Optimal birthing position
Getting your baby into the best birth position
Tommy's PregnancyHub
The ideal position for your baby to be in for labour and birth is head down, their back towards the front of your stomach.
The best position for your baby to be in for labour and birth is head down, facing your back - so that their back is towards the front of your tummy. This is called the occipito-anterior position. It allows them to move more easily through the pelvis.
If your baby is head down (cephalic) but facing your tummy (their back to your back), this is called the occipito-posterior position.
If your baby is legs and bottom down, this is called the 'breech' position.
Research shows that these the main benefits of the anterior position are that you are:
- less likely to have an emergency caesarean-section.
- more likely to have a quicker and more straightforward labour and birth.
- may require less pain-relief.
Why is the anterior position the best for giving birth?
In this position, your baby will fit through your pelvis more easily. The back of his head will be pressing more evenly on your cervix, helping it to open and your labour to progress.
Your baby’s back is the heaviest part of its body so it will naturally move towards the lowest side of your abdomen. That’s why upright, forward-leaning positions may be helpful during the last few weeks of your pregnancy (from 34 weeks if it’s your first, or 37 weeks for subsequent pregnancies).
What exercises can I do to move my baby into the ideal position for birth?
Unfortunately there is little research to show that specific exercises are effective in moving the baby into the ideal position before birth.
You may have heard that spending time on your hands and knees or doing other exercises could help encourage the baby to change position. But this is not shown in research studies into this topic. A 2005 review of research into going on hands and knees to move the baby found that it was not effective and shouldn’t be recommended for this. However, it did find that the position helped to ease back pain.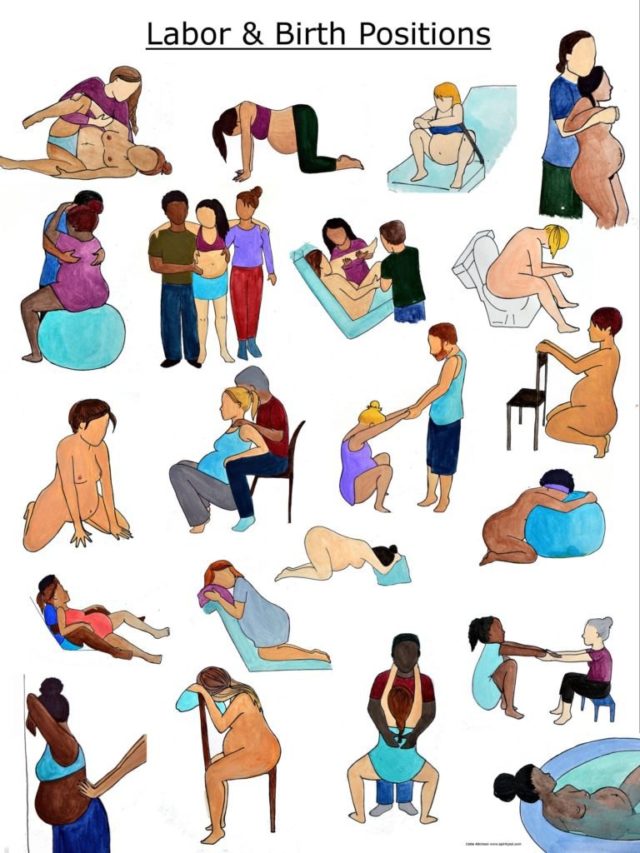
A more recent 2016 research study looked at whether the position helped to move the baby in the first stage of labour. It was not shown to be effective, but again women reported that it was a comfortable to be in while giving birth.
How do I know what position my baby is in?
Ask your midwife to help you work out the position of your baby.
When you feel your baby wriggling, try to visualise which body part is moving. You could even note down where you’re feeling the kicks. Little tickles are probably tiny hands, while more definite movements could be a knee, elbow, or foot.
Your baby’s head will feel hard and round, while bottoms usually feel a bit softer.
Anterior baby: You will probably feel kicks under your ribs. Your baby’s back will feel hard and rounded on one side of your tummy. Your belly button might poke out. This is the ideal position for baby to be in.
Posterior baby: You’ll probably feel more kicks on the front of your tummy, your belly-button might dip and the tummy area feel more squashy. When the baby is in a posterior position, labour can be longer, more painful and is more likely to end with caesarean or instrumental deliveries.
When the baby is in a posterior position, labour can be longer, more painful and is more likely to end with caesarean or instrumental deliveries.
Should I be worried if my baby is not in the ideal position for birth?
No, most babies turn during labour to the anterior position. Only 5-8 babies out of every 100 will stay in the posterior position.
You can read more about birth position and pregnancy in the Royal College of Midwives' document (written for midwives) Evidence Based Guidelines for Midwifery-Led Care in Labour, Persistent Lateral and Posterior Fetal Positions at the Onset of Labour.
Review dates
Reviewed: 01 April 2016 | Next review: 01 April 2019
This content is currently being reviewed by our team. Updated information will be coming soon.
Back to top
13 Best Labor and Birthing Positions
For nine months you prep and plan for baby’s arrival. You read books, watch videos and maybe even take a birthing class or two. But while movies and TV shows have led many of us to believe both labor and delivery happen while lying on your back with your legs spread wide, anyone who’s been through the experience will tell you it doesn’t have to play out that way.
You read books, watch videos and maybe even take a birthing class or two. But while movies and TV shows have led many of us to believe both labor and delivery happen while lying on your back with your legs spread wide, anyone who’s been through the experience will tell you it doesn’t have to play out that way.
There are actually a variety of labor positions you can assume during the first phases of childbirth and a whole other set that makes for good birthing positions when it’s time to push—and they don’t all call for you to be flat on your back. “Rotating between different labor and birthing positions is important to optimize conditions for the mom and baby,” says Sara Twogood, MD, an obstetrician gynecologist at Cedars Sinai Medical Center in Los Angeles and author of Ladypartsblog.com. “For Mom, this could mean making her more comfortable, especially if she’s having a medication-free birth. It can also mean maximizing the space in her pelvis so baby has more room.”
Here’s a primer on some of the best labor and birthing positions to help you prepare for the big day.
In this article:
Best labor positions
Best birthing positions
Best Labor Positions
The process of giving birth takes work (it’s not called “labor” for nothing). But that doesn’t mean you shouldn’t find a way to be as comfortable as humanly possible. “Labor positions are used during the labor process to help ease discomfort, move the baby down through the pelvis and encourage optimal fetal positioning,” says Lindsey Bliss, a birth doula and co-director of Carriage House Birth in New York City. “If you end up choosing not to utilize drugs for pain management, labor positions are essential for easing discomfort.”
Active labor, the phase in which contractions come on strong, is often when things really start to hurt. But keep in mind that women don’t start pushing until the cervix is fully dilated—for some women, this happens quickly; for others, not so much. So as your body and baby prepare for delivery, there are several labor positions your doctor or midwife may suggest to get you to the pushing point more comfortably. “Labor and delivery nurses are usually really great at helping a woman move around, even with an epidural, to find the labor positions that feel best for them,” Twogood says. “I recommend women try out a number of positions during labor. Every woman and baby is different, and what works for one woman won’t be ideal for another.”
“Labor and delivery nurses are usually really great at helping a woman move around, even with an epidural, to find the labor positions that feel best for them,” Twogood says. “I recommend women try out a number of positions during labor. Every woman and baby is different, and what works for one woman won’t be ideal for another.”
Check out some of the most common labor positions:
The hands and knees position
The all fours position calls for you to get down onto your hands and knees, either in bed or on a floor mat. “The hands and knees position is a great one, since it helps open the pelvis,” says Rebekah Wheeler,** RN, CNM, is a certified nurse-midwife in the Bay Area, California. . Adds Megan Cheney, MD, MPH, medical director of the Women’s Institute at Banner University Medical Center in Phoenix, “Sometimes baby’s heart rate responds better when you’re in the hands and knees position, especially if baby isn’t in the best spot.”
Pros:
Cons:
- Your arms may get tired
The sitting position
When you feel baby’s weight bearing down, you may just want to sit down—and that’s okay. Whether it’s in a birthing chair or even on a toilet, sitting and spreading your legs in this labor position can relieve some of the pressure on your pelvis.
Whether it’s in a birthing chair or even on a toilet, sitting and spreading your legs in this labor position can relieve some of the pressure on your pelvis.
Pros:
- Good for resting
- Can still be used with a fetal monitoring machine
- Sitting on a toilet relaxes the perineum, which can help reduce tearing
Cons:
- A hard toilet seat can become uncomfortable
- May not be an option if you’ve had high blood pressure during pregnancy
Birthing ball positions
Besides sitting on a birthing chair or toilet, you can also work the birthing ball into your labor positions. There are more than a few women who hail the prop as their BFF during labor and delivery. “Birthing balls provide support while you shift around,” Twogood says. “Women who want movement in their hips seem to find them helpful.” You can use a birthing ball in several ways: Some women sit or rock on it, lean against it or simply drape their upper bodies over it while kneeling. It can even be used as support while squatting. “I’m a huge fan,” Bliss says. “It’s great because women can continue bouncing and moving through the contractions even while being monitored.” Check beforehand to see if your hospital uses wireless fetal monitors; if not, you’ll be limited in how far you can move in these labor positions.
It can even be used as support while squatting. “I’m a huge fan,” Bliss says. “It’s great because women can continue bouncing and moving through the contractions even while being monitored.” Check beforehand to see if your hospital uses wireless fetal monitors; if not, you’ll be limited in how far you can move in these labor positions.
Pros:
-
Can help move baby into a favorable birthing position
-
Relieves back pressure
-
Birthing ball labor positions can help encourage dilation and move baby deeper into the pelvis
Cons:
The squatting position
Squats rarely top anyone’s list of favorite exercises, but on the day you give birth, you may want to give them a try as one of your labor positions. Squatting can be done against a wall or with the support of a chair or partner.
Pros:
Cons:
- May become tiring
The side-lying position
Lying on your side is one of the best labor positions to try when you need a rest.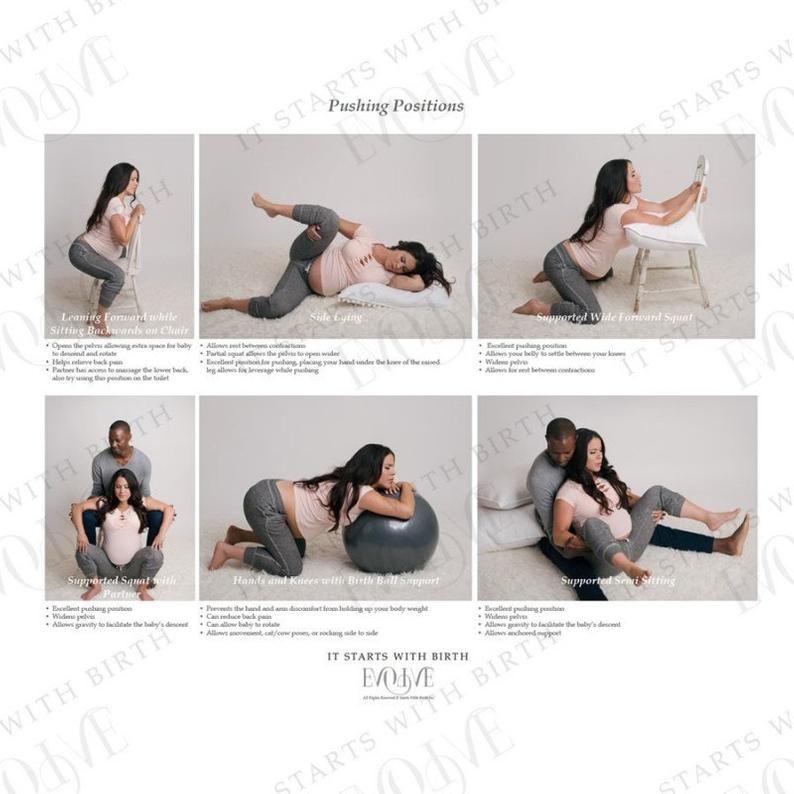 That said, just because you’re lying down doesn’t mean your body is taking a break from labor; on the contrary, it can actually help baby move into the ready position. “Side-lying and using a peanut-shaped birthing ball between the legs are wonderful tools for getting baby to descend and rotate,” Bliss says. “I encourage my clients to flip from side to side during the process to help baby come down and out.”
That said, just because you’re lying down doesn’t mean your body is taking a break from labor; on the contrary, it can actually help baby move into the ready position. “Side-lying and using a peanut-shaped birthing ball between the legs are wonderful tools for getting baby to descend and rotate,” Bliss says. “I encourage my clients to flip from side to side during the process to help baby come down and out.”
Pros:
-
Helps get oxygen to baby
-
Can be used if you have high blood pressure
-
Makes it easier to relax during contractions
Cons:
- May be difficult to assess fetal heartbeat
The upright position
Gravity may not be your best friend during pregnancy, but you can make it work to your advantage during childbirth through upright labor positions. Whether you’re standing, walking or swaying, simply being vertical can get you closer to the finish line.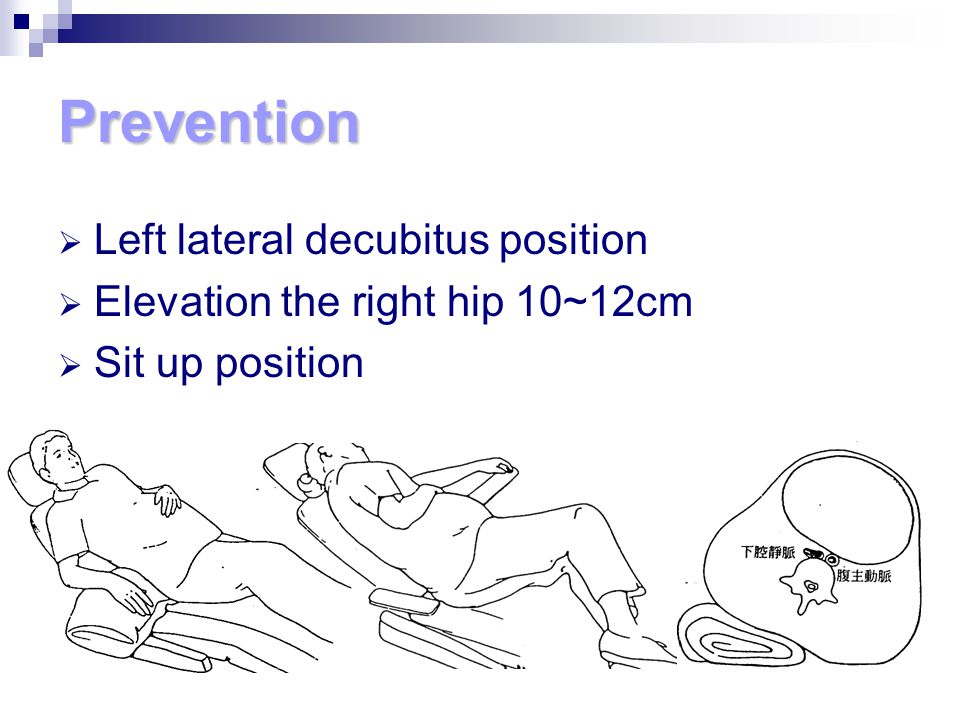 “Walking can be helpful for women who are waiting for labor to progress,” Cheney says. Amy, a mother of two from Connecticut, found that to be the case. “I walked laps around the hospital wing to speed things up,” she says. Swaying while using another person as support is also a good way to work through labor. “Rocking your hips keeps baby moving lower and lower,” Wheeler says. (It’s also good for getting a final hug of support from your partner before the main event!) Here are some other things to consider when it comes to the upright position:
“Walking can be helpful for women who are waiting for labor to progress,” Cheney says. Amy, a mother of two from Connecticut, found that to be the case. “I walked laps around the hospital wing to speed things up,” she says. Swaying while using another person as support is also a good way to work through labor. “Rocking your hips keeps baby moving lower and lower,” Wheeler says. (It’s also good for getting a final hug of support from your partner before the main event!) Here are some other things to consider when it comes to the upright position:
Pros:
Cons:
The lunging position
Doing lunges during labor may not sound like your idea of a good time, but lunging is one of the labor positions you may want to give a whirl. Unlike at the gym, you can put your foot up on a chair for these lunges: Simply lean your body forward onto the raised foot when you feel a contraction coming on. You can repeat it as many times as you want.
Pros:
Cons:
- Requires a partner to help you keep your balance
The stair-climbing position
If labor has been progressing nicely and then starts to slow down, baby might need extra encouragement to slip into the optimal position for birth. You may want to consider climbing stairs as one of your labor positions, since it can help baby shift.
Pros:
Cons:
- Can be tiring, especially if you’ve been in labor for a while
Best Birthing Positions
You’ve made it through the first stages of labor—congrats! Now it’s time to switch things up and assume birthing positions for the final stretch. “Birthing positions are used to push baby out,” Bliss says. Like labor positions, birthing positions don’t always equal lying on your back. In fact, “women who are in bed tend to experience more pain than women who move around,” Wheeler says. Here are some of the best birthing positions to try.
Squatting birth positions
Squats aren’t only great to do during labor, but they’re also among the popular birthing positions. Remember, when it comes to labor and delivery, gravity is on your side.
Pros:
Cons:
Reclining birth positions
Childbirth is hard work, and you might need to take a break—which is why many women opt for reclining birthing positions. Keep in mind, “reclining” can mean a number of things—yes, you can lie down in bed, but you can also recline against a wall, a chair or another person.
Pros:
- Can release tension and relax the muscles
- May be a good alternative if a woman is tired but doesn’t want to lie down completely
Cons:
- Can work against gravity
Birthing stool positions
A birthing stool can be used in a variety of birthing positions: Women can squat on it, get in the all fours position and use it to support the arms or even rock back and forth with it, depending on the design of the stool. Bonus: If you like the idea of a water birth, there are some birthing stool models that work in the water.
Bonus: If you like the idea of a water birth, there are some birthing stool models that work in the water.
Pros:
-
Can help baby move farther down
-
Relieves stress on the back
-
Can increase dilation of the cervix
Cons:
- Women may experience increased blood loss
Birthing bar positions
Call it the birthing stool’s cousin: The birthing bar is an attachment that can be added to many labor beds to help support birthing positions. With a birthing bar, you can sit up at any time and squat, leaning on the bar for support. “The birthing bar can be an awesome tool. You can wrap a towel on it to make it easier to use and switch positions,” Wheeler says. That proved to be true for Jennifer, a mom of two from Connecticut, who recalls that “after about two hours of pushing with no success, the birthing bar was put on the bed. It helped me get the resistance I needed to push to the point where the doctor could intervene.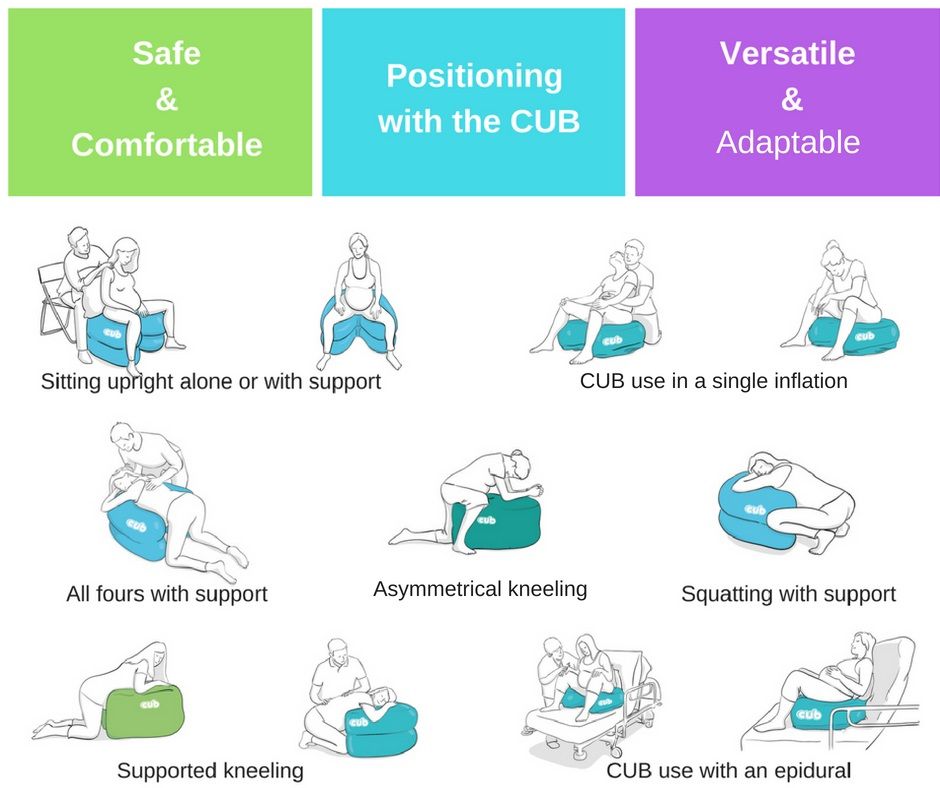 ”
”
Pros:
Cons:
- May not be available at all hospitals
Kneeling birth positions
If baby is facing Mom’s abdomen instead of her back, kneeling can help them turn to get into the proper position. Kneeling is one of the most popular birthing positions because it also gives mom a much-needed break.
Pros:
Cons:
- May be difficult for continuous fetal monitoring
When it comes to labor and birthing positions, discuss all options with your doctor or midwife to land on the ones that will be most comfortable and practical for you. “Every baby and mom responds to positions differently. It’s the job of the labor assistant to help figure out what works best,” Wheeler says. Whichever labor and birthing positions you choose, it’ll all be worth it when baby is finally placed in your arms.
Updated February 2020
Expert bios:
Sara Twogood, MD, FACOG, is a board certified obstetrician-gynecologist at Cedars Sinai Medical Center in Los Angeles. Previously, she held a faculty appointment at USC Keck School of Medicine and practiced general OBGYN in an affiliated private practice. Twogood is also the author of Ladypartsblog.com, which covers topics relating to fertility and pregnancy, and the founder of FemEd, a program designed to empower females through health education.
Previously, she held a faculty appointment at USC Keck School of Medicine and practiced general OBGYN in an affiliated private practice. Twogood is also the author of Ladypartsblog.com, which covers topics relating to fertility and pregnancy, and the founder of FemEd, a program designed to empower females through health education.
Lindsey Bliss is a birth doula and co-founder of Carriage House Birth, a doula agency established in New York City in 2012 that now serves Los Angeles as well.
Rebekah Wheeler, RN, CNM, MPH, is a certified nurse-midwife in the Bay Area, California. She is the founder of the Malawi Women’s Health Collective, a small non-profit organization, and has served on the boards of the California Nurse-Midwifery Association, Planned Parenthood of Rhode Island and the Women’s Health and Education Fund of Southeastern Massachusetts. She holds a Master’s of Public Health and a Master’s of Science in Nursing from Yale University.
Megan Cheney, MD, MPH, is an ob-gyn and the medical director of the Women’s Institute at Banner University Medical Center in Phoenix, Arizona. She earned her medical degree from University of Arizona College of Medicine in 2009.
Please note: The Bump and the materials and information it contains are not intended to, and do not constitute, medical or other health advice or diagnosis and should not be used as such. You should always consult with a qualified physician or health professional about your specific circumstances.
Plus, more from The Bump:
4 Must-Know Strategies for an Easier Labor and Delivery
5 Medication Options for Pain Relief During Labor
What to Expect During the Different Stages of Labor
Baby posture during childbirth, what is the best?
Pregnancy is a stage of hope and joy, but also of fear and uncertainty in a situation that, while natural, is at the same time unusual. Childbirth often proceeds as they wish, but are not afraid. One of the things expectant mothers worry about the most, besides pain, is if the baby fits well in the pelvis and if your posture is adequate for a natural birth.
Childbirth often proceeds as they wish, but are not afraid. One of the things expectant mothers worry about the most, besides pain, is if the baby fits well in the pelvis and if your posture is adequate for a natural birth.
Normally, the baby is placed in the “exit position” from about the eighth month of pregnancy, but this can happen later or even shortly before delivery if the woman has already had children. This is called investment. The child descends and is placed in the mother's pelvis, usually with the head down, but may sometimes assume other positions.
The position of the baby in the uterus can be determined by ultrasound. Experienced midwives can also know the baby's position by feeling the mother's abdomen. However, until At birth, it is impossible to know with certainty what position the baby will take. to go outside because, although the space has decreased in recent weeks, the amniotic fluid allows some mobility. Also, sometimes the same contractions cause babies coming into one position to change at the last minute.
Also, sometimes the same contractions cause babies coming into one position to change at the last minute.
It is very important to know the presentation in which the child is in the last trimester, since the development of childbirth largely depends on this. In 1996, New Zealand midwife Jean Sutton published her book with antenatal educator Pauline Scott. "Understanding and Learning Optimal Fetal Position" (Understanding and Teaching Optimal Fetal Position). In it, they develop the theory that the movements and changes in the posture of the mother in the last weeks of pregnancy can influence the position that the baby assumes at birth. This is vital because, according to this theory, many of the difficulties during childbirth are due to the fact that the baby's presentation is not optimal for its normal development. But what is the optimal fetal position and what can we do to achieve it?
There are three types of presentation of the baby in the womb: head (head down), breech (breech) and transverse (The baby's head is on one side of the mother's uterus, and its back is on the opposite side , forming an angle 90º with the axis of the uterus).
Index
- 1 Head presentation
- 1.1 Front head presentation
- 1.2 Rear head presentation
- 2 GHOGING PRICE or Presentation
- 3 Transverse representation
- 4 What can you make to make your child the optimal situation?
- 4.1 Pay special attention to your posture
- 4.2 Do exercises that promote optimal fetal position.
- 4.3 External head version
- 4.4 Moxibustions
Head presentation
There are two types in this view: front head and back head.
Anterior head presentation
The child lies upside down, with his back to the mother's stomach. This would be p the ideal position for childbirth . The baby's head curves, the chin rests on the chest, and the top of the head (the narrowest part of the head) crosses the birth canal first.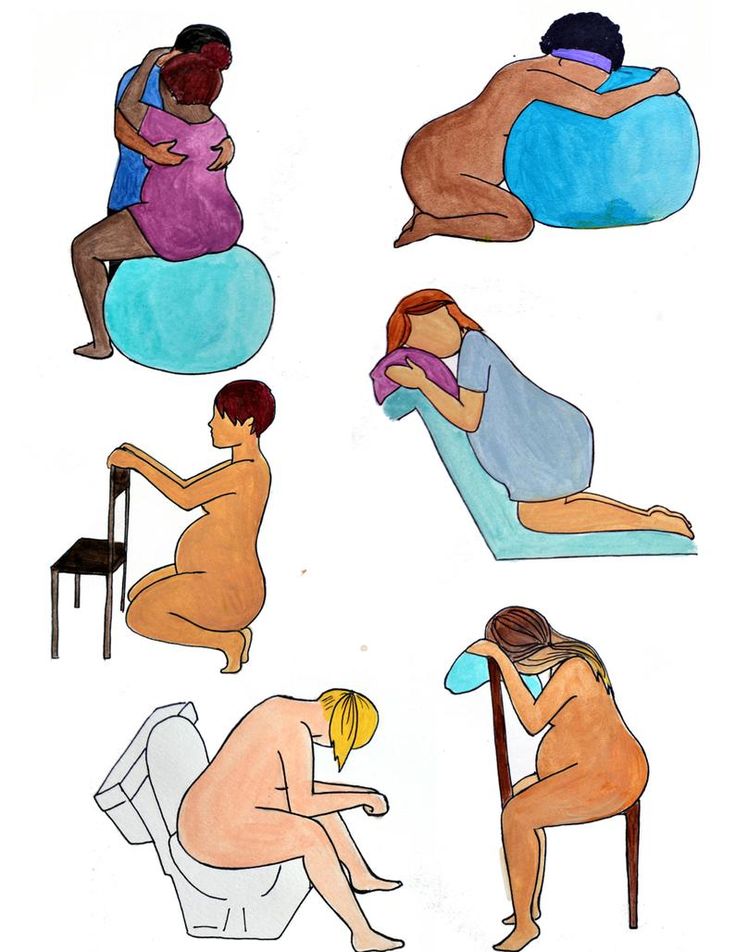
Posterior cephalic presentation
In this presentation, the baby is also head down, but with his back to his mother and his face to his stomach. Thus, the child's head does not bend, and the chin does not tilt. your posture is less flexible when adapting to the birth canal resulting in longer and more painful contractions. This position does not mean that a caesarean section must be performed, the birth can be vaginal, but it will probably take longer because lowering the baby is more difficult.
Breech presentation or breech presentation
In this position, the baby's head is up and the buttocks are down. It is the baby's pelvis is in contact with the mother's pelvis . Usually the baby is placed in the head position between 28 and 32 weeks, but others turn it over several times before delivery, especially if there is excess amniotic fluid. Some, about 3%, never turn and remain in breech or breech position.
The fact that the baby is in a breech position during the last weeks of pregnancy usually causes concern for expectant mothers, since Breech presentation of the child is usually associated with a caesarean section. But is caesarean section really indicated in these cases? Can I try vaginal delivery?
In 2000, the results of a large study called "Break Presentation Test Time". According to this study, in breech presentations caesarean section should be the method of choice over vaginal delivery as it seemed to reduce neonatal morbidity. These results were quickly accepted by the international medical community, which opted to schedule a caesarean section rather than attempt a vaginal delivery when full-term babies were presented in a breech presentation.
While the recommendation for urgent breech testing has been accepted by most important international health organizations, including SEGO (Spanish Society of Gynecology and Obstetrics), there have been a few, such as the Department of Health of the Ministry of Health. of the Basque government, which ruled for non-compliance with these recommendations based on the fact that their health conditions, protocols and professional skills differed from those in the countries participating in the study. For this reason, successful vaginal births are still carried out in settings where experienced medical personnel are available.
of the Basque government, which ruled for non-compliance with these recommendations based on the fact that their health conditions, protocols and professional skills differed from those in the countries participating in the study. For this reason, successful vaginal births are still carried out in settings where experienced medical personnel are available.
After the publication of this study, numerous articles calling into question its reliability since recommendations for assistance with government deliveries were not met in all analyzed deliveries. According to these recommendations, interventions were to be minimal, and all births took place in a high-level medical setting. In 2006, another study was conducted, four times the size of the Term Trial. In this study called PREMODA, it was seen that there were no significant differences in neonatal and perinatal morbidity between breech delivery and cesarean delivery. At this time, SEGO no longer recommends a caesarean section as the first option for a breech baby. Rather, it leaves the door open for vaginal delivery if certain conditions are met: proper development of the fetus and weight less than 4 kg, so that the baby does not look up and that the buttocks or feet are in the canal. birth.
Rather, it leaves the door open for vaginal delivery if certain conditions are met: proper development of the fetus and weight less than 4 kg, so that the baby does not look up and that the buttocks or feet are in the canal. birth.
Transverse view
In this position, the long axis of the fetus forms an angle of 90º with the axis of the uterus, ie the head is on one side of the mother's abdomen and the buttocks are on the opposite side.
In this case, contrary to breech presentation, attempting vaginal delivery is dangerous because there is a high risk of injury and even death for both the baby and the mother.
What can you do to get your child in the best position?
As we have seen, the ideal position for delivery is to place the baby in the forward head position. However, if your baby is presented in other positions, don't be discouraged as there is a chance he will roll over in the final weeks or even during labor. Some Tricks and tricks can help your child stay or head into position. Pay special attention to your posture belly. Try to tilt your pelvis back when you're sitting, making sure your knees are lower than your hips, and avoid positions where you lean back because your back is lower than your belly, preferring to have your baby at the back of your head.
Pay special attention to your posture belly. Try to tilt your pelvis back when you're sitting, making sure your knees are lower than your hips, and avoid positions where you lean back because your back is lower than your belly, preferring to have your baby at the back of your head.
Do exercises that promote optimal fetal position.
Swimming is the perfect exercise for your little one to get into a head position. The best thing is that swim upside down and avoid swimming on your back so that the baby can position itself correctly.
Practice yoga for 10-15 minutes a day, especially cat pose and Muslim pose. Cat Pose is done on all fours, with the arms in line with the shoulders and the knees apart at the hips. The back is arched up with the chin down and then slowly stretched until it is straight as the head is lifted. The Muslim Pose is performed standing on all fours, moving the torso back and pressing the chest to the ground with arms extended forward.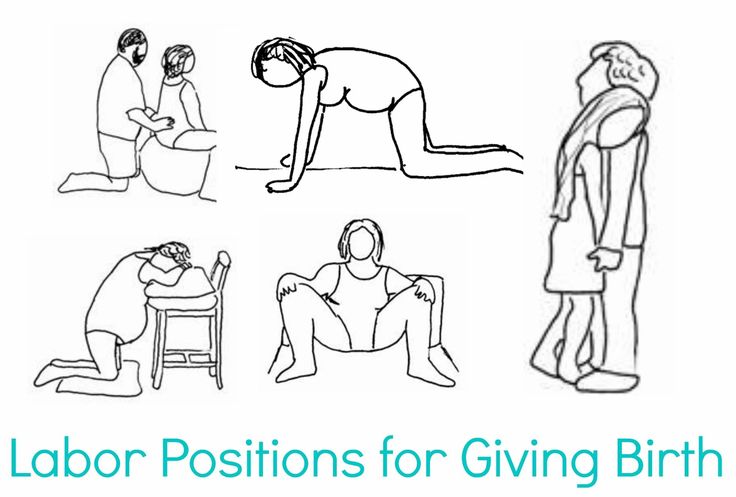
Use one Pilates Ball for rocking exercises especially those where you lean forward.
Take advantage while watching TV by sitting on a chair facing 's back and leaning on top of it. You can also kneel on the floor, leaning on a chair or pillows.
External head version
External head version is a set of maneuvers that are performed on the mother's abdomen, to bring babies into a breech or lateral presentation in the head position. Before it is carried out, an ultrasound is performed to determine the exact position of the baby, the fetal heartbeat is monitored and a medicine is applied that relaxes the muscles of the uterus and facilitates the process. The gynecologist will then proceed to press on different points and gently massage to try to position the baby more cephalad.
The external head version is a fairly safe technique and with a high probability of success, but it has the disadvantage that it can induce labor, so it should only be done in medical settings and with full-term babies.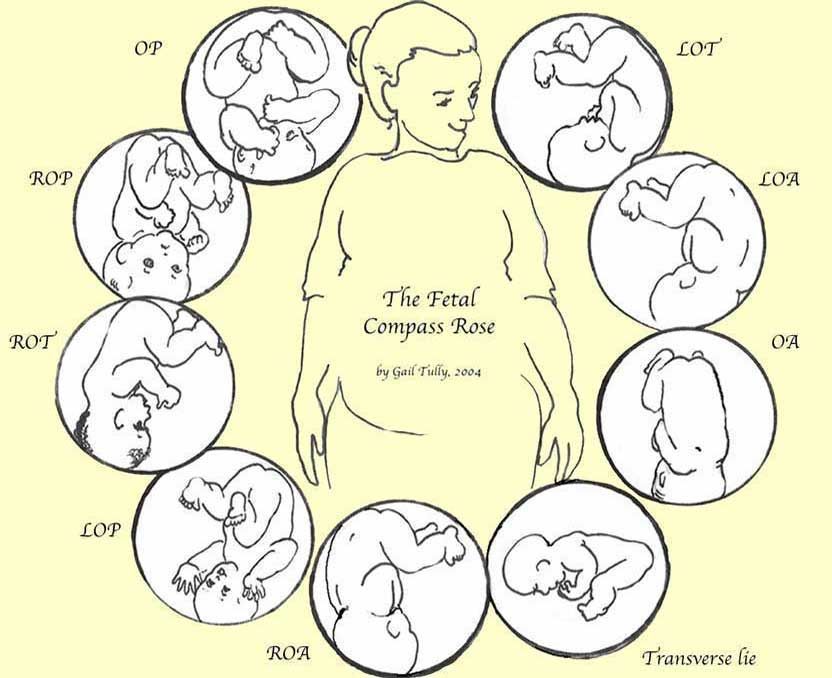
Moxibustion
This method is recommended by WHO for breech presentation and can be performed from 32 weeks. It is a traditional Chinese medicine method consisting of to stimulate various points of the body with the heat from the combustion of wormwood (moxa) , an herb that stimulates pelvic and uterine circulation, as well as stimulation of the adrenal cortex, which ultimately stimulates fetal activity. If the child is in breech presentation, mark stimulate is the outer area of the pinky nail . The success rate is quite high, as shown by various studies, and unlike the external head version, it does not have the disadvantage of being able to induce labor.
As you can see, until the last moment, there is a chance that your child will turn around, and you will have various resources at hand to help him. In principle there is no need to prescribe a caesarean section. In addition, this is also associated with risks, as it is a surgical procedure, so the benefit-risk ratio must be assessed. In any case, if it is necessary, you should know that there is no need to schedule it, since it can be done after the delivery has started. In this way, your baby will benefit from previous births, which will help him adapt to the ectopic environment. If your child is in a breech or lateral presentation, the first thing to do is to remain calm, because all is not lost. And above all, regardless of your position, try to enjoy the unique and unrepeatable moments that pregnancy offers you.
In any case, if it is necessary, you should know that there is no need to schedule it, since it can be done after the delivery has started. In this way, your baby will benefit from previous births, which will help him adapt to the ectopic environment. If your child is in a breech or lateral presentation, the first thing to do is to remain calm, because all is not lost. And above all, regardless of your position, try to enjoy the unique and unrepeatable moments that pregnancy offers you.
consequences for the child in case of incorrect position
January 18, 2022
47325
36
6
Breech presentation for most expectant mothers is a very disturbing moment - how the child will be born, is a caesarean section always indicated in such cases, what complications are possible. Let's answer these and many other questions in this article.
Breech presentation of the fetus is one of the options for the location of the child in the uterus of the mother. If we could look into a woman's belly, we would see a child who seems to be "sitting" in the uterus, and his head is pointing up. Normally, breech presentation lasts up to 32 weeks, and then the baby, as a rule, turns over and directs the head to the birth canal.
If we could look into a woman's belly, we would see a child who seems to be "sitting" in the uterus, and his head is pointing up. Normally, breech presentation lasts up to 32 weeks, and then the baby, as a rule, turns over and directs the head to the birth canal.
Article content
- Can a woman determine the presentation of the fetus?
- What is breech presentation
- Common causes of presentation
- How to determine breech presentation
- What to do to make the child roll over
- What can a woman do
- What can an obstetrician do
- What can a doctor do
- FAQ
Can a woman identify fetal presentation?
Only an experienced doctor who leads the pregnancy can determine the breech presentation, and the assumption is confirmed with the help of ultrasound.
In the event that the baby is positioned “incorrectly”, the doctor may recommend special exercises to turn the baby over into the optimal position for childbirth. This is important, because it is at 32-34 weeks that you need to undergo an examination and make sure that the baby has taken the right direction.
What is breech presentation
Doctors distinguish two types of breech presentation:
| Gluteal | In such a situation, during childbirth at the birth of a baby, the buttocks are the first to be born. The legs are located along the body. This option is the most favorable, rarely gives complications, so childbirth is most often carried out naturally. |
| foot | At birth, the legs appear first, such a presentation. |
Common causes of presentation
Of course, any expectant mother has a question - why does breech presentation occur. There are many reasons for this, the main ones are:
There are many reasons for this, the main ones are:
- multiple pregnancy - when there are two or three babies in the uterus, it is difficult for them to move and turn over head down
- polyhydramnios - in such a situation, the baby can move a lot and simply not take the correct position before childbirth
- oligohydramnios - in a situation where there is little amniotic fluid, the child simply cannot take the correct position
- cord entanglement
- fibroids or other diseases of the uterus
How to determine breech presentation
It is impossible to independently determine the position of the child.
To understand what kind of presentation a child has, you can use:
| Visual examination and palpation of the abdomen by an experienced specialist | So he determines where the head is and where the legs of the fetus are |
| Feeling the baby through the vagina | This method is used if a woman has entered an emergency delivery and is already in them. |
| ultrasound | The most reliable way to determine the position of the baby. The procedure is carried out at 32-34 weeks, when the baby takes its final position |

Example
A pregnant woman at 38 weeks was diagnosed with breech presentation. The woman was advised certain exercises in order to delicately turn the fetus over. The task was unsuccessful, so the specialist tried to make an obstetric coup, however, this did not lead to the desired result. As a result, the doctor decided to carry out the delivery by surgery and perform a caesarean section. The operation was successful, mother and child are doing well.
How to make a child roll over
In this matter, three directions need to be considered: what the woman herself can do, what her obstetrician-gynecologist can do, and what the doctor in charge of childbirth can do.
What a woman can do
Let's figure out what may depend on the future mother herself, and what she can do.
- First, tune in a positive way. The state of the child largely depends on the psychological state of the mother, so it is not recommended to be nervous and anxious.
- Second, talk to your child and ask him to roll over. Skeptics may scoff at such advice, but experienced psychologists and obstetricians say that this method works.
- And finally, do special exercises, for example, turns. Starting position - lying on your back, legs slightly bent at the knees. Gently and smoothly, without jerking, you need to turn on your right side and lie down in this position for 2 minutes. After that, roll over to your left side and also lie down. Repeat 5 times for each side. All movements should be as delicate as possible.
What a midwife can do
If mom did not succeed in stimulating the coup, this is absolutely normal. At a period of more than 35 weeks, an obstetrician takes over, who tries to make the so-called obstetric coup. During the procedure, with the help of special manipulations, he acts on the woman's stomach, trying to give the fetus the optimal position for childbirth. However, it is impossible not to notice that most of the babies "inverted by the midwife" will soon return to the breech presentation.
However, it is impossible not to notice that most of the babies "inverted by the midwife" will soon return to the breech presentation.
What a doctor can do
Quite often, in order to reduce the risks for both the mother and her baby, the doctor decides to perform a caesarean section. However, many women give birth naturally.
The choice of birth management is always personalized, taking into account the individual characteristics of the mother and her child. It is important to choose a good specialist at the initial stage of pregnancy.
FAQ
Breech presentation of the fetus at the 20th week of pregnancy - is it dangerous?
+
Absolutely not. We begin to talk about the fact that breech presentation is a conditional pathology no earlier than 32 weeks. Until this time, the child may roll over, and sometimes more than once. I will say even more - at this time the child is most often located with his legs down and this is absolutely normal.
Foot presentation - is it the wrong position of the fetus?
+
What gestational age are we talking about? Initially, the child “tumbles” in his mother’s stomach, then most often he is just the same in a foot or breech presentation, when his legs are down and his head is up. And only closer to childbirth, a coup usually occurs and the child is located head down - at the entrance to the birth canal. If this does not happen, we can talk about the breech / foot / breech presentation.
What are the consequences of breech presentation for a child?
+
In general, with the correct management of childbirth, there will be no negative consequences for the child. He can suffer only if the doctor chooses the wrong method of obstetric care. In all other respects, there are no problems, the fetus develops absolutely normally.
How to understand that the child turned upside down?
+
The position of the child in the womb can only be determined by a competent specialist.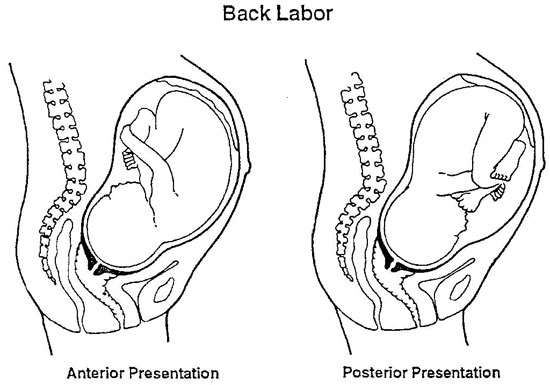 The most effective and reliable method is ultrasound.
The most effective and reliable method is ultrasound.
And is there an unstable position of the fetus?
+
The fetus rotates many times during the entire pregnancy, at the end of the third trimester it usually turns head down and takes this position until delivery. However, it also happens that the child rolls over several times. In this case, we can talk about the unstable position of the fetus.
What is an obstetric revolution?
+
During the procedure, with the help of special manipulations, he acts on the woman's stomach, trying to give the fetus the optimal position for childbirth. However, it is impossible not to notice that most of the babies "inverted by the midwife" will soon return to the breech presentation.
Breech presentation of the fetus at 34 weeks of gestation - normal or pathological?
+
Breech presentation at this time is not a "final verdict. " the baby can still roll over. If this does not happen, the doctor will assess the size and position of the child closer to the MDD and decide on the tactics of childbirth.
" the baby can still roll over. If this does not happen, the doctor will assess the size and position of the child closer to the MDD and decide on the tactics of childbirth.
How to understand if the child turned upside down?
+
You yourself will not be able to understand this, or at least be sure that the coup has happened. I would recommend that you do an ultrasound - with the help of this study it will become known in which presentation your baby is.
We publish only verified information
Article author
Menshikova Maria Viktorovna obstetrician-gynecologist
Experience 38 years
Consultations 1816
Art. 46
46
Specialist with extensive practical experience. He has a certificate of a mammologist, a certificate of professional certification. Participates in foreign business trips and individual training programs (Los Angeles).
- 1982 - 1986 NPO MONIIAG - obstetrician-gynecologist
- 1987 - 1989 VNITs OZMIR - obstetrician-gynecologist
- 1989 - 1992 departmental polyclinic st. Moscow - Kurskaya - obstetrician-gynecologist
- 1992 - 2001 NCO MONIIAG - obstetrician-gynecologist
- 2007 - 2008 NP KMIKM - doctor administrator
- 2009 - 2013 Pereslavl Central District Hospital, women's consultation - obstetrician-gynecologist
- 2020 to present Teledoctor24 LLC - doctor - consultant (gynecologist)
Sources
- ... Savelyeva G.M., Shalina R.I., Panina O.B.
 "Obstetrics" - M .: "GEOTAR - Media", 2010
"Obstetrics" - M .: "GEOTAR - Media", 2010 - ... Chernukha E.A., Puchko T.K. "Pelvic presentation of the fetus", a guide for doctors - M .: "GEOTAR - Media", 2007
- ... Clinical protocol "Management of pregnancy and childbirth in breech presentation of the fetus" // Institute of Health and Family. Project "Mother and Child" - 2011
Share:
Category: Pregnancy and childbirth
About health Pregnancy and childbirth About children healthy lifestyle Psychology Neurology Gastroenterology Personal care Medicines and dietary supplementsPrevious article
Salt room
Next article
Diastasis after childbirth
Other related articles
Monakhova Albina Petrovna
10.