Missed miscarriage blood clots
Treating miscarriage | The Royal Women's Hospital
If a miscarriage has begun, there is nothing that can be done to stop it. Any treatment you have will be aimed at avoiding heavy bleeding and infection.
A discussion with the doctor or nurse will help you to work out which treatment options are best and safest for you.
On this page:
- No treatment (expectant management)
- Treatment with medicine
- Surgical treatment (curette)
- Waiting for treatment
- After a miscarriage
No treatment (expectant management)
You can choose to wait and see what will happen. This is called 'expectant management'. If nothing is done, sooner or later the pregnancy tissue will pass naturally. If it is an incomplete miscarriage (where some but not all pregnancy tissue has passed) it will often happen within days, but for a missed miscarriage (where the fetus or embryo has stopped growing but no tissue has passed) it might take as long as three to four weeks.
While you are waiting you may have some spotting or bleeding, much like a period. When the pregnancy tissue passes, you are likely to have heavier bleeding with crampy, period-like pains. You can use sanitary pads and take pain relieving tablets, such as paracetamol.
If your miscarriage is incomplete, with just a small amount of pregnancy tissue remaining, it’s probably best to take a wait and see approach. But if there is heavy bleeding or signs of infection you will need treatment.
If the tissue does not pass naturally or you have signs of infection, the doctor will recommend a dilatation and curettage (D&C). You and the doctor can discuss and decide the preferred option for you.
Things to know
- There are many reasons why some women prefer to wait and see. It may feel more natural, it may help with the grieving process or it may give you more of a sense of control.
- Some women become worried or frightened when the bleeding gets heavier, especially if blood clots, tissue or even a recognisable embryo is passed.
- Usually, the wait and see approach takes longer than any other approaches such as surgery or medication. Sometimes bleeding can last for up to four weeks.
- Although excessive bleeding and blood transfusion are very rare, they are slightly more common with expectant management than with surgery.
- A few women still need to have surgery – sometimes urgently – if they develop infection, bleed heavily or if the tissue does not pass naturally.
- The waiting time can be emotionally draining for some women.
Treatment with medicine
Medicine is available that can speed up the process of passing the pregnancy tissue. For an incomplete miscarriage, the medicine will usually encourage the pregnancy tissue to pass within a few hours. At most it will happen within a day or two. For a missed miscarriage, it may happen quickly, but it can take up to two weeks and, occasionally, longer.
- Medication is not suitable if there is very heavy bleeding or signs of infection.
 It is usually not recommended for pregnancies that are older than about nine weeks.
It is usually not recommended for pregnancies that are older than about nine weeks. - If the tissue does not pass naturally, eventually your doctor will recommend a dilatation and curettage (D&C).
Things to know
- The pregnancy tissue will pass between four to six hours after taking the medicine, during which time you may be in hospital. After a few hours, if the pregnancy hasn’t passed, you may be sent home to wait. This will depend on where you are and which hospital you are in.
- The medicine has side effects which usually pass in a few hours but can be unpleasant, such as nausea, vomiting, diarrhoea, fever and chills. The tablets can be swallowed or dissolved under the tongue, or inserted in the vagina.
- After receiving the medication there may be some spotting or bleeding like a period. When the pregnancy tissue passes, you are likely to notice heavier bleeding and clots with strong cramping, period-like pains. You can use sanitary pads and take pain relieving tablets such as paracetamol.
- Some women may need stronger pain killers or a pain relieving injection.
- A few women still need to have surgery, sometimes urgently, if they develop infection, bleed heavily or if the tissue does not pass.
Surgical treatment (curette)
A D&C (or ‘curette’) is a minor operation. The full name is dilatation and curettage. It is done in an operating theatre, usually under general anaesthetic. There is no cutting involved because the surgery happens through the vagina. The cervix (neck of the uterus) is gently opened and the remaining pregnancy tissue is removed so that the uterus is empty. Usually the doctor is not able to see a recognisable embryo.
The actual procedure usually only takes five to ten minutes, but you will usually need to be in the hospital for around four to five hours. Most of this time will be spent waiting and recovering.
You may have to wait a day or two to have a curette and sometimes, while you are waiting, the pregnancy tissue will pass on its own. If this happens and all of the tissue is passed you may not need to have a curette.
If this happens and all of the tissue is passed you may not need to have a curette.
A curette is done in the following circumstances:
- You have heavy or persistent bleeding and/or pain.
- The medical staff advise that this is a better option for you; this may be because of the amount of tissue present, especially with a missed miscarriage.
- This is an option you prefer.
Things to know
The risks of a D&C are very low, but include:
- some pregnancy tissue remains in uterus. This can cause prolonged or heavy bleeding and the operation may need to be repeated
- infection needing antibiotics
- damage to the cervix or uterus. This is very rare (around 1 in 1000) and, when it does happen, it is usually a small hole or tear which will heal itself
- excessive bleeding (very rare)
- anaesthetic risks. These are very low for healthy women, but no anaesthetic or operation is without risk.
Waiting for treatment
If you have heavy bleeding with clots and crampy pain, it is likely that you are passing the pregnancy tissue. The bleeding, clots and pain will usually settle when most of the pregnancy tissue has been passed. Sometimes the bleeding will continue to be heavy and you may need further treatment.
The bleeding, clots and pain will usually settle when most of the pregnancy tissue has been passed. Sometimes the bleeding will continue to be heavy and you may need further treatment.
You should go to your nearest emergency department if you have:
- increased bleeding, for instance soaking two pads per hour and/or passing golf ball sized clots
- severe abdominal pain or shoulder pain
- fever or chills
- dizziness or fainting
- vaginal discharge that smells unpleasant
- diarrhoea or pain when you open your bowels.
What to do while you are waiting
- You can try to rest and relax at home.
- Usual activity that is not too strenuous will not be harmful. You can go to work if you feel up to it.
- If you have pain you can take paracetamol.
- If there is bleeding, use sanitary pads rather than tampons.
After a miscarriage
- It is usual to have pain and bleeding after a miscarriage.
 It will feel similar to a period and will usually stop within two weeks. You can take ordinary painkillers for the pain. Your next period will usually come in four to six weeks after a miscarriage.
It will feel similar to a period and will usually stop within two weeks. You can take ordinary painkillers for the pain. Your next period will usually come in four to six weeks after a miscarriage. - See a doctor or attend a hospital emergency department if you have strong pain and bleeding (stronger than period pain), abnormal discharge, (especially if it is smelly), or fever. These symptoms may mean that you have an infection or that tissue has been left behind.
- Try and avoid vaginal sex until the bleeding stops and you feel comfortable.
- Use sanitary pads until the bleeding stops (do not use tampons).
- All contraceptive methods are safe after a miscarriage
- See a GP (local doctor) in four to six weeks for a check-up.
Anti-D injection after a miscarriage
It is important to have your blood group checked. If you’re RhD negative and the fetus is RhD positive this can cause problems for future pregnancies. This is because the fetus’s blood cells have RhD antigen attached to them, whereas yours do not. If small amounts of the fetus’s blood mixes with your blood, your immune system may perceive this difference in blood cells as a threat and produce antibodies to fight against the fetus’s blood. Once your body has made these antibodies they can’t be removed. This is unlikely to have caused your miscarriage and is more likely to affect future pregnancies. Women with a negative blood type usually need an Anti-D injection, which will stop the antibodies forming.
If small amounts of the fetus’s blood mixes with your blood, your immune system may perceive this difference in blood cells as a threat and produce antibodies to fight against the fetus’s blood. Once your body has made these antibodies they can’t be removed. This is unlikely to have caused your miscarriage and is more likely to affect future pregnancies. Women with a negative blood type usually need an Anti-D injection, which will stop the antibodies forming.
Future pregnancies after a miscarriage
One of the most common concerns following a miscarriage is that it might happen again. However, if you have had one miscarriage the next pregnancy will usually be normal.
If you do try for another pregnancy, try and avoid smoking, alcohol and excess caffeine as they increase the risk of miscarriage. It is recommended that all women take folic acid while trying to conceive, and continue until three months of pregnancy. In your next pregnancy you are encouraged to see your GP and have an ultrasound at about seven weeks. If ultrasound is done too early in pregnancy the findings are often uncertain and cause unnecessary worry.
If ultrasound is done too early in pregnancy the findings are often uncertain and cause unnecessary worry.
Feelings and reactions
There is no ‘right’ way to feel following a miscarriage. Some degree of grief is very common, even if the pregnancy wasn’t planned. Partners may react quite differently, just as people can respond differently to a continuing pregnancy. Feelings of loss may persist for some time and you may have mixed feelings about becoming pregnant again. Some friends and family may not understand the depth of emotion that can be attached to a pregnancy and may unreasonably expect for you to move on before you are ready.
Some couples decide that they want to try for a pregnancy straight away, while others need time to adjust to their loss. If you feel anxious about a possible loss in future pregnancies, you may find it helpful to talk to someone about this. If it’s difficult to speak with your friends and family about these issues, your doctor, community support group and counsellors can provide information and assistance.
Related Health Topics
-
- Treatment for miscarriage
Treatment for miscarriage is aimed at avoiding heavy bleeding and infection. It is also aimed at looking after you, physically and emotionally.
-
- (English) PDF (302 KB)
- Treatment for miscarriage
The Women’s does not accept any liability to any person for the information or advice (or use of such information or advice) which is provided on the Website or incorporated into it by reference. The Women’s provide this information on the understanding that all persons accessing it take responsibility for assessing its relevance and accuracy. Women are encouraged to discuss their health needs with a health practitioner. If you have concerns about your health, you should seek advice from your health care provider or if you require urgent care you should go to the nearest Emergency Dept.
If you have concerns about your health, you should seek advice from your health care provider or if you require urgent care you should go to the nearest Emergency Dept.
Bleeding, Clots, Timing, and Other Signs
Miscarriage is fairly common in the first trimester. It happens in about 10 percent of known pregnancies.
In some cases, miscarriage can occur before you know you’re pregnant. If this happens, you might not notice anything different from your usual period.
The further along you are in a pregnancy, the less likely it is that a miscarriage will feel like a period.
Continue reading to learn more about early miscarriage, including specific symptoms to watch for, when you should see a doctor, and more.
The most common symptoms of early miscarriage are cramping and bleeding.
However, spotting or light bleeding during early pregnancy aren’t always a sign of miscarriage. If this happens, watch for any other unusual symptoms.
Other symptoms of miscarriage
- cramping in your abdomen or lower back (This could start out like period cramps, but the pain typically worsens over time.
 )
) - nausea
- diarrhea
- passing fluids, larger-than-normal blood clots, or tissue from your vagina
Timing
A miscarriage can happen any time after fertilization. If you didn’t know you were pregnant, it would be easy to mistake it for a period.
Both a period and a miscarriage can cause spotting to heavy bleeding.
After the first eight weeks or so, it’s less likely that you’ll mistake a miscarriage for a period.
Duration
You know how long and heavy your typical period is.
During a miscarriage, bleeding gets heavier and lasts longer than a period.
As your cervix starts to dilate, cramping may become more painful than typical period cramping.
Characteristics
Bleeding during miscarriage can appear brown and resemble coffee grounds. Or it can be pink to bright red.
It can alternate between light and heavy or even stop temporarily before starting up again.
If you miscarry before you’re eight weeks pregnant, it might look the same as a heavy period. Later, you’re more likely to notice fetal or placental tissue.
Later, you’re more likely to notice fetal or placental tissue.
Menstruation products
Heavy bleeding, pieces of tissue, or large blood clots on your menstruation products could mean that you’re having more than a heavy period.
See a doctor if you’re soaking through a tampon or pad every hour for more than two consecutive hours.
You should call a doctor or other healthcare provider any time you experience unexpected pain or excessive bleeding.
These symptoms can result from an ectopic pregnancy. This occurs when a fertilized egg has implanted outside the uterus, possibly inside a fallopian tube. It’s a medical emergency.
You should also call a doctor if you experience bleeding alongside:
- mucus
- tissue
- blood clots
- what feels like uterine contractions
If you believe you’re having a miscarriage, ask your doctor the following:
- Should I collect a sample of blood or tissue? (This isn’t always necessary.
 )
) - Should I go to an emergency room or make an office appointment?
- Is it fine to drive myself, or do you recommend against it?
If it appears that you’ve had a miscarriage, your doctor will want to perform a physical exam.
Be sure to discuss all your symptoms, including the amount of:
- bleeding
- clotting
- pain
- any tissue that may have been expelled
Testing may include:
- an ultrasound to check the uterus for signs of an embryo or a heartbeat
- a blood test to check for human chorionic gonadotropin (hCG), a substance that indicates pregnancy
There’s no way to stop a miscarriage in progress. If your doctor determines that you’ve experienced a miscarriage, they’ll want to check for:
- signs of infection
- uncontrollable bleeding
- tissue that may be left in your uterus
It can take two weeks or more to completely expel the tissue naturally. Your doctor will review with you typical bleeding patterns to expect. If you have heavy bleeding lasting several days or any signs of infection, you may need medical treatment.
If you have heavy bleeding lasting several days or any signs of infection, you may need medical treatment.
If your doctor isn’t sure that all of the pregnancy tissue has been cleared from your uterus, they may order an ultrasound to confirm.
Your doctor can prescribe medication, such as misoprostol (Cytotec), to increase uterine contractions to help you expel the tissue.
You’ll experience cramping and bleeding as you pass tissue and blood.
Most people pass the tissue within 24 hours after taking the drug. For others, it can take a few days to complete. Either way, it doesn’t require a hospital stay.
Your doctor may be able to prescribe pain medication to help ease your symptoms.
If your blood type is Rh negative, you’ll need an injection of Rh immunoglobulin. This may help prevent complications in a future pregnancy.
There are also a few surgical options to remove tissue from the uterus. This includes:
- Vacuum aspiration.
 Your doctor inserts a thin tube that contains a suction device into your uterus. This can be done with local anesthesia in your doctor’s office.
Your doctor inserts a thin tube that contains a suction device into your uterus. This can be done with local anesthesia in your doctor’s office.
- Dilation and curettage (D&C). Your doctor dilates your cervix, and then uses an instrument called a curette to scrape your uterine lining. This can be done at a surgical center or operating room on an outpatient basis. Regional or general anesthesia can be used.
Both of these treatments have been well-studied and are considered safe. They each carry a very small risk of serious complications.
If you’ve experienced a miscarriage, it’s important to understand that it isn’t your fault.
In many cases, doctors are unable determine the cause. Here are some things that can contribute to miscarriage:
During the first trimester
As many as 80 percent of miscarriages occur in the first trimester.
When a miscarriage occurs in the first five weeks after fertilization, it’s called a “chemical pregnancy. ” It’s so early that you might not have known you were pregnant.
” It’s so early that you might not have known you were pregnant.
Although your period may seem heavier than usual, there might not be any other noticeable sign of miscarriage.
Miscarriages in the first trimester often have to do with chromosome abnormalities that interfere with normal development. Missing or extra chromosomes are linked to 50 percent of all miscarriages.
Sometimes, a fertilized egg simply doesn’t develop into an embryo (blighted ovum).
It may help to know that having sex, exercising, morning sickness, and previous use of oral contraceptives don’t cause miscarriage. Even an accidental fall doesn’t necessarily cause it.
According to the American College of Obstetricians and Gynecologists (ACOG), smoking and alcohol consumption in the first trimester may result in a slightly higher risk of miscarriage. But the research on this is mixed.
It’s also worth noting that drinking less than 200 milligrams of caffeine per day doesn’t appear to increase the risk of miscarriage.
Some things that may increase the risk of early miscarriage are:
- fibroids or other abnormalities of the uterus
- hyperthyroidism or hypothyroidism
- uncontrolled diabetes
- use of cocaine or similar drugs
During the second trimester
About 2 to 3 percent of miscarriages occur during the second trimester.
Some things that may increase the risk are:
- conditions that can cause blood clots
- early preeclampsia or eclampsia
- fetal abnormalities
- fibroids or other abnormalities of the uterus
- infection of the uterus
- lupus
- prior surgery of the cervix
- trauma
- uncontrolled diabetes
- hyperthyroidism or hypothyroidism
- high blood pressure
- use of cocaine or similar drugs
During the third trimester
Losing a pregnancy starting from the 20th week of pregnancy and into the third trimester is considered stillbirth, not miscarriage.
In general, the risk of stillbirth increases with maternal age.
If you’ve experienced a miscarriage, it doesn’t mean you’ll have another, and it doesn’t mean you can’t have children.
Most people who experience a miscarriage can go on to have a successful pregnancy.
Miscarriage shouldn’t affect your ability to get pregnant. You can ovulate and become pregnant within two weeks of an early miscarriage.
If you don’t want to become pregnant again, you should use birth control right away.
About 1 percent of people have multiple miscarriages. If you’ve experienced several miscarriages, your doctor might recommend special testing.
Even if you’ve had three miscarriages in a row, there’s a 70 percent chance your next pregnancy will be successful.
Your doctor will probably advise you to avoid sex, tampons, and douches for two weeks. This will help prevent infection.
They may also want you to take a pregnancy test after about two weeks. This can help them determine whether your hormone levels are back to normal.
In the meantime, call your doctor if you:
- are bleeding heavier than expected or notice that the blood stays bright red
- are soaking through more than two maxi pads an hour for more than two hours
- notice a foul-smelling discharge
- experience abdominal tenderness or severe pain
- have persistent cramping
- develop a fever or chills
For the first few days, you may notice blood clots and tissue passing, but this should taper off after about a week. It will take about four to eight weeks for your regular period to return.
Mild exercise following an early miscarriage is usually fine, but check with your doctor. It may depend on how far along you were, as well as your overall health.
There are many emotions a person might have following a miscarriage. Some feel anger, sadness, or profound loss. Others might feel relieved.
These feelings may have to do with whether you knew you were pregnant or if you were trying to have a baby.
Pregnancy and miscarriage also cause hormone fluctuations, which can affect your emotions.
Everyone is different, so there’s no correct way to feel about experiencing a miscarriage. It may take some time for you to process everything.
You may find it helpful to talk to your partner, family, or friends about what you’re going through.
You may also consider looking into support groups for people who have experienced miscarriage. Sometimes it helps to talk to others who have been through the same thing.
Here are a few places to seek support:
- your doctor’s office or local hospital for referrals to support services
- clergy
- Compassionate Friends, which has a searchable database of local chapters
- March of Dimes Loss and Grief Forum
- Share Pregnancy & Infant Loss Support which offers online support and information on how to find local groups
If grief continues to worsen after a few weeks, talk to a doctor about your options for treatment. You may benefit from grief counseling or treatment for depression.
You may benefit from grief counseling or treatment for depression.
Miscarriage isn’t your fault.
Physical recovery generally takes a few weeks. Everyone has their own timetable for emotional recovery.
There’s no need to rush yourself or to pretend to “get over it” for anyone else’s sake.
And if you need it, reaching out for support is a reasonable thing to do. You aren’t alone in this.
Miscarriage due to missed pregnancy | Articles by EMC doctors about diseases, diagnosis and treatment
What is a miscarriage?
According to medical statistics, miscarriage is the most common complication during pregnancy. About 10-20% of all recorded pregnancies end in miscarriage. Miscarriage is a sporadic, sudden, termination of pregnancy, which is accompanied by complete or partial emptying of the uterus.
Missed pregnancy loss (MP) can be seen on ultrasound. It consists in confirming the non-viability of the fetus without bleeding. The ST can end in a miscarriage, when the body gets rid of the dead fetus on its own, or in a medical abortion, when medical or surgical manipulations are used to clean the uterine cavity.
Causes of miscarriage and miscarriage
80% of miscarriages occur in the first trimester before 12 weeks. In 50% of cases, this occurs due to genetic defects in the fetus. The threat of miscarriage due to chromosomal abnormalities decreases with the course of pregnancy: by 20 weeks it is 10-20% versus 41-50% in the first trimester. The main cause of genetically determined early miscarriages are autonomous trisomies - when three homologous chromosomes are present in the cells instead of two. Such defects occur at the time of conception and are not subject to correction. They lead to miscarriage or to the development of severe genetic diseases. In addition to genetics, immunological, endocrine and infectious causes are distinguished.
In the second trimester, various diseases and disorders in the mother's body become the main cause of miscarriage.
There is a list of factors that can trigger early pregnancy loss:
-
woman's age. At the age of 20-30 years, the risk of spontaneous miscarriage is 9-17%, at 35-40 years old - 20%, at 40-45 - 40%;
-
alcohol abuse;
-
abuse of caffeine;
-
smoking;
-
drug use;
-
chronic diseases of the mother;
-
maternal infections;
-
use of medications incompatible with pregnancy;
-
history of spontaneous abortion. The risk of subsequent pregnancy loss in women with one miscarriage in history is 18-20%, with two - 30%, with three - 43%.
Symptoms and signs of miscarriage
You can suspect a miscarriage by sudden spotting and sharp pain in the lower abdomen. If these symptoms appear, seek immediate medical attention. The doctor must conduct an ultrasound diagnosis. Transvaginal scanning (TVS) is considered the gold standard for diagnostics - when the sensor is inserted into the uterus through the vagina. If TVS is not available, a transabdominal scan can be applied - through the anterior abdominal wall.
If TVS is not available, a transabdominal scan can be applied - through the anterior abdominal wall.
Missed pregnancy may be asymptomatic and not manifest until the next scheduled ultrasound.
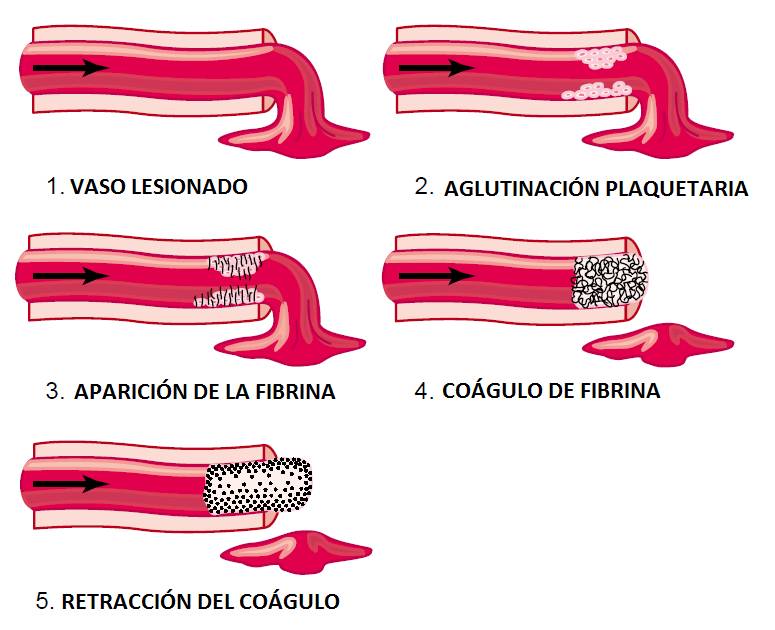
How does a miscarriage happen?
The miscarriage process has four stages. This does not happen overnight and lasts from several hours to several days.
The first stage - the threat of miscarriage. Among the symptoms: pulling pains in the lower abdomen, scanty blood discharge, increased uterine tone. The process of detachment of the placenta from the place of attachment in the uterus begins. The internal os is closed. The main thing is to seek help in time, then with proper therapy if there is a chance to stop the miscarriage and save the pregnancy.
The second stage - the beginning of a miscarriage. Strong discharge, the cervical canal is ajar, the doctor diagnoses the final detachment of the placenta.
The third stage is a miscarriage in progress. You can feel the regular contractions of the uterus, the outcome of the fetus, placenta and uterine contents, profuse blood discharge has begun.
You can feel the regular contractions of the uterus, the outcome of the fetus, placenta and uterine contents, profuse blood discharge has begun.
The last fourth stage is a complete miscarriage. The pregnancy is interrupted, the uterine cavity does not contain the fetus and products of conception.
How to determine the ST?
It should be remembered that a miscarriage can be diagnosed only during an ultrasound examination. Home tests will not give reliable results. Ultrasound will show the presence or absence of a heartbeat in the fetus.
Treatment of miscarriage and miscarriage
Due to the fact that the vast majority of spontaneously terminated pregnancies are due to genetic abnormalities (non-viability) of the fetus, then, speaking about the treatment of miscarriage, it is worth talking about ensuring complete and safe cleansing of the uterus, preventing infection and preventing bruising. With the help of an ultrasound examination, the doctor will check whether the uterus has completely cleared. If yes, then no additional treatment is required. In the event of an incomplete miscarriage or STD, the patient will be indicated for surgical or medical cleaning. If the miscarriage is only in a state of threat, the treatment tactics will be aimed at blocking uterine contractions and stopping the development of a miscarriage. If you need treatment for a missed pregnancy in Moscow, contact our specialists.
If yes, then no additional treatment is required. In the event of an incomplete miscarriage or STD, the patient will be indicated for surgical or medical cleaning. If the miscarriage is only in a state of threat, the treatment tactics will be aimed at blocking uterine contractions and stopping the development of a miscarriage. If you need treatment for a missed pregnancy in Moscow, contact our specialists.
signs, symptoms and causes. How to determine a frozen pregnancy. Clinic Ak. Grishchenko
03/15/2021
Not always long-awaited and such a desired pregnancy ends with the birth of a baby. Sometimes women find out that the pregnancy has stopped. Unfortunately, this problem is not rare. According to statistics, in about 15% of cases, the planned babies "freeze" in the womb for one reason or another.
CONTENT:
- What is it?
- Dangerous timing: when can it happen?
- Why is this happening?
- How do doctors determine missed pregnancy?
- Signs and symptoms
- How to recover from a missed pregnancy?
- What tests to pass after?
- Answers from experts on whether ST cleanup is required.
- Frequently asked questions for which go to the forum.
What is it?
A dead pregnancy is a pregnancy that initially met all medical standards, but suddenly stopped developing in a certain period. The cessation of progress in the development of the fetus leads to its death, but it remains in the uterine cavity. For this reason, such a pathology is called a failed miscarriage.
In fact, at the very beginning, everything happens, as in a normal pregnancy - the egg is fertilized, enters the uterus and is implanted for further development, but it stops at one moment. This pathology also includes the syndrome of "empty fetal egg". It is the development of fetal membranes in which there is no embryo. With this syndrome, a pregnancy test is positive, as well as an analysis for hCG.
Dangerous timing: when can it happen?
The development of the fetus can stop at any time up to 28 weeks (in rare cases, the cessation of development can occur later), but the greatest likelihood of such a pathology occurs in the first trimester. There are also several periods with the highest risk of miscarriage, these include the following periods:
There are also several periods with the highest risk of miscarriage, these include the following periods:
- 3-4 weeks;
- 8-10 weeks;
- 16-18 weeks.
It is these terms that most often become critical for pregnancy.
Causes of miscarriage?
Even doctors are not always able to find out exactly why a miscarriage happened. In modern medicine, there are a number of reasons that can cause such a pathology. All of them are divided into several large groups:
- Genetic pathologies . It is these reasons that most often provoke a halt in fetal development. Pathological genes or the presence of an extra chromosome in the embryo can cause the development of many defects that are incompatible with life, which leads to termination of pregnancy. Often, genetic pathologies cause a stop in the development of pregnancy in the eighth to tenth week.
- Infections . A missed pregnancy can also often happen due to the presence of infectious diseases, since during the period of bearing a child, a woman experiences a rather serious decline in immune defenses.
 Especially dangerous for this period are TORCH infections, which include rubella, cytomegalovirus, herpes and toxoplasmosis. The greatest danger to the fetus is the first "meeting" of the mother with the infection in an already pregnant state. Therefore, when registering, pregnant women are strongly recommended to be screened for these types of infections. Even seemingly simple and familiar diseases such as influenza or SARS can cause pathology, especially in the early stages, when vital organs are formed in the fetus. The infection can affect the fetus directly, causing various types of anomalies, or on the membranes, resulting in a significant lack of oxygen or nutrients to the fetus.
Especially dangerous for this period are TORCH infections, which include rubella, cytomegalovirus, herpes and toxoplasmosis. The greatest danger to the fetus is the first "meeting" of the mother with the infection in an already pregnant state. Therefore, when registering, pregnant women are strongly recommended to be screened for these types of infections. Even seemingly simple and familiar diseases such as influenza or SARS can cause pathology, especially in the early stages, when vital organs are formed in the fetus. The infection can affect the fetus directly, causing various types of anomalies, or on the membranes, resulting in a significant lack of oxygen or nutrients to the fetus. - Hormonal disorders . Hormonal balance is extremely important for the normal bearing of a child. Therefore, with a lack of progesterone or an excess of male hormones (androgens), the likelihood of miscarriage significantly increases. Any hormonal disruptions are recommended to be treated before pregnancy.
- Antiphospholipid syndrome . Because of them, the formation of placental vessels or their blockage may also decrease, which leads to a violation of the fetus receiving the necessary nutrition.
- Teratozoospermia . This cause of a missed pregnancy is associated with pathologies in the seminal fluid of a man. With teratozoospermia, spermatozoa have an irregular structure, so fertilization with such a cell leads to abnormalities in the development of the embryo.
- Lifestyle . The presence of bad habits, as well as lifestyle during childbearing (and the planning period) can also adversely affect the development of the embryo, causing it to freeze. The use of alcoholic beverages, smoking, stress, occupational hazards, daily routine, sedentary lifestyle, unbalanced diet - all this is considered negative factors for pregnancy.
- Other factors. Pregnancy fading can also occur due to a sharp change in climate, a history of abortions (especially if there were several).
In some cases, several causes can be found at once, which could lead to a pregnancy fading.
How do doctors determine missed pregnancy?
At each examination of a pregnant woman, the gynecologist determines the size of the uterus, so if they do not correspond to the current period, the specialist may suspect the fetal fading. But such a diagnosis is made only after an ultrasound examination. In rare cases, ultrasound is not performed - if the woman turned to the doctor late and intoxication of the body has already occurred due to the death of the fetus.
Signs and symptoms
The symptoms of miscarriage in any trimester are the same. The main signs that may indicate such a pathology are:
- vaginal discharge with blood impurities;
- general weakness, chills, fever;
- drawing pains in the lower part of the abdomen;
- cessation of swelling and soreness of the mammary glands;
- abrupt disappearance of manifestations of toxicosis;
- absence of fetal movements (with pathology in the second trimester).
Despite the presence of characteristic symptoms of pathology, often the cessation of fetal development goes unnoticed, since the basal temperature can remain within 37 degrees, and the hCG level remains high for several more weeks. In this case, the woman learns about the problem only at the next appointment with the doctor or a planned ultrasound.
How to recover from a missed pregnancy?
If such a pathology occurs, it is imperative to remove the dead embryo from the uterine cavity, if this did not happen naturally. For this, a cleaning is carried out, with the help of which all particles of the fetal membranes are removed from the uterus. Both scraping and vacuum can be used. If the fading occurred at a very early date, doctors may suggest a medical abortion, which is somewhat more gentle for the woman, including psychologically.
Doctors recommend to refrain from the next pregnancy for six months (according to the recommendation of the World Health Organization).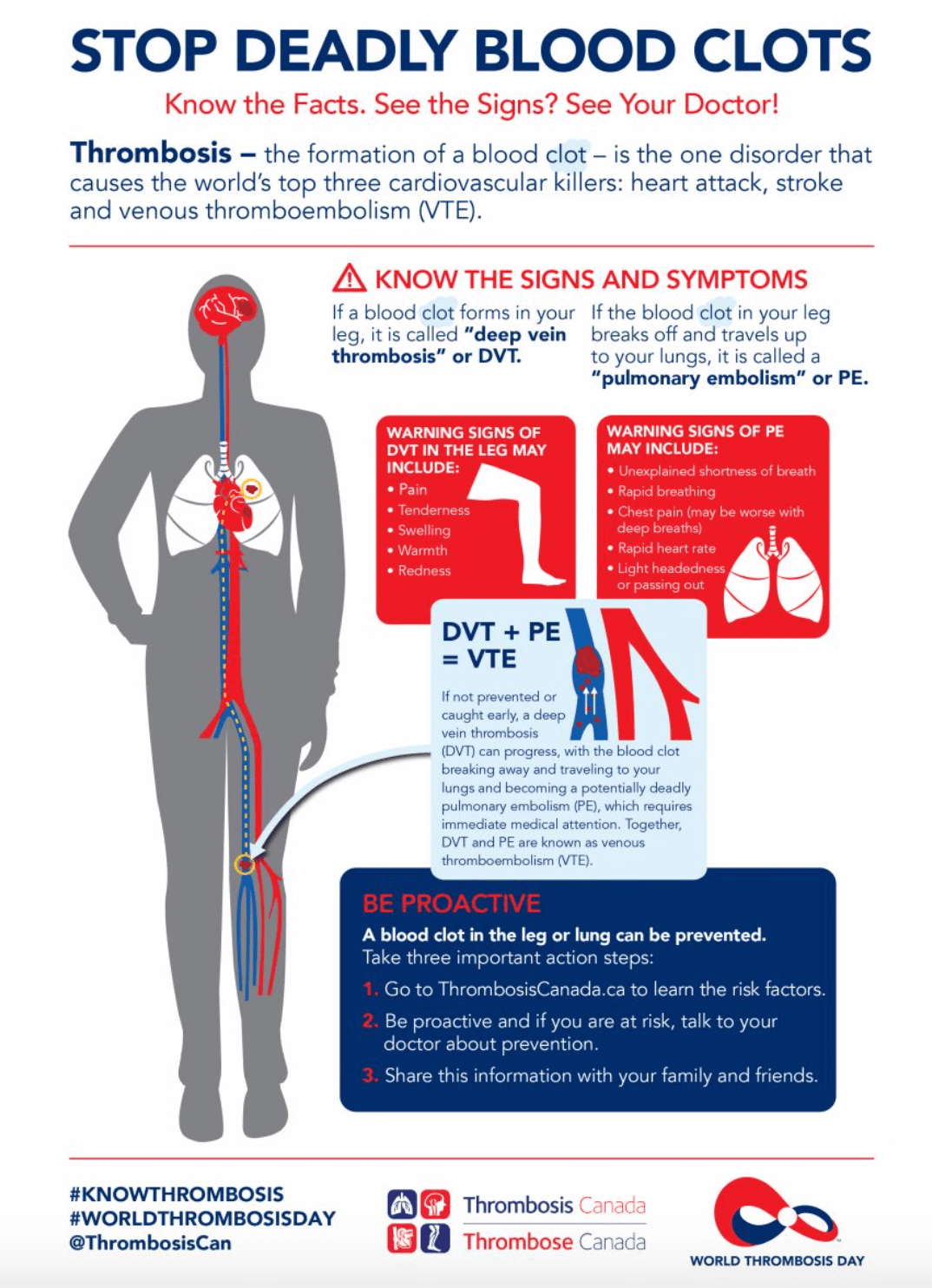 This time is enough for the body to recover after what happened. Therefore, during this time, women are advised to take oral contraceptives, which minimize the likelihood of conception, and also allow you to normalize hormonal levels.
This time is enough for the body to recover after what happened. Therefore, during this time, women are advised to take oral contraceptives, which minimize the likelihood of conception, and also allow you to normalize hormonal levels.
During recovery, it is also recommended to lead the most healthy and active lifestyle, take care of a balanced diet and take vitamin complexes. A woman definitely needs psychological support, and if she endured the incident especially hard, she may need the help of specialists - a psychologist or psychiatrist. This will help you get back to normal and prepare for your next pregnancy.
What tests to take after?
Before becoming pregnant after a missed pregnancy, it is necessary to exclude the possibility of a recurrence of what happened. Treatment should be appropriate to the problem that caused the pathology. Therefore, it is extremely important to undergo a complete examination, which will help determine the cause of the fetal development fading. According to the results of the examination, doctors prescribe treatment in accordance with the detected diseases.
According to the results of the examination, doctors prescribe treatment in accordance with the detected diseases.
It is recommended to undergo an examination after the restoration of the woman's menstrual cycle (usually takes about 30 days after cleansing). But both spouses should be tested. The full examination includes:
- genetic testing of spouses;
- tests for TORCH infections;
- study of hormonal levels;
- blood coagulogram;
- Gynecological ultrasound;
- spermogram;
- immunogram.
This examination is usually sufficient to determine the causes of miscarriage, both early and late. The attending physician may prescribe additional studies if necessary. All these examinations can be done at the IVF and infertility treatment clinic of Academician V.I. Grishchenko.
Missed pregnancy is not a verdict - in 90% of cases, after the occurrence of such a pathology, spouses become happy parents of healthy babies in the near future. The main thing is to undergo a complete examination and eliminate the cause of the pathology. And if necessary, you can go through the procedure of artificial insemination (IVF).
The main thing is to undergo a complete examination and eliminate the cause of the pathology. And if necessary, you can go through the procedure of artificial insemination (IVF).
Answers from specialists in the field of reproduction, fertility, women's health about whether cleaning is mandatory during a missed pregnancy.
On the Internet, the question is often asked: “Is it necessary to do curettage during a missed pregnancy (ZB)?”
We asked this question to our doctors:
Parashchuk Valentin Yuryevich
Head Physician of Academician Grishchenko Clinic, obstetrician-gynecologist, reproductologist.
Good afternoon. If the pregnancy froze at an early stage and there are no signs that it is going to resolve itself, that is, there is no bleeding, then it is advisable to evacuate the contents of the uterine cavity, that is, to do curettage. If the pregnancy seeks to resolve itself, then it can come out on its own. And then curettage is not required, you can just look at the ultrasound as soon as the discharge ends, that there are no inclusions in the uterine cavity, that there are no elements of the fetal egg in the uterine cavity.
If the pregnancy seeks to resolve itself, then it can come out on its own. And then curettage is not required, you can just look at the ultrasound as soon as the discharge ends, that there are no inclusions in the uterine cavity, that there are no elements of the fetal egg in the uterine cavity.
Another situation is when the pregnancy has stalled and you really need to evacuate the contents, and then there are alternative methods, sometimes they offer the so-called "medical abortion", that's the term. And it is more correct to do a scraping, or a vacuum, if the time permits. Because, sometimes, after these very medical abortions, you have to do scraping, but already in fact of complications. Because the entire contents of the uterine cavity does not always come out completely, and now inflammation joins, this is a big trauma for the uterus, this is already a conditionally urgent condition, and it is better not to allow it. Therefore, it is better to do a moderate, without severe injury and without complications, curettage on time than to do it as a necessary measure. When it is already clear that this is a frozen pregnancy, tactics can be discussed, but it is important to really understand when it is, which are such dangerous or alarming calls.
When it is already clear that this is a frozen pregnancy, tactics can be discussed, but it is important to really understand when it is, which are such dangerous or alarming calls.
The main complaint is if the uterus is already frozen and the uterus is trying to get rid of the pregnancy, then this is bloody discharge, that is, the pregnancy is already rejected. But it happens that she freezes and the patient knows absolutely nothing about it, and they become a godsend at a later date, when she is told that the fetal egg does not match in size, that she stopped earlier, and this cannot be suspected in any way. Therefore, if there are pains, pulling pains in the lower abdomen, spotting, you should definitely consult a doctor. Firstly, because it is not a fact that it is frozen. Or maybe it’s a threat of pregnancy fading, and you can turn in time, respond in time, stop the process and save the pregnancy. And if she really froze, then react in time and get rid of the fetal egg that has already stopped in development, without allowing any complications. In any case, if pain or spotting occurs during pregnancy, at any time, this is an indication to consult a doctor. There should be no pain, there should be no blood.
In any case, if pain or spotting occurs during pregnancy, at any time, this is an indication to consult a doctor. There should be no pain, there should be no blood.
Alipova Elena Konstantinovna
Obstetrician-gynecologist, reproductologist, ultrasound specialist.
The question is unconditional that the miscarriage must be removed from the uterus. That is, non-developing tissues, they are the source of the inflammatory process in the first place, and these tissues should be removed as soon as possible. The best method is still scraping.
As for not deleting at all, this is not even discussed. You can talk a little about medical abortion, but in my opinion, he also has no right to exist with a missed pregnancy. First, because everything needs to be done:
- fast;
- as carefully as possible.

And most the main thing is that scraping products, concept products, as they say now, can be sent in this case for genetic testing . And this, with a frozen pregnancy, is very important because, well, what happened, it happened, and everyone is interested in the question of why it happened. A genetic study of abortive material helps in about 80% of cases to answer the question of what happened after all. If genetics is to blame, this is one conversation, if everything is in order from a genetic point of view, additional examinations will be directed in another direction.
Lutsky Andrey Sergeevich
Obstetrician-gynecologist, reproductologist.
Hello. Today we will talk about missed pregnancy. There are surgical methods, such as curettage, vacuum aspiration and hysteroscopic removal of the ovum, and medical methods, the so-called "medical abortion" . Medical methods of abortion are indicated for women who have already had pregnancies in the past and had natural childbirth. This is due to the fact that the cervix of the uterus in such women is ajar and during induction, artificial induction of uterine contractions, a complete spontaneous abortion occurs, no residues remain in the uterine cavity. If the girl is nulliparous, then medical abortion often gives complications. Not everything comes out of the uterine cavity. Parts of the membranes remain, clots, and, let's say, a delay of these parts occurs and there may be an inflammatory process, as a result of which, subsequently, surgical intervention is required - curettage or vacuum aspiration. The method of terminating a missed pregnancy is chosen by the attending physician based on these data. In our clinic, we often encounter missed pregnancy in those women who want to give birth to their child. And to understand the genetics of the fetus, we often recommend hysteroscopic removal or vacuum aspiration of the ovum.
Medical methods of abortion are indicated for women who have already had pregnancies in the past and had natural childbirth. This is due to the fact that the cervix of the uterus in such women is ajar and during induction, artificial induction of uterine contractions, a complete spontaneous abortion occurs, no residues remain in the uterine cavity. If the girl is nulliparous, then medical abortion often gives complications. Not everything comes out of the uterine cavity. Parts of the membranes remain, clots, and, let's say, a delay of these parts occurs and there may be an inflammatory process, as a result of which, subsequently, surgical intervention is required - curettage or vacuum aspiration. The method of terminating a missed pregnancy is chosen by the attending physician based on these data. In our clinic, we often encounter missed pregnancy in those women who want to give birth to their child. And to understand the genetics of the fetus, we often recommend hysteroscopic removal or vacuum aspiration of the ovum.
Yuliya Vladimirovna Labuznaya
Obstetrician-gynecologist of the department of operative gynecology, doctor of the cervical pathology office
Hello. Today I will try to answer the most frequently asked questions regarding non-developing pregnancy. Perhaps I’ll start with such a rink: “Is it necessary to do vacuum aspiration of the contents of the uterine cavity, that is, the evacuation of a missed pregnancy, if a non-developing pregnancy is diagnosed?” And so let's deal with the concept. A non-developing pregnancy is a pathological condition in which pregnancy fades, but spontaneous expulsion from the uterine cavity does not occur. At the same time, the woman herself does not immediately understand what happened to her. The first signs of a missed pregnancy can appear 2-3 weeks after the incident. The fetal egg, which is located in the uterine cavity, undergoes various pathological changes, adversely affecting the endometrium, thereby causing an inflammatory process called "endometritis".
The fetal egg, which is located in the uterine cavity, undergoes various pathological changes, adversely affecting the endometrium, thereby causing an inflammatory process called "endometritis".
If a woman decides to wait for the spontaneous expulsion of a missed pregnancy from the uterine cavity, what happens? The endometrium tries to reject the frozen fetal egg, but the inflammatory processes taking place in this endometrium slow down this process, and the process can last from several days to several weeks. Which absolutely negatively affects the endometrium and contributes to the development of the inflammatory process further. There is an act that the fetal egg from the uterine cavity, as it were, came out, but not completely. There is a part of him left. From this part, often, a placental polyp is formed. The presence of a placental polyp in the uterine cavity contributes to the prevention of a subsequent pregnancy. Before the onset, planning a subsequent pregnancy, such a pali must be removed. In addition, the presence of a fetal egg in the uterine cavity for four weeks or more significantly increases the risk of bleeding. Therefore, the best solution to such an issue, in the presence of a missed pregnancy in a patient, is vacuum aspiration of the contents of the uterine cavity with the appointment of subsequent anti-inflammatory therapy.
In addition, the presence of a fetal egg in the uterine cavity for four weeks or more significantly increases the risk of bleeding. Therefore, the best solution to such an issue, in the presence of a missed pregnancy in a patient, is vacuum aspiration of the contents of the uterine cavity with the appointment of subsequent anti-inflammatory therapy.
The second issue is the errors in the diagnosis of non-developing pregnancy. For example, at 5-6 weeks, an ultrasound examination, in order to avoid such errors, is carried out by at least two specialists. If there are no clear criteria for non-developing pregnancy, it is recommended for the patient to repeat this study after 3-7 days. Again, to avoid mistakes. In addition, in parallel, the task of such an analysis as an analysis of human chorionic gonadotropin in the blood is mandatory. If the pregnancy develops, the hCG will increase accordingly, if the pregnancy is still frozen, then the hCG will either fall or not grow at all. If the gestational age is 7-8 weeks, then according to the ultrasound examination, the heart rate of the embryo will be absent. In addition, there will be a discrepancy between the size of the fetal egg and the gestational age. At gestational age 9-12 weeks, in addition to the lack of heart rate and the discrepancy between the gestational age and the size of the fetal egg, there will also be no movement of the embryo. It should always be remembered that every woman has the right to take a closer look at the ultrasound in a few days for an accurate diagnosis, to control the human chorionic gonadotropin, in fact, in order to avoid errors in the diagnosis of "non-developing pregnancy".
In addition, there will be a discrepancy between the size of the fetal egg and the gestational age. At gestational age 9-12 weeks, in addition to the lack of heart rate and the discrepancy between the gestational age and the size of the fetal egg, there will also be no movement of the embryo. It should always be remembered that every woman has the right to take a closer look at the ultrasound in a few days for an accurate diagnosis, to control the human chorionic gonadotropin, in fact, in order to avoid errors in the diagnosis of "non-developing pregnancy".
Answers to frequently asked and discussed questions on the forums:
✅ Can an ultrasound erroneously show a miscarriage?
The misdiagnosis of non-developing pregnancy occurs in the early stages. In our clinic, in order to avoid such errors, ultrasound at 5-6 weeks is performed by at least two specialists. If there are no clear criteria for non-developing pregnancy, then the patient is recommended to do a second study after 3-7 days. And on re-examination, it may turn out that the missed pregnancy was normal.
And on re-examination, it may turn out that the missed pregnancy was normal.
✅ With a missed pregnancy, is it possible to do without cleaning?
If a frozen pregnancy tends to resolve itself, then it can come out on its own, and then curettage (cleansing) is not required. As soon as the discharge ends, it is necessary to check on an ultrasound scan that there are no elements of the ovum left in the uterine cavity. If the pregnancy froze at an early stage and there are no signs that it is going to resolve itself, that is, there is no bleeding, then it is advisable to do a curettage.
✅ Frozen pregnancy - cleaning or pills?
Medical termination of pregnancy is indicated for women who have had pregnancies in the past and had natural childbirth. But it is more correct to do a scraping, or a vacuum, if the time permits. Because, sometimes, after medical abortions, you also have to do scraping, but already in fact of complications. Because the contents of the uterine cavity do not always come out completely, and inflammation is added, and this is a big trauma for the uterus and it is better not to allow this. Therefore, it is better to do a moderate, without severe injury and without complications, curettage on time than to do it as a necessary measure. And most importantly, scraping products can be sent for genetic testing to identify the causes of fetal development fading.
Therefore, it is better to do a moderate, without severe injury and without complications, curettage on time than to do it as a necessary measure. And most importantly, scraping products can be sent for genetic testing to identify the causes of fetal development fading.
✅ Can there be a miscarriage without symptoms?
It happens that the pregnancy stops, and the patient knows absolutely nothing about it, and this is discovered at a later date, when she is told that the fetal egg does not correspond in size, that the pregnancy stopped earlier, but this, unfortunately, it is impossible to suspect in advance. The first signs of a non-developing pregnancy can appear 2-3 weeks after the incident. These are spotting or pulling pains in the lower abdomen. With these symptoms, you should definitely consult a doctor.
✅ How long to wait for a miscarriage with a missed pregnancy?
If a woman decides to wait for the spontaneous expulsion of an undeveloped pregnancy, what happens? The endometrium tries to reject the frozen fetal egg, but the inflammatory processes taking place in this endometrium slow down this process, and the process can last from several days to several weeks.

:no_upscale()/cdn.vox-cdn.com/uploads/chorus_asset/file/3419302/Screen_Shot_2015-02-17_at_2.45.02_PM.0.png)