Induction labor steps
Inducing Labor (for Parents) - Nemours KidsHealth
It's common for many pregnant women, especially first-time mothers, to watch their baby's due date come and go without so much as a contraction. The farther away from the expected delivery date (called the EDD) you get, the more anxious you might become. You may start to wonder — is this baby ever going to come?
Late pregnancy can be challenging — you may feel large all over, your feet and back might hurt, you might not have the energy to do much of anything, and you're beyond ready to meet the little one you've nurtured all this time. Which is why waiting a little longer than you'd expected can be particularly hard.
Still, being past your due date doesn't guarantee that your doctor (or other health care provider) will do anything to induce (or artificially start) labor — at least not right away.
What Is It?
Labor induction is what doctors use to try to help labor along using medications or other medical techniques. Years ago, some doctors routinely induced labor. But now it's not usually done unless there's a true medical need for it. Labor is usually allowed to take its natural course. However, in some situations, a health care provider may recommend induction.
Why It's Done
Your doctor might suggest an induction if:
- your water broke but you are not having contractions
- your baby still hasn't arrived by 2 weeks after the due date (when you're considered post-term — more than 42 weeks into your pregnancy)
- you have an infection in the uterus (called chorioamnionitis)
- you have certain risk factors (e.g., gestational diabetes or high blood pressure)
- there is not enough amniotic fluid
- there is a problem with the placenta
- the baby is not growing appropriately
Induction also can be appropriate under certain circumstances, as with a mother who is full term and has a history of rapid deliveries or lives far from a hospital.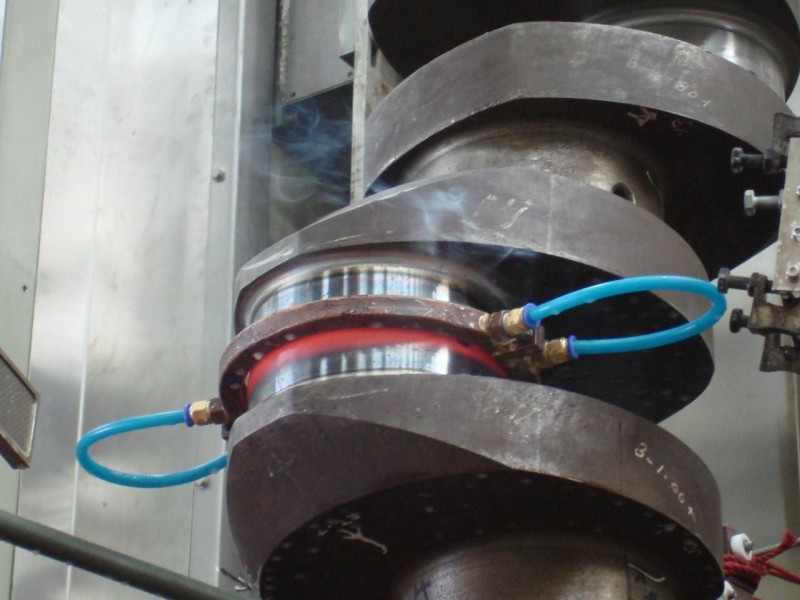
Some mothers request elective inductions for convenience, but these do come with risks. Doctors try to avoid inducing labor early because the due date may be wrong and/or the woman's cervix might not be ready yet.
Page 2
How It's Done
Some methods of induction are less invasive and carry fewer risks than others. Ways that doctors may try to induce labor by getting contractions started include:
- Stripping the membranes. The doctor puts on a glove and inserts a finger into the vagina and through the cervix (the opening that connects the vagina to the uterus). He or she moves the finger back and forth to separate the thin membrane connecting the amniotic sac (which houses the baby and amniotic fluid) to the wall of the uterus. When the membranes are stripped, the body releases hormones called prostaglandins, which help prepare the cervix for delivery and may bring on contractions. This method works for some women, but not all.
- Breaking your water (also called an amniotomy).
 The doctor ruptures the amniotic sac during a vaginal exam using a little plastic hook to break the membranes. If the cervix is ready for labor, amniotomy usually brings on labor in a matter of hours.
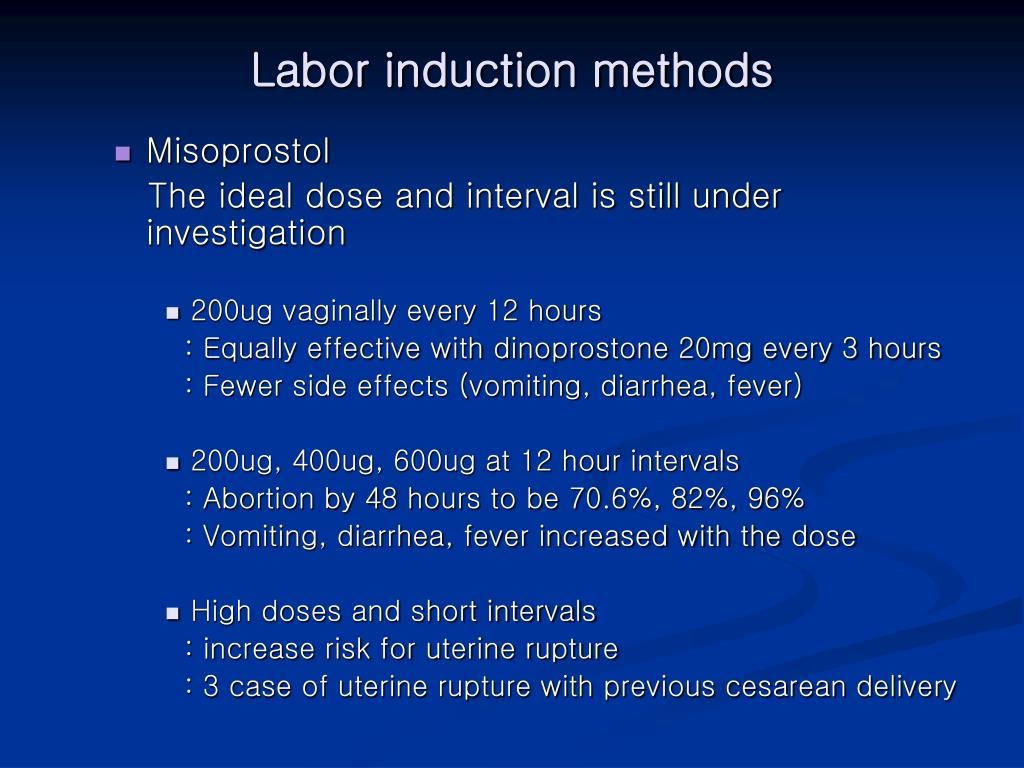
The doctor ruptures the amniotic sac during a vaginal exam using a little plastic hook to break the membranes. If the cervix is ready for labor, amniotomy usually brings on labor in a matter of hours. - Giving the hormone prostaglandin to help ripen the cervix. A gel or vaginal insert of prostaglandin is inserted into the vagina or a tablet is given by mouth. This is typically done overnight in the hospital to make the cervix "ripe" (soft, thinned out) for delivery. Administered alone, prostaglandin may induce labor or may be used before giving oxytocin.
- Giving the hormone oxytocin to stimulate contractions. Given continuously through an IV, the drug (Pitocin) is started in a small dose and then increased until labor is progressing well. After it's administered, the fetus and uterus need to be closely monitored. Oxytocin is also frequently used to spur labor that's going slowly or has stalled.
What Will It Feel Like?
Stripping the membranes can be a little painful or uncomfortable, although it usually only takes a minute or so. You may also have some intense cramps and spotting for the next day or two.
You may also have some intense cramps and spotting for the next day or two.
It can also be a little uncomfortable to have your water broken. You may feel a tug followed by a warm trickle or gush of fluid.
With prostaglandin, you might have some strong cramping as well. With oxytocin, contractions are usually more frequent and regular than in a labor that starts naturally.
Page 3
Risks and Precautions
Inducing labor is not like turning on a faucet. If the body isn't ready, an induction might fail and, after hours or days of trying, a woman may end up having a cesarean delivery (C-section). This appears to be more likely if the cervix is not yet ripe.
If the doctor ruptures the amniotic sac and labor doesn't begin, another method of inducing labor also might be necessary because there's a risk of infection to both mother and baby if the membranes are ruptured for a long time before the baby is born.
When prostaglandin or oxytocin is used, there is a risk of abnormal contractions developing. In that case, the doctor may remove the vaginal insert or turn the oxytocin dose down. While it is rare, there is an increase in the risk of developing a tear in the uterus (uterine rupture) when these medications are used. Other complications associated with oxytocin use are low blood pressure and low blood sodium (which can cause problems such as seizures).
In that case, the doctor may remove the vaginal insert or turn the oxytocin dose down. While it is rare, there is an increase in the risk of developing a tear in the uterus (uterine rupture) when these medications are used. Other complications associated with oxytocin use are low blood pressure and low blood sodium (which can cause problems such as seizures).
Another potential risk of inducing labor is giving birth to a late pre-term baby (born after 34 and before 37 weeks). Why? Because the due date (EDD) may be wrong. Your due date is 40 weeks from the first day of your last menstrual period (LMP).
Babies born late pre-term are generally healthy but may have temporary problems such as jaundice, trouble feeding, problems with breathing, or difficulty maintaining body temperature. They may also be more likely than full term babies to have developmental or school problems later on.
Even though inductions do come with risks, going beyond 42 weeks of pregnancy can be risky, too. Many babies are born "post-term" without any complications, but concerns include:
Many babies are born "post-term" without any complications, but concerns include:
- A vaginal delivery may become harder as the baby gets bigger. As babies get bigger, the chance of an injury during delivery, such as a broken bone, increases.
- The placenta that helps to provide the baby with nourishment is deteriorating.
- The amniotic fluid can become low or contain meconium — the baby's first feces. If the baby breathes in meconium, it can cause breathing problems.
Old wives' tales abound about ways to induce labor, such as the use of castor oil. It is not safe to try to artificially start labor yourself by taking castor oil, which can lead to nausea, diarrhea, and dehydration. And herbs and herbal supplements meant to induce labor can be harmful. Breast stimulation can cause uterine contractions by causing the release of oxytocin. However, some studies have suggested that the baby might have abnormal heartbeats after breast stimulation. Some women feel that having sex in late pregnancy can induce labor, but there is no conclusion on this yet.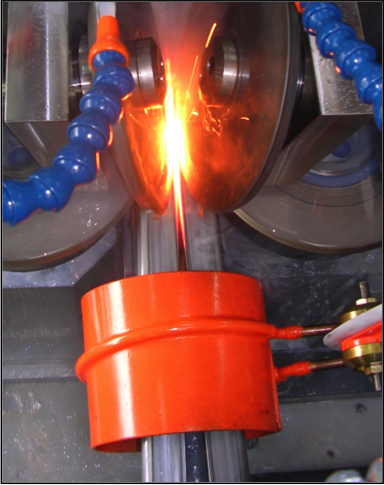
Talk to your doctor before doing anything to try to encourage your little one's arrival. Inducing labor is best left to medical professionals — you may cause more harm than good.
As frustrating as it can be waiting for your baby to finally decide to arrive, letting nature take its course is often best, unless your doctor tells you otherwise. Before you know it, you'll be too busy to remember your baby was ever late at all!
Labor induction - Mayo Clinic
Overview
Labor induction — also known as inducing labor — is prompting the uterus to contract during pregnancy before labor begins on its own for a vaginal birth.
A health care provider might recommend inducing labor for various reasons, primarily when there's concern for the mother's or baby's health. An important factor in predicting whether an induction will succeed is how soft and expanded the cervix is (cervical ripening). The gestational age of the baby as confirmed by early, regular ultrasounds also is important.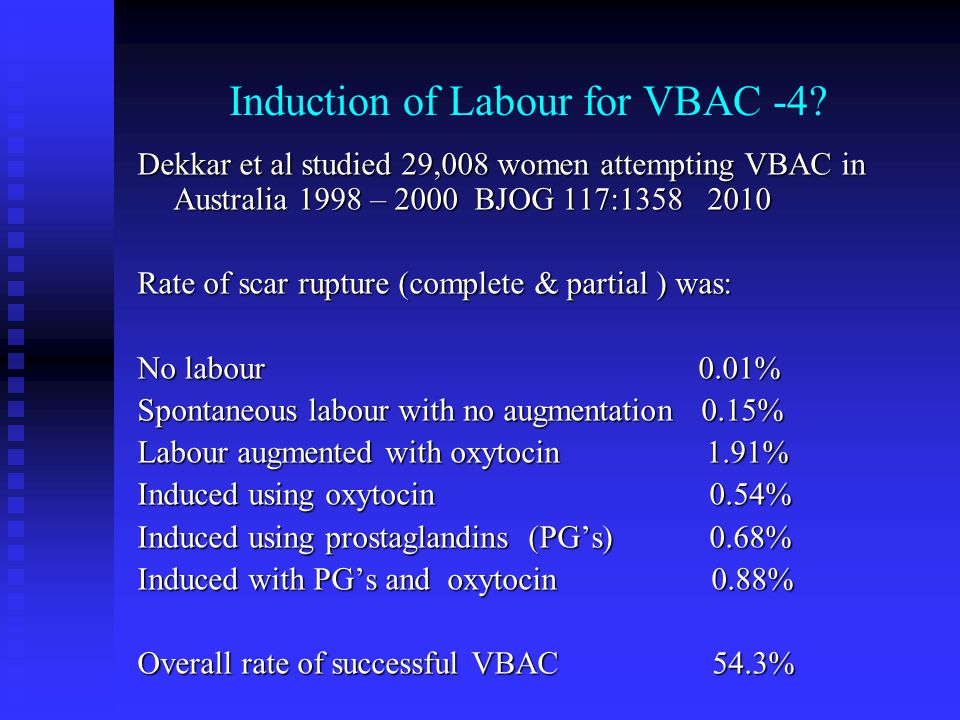
If a health care provider recommends labor induction, it's typically because the benefits outweigh the risks. If you're pregnant, understanding why and how labor induction is done can help you prepare.
Products & Services
- Book: Mayo Clinic Family Health Book, 5th Edition
- Book: Mayo Clinic Guide to a Healthy Pregnancy
- Newsletter: Mayo Clinic Health Letter — Digital Edition
Why it's done
To determine if labor induction is necessary, a health care provider will likely evaluate several factors. These include the mother's health and the status of the cervix. They also include the baby's health, gestational age, weight, size and position in the uterus. Reasons to induce labor include:
- Nearing 1 to 2 weeks beyond the due date without labor starting (postterm pregnancy).
- When labor doesn't begin after the water breaks (prelabor rupture of membranes).
- An infection in the uterus (chorioamnionitis).
- When the baby's estimated weight is less than the 10th percentile for gestational age (fetal growth restriction).
- When there's not enough amniotic fluid surrounding the baby (oligohydramnios).
- Possibly when diabetes develops during pregnancy (gestational diabetes), or diabetes exists before pregnancy.
- Developing high blood pressure in combination with signs of damage to another organ system (preeclampsia) during pregnancy. Or having high blood pressure before pregnancy, developing it before 20 weeks of pregnancy (chronic high blood pressure) or developing the condition after 20 weeks of pregnancy (gestational hypertension).
- When the placenta peels away from the inner wall of the uterus before delivery — either partially or completely (placental abruption).
- Having certain medical conditions. These include heart, lung or kidney disease and obesity.
Elective labor induction is the starting of labor for convenience when there's no medical need. It can be useful for women who live far from the hospital or birthing center or who have a history of fast deliveries.
It can be useful for women who live far from the hospital or birthing center or who have a history of fast deliveries.
A scheduled induction might help avoid delivery without help. In such cases, a health care provider will confirm that the baby's gestational age is at least 39 weeks or older before induction to reduce the risk of health problems for the baby.
As a result of recent studies, women with low-risk pregnancies are being offered labor induction at 39 to 40 weeks. Research shows that inducing labor at this time reduces several risks, including having a stillbirth, having a large baby and developing high blood pressure as the pregnancy goes on. It's important that women and their providers share in decisions to induce labor at 39 to 40 weeks.
Request an Appointment at Mayo Clinic
From Mayo Clinic to your inbox
Sign up for free, and stay up to date on research advancements, health tips and current health topics, like COVID-19, plus expertise on managing health.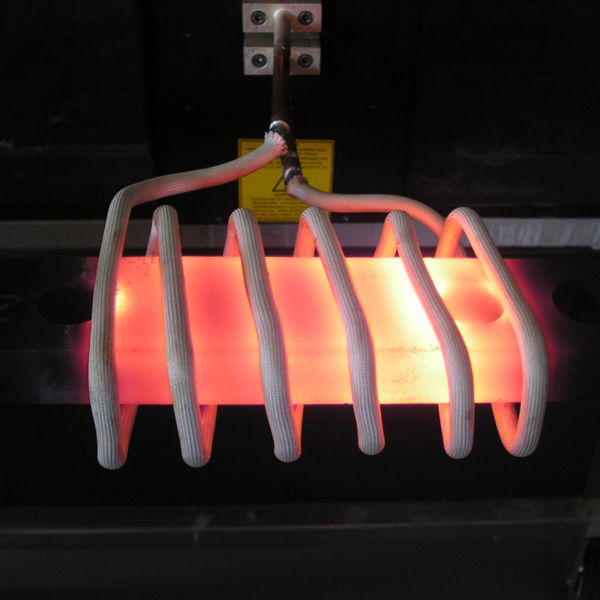
To provide you with the most relevant and helpful information, and understand which information is beneficial, we may combine your email and website usage information with other information we have about you. If you are a Mayo Clinic patient, this could include protected health information. If we combine this information with your protected health information, we will treat all of that information as protected health information and will only use or disclose that information as set forth in our notice of privacy practices. You may opt-out of email communications at any time by clicking on the unsubscribe link in the e-mail.
Risks
Uterine incisions used during C-sections
Uterine incisions used during C-sections
A C-section includes an abdominal incision and a uterine incision. After the abdominal incision, the health care provider will make an incision in the uterus. Low transverse incisions are the most common (top left).
After the abdominal incision, the health care provider will make an incision in the uterus. Low transverse incisions are the most common (top left).
Labor induction carries various risks, including:
- Failed induction. An induction might be considered failed if the methods used don't result in a vaginal delivery after 24 or more hours. In such cases, a C-section might be necessary.
- Low fetal heart rate. The medications used to induce labor — oxytocin or a prostaglandin — might cause the uterus to contract too much, which can lessen the baby's oxygen supply and lower the baby's heart rate.
- Infection. Some methods of labor induction, such as rupturing the membranes, might increase the risk of infection for both mother and baby. The longer the time between membrane rupture and labor, the higher the risk of an infection.
-
Uterine rupture. This is a rare but serious complication in which the uterus tears along the scar line from a prior C-section or major uterine surgery.
 Rarely, uterine rupture can also occur in women who have not had previous uterine surgery.
Rarely, uterine rupture can also occur in women who have not had previous uterine surgery.An emergency C-section is needed to prevent life-threatening complications. The uterus might need to be removed.
- Bleeding after delivery. Labor induction increases the risk that the uterine muscles won't properly contract after giving birth, which can lead to serious bleeding after delivery.
Labor induction isn't for everyone. It might not be an option if:
- You've had a C-section with a classical incision or major uterine surgery
- The placenta is blocking the cervix (placenta previa)
- Your baby is lying buttocks first (breech) or sideways (transverse lie)
- You have an active genital herpes infection
- The umbilical cord slips into the vagina before delivery (umbilical cord prolapse)
If you have had a C-section and have labor induced, your health care provider is likely to avoid certain medications to reduce the risk of uterine rupture.
How you prepare
Labor induction is typically done in a hospital or birthing center. That's because mother and baby can be monitored there, and labor and delivery services are readily available.
What you can expect
During the procedure
There are various ways of inducing labor. Depending on the circumstances, the health care provider might use one of the following ways or a combination of them. The provider might:
-
Ripen the cervix. Sometimes prostaglandins, versions of chemicals the body naturally produces, are placed inside the vagina or taken by mouth to thin or soften (ripen) the cervix. After prostaglandin use, the contractions and the baby's heart rate are monitored.
In other cases, a small tube (catheter) with an inflatable balloon on the end is inserted into the cervix. Filling the balloon with saline and resting it against the inside of the cervix helps ripen the cervix.
- Sweep the membranes of the amniotic sac.
 With this technique, also known as stripping the membranes, the health care provider sweeps a gloved finger over the covering of the amniotic sac near the fetus. This separates the sac from the cervix and the lower uterine wall, which might help start labor.
With this technique, also known as stripping the membranes, the health care provider sweeps a gloved finger over the covering of the amniotic sac near the fetus. This separates the sac from the cervix and the lower uterine wall, which might help start labor. -
Rupture the amniotic sac. With this technique, also known as an amniotomy, the health care provider makes a small opening in the amniotic sac. The hole causes the water to break, which might help labor go forward.
An amniotomy is done only if the cervix is partially dilated and thinned, and the baby's head is deep in the pelvis. The baby's heart rate is monitored before and after the procedure.
- Inject a medication into a vein. In the hospital, a health care provider might inject a version of oxytocin (Pitocin) — a hormone that causes the uterus to contract — into a vein. Oxytocin is more effective at speeding up labor that has already begun than it is as at cervical ripening.
 The provider monitors contractions and the baby's heart rate.
The provider monitors contractions and the baby's heart rate.
How long it takes for labor to start depends on how ripe the cervix is when the induction starts, the induction techniques used and how the body responds to them. It can take minutes to hours.
After the procedure
In most cases, labor induction leads to a vaginal birth. A failed induction, one in which the procedure doesn't lead to a vaginal birth, might require another induction or a C-section.
By Mayo Clinic Staff
Related
Products & Services
what is it? Typhlotechnical aids for the blind
In the broadest sense, typhlotechnical equipment is a combination of various devices, technical devices and methods of their use that allow people with significant visual impairments to obtain the necessary information using other types of sensitivity (auditory, tactile, vibrational). typhlotechnics include all kinds of special tools that help visually impaired and blind people in training, professional activities, orientation in space, in cultural and domestic services.
Order
The main functions of tiflotechnics
The main tasks of tiflotechnics are not only the possibility of removing restrictions caused by total or significant loss of vision, but also expanding the ways of using special technical means, as well as the possibility of participation of such people in labor activities and the creation of additional conditions, raising the level of their cultural development.
Author of many scientific papers related to the teaching of geography to the blind, the work of blind teachers, the employment of the blind - Sverlov V.S. believed that tiflotechnics is any technique that is created specifically for people deprived of vision, and plays an important role for them.
Fundamental differences between tiflotechnique and conventional technical device include:
- the presence of special features and additional information about the surrounding space, which can only be obtained with the help of tiflopribor;
- the presence of constructive data that allows the blind with the help of a tiflopribor to supplement actions that require the presence of a visual function.
Ordinary smartphone , which has been successfully used by both sighted and blind users for a long time, does not belong to the category of thiflotechnics. Because the blind receive through it information that does not have a visual basis. Whereas cane is considered a tiflo technical tool and is used as a special device that performs support and signal functions, as well as the function of orientation when moving.
The specifics of the functional purpose of tiflotechniques
Currently, the following categories of functional purpose of tiflotechniques are distinguished:
- educational tiflotechnique, which helps to enrich the educational program and methods of teaching the visually impaired and the blind in schools, secondary vocational education institutions and higher educational institutions;
- industrial tiflotechnics, which increase labor productivity and allow the visually impaired and blind to master new professions and types of skilled labor;
- tiflotechnics for cultural and community purposes, expanding cognitive activity in everyday conditions and forming the basis for increasing the level of cultural and physical development of the visually impaired and the blind.

Types of typhlotechnics
In order to independently navigate in space, a person with partial or complete loss of vision must use various typhlotechnical means.
Conventionally, tiflotechnics can be divided into 4 types:
1. Visual aids are tactile indicators and tactile-sound devices: mnemonic diagrams, plates, stands. These devices help a person unaided to navigate in any room or on the street, using tactile sensations and hearing.
2. Means of detection are walking sticks, echo sounders, as well as individual typhlo devices for recognizing objects and objects. Individual tiflopribors include laser tiflotechnique, which allows, when pointing a laser beam, to obtain information about objects and objects in front of a person (tiflomarker with tiflomarks).
3. Information means are information tactile-sensor terminals, visual-acoustic systems and radio modules. These devices are universal and are intended for all people, including those with visual impairments.
4. indicators are light and sound beacons, Braille signs, tactile pictograms and tactile ground markers. These devices allow a blind person to determine the right direction when moving on an object. Tactile ground markers include tactile tiles, indicators, guides and tactile mudguard systems.
Psychophysiological foundations of tiflotechnics
Tyflotechnics is based on the generally accepted principles of psychology, pedagogy and human physiology, takes into account recommendations that relate to many branches of medicine, and also uses the laws of optics, acoustics, electronic automation and technology, information theory and cybernetics.
Tiflotechnics helps to restore lost visual functions through the use of special technical devices and assistive devices. It contributes to the elimination of stiffness, supports and develops the natural motor need of a person with limited vision, helps his full-fledged all-round development on an equal basis with other people.
| Selection from the database: At present, psychology is not only a serious science, SETTING AND AUTOMATION OF SOUND.docx, TKP 609-2017 Automation of distribution networks.pdf which are one of the hits d, Involving parents in the management of education is one of, Testing in the discipline Automation of technological processes, A.P. Arkharov (2011) Automation of production processes in m, Communication, both personal and business is a necessary part, What is a strategic factor in increasing susceptibility to, The basis of creative management is creative thinking.doc 1 2 3 4 5 6 7 8 9 10 11 INTRODUCTION Automation is one of the most important factors in the growth of labor productivity in industrial production. A continuous condition for accelerating the growth rate of automation is the development of technical means of automation. The technical means of automation include all devices included in the control system and designed to receive information, transmit, store and convert it, as well as to implement control and regulatory actions on the technological control object. The development of technological means of automation is a complex process, which is based on the interests of automated production-consumers, on the one hand, and the economic capabilities of enterprises - manufacturers of means, on the other. The primary stimulus for development is to increase the efficiency of production - consumers, through the introduction of new technology can be expedient only if the costs are quickly paid back. Therefore, the criterion for all decisions on the development and implementation of new tools should be the total economic effect, taking into account all the costs of development, production and implementation. Accordingly, for the development, manufacture, first of all, those options for technical means that provide the maximum total effect should be taken. With strict adherence to this principle of development and implementation of new tools, the process of their development is strictly optimal and, as a result, objective. However, a sufficiently rigorous substantiation of the optimality of means at the stage of their development and implementation is practically impossible due to the complexity and limited accuracy of estimates of the total expected effect. The presence of such a criterion makes it possible to consider the development of technical means of automation as an objective process as a whole. Accordingly, the constantly updated composition of technical means of automation and their technical characteristics can be regarded as approaching, on average, optimal at a given stage in the development of material production. In accordance with the decisions of the Government of Russia, it is now necessary to ensure the further economic progress of society, accelerate scientific and technological progress, and increase the efficiency of social production in order to get the country out of the crisis as soon as possible. At present, special attention is paid to the need for the rapid development of the machine-building industry. The constant expansion of automation is one of the main features of the industry at this stage. Particular attention is paid to the issues of industrial ecology and labor safety in production. When designing modern technology, equipment and structures, it is necessary to scientifically substantiate the development of safety and harmlessness of work. In connection with the development of industry, environmental pollution has increased, so the rational use of natural resources is a matter of national importance. 1 ANALYSIS OF THE AUTOMATION OBJECT
1. Currently, in the thermal shops of the plant, (in particular KumAPP), the most used for further metal processing is the preheating of workpieces in resistance furnaces. A metal heating furnace consists of the following main structural elements: a frame, lining, mechanisms for moving billets through the furnace, mechanisms for loading and unloading heating elements, and a shielding gas supply system. Various materials are used in the manufacture of ovens. Separate units of furnaces operate at temperatures not exceeding 100ºС, therefore, for their manufacture, ordinary carbon steels and cast irons used in mechanical engineering are used. Some furnace components operate at temperatures close to 1000ºC, so they are made of special steels or refractory materials. The furnace has a working space where the workpieces are heated. The working space of the furnace is arranged in such a way as to ensure uniform heating of the heated workpieces. 1.3 Technological process of heating metal in furnaces (heat treatment) The process of heating metal billets in electric furnaces can be conditionally divided into the following periods: loading of billets into the furnace, their heating and release. The workpieces are loaded into the furnace through the loading window. The workpieces move in the furnace along two guides laid on transverse supports. The heating time for volumetric hardening of a part made of steel grade 45 takes 35-40 minutes. The temperature of the electric oven KS 800 is set to 850±10ºС. Temperature control is carried out by a potentiometer GOST 7164-78. Hardening is carried out at an oil temperature of 20-70ºС. Oil temperature control is carried out with a thermometer 0-150ºС GOST 28498-90. Tempering at 300°C for 2 hours. The part is shaped like a ring with a cross section of 10 mm; Ø outer 40 mm; height 28mm. Workpiece hardness 39.5…50.5 HRC. The control is carried out pr. Brinel tsh-2 m GOST23677-79 ball Ø2.5mm. Picture 1.1 - Shaft blanks; physical properties of the metal (thermal conductivity, heat capacity and thermal diffusivity) and a number of other factors, but even with the optimal combination of the above parameters, the heating period of the workpieces in furnaces is long and one of the main disadvantages of metal heating in furnaces. 2. The absence of a temperature control system at the time of billets and furnace delivery creates certain difficulties in processing metal after it has been heated. The need to create such a system is due to the fact that in its absence it is possible to obtain overheated or underheated metal, which, in turn, negatively affects the course of the further technological process. 3. When heated in flame or electric furnaces, the surface of parts comes into contact with furnace gases. In particular, the harmful substances contained in the smoke have a harmful effect on the health of workers. The need to use a smoke exhaust system due to the negative impact of smoke is an economic disadvantage , as well as a disadvantage in terms of the occupied production area. Also, the impossibility of saving space due to the large dimensions of the furnaces themselves creates significant difficulties in their operation and rational use of space in production. Thus, the disadvantages of heating furnaces are a rather long heating time, and a large loss of metal that goes into scale, an adverse impact on the environment, the absence of a temperature control system at the time the blanks are taken out of the furnace, large dimensions of the furnaces, as well as the requirement for a large consumption of electricity, lower efficiency and ease of use. During operation, metal heating furnaces must provide heating of the appropriate temperature, minimum metal waste, low power consumption and maximum productivity, i.e. the main factors of operation should be economy and compliance with environmental requirements, as well as the reduction of human labor resources. 1.5 The main directions of increasing the efficiency of metal heating technical processes To meet such requirements, it is planned to replace resistance furnaces with induction heating units (Figure 1.2). Induction heating refers to heating by non-contact transfer of energy to a heated body using electromagnetic waves. Induction heating is widely used in industry and research. New technological processes are being developed, such as high-temperature heating, metal heating for plastic deformation at industrial and elevated frequencies.
detail Figure. 1.2-Induction heating installation. Replacing the ovens with induction heating units, it is planned to install a temperature control system that includes three pyrometers, as well as two optical pairs that control loading and unloading. The operation of the power supply and load control (inductor) is carried out by a thyristor frequency converter (TFC). A PC is supposed to be used as a control machine that receives signals from pyrometers about the current temperature and from sensors about the process of loading and unloading. The use of induction heating and the prospects for its development in the conditions of production intensification are due to a number of permanent reasons: Heating up a gas furnace or a resistance furnace with their massive lining takes hours and consumes up to 40% of the energy consumed per shift. Ease of maintenance and especially repair of the installation, which usually comes down to replacing the inductor, which takes several tens of minutes. High reliability due to low lining temperature. Small waste of metal, which is 2-4 times less than in flame furnaces and resistance furnaces, due to the high heating rate and the presence of a stagnant gas environment in a small air gap between the lining and the heating object. Increased die life by 20-30% due to reduced scale layer and increased material ductility due to rapid heating, which is one of the significant savings. Ease of automation and mechanization of the process.  High productivity and good space utilization. Dramatic improvement in working conditions due to a drastic reduction in the release of heat, gases and solid particles compared to flame and resistance furnaces. Establishing a temperature control system at the time of issuing blanks will help control the heating process to exclude the possibility of obtaining underheated or overheated metal, which will positively affect the process of further metal processing. Optical sensors will monitor whether the workpiece is inside the inductor or outside it and send a signal to the control machine, which will process the information and give a command to turn the inductor off and on. The block of sensors located in the TFC are designed to generate feedback synchronization signals, protection and signaling and for electrical isolation of the PC from the power circuit. Thanks to the connection of a computer, the speed of processing information from sensors and pyrometers of the entire technological process will increase, it will significantly reduce the time of the entire technological process, significantly reduce labor resources and minimize the role of a person. A number of the above advantages create fertile ground for the automated use of induction heating installations in production instead of large gas flame furnaces and resistance furnaces. 2 DESIGN PART 2.1 Technical design of the control system In this part of the course project, the selection of equipment elements was made, the system operation algorithm and structural diagram were developed, and the thermal and electrical calculation of the inductor was carried out. 2.2 Physical essence of induction heating The method of induction heating is based on the use of the following laws and phenomena:
When using the method of induction heating, one also has to take into account the presence of other phenomena that cause the peculiarity of the distribution of currents in the inductor and the heated workpiece. 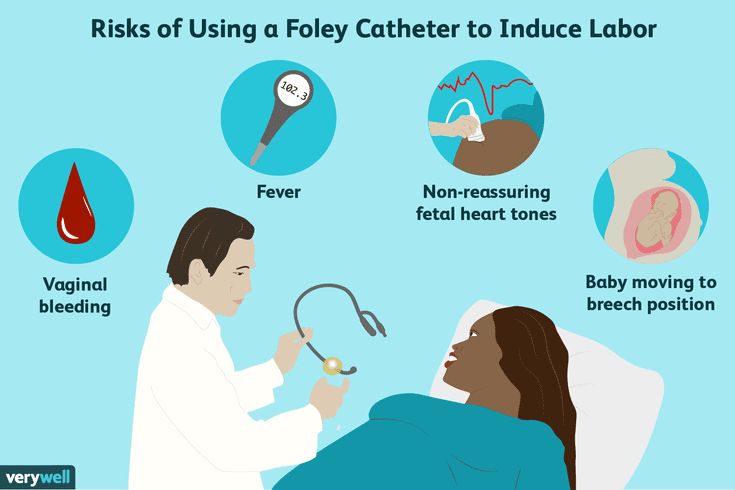 Let us briefly characterize these phenomena. Let us briefly characterize these phenomena. For the method of induction heating, the significance of electromagnetic induction lies primarily in the ability to transfer electromagnetic energy to a heated object without resorting to contacts. The skin effect is the basis of induction heating. It is expressed in the uneven distribution of current over the cross section of the conductor, in which the highest current density is observed at one of the surface of the conductor. The current density for different points of the cross section of the conductor will not be the same. The higher the current frequency, the greater the inductive reactance in the center of the conductor and the lower the current density. Proximity effect is a kind of surface of conductors as a result of the total interaction of electromagnetic fields of all conductors with the current included in the system under consideration. The pattern of the magnetic field and current distribution in the case of the proximity effect is shown in fig. Figure 2.1-Picture of the magnetic field and current distribution under the proximity effect : a) identically directed currents, b) oppositely directed currents. Using the proximity effect, you can choose the appropriate shape of the inductor to concentrate heat in certain parts of the surface of the treated body. The proximity effect is the stronger, the smaller the distance between the conductors and the stronger the skin effect, that is, the greater the ratio of conductor thickness to current penetration depth. 2.2 shows the picture of the magnetic field of the inductor, inside which is placed a metal cylinder. The current in the inductor, due to the ring effect and the proximity effect, is concentrated on its inner surface, in most of it with an almost uniform density, which slightly increases towards the corners of the drive. This is explained by the fact that the current filaments lying at the corners of the wire are covered by a smaller magnetic flux than those located in the middle part, and a smaller counter-emf is induced in the filaments than in the filaments located in the middle part of the wire.
Figure 2.2-Magnetic field of the inductor, inside which the heated part is placed . On the contrary, the current flows in the cylinder precisely under the influence of the emf induced in the cylinder. This emf is the greater, the greater the magnetic flux associated with the considered annular current filament. It can be seen from the field picture that the current filaments located in the middle plane of the inductor are associated with the highest magnetic flux, where the maximum incandescence (surface density) of the current is observed. Outside the inductive wire, the induced current drops rapidly. Thus, the current induced in the cylinder is concentrated in a strip whose width differs little from the width of the inductor. We will assume that the width of this band, called active, is approximately equal to the width of the inductor. With an increase in the heating temperature of steel parts, the specific resistance ρ increases and above 1000˚С reaches its maximum value. The magnetic permeability in the range of 600-700˚С is almost independent of temperature, but with its further increase it drops sharply and reaches a minimum value equal to the magnetic permeability of vacuum (μ=1). For practical calculations, the depth of penetration δ of the current into the metal is calculated using simplified formulas: for steel parts at a temperature of 15 ° C (2.1) and at a temperature of 760ºС (2.2) for copper at a temperature of 15ºС (2.3) where δ is the current penetration depth, mm; f is the current frequency, Hz. From the data given in Table 2.1 it follows that with an increase in the heating temperature of the metal, the current penetration depth increases and reaches its maximum value at the temperature of the loss of magnetic properties - the Curie point. For most steels, magnetic transformations occur in the critical temperature range of 765-780˚C, at which the magnetic permeability drops sharply and becomes equal to unity. Μ=1 Gs/Oe | At t=15˚С, P=1.8 10 -6 Ω cm, Μ=1 G /E | |
| 50 2500 10000 100000 1000000 | 0.5 0.067 0.011 9000
0.0002 0.0002 0.0002 0.0002 0.0002 0.0002 0.0002 0.0002 0.0002 0.0002 0.0002 0.0002 0.0002 0.0002 0.0002 0.000 0.000 0.000 0.000 0.000 0.000EAL 1.0 0.5 0.16 0.05 | 1.0 0.13 0.07 0.022 0.007 |

 Therefore, the only objective criterion for the optimality of funds can only be their wide practical operation, which allows you to display unsuccessful decisions and developments and develop those principles, schemes and designs that generally meet the requirements of maximum efficiency.
Therefore, the only objective criterion for the optimality of funds can only be their wide practical operation, which allows you to display unsuccessful decisions and developments and develop those principles, schemes and designs that generally meet the requirements of maximum efficiency.  To do this, it is necessary to develop and implement highly effective methods for improving the strength properties, corrosion resistance, heat and cold resistance of the metals and alloys used. The use of automated lines and machines, automatic manipulators with program control will make it possible to exclude manual unskilled labor, especially in difficult and harmful conditions for humans.
To do this, it is necessary to develop and implement highly effective methods for improving the strength properties, corrosion resistance, heat and cold resistance of the metals and alloys used. The use of automated lines and machines, automatic manipulators with program control will make it possible to exclude manual unskilled labor, especially in difficult and harmful conditions for humans.  2 Description of the existing equipment
2 Description of the existing equipment 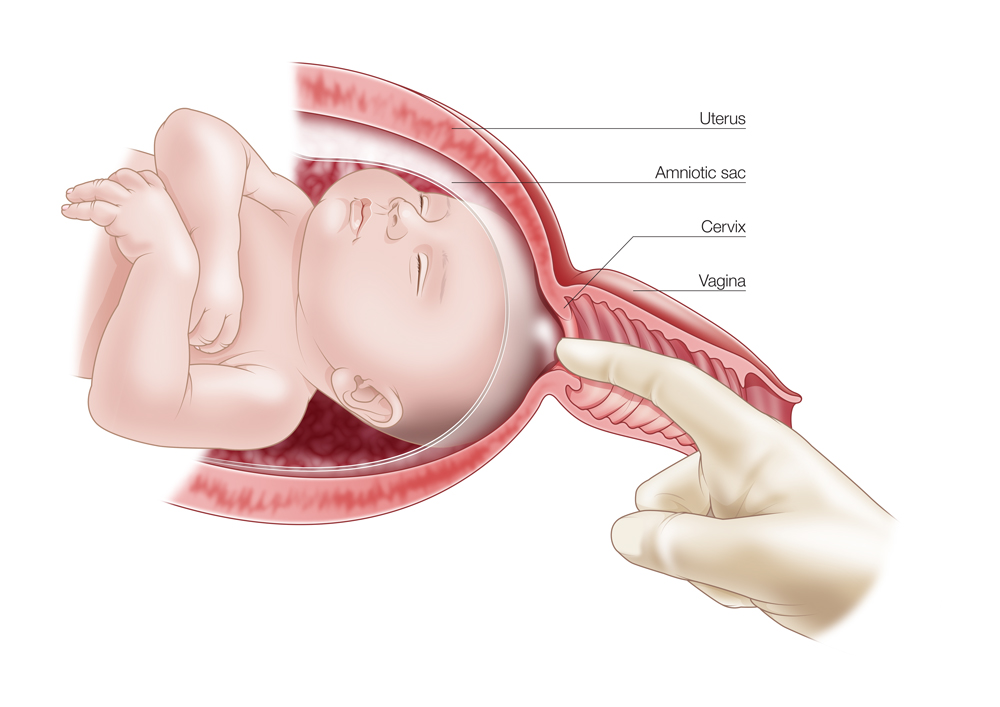
 Part weight 0.19.
Part weight 0.19.  As a result, the metal oxidizes and scale forms on the parts. With an increase in temperature and exposure time, oxidation increases sharply. The formation of scale causes waste (loss) of the metal and distorts the geometric shape of the parts. The surface of the steel under the scale is corroded and uneven, which makes it difficult to process the metal with a cutting tool. Scale from the surface of parts is removed by pickling in sulfuric acid or by cleaning in shot blasting plants. Due to the resulting metal waste, soot and smoke during the operation of furnaces, they adversely affect the environment as a whole.
As a result, the metal oxidizes and scale forms on the parts. With an increase in temperature and exposure time, oxidation increases sharply. The formation of scale causes waste (loss) of the metal and distorts the geometric shape of the parts. The surface of the steel under the scale is corroded and uneven, which makes it difficult to process the metal with a cutting tool. Scale from the surface of parts is removed by pickling in sulfuric acid or by cleaning in shot blasting plants. Due to the resulting metal waste, soot and smoke during the operation of furnaces, they adversely affect the environment as a whole. 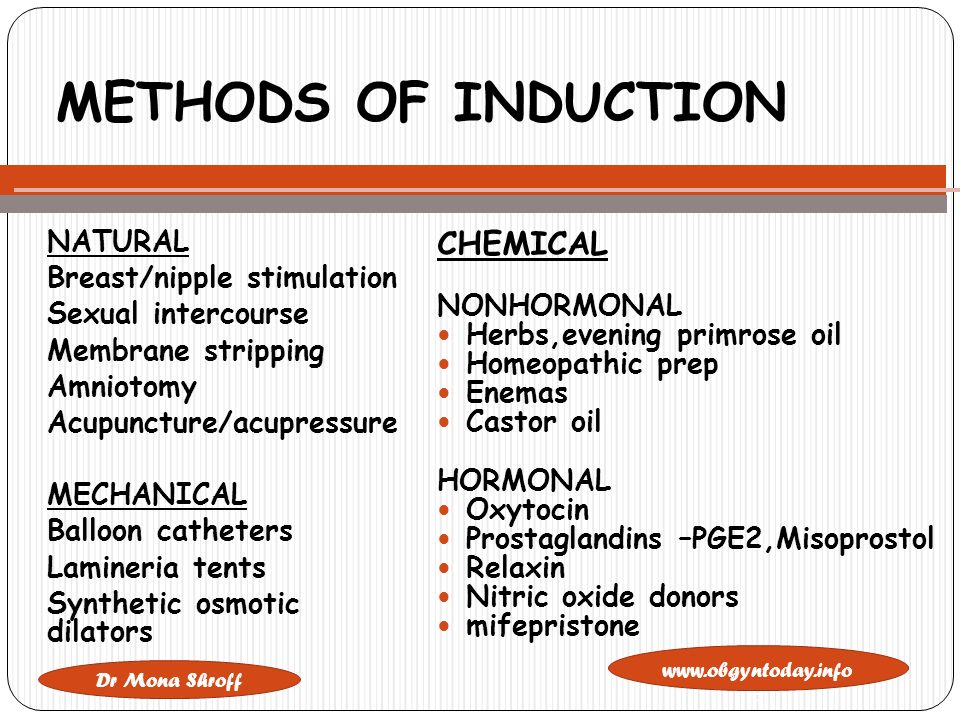
 Induction installations basically have an inductor-conductor of a special shape, powered by alternating electric current. When current flows through the inductor, an alternating electromagnetic field arises. When an alternating field occurs on metallic bodies, the latter are heated.
Induction installations basically have an inductor-conductor of a special shape, powered by alternating electric current. When current flows through the inductor, an alternating electromagnetic field arises. When an alternating field occurs on metallic bodies, the latter are heated. 

 2.1
2.1 

 After the steel loses its magnetic properties with the formation of austenite, the depth of current penetration increases sharply. -4 Ω cm,
After the steel loses its magnetic properties with the formation of austenite, the depth of current penetration increases sharply. -4 Ω cm, The highest value of the current penetration is called hot penetration depth and indicated Δ mountains .
Approximately it can be determined by the simplified formula
(2.4)
Knowing the dependence of the depth of current penetration on temperature, the process of inductive heating of steel can be represented as follows.
At the first moment, heating of steel begins in a thin surface layer equal to the depth of current penetration into the cold metal. After the loss of magnetic properties by this layer, the current penetration depth increases and the layer located deeper is heated, the temperature increase in the first heated layer slows down.
After the loss of magnetic properties of the second layer, the third layer begins to heat up rapidly, and so on. The limit of growth of the current penetration depth is the hot penetration depth.
The temperature increase in the hot penetration layer occurs due to induced currents, and in deeper layers, mainly due to thermal conductivity.
Selection and assignment of equipment items. The device for induction heating includes a complex of functional elements connected in a certain sequence: a source of electrical energy; a converter of electrical energy of one type of current to another; load element (consumer of electrical energy) unit for converting electrical energy into thermal energy; technological prefix; control unit and control of the electric mode of the technological process; the control and monitoring unit achieves the technological mode of process control; facilities and auxiliary equipment.
As a power source for induction installations, it uses thyristor current converters of industrial frequency 50 Hz into alternating current of increased frequency 0.5-1 kHz. The frequency converter is carried out by switching direct current controlled silicon valves - thyristors.
Advantages of semiconductor thyristor frequency converters: efficiency is 7-15% higher than machine; instant readiness for work; the ability to adjust the operating frequency, which allows you to create optimal heating modes; short downtime associated with repairs; small weight loads; less need for cooling water.
The control and monitoring unit for the energy mode of the device for induction heating contains a system of sensors, actuators and instrumentation. We choose pyrometers as control and measuring devices, which measure the current temperature of the heated body and send information about this temperature to the control machine. Pyrometers are installed inside the inductor. The system of sensors installed at the inlet of the heating element controls the progress of loading and unloading workpieces.