Placenta not working well
Placental insufficiency | Pregnancy Birth and Baby
Placental insufficiency | Pregnancy Birth and Baby beginning of content2-minute read
Listen
Sometimes the placenta does not work properly. This will mean the baby does not get the oxygen and nutrients they need. If you have placental insufficiency, your baby may not grow well or may develop complications during labour.
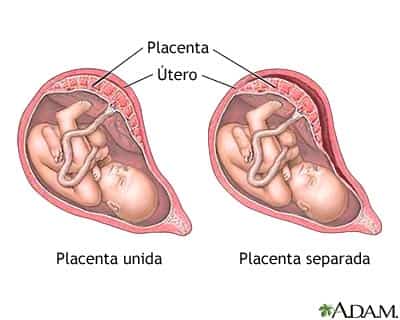
The condition can lead to problems both for mother and baby. It's linked to pre-eclampsia and placental abruption, when the placenta peels away from the wall of the uterus.
It can also prevent the baby from growing at a normal rate in the womb, known as intrauterine growth restriction (IUGR). There can be serious complications for the baby, including lack of oxygen during the birth, premature labour, low blood sugar, too little calcium in the blood, or too many red blood cells and sometimes even stillbirth.
What causes placental insufficiency?
Placental insufficiency occurs either because the placenta doesn’t grow properly, or because it’s damaged.
Sometimes the placenta may not grow to be big enough — for example, if you are carrying twins or more. Sometimes it has an abnormal shape or it doesn’t attach properly to the wall of the uterus.
Your lifestyle can also damage the placenta. Placental insufficiency can occur if you smoke or take some kinds of illegal drugs while you’re pregnant. Medical conditions such as diabetes, pre-eclampsia and blood clotting conditions also increase your risk.
What are the symptoms of placental insufficiency?
Placental insufficiency has no symptoms. Sometimes it’s diagnosed when women realise their baby isn’t moving as much. Other signs the baby may not be developing properly are that your abdomen is smaller than in previous pregnancies.
The condition may be picked up during your routine antenatal tests, which measure the growth of your uterus and the baby.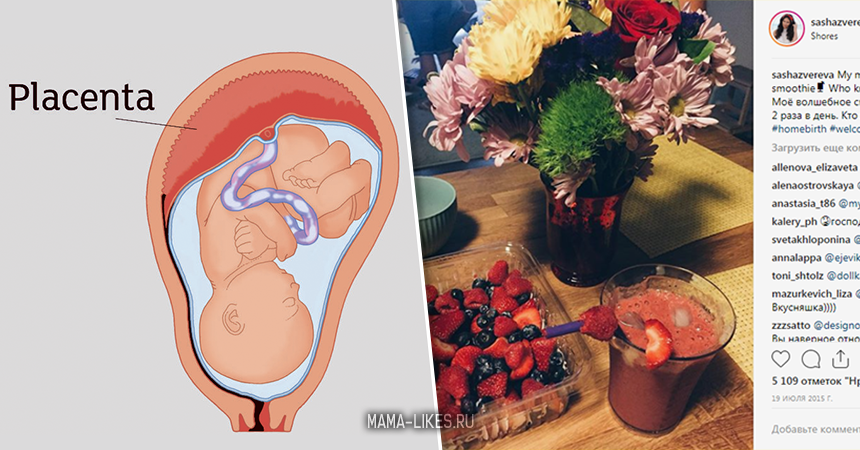 Sometimes it’s noticed during a routine ultrasound.
Sometimes it’s noticed during a routine ultrasound.
How is placental insufficiency treated?
If your doctor suspects placental insufficiency, they will keep a close eye on your baby's growth. You will be asked to keep a record of the baby's movements and let your medical team know if you notice any changes.
Treatment will depend on the stage of the pregnancy. If you’re under 37 weeks, your doctor may decide to wait for as long as possible and keep a close eye on the baby. But if you are full term or there are signs that your baby is under stress, they may decide to induce labour or deliver the baby with a caesarean.
Sources:
MedlinePlus (Placental insufficiency), Healthline (Placental insufficiency), Department of Health (Fetal growth restriction and well-being), RANZCOG (Intrauterine Growth Restriction: Screening, Diagnosis, and Management)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: February 2020
Back To Top
Related pages
- Placenta complications in pregnancy
- What is the placenta?
Need more information?
Placenta complications in pregnancy
The placenta develops inside the uterus during pregnancy and provides your baby with nutrients and oxygen. If something goes wrong, it can be serious.
Read more on Pregnancy, Birth & Baby website
What is the placenta?
The placenta is crucial to keeping your baby alive and well during pregnancy. Read more here.
Read more on Pregnancy, Birth & Baby website
Causes of Preterm Labour - Miracle Babies
There are many causes of preterm birth
Read more on Miracle Babies Foundation website
Causes - Miracle Babies
Every year in Australia around 48,000 newborn babies require the help of a NICU or SCN, there are many factors linked to premature birth and also many that remain unexplained
Read more on Miracle Babies Foundation website
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now entering.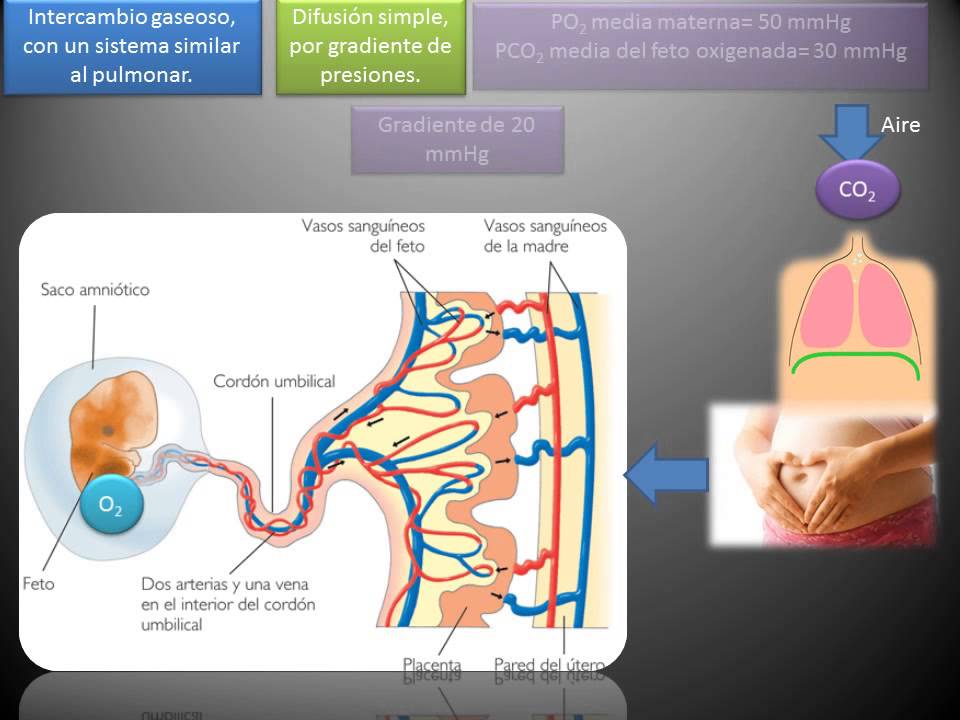
Need further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.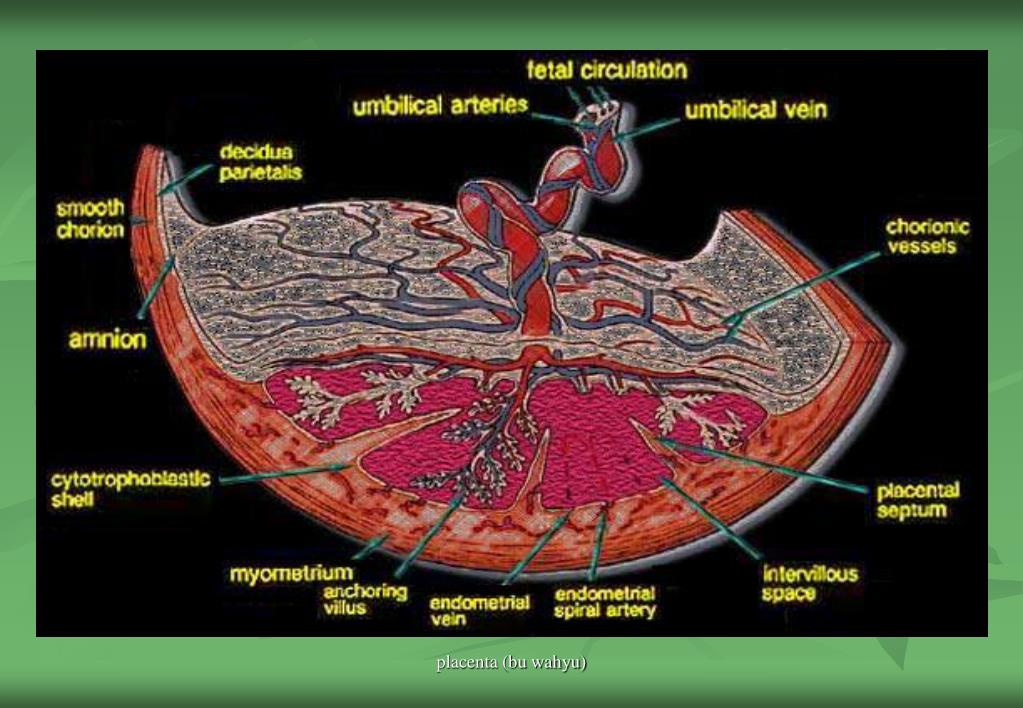
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
Placental Insufficiency: Causes, Symptoms, and Diagnosis
Placental Insufficiency: Causes, Symptoms, and DiagnosisMedically reviewed by Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT — By Sandy Calhoun Rice on January 8, 2018
Overview
The placenta is an organ that grows in the womb during pregnancy. Placental insufficiency (also called placental dysfunction or uteroplacental vascular insufficiency) is an uncommon but serious complication of pregnancy. It occurs when the placenta does not develop properly, or is damaged. This blood flow disorder is marked by a reduction in the mother’s blood supply. The complication can also occur when the mother’s blood supply doesn’t adequately increase by mid-pregnancy.
The complication can also occur when the mother’s blood supply doesn’t adequately increase by mid-pregnancy.
When the placenta malfunctions, it’s unable to supply adequate oxygen and nutrients to the baby from the mother’s bloodstream. Without this vital support, the baby cannot grow and thrive. This can lead to low birth weight, premature birth, and birth defects. It also carries increased risks of complications for the mother. Diagnosing this problem early is crucial to the health of both mother and baby.
Vital functions of the placenta
The placenta is a highly complex biological organ. It forms and grows where the fertilized egg attaches to the wall of the uterus.
The umbilical cord grows from the placenta to the baby’s navel. It allows blood to flow from mother to baby, and back again. The mother’s blood and the baby’s blood are filtered through the placenta, but they never actually mix.
The placenta’s primary jobs are to:
- move oxygen into the baby’s bloodstream
- carry carbon dioxide away
- pass nutrients to the baby
- transfer waste for disposal by the mother’s body
The placenta has an important role in hormone production as well.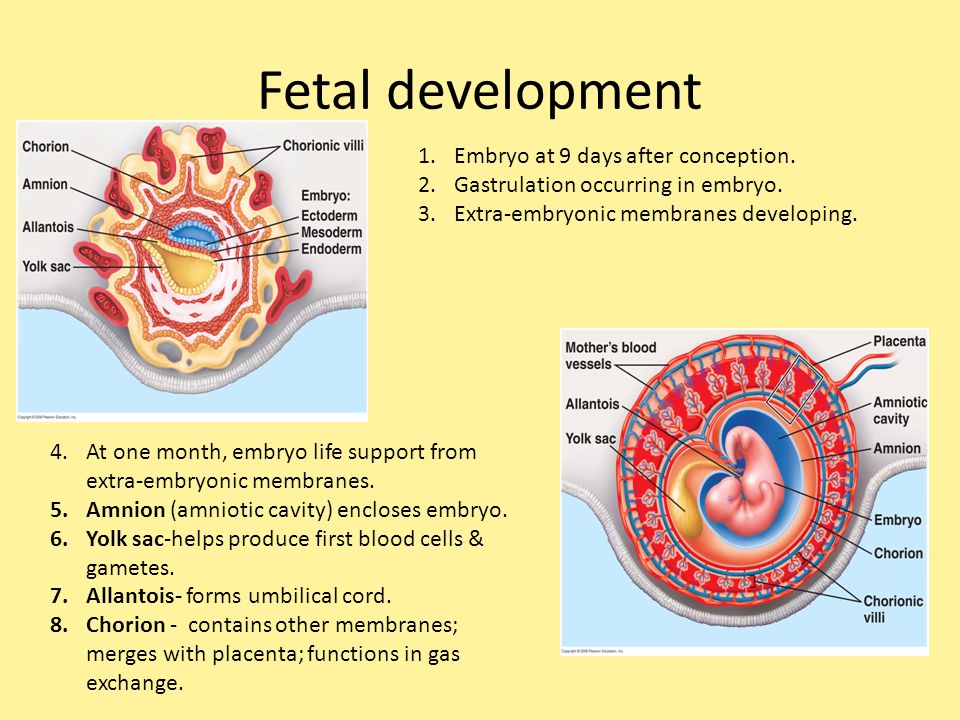 It also protects the fetus from harmful bacteria and infections.
It also protects the fetus from harmful bacteria and infections.
A healthy placenta continues to grow throughout the pregnancy. The American Pregnancy Association estimates that the placenta weighs 1 to 2 pounds at the time of birth.
The placenta is removed during labor. According to the Mayo Clinic, it’s delivered between 5 and 30 minutes after the baby.
Causes of insufficiency
Placental insufficiency is linked to blood flow problems. While maternal blood and vascular disorders can trigger it, medications and lifestyle habits are also possible triggers.
The most common conditions linked to placental insufficiency are:
- diabetes
- chronic high blood pressure (hypertension)
- blood clotting disorders
- anemia
- certain medications (particularly blood thinners)
- smoking
- drug abuse (especially cocaine, heroin, and methamphetamine)
Placental insufficiency may also occur if the placenta doesn’t attach properly to the uterine wall, or if the placenta breaks away from it (placental abruption).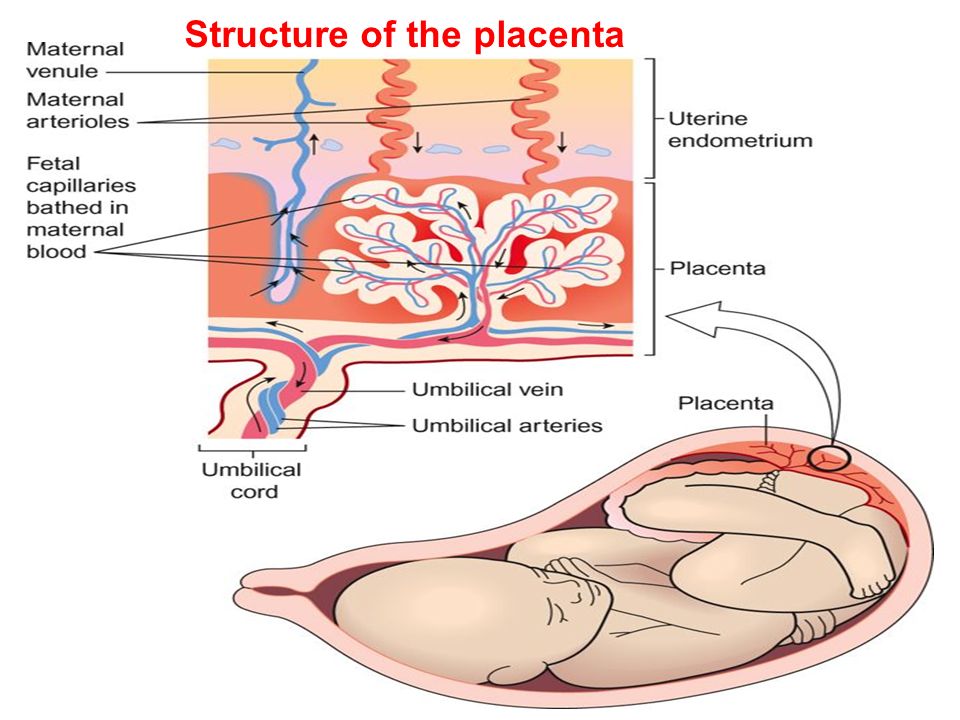
Symptoms
There are no maternal symptoms associated with placental insufficiency. However, certain clues can lead to early diagnosis. The mother may notice that the size of her uterus is smaller than in previous pregnancies. The fetus may also be moving less than expected.
If the baby isn’t growing properly, the mother’s abdomen will be small, and the baby’s movements will not be felt much.
Vaginal bleeding or preterm labor contractions may occur with placental abruption.
Complications
Mother
Placental insufficiency is not usually considered life-threatening to the mother. However, the risk is greater if the mother has hypertension or diabetes.
During pregnancy, the mother is more likely to experience:
- preeclampsia (elevated blood pressure and end-organ dysfunction)
- placental abruption (placenta pulls away from the uterine wall)
- preterm labor and delivery
The symptoms of preeclampsia are excess weight gain, leg and hand swelling (edema), headaches, and high blood pressure.
Baby
The earlier in the pregnancy that placental insufficiency occurs, the more severe the problems can be for the baby. The baby’s risks include:
- greater risk of oxygen deprivation at birth (can cause cerebral palsy and other complications)
- learning disabilities
- low body temperature (hypothermia)
- low blood sugar (hypoglycemia)
- too little blood calcium (hypocalcemia)
- excess red blood cells (polycythemia)
- premature labor
- cesarean delivery
- stillbirth
- death
Diagnosis and management
Getting proper prenatal care can lead to an early diagnosis. This can improve outcomes for the mother and the baby.
Tests that can detect placental insufficiency include:
- pregnancy ultrasound to measure the size of the placenta
- ultrasound to monitor the size of the fetus
- alpha-fetoprotein levels in the mother’s blood (a protein made in the baby’s liver)
- fetal nonstress test (involves the wearing of two belts on the mother’s abdomen and sometimes a gentle buzzer to wake the baby) to measure the baby’s heart rate and contractions
Treating maternal high blood pressure or diabetes can help improve the baby’s growth.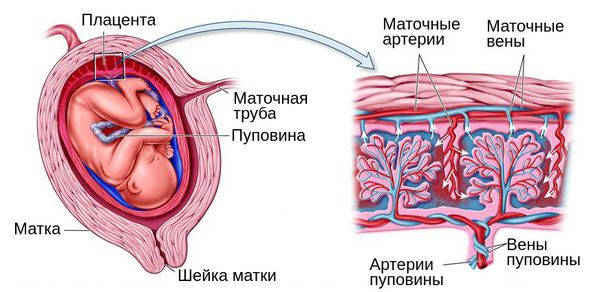
A maternity care plan may recommend:
- education on preeclampsia, as well as self-monitoring for the disease
- more frequent doctor visits
- bed rest to conserve fuel and energy for the baby
- consultation with a high-risk maternal fetal specialist
You may need to keep a daily record of when the baby moves or kicks.
If there is concern about premature birth (32 weeks or earlier), the mother may receive steroid injections. Steroids dissolve through the placenta and strengthen the baby’s lungs.
You may need intensive outpatient or inpatient care if preeclampsia or intrauterine growth restriction (IUGR) become severe.
Outlook
Placental insufficiency can’t be cured, but it can be managed. It’s extremely important to receive an early diagnosis and adequate prenatal care. These can improve the baby’s chances of normal growth and decrease the risk of birth complications. According to Mount Sinai Hospital, the best outlook occurs when the condition is caught between 12 and 20 weeks.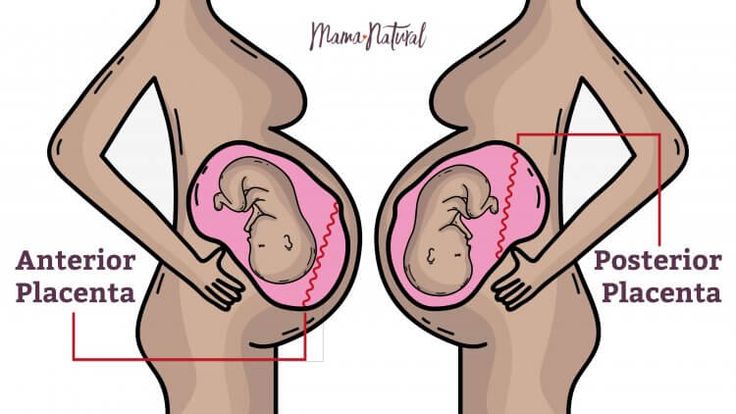
Last medically reviewed on January 9, 2018
- Parenthood
- Pregnancy
- Pregnancy Complications
How we vetted this article:
Healthline has strict sourcing guidelines and relies on peer-reviewed studies, academic research institutions, and medical associations. We avoid using tertiary references. You can learn more about how we ensure our content is accurate and current by reading our editorial policy.
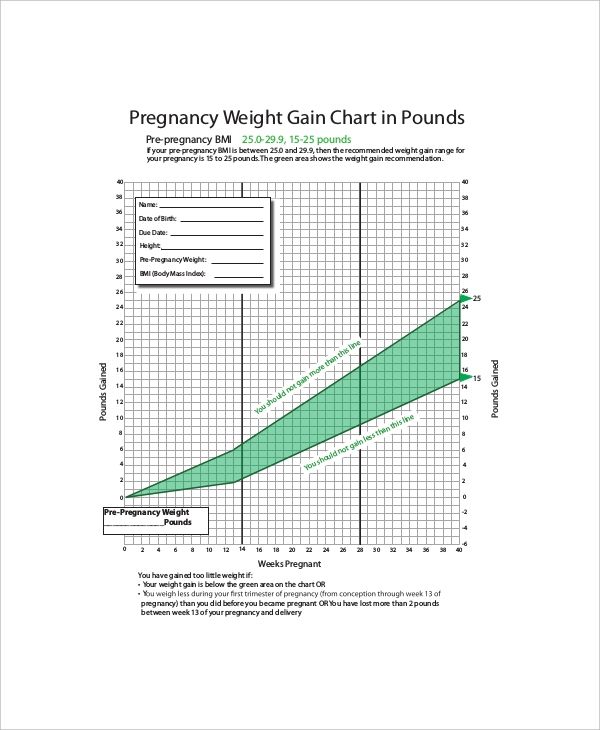
- Eating for two when over or under weight. (2015).
americanpregnancy.org/pregnancy-health/eating-for-two/ - Mayo Clinic Staff. (2015). Pregnancy week by week.
mayoclinic.org/healthy-lifestyle/pregnancy-week-by-week/in-depth/placenta/art-20044425 - Placental insufficiency. (n.d.).
mountsinai.on.ca/care/placenta-clinic/complications/placentalinsufficiency
Our experts continually monitor the health and wellness space, and we update our articles when new information becomes available.
Current Version
Jan 9, 2018
By
Sandy Calhoun Rice
Edited By
Nizam Khan (TechSpace)
Medically Reviewed By
Debra Rose Wilson, PhD, MSN, RN, IBCLC, AHN-BC, CHT
Share this article
Medically reviewed by Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT — By Sandy Calhoun Rice on January 8, 2018
related stories
Birth Defects
When Baby Comes Early: What Is Your Risk?
Why You Shouldn’t Worry About an Anterior Placenta
Preeclampsia: Causes, Diagnosis, and Treatments
Second Trimester Pregnancy Complications
Read this next
Birth Defects
Medically reviewed by Karen Gill, M.D.
Find information on birth defects, including what causes them, how they're diagnosed, and how they can be prevented.
READ MORE
When Baby Comes Early: What Is Your Risk?
Medically reviewed by Tyler Walker, MD
A number of social factors affect a woman's risk for preterm labor.
 Discover what they are here.
Discover what they are here.READ MORE
Why You Shouldn’t Worry About an Anterior Placenta
Medically reviewed by Valinda Riggins Nwadike, MD, MPH
An anterior placenta positioning during pregnancy isn’t usually cause for concern. Here’s what your doctor will keep an eye on leading up to labor and…
READ MORE
Preeclampsia: Causes, Diagnosis, and Treatments
Medically reviewed by Mia Armstrong, MD
Preeclampsia is when you have high blood pressure and protein in your urine during pregnancy or after delivery. Learn about symptoms, treatment, and…
READ MORE
Second Trimester Pregnancy Complications
Medically reviewed by Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT
By the second trimester of your pregnancy, you should be feeling better than you did in the first trimester.
 However, every pregnancy is different…
However, every pregnancy is different…READ MORE
Placenta Delivery: What to Expect
After delivering your baby, you’re not quite done. There’s still the placenta to contend with. Here’s what to expect.
READ MORE
What Is Placental Abruption?
Medically reviewed by Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT
Placental abruption occurs during a pregnancy when the placenta detaches from the uterine wall too early. This can cause bleeding and complications…
READ MORE
Pregnancy Complications
Medically reviewed by Michael Weber, MD
Sometimes a pregnant woman’s existing health conditions can contribute to problems, and other times new conditions arise because of body and hormonal…
READ MORE
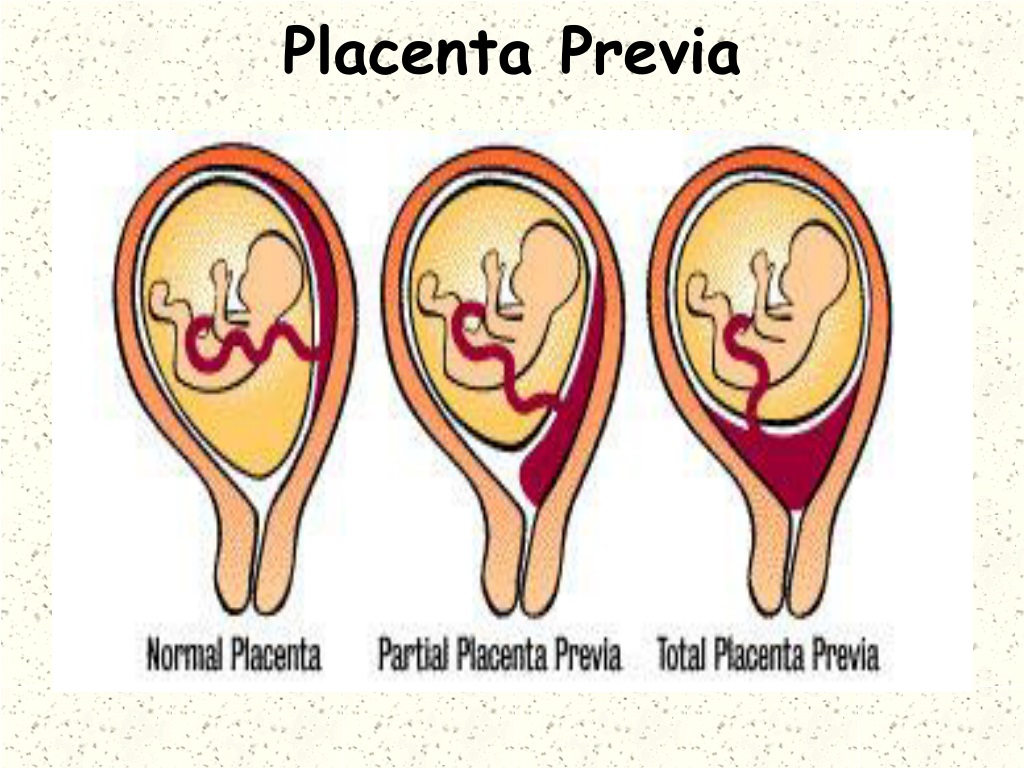
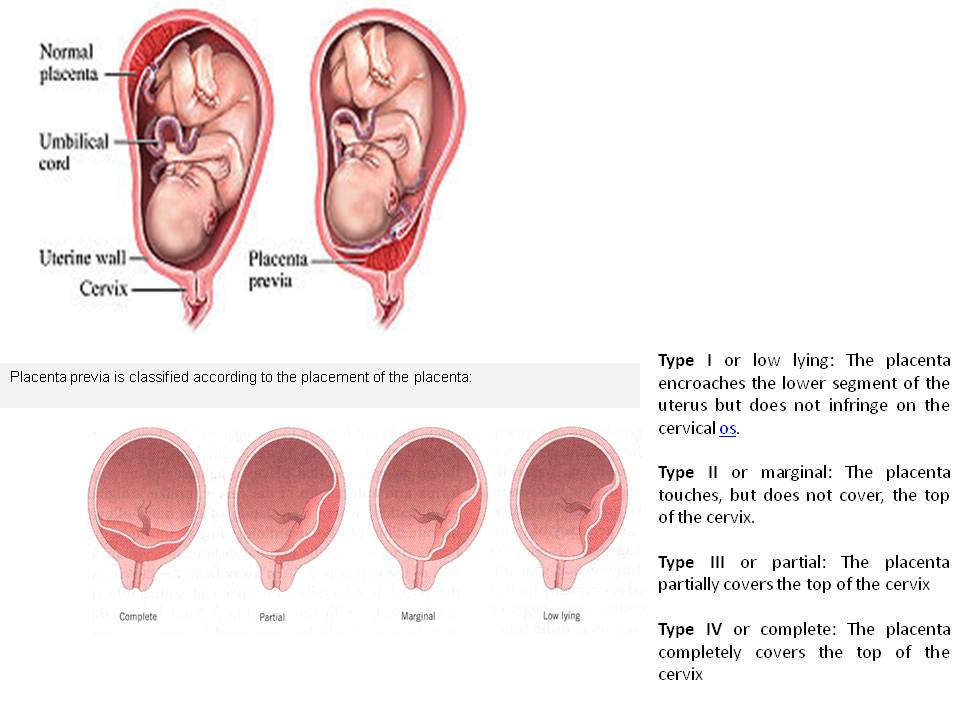
Placenta Previa
Medically reviewed by Fernando Mariz, MD
Placenta previa is when the placenta covers the opening of the cervix during the last months of pregnancy.
 Find out about symptoms and treatment.
Find out about symptoms and treatment.READ MORE
What Is a Nurse Midwife and How to Tell If They Are Right for You
Medically reviewed by Meredith Wallis, MS, APRN, CNM, IBCLC
A nurse midwife is a nurse with education, training, and certification to provide prenatal, delivery, and women's care.
READ MORE
Placental insufficiency - what is it and how to treat it
- Types and causes of placental insufficiency
- Diagnosis of placental insufficiency
- Treatment of placental insufficiency
Most women know that the placenta connects mother and baby during pregnancy and provides nutrients and oxygen to the baby.
Are there situations when the placenta ceases to perform its function correctly and fully? Is it possible to somehow prevent this?
What is the function of the placenta
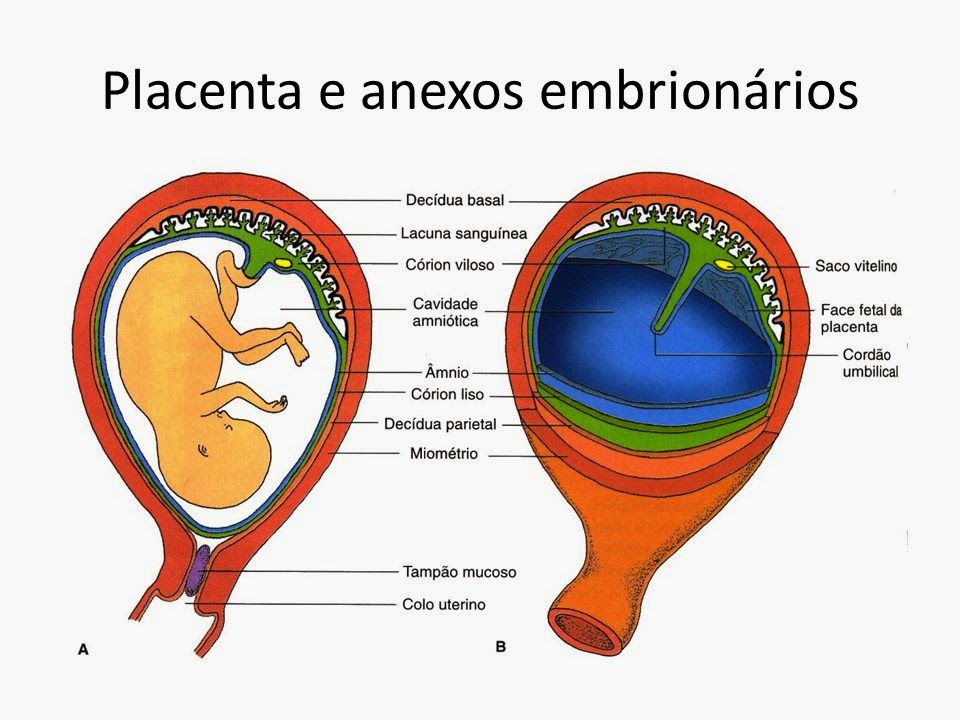
So, the placenta is an important organ that is formed only during pregnancy.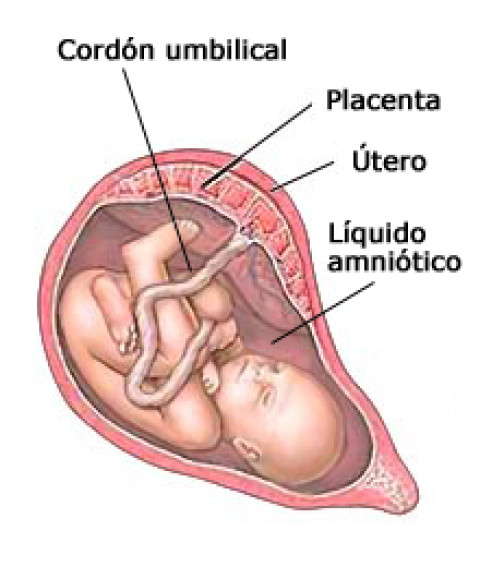 The placenta is formed from the chorion - the embryonic membranes of the fetus. At the very beginning of pregnancy, chorionic villi - outgrowths of the membrane - evenly cover the entire surface of the fetal egg, starting from the second month of pregnancy, on one side of the fetal egg, the villi begin to lengthen, increase in size and form the placenta.
The placenta is formed from the chorion - the embryonic membranes of the fetus. At the very beginning of pregnancy, chorionic villi - outgrowths of the membrane - evenly cover the entire surface of the fetal egg, starting from the second month of pregnancy, on one side of the fetal egg, the villi begin to lengthen, increase in size and form the placenta.
Inside the villi flows the blood of the baby, and outside they are bathed in the blood of the mother. Between the blood flow of mother and baby there is only one layer of cells, which plays the role of a barrier between the body of mother and child. Thanks to this membrane, the blood of the mother and fetus does not mix.
However, in recent years it has become known that fetal blood cells still penetrate the placental barrier into the mother's bloodstream, and thanks to this, it has become possible to conduct genetic analyzes and determine chromosomal abnormalities, Rh factor and fetal sex from the blood of a pregnant woman (non-invasive prenatal test) .
In the placenta, there is a constant exchange of substances between mother and child. Oxygen and nutrients are supplied from the mother's blood to the fetus, carbon dioxide and metabolic products from the fetus back to the mother, to be removed from the body.
The placental barrier performs an immunological function, as it allows some protective antibodies - blood cells that fight infectious agents, in addition, it is impervious to certain harmful substances, viruses and bacteria. Unfortunately, the placental barrier is easily overcome by drugs, alcohol, nicotine, components of many drugs and some viruses.
An important function of the placenta is the production of hormones and biologically active substances. First of all, these are hormones that are important for successful pregnancy, for example, chorionic gonadotropin, placental lactogen, estrogens, etc.
Unfortunately, things don't always go well. Due to a variety of reasons, deviations in the development and functioning of the placenta may occur at different stages of pregnancy. These changes never go unnoticed for mom and baby, and often have dire consequences.
These changes never go unnoticed for mom and baby, and often have dire consequences.
If the placenta ceases to perform its functions to the fullest, the so-called placental insufficiency develops. In fact, it consists in the deterioration of blood circulation in the mother-placenta-fetus system.
Types and causes of placental insufficiency
Doctors distinguish between acute and chronic placental insufficiency:
Acute placental insufficiency
This is a condition that requires urgent medical intervention. It is characterized by a rapid deterioration in placental blood flow. Acute placental insufficiency occurs mainly as a result of placental abruption or the death of certain areas of placental tissue, for example, during the formation of blood clots in the vessels. Abdominal trauma, antiphospholipid syndrome can serve as the cause of detachment.
Phospholipids are complex fats that are part of the membranes of all body cells. In some cases, the body's immune system produces a large number of antibodies to some of its own phospholipids and proteins that bind these lipids.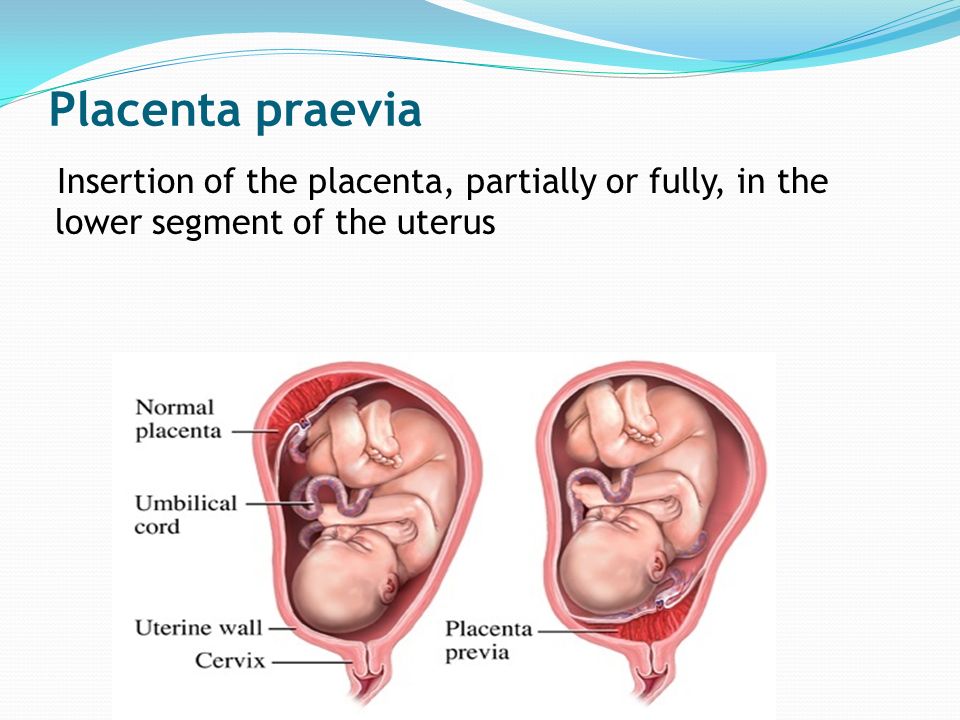 They are called antiphospholipid antibodies and, when interacting with the cells of the body, cause cell damage and activation of the blood coagulation system, which leads to thrombosis.
They are called antiphospholipid antibodies and, when interacting with the cells of the body, cause cell damage and activation of the blood coagulation system, which leads to thrombosis.
Antiphospholipid syndrome is the most common cause of thrombotic complications in pregnancy, including placental abruption and acute placental insufficiency.
A severe course of gestosis, a formidable complication of the second half of pregnancy, manifested by edema, increased pressure and the appearance of protein in the urine, can also cause placental abruption.
Acute placental insufficiency develops when more than 2/3 of the placental surface is detached.
In case of acute placental insufficiency, it is necessary to perform a caesarean section as soon as possible to save the life of the baby and mother.
Chronic placental insufficiency
Chronic placental insufficiency is much more common in pregnant women. In this case, there is a violation of the formation and maturation of the placenta, the uteroplacental and fetal-placental blood flow decreases, gas exchange and metabolism in the placenta are limited, and the synthesis of placental hormones decreases.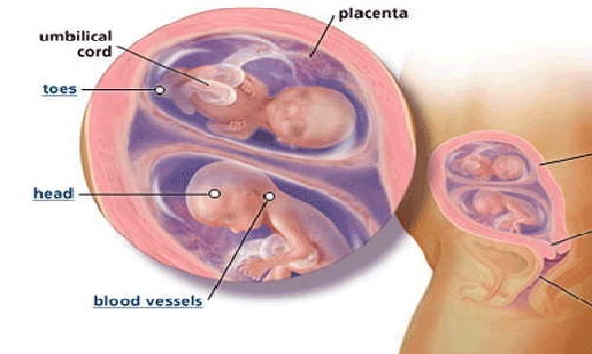 All these changes determine the insufficient supply of oxygen and nutrients to the baby, cause a delay in the growth and development of the fetus.
All these changes determine the insufficient supply of oxygen and nutrients to the baby, cause a delay in the growth and development of the fetus.
The most common causes of placental insufficiency are previous abortions, especially surgical abortion during the first pregnancy, smoking, while the number and strength of cigarettes smoked do not matter, since tobacco smoke, not nicotine, has a negative effect on the formation of defective placental vessels.
The risk group for the development of placental insufficiency also includes women with chronic diseases such as arterial hypertension, iron deficiency anemia, pyelonephritis, diabetes, thyroid disease.
In recent years, there has been a significant increase in placental insufficiency caused by bacteria, viruses, fungi. The reason for this can be both an acute infection suffered by the expectant mother during pregnancy, and the activation of a chronic infectious process in the body of a pregnant woman.
Of no small importance in the formation of chronic placental insufficiency is the pathology of the uterus: endometriosis, malformations of the uterus (saddle-shaped, bicornuate). Doctors also consider uterine fibroids to be a risk factor. Of course, a number of drugs have an adverse effect on the formation of the placenta and the development of the fetus. Currently, a list of drugs that are not approved for use during pregnancy has been defined.
Doctors also consider uterine fibroids to be a risk factor. Of course, a number of drugs have an adverse effect on the formation of the placenta and the development of the fetus. Currently, a list of drugs that are not approved for use during pregnancy has been defined.
Also of great importance in the development of placental insufficiency is thrombophilia - an increased tendency of the body to form blood clots - blood clots in the vessels.
In some cases, placental insufficiency may be due to the presence of chromosomal abnormalities in the fetus, in particular in Down syndrome (the presence of an additional chromosome 21 in the fetus) or Edwards syndrome (an additional chromosome 18 in the fetus), placental dysfunction is diagnosed already in the early stages of pregnancy.
It should be noted that among the complications of pregnancy, most often leading to the development of chronic placental insufficiency, a significant factor is preeclampsia (or late preeclampsia) - a complication of the second half of pregnancy, manifested by edema, increased pressure and the appearance of protein in the urine.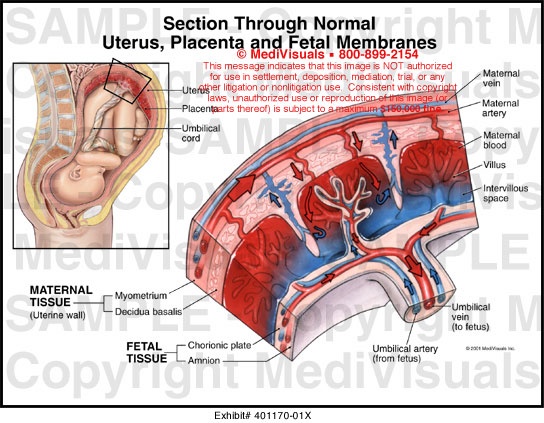
Regardless of the factors contributing to the development of placental insufficiency, it is based on circulatory disorders in the uterine-placental complex, leading to disruption of all functions of the placenta. Consequently, the symptoms of chronic placental insufficiency will be due to a lack of oxygen and nutrients to the fetus.
This is, first of all, intrauterine fetal growth retardation - a lag in the size of the fetus and a slowdown in its growth. Often there is a change in the motor activity of the fetus. At first there may be some increase in movements, and then a decrease. Violation of the protective function of the placenta leads to intrauterine infection of the fetus under the action of pathogenic (pathogenic) microorganisms penetrating the placenta. The fetus, the development of which occurs in conditions of placental insufficiency, is much more at risk of trauma during childbirth, they have a violation of adaptation to extrauterine life, increased morbidity in the first year of life.
According to the time of occurrence, doctors divide placental insufficiency into early and late.
Early (or primary) placental insufficiency
Develops before 16 weeks of gestation. It occurs already at the stage of placenta formation and is associated with diseases of a pregnant woman that are present before pregnancy, for example, with uterine pathology, chronic arterial hypertension, and endocrinological diseases. In this case, the formation of defective vessels in the placenta occurs.
Late (or secondary) placental insufficiency
Occurs after 16 weeks of pregnancy and is most often associated with diseases that have already occurred during pregnancy. Most often, these are iron deficiency anemia (that is, a decrease in the concentration of hemoglobin and iron in the blood), gestational diabetes mellitus (that is, a violation of the absorption of glucose by the body that occurred during pregnancy), past viral and bacterial infections.
It is important to subdivide placental insufficiency into compensated and decompensated forms.
Compensated placental insufficiency
It develops, for example, with the threat of abortion and mild forms of late preeclampsia, if these complications are successfully amenable to medical correction.
Decompensated placental insufficiency
Causes the development of fetal growth retardation, chronic intrauterine hypoxia, up to fetal death.
Diagnosis of placental insufficiency
It is almost impossible to treat an already developed placental insufficiency, so doctors actively seek to identify pregnant women at risk of developing placental dysfunction. If placental insufficiency is detected in the 3rd trimester of pregnancy, there is no effective treatment, unfortunately. Therefore, all methods of identifying in the early stages of pregnancy those women whose formation of the placenta has been disturbed are being very actively used.
First of all, when registering for pregnancy, the most significant risk factors are identified - smoking, abortions, aggravated heredity (low birth weight, tendency to thrombosis), the presence of chronic diseases of the heart, blood vessels, diabetes mellitus.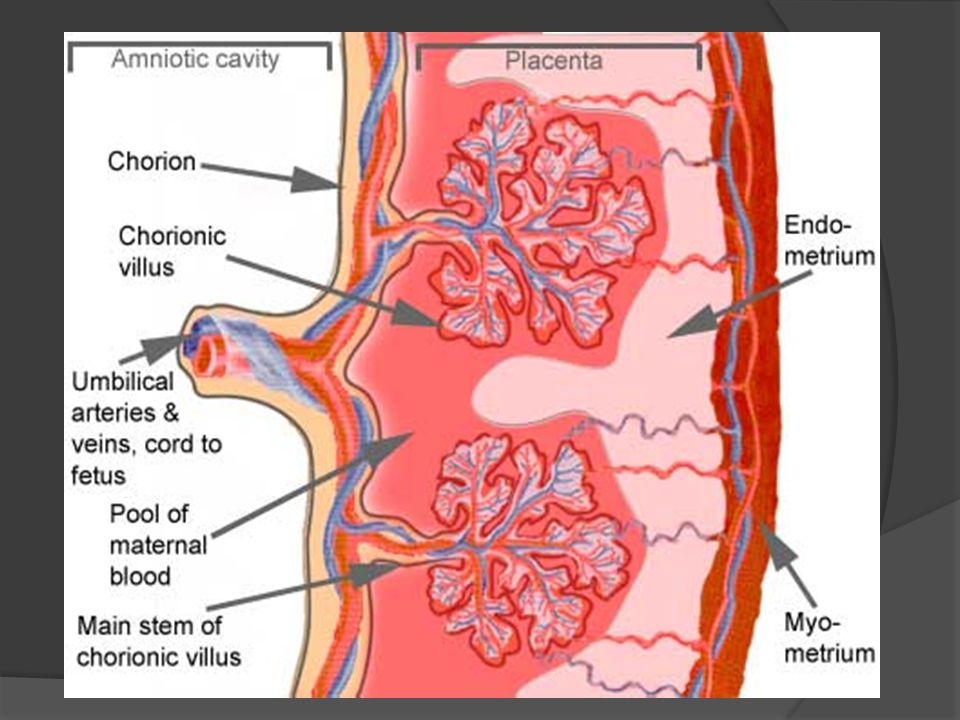
Preventive measures against the development of placental insufficiency are especially relevant and necessary until 16-17 weeks of pregnancy, when the formation of placental structures occurs.
Significant assistance in assessing the risk of developing placental insufficiency is provided by prenatal screening, which is carried out at 11-14 weeks of pregnancy. It is carried out to detect Down syndrome, Edwards syndrome and other chromosomal diseases in the fetus. Currently, the most relevant is to conduct a comprehensive early screening of a pregnant woman to predict the risk of developing placental insufficiency, preeclampsia and intrauterine growth retardation. Since this type of diagnostics is one of the most modern and advanced, unfortunately, it is not yet included in the list of services provided in the antenatal clinic within the framework of compulsory medical insurance, but is available to everyone in prenatal diagnostic centers.
Determination of proteins produced by the placenta
First of all, the PAPP-A protein is determined, it is also a marker of chromosomal abnormalities of the fetus.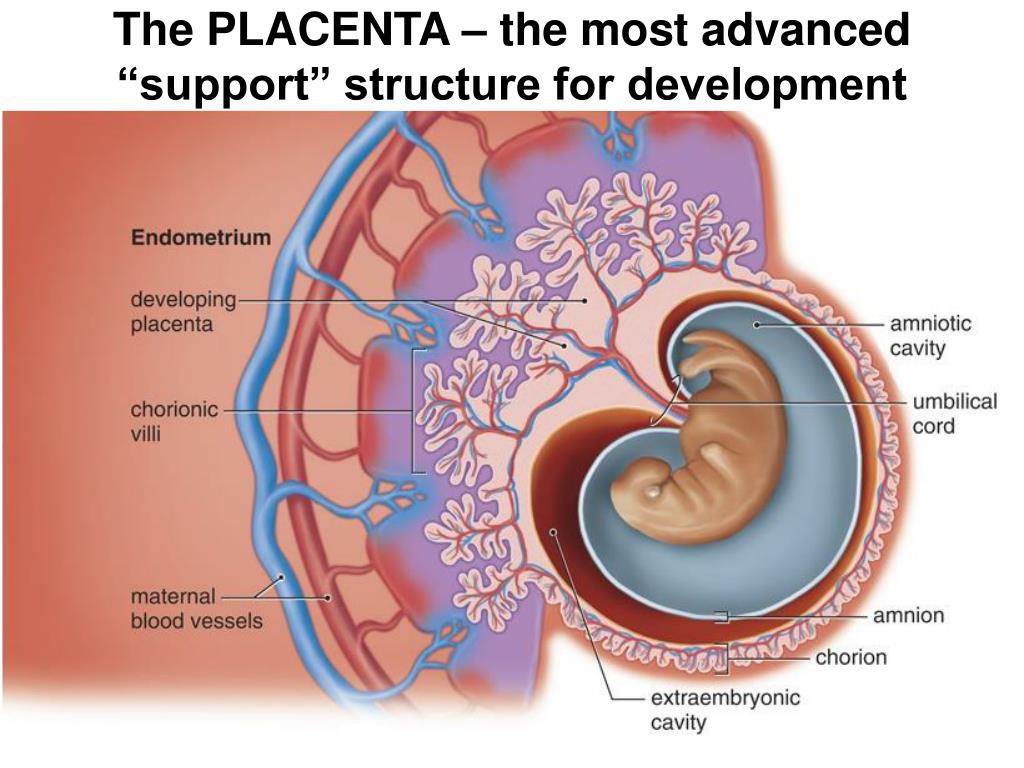 A decrease in the concentration of PAPP-A in the blood at 11-14 weeks of gestation occurs in pregnant women who have a high risk of placental insufficiency and fetal growth retardation.
A decrease in the concentration of PAPP-A in the blood at 11-14 weeks of gestation occurs in pregnant women who have a high risk of placental insufficiency and fetal growth retardation.
The second placental hormone that helps in assessing the risk of placental insufficiency is PIGF (placental growth factor). Its concentration in the blood decreases long before the first manifestations of placental insufficiency. Its definition is not as widely used as PAPP-A, but many laboratories have already included this protein in 1st trimester prenatal screening. It is extremely important when screening the 1st trimester to measure blood flow in the vessels of the uterus. It has been unambiguously proven that the narrowing of the vessels of the uterus, determined during the study, indicates the inferiority of the formation of the placenta, which will worsen with increasing gestational age and lead to a decrease in the nutrition of the baby and the supply of oxygen, that is, to the development of placental insufficiency and fetal growth retardation. With normal sizes of uterine vessels at 11-14 weeks of gestation, the risk of severe placental insufficiency is negligible.
With normal sizes of uterine vessels at 11-14 weeks of gestation, the risk of severe placental insufficiency is negligible.
The next mandatory screening ultrasound is at 20-21 weeks of gestation. In this case, measurements of the fetus must be carried out in order to assess whether there is a lag in growth. After all, with oxygen starvation, the growth rate of the fetus slows down and its size begins to lag behind the norm for each period of pregnancy. In addition, the doctor must evaluate the condition and maturity of the placenta. During ultrasound, dopplerometry of the uterine vessels is also performed to detect early changes that precede the clinical manifestations of placental insufficiency.
In patients belonging to the high-risk group, in addition to ultrasound and dopplerometry, daily monitoring of blood pressure fluctuations is also carried out, the amount of protein in the urine sample collected per day is determined, and the indicators of the blood coagulation system are evaluated.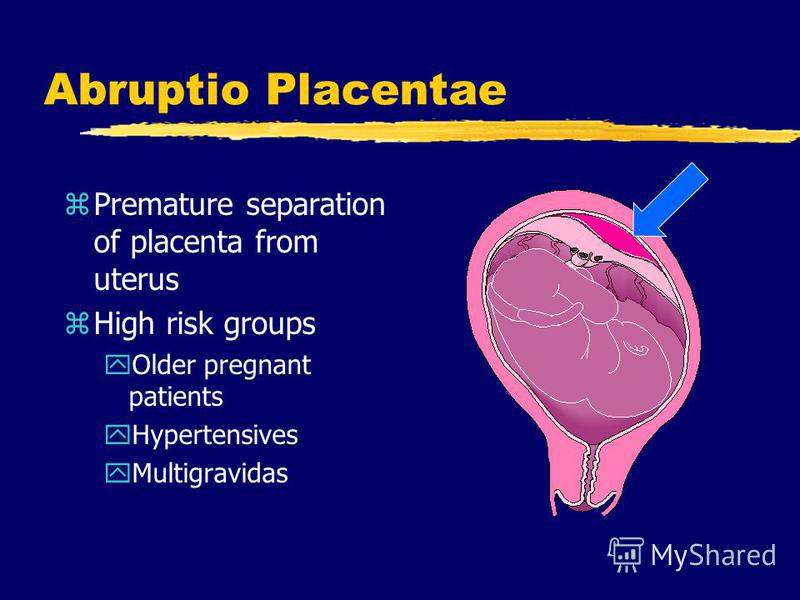
The third ultrasound is performed for all expectant mothers at 30-34 weeks of pregnancy. The doctor measures the circumference of the head and abdomen of the crumbs, the length of the bones of his arms and legs, and calculates the estimated weight of the fetus. These measurements allow the doctor to make sure that the baby is developing normally. The structure of the placenta is also important, the presence of signs of aging in it, as a result of which it usually ceases to fully supply the baby with blood, which means that it ceases to have enough oxygen and nutrients and the development of the child is disturbed. During ultrasound, the amount and type of amniotic fluid is assessed, which can also change with intrauterine fetal suffering.
Doppler
Doppler of the placental and umbilical cord vessels (method of studying blood flow velocities in these vessels) also allows you to assess the well-being of the baby. The doctor examines the blood flow in the arteries of the uterus, umbilical cord, heart and brain of the child.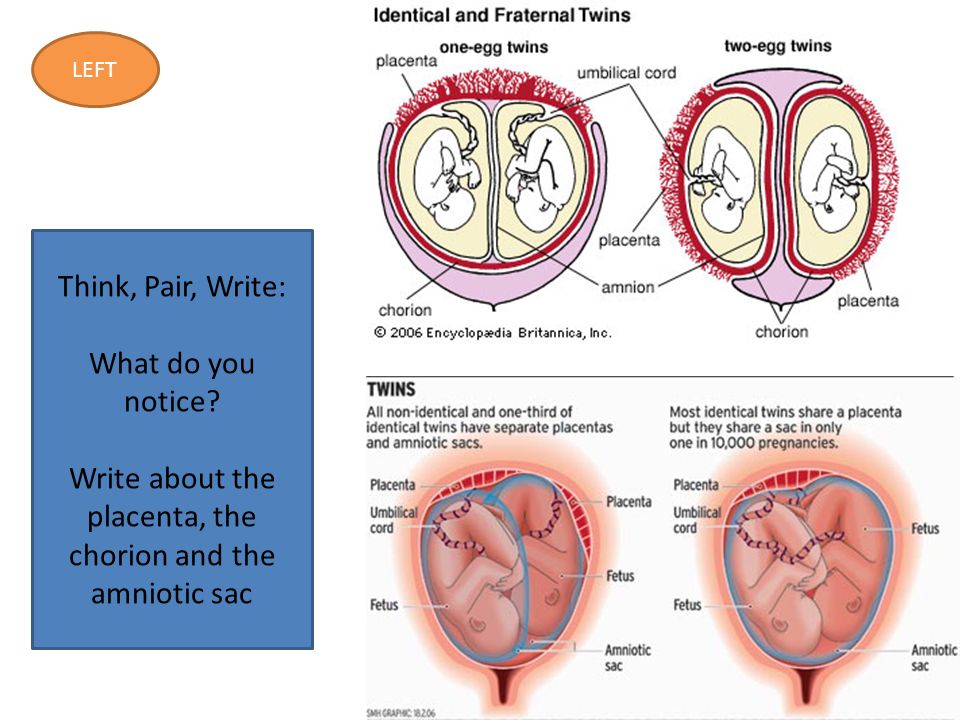 This study allows you to determine whether the placenta is working well, whether there are signs of a lack of oxygen in the baby, or the development of preeclampsia in the mother. With a decrease in the speed of blood flow in any vessel, one can speak of fetal malnutrition of varying severity.
This study allows you to determine whether the placenta is working well, whether there are signs of a lack of oxygen in the baby, or the development of preeclampsia in the mother. With a decrease in the speed of blood flow in any vessel, one can speak of fetal malnutrition of varying severity.
A well-timed examination makes it possible to identify the initial stages of blood supply deficiency. In such cases, treatment can prevent formidable complications, such as hypoxia and intrauterine growth retardation of the baby. Dopperometry is carried out at 20-21 weeks and at 30-32 weeks of pregnancy, if there are changes, control is carried out at least every two weeks.
Cardiotocography
This is an important method for assessing the condition of the fetus. CTG is performed at a gestational age of 33 weeks or more, since only at this stage of the intrauterine development of the baby is a complete regulation of the activity of the cardiovascular system of the fetus established by the centers of the spinal cord and brain.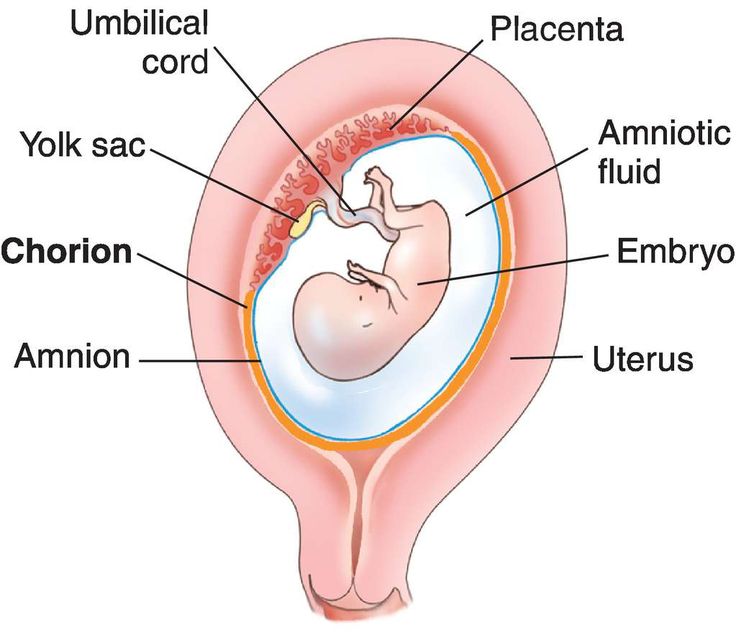 Recording of fetal heartbeats is carried out for 20-40 minutes, and if necessary, the study can be extended up to 1.5 hours.
Recording of fetal heartbeats is carried out for 20-40 minutes, and if necessary, the study can be extended up to 1.5 hours.
The device registers and records the baby's heart rate. The obstetrician-gynecologist evaluates the heartbeat recording curve, episodes of slowing down and a sharp increase in the fetal heart rate, and based on these data, makes a conclusion about how comfortable the baby feels in the mother's stomach. For example, with a decrease in the concentration of oxygen in the blood of the fetus, its supply to the cells of the nervous system also decreases, which in turn affects the heart rate. In the normal course of pregnancy, CTG is performed after 33 weeks 1 time in 10-14 days, sometimes more often. Some clinics currently offer the service of continuous CTG monitoring, which becomes relevant in the presence of signs of placental insufficiency. A pregnant woman is given a monitor that records changes in the baby's heart activity and these data are transmitted via the Internet to the attending physician.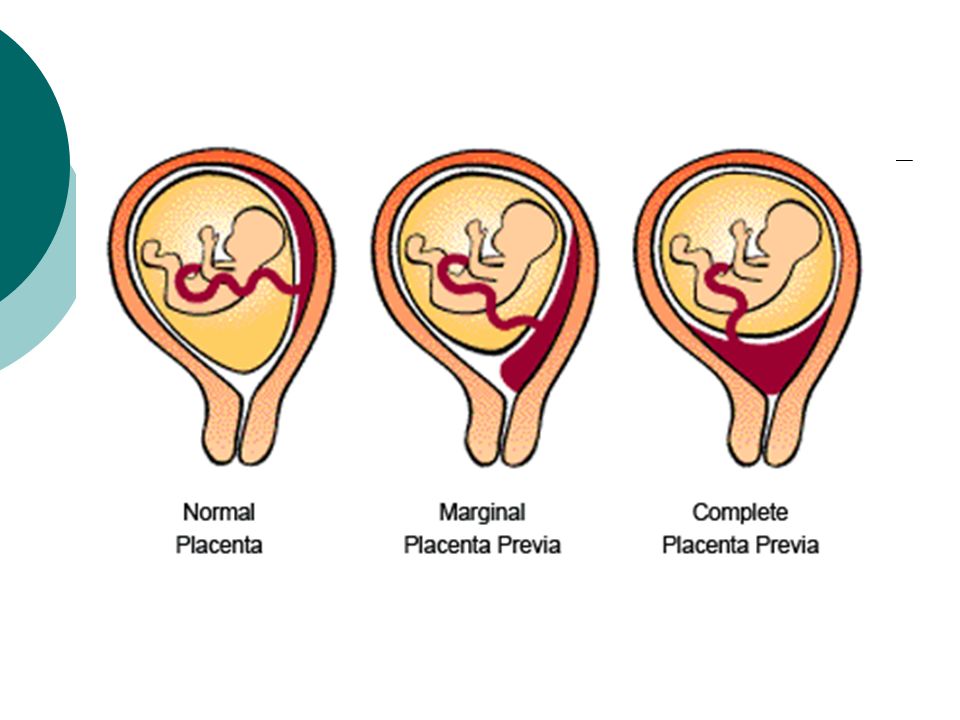
Treatment of placental insufficiency
There are currently no specific treatments for placental insufficiency because there are no drugs that selectively improve uteroplacental blood flow. That is why all measures to combat placental insufficiency are aimed at prevention. If the patient is at high risk for the development of placental insufficiency, from early pregnancy she is prescribed drugs whose effectiveness is well proven and which prevent the early development of severe placental dysfunction.
If during the additional methods of assessing the condition of the fetus, initial disturbances in the supply of oxygen to the baby are detected, drug treatment is carried out aimed at increasing the flow of blood and oxygen through the placenta and mandatory control examinations against the background of ongoing therapy. If the changes are serious and the baby experiences a pronounced deficiency of oxygen and nutrients, his condition suffers, then in such cases an emergency delivery is performed.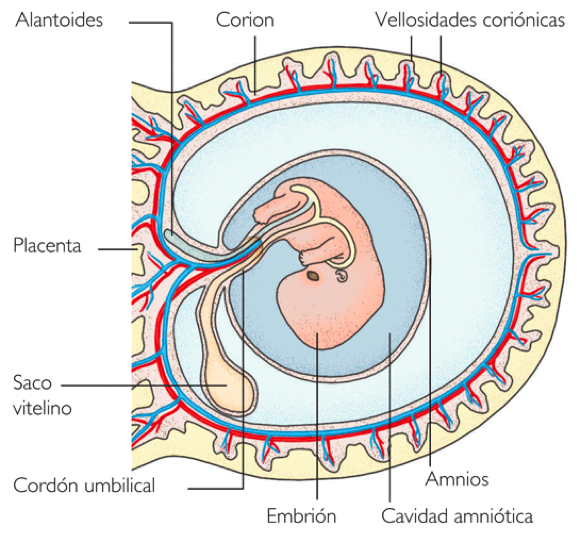
Premature placental abruption: what a future mother needs to know and how not to miss its signs | Blog
First, let's talk about what is the placenta?
The placenta is the embryonic organ that connects the body of mother and child. Its uniqueness lies in the fact that it is the only "disposable" organ. The placenta begins to develop from the 2nd week of pregnancy, forms up to 15-16 weeks and reaches full functional maturity by 36 weeks. And after the birth of the fetus (in the third stage of childbirth), it separates and leaves the mother's body, starting the process of lactation at the endocrinological level.
The placenta performs important functions such as gas exchange, nutrient exchange between mother and child, provides immunological protection and works as an endocrine gland, producing hormones necessary for the development of the fetus and the normal course of pregnancy. Every minute, about 500 ml of blood enters the placenta, but at the same time it is a kind of barrier that does not allow the blood of the mother and child to mix, and also prevents many toxic substances from entering the bloodstream of the baby.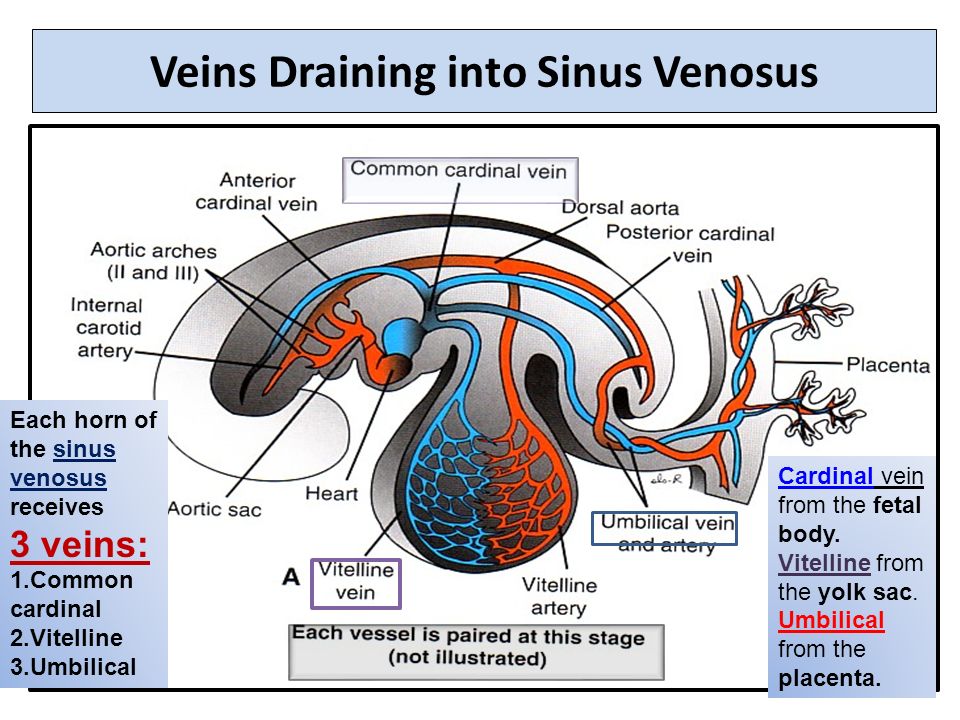
In this article we will talk about placental abruption.
This condition is quite rare (up to 1.5% of all pregnancies), but causes such threatening complications as massive bleeding and hemorrhagic shock, fetal distress, which in some cases can cause death. Normally, the detachment of the placenta from the inner wall of the uterus occurs only after the birth of the fetus. If this happens before the onset of labor, as well as in the first or second stage of labor, this is the premature detachment of a normally located placenta. This condition is a very dangerous pathology that requires immediate diagnosis and decision of further medical tactics in the near future.
Causes of premature placental abruption
Unfortunately, the only cause of premature placental abruption has not been established to date. There are many theories, but in general, the occurrence of this condition is associated with many provoking factors.
Major risk factors include:
- arterial hypertension,
- diabetes mellitus
- pregnant woman over 40 years old
- multiple pregnancy
- polyhydramnios
- postterm pregnancy and large fetus
- previous uterine surgery
- blood coagulation disorder,
- autoimmune diseases
- kidney disease
- bad habits such as smoking and drug use
- inflammatory diseases of the uterus and placenta, anomalies in the development of the uterus.
Causes that can provoke placental abruption: physical trauma of a pregnant woman (accident, fall, blow to the stomach), disruption of the contractile activity of the uterus, stress, gross obstetric manipulations.
Types of placental abruption
There are the following types of placental abruption: partial and complete.
Partial detachment, in turn, can be central and marginal.
Why is this classification so important? And because both the clinical picture and medical tactics depend on the place and volume of the detachment. Partial detachment can be progressive or non-progressive.
Non-progressive detachment has a significantly better prognosis for a pregnant woman, because in this case, conservative treatment is possible with preservation of pregnancy.
Symptoms of placental abruption:
Here is a triad of main symptoms that may be a sign of placental abruption:
- abdominal pain, feeling of increased uterine tone;
- spotting from the genital tract;
- violation of the fetal heartbeat, which indicates fetal distress.
Also, a woman can feel the baby's reaction to a decrease in the amount of oxygen supplied to him due to placental abruption - he begins to move more actively, reacting to hypoxia.
These symptoms do not always appear at the same time! For example, with marginal abruption of the placenta, blood flows into the vagina, which means that the woman sees signs of bleeding. With central detachment, a retroplacental hematoma is formed. Bleeding is internal, which means that a pregnant woman may not notice its signs. The appearance of an accelerated heartbeat in a woman, a decrease in blood pressure, nausea, dizziness, and severe weakness may indicate internal bleeding.
However, with central placental abruption, blood accumulates in front of the placenta and begins to “press” on nearby tissues. As a result, a pronounced pain syndrome occurs.
It must be emphasized that if at least one of the symptoms appears, it is necessary to immediately inform the doctor about it! This condition can be very dangerous for you and your baby, so it is important to diagnose it in a timely manner.
Diagnosis of placental abruption
Diagnosis of placental abruption is based not only on clinical symptoms and gynecological examination. Ultrasound diagnostics is the main method that allows you to accurately assess the location and area of the exfoliated area of the placenta and see the presence or absence of a hematoma. Also, ultrasound can distinguish premature detachment from placenta previa (its abnormal location, in which it overlaps the internal pharynx of the cervix). This condition can have similar symptoms, as it is often accompanied by bleeding. The condition of the fetus and the degree of its hypoxia will be determined using cardiotocography, and Dopplerography, in turn, assesses violations of the uteroplacental circulation. Based on these examination results, the obstetrician-gynecologist, and more often a council of doctors, decides on the type of further medical tactics.
Treatment of placental abruption
Treatment of placental abruption always requires hospitalization of the pregnant woman in the maternity hospital for constant monitoring of her condition. In cases of non-progressive mild placental abruption with a stable state of the mother and fetus, conservative tactics with drug therapy and preservation of pregnancy are possible. Progressive detachment, as well as severe detachment, certainly requires an emergency caesarean section.
In cases of non-progressive mild placental abruption with a stable state of the mother and fetus, conservative tactics with drug therapy and preservation of pregnancy are possible. Progressive detachment, as well as severe detachment, certainly requires an emergency caesarean section.
In case of complete detachment of the placenta, with the rapid progression of this condition, massive bleeding occurs, which threatens the life of both the pregnant woman and the child. In such a situation, surgeons always prioritize the life of a woman and do everything necessary to save her. Some cases may, unfortunately, require even such radical surgical tactics as removal of the uterus. However, at the current level of development of medicine, more and more technologies are emerging that, with timely assistance, can save not only the life of the mother and child, but also the reproductive functions of a woman. In particular, our obstetrician-gynecologists and anesthesiologists use up-to-date international medical protocols to ensure the safest possible delivery.