Is diarrhea a symptom of ectopic pregnancy
unusual cause of diarrhoea in a young female | QJM: An International Journal of Medicine
Navbar Search Filter QJM: An International Journal of MedicineThis issueMedicine and HealthBooksJournalsOxford Academic Mobile Microsite Search Term
Close
Navbar Search Filter QJM: An International Journal of MedicineThis issueMedicine and HealthBooksJournalsOxford Academic Microsite Search Term
Advanced Search
Journal Article
Nithya Ratnavelu,
Nithya Ratnavelu
Search for other works by this author on:
Oxford Academic
PubMed
Google Scholar
Michael J. Daly
Michael J. Daly
Search for other works by this author on:
Oxford Academic
PubMed
Google Scholar
QJM: An International Journal of Medicine, Volume 104, Issue 2, February 2011, Pages 161–162, https://doi.org/10.1093/qjmed/hcq070
Published:
14 May 2010
- Split View
-
- Article contents
- Figures & tables
- Video
- Audio
- Supplementary Data
-
Cite
Cite
Nithya Ratnavelu, Michael J.
 Daly, An unusual cause of diarrhoea in a young female, QJM: An International Journal of Medicine, Volume 104, Issue 2, February 2011, Pages 161–162, https://doi.org/10.1093/qjmed/hcq070
Daly, An unusual cause of diarrhoea in a young female, QJM: An International Journal of Medicine, Volume 104, Issue 2, February 2011, Pages 161–162, https://doi.org/10.1093/qjmed/hcq070Select Format Select format.ris (Mendeley, Papers, Zotero).enw (EndNote).bibtex (BibTex).txt (Medlars, RefWorks)
Close
-
Permissions
-
- More
Navbar Search Filter QJM: An International Journal of MedicineThis issueMedicine and HealthBooksJournalsOxford Academic Mobile Microsite Search Term
Close
Navbar Search Filter QJM: An International Journal of MedicineThis issueMedicine and HealthBooksJournalsOxford Academic Microsite Search Term
Advanced Search
In March 2010, a 32-year-old woman presented to hospital following 4 days of profuse watery diarrhoea. Her medical history included mild asthma, hypertension, ischaemic heart disease (myocardial infarction treated with balloon angioplasty 11 years previously) and she was a cigarette smoker of 20 per day for 18 years. Regular medications comprised ramipril, doxazosin and salbutamol inhalers prn. On admission, she was apyrexic, tachycardic (124 bpm), hypertensive (blood pressure 152/82 mmHg) and was noted to be morbidly obese (body mass index: 41 kg/m2). Clinical examination revealed no abnormality. Urinalysis was unremarkable. Initial laboratory investigations showed: Hb 13.7 g/dl [normal range (NR) 11.5–16.5 g/dl], leucocyte count 11.0 × 109/l (NR 4.0–10.0 x 109/l), urea 4.1 mmol/l (NR 3.3–8.8 mmol/l), creatinine 73 µmol/l (NR 40–110 µmol/l) and C-reactive protein 10.0 mg/l (NR 1.0–10.0 mg/l). She was biochemically euthyroid. Electrocardiogram showed a sinus rhythm and Q-waves consistent with an old inferior territory infarct. Serum β-hCG was markedly elevated at 8877 IU/l (NR <5 IU/l in non-pregnant women)—a titre consistent with 6 weeks gestation.
Her medical history included mild asthma, hypertension, ischaemic heart disease (myocardial infarction treated with balloon angioplasty 11 years previously) and she was a cigarette smoker of 20 per day for 18 years. Regular medications comprised ramipril, doxazosin and salbutamol inhalers prn. On admission, she was apyrexic, tachycardic (124 bpm), hypertensive (blood pressure 152/82 mmHg) and was noted to be morbidly obese (body mass index: 41 kg/m2). Clinical examination revealed no abnormality. Urinalysis was unremarkable. Initial laboratory investigations showed: Hb 13.7 g/dl [normal range (NR) 11.5–16.5 g/dl], leucocyte count 11.0 × 109/l (NR 4.0–10.0 x 109/l), urea 4.1 mmol/l (NR 3.3–8.8 mmol/l), creatinine 73 µmol/l (NR 40–110 µmol/l) and C-reactive protein 10.0 mg/l (NR 1.0–10.0 mg/l). She was biochemically euthyroid. Electrocardiogram showed a sinus rhythm and Q-waves consistent with an old inferior territory infarct. Serum β-hCG was markedly elevated at 8877 IU/l (NR <5 IU/l in non-pregnant women)—a titre consistent with 6 weeks gestation. Subsequent transvaginal ultrasound showed an empty uterus, free fluid in the Pouch of Douglas and an ectopic pregnancy with a foetal heart pulsation (Figure 1).
Subsequent transvaginal ultrasound showed an empty uterus, free fluid in the Pouch of Douglas and an ectopic pregnancy with a foetal heart pulsation (Figure 1).
Figure 1.
Open in new tabDownload slide
Crown-rump length measurement of live ectopic pregnancy in right fallopian tube as seen on transvaginal ultrasound.
Laparoscopy, performed under general anaesthetic, revealed haemoperitoneum and an unruptured right tubal ectopic pregnancy (Figure 2) and she was treated with a right salpingectomy. Subsequent histopathology showed a small focus of salpingitis isthmica nodosa, a predisposing factor for tubal ectopic pregnancy. The patient had an uneventful post-operative course and was discharged home the next day.
Figure 2.
Open in new tabDownload slide
Unruptured ectopic pregnancy in distended fallopian tube as seen on laparoscopy.
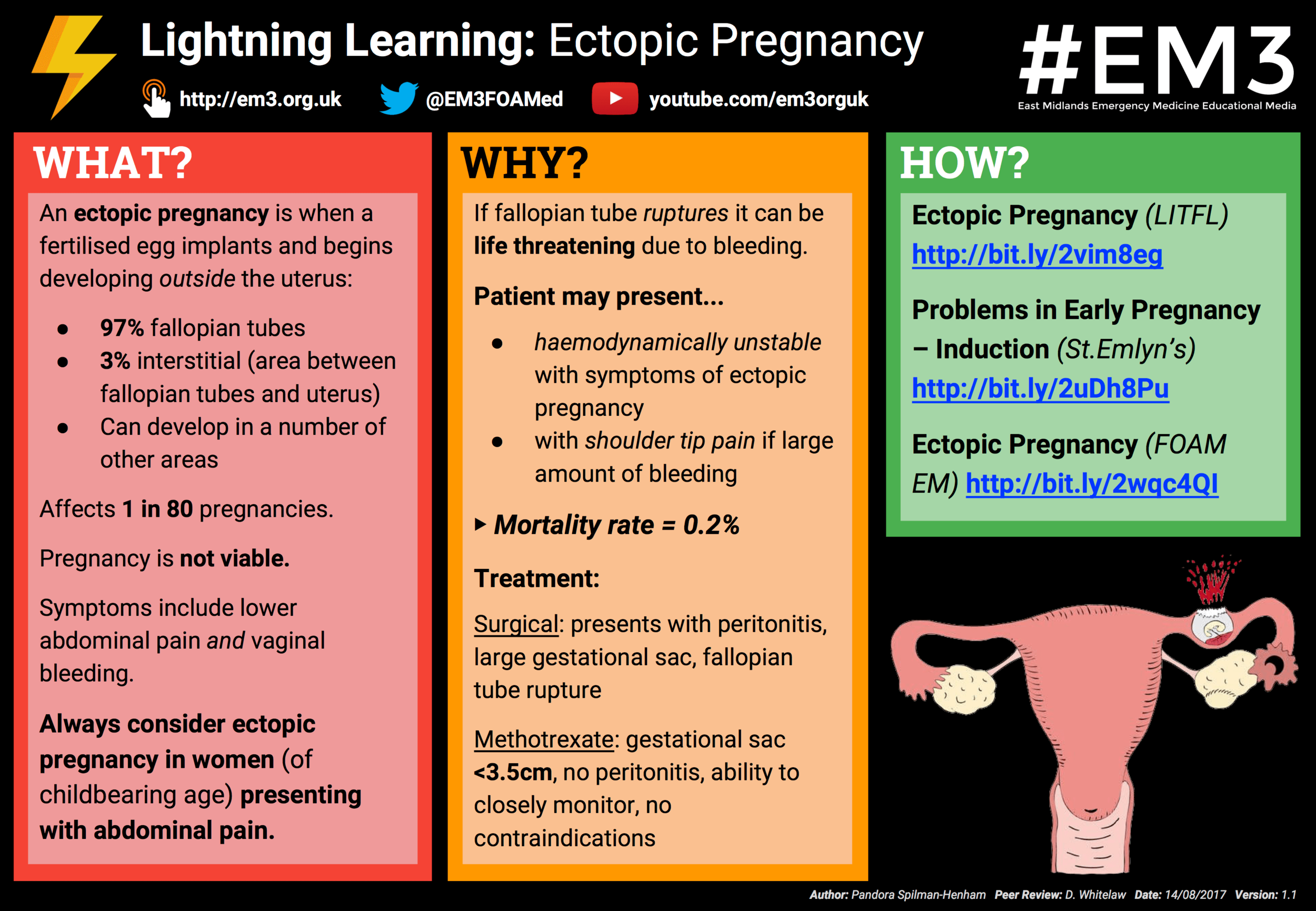
Ectopic pregnancies are relatively common (11.1/1000 maternities) and usually occur as a result of either decreased blastocyst motility along the fallopian tube or alterations in the tubal environment facilitating early implantation. 1 These include previous ectopic pregnancy, structural tubal abnormality, pelvic imflammatory disease, assisted reproduction techniques, intrauterine contraceptive devices and tubal surgery, e.g. salpingotomy and tubal ligation.2
1 These include previous ectopic pregnancy, structural tubal abnormality, pelvic imflammatory disease, assisted reproduction techniques, intrauterine contraceptive devices and tubal surgery, e.g. salpingotomy and tubal ligation.2
The hallmarks of presentation are bleeding per vaginum, localized abdominal pain, shoulder-tip pain, collapse and diarrhoea. The immediate danger once symptomatic is that of delayed diagnosis, resulting in tubal rupture, haemorrhage, shock and ultimately death. It is therefore of utmost importance that ectopic pregnancy be excluded in any woman, presenting with any of the above symptoms, in whom an intrauterine pregnancy has not been confirmed by ultrasound. Diarrhoea is a presenting symptom in many ectopic pregnancies. As in this case, a difficult clinical examination in combination with an uncommon presenting symptom can result in delayed diagnosis and complication development.
Tubal pregnancy can be managed by laparotomy, operative laparoscopy, medically, i. e. methotrexate, and occasionally by observation alone. Management must be tailored to the clinical condition and future fertility requirements of the woman. In the context of serum β-hCG level >3000 IU/l and a positive foetal heart, expectant and medical management are discouraged.3
e. methotrexate, and occasionally by observation alone. Management must be tailored to the clinical condition and future fertility requirements of the woman. In the context of serum β-hCG level >3000 IU/l and a positive foetal heart, expectant and medical management are discouraged.3
In summary, atypical presentations of ectopic pregnancies are important to recognize as they can often mimic gastrointestinal disease. It is recommended that women of reproductive age, who present with diarrhoea, vomiting and/or collapse, be investigated for possible ectopic pregnancy.4 Clinicians should use a combination of clinical suspicion, serum β-hCG tracking and ultrasound scanning to diagnose ectopic pregnancies in a timely manner.
Conflict of interests: None declared.
1
Shaw
JL
,
,
Critchley
HO
,
Horne
AW
.
Current knowledge of the aetiology of human tubal ectopic pregnancy
,
Hum Reprod Update
,
2010
2
Lenore
JL
.
Ectopic pregnancy
,
Am Fam Physician
,
2000
, vol.
61
(pg.
1080
-
88
)
3
Royal College of Obstetricians and Gynaecologists
,
The Management of Tubal Pregnancy. Green-top Guideline No. 21
,
2004
London
RCOG
4
Lewis
G
.
The Confidential Enquiry into Maternal and Child Health (CEMACH)
,
Saving Mothers’ Lives: reviewing maternal deaths to make motherhood safer 2003–2005
,
2007
London, CEMACH
The Seventh Report on Confidential Enquiries into Maternal Deaths in the United Kingdom
© The Author 2010. Published by Oxford University Press on behalf of the Association of Physicians. All rights reserved. For Permissions, please email: [email protected]
© The Author 2010. Published by Oxford University Press on behalf of the Association of Physicians. All rights reserved. For Permissions, please email: [email protected]
Issue Section:
Case reports
Download all slides
Advertisement
Citations
Altmetric
More metrics information
Email alerts
Article activity alert
Advance article alerts
New issue alert
Receive exclusive offers and updates from Oxford Academic
Citing articles via
-
Latest
-
Most Read
-
Most Cited
LEOPARD syndrome with hypertrophic cardiomyopathy
Hospital size, remoteness and stroke outcome
Postpartum scleroderma renal crisis with renal thrombotic microangiopathy
Combined posterior spinal cord and ipsilateral cerebellar infarction
Early menarche and enhanced risk for the development of health problems
Advertisement
Ectopic pregnancy - Symptoms - NHS
Symptoms of an ectopic pregnancy usually develop between the 4th and 12th weeks of pregnancy.
Some women don't have any symptoms at first. They may not find out they have an ectopic pregnancy until an early scan shows the problem or they develop more serious symptoms later on.
Main symptoms
You may have an ectopic pregnancy if you miss a period, have a positive pregnancy test, and have other signs of pregnancy.
Contact your GP or call NHS 111 if you have a combination of any of these symptoms and you think you might be pregnant – even if you haven't had a positive pregnancy test.
Vaginal bleeding
Vaginal bleeding tends to be a bit different to your regular period. It often starts and stops, and may be watery and dark brown in colour.
Some women mistake this bleeding for a regular period and don't realise they're pregnant.
Vaginal bleeding during pregnancy is relatively common and isn't necessarily a sign of a serious problem, but you should seek medical advice if you experience it.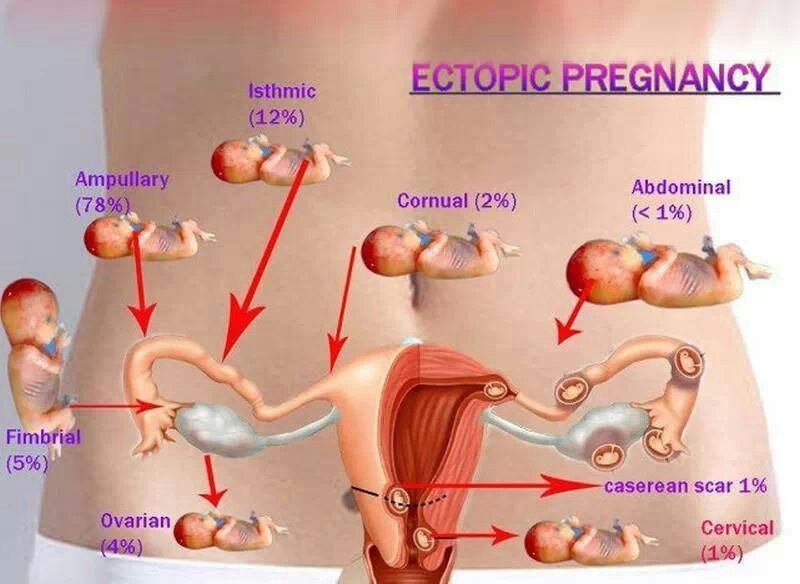
Tummy pain
You may experience tummy pain, typically low down on one side. It can develop suddenly or gradually, and may be persistent or come and go.
Tummy pain can have lots of causes, including stomach bugs and trapped wind, so it doesn't necessarily mean you have an ectopic pregnancy.
But you should get medical advice if you have it and think you might be pregnant.
Shoulder tip pain
Shoulder tip pain is an unusual pain felt where your shoulder ends and your arm begins.
It's not known exactly why it occurs, but it can be a sign of an ectopic pregnancy causing some internal bleeding, so you should get medical advice right away if you experience it.
Discomfort when going to the toilet
You may experience pain when going for a pee or poo.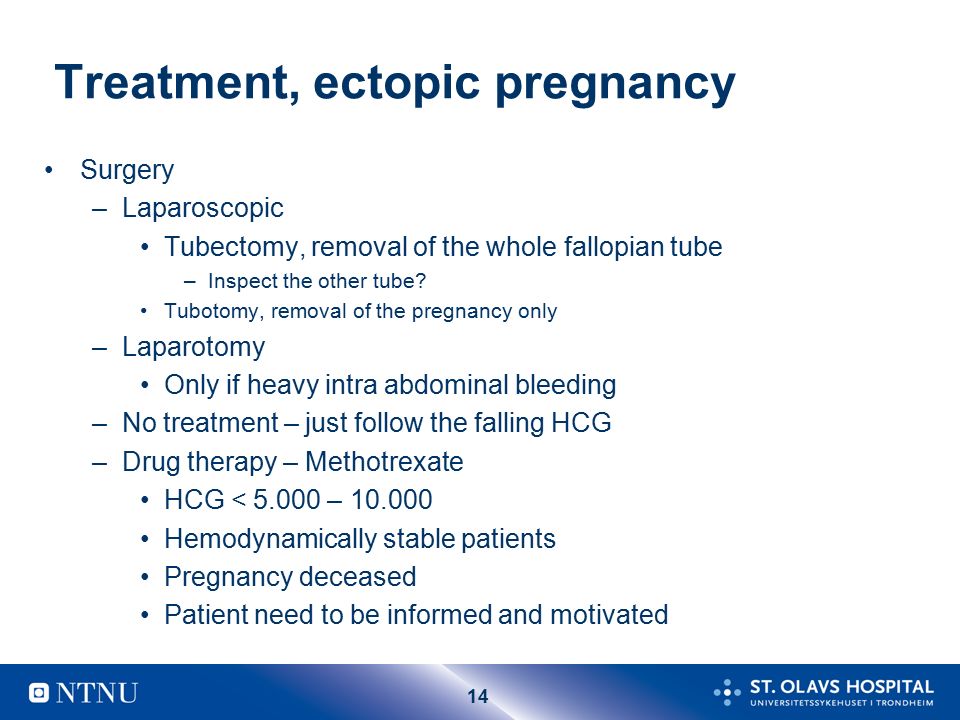 You may also have diarrhoea.
You may also have diarrhoea.
Some changes to your normal bladder and bowel patterns are normal during pregnancy, and these symptoms can be caused by urinary tract infections and stomach bugs.
But it's still a good idea to seek medical advice if you experience these symptoms and think you might be pregnant.
Symptoms of a rupture
In a few cases, an ectopic pregnancy can grow large enough to split open the fallopian tube. This is known as a rupture.
Ruptures are very serious, and surgery to repair the fallopian tube needs to be carried out as soon as possible.
Signs of a rupture include a combination of:
- a sharp, sudden and intense pain in your tummy
- feeling very dizzy or fainting
- feeling sick
Call 999 for an ambulance or go to your nearest accident and emergency (A&E) department immediately if you experience these symptoms.
Page last reviewed: 23 August 2022
Next review due: 23 August 2025
Ectopic pregnancy - symptoms and causes
An ectopic pregnancy is when a fertilized egg attaches itself outside the uterine cavity, in the fallopian tube. The normal course of pregnancy is characterized by the fact that the egg is fertilized in the fallopian tube, and then through the same tube enters the uterus, and is fixed on the uterine mucosa.
If the tube is damaged or its function is disturbed, then this movement does not occur, the zygote is attached directly to the tube. Similarly, if there are any abnormalities, then the zygote can attach to the ovary, remain in the abdominal cavity, or descend into the cervix. nine0003
At the same time, the development of the fetus continues, and all the symptoms of pregnancy are present. The patients have no complaints. But the appearance of the first symptoms is possible for a period of 5 weeks, and this range is up to 14 weeks. In an ectopic pregnancy, the development of the child is impossible, and termination is required because the developing zygote can rupture the fallopian tube. Such a gap is a life-threatening condition, because it is accompanied by heavy bleeding.
In an ectopic pregnancy, the development of the child is impossible, and termination is required because the developing zygote can rupture the fallopian tube. Such a gap is a life-threatening condition, because it is accompanied by heavy bleeding.
Symptoms of ectopic pregnancy
As already mentioned, initially there are no symptoms of an ectopic pregnancy, except for the usual delay in menstruation, which is regarded by everyone as the onset of a desired pregnancy. And only on ultrasound at an early stage you can see this pathology. However, at 5-14 weeks, the so-called tubal abortion occurs, which has the following symptoms:
Signs of rupture of the fallopian tube:
- severe sharp pain;
- dizziness and pre-syncope; nine0015 nausea and vomiting;
- diarrhea;
- Pain that occurs on one side of the abdomen and radiates very clearly in the shoulder. It can increase with urination and bowel movements;
- dark, less often bright red spotting from the vagina appears.
 If the rupture of the tube occurred for a period of 5 weeks, then many women take the discharge simply as the beginning of painful menstruation.
If the rupture of the tube occurred for a period of 5 weeks, then many women take the discharge simply as the beginning of painful menstruation.
What causes shoulder pain when a tube ruptures in an ectopic pregnancy? Bleeding irritates the phrenic nerve. This nerve is located in the muscle that separates the chest cavity from the abdominal cavity. Its main function is participation in the process of respiration. Irritation of the phrenic nerve causes referred pain in the shoulder joint. nine0003
Often, the atypical symptoms of a tube rupture can mislead a woman about her condition. These are symptoms of diseases of the gastrointestinal tract, which are accompanied by diarrhea and vomiting.
The most acute and severe symptom of a tube rupture is shock, which is manifested by the following symptoms:
- dizziness and fainting;
- sudden sharp pain in the abdomen;
- nausea;
- increased heart rate; nine0016
- pallor;
- diarrhea.
Since this is a life-threatening condition, an ambulance must be called immediately.
Other articles:
Section: Obstetrics and gynecology Diagnostics Gynecological operationsterms, signs, symptoms of ectopic pregnancy
An ectopic pregnancy is the attachment and development of an embryo outside the uterus. The condition is dangerous to health and, in the absence of medical assistance, leads to severe complications or death. nine0003
Causes of an ectopic pregnancy
An ectopic pregnancy is formed when the tubes are blocked, due to which the egg cannot enter the uterine cavity. Pathology is caused by such factors:
- adhesive process after an unsuccessful surgical intervention;
- hormonal imbalance due to stress, contraceptives, drugs, endocrine dysfunction;
- genetic predisposition; nine0016
- inflammatory processes;
- genital injuries;
- malignant or benign neoplasms;
- congenital anomalies of the structure of the genital organs;
- frequent change of sexual partners, which leads to infectious diseases.
Women who have had a surgical abortion are susceptible to ectopic pregnancy. Curettage destroys the mucous membrane, leads to endometriosis and scarring, which prevents the egg from entering the uterine cavity. The more abortions in history, the higher the risk of pathology. nine0003
Women who smoke are 3 times more likely to have an ectopic pregnancy than non-smokers. Nicotine inhibits the epithelial function of the fallopian tubes, which ensures the promotion of the embryo.
The risk of ectopic pregnancy is increased in women aged 35-45 years. This is due to age-related physiological and hormonal changes in the body. The probability of an ectopic pregnancy is 30% higher in women who have already suffered a pathological condition and have not completed a full course of treatment.
How to distinguish an ectopic pregnancy from a normal one
Signs of an ectopic pregnancy are similar to those of a normal pregnancy until the 3rd week of its development. With a positive result on the test, the second strip may be colored a little lighter. The following symptoms are observed:
With a positive result on the test, the second strip may be colored a little lighter. The following symptoms are observed:
- dizziness, drowsiness, weakness, nausea;
- absence of menstruation;
- change in taste preferences;
- breast enlargement.
At 5-6 weeks growth of the fetal egg becomes more intense, pathological signs appear:
- regular pulling pain that radiates to the perineum or anus;
- diarrhea, vomiting;
- pain during urination or defecation;
- bloody discharge that does not look like menstruation;
- spasmodic pain localized at the site of attachment of the embryo.
If you experience one or more symptoms of an ectopic pregnancy, you should consult a gynecologist. Timely medical attention will prevent health complications. nine0003
Spontaneous termination of pregnancy begins by 5-8 weeks. The growing embryo causes a rupture of the tube and provokes internal bleeding.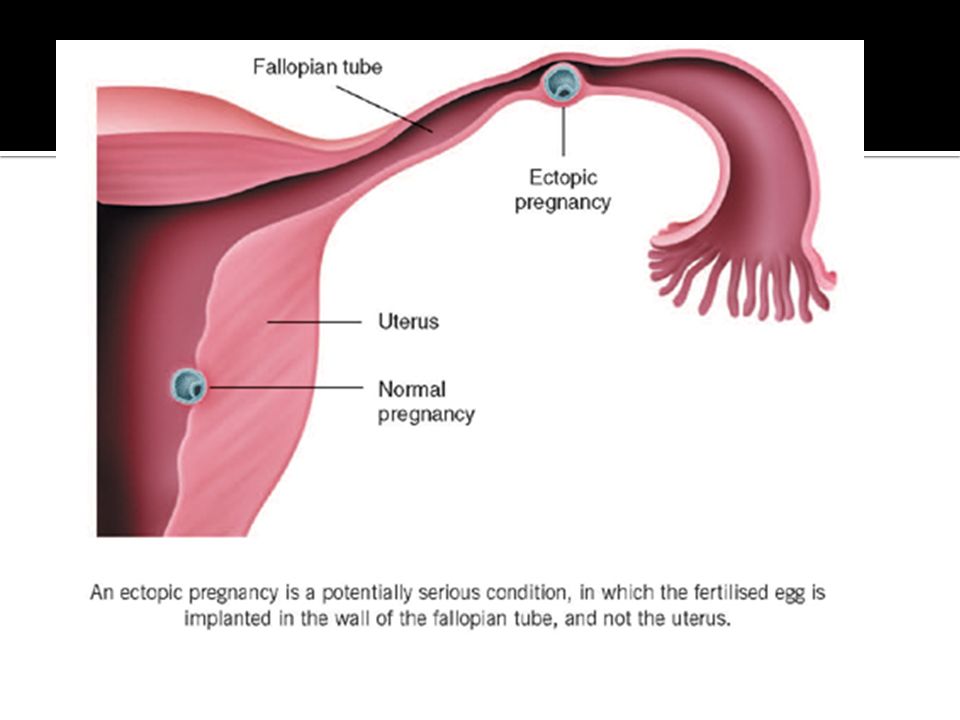 The condition is accompanied by weakness, blanching, loss of consciousness. If emergency care is not provided at this stage, the woman may die from hemorrhagic shock.
The condition is accompanied by weakness, blanching, loss of consciousness. If emergency care is not provided at this stage, the woman may die from hemorrhagic shock.
Methods for diagnosing ectopic pregnancy
At the beginning of the examination, the doctor conducts an examination and history taking. Based on the results, a diagnosis is made. An ectopic pregnancy is detected in several ways:
- Ultrasound. Detects the presence of an embryo in the uterus. To determine the exact location of the ovum, a transvaginal ultrasound is performed using a transducer.
- Daily monitoring of hCG levels. In contrast to normal, with an ectopic pregnancy, the indicator is different.
- Laparoscopy. Indicated in cases where the position of the gestational sac cannot be determined by ultrasound. Diagnosis is made with an endoscope through a small incision in the abdomen. If an ectopic pregnancy is detected for a short period, laparoscopic extraction of the embryo is possible if its size does not exceed 2 cm.