnosis. Ultrasound for ectopic pregnancy diagnosis is just one tool your…
READ MORE
Is It Safe to Consume Flaxseeds During Pregnancy?
Given the inconclusive and conflicting stances about eating flaxseeds during pregnancy, it might be better to err on the side of caution.
READ MORE
Pregnancy After Miscarriage: Answers to Your Questions
Medically reviewed by Amanda Kallen, MD
Getting pregnant after a miscarriage can be an emotional experience, filled with joy but also anxiety and guilt. Learn more about pregnancy after…
READ MORE
What Is a Nurse Midwife and How to Tell If They Are Right for You
Medically reviewed by Meredith Wallis, MS, APRN, CNM, IBCLC
A nurse midwife is a nurse with education, training, and certification to provide prenatal, delivery, and women's care.
READ MORE
Your 6-Week Ultrasound: What to Expect
Medically reviewed by Valinda Riggins Nwadike, MD, MPH
We'll tell you all about the 6-week ultrasound, including why your doctor may have ordered it, what the risks are, and what it means if no heartbeat…
READ MORE
What Is It, Procedure, Risks, Labor, & More
External Cephalic Version: What Is It, Procedure, Risks, Labor, & MoreMedically reviewed by Holly Ernst, PA-C — By Becky Young on April 12, 2018
What is external cephalic version?
An external cephalic version is a procedure used to help turn a baby in the womb before delivery. During the procedure, your healthcare provider places their hands on the outside of your belly and attempts to manually turn the baby.
During the procedure, your healthcare provider places their hands on the outside of your belly and attempts to manually turn the baby.
This procedure may be recommended if your baby is in a breech position. This means that their bottom or feet are pointing down toward the vagina, and their head is at the top of your uterus, near your rib cage. A vaginal breech birth is more complicated than a birth where the baby is head down, so it’s preferable that baby is head down before labor starts.
Some women opt to birth their babies via cesarean delivery (C-section) rather than attempt a vaginal breech birth if they’re near or past their estimated due date and the baby still hasn’t turned.
Is it safe?
Most women who are 37 weeks pregnant with a baby in the breech position are candidates for an external cephalic version. The procedure has been found to be successful in turning these babies into a head-down position in around 50 percent of cases. Since breech babies often result in C-sections, a successful external cephalic version may reduce your need for this type of delivery, which is considered an abdominal surgery.
There are some situations in which your healthcare providers may suggest an external cephalic version isn’t right for you. This procedure may not be right for you if:
- you’re already in labor or experiencing any vaginal bleeding
- you’ve had any issues with your placenta during the pregnancy
- there are signs of or concerns for fetal distress
- you are pregnant with more than one baby, such as twins or triplets
- you have any structural abnormalities in your uterus, like large fibroids
Your healthcare provider may also advise against the procedure if you’ve had a previous C-section, your baby is suspected to be larger than average, or you have low or high levels of amniotic fluid. These risk factors are based upon clinical opinion, so you should talk with your healthcare provider to see what they recommend based on your individual pregnancy.
You discuss external cephalic version between 34 and 37 weeks of pregnancy with your doctor if your baby is noted to be breech. Babies often turn on their own before 34 weeks, so there is no need to attempt the procedure earlier in the pregnancy.
The procedure does increase your risk for premature labor and fetal distress. For that reason, most healthcare providers recommend waiting until you’re at term, or 37 weeks pregnant, to attempt this procedure. That reduces risk for complications in your baby if you do need to deliver shortly following the procedure.
You can also talk with your doctor about waiting past 37 weeks, as the baby may spontaneously turn to a head-down position.
The most common risk with an external cephalic version is a temporary change in your baby’s heart rate, which occurs in about 5 percent of cases. Serious complications are extremely rare but can include the need for emergency C-section, vaginal bleeding, loss of amniotic fluid, and umbilical cord prolapse.
What to expect during the procedure
The procedure will normally be performed by an obstetrician. During an external cephalic version, your doctor will place their hand on your belly to physically push the baby into the optimal position. The procedure usually takes around 5 minutes and your baby’s heart rate will be monitored before, during, and after the procedure. If your doctor suspects your baby isn’t responding well to the procedure, it will be stopped.
Many women report that the procedure is uncomfortable, but medications can be used to reduce the amount of pain felt. Using certain medications during the procedure may also increase the chances of successfully turning the baby. This may be because the medication helps your muscles and uterus relax, allowing the healthcare provider to successfully turn the baby more easily.
How will this procedure affect labor and delivery?
If an external cephalic version is successful, then most of the time labor progresses in a regular way following the procedure. The procedure doesn’t generally affect the length of your labor.
There is a small risk that the procedure will rupture membranes e. This can mean that you will begin labor earlier than you might otherwise have done, and your contractions may be more intense from the beginning of labor instead of building in intensity as the labor progresses.
If the procedure is unsuccessful and your baby remains in the breech position, you could opt for a C-section or choose to attempt a vaginal breech delivery.
One of the main risks involved with a vaginal breech delivery is that your baby’s head could become trapped in the birth canal. The other serious concern is umbilical cord prolapse. With umbilical cord prolapse, the umbilical cord leaves your body before your baby. That increases the risk of the cord becoming compressed during delivery, which cuts off the baby’s supply of oxygen and nutrients.
Both of these complications are a medical emergency. Evidence does show an increased risk of perinatal mortality in planned vaginal breech birth as opposed to a C-section with breech presentation.
Are there other ways to turn the baby?
There are a number of different exercises you can try to attempt to turn your baby from the breech position, though these haven’t been proven in studies to be effective in spontaneously turning the breech baby. Always talk to your healthcare provider before trying these exercises to make sure that they are safe for your pregnancy.
Hip tilt
- Lie on the floor in front of a sofa or chair, with your feet on the sofa or chair. Place cushions under your hips to offer additional support. Your hips should be elevated about 1.5 feet above your head, and your body should be at a 45-degree angle.
- Hold this position for 10 to 15 minutes, three times a day. It’s best to do this when your baby is active.
Pelvic rotations
- Stand or sit on an exercise or birthing ball.
- Once you are in position, gently rotate your hips clockwise in a circular movement. Repeat 10 rotations.
- Switch directions, rotating your hips counterclockwise for 10 rotations.

- Repeated three times a day
Rocking back and forth
- Place your hands and knees on the floor.
- Keeping your hands and knees in place, gently rock your body back and forth.
- Do this for 15 minutes. Repeat up to three times a day.
Walk or swim
- Walk, swim, or engage in another low-impact exercise.
- Do this for 30 minutes a day. Staying active may help your baby move out of the breech position.
The takeaway
It’s recommended that an external cephalic version be offered to all women who have a baby in breech position at or close to term, where there are no other complications. The procedure has been shown to be successful in around half of all cases and may lower the likelihood that a C-section will be needed. There are some possible risks, so be sure to discuss the risks and benefits with your healthcare provider before moving forward with this procedure.
Last medically reviewed on April 12, 2018
- Parenthood
- Pregnancy
- 3rd Trimester
How we reviewed this article:
Healthline has strict sourcing guidelines and relies on peer-reviewed studies, academic research institutions, and medical associations. We avoid using tertiary references. You can learn more about how we ensure our content is accurate and current by reading our editorial policy.
We avoid using tertiary references. You can learn more about how we ensure our content is accurate and current by reading our editorial policy.
- Berhan Y, et al. (2015). The risks of planned vaginal breech delivery versus planned caesarean section for term breech birth: A meta-analysis including observational studies. DOI:
10.1111/1471-0528.13524 - Grootscholten K, et al. (2008). External cephalic version-related risks: A meta-analysis [Abstract]. DOI:
10.1097/AOG.0b013e31818b4ade - Kathpalia BSK, et al. (2012). Outcome of external cephalic version in breech presentation. DOI:
10.1016/S0377-1237(12)60036-7 - Kuppens SM, et al. (2017). Fetal heart rate abnormalities during and after external cephalic version: Which fetuses are at risk and how are they delivered? DOI:
10.1186/s12884-017-1547-6 - Lim PS, et al. (2014). Successful external cephalic version: Factors predicting vaginal birth.
 DOI:
DOI:
10.1155/2014/860107 - Wang Z-H, et al. (2017). Remifentanil analgesia during external cephalic version for breech presentation in nulliparous women at term: A randomized controlled trial. DOI:
10.1097/MD.0000000000006256 - What happens if your baby is breech? (2017).
nhs.uk/conditions/pregnancy-and-baby/breech-birth/
Share this article
Medically reviewed by Holly Ernst, PA-C — By Becky Young on April 12, 2018
related stories
What Is Back Labor and What Causes It?
Can You Turn a Transverse Baby?
What You Need to Know If Your Baby Is in an Oblique Lie
Is It Safe to Use Exercise to Induce Labor?
How Early Can You Safely Give Birth?
Read this next
What Is Back Labor and What Causes It?
Medically reviewed by Valinda Riggins Nwadike, MD, MPH
Back labor can happen when your baby's head is against your cervix.
 We'll tell you what it's like and how to manage it.
We'll tell you what it's like and how to manage it.READ MORE
Can You Turn a Transverse Baby?
Medically reviewed by Valinda Riggins Nwadike, MD, MPH
As you near the end of your pregnancy, you may worry that your baby's transverse position will cause issues during delivery. Learn more about possible…
READ MORE
What You Need to Know If Your Baby Is in an Oblique Lie
Medically reviewed by Valinda Riggins Nwadike, MD, MPH
An oblique lie is a fetal position in which baby's head is just to the side of the pelvic inlet. It presents some challenges, but there are ways to…
READ MORE
Is It Safe to Use Exercise to Induce Labor?
Medically reviewed by Michael Weber, MD
If you’re pregnant and past your due date, you might wonder if exercising will help induce labor.
 Here’s the truth.
Here’s the truth. READ MORE
How Early Can You Safely Give Birth?
Medically reviewed by Meredith Wallis, MS, APRN, CNM, IBCLC
Not all babies arrive on their due dates — in fact, most don't. So how many weeks early is safe to give birth? Learn more about why certain weeks are…
READ MORE
Can Ectopic Pregnancy Be Diagnosed With Ultrasound?
Medically reviewed by Valinda Riggins Nwadike, MD, MPH
Ectopic pregnancy is a serious condition that requires accurate and swift diagnosis. Ultrasound for ectopic pregnancy diagnosis is just one tool your…
READ MORE
Is It Safe to Consume Flaxseeds During Pregnancy?
Given the inconclusive and conflicting stances about eating flaxseeds during pregnancy, it might be better to err on the side of caution.

READ MORE
Pregnancy After Miscarriage: Answers to Your Questions
Medically reviewed by Amanda Kallen, MD
Getting pregnant after a miscarriage can be an emotional experience, filled with joy but also anxiety and guilt. Learn more about pregnancy after…
READ MORE
What Is a Nurse Midwife and How to Tell If They Are Right for You
Medically reviewed by Meredith Wallis, MS, APRN, CNM, IBCLC
A nurse midwife is a nurse with education, training, and certification to provide prenatal, delivery, and women's care.
READ MORE
Your 6-Week Ultrasound: What to Expect
Medically reviewed by Valinda Riggins Nwadike, MD, MPH
We'll tell you all about the 6-week ultrasound, including why your doctor may have ordered it, what the risks are, and what it means if no heartbeat…
READ MORE
Efficiency of on-line hemodiafiltration in chronic kidney disease: risk factors and improvement in the assessment of fluid excretion rates | Zarya
1. Rybakova OB, Denisov AYu, Shilo VYu. Hemodiafiltration in the treatment of end-stage renal disease. Nephrology and dialysis 2001; 3(4): 406–410 Rybakova OB, Denisov AYu, Shilo VYu. Hemodiafiltration in the treatment of end-stage renal failure. Nephrology and dialysis 2001; 3(4): 406–410
Rybakova OB, Denisov AYu, Shilo VYu. Hemodiafiltration in the treatment of end-stage renal disease. Nephrology and dialysis 2001; 3(4): 406–410 Rybakova OB, Denisov AYu, Shilo VYu. Hemodiafiltration in the treatment of end-stage renal failure. Nephrology and dialysis 2001; 3(4): 406–410
2. Poz YaL, Strokov AG, Kopylova YuV. Hemodiafiltration. History, development and modern standards. Bulletin of Transplantology and Artificial Organs 2014;16(1):54–64. doi: 10.15825/1995-1191-2014-1-54-64 Poz YaL, Strokov AG, Kopylova YuV. Hemodiafiltration. History, development and modern standards. Bulletin of transplantology and artificial organs 2014;16(1):54–64. doi: 10.15825/1995-1191-2014-1-54-64
3. Lin CL, Yang CW, Chiang CC et al. Long-term on-line hemodiafiltration reduces predialysis beta-2-microglobulin levels in chronic hemodialysis patients. Blood Purif 2001;19(3):301–307. doi: 10.1159/000046958
4. Lornoy W, Becaus I, Billiouw JM et al. On-line haemodiafiltration. Remarkable removal of beta2-microglobulin. Long-term clinical observations. Nephrol Dial Transplant 2000;15 Suppl 1:49-54. doi: 10.1093/oxfordjournals.ndt.a027964
Remarkable removal of beta2-microglobulin. Long-term clinical observations. Nephrol Dial Transplant 2000;15 Suppl 1:49-54. doi: 10.1093/oxfordjournals.ndt.a027964
5. Pedrini LA, De Cristofaro V, Comelli M et al. Long-term effects of high-efficiency on-line haemodiafiltration on uraemic toxicity. A multicentre prospective randomized study. Nephrol Dial Transplant 2011 Aug;26(8):2617–2624. doi: 10.1093/ndt/gfq761
6. Penne EL, van der Weerd NC, Blankestijn PJ et al. Role of residual kidney function and convective volume on change in beta2-microglobulin levels in hemodiafiltration patients. Clin J Am Soc Nephrol 2010 Jan;5(1):80–86. doi: 10.2215/CJN.03340509
7. Baldamus CA, Pollok M. (1989) Ultrafiltration and Hemofiltration: Practical Applications. In: Maher J.F. (eds) Replacement of Renal Function by Dialysis. Springer, Dordrecht. doi: 10.1007/978-94-009-1087-4_14
8. Maduel F, del Pozo C, Garsia H et al. Change from conventional haemodiafiltration to on-line haemodiafiltration. Nephrol Dial Transplant 1999 May;14(5):1202–1207. doi: 10.1093/ndt/14.5.1202
Nephrol Dial Transplant 1999 May;14(5):1202–1207. doi: 10.1093/ndt/14.5.1202
9. Odell RA, Slowiachek P, Moran JE et al. Beta 2-microglobulin kinetics in end-stage renal failure. Kidney Int 1991 May;39(5):909–919. doi: 10.1038/ki.1991.114
10. Ahrenholz P, Wincler RE, Ramlow W et al. On-line hemodiafiltration with pre- and postdilution: a comparison of efficacy. Int J Artif Organs 1997 Feb;20(2):81–90
11. Bowry SK, Gatti E. Impact of hemodialysis therapy on anemia of chronic kidney disease: the potential mechanisms. Blood Purif 2011;32(3):210–219. doi: 10.1159/000329573
12. Vaslaki L, Major L, Berta K et al. On-line haemodiafiltration versus haemodialysis: stable haematocrit with less erythropoietin and improvement of other relevant blood parameters. Blood Purif 2006;24(2):163–173. doi: 10.1159/0000
13. Locatelli F, Manzoni C, Del Vecchio L et al. Management of anemia by convective treatments. Contrib Nephrol 2011;168:162–172. doi: 10.1159/000321757
14. Grillo P, Bonforte G, Bagaretty I, Scanziani R et al. Haemodiafiltration with substitution of fluid prepared on line decreases rHuEPO consumption. Nephrol Dial Transplant 1999; fourteen; A207
Grillo P, Bonforte G, Bagaretty I, Scanziani R et al. Haemodiafiltration with substitution of fluid prepared on line decreases rHuEPO consumption. Nephrol Dial Transplant 1999; fourteen; A207
15. Bonforte G, Grillo P, Zerbi S, Surian M. Improvement of anemia in hemodialysis patients treated by hemodiafiltration with high-volume on-line-prepared substitution fluid. Blood Purif 2002; 20(4):357–363. doi: 10.1159/000063104
16. Lornoy W, De Meester J, Becaus I et al. Impact of convective flow on phosphorus removal in maintenance hemodialysis patients. J Ren Nutr 2006 Jan;16(1):47–53. doi: 10.1053/j.jrn.2005.10.008
17. Davenport A, Gardner C, Delaney M. The effect of dialysis modality on phosphate control: haemodialysis compared to haemodiafiltration. The Pan Thames Renal Audit. Nephrol Dial Transplant 2010 Mar;25(3):897–901. doi: 10.1093/ndt/gfp560
18. Penne EL, van der Weerd NC, van den Dorpel MA et al. Short-term effects of online hemodiafiltration on phosphate control: a result from the randomized controlled Convective Transport Study (CONTRAST). Am J Kidney Dis 2010 Jan;55(1):77–87. doi:10.1053/j.ajkd.2009.09.023
Am J Kidney Dis 2010 Jan;55(1):77–87. doi:10.1053/j.ajkd.2009.09.023
19. Wanner C, Bahner U, Mattern R et al. Effect of dialysis flux and membrane material on dyslipidaemia and inflammation in haemodialysis patients. Nephrol Dial Transplant 2004 Oct;19(10):2570-2575. doi: 10.1093/ndt/gfh515
20. Schiffl H, Lang SM. Effects of dialysis purity on uremic dyslipidemia. Ther Apher Dial 2010 Feb;14(1):5–11. doi: 10.1111/j.1744-9987.2009.00713.x
21. Panichi V, Rizza GM, Paoletti S et al. Chronic inflammation and mortality in haemodialysis: effect of different renal replacement therapies. Results from the RISCAVID study. Nephrol Dial Transplant 2008 Jul;23(7):2337–2343. doi: 10.1093/ndt/gfm951
22. Ramírez R, Martín-Malo A, Aljama P. Evolution of the concept of biocompatibility and the cardioprotective effect of on-line hemodiafiltration. Contrib Nephrol 2011;175:110–116. doi: 10.1159/000333294
23. Filiopoulos V, Hadjiyannakos D, Metaxaki P et al. Inflammation and oxidative stress in patients on hemodiafiltration. Am J Nephrol 2008;28(6):949–957. doi: 10.1159/000142724
Am J Nephrol 2008;28(6):949–957. doi: 10.1159/000142724
24. Masakane I. Choice of modality with the use of highperformance membrane and evaluation for clinical effects. Contrib Nephrol 2011;173:84–94. doi: 10.1159/000328959
25. Gatti E, Ronco C. Seeking an optimal renal replacement therapy for the chronic kidney disease epidemic: the case for on-line hemodiafiltration. Contrib Nephrol. 2011;175:170–185. doi: 10.1159/000333636
26. Canaud B, Bragg-Gresham JL, Marshall MR et al. Mortality risk for patients receiving hemodiafiltration versus hemodialysis: European results from the DOPPS. Kidney Int 2006 Jun; 69(11):2087–2093. doi: 10.1038/sj.ki.5000447
27. Penne EL, van der Weerd NC, Bots ML et al. Patient- and treatment-related determinants of convective volume in post-dilution haemodiafiltration in clinical practice. Nephrol Dial Transplant 2009Nov;24(11):3493–3499. doi: 10.1093/ndt/gfp265
28. Grooteman MP, van de Dorpel MA, Bots ML et al. Effect of online hemodiafiltration on all-cause mortality and cardiovascular outcomes. J Am Soc Nephrol 2012 Jun;23(6):1087–1096. doi: 10.1681/ASN.2011121140
J Am Soc Nephrol 2012 Jun;23(6):1087–1096. doi: 10.1681/ASN.2011121140
29. Ok E, Asci G, Ok ES et al. Mortality and cardiovascular events in online haemodiafiltration (OL-HDF) compared with highflux dialysis: results from the Turkish OL-HDF Study. Nephrol Dial Transplant 2013 Jan;28(1):192–202. doi: 10.1093/ndt/gfs407
30. Davenport A, Peters SA, Bots ML et al. Higher convection volume exchange with online hemodiafiltration is associated with survival advantage for dialysis patients: the effect of adjustment for body size. Kidney Int 2016 Jan;89(1):193–199. doi: 10.1038/ki.2015.264
31. Maduell F, Moreso F, Pons M et al. High-efficiency postdilution online hemodiafiltration reduces all-cause mortality in hemodialysis patients. J Am Soc Nephrol 2013 Feb;24(3):487–497. doi: 10.1681/ASN.2012080875
LLC ETsV, Moscow (TIN 7743006206), details, extract from the Unified State Register of Legal Entities, address, mail, website, telephone, financial indicators
Refresh browser
Refresh browser
Capabilities
Integration
About the system
Statistics
Contacts
CfDJ8HJyMSOWarhLkJBDZs2NT-GqjyN_Zpp7c-KQ3j-m9SEWCbhrwOE3q6ZSHtKK8z88aipliqSHEzcwfXRL7pH9FOMotXUyvTyWKXrTrZ9SKFBAnJo6gUicyr1TxStVNRNWAmoiFxnINAupelb2R6eThm4
Description of the search engine
search encyclopedia
TIN
OGRN
Sanction lists
Company search
Head of the organization
Court cases
Affiliation Check
Execution proceedings
Organization details
Information about the beneficiaries
Organization's current account
Credit risk assessment
Checking the blocking of the current account
Number of employees
Authorized capital of the organization
Bankruptcy check
Date of registration
Checking the counterparty by TIN
checkpoint
OKPO
Tenders and public procurement
Customer search (B2B)
Legal address
Analysis of the financial condition
Organization founders
Financial statements
OKTMO
OKVED
Company Comparison
Trademark Check
License check
Extract from the Unified State Register of Legal Entities
Competitor analysis
Organization website
OKOPF
Registration Information
OKFS
Branches and representative offices
OKOGU
OKATO
Register of dishonest suppliers
Company rating
Check yourself and the counterparty
due diligence
Banking licenses
Scoring of counterparties
Alcohol licenses
Media monitoring
Signs of economic activity
Reputational risks
Compliance
Company OOO ETsV, address: Moscow, per. Bolshoy Zlatoustinskiy, 6/6 bld. 3-4-5 office 202 was registered on 19.08.2002. The organization was assigned TIN 7743006206, PSRN 1027739081226, KPP 770101001. The main activity is the management of the operation of the housing stock for a fee or on a contractual basis, in total 11 types of activities are registered according to OKVED. There are no connections with other companies.
Bolshoy Zlatoustinskiy, 6/6 bld. 3-4-5 office 202 was registered on 19.08.2002. The organization was assigned TIN 7743006206, PSRN 1027739081226, KPP 770101001. The main activity is the management of the operation of the housing stock for a fee or on a contractual basis, in total 11 types of activities are registered according to OKVED. There are no connections with other companies.
Number of co-owners (according to the Unified State Register of Legal Entities): 1, general director - Lupova Maria Alexandrovna. The size of the authorized capital is 20,000 rubles.
ETsV LLC did not participate in tenders. 15 enforcement proceedings were initiated against the company. LLC ETsV did not participate in arbitration cases.
Details of LLC ETsV, legal address, official website and extract from the Unified State Register of Legal Entities are available in the SPARK system (demo access is free).
Full verification of counterparties in SPARK
- Unpaid debts
- Arbitration cases
- Communications
- Reorganizations and bankruptcy
- Other risk factors
Complete information about the company OOO ETsV
299₽
- Company registration data
- Manager and principal owners
- Contact information
- Risk factors
- Signs of economic activity
- Key financial indicators in dynamics
- Check according to the registers of the Federal Tax Service
Buy Example
999₽
Monitoring of changes for the year is enabled
- Company registration data
- History of changes in managers, names, addresses
- Full list of addresses, phone numbers, websites
- Details of co-owners from various sources
- Related companies
- Activity details
- Financial statements for several years
- Financial assessment
Buy Example
Is free
- Complete information report - SPARK PROFILE
- Adding contact details: phone, website, mail
- Adding a description of the company's activities
- Download logo
- Loading documents
Edit data
SPARK-Risks for 1C
Reliability assessment and monitoring of counterparties
Learn more
Application for demo access
Applications with corporate email are processed faster.