Infant size percentile
Baby growth charts: Percentiles, reading a growth chart, and more
Baby growth charts track your child's growth over time and compare it to that of similar babies. Growth charts can show you how your baby's growing and alert your doctor if there's a potential problem. It's easy to get caught up in growth chart percentiles and how your baby measures up, but keep in mind that there's a wide range of normal. Also, what you see on your baby's growth chart now doesn't predict their size as an adult.
What is a baby growth chart?
A baby growth chart is a tool that your baby's doctor will use to track their growth over time and compare it to other babies the same age and sex. Growth charts were developed using measurements from thousands of children.
At every doctor visit, your baby's healthcare provider will measure:
- Your baby's weight
- Your baby's height/length (measured lying down)
- Your baby's head circumference (measured around the head above the eyebrows)
The doctor will plot these measurements on the growth chart and show it to you. Depending on where the measurements fall on the chart, you can see how your baby's growth compares to that of similar babies.
Your baby's growth chart can give you a general picture of how they're developing physically, and their doctor will use it to determine whether your baby is growing in a healthy way.
But try not to get too hung up on your baby's growth chart – it's not the last word on how your baby is doing. There's a wide range of normal, and your baby's measurements don't mean they'll be short or tall, or fat or skinny, as an adult. The most important thing is that your baby is growing at a steady, appropriate rate over time.
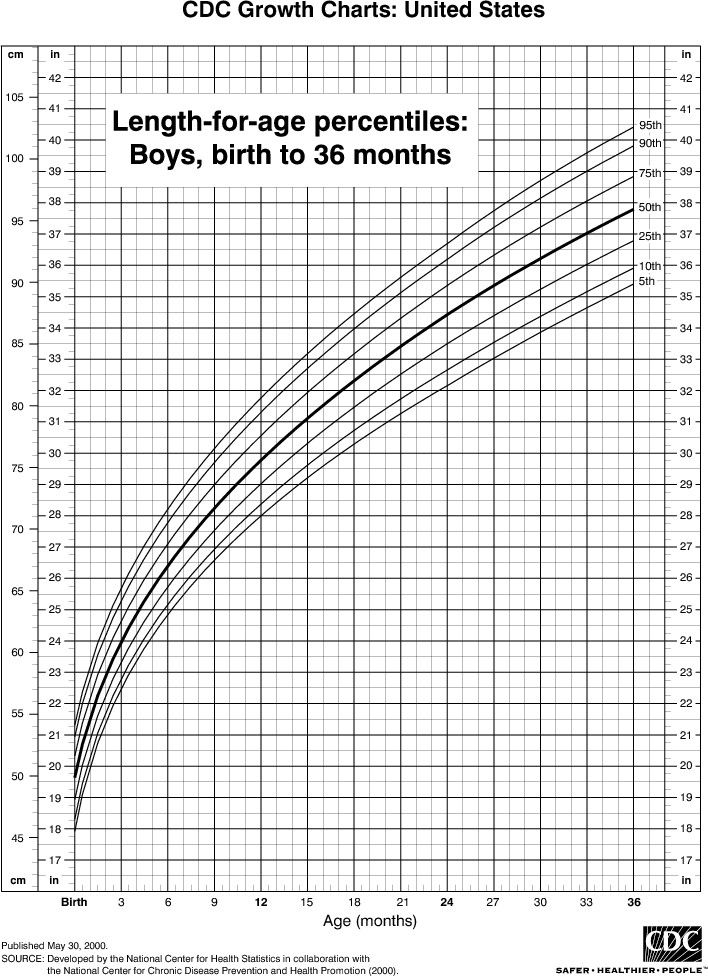
Note: The U.S. Centers for Disease Control (CDC) recommends that doctors use the charts from the World Health Organization (WHO) for the first 24 months of a child's life. After age 2, doctors typically use the CDC's growth charts, which are similar but based on different data.
The charts from both organizations show length in inches and centimeters as well as weight in pounds and kilograms.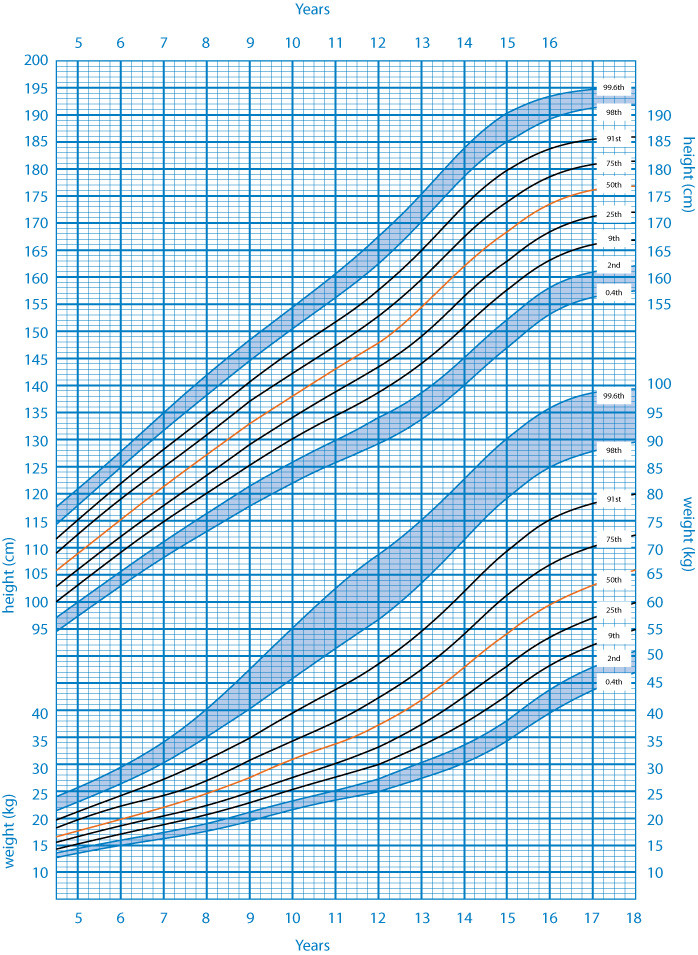 Both charts also use percentiles, which compare averages of children broken down by age.
Both charts also use percentiles, which compare averages of children broken down by age.
How do growth chart percentiles work?
This is easiest to explain by example. If your 3-month-old daughter is in the 40th percentile for weight, that means 40 percent of 3-month-old girls weigh less than your baby, and 60 percent weigh more.
The higher the percentile number, the bigger your baby is compared to other babies the same age. If your baby is in the 50th percentile, that means they fall right in the middle of the pack.
To chart your baby's growth at home, try our growth percentile calculator.
Percentiles in a growth chart aren't like grades in school. A higher percentile isn't better, and a lower percentile doesn't mean there's anything wrong with your baby.
Let's say both parents are shorter than average, and your baby grows up to have the same stature. It would be perfectly normal for them to rank consistently in the 10th percentile for height and weight as they grow up.
What's important to remember is that your doctor is watching how your baby grows, not just how much.
Babies tend to go through rapid growth spurts, during which they might put on a little extra weight or length. Other months they may grow only a fraction of what they normally do. Your child's doctor notes individual peaks and valleys, but they'll be more focused on the overall pattern of growth.
Should I worry about my baby's growth?
It could be cause for concern if your baby's percentile changes significantly. For example, if they're consistently been around the 50th percentile for weight and then suddenly drops into the 15th, your baby's doctor will want to figure out why. There could be a medical reason for the change that needs further evaluation.
A minor illness or a change in your baby's eating patterns might result in a smaller drop, in which case the doctor may just follow your baby's growth more closely for a while.
If your baby hasn't been sick but their weight gain is slowing down while they're still growing in length, your child's doctor may suggest increasing the number of feedings. You may have to go in for more frequent visits to make sure that your baby starts gaining weight again.
You may have to go in for more frequent visits to make sure that your baby starts gaining weight again.
There are times when gaining or losing faster than usual is a good thing. If your baby was underweight, for example, it may be a good sign that they're gaining ounces faster than growing inches.
Also, being at one end of the growth spectrum isn't always a reason to worry. For example, if your baby is very short and both parents are relatively short, then it may be perfectly appropriate for them to be in the lowest 5 percent.
But if your baby is very short and both parents are average height or taller, or if your baby is very slender and both parents are average weight or larger, then the doctor will make sure that there's no problem with the baby's growth (like a hormone deficiency or genetic problem).
Also, if your baby is in the top 5 percent for weight, the doctor will keep an eye on their growth – and possibly counsel you about their feedings – to make sure they aren't at risk for obesity.
If your baby's head measurement is much smaller than average, the doctor will make sure that their brain is growing and developing normally (a baby's brain growth is reflected in the size of their skull). If your baby's head circumference is much larger than average, they'll be further evaluated to make sure that they don't have excess fluid in the brain, a condition called hydrocephalus.
How much does birth weight determine future growth?
Birth weight seems to matter less than you might think. Genes, not newborn weight, generally determine adult size. Petite babies sometimes grow to be strapping adults, and large babies can become slender over the years.
A baby's parents are the best indicator – are you and your partner tall, short, or average? Slender, heavy, or medium? Chances are, your child will be similarly built as an adult.
Child height predictor: How tall your child will be
girlboy
Child's age
Child's height *
Child's weight *
Mother's height *
Father's height *
Curious to find out how tall your child will be when they grow up? We can't see the future, but with a little math and science, we can make a pretty good guess about how tall they'll be when they're 18 – with a margin of error under 2 inches.
This calculator works for children age 2 and up. (Depending on your child's age, we'll use some or all of the information you entered in our calculations.) You may get inaccurate results for children who are exceptionally tall or are already taller than both their parents.
The Height Predictor is meant to be a fun tool, and doesn't guarantee your child will be this height when they grow up. If you're concerned about your child's growth, talk to their healthcare provider.
How to tell how tall your child will be
There are a few different methods of predicting how tall your child will be when they grow up. Our Child Height Predictor tool uses the Khamis-Roche method, which is based on a study conducted in the 1990s with about 400 participants.
The method takes a child's height, weight, and the average height of their parents, then uses ratios to determine how to calculate the child's predicted height at age 18. A previous method also used the child's skeletal age, which is how mature a child's bones are and requires an X-ray.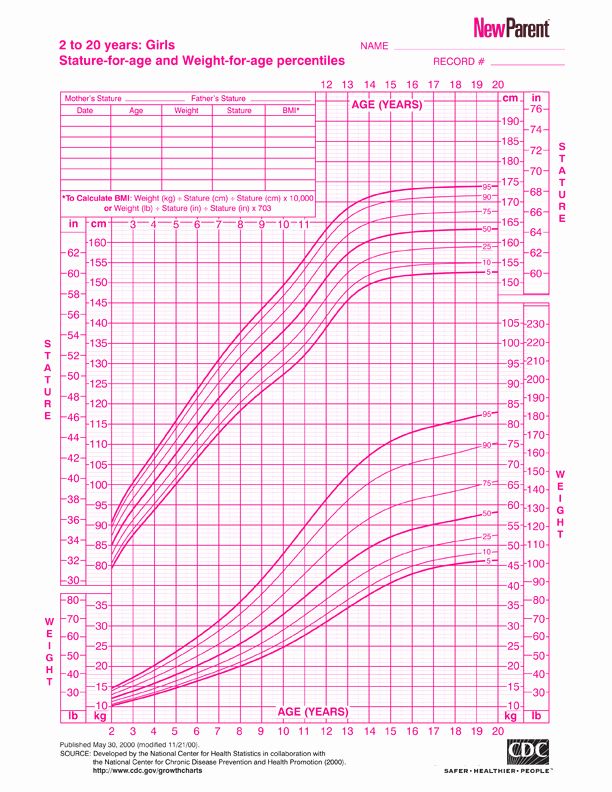 But the Khamis-Roche researchers wanted to find a way parents could predict their child's height without having to get an X-ray taken.
But the Khamis-Roche researchers wanted to find a way parents could predict their child's height without having to get an X-ray taken.
If you want to test out other ways to predict your child's height at home, these are a couple methods you can try:
Two years times two
Children grow a ton in their first few years of life – in fact, their first growth spurt from baby to toddler accounts for about half of their adult height. One simple way to predict how tall your child will be when they grow up is to take their height at age 2 if they're a boy or 18 months if they're a girl and double it. (Girls grow a little faster than boys.)
This method has been around for a long time, but there isn't any scientific research about how accurate it is.
Mid-parental method
Another way to estimate your child's adult height is to add together the height of both parents and divide it by two.
Then, some methods say to add 5 inches if they're a boy and subtract 5 inches if they're a girl; others say to only add or subtract 2 ½ inches. There's a high margin of error with this method – it could be off by 4 inches.
There's a high margin of error with this method – it could be off by 4 inches.
Rebekah Wahlberg
Rebekah Wahlberg is an associate editor at BabyCenter, the world's number one digital parenting resource. She lives in Southern California with her silly dog Booger, where she enjoys hiking, yoga, and watching Netflix when she "should" be reading. Wahlberg is passionate about creating content that helps parents and parents-to-be equip themselves with everything they need to succeed.
Advertisement | page continues below
Fetal growth retardation, the fetus is not gaining weight, what to expect? Part 2 – Family Clinic
In one of the previous articles, we discussed the topic of fetal growth retardation. We got acquainted with some competent terms, and came to the conclusion that the diagnosis is made on the basis of ultrasound parameters, when certain indicators are less than normal.
In this article, we will consider the norms for the size of the fetus, what are they?
Each doctor who performs ultrasound during pregnancy has a special table (it can be in paper or electronic form) that indicates the parameters, weeks of gestation, and percentiles: namely the 10th percentile, 50th percentile and 9th percentile0th percentile. A percentile is a statistic. The number of percentiles can change, as well as the number of parameters. It is important to understand that the fetus does not grow according to a textbook, but according to its genetic program, and the tasks of an obstetrician-gynecologist with an ultrasound doctor should be understood in dynamics: is it an individual feature of the baby of such intrauterine growth or, indeed, due to placental insufficiency, he lags behind in growth. There are a number of malformations and chromosomal diseases, due to which the fetus is stunted, but then the doctor will suspect this on an ultrasound scan and send it for additional examination.
A percentile is a statistic. The number of percentiles can change, as well as the number of parameters. It is important to understand that the fetus does not grow according to a textbook, but according to its genetic program, and the tasks of an obstetrician-gynecologist with an ultrasound doctor should be understood in dynamics: is it an individual feature of the baby of such intrauterine growth or, indeed, due to placental insufficiency, he lags behind in growth. There are a number of malformations and chromosomal diseases, due to which the fetus is stunted, but then the doctor will suspect this on an ultrasound scan and send it for additional examination.
So, an example of a table of indicators of intrauterine dimensions of the fetus. Let's take the example of 33 weeks pregnant. This line is highlighted in red. Percentiles indicate the relative position of an individual in the standardization sample. These are some average statistical indicators that help, first of all, doctors navigate between the norm and pathology. If your gestational age is 33 weeks, and all indicators of fetometry (sizes of different parts of the fetal body) fit into this line, highlighted in red, then there is no reason for alarm. "According to the textbook" is the 50th percentile (the most common indicator of the norm in the population). But the fetus can be larger or smaller. Remember how at school age you lined up in physical education classes, who is taller, who is lower, but all the good guys turned out to be. In percentiles, the same logic, someone is larger (then the doctor will say the phrase: the biparietal size corresponds to 90 percentile for 33 weeks gestation), someone smaller (then the doctor will say the phrase: the size of the femur corresponds to the 10 percentile for 33 weeks gestation). Both of these are normal, and there is no cause for alarm.
If your gestational age is 33 weeks, and all indicators of fetometry (sizes of different parts of the fetal body) fit into this line, highlighted in red, then there is no reason for alarm. "According to the textbook" is the 50th percentile (the most common indicator of the norm in the population). But the fetus can be larger or smaller. Remember how at school age you lined up in physical education classes, who is taller, who is lower, but all the good guys turned out to be. In percentiles, the same logic, someone is larger (then the doctor will say the phrase: the biparietal size corresponds to 90 percentile for 33 weeks gestation), someone smaller (then the doctor will say the phrase: the size of the femur corresponds to the 10 percentile for 33 weeks gestation). Both of these are normal, and there is no cause for alarm.
As in the previous article on fetal growth retardation, let's repeat the main fetometric indicators that guide the assessment of intrauterine growth of the fetus: biparietal size, head circumference, abdominal circumference, femur length.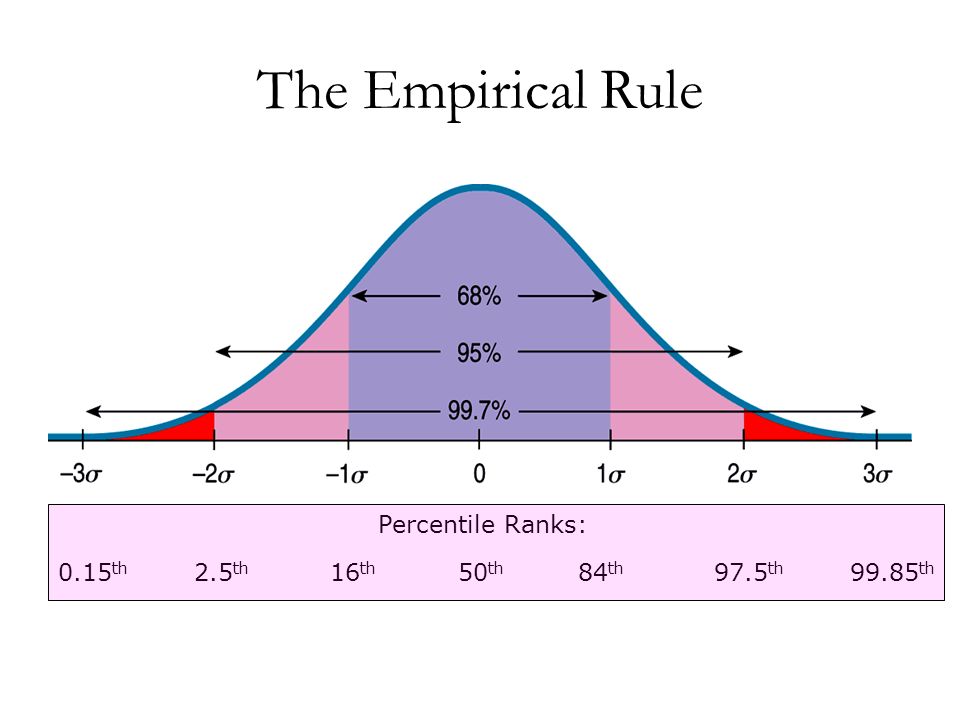 These indicators are highlighted in the table with multi-colored columns. The estimated fetal weight is calculated using a mathematical formula based on these figures.
These indicators are highlighted in the table with multi-colored columns. The estimated fetal weight is calculated using a mathematical formula based on these figures.
In this article, we tried to get acquainted with the principles of assessing intrauterine fetal growth, we saw percentiles and their spread. If you are diagnosed with fetal growth retardation, consult this plate with your doctor to find out if this is true, ask your doctor for an ultrasound. And remember, your baby is individual, the best and most beautiful, let him also grow individually in utero, according to his genetic program.
Obstetrician-gynecologists and ultrasound doctors of the FAMILY CLINIC are ready to answer all questions about the development of the fetus and the course of pregnancy, as well as take care of your pregnancy so that you have a healthy baby.
Which fruit is better - small or large?
It is often necessary to answer the questions of desperate women who, after undergoing an ultrasound scan, suddenly find out that their child is lagging behind in growth (or intrauterine development), and, as always, they need to urgently go to the hospital for treatment.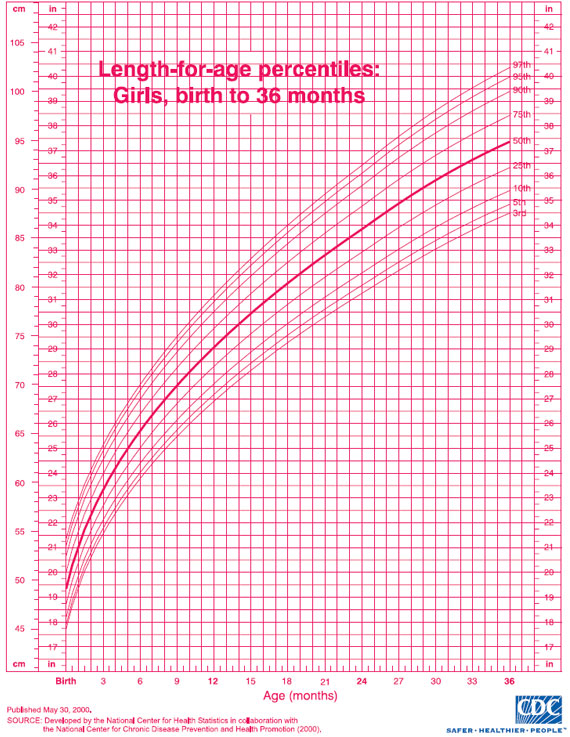 When you start to clarify how the measurements were taken and on what basis the diagnosis was made, in most cases the diagnosis is “sucked out of thin air”. When it came to a large child, often a woman was forced to “go on a diet” and even starve.
When you start to clarify how the measurements were taken and on what basis the diagnosis was made, in most cases the diagnosis is “sucked out of thin air”. When it came to a large child, often a woman was forced to “go on a diet” and even starve.
Before we share information about fetal growth retardation syndrome or intrauterine growth retardation with you, let's discuss a few questions about defining this fetal condition.
Is it correct to speak about height or development, or about weight?
What is meant by intrauterine growth retardation?
Surprisingly, the growth charts are actually fetal weight charts. Why, then, by the weight of the fetus determine its deviations in growth? Disputes on this issue between clinicians are still going on. In some sources you will find mention of developmental delay. However, we are talking, rather, about growth retardation, since it is determined by measuring the parameters of the fetus - the size of its body parts.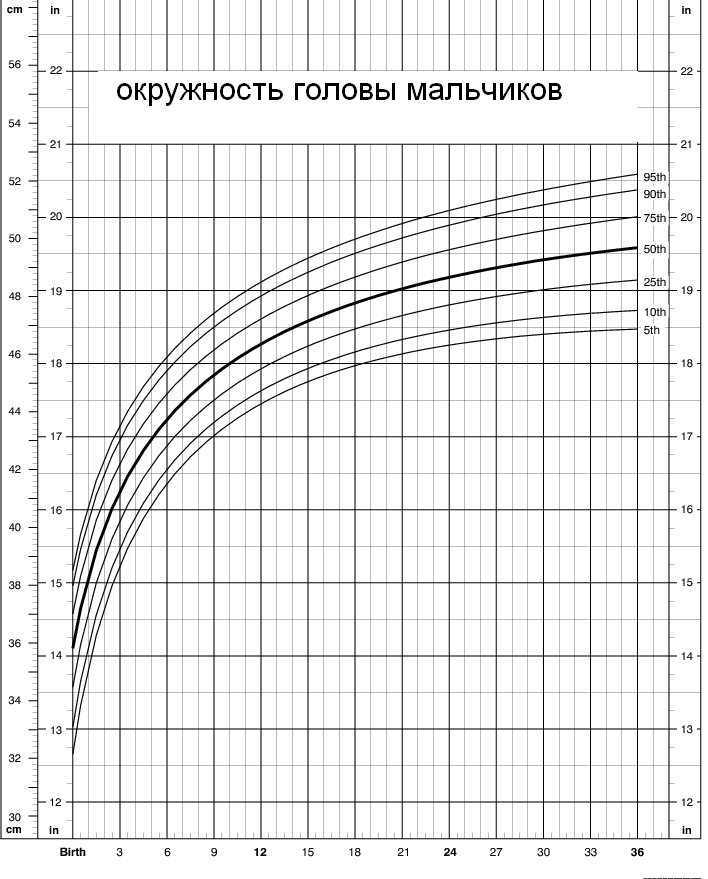 Usually, there are no developmental abnormalities, that is, in the shape and structure of organs and organ systems - a normal small fetus, except in cases where growth retardation is caused by a number of fetal diseases. From a medical point of view, the size of the fetus itself does not say much, therefore, the weight of the fetus is calculated, although conditionally, however, by comparing the weight of the child after a certain period of time, it is possible to more accurately determine whether he is lagging behind in growth or not.
Usually, there are no developmental abnormalities, that is, in the shape and structure of organs and organ systems - a normal small fetus, except in cases where growth retardation is caused by a number of fetal diseases. From a medical point of view, the size of the fetus itself does not say much, therefore, the weight of the fetus is calculated, although conditionally, however, by comparing the weight of the child after a certain period of time, it is possible to more accurately determine whether he is lagging behind in growth or not.
It is also important to understand that we can judge the growth of something or someone only in a certain period of time, and also taking into account a number of facts. For example, you meet a friend on the street with her child. If you do not know how old the child is, then you will approximately determine the age of the child by his height, constitution, and only then by other parameters. What if the child is just small? But what if the child was "fed" and he is big?
It is impossible to feed the fetus, therefore, in obese women, on the contrary, the fetuses are more often small in size (with the exception of women with gestational diabetes).
But poor nutrition of the mother can affect the growth of the fetus - he will not have enough nutrients.
Thus, it was determined: in order to judge the development and growth, it is necessary to observe the growth of the fetus in dynamics, that is, at certain intervals . Why are these intervals important and how long should they last? Once, a woman sent me ultrasound data at 12 weeks and at 32 weeks, and asked me to comment if I see any delay in the growth of her child. First, it is impossible to compare first trimester ultrasound data with third trimester ultrasound data. The conclusion with such a comparison will always be the same: pregnancy is progressing, therefore, why be nervous and worried?
For comparison, periods of 2-4 weeks are necessary, and the size of the fetus is monitored in such cases not earlier than the 20th week.![]() If no serious deviations are found, then the woman is offered to come for a second ultrasound in 4 weeks. If any abnormalities are found in the child's organs, in addition to growth retardation, then the woman is offered to undergo an ultrasound in 1-2 weeks.
If no serious deviations are found, then the woman is offered to come for a second ultrasound in 4 weeks. If any abnormalities are found in the child's organs, in addition to growth retardation, then the woman is offered to undergo an ultrasound in 1-2 weeks.
According to the medical definition , intrauterine growth retardation is understood as the state of the fetus when its weight is 10 percentile (centile) or more behind the average for a particular gestational age.
An explanation of what percentiles are is needed here. If, for example, an ultrasound examination of one hundred pregnant women at 28 weeks of gestation is carried out, then the measurements of their fetuses will be different. It turns out that for someone the dimensions will be minimal, for someone the maximum for this period of pregnancy. Now imagine that, based on these data, a graph was built where a relationship was drawn between the number of women with the same fetal parameters and the value of these parameters.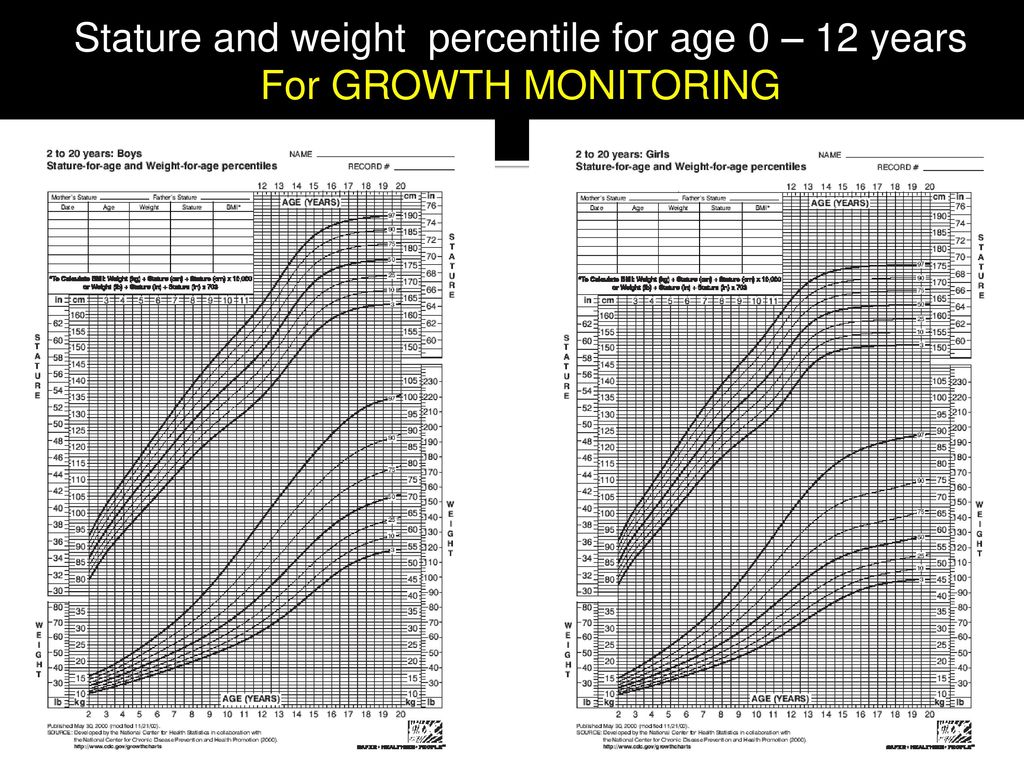 And it turned out that in more women, the dimensions of the fetus (for example, head circumference) are such and such - this will be the median, and for all other women, the dimensions can deviate to the right and left (be larger, smaller), which is not always a pathology. Thus, for a better understanding of the graph, it was divided into 100 parts - centiles (percentiles). Percentiles are erroneously called percentages, although this is not an entirely accurate definition. The indicator that occurs in the largest number of fetuses was taken as the norm, and 10 centiles to the left and 10 centiles to the right (and all the indicators that entered on this chart between two centiles) will also be considered the norm.
And it turned out that in more women, the dimensions of the fetus (for example, head circumference) are such and such - this will be the median, and for all other women, the dimensions can deviate to the right and left (be larger, smaller), which is not always a pathology. Thus, for a better understanding of the graph, it was divided into 100 parts - centiles (percentiles). Percentiles are erroneously called percentages, although this is not an entirely accurate definition. The indicator that occurs in the largest number of fetuses was taken as the norm, and 10 centiles to the left and 10 centiles to the right (and all the indicators that entered on this chart between two centiles) will also be considered the norm.
Based on these data, graphs of changes in the size of the fetus with the gestational age are built. Thus, a graph of the same head size, for example, has three lines: a middle line, one above, and one below (10 centiles up and down). By measuring the size of the fetus, the doctor looks at the graph and determines what this size should be at such and such a gestational age. If the size does not go beyond the two percentile curves, then there are no deviations from the norm. What if it comes out? This does not always mean that there are deviations. This is where the analysis of measurements over time is important.
If the size does not go beyond the two percentile curves, then there are no deviations from the norm. What if it comes out? This does not always mean that there are deviations. This is where the analysis of measurements over time is important.
Again, the inquisitive reader will ask, what does the child's weight and growth retardation have to do with it? Where is the connection between the size of the fetus, its height and weight hidden here? Unfortunately, the modern approach to diagnosing intrauterine growth retardation syndrome suffers due to the fact that weight is still taken as the main criterion for assessing fetal development. However, more and more doctors take into account the size of the fetus, their changes in dynamics, and not just the calculated weight of the child.
Why is performance important?
Firstly , when you analyze many cases, it turns out that neither the woman nor the doctor really knows the exact gestational age. Some doctors still use the old formulas for calculating the gestational age, and if a woman visits several doctors, then each sets the terms in their own way. Let me remind you that with the natural conception of pregnancy with a normal regular menstrual cycle, the gestational age is determined by the first day of the last menstruation. Ultrasound at 12 weeks of gestation is the most accurate method in determining the duration of pregnancy. Therefore, it is always necessary to proceed either from the last menstruation, or ultrasound at 12 weeks. So it turns out that when you specify the gestational age, then often all the indicators given are normal, and not ahead or behind compared to the norm.
Some doctors still use the old formulas for calculating the gestational age, and if a woman visits several doctors, then each sets the terms in their own way. Let me remind you that with the natural conception of pregnancy with a normal regular menstrual cycle, the gestational age is determined by the first day of the last menstruation. Ultrasound at 12 weeks of gestation is the most accurate method in determining the duration of pregnancy. Therefore, it is always necessary to proceed either from the last menstruation, or ultrasound at 12 weeks. So it turns out that when you specify the gestational age, then often all the indicators given are normal, and not ahead or behind compared to the norm.
Second , any measurement may be an error. This must be taken into account when almost all indicators are normal, with the exception of one or two. After all, when taking measurements, it is important the position of the fetus, which is not always obtained “on order”, the skills of the doctor, his knowledge of such a branch of medicine that studies fetal diseases, the correct settings of the ultrasound machine are important.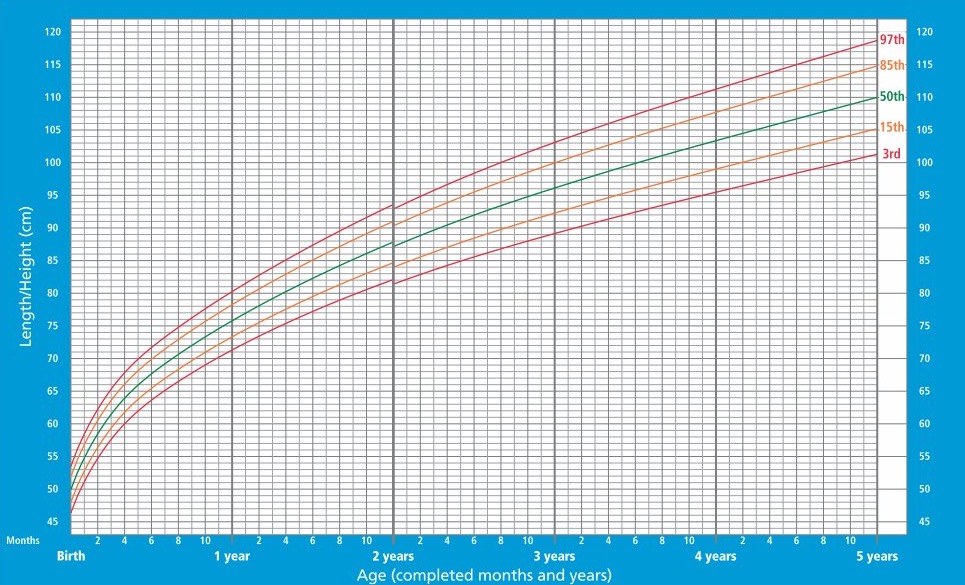
Thirdly , which is more important in terms of pregnancy prognosis: a sharp drop in the child's weight from normal to abnormal in a short period of time or constantly low weight that does not change sharply along the level of the graph (does not go beyond the initial percentile) during a long period of pregnancy? Rapidly maturing changes should always be of concern to doctors, since it is very difficult to predict a favorable prognosis in such cases, and usually this is a poor indicator. In such cases, it is often necessary to apply urgent measures of treatment or delivery.
The baby's weight is calculated based on measurements of the circumference of the abdomen, the diameter of the head, the length of the femur and many other parameters. This is usually done by a computer program entered into the ultrasound machine automatically during the measurement. Modern ultrasound machines have programs with graphs where you can enter measurement data from a woman and then follow the size of the fetus over a certain period.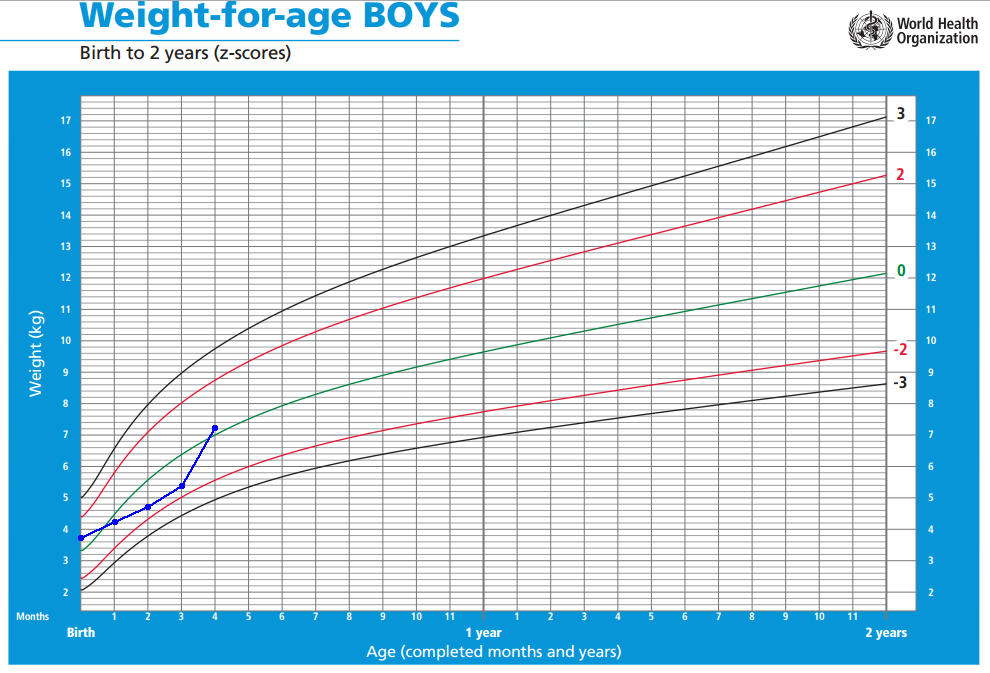 Ultrasound images (images) are stored in the machine's computer, and can also be transferred to other computer databases, where they can be viewed by other doctors. Almost any measurement, if necessary, can be rechecked without additional ultrasound. It all depends on the doctor's skills to understand what he sees on the ultrasound image.
Ultrasound images (images) are stored in the machine's computer, and can also be transferred to other computer databases, where they can be viewed by other doctors. Almost any measurement, if necessary, can be rechecked without additional ultrasound. It all depends on the doctor's skills to understand what he sees on the ultrasound image.
Women often ask to check certain ultrasound measurements because they are not sure that the measurements are correct, especially when doctors make different diagnoses and offer different treatments. No need to quibble over one indicator! It is important to look at indicators in combination with others. Since the baby's weight is calculated by computer programs (one device can have 7 weight calculation equations), even with some measurement data, the doctor cannot accurately determine the weight of the fetus. There are websites where a pregnant woman is asked to enter a series of ultrasound examination data and calculate the weight of the fetus. This weight is called estimated, not exact. The longer the pregnancy, the greater the calculation error. Therefore, the weight is recorded with allowable deviations: plus, minus so many grams to the average weight.
This weight is called estimated, not exact. The longer the pregnancy, the greater the calculation error. Therefore, the weight is recorded with allowable deviations: plus, minus so many grams to the average weight.
Abbreviated ultrasound measurements of parameters that are often used to determine gestational age and baby weight are as follows:
- Biparietal Head Size (BPD)
- LZR (OFD) - fronto-occipital size
- OG (HC) - head circumference
- DLB (FL) - thigh length
- coolant (AC) - abdominal circumference
- SVD (GS) - the average inner diameter of the ovum
- KTP (KTP, CRL) - coccyx-parietal size of the embryo / fetus
There are also a number of other options. Of course, for many of you, these parameters and their abbreviations mean nothing and are not at all clear. But very often, when you get your hands on the result of an ultrasound examination, you ask questions about what they mean for the future of pregnancy, you try to find answers to questions by researching books and the Internet in order to compare your indicators with the norm. Modern pregnant women, constantly going through tests, often artificially created by their environment, including medical workers, do not leave unnoticed even such specific indicators as ultrasound data and test results.
Modern pregnant women, constantly going through tests, often artificially created by their environment, including medical workers, do not leave unnoticed even such specific indicators as ultrasound data and test results.
To help you find out if your baby's measurements are normal, I've included a table that many obstetricians use. Please note that your fetus may be smaller or larger, especially if the gestational age is not calculated correctly. But you don't need to get upset. As I mentioned earlier, the growth of the fetus must be monitored in dynamics, that is, over a period of time.
| Weeks | BPR (cm) | LZR(cm) | exhaust (cm) | coolant (cm) | dB (cm) | CTE (cm) | Weight (g) |
| 12 | 2.0 | - | - | 5.3 | - | 4.7 | |
| 13 | 2.4 | - | - | 6.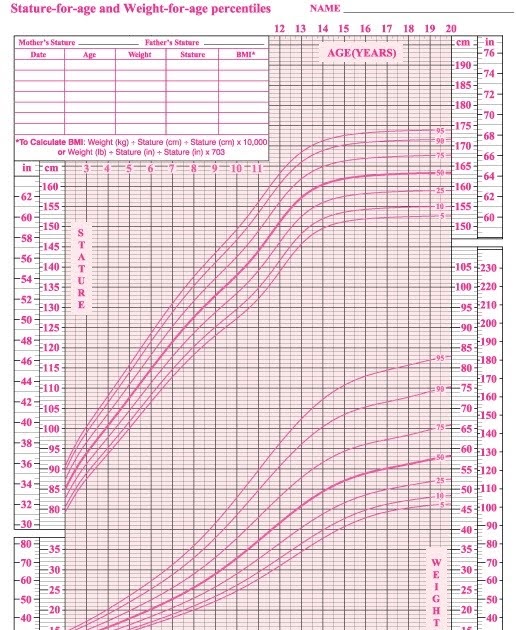 3 3 | 1.0 | 6.0 | 14 |
| 14 | 2.8 | 3.1 | 10.6 | 7.5 | 1.2 | 7.3 | 25 |
| 15 | 3.2 | 3.8 | 11.5 | 8.5 | 1.6 | 8.6 | 50 |
| 16 | 3.5 | 4.1 | 12.7 | 9.7 | 1.8 | 9.7 | 80 |
| 17 | 3.8 | 4.6 | 14.0 | 10.7 | 2.2 | 11.0 | 100 |
| 18 | 4.2 | 5.0 | 15.2 | 11.6 | 2.5 | 12.0 | 150 |
| 19 | 4.6 | 5.4 | 16.4 | 12.6 | 2.5 | 13.0 | 200 |
| 20 | 4.9 | 5.8 | 17.6 | 13.5 | 3.1 | 14.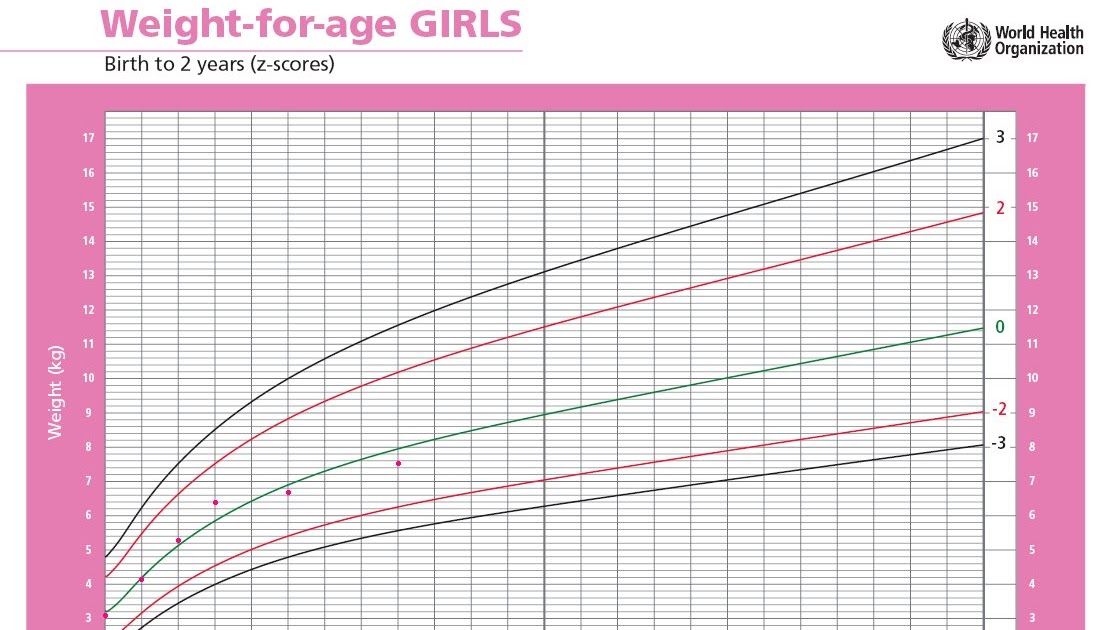 0 0 | 250 |
| 21 | 5.2 | 6.3 | 19.0 | 14.5 | 3.4 | Body length | 300 |
| 22 | 5.6 | 6.7 | 20.3 | 15.5 | 3.6 | 27.8 | 350 |
| 23 | 5.9 | 7.2 | 21.5 | 16.5 | 3.9 | 28.9 | 450 |
| 24 | 6.2 | 7.6 | 22.6 | 17.3 | 4.1 | 30.0 | 530 |
| 25 | 6.5 | 8.0 | 24.0 | 18.3 | 4.4 | 33.0 | 700 |
| 26 | 6.8 | 8.4 | 25.1 | 19.1 | 4.7 | 35.6 | 850 |
| 27 | 7.1 | 8.8 | 26.3 | 20.2 | 4.9 | 36.6 | 1000 |
| 28 | 7.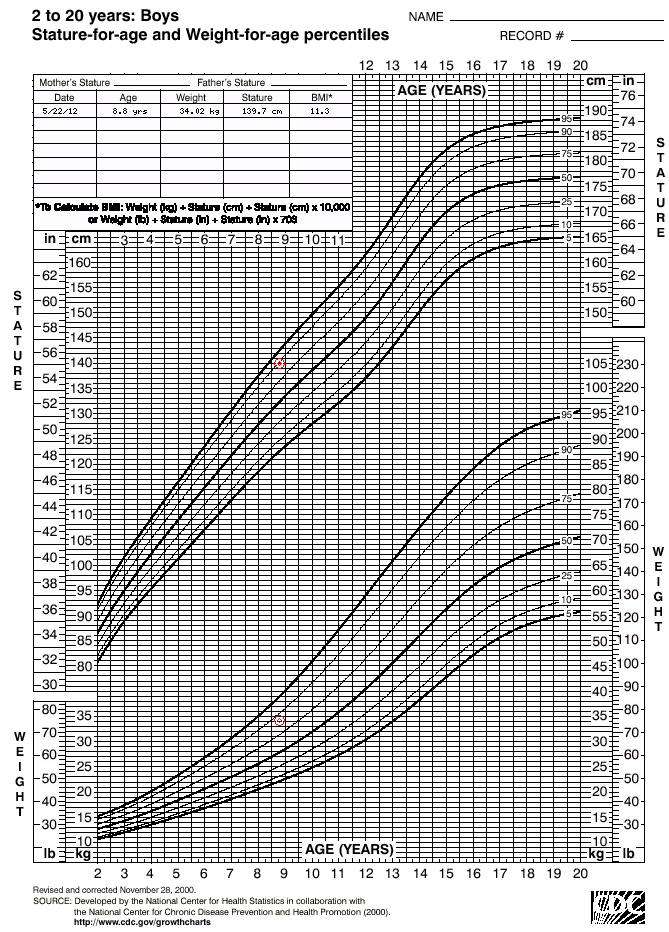 4 4 | 9.1 | 27.4 | 21.1 | 5.1 | 37.6 | 1100 |
| 29 | 7.7 | 9.5 | 28.4 | 22.2 | 5.4 | 38.6 | 1250 |
| 30 | 8.0 | 9.8 | 29.3 | 23.0 | 5.6 | 39.9 | 1400 |
| 31 | 8.2 | 10.0 | 30.3 | 24.0 | 5.9 | 41.1 | 1600 |
| 32 | 8.5 | 10.3 | 31.1 | 24.9 | 6.1 | 42.4 | 1800 |
| 33 | 8.7 | 10.5 | 31.8 | 25.8 | 6.3 | 43.7 | 2000 |
| 34 | 8.9 | 10.7 | 32.5 | 26.8 | 6.5 | 45.0 | 2250 |
| 35 | 9.1 | 10. 9 9 | 33.2 | 27.7 | 6.7 | 46.0 | 2550 |
| 36 | 9.3 | 11.1 | 33.7 | 28.7 | 6.9 | 47.4 | 2750 |
| 37 | 9.5 | 11.2 | 34.0 | 29.6 | 7.1 | 48.6 | 2950 |
| 38 | 9.6 | 11.3 | 34.4 | 30.6 | 7.3 | 49.8 | 3100 |
| 39 | 9.8 | 11.4 | 34.7 | 31.5 | 7.4 | 50.7 | 3250 |
| 40 | 9.9 | 11.5 | 34.9 | 32.0 | 7.5 | 51.2 | 3400 |
Who is to blame and what to do?
Thus, if, according to several independent ultrasounds, the weight of the child was below the 10th percentile for a certain gestational age, then they speak of intrauterine growth retardation syndrome. Logically, the question arises: is it bad or is it normal for a particular fetus? If the gestational age is specified, and the fetus is indeed stunted, it is necessary to find out the reason: why?
Logically, the question arises: is it bad or is it normal for a particular fetus? If the gestational age is specified, and the fetus is indeed stunted, it is necessary to find out the reason: why?
There is an erroneous opinion that small mothers have small children, and big mothers have big children (large fruits). This is not entirely true. Weight is not inherited and does not depend on the constitution of the mother. However, small mothers of small stature have lower birth rates for large children, and, conversely, smaller children are born more often to such mothers, but very rarely their weight exceeds the 10th percentile.
All causes of fetal growth retardation can be divided into three groups :
- maternal (malnutrition, smoking, drug and alcohol abuse, cardiovascular disease, uncontrolled diabetes mellitus, lung failure and other diseases),
- maternal-fetal (any diseases that can lead to placental insufficiency - hypertension, kidney disease, placental abruption, placental development disorder, etc.
 )
) - fetal (viral diseases of the fetus, multiple pregnancy, congenital malformations).
Establishing the cause is very important, because the treatment will depend on it, although most often there is no treatment as such when the causes are found in the fetus and placenta. But maternal diseases, bad habits and lifestyle can be changed.
If there is some factor that adversely affects the growth and development of the fetus, the processes of survival and self-preservation in the child are enhanced, the child resists this factor and tries to survive and live to the term of birth - the redistribution of blood volume begins: it enters the vital important organs - the heart and brain, and the blood supply to other organs is reduced (liver, kidneys, intestines), and unnecessary fetal movements and energy expenditure are also eliminated. By understanding the process of adaptation of the fetus to a harmful factor (or factors), it is possible to determine its physical condition (biophysical profile) even before the appearance of pronounced deviations in growth and development.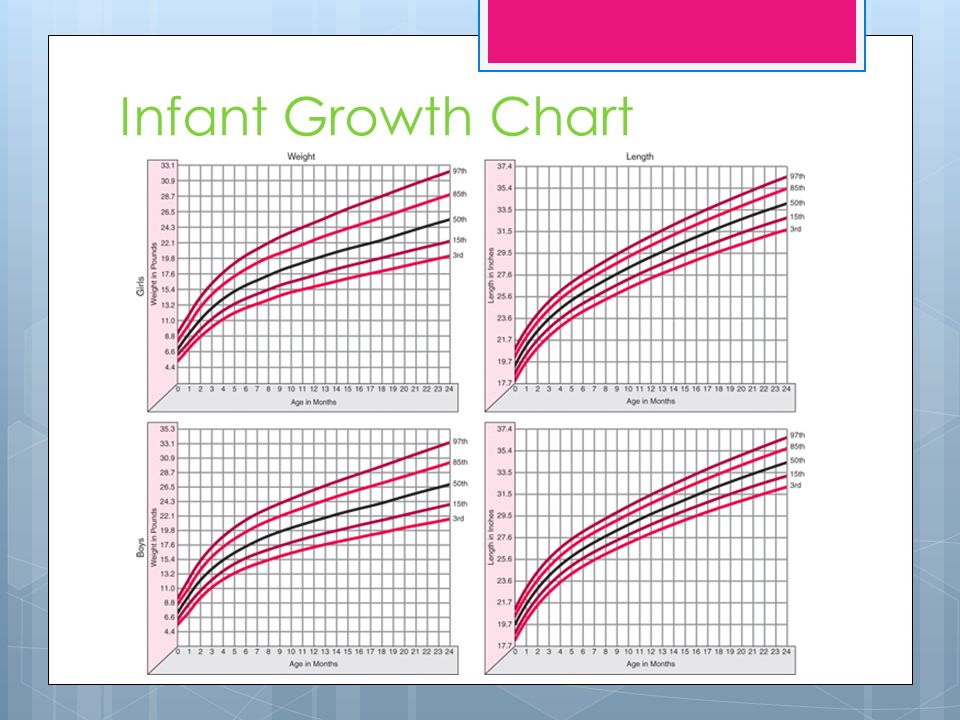
There are two types of fetal growth retardation syndrome - symmetrical and asymmetric.
Symmetrical delay , which occurs in 20% of cases, is called growth retardation of the first type. At the same time, the dimensions of the head and torso lag behind normal indicators in the same way, and such growth retardation has been observed since the second trimester of pregnancy. Often it is associated with viral infections and fetal malformations.
In most cases (80%) there are asymmetric fetal growth retardation - the second type, when the brain (head) develops normally, and the trunk (abdominal circumference) lags behind in growth, while the head/abdomen ratio will be increased. This type of delay is observed in the presence of maternal and placental causes, and occurs in late pregnancy. However, the prediction for this type of delay is much better than the first type.
Previously, doctors used to measure the growth of the uterus (height of the fundus of the uterus), according to which the diagnosis of fetal growth retardation was made: if the height of the fundus of the uterus lagged behind the indicators for a given gestational age, it means that not everything is in order with the fetus - this is usually how the diagnosis was made intrauterine growth retardation.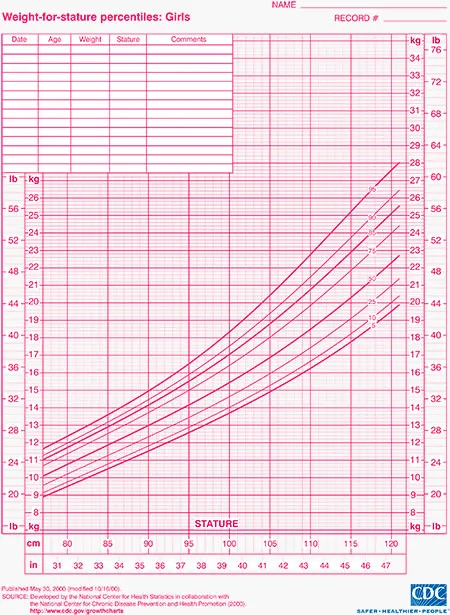 Often, the calculation of the child's weight by measuring the external parameters of the mother had large errors (an error of 400-500 g), and not all doctors were able to make such measurements correctly. With the advent of ultrasound, it is possible to measure the size of the child itself, regardless of the external parameters of the woman, as well as assess the condition of the placenta, the amount of amniotic fluid, which is also important in making a diagnosis. After all, it is not so important to state the fact of fetal growth retardation, but to find out the cause that caused it, because further tactics and treatment of a pregnant woman or fetus will depend on this.
Often, the calculation of the child's weight by measuring the external parameters of the mother had large errors (an error of 400-500 g), and not all doctors were able to make such measurements correctly. With the advent of ultrasound, it is possible to measure the size of the child itself, regardless of the external parameters of the woman, as well as assess the condition of the placenta, the amount of amniotic fluid, which is also important in making a diagnosis. After all, it is not so important to state the fact of fetal growth retardation, but to find out the cause that caused it, because further tactics and treatment of a pregnant woman or fetus will depend on this.
So, if fetal growth restriction is suspected, what should be done?
First , do not panic, do not be nervous and suffer, but clarify the gestational age first.
Secondly , it is necessary to repeat the ultrasound in 2-4 weeks.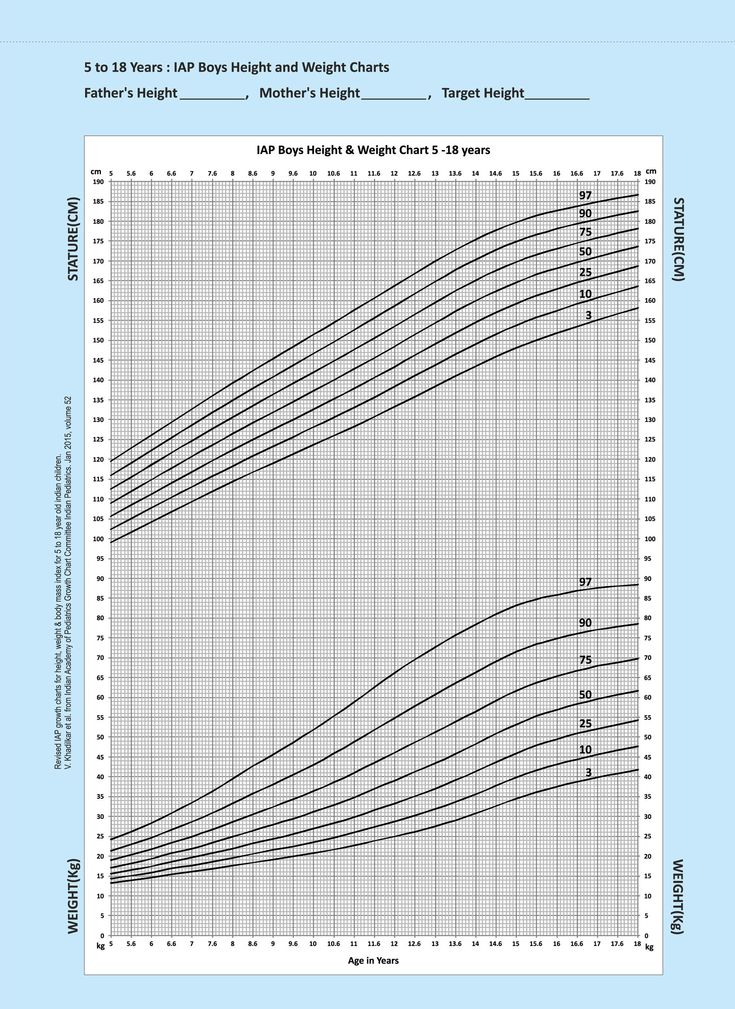
Thirdly, approach the question analytically: are there reasons for fetal growth retardation? If such causes exist, the next question is: how can they be eliminated or reduced? From here begins the choice of treatment, if such a choice exists. It is also important to determine the "well-being" of the child - how does he react to growth retardation, in addition to lagging behind in weight and other parameters? Here, Doppler ultrasound, CTG, and the determination of the biophysical profile of the fetus come to the rescue.
The further tactics of doctors will depend on the degree of fetal growth retardation, and in some cases, an emergency delivery is performed in the interests of the child (most often by caesarean section, because a premature and underdeveloped child may not be able to cope with the process of self-survival during natural childbirth, which are often sluggish and long, since neither the uterus nor the cervix are ready for childbirth).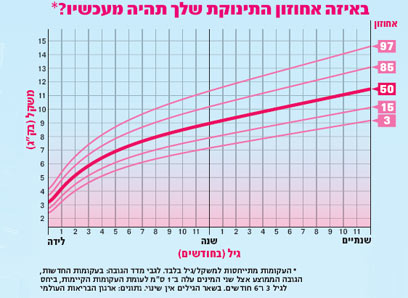
In some cases, a woman may be advised to stay in bed, but this does not mean that the woman must be in the hospital all the time. Usually, women who have a significant fetal growth retardation syndrome are sent to the hospital for examination.
Unfortunately, there are no universal medications that could help in the treatment of fetal growth retardation syndrome, since there are many causes of this problem, and therefore treatment is always individual .
All the traditional arsenal that doctors of the Soviet and post-Soviet schools still use (chimes, hofitol and many other drugs) are completely ineffective, but are just a tribute to the old tradition, a manifestation of dogmatism. The less you load a pregnant woman with drugs, the safer it is for her and her baby.
In cases where there are factors of malnutrition and bad habits, fetal growth retardation is easier to prevent than to cure later. Therefore, the prevention of fetal growth retardation begins with proper preparation for pregnancy.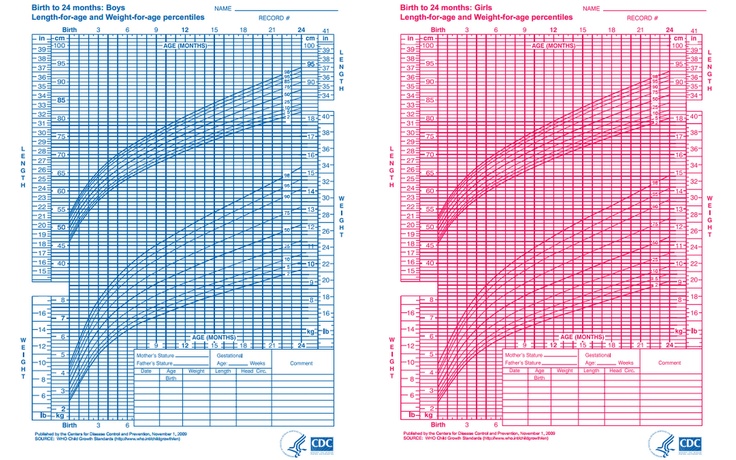
What can happen if fetal growth retardation is not taken into account? Such children, although they can be full-term, are often weaker, so they may suffer asphyxia (suffocation) during childbirth, have more health problems after birth, and the mortality of such children is higher, as is stillbirth. Mental retardation is also observed in this group of children more often.
A few words about macrosomia
The opposite of growth retardation syndrome is fetal growth advance, or large fetal size when the weight is beyond the 90th percentile. This condition is called macrosomia. It is a mistake to think that the larger the fetus, the healthier it is (and a fetus weighing more than 4000 grams at birth is also considered large).
Causes of macrosomia other than fetal growth retardation. In women suffering from 1-2 degrees of obesity, the size of the fetus can be large, but in women with a high degree of obesity, on the contrary, fetal growth retardation is often observed.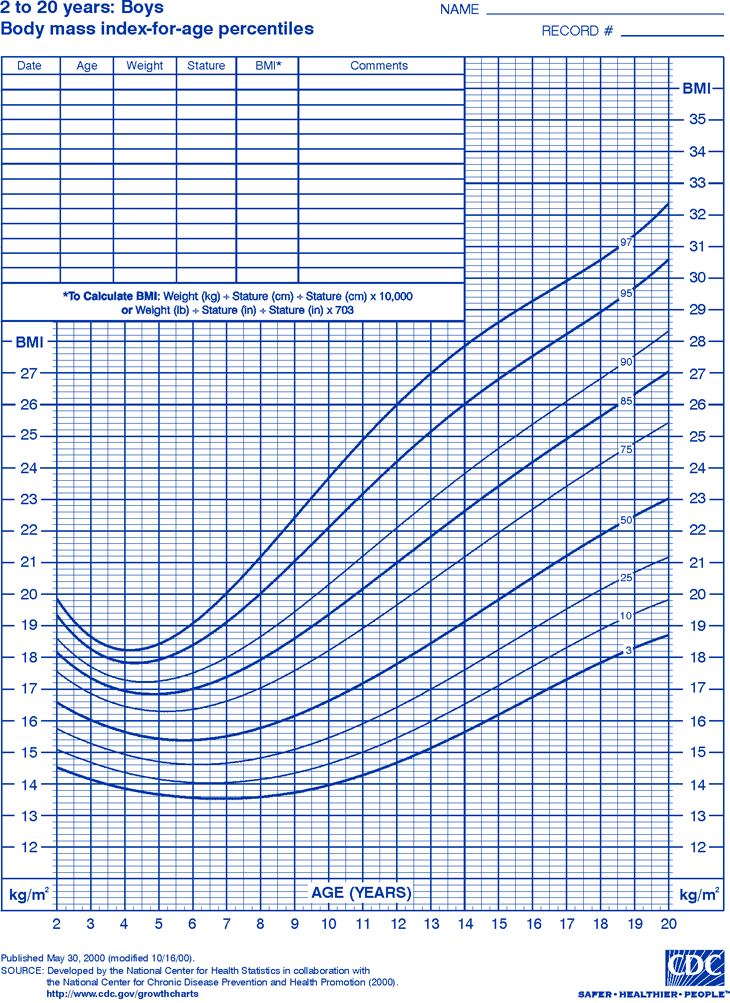 Obese women often suffer from diabetes mellitus (type 2), so macrosomia is also observed in such pregnant women. There is also a relationship between previous pregnancies: if a woman had pregnancies with a large fetus, then the next pregnancy can also be a large fetus. Also, the more pregnancies, the, usually, the weight of the child is greater.
Obese women often suffer from diabetes mellitus (type 2), so macrosomia is also observed in such pregnant women. There is also a relationship between previous pregnancies: if a woman had pregnancies with a large fetus, then the next pregnancy can also be a large fetus. Also, the more pregnancies, the, usually, the weight of the child is greater.
Macrosomia is diagnosed by ultrasound with the construction of graphs of the growth of the child and changes in his weight during pregnancy. Treatment exists only in cases of gestational diabetes, when a woman strictly monitors her blood sugar levels.
A large weight during pregnancy is not dangerous for the fetus itself, but serious problems can arise during childbirth, which can lead to fetal death and stillbirth, or lead to fractures of the newborn's collarbone, ruptures of the woman's birth canal and other complications. Therefore, it is always important to choose the right method of delivery in such women and to monitor the condition of the fetus very carefully during childbirth.