Nt scan what is normal range
Normal reference range of fetal nuchal translucency thickness in pregnant women in the first trimester, one center study
J Res Med Sci. 2015 Oct; 20(10): 969–973.
doi: 10.4103/1735-1995.172786
,,,1 and 2
Author information Article notes Copyright and License information Disclaimer
Background:
Considering that establishment of reference value of nuchal translucency (NT)-related to the crown rump length (CRL) during the first trimester will be helpful for determining an appropriate cutoff level for screening of increased NT thickness-related abnormalities, we determined the NT thickness and investigated its relation with different chromosomal and nonchromosomal abnormalities among a large sample size of pregnant Iranian women.
Materials and Methods:
In this analytic cross-sectional study, pregnant women who were in their first trimester were enrolled at their antenatal visit. Using an abdominal ultrasonography, the fetal NT thickness of the studied population was measured. Those with increased NT thickness were determined. The reference value of NT thickness (5th, 25th, 50th, 75th, and 95th percentiles) within each 5-mm range of CRL and during the 11th, 12th, and 13th gestational weeks were determined. The presences of the different chromosomal and nonchromosomal abnormalities were compared in women with different percentiles of NT thickness who underwent amniocentesis and those who did not.
Results:
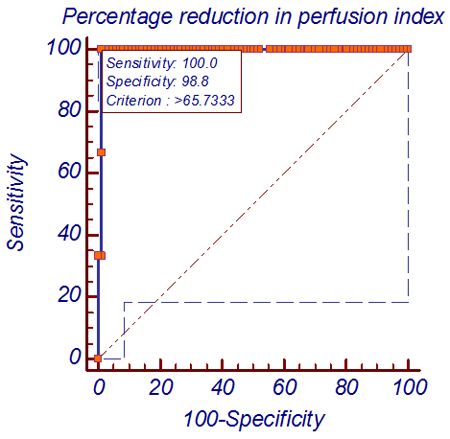
1,614 pregnant women were evaluated. The mean NT thickness was 1.30 ± 0.54 mm. Increased NT thickness >2 mm and >95th percentile according to their gestational age (GA) was detected in 89 (5.5%) and 58 (3.6%) pregnant women. The reference 95th percentile value range for NT was 1.8-2.35 and increased NT thickness according to our obtained values was associated significantly with chromosomal abnormalities.
Conclusion:
The obtained reference range in our studied population was different from that reported for other ethnic groups and it is suggested that using this values are more favorable for screening of chromosomal abnormalities during the first trimester of pregnancy than the recommended single cutoff value.
Keywords: Crown rump length (CRL), nuchal translucency (NL), reference values
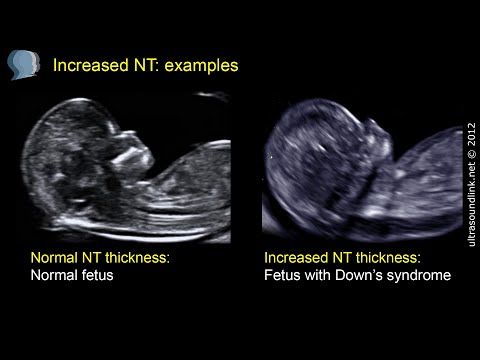
Nuchal translucency (NT) is the normal fluid-filled subcutaneous space between the back of the fetal skin and the overlying skin.[1] NT is visible and can be measured by ultrasonographic imaging between 11 weeks and 14 weeks gestation.[2] Increased NT is associated with different fetal chromosomal and nonchromosomal abnormalities. There is growing evidence that increased NT thickness during the first trimester of pregnancy in a chromosomally normal fetus is associated with numerous fetal structural abnormalities, genetic syndromes, heart defects, and poor perinatal outcomes such as miscarriage and intrauterine death.[3,4,5]
The first definition for increased NT was a measure >95th percentile for a given crown rump length (CRL) and a NT value of 2.5-3 mm, which was reported as a normal range for the marker. Recently, some studies indicated that NT >99th percentile or NT value that exceeds of 3. 5 mm are associated with the most common adverse outcomes.[6,7]
5 mm are associated with the most common adverse outcomes.[6,7]
The utility of NT as a sensitive and noninvasive ultrasonographic marker for screening and detection of aneuploidies and major structural anomalies in modern obstetrical practice has been demonstrated recently. Its use as a new screening method for the mentioned purposes has been developed in many developed countries.[8,9,10]
Since the introduction of NT thickness, several studies worldwide have determined the normal range of NT in different populations. The results were different regarding the normative value of NT. One of the explanations for the reported great variety of NT thickness range is ethnic variation.[11,12,13,14,15] However, there are still controversies regarding the role of ethnicity on the value of NT. Some reported a significant role of ethnicity in this regard, whereas others did not support the association.[16,17] However, recently the establishment of reference value for NT in different populations was performed.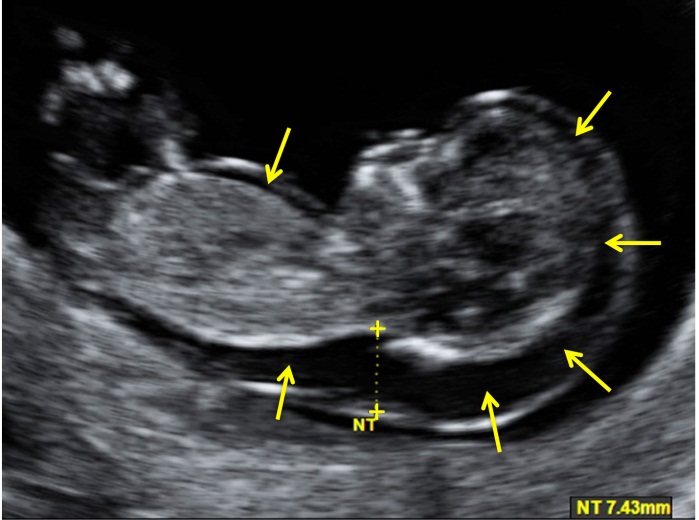 It is suggested that ethnic and region-specific reference value of NT could have a significant impact on its screening efficacy and using a single cutoff for fetal NT could not be an appropriate tool in this field.[18]
It is suggested that ethnic and region-specific reference value of NT could have a significant impact on its screening efficacy and using a single cutoff for fetal NT could not be an appropriate tool in this field.[18]
So considering that establishment of reference value of NT related to the CRL during the first trimester will be helpful for determining an appropriate cutoff level for screening of increased NT thickness-related abnormalities and the presence of few reports in this field among the Iranian population, in this study we determined the reference values of NT thickness among Isfahani pregnant women to evaluate the role of ethnicity on the normative value of NT as well as the association of increased NT thickness with chromosomal and nonchromosomal abnormalities during the first trimester.
In this analytic cross-sectional study, pregnant women referred to a private radiology center for ultrsonographic assessment during the antenatal visit in their first trimester were enrolled. The study was performed from January 2013 to December 2013 in Isfahan, Isfahan Province, Iran.
The study was performed from January 2013 to December 2013 in Isfahan, Isfahan Province, Iran.
The protocol of the study was approved by the Regional Ethics Committee of Isfahan University of Medical Sciences.
Pregnant women with gestational age (GA) of 11-13 weeks and 6 days and/or CRL 45-84 mm were included.
The pregnant women were selected by the consecutive method. Those who did not agree to have the ultrasonography performed, with multiple pregnancies, fetal malformation, and those with inappropriate cooperation were excluded. Written informed consent was obtained from all the selected participants. The selected pregnant women underwent abdominal ultrasonography. The sonography was performed by an expert radiologist. The fetal NT thickness of the studied population was measured.
Those with NT thickness of 2 mm were considered as women with increased NT thickness.[19]
The mean of CRL and GA were compared in women with and without increased NT thickness.
The reference value of NT thickness (5th, 25th, 50th, 75th, and 95th percentiles) within each 5-mm range of CRL and during the 11th, 12th, and 13th gestational weeks were determined.
Women with NT thickness of >95th percentile were determined. The women were followed up and fetal outcomes were evaluated by the neonatologists at birth. The presence of different chromosomal abnormalities as well as nonchromosomal abnormalities including cardiac malformation, genitourinary or renal abnormalities, diaphragmatic hernia, spontaneous miscarriage, and intrauterine fetal death (IUFD) were compared in women with different percentiles of NT thickness who underwent amniocentesis and those who did not.
Ultrasonographic measurements
The ultrasonographic measurements were performed in pregnant women in a supine position.
Fetal CRL and NT thickness measurements were performed by transabdominal ultrsonography using a multi fz: 3. 5 MHz tranduser (GE Volusun 730). The measurement was performed based on the criteria recommended by the Fetal Medicine Foundation (FMF).[20] According to the criteria, the fetus should be in a neutral position, with the head aligned with the spine in a way that fetus occupied at least 75% of the image. NT was defined as the black area between the inner skin outlines echo and the outer border of the soft tissue overlying the cervical spine.
5 MHz tranduser (GE Volusun 730). The measurement was performed based on the criteria recommended by the Fetal Medicine Foundation (FMF).[20] According to the criteria, the fetus should be in a neutral position, with the head aligned with the spine in a way that fetus occupied at least 75% of the image. NT was defined as the black area between the inner skin outlines echo and the outer border of the soft tissue overlying the cervical spine.
The maximal thickness of the black area was measured with caliper placed on the inner borders of the NT space, perpendicular to the long axis of the fetus when a sagittal section with a neutral position of the fetus was obtained. The measurements were recorded to the nearest 0.1-mm interval. At least three NK measurements were taken and the largest was recorded.
CRL was measured at the same time and recorded.
Statistical analysis
Data were analyzed using Statistical Package for the Social Sciences (SPSS) version 21 (SPSS Inc.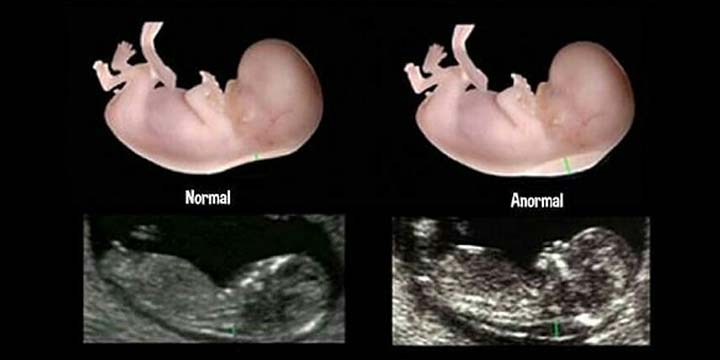 , Chicago, IL, USA). Using regression equation, the expected 5th, 25th, 50th, 75th, and 5th percentile values of NT thickness according to the CRL categories of CRL (5-mm interval) and GA (11th, 12th, and 13th weeks) were obtained. Quantitive and qualitative values were compared using the t-test and chi-square test, respectively. P value of <0.05 was considered to be statistically significant.
, Chicago, IL, USA). Using regression equation, the expected 5th, 25th, 50th, 75th, and 5th percentile values of NT thickness according to the CRL categories of CRL (5-mm interval) and GA (11th, 12th, and 13th weeks) were obtained. Quantitive and qualitative values were compared using the t-test and chi-square test, respectively. P value of <0.05 was considered to be statistically significant.
During this study, 1,614 pregnant women were evaluated. Among the studied pregnant women 382 (23.7%), 871 (54.0%), and 361 (22.4) were in the 11th, 12th, and 13th gestational week. The mean of GA, CRL, and NT thickness in the studied population were 12.46 ± 0.62 weeks, 59.35 ± 8.35 mm, and 1.30 ± 0.54 mm, respectively. Pearson correlation test indicated that there was a significant positive correlation between NT and CRL (r = 0.238, P < 0.001), NT and GA (r = 0. 24, P < 0.001 and GA) and CRL (r = 0.8, P < 0.001).
24, P < 0.001 and GA) and CRL (r = 0.8, P < 0.001).
Increased NT thickness (NT >2 mm) was detected in 89 (5.5%) pregnant women. The mean of CRL and GA in pregnant women with normal and increased NT thickness are presented in .
Table 1
Mean ± SD of CRL and GA in pregnant women with normal and increased NT thickness
Open in a separate window
The expected 5th, 25th, 50th, 75th, and 95th percentile values of NT thickness to CRL and GA are listed in Tables and . Using the obtained reference value of NT, 58 (3.6%) pregnant women were determined as those with NT thickness >95th percentile according to their GA. During follow-up, 31/58 (53.4%) underwent amniocentesis. Distribution of chromosomal and nonchromosomal abnormalities in pregnant women with NT thickness >95th percentile according to their GA in total and among those with and without amniocentesis are presented in . Frequency of chromosomal abnormalities were significantly higher in those pregnant women with increased NT thickness who underwent the amniocentesis procedure (P = 0.001). The frequency of different nonchromosomal abnormalities were not significantly different between the two studied groups (P > 0.05).
Frequency of chromosomal abnormalities were significantly higher in those pregnant women with increased NT thickness who underwent the amniocentesis procedure (P = 0.001). The frequency of different nonchromosomal abnormalities were not significantly different between the two studied groups (P > 0.05).
Table 2
The expected 5th, 25th, 50th, 75th, and 95th percentile values of NT thickness (mm) to CRL
Open in a separate window
Table 3
The expected 5th, 25th, 50th, 75th, and 95th percentile values of NT thickness (mm) to gestational age (GA)
Open in a separate window
Table 4
Distribution of chromosomal and nonchromosomal abnormalities in pregnant women with NT thickness >95th percentile according to their GA in total and among those with and without amniocentesis
Open in a separate window
In this study, we determined the reference values of NT thickness among pregnant Isfahani women to evaluate the role of ethnicity on the normative value of NT as well as the association of increased NT thickness with chromosomal and nonchromosomal abnormalities during the first trimester. The results indicated that the reference 95th percentile value range for NT was 1.8-2.35 and increased NT thickness according to our obtained values was associated significantly with chromosomal abnormalities.
The results indicated that the reference 95th percentile value range for NT was 1.8-2.35 and increased NT thickness according to our obtained values was associated significantly with chromosomal abnormalities.
Several reports from different parts of the worlds and Iran have demonstrated the utility of NK measurement for screening different chromosomal and nonchromosomal abnormalities.[20,21,22,23]
Most of the studies have used the recommended definition for NT thickness by the FMF (i.e., 2.5-3 mm),[6] whereas recent studies reported that using NT thickness as a continuous variable was more appropriate than using a single cutoff value for the fetal NT and consequently, the outcomes of its increased values and screening programs.[18] So, establishment of reference values of NT have been developed in different regions and ethnic groups worldwide.
Though there were studies in Iran, which investigated the association between increased NT value and Down syndrome[22] and adverse pregnancy outcome including miscarriage, fetal loss, and fetal abnormalities,[23] there was not any study, which reported the normative value of NT thickness for the Iranian population. So, this study was designed to determine the ethnic specific reference value of NT thickness for pregnant Iranian women. Our results indicated that the median NT thicknesses for a CRL between 45 mm and 80 mm ranged from 1.00 to 1.65 mm, and the 95th percentiles ranged from 1.8 to 2.35 mm. The median NT thickness for GA were 1.0 mm, 1.2 mm, and 1.4 mm for gestational age of 11 weeks, 12 weeks, and 13 weeks, respectively, and the 95th percentiles of NT thickness were 1.8, 1.9, and 2.2 for gestational age of 11 weeks, 12 weeks, and 13 weeks, respectively.
So, this study was designed to determine the ethnic specific reference value of NT thickness for pregnant Iranian women. Our results indicated that the median NT thicknesses for a CRL between 45 mm and 80 mm ranged from 1.00 to 1.65 mm, and the 95th percentiles ranged from 1.8 to 2.35 mm. The median NT thickness for GA were 1.0 mm, 1.2 mm, and 1.4 mm for gestational age of 11 weeks, 12 weeks, and 13 weeks, respectively, and the 95th percentiles of NT thickness were 1.8, 1.9, and 2.2 for gestational age of 11 weeks, 12 weeks, and 13 weeks, respectively.
The distribution of the NT thickness for CRL has been reported in many studies. The median NT thicknesses has been reported to be 1.2-1.9 mm, 1.22-2.10 mm, and 1.19-1.73 mm for a CRL between 45 mm and 80 mm in Japan, Korea, and Brazil, respectively.[11,12,13] Our reported median value was lower than the other reports.
The 95th NT thickness percentiles have been reported to be 2.1-3.2 mm, 2.14-2.3 mm, 1.57-2. 10 mm, 1.00-2.90 mm, and 1.84-2.35 mm for a CRL between 45 mm and 80 mm in Japan, Korea, Brazil, Thailand, and China, respectively.[11,12,13,14,15] Our results were similar to the reported reference value range of Brazil.[13] Although there was no report from the Eastern Mediterranean region in this field, the values were not similar to the values reported from the Asian countries.
10 mm, 1.00-2.90 mm, and 1.84-2.35 mm for a CRL between 45 mm and 80 mm in Japan, Korea, Brazil, Thailand, and China, respectively.[11,12,13,14,15] Our results were similar to the reported reference value range of Brazil.[13] Although there was no report from the Eastern Mediterranean region in this field, the values were not similar to the values reported from the Asian countries.
Reported variations in the index measurements in the different studies might have been due to factors such as radiologist experience, quality of the ultrasound, method of measurement, and an inappropriate fetal and nuchal cord position. In addition, as mentioned by Kor-anantaku et al. in Thailand some investigators have considered the average of two or three measurements of NT thickness, whereas others considered the largest measurement.[14]
There are controversial reports regarding the impact of ethnicity on NT thickness values and its utility for screening. Thilaganathan et al. have investigated the possible role of ethnicity on NT screening and concluded that the reported differences could not have a significant impact in this regard.[24] Many other studies have also showed that ethnic differences in NT measurements are not clinically significant, especially when it used for screening of Down syndrome.[17,24,25] However, it seems that using ethnic-specific reference values of NT thickness could help us in the first trimester screening programs mainly for chromosomal abnormality, especially when they are integrated with other ultrasonographic and biochemical measurements.
have investigated the possible role of ethnicity on NT screening and concluded that the reported differences could not have a significant impact in this regard.[24] Many other studies have also showed that ethnic differences in NT measurements are not clinically significant, especially when it used for screening of Down syndrome.[17,24,25] However, it seems that using ethnic-specific reference values of NT thickness could help us in the first trimester screening programs mainly for chromosomal abnormality, especially when they are integrated with other ultrasonographic and biochemical measurements.
In this study using the single cutoff value of 2 mm, 5.5% of the studied pregnant women were considered to have high-risk pregnancy and after using our obtained reference value the rate decreased to 3.6%. Thus, it seems that using normative values of NT thickness is more useful for the first trimester screening and it could optimize the screening results by reducing false positive cases.
In addition, there was significant association between performing the amniocentesis procedure and detection of chromosomal abnormalities among women with increased NT thickness.
The advantage of the current study was a larger sample size of enrolled pregnant women.
The limitation of the current study was that we did not determine the sex-specific reference value of 95th percentiles of NT and its association with both chromosomal and nonchromosomal abnormalities. We followed up only pregnant women with increased NT thickness and did not determine the frequency of the mentioned abnormalities in pregnant women with normal NT. It was due to the reason that follow-up of that large a sample size was not assessable in the framework of the current study. In addition, we enrolled the patients who were referred to a single referral radiologic center, which could not be a representative sample of the whole population. It is suggested that the large sample size of the studied population could partially alleviate the abovementioned limitation.
Further, the planning of further studies that also determine the 99th percentile values of NT thickness is recommended because recent studies demonstrated that chromosomal and nonchromosomal abnormalities are mainly associated with the 99th percentile value of NT thickness.[7]
The results of our study indicated the reference value of NT thickness in a large sample size of Isfahani pregnant women. The obtained reference range in our studied population was different from that reported for other ethnic groups and it is suggested that using this values are more favorable for screening of chromosomal abnormalities during the first trimester of pregnancy than the recommended single cutoff value. The relation between increased NT thicknesses with chromosomal abnormalities also confirms its utility. The results of the current study could be used as baseline information for other follow-up studies and designing first trimester screening programs.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
All authors contributed in the conception of the work, conducting the study, revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work.
The study was supported by Isfahan University of Medical Sciences (research project number; 393486).
1. Nicolaides KH, Azar G, Byrne D, Mansur C, Marks K. Fetal nuchal translucency: Ultrasound screening for chromosomal defects in first trimester of pregnancy. BMJ. 1992;304:867–9. [PMC free article] [PubMed] [Google Scholar]
2. Szabó J, Gellén J. Nuchal fluid accumulation in trisomy-21 detected by vaginosonography in first trimester. Lancet. 1990;336:1133. [PubMed] [Google Scholar]
3. Vogel M, Sharland GK, McElhinney DB, Zidere V, Simpson JM, Miller OI, et al. Prevalence of increased nuchal translucency in fetuses with congenital cardiac disease and a normal karyotype. Cardiol Young. 2009;19:441–5. [PubMed] [Google Scholar]
4. Bilardo CM, Müller MA, Pajkrt E, Clur SA, van Zalen MM, Bijlsma EK. Increased nuchal translucency thickness and normal karyotype: Time for parental reassurance. Ultrasound Obstet Gynecol. 2007;30:11–8. [PubMed] [Google Scholar]
Bilardo CM, Müller MA, Pajkrt E, Clur SA, van Zalen MM, Bijlsma EK. Increased nuchal translucency thickness and normal karyotype: Time for parental reassurance. Ultrasound Obstet Gynecol. 2007;30:11–8. [PubMed] [Google Scholar]
5. Saldanha FA, Brizot Mde L, Moraes EA, Lopes LM, Zugaib M. Increased fetal nuchal translucency thickness and normal karyotype: Prenatal and postnatal follow-up. Rev Assoc Med Bras. 2009;55:575–80. [PubMed] [Google Scholar]
6. Salman Guraya S. The associations of nuchal translucency and fetal abnormalities; significance and implications. J Clin Diagn Res. 2013;7:936–41. [PMC free article] [PubMed] [Google Scholar]
7. Souka AP, Von Kaisenberg CS, Hyett JA, Sonek JD, Nicolaides KH. Increased nuchal translucency with normal karyotype. Am J Obstet Gynecol. 2005;192:1005–21. [PubMed] [Google Scholar]
8. Stefanovic V, Äyräs O, Eronen M, Paavonen1 J, Tikkanen M. Clinical utility of nuchal translucency screening. Res Rep Neonatol. 2014;4:169–76. [Google Scholar]
[Google Scholar]
9. Snijders RJ, Noble P, Sebire N, Souka A, Nicolaides KH. UK Multicentre Project on assessment of risk of trisomy 21 by maternal age and fetal nuchal-translucency thickness at 10-14 weeks of gestation. Fetal Medicine Foundation First Trimester Screening Group. Lancet. 1998;352:343–6. [PubMed] [Google Scholar]
10. Miron P, Côté YP, Lambert J. Nuchal translucency thresholds in prenatal screening for down syndrome and trisomy 18. J Obstet Gynaecol Can. 2009;31:227–35. [PubMed] [Google Scholar]
11. Hasegawa J, Nakamura M, Hamada S, Matsuoka R, Ichizuka K, Sekizawa A, et al. Distribution of nuchal translucency thickness in Japanese fetuses. J Obstet Gynaecol Res. 2013;39:766–9. [PubMed] [Google Scholar]
12. Chung JH, Yang JH, Song MJ, Cho JY, Lee YH, Park SY, et al. The distribution of fetal nuchal translucency thickness in normal Korean fetuses. J Korean Med Sci. 2004;19:32–6. [PMC free article] [PubMed] [Google Scholar]
13. Araujo Júnior E, Pires CR, Martins WP, Nardozza LM, Filho SM. Reference values of nuchal translucency thickness in a Brazilian population sample: Experience from a single center. J Perinat Med. 2014;42:255–9. [PubMed] [Google Scholar]
Reference values of nuchal translucency thickness in a Brazilian population sample: Experience from a single center. J Perinat Med. 2014;42:255–9. [PubMed] [Google Scholar]
14. Kor-Anantakul O, Suntharasaj T, Suwanrath C, Chanprapaph P, Sirichotiyakul S, Ratanasiri T, et al. Distribution of normal nuchal translucency thickness: A multicenter study in Thailand. Gynecol Obstet Invest. 2011;71:124–8. [PubMed] [Google Scholar]
15. Sun Q, Xu J, Hu SQ, Chen M, Ma RM, Lau TK, et al. Distribution and normal reference range of fetal nuchal translucency thickness in Kunming pregnant women in the first trimester. Zhonghua Fu Chan Ke Za Zhi. 2012;47:514–7. [PubMed] [Google Scholar]
16. Huang T, Wang F, Boucher K, O’Donnell A, Rashid S, Summers AM. Racial differences in first trimester nuchal translucency. Prenat Diagn. 2007;27:1174–6. [PubMed] [Google Scholar]
17. Chen M, Lam YH, Tang MH, Lee CP, Sin SY, Tang R, et al. The effect of ethnic origin on nuchal translucency at 10-14 weeks of gestation. Prenat Diagn. 2002;22:576–8. [PubMed] [Google Scholar]
Prenat Diagn. 2002;22:576–8. [PubMed] [Google Scholar]
18. Taipale P, Hiilesmaa V, Salonen R, Ylöstalo P. Increased nuchal translacency as a marker for fetal chromosomal defects. N Engl J Med. 1997;337:1654–8. [PubMed] [Google Scholar]
19. Kim SM, Jun JK. Simplified protocol of nuchal translucency measurement: Is it still effective? Obstet Gynecol Sci. 2013;56:307–11. [PMC free article] [PubMed] [Google Scholar]
20. Kagan KO, Avgidou K, Molina FS, Gajewska K, Nicolaides KH. Relation between increased fetal nuchal translucency thickness and chromosomal defects. Obstet Gynecol. 2006;107:6–10. [PubMed] [Google Scholar]
21. Barati M, Zargar M, Masihi S, Taherpour S. Evaluation of nuchal translucency measurement in first trimester pregnancy. Int J Fertil Steril. 2011;5:35–8. [PMC free article] [PubMed] [Google Scholar]
22. Elahifar MA, Hasanzadeh M, Dahmardeh H, Elahifar A. The relationship between thickness of nuchal translucency and Down syndrome in the first trimester of pregnancy. Zahedan J Res Med Sci. 2012;14:26–8. [Google Scholar]
Zahedan J Res Med Sci. 2012;14:26–8. [Google Scholar]
23. Tahmasebpour A, Rafiee NB, Ghaffari S, Jamal A. Increased nuchal translucency and pregnancy outcome. Iran J Public Health. 2012;41:92–7. [PMC free article] [PubMed] [Google Scholar]
24. Thilaganathan B, Khare M, Williams B, Wathen NC. Influence of ethnic origin on nuchal translucency screening for Down's syndrome. Ultrasound Obstet Gynecol. 1998;12:112–4. [PubMed] [Google Scholar]
25. Hsu JJ, Hsieh CC, Chiang CH, Lo LM, Hsieh TT. Preliminary normal reference values of nuchal translucency thickness in Taiwanese fetuses at 11-14 weeks of gestation. Chang Gung Med J. 2003;26:12–9. [PubMed] [Google Scholar]
Chromosomally and Anatomically Normal Fetuses With Increased First Trimester Nuchal Translucency Conceived by ICSI
Iran J Radiol. 2015 Apr; 12(2): e7157.
Published online 2015 Apr 21. doi: 10.5812/iranjradiol.7157
1,* and 1
Author information Article notes Copyright and License information Disclaimer
Nuchal translucency (NT) measurements in the first trimester screening between 11 and 14 weeks’ gestation are regarded as a clear marker for aneuploidies. The presence of a thickened NT, even if the karyotype is normal, can be associated with structural abnormalities. Having an abnormal screening of NT, parents and physicians could face dilemma over abortion particularly in a case of IVF/ICSI fetuses. Measurement of the NT thickness combined with biochemical markers has a false-positive rate of 5%. Hereby we present six cases of chromosomally normal fetuses with an increased NT thickness in the first trimester, a normal karyotype and normal follow-up scans, who had a good prognosis for a normal early childhood. This report may help increase the confidence of couples who are reluctant to terminate the pregnancy.
The presence of a thickened NT, even if the karyotype is normal, can be associated with structural abnormalities. Having an abnormal screening of NT, parents and physicians could face dilemma over abortion particularly in a case of IVF/ICSI fetuses. Measurement of the NT thickness combined with biochemical markers has a false-positive rate of 5%. Hereby we present six cases of chromosomally normal fetuses with an increased NT thickness in the first trimester, a normal karyotype and normal follow-up scans, who had a good prognosis for a normal early childhood. This report may help increase the confidence of couples who are reluctant to terminate the pregnancy.
Keywords: Congenital Abnormalities, Prenatal Diagnosis, Nuchal Translucency Measurement
Fetal nuchal translucency (NT) refers to the sonographic appearance of subcutaneous edema in the fetal neck measured according to the fetal medicine foundation (FMF) guidelines. NT is defined as the maximal thickness of the sonolucent zone (fluid accumulation) between the inner aspect of the fetal skin and the outer aspect of the soft tissue overlying the cervical spine or the occipital bone (). To avoid false negative or positive results, the fetus should be in a neutral position, with the head in line with the spine. During the scan, more than one measurement must be taken and the maximum one that meets the criteria should be considered.
To avoid false negative or positive results, the fetus should be in a neutral position, with the head in line with the spine. During the scan, more than one measurement must be taken and the maximum one that meets the criteria should be considered.
Open in a separate window
According to the FMF guidelines, NT is measured as the maximal thickness of the sonolucent zone (fluid accumulation) between the inner aspect of the fetal skin and the outer aspect of the soft tissue overlying the cervical spine or the occipital bone.
For this report, the outcome of 703 pregnancies presenting at Royan Institute after intra cytoplasmic sperm injection (ICSI) between the years 2008 and 2009 were reviewed. First trimester measurements of NT were performed during the routine first trimester screening for 856 fetuses. A total of 12 fetuses with an increased NT (NT ≥ 3) were considered for further investigation. In the follow-up ultrasounds, six out of 12 fetuses showed no anomalies and the result of amniocentesis (karyotype), fetal echocardiography and triple test or double test (the biochemical markers of pregnancy-associated plasma protein-A and free β-human chorionic gonadotropin) were also normal. Six healthy neonates were followed during their first and second year by routine pediatrician visits and the mental, physical or motor developmental delay was not observed in any of the cases and their functions were normal.
Six healthy neonates were followed during their first and second year by routine pediatrician visits and the mental, physical or motor developmental delay was not observed in any of the cases and their functions were normal.
All sonographic measurements were carried out by an expert radiologist with 10 years of experience and FMF certification in the measurement of NT. Images were saved and re-checked by another expert radiologist. Increased NT can be associated with a high incidence rate of chromosomal and non-chromosomal abnormalities. However, in nine studies that have addressed the issue of pediatric long-term follow-up of chromosomally and anatomically normal fetuses with increased NT, this measurement was suggested to be an indefinite indicator for the evaluation of fetal anomalies (1-9).
2.1. Case 1
A 28-year-old woman with a twin pregnancy, which was conceived by ICSI, was referred for routine screening test in the first trimester. The result of semen analysis showed a low motility (35%) with a high abnormal morphology (87%). In the routine first trimester screening at 12 weeks and 2 days of gestation, the NT measurements of the first fetus was 3.4 mm (normal range for this age is 1.2-3.1 mm). Although she refused to undergo the triple test and we had no result for amniocentesis (karyotype) and fetus echocardiography, follow-up ultrasounds revealed normal results. Two healthy babies (boy and girl) were born at 37 weeks of pregnancy. The weights of the newborns were 2400 grams and 3400 grams. Neonates were followed during the first 2 years of their life and none of them had developmental delay.
In the routine first trimester screening at 12 weeks and 2 days of gestation, the NT measurements of the first fetus was 3.4 mm (normal range for this age is 1.2-3.1 mm). Although she refused to undergo the triple test and we had no result for amniocentesis (karyotype) and fetus echocardiography, follow-up ultrasounds revealed normal results. Two healthy babies (boy and girl) were born at 37 weeks of pregnancy. The weights of the newborns were 2400 grams and 3400 grams. Neonates were followed during the first 2 years of their life and none of them had developmental delay.
2.2. Case2
A 35-year-old woman, who was conceived by ICSI, was referred for the routine screening test during her pregnancy. Her obstetric and medical history revealed primary infertility for a period of 7 years, mild endometriosis and polycystic ovaries. The result of semen analysis indicated low motility (35%) and high abnormal morphology (88%). During the routine first trimester screening at 13 weeks of gestation, NT was measured at 3 mm. The normal range of NT for this age is 1.6-2.4 mm. Nuchal skin fold (NF) measurements and prenatal follow-up ultrasound findings were normal. A Triple test was performed, and it showed a positive result and a high risk of trisomy 21. The patient was referred for amniocentesis or chorionic villus sampling. The amniocentesis findings were normal and a healthy baby girl (weight = 3600 grams) was born after a full-term pregnancy. She was followed during the first and second year of life and no developmental delay was detected.
The normal range of NT for this age is 1.6-2.4 mm. Nuchal skin fold (NF) measurements and prenatal follow-up ultrasound findings were normal. A Triple test was performed, and it showed a positive result and a high risk of trisomy 21. The patient was referred for amniocentesis or chorionic villus sampling. The amniocentesis findings were normal and a healthy baby girl (weight = 3600 grams) was born after a full-term pregnancy. She was followed during the first and second year of life and no developmental delay was detected.
2.3. Case 3
A 33-year-old pregnant woman conceived by ICSI was referred for a routine screening test. Her obstetric and medical histories were unremarkable. The result of semen analysis indicated low motility (30%) and high abnormal morphology (81%). The result of the routine first trimester screening at 11 weeks and 5 days gestation showed a significant increased NT (NT = 5). The normal range of NT for this age is 1-2.8 mm. Later examination revealed that collection of fluid was not confined to the neck but was enveloped throughout the fetus. The result of follow-up such as prenatal ultrasound findings, result of an amniocentesis (karyotype) and echocardiography were reported normal. She gave birth to a healthy baby boy (weight = 3500 grams) at 37 weeks of pregnancy by elective cesarean section at term. Follow-up after birth till 2 years has revealed no developmental delay.
The result of follow-up such as prenatal ultrasound findings, result of an amniocentesis (karyotype) and echocardiography were reported normal. She gave birth to a healthy baby boy (weight = 3500 grams) at 37 weeks of pregnancy by elective cesarean section at term. Follow-up after birth till 2 years has revealed no developmental delay.
2.4. Case 4
A 26-year-old woman who was conceived by ICSI was referred for a routine screening test during her pregnancy. Her obstetric and medical history showed 8 years of primary infertility and polycystic ovaries. The result of semen analysis showed a low sperm concentration with a low total sperm count, low motility (30%) and high abnormal morphology (86%). First trimester measurement of NT at 12 weeks of gestation was 3.2 mm during the routine first trimester screening. The normal range of NT for this age is 1.1-3 mm. Although she refused to undergo amniocentesis (karyotype) and fetal echocardiography, triple test and follow-up prenatal ultrasound findings were normal. She gave birth at term to a healthy baby boy at 38 weeks (weight = 3500 grams). The 2-year follow-up after birth revealed no developmental delay.
She gave birth at term to a healthy baby boy at 38 weeks (weight = 3500 grams). The 2-year follow-up after birth revealed no developmental delay.
2.5. Case 5
Following the routine screening test during pregnancy, a 31-year-old woman (conceived by ICSI) was referred to this institute. Her obstetric and medical history apart from 7 years primary infertility was unremarkable. The result of semen analysis revealed a low motility (35%) and a high abnormal morphology (92%). The result of routine first trimester screening at 12 weeks and 5 days of gestation showed an increased NT (3.3 mm) and generalized edema. The normal range of NT for this age is 1.5-3 mm. Although she refused to do the triple test and fetal echocardiography, follow-up prenatal ultrasound findings and amniocentesis (karyotype) were normal. She gave birth to a healthy term baby girl (weight = 3400 grams). Follow-up after birth revealed no developmental delay.
2.6. Case 6
A 30-year-old patient (conceived by ICSI) first presented to our institute at 12 weeks and 1 day of gestation and a twin pregnancy was detected. The second fetus was diagnosed with an increased NT (NT = 3.5 mm). The normal range of NT for this age is 1.2-3 mm. The couples’ history was significant for abnormal semen analysis. The result of semen analysis showed a sperm motility of 35% and an abnormal morphology of 80%. In this case, follow-up prenatal ultrasound findings and triple test were normal. Amniocentesis (karyotype) and echocardiography were cancelled because the patient refused to do so. Two healthy babies (boy and girl) were born at 37 weeks of pregnancy. The weights of the newborns were 2400 grams and 2900 grams. The neonates were followed for the first and second year of their life and none of them had developmental delay.
The second fetus was diagnosed with an increased NT (NT = 3.5 mm). The normal range of NT for this age is 1.2-3 mm. The couples’ history was significant for abnormal semen analysis. The result of semen analysis showed a sperm motility of 35% and an abnormal morphology of 80%. In this case, follow-up prenatal ultrasound findings and triple test were normal. Amniocentesis (karyotype) and echocardiography were cancelled because the patient refused to do so. Two healthy babies (boy and girl) were born at 37 weeks of pregnancy. The weights of the newborns were 2400 grams and 2900 grams. The neonates were followed for the first and second year of their life and none of them had developmental delay.
Although measurement of the NT thickness combined with biochemical markers has a false-positive rate of 5% (10), it is regarded as a basic screening test with high sensitivity for identifying fetuses at risk for aneuploidy (1, 11, 12). However, NT is increased in 4.4% of euploid fetuses who are at risk for fetal anomalies and an adverse pregnancy outcome (12).
For this report first trimester ultrasound screening was performed for 703 women with a total number of 856 fetuses who were conceived by ICSI. First trimester measurement of NT was performed for 856 fetuses and 12 out of 856 fetuses with increased NT (NT ≥ 3) were taken for further investigation. In this report, six out of 12 cases who were chromosomally and anatomically normal fetuses with increased first trimester NT were described in detail. All these six fetuses had favorable prognosis despite the increased NT. We had no chromosomal report of the remained six fetuses because of reduction due to multiple pregnancies (4/12) and intrauterine fetal death (IUFD 2/12).
The chance of delivering a healthy baby decreases with NT thickness from approximately 70% for an NT of 3.5-4.4 mm to about 15% for an NT of 6.5 mm or more (13). Based on previous studies, fetuses with increased NT (less than 4 mm), normal karyotype and normal findings in the 20-week scan, showed a markedly increased favorable outcome (14). After a normal detailed genetic sonography and fetal echocardiography, the incidence of adverse outcome and developmental delay were not significantly different from the normal population (9). According to studies performed by Souka et al. fetuses with increased NT thickness have a high risk of adverse or poor pregnancy outcome (1, 13). In this study, we only had one case of increased NT and intrauterine fetal death (IUFD) and one case of premature rupture of the membranes (PROM).
After a normal detailed genetic sonography and fetal echocardiography, the incidence of adverse outcome and developmental delay were not significantly different from the normal population (9). According to studies performed by Souka et al. fetuses with increased NT thickness have a high risk of adverse or poor pregnancy outcome (1, 13). In this study, we only had one case of increased NT and intrauterine fetal death (IUFD) and one case of premature rupture of the membranes (PROM).
This report is limited in number and should be further completed. In this series, semen analysis of all six cases were abnormal with a low motility of 30-35% and a high abnormal morphology of 80-92%. Although specific semen preparation technique in the case of impaired semen parameters in ART cycles is advisable, couples diagnosed with male-factor infertility should receive genetic counseling about the increased risk of congenital abnormalities before IVF-ICSI (15). This report provided six cases of increased NT with normal outcomes. It may help increase the confidence of couples who are reluctant to terminate the pregnancy. However, caution is necessary in cases of increased NT and parents should be offered a detailed fetal evaluation (genetic sonography) at the end of the first trimester and also at 18-22 weeks of gestation. Triple test, amniocentesis, fetal echocardiography and follow-up after birth are necessary.
It may help increase the confidence of couples who are reluctant to terminate the pregnancy. However, caution is necessary in cases of increased NT and parents should be offered a detailed fetal evaluation (genetic sonography) at the end of the first trimester and also at 18-22 weeks of gestation. Triple test, amniocentesis, fetal echocardiography and follow-up after birth are necessary.
1. Souka AP, Krampl E, Bakalis S, Heath V, Nicolaides KH. Outcome of pregnancy in chromosomally normal fetuses with increased nuchal translucency in the first trimester. Ultrasound Obstet Gynecol. 2001;18(1):9–17. doi: 10.1046/j.1469-0705.2001.00454.x. [PubMed] [CrossRef] [Google Scholar]
2. Van Vugt JM, Tinnemans BW, Van Zalen-Sprock RM. Outcome and early childhood follow-up of chromosomally normal fetuses with increased nuchal translucency at 10-14 weeks' gestation. Ultrasound Obstet Gynecol. 1998;11(6):407–9. doi: 10.1046/j.1469-0705.1998.11060407.x. [PubMed] [CrossRef] [Google Scholar]
3. Brady AF, Pandya PP, Yuksel B, Greenough A, Patton MA, Nicolaides KH. Outcome of chromosomally normal livebirths with increased fetal nuchal translucency at 10-14 weeks' gestation. J Med Genet. 1998;35(3):222–4. [PMC free article] [PubMed] [Google Scholar]
Brady AF, Pandya PP, Yuksel B, Greenough A, Patton MA, Nicolaides KH. Outcome of chromosomally normal livebirths with increased fetal nuchal translucency at 10-14 weeks' gestation. J Med Genet. 1998;35(3):222–4. [PMC free article] [PubMed] [Google Scholar]
4. Adekunle O, Gopee A, el-Sayed M, Thilaganathan B. Increased first trimester nuchal translucency: pregnancy and infant outcomes after routine screening for Down's syndrome in an unselected antenatal population. Br J Radiol. 1999;72(857):457–60. doi: 10.1259/bjr.72.857.10505009. [PubMed] [CrossRef] [Google Scholar]
5. Maymon R, Jauniaux E, Cohen O, Dreazen E, Weinraub Z, Herman A. Pregnancy outcome and infant follow-up of fetuses with abnormally increased first trimester nuchal translucency. Hum Reprod. 2000;15(9):2023–7. [PubMed] [Google Scholar]
6. Hiippala A, Eronen M, Taipale P, Salonen R, Hiilesmaa V. Fetal nuchal translucency and normal chromosomes: a long-term follow-up study. Ultrasound Obstet Gynecol. 2001;18(1):18–22. doi: 10.1046/j.1469-0705.2001.00481.x. [PubMed] [CrossRef] [Google Scholar]
doi: 10.1046/j.1469-0705.2001.00481.x. [PubMed] [CrossRef] [Google Scholar]
7. Senat MV, De Keersmaecker B, Audibert F, Montcharmont G, Frydman R, Ville Y. Pregnancy outcome in fetuses with increased nuchal translucency and normal karyotype. Prenat Diagn. 2002;22(5):345–9. doi: 10.1002/pd.321. [PubMed] [CrossRef] [Google Scholar]
8. Cheng CC, Bahado-Singh RO, Chen SC, Tsai MS. Pregnancy outcomes with increased nuchal translucency after routine Down syndrome screening. Int J Gynaecol Obstet. 2004;84(1):5–9. [PubMed] [Google Scholar]
9. Senat MV, Bussieres L, Couderc S, Roume J, Rozenberg P, Bouyer J, et al. Long-term outcome of children born after a first-trimester measurement of nuchal translucency at the 99th percentile or greater with normal karyotype: a prospective study. Am J Obstet Gynecol. 2007;196(1):53 e1–6. doi: 10.1016/j.ajog.2006.08.026. [PMC free article] [PubMed] [CrossRef] [Google Scholar]
10. Nicolaides KH, Spencer K, Avgidou K, Faiola S, Falcon O.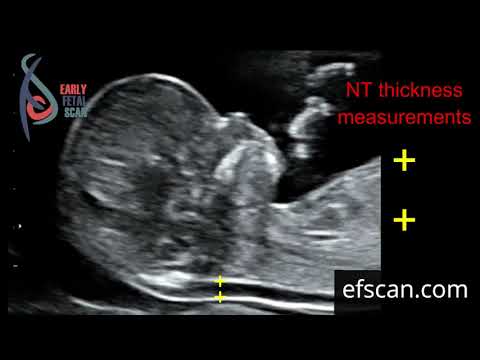 Multicenter study of first-trimester screening for trisomy 21 in 75 821 pregnancies: results and estimation of the potential impact of individual risk-orientated two-stage first-trimester screening. Ultrasound Obstet Gynecol. 2005;25(3):221–6. doi: 10.1002/uog.1860. [PubMed] [CrossRef] [Google Scholar]
Multicenter study of first-trimester screening for trisomy 21 in 75 821 pregnancies: results and estimation of the potential impact of individual risk-orientated two-stage first-trimester screening. Ultrasound Obstet Gynecol. 2005;25(3):221–6. doi: 10.1002/uog.1860. [PubMed] [CrossRef] [Google Scholar]
11. Pandya PP, Kondylios A, Hilbert L, Snijders RJ, Nicolaides KH. Chromosomal defects and outcome in 1015 fetuses with increased nuchal translucency. Ultrasound Obstet Gynecol. 1995;5(1):15–9. doi: 10.1046/j.1469-0705.1995.05010015.x. [PubMed] [CrossRef] [Google Scholar]
12. Snijders RJ, Noble P, Sebire N, Souka A, Nicolaides KH. UK multicentre project on assessment of risk of trisomy 21 by maternal age and fetal nuchal-translucency thickness at 10-14 weeks of gestation. Fetal Medicine Foundation First Trimester Screening Group. Lancet. 1998;352(9125):343–6. [PubMed] [Google Scholar]
13. Souka AP, Von Kaisenberg CS, Hyett JA, Sonek JD, Nicolaides KH. Increased nuchal translucency with normal karyotype. Am J Obstet Gynecol. 2005;192(4):1005–21. doi: 10.1016/j.ajog.2004.12.093. [PubMed] [CrossRef] [Google Scholar]
Am J Obstet Gynecol. 2005;192(4):1005–21. doi: 10.1016/j.ajog.2004.12.093. [PubMed] [CrossRef] [Google Scholar]
14. Bilardo CM, Muller MA, Pajkrt E, Clur SA, van Zalen MM, Bijlsma EK. Increased nuchal translucency thickness and normal karyotype: time for parental reassurance. Ultrasound Obstet Gynecol. 2007;30(1):11–8. doi: 10.1002/uog.4044. [PubMed] [CrossRef] [Google Scholar]
15. Allen VM, Wilson RD, Cheung A, Genetics Committee of the Society of O, Gynaecologists of C, Reproductive Endocrinology Infertility Committee of the Society of O, et al. Pregnancy outcomes after assisted reproductive technology. J Obstet Gynaecol Can. 2006;28(3):220–50. [PubMed] [Google Scholar]
How to choose a scanner
An efficient office today is unimaginable without an electronic document management system - whether it's an industrial-scale product or storing important documents in Excel. Thus, many documents - be it contracts, primary accounting documentation, orders, important letters - in a word, all important documents - we have long been accustomed to storing in scanned form.
What is a scanner and what criteria should be followed when choosing this machine?
Scanner - a device designed to convert analog information into digital form.
There are several types of scanners:
Handheld scanners - devices process document strips no more than 12 cm wide and are used more often by mobile PC owners. They are slow, have low optical resolution (no more than 100 dpi), and often scan images skewed. Gradually, these models disappear from the market due to the inconvenience of use and lack of competitiveness in cost with other types of scanners.
these devices are easy to use and quite versatile in terms of scope. The design of such scanners allows you to scan any original - be it a single page with the necessary object, an unfolded book, or even the front side of a box. The main part of such scanners is the reading head moving along the object with the image located on the glass surface. In some models, the head is stationary, and the document, along with the glass, moves relative to it. The price range for such scanners is very wide. The only drawback of this type of devices can be considered the size of the scanned image - it does not exceed the size of the A2 format, and devices with A4 or A3 formats are considered standard models.
The price range for such scanners is very wide. The only drawback of this type of devices can be considered the size of the scanned image - it does not exceed the size of the A2 format, and devices with A4 or A3 formats are considered standard models.
document scanners (also known as sheet feed or automatic) are devices that feed document pages between guide rollers. Such scanners are very convenient for scanning documents consisting of a large number of pages (contracts, for example). The scanning process is fast and convenient - you do not need to feed each individual sheet, just load them in a certain order into a special container.
Slide Scanners - Scanners designed to scan film negatives. The principle of operation of a slide scanner is almost the same as a flatbed scanner, except that the original is between the light source and the reading head. Such scanners, as a rule, are used narrowly professionally. The main advantage of this type of scanner is that at a much lower price they allow you to get the same quality as on the most professional and expensive drum scanners.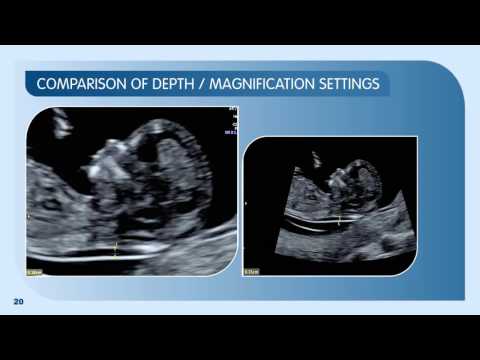
drum scanners can be called professional, they are used mainly in the printing industry. In terms of light sensitivity, such a device is seriously superior to standard tablet devices. The resolution of such scanners is usually between 8000 and 24000 dpi. In scanners of this type, the original is fixed with a special tape or oil on the surface of a transparent cylinder (drum) rotating at high speed (from 300 to 1350 rpm), and the scanning receiver reads the image pixel by pixel with high accuracy. A beam of light passing through a slide (or reflected from an opaque original), which is created using a laser, through a system of mirrors, enters the PMT (photomultiplier tube), where it is digitized. When scanning transparent originals, an internal light source is used, which is located inside the drum, and when scanning reflective (opaque) originals, an external light source is used.
Main characteristics of scanners:
Resolution
There are two types of scanner resolution: optical and interpolation. Optical resolution is responsible for the quality of the image on the scanned document, the higher this type of resolution, the better, of course.
Optical resolution is responsible for the quality of the image on the scanned document, the higher this type of resolution, the better, of course.
Interpolation (sometimes called mechanical) resolution is a software resolution, it is obtained by processing the image received from the scanner using the driver.
Color rendering
The determining criterion for this characteristic is the color depth. The color rendering level should be high, especially if the scanner is going to be used to scan color images. The greater the color depth, the more accurate the color reproduction will be.
Density range (dynamic range)
This factor characterizes what range of optical densities of the document the scanner can "read" without losing shades in the highlights and shadows of the original. The maximum optical density of the scanner is the optical density of the original, which the scanner still distinguishes from complete darkness. All shades of the original darker than this border the scanner will not be able to distinguish. This value very well separates simple office scanners from more professional models. As a rule, for most flatbed scanners, this value ranges from 1.7D (standard office models) to 3.4D (semi-professional models). Most paper originals have an optical density of no more than 2.5D. Slides require a dynamic range of more than 2.7 D. And only negatives and X-rays have higher densities (3.3D - 4.0D), and it is advisable to buy a scanner with a higher dynamic range if you plan to work mainly with them.
This value very well separates simple office scanners from more professional models. As a rule, for most flatbed scanners, this value ranges from 1.7D (standard office models) to 3.4D (semi-professional models). Most paper originals have an optical density of no more than 2.5D. Slides require a dynamic range of more than 2.7 D. And only negatives and X-rays have higher densities (3.3D - 4.0D), and it is advisable to buy a scanner with a higher dynamic range if you plan to work mainly with them.
Computer interface
Parallel or serial interface with connection to LPT or COM port. These interfaces are characterized by particularly slow connection, such models are increasingly losing their popularity. USB interface. Devices with this connection version are somewhat more expensive than the previous ones, but the connection speed is higher. The scanning speed of USB 1.1 is slower, USB 2.0 is faster.
FireWire interface (IEEE 1394) - version specially designed for graphics and video. Such models are presented on the market relatively recently. Recently, scanners with two interfaces (for example, LPT and USB) have also been produced. It's pretty convenient. You can connect the scanner to an old PC (without USB) via a parallel interface, or via USB when using modern computers.
Such models are presented on the market relatively recently. Recently, scanners with two interfaces (for example, LPT and USB) have also been produced. It's pretty convenient. You can connect the scanner to an old PC (without USB) via a parallel interface, or via USB when using modern computers.
What documents are you planning to scan?
If you'll be scanning mostly text documents in black and white, you'll be fine with just about any flatbed machine that isn't the most expensive or high-end one.
If you plan to scan color images, whether they are photographs, various brochures or marketing flyers, you should pay more attention to the choice of scanner characteristics, such as color reproduction and high resolution.
Software
A Twain driver must be supplied with the scanner. With it, you can set the required scanning area, select the parameters of the scanning process. The convenience of the interface of this program is important - the availability and the ability to save the necessary settings to obtain an image of maximum quality - color correction, brightness settings, scanning contrast, etc.
|
::: Contacts »
load in ENGLISH «
|
::: ACCESSORIES To NT-206 ::: Additional accessories to expand and complementary basic functions ACM NT-206
|
 ..
.. 
 , 24x42 mm dia. (without connecting cable), weight <70 g
, 24x42 mm dia. (without connecting cable), weight <70 g  ..
..  ..
.. 
 ..
..  ..
.. 
 Provides electrical isolation to the probe from the body of the device. Additionally contains a circuit for applying electrical potential to the probe.
Provides electrical isolation to the probe from the body of the device. Additionally contains a circuit for applying electrical potential to the probe.  ..
.. 
 ..
..  ..
..