How to stop acid reflux while pregnant
Indigestion and heartburn in pregnancy
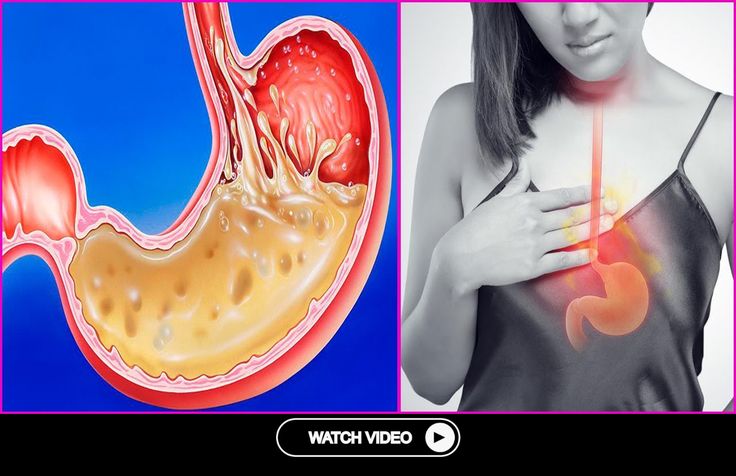
Indigestion, also called heartburn or acid reflux, is common in pregnancy. It can be caused by hormonal changes and the growing baby pressing against your stomach.
You can help ease indigestion and heartburn by making changes to your diet and lifestyle, and there are medicines that are safe to take in pregnancy.
Symptoms of indigestion and heartburn
Symptoms of indigestion and heartburn include:
- a burning sensation or pain in the chest
- feeling full, heavy or bloated
- burping or belching
- feeling or being sick
- bringing up food
Symptoms usually come on soon after eating or drinking, but there can sometimes be a delay between eating and developing indigestion.
You can get symptoms at any point during your pregnancy, but they are more common from 27 weeks onwards.
Things you can do to help with indigestion and heartburn
Changes to your diet and lifestyle may be enough to control your symptoms, particularly if they are mild.
Eat healthily
You're more likely to get indigestion if you're very full.
If you're pregnant, it may be tempting to eat more than you would normally, but this may not be good for you or your baby.
Find out more about a healthy diet in pregnancy and foods to avoid.
Change your eating and drinking habits
You may be able to control your indigestion with changes to your eating habits.
It can help to eat small meals often, rather than larger meals 3 times a day, and to not eat within 3 hours of going to bed at night.
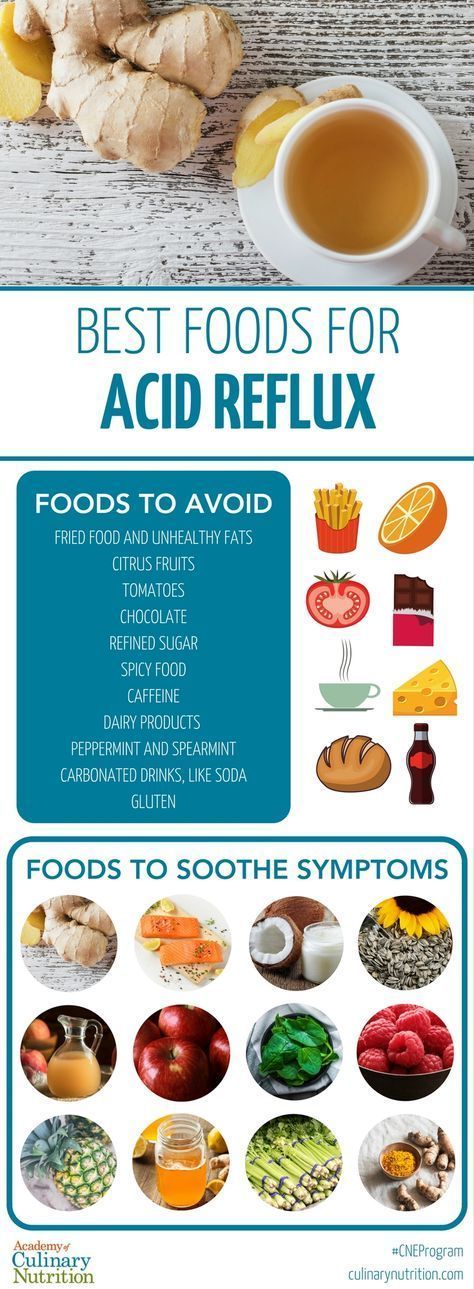
Cutting down on drinks containing caffeine, and foods that are rich, spicy or fatty, can also ease symptoms.
Keep upright
Sit up straight when you eat. This will take the pressure off your stomach. Propping your head and shoulders up when you go to bed can stop stomach acid coming up while you sleep.
Stop smoking
Smoking when pregnant can cause indigestion, and can seriously affect the health of you and your unborn baby.
When you smoke, the chemicals you inhale can contribute to your indigestion. These chemicals can cause the ring of muscle at the lower end of your gullet to relax, which allows stomach acid to come back up more easily. This is known as acid reflux.
Smoking also increases the risk of:
- your baby being born prematurely (before week 37 of your pregnancy)
- your baby being born with a low birthweight
- sudden infant death syndrome (SIDS), or "cot death"
There's lots of help available to stop smoking. Talk to your midwife or call the NHS Smokefree helpline on 0300 123 1044. Find out more about stopping smoking in pregnancy.
Talk to your midwife or call the NHS Smokefree helpline on 0300 123 1044. Find out more about stopping smoking in pregnancy.
Avoid alcohol
Drinking alcohol can cause indigestion. During pregnancy, it can also lead to long-term harm to the baby. It's safest to not drink alcohol at all in pregnancy.
Find out more about alcohol and pregnancy
When to get medical help
See your midwife or GP if you need help managing your symptoms or if changes to your diet and lifestyle do not work. They may recommend medicine to ease your symptoms.
You should also see your midwife or GP if you have any of the following:
- difficulty eating or keeping food down
- weight loss
- stomach pains
Your midwife or GP may ask about your symptoms and examine you by pressing gently on different areas of your chest and stomach to see whether it's painful.
If you're taking prescription medicines
Speak to your GP if you're taking medicine for another condition, such as antidepressants, and you think it may be making your indigestion worse. They may be able to prescribe an alternative medicine.
Never stop taking a prescribed medicine unless you're advised to do so by your GP or another qualified healthcare professional who's responsible for your care.
Medicines for indigestion and heartburn
Medicines for indigestion and heartburn during pregnancy include:
- antacids – to neutralise the acid in your stomach (some are available over the counter from a pharmacist)
- alginates – to relieve indigestion caused by acid reflux by stopping the acid in your stomach coming back up your gullet
You may only need to take antacids and alginates when you start getting symptoms. However, your GP may recommend taking them before symptoms come on – for example, before a meal or before bed.
However, your GP may recommend taking them before symptoms come on – for example, before a meal or before bed.
If you're taking iron supplements as well as antacids, do not take them at the same time. Antacids can stop iron from being absorbed by your body.
If antacids and alginates do not improve your symptoms, your GP may prescribe a medicine to reduce the amount of acid in your stomach. 2 that are widely used in pregnancy and not known to be harmful to an unborn baby are:
- ranitidine – a tablet you take twice a day
- omeprazole – a tablet you take once a day
Causes of indigestion in pregnancy
Symptoms of indigestion come when the acid in your stomach irritates your stomach lining or your gullet. This causes pain and a burning feeling.
When you're pregnant, you're more likely to have indigestion because of:
- hormonal changes
- the growing baby pressing on your stomach
- the muscles between your stomach and gullet relaxing, allowing stomach acid to come back up
You may be more likely to get indigestion in pregnancy if:
- you had indigestion before you were pregnant
- you've been pregnant before
- you're in the later stages of pregnancy
Video: Eating well on a budget
In this video, a dietitian gives advice on how to eat healthily on a budget.
Media last reviewed: 13 January 2021
Media review due: 13 January 2024
Pregnancy Heartburn? 7 Ways to Get Relief
Keywords
Kathryn Walker, MD
Women and Newborn
Learn more about women and newborn services we offer.
Expectant mothers everywhere are aching to know one thing: “How can I get some relief from this awful pregnancy heartburn?”
To help ease your pain, here are some answers to your “burning” questions. (Pardon the pun.)
(Pardon the pun.)
When you’re growing a human being, you don’t have time for that yucky acid reflux. But your usual go-to methods for treating it may not be safe for your unborn baby. (Remember Pepto Bismol? That’s on the No Fly List for moms-to-be, according to FDA recommendations.)
Instead, here are some of the safest and best ways to get rid of heartburn when you’re pregnant:
- Dip into some yogurt. Its probiotics and soothing texture make yogurt a great option for extinguishing heartburn – or at least dousing the flames a little.
- Drink milk with honey. According to the American Pregnancy Association, a tablespoon of honey mixed in a glass of warm milk may be just what you need to neutralize heartburn-causing acid.
- Snack on almonds. Munching on a handful of almonds may provide heartburn relief since these nuts have a lower acidity level than others.
- Eat pineapple or papaya.
 For some women, the digestive enzymes in pineapple and papaya have helped ease symptoms. Eating these fruits after your meals can aid digestion and reduce your chances of heartburn.
For some women, the digestive enzymes in pineapple and papaya have helped ease symptoms. Eating these fruits after your meals can aid digestion and reduce your chances of heartburn. - Try a little ginger. You probably knew ginger was a good remedy for an upset stomach. Well, that makes it a helpful candidate for fighting off heartburn, too. Among ginger’s many benefits, it can reduce inflammation and prevent stomach acid from traveling up the esophagus.
- Chew sugar-free gum. Another effective method for taming the burn is to chew some sugar-free gum. One study found that chewing sugar-free gum for 30 minutes after a meal can reduce acid reflux.
- Take (doctor-approved) medication. When all else fails, certain medications are considered safe to use for pregnancy heartburn relief. Just make sure you speak to your doctor or OB-GYN first. If your heartburn is severe, they may prescribe special medication to help control it.
While not every tip mentioned above may work to ease your symptoms, you’ve got nine months to try them all and figure out what works.
It’s important to be extremely careful about the medications you take when pregnant.
For heartburn relief, over-the-counter antacids (such as Tums, Mylanta, Rolaids, and Maalox) are all considered safe medications to use during pregnancy.
As always, consult with your provider about any medications you’re taking – even if they’re considered safe. (This is especially true for high-risk pregnancies.)
If you experience any unusual symptoms while taking an over-the-counter medication, call your doctor immediately.
They say prevention is the best medicine, so knowing common heartburn triggers can help you keep the acid at bay.
Of course, pregnancy itself is a major trigger for heartburn. As your growing uterus puts pressure on your stomach, this pushes stomach acid up your throat.
Those lovely hormones are no help either.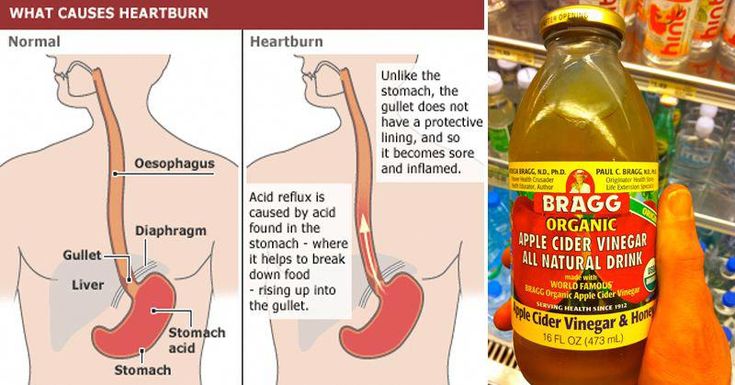 They tend to relax the valve between your stomach and esophagus, which makes it easier for acid to make its way upward.
They tend to relax the valve between your stomach and esophagus, which makes it easier for acid to make its way upward.
While there’s nothing you can do to stop this entirely, there are a few things that can help prevent heartburn from flaring up during pregnancy:
- Avoid lying down after eating. It may be tempting to take a post-meal nap, but if you want to prevent heartburn, don’t lie down after eating. Consider napping in an upright recliner instead.
- Prop yourself up at night. It’s hard enough to sleep well while pregnant without throwing acid reflux on top of everything. To prevent nighttime heartburn, try propping yourself up when you go to sleep to counteract the acid.
- Don’t eat before bedtime. In addition to propping yourself up at night, try not to eat anything within three hours of hitting the sack.
- Skip spicy, acidic, or fried foods. Ask yourself: Are those greasy chips worth being doubled over in pain later? (Probably not.
 ) If you want to avoid the risk, steer clear of any and all rich, fatty foods. Not only will this help prevent heartburn, but making more nutritious choices helps ensure that you your baby is getting the important vitamins and minerals that they need to stay healthy in utero.
) If you want to avoid the risk, steer clear of any and all rich, fatty foods. Not only will this help prevent heartburn, but making more nutritious choices helps ensure that you your baby is getting the important vitamins and minerals that they need to stay healthy in utero. - Eat small meals, but more frequently. Your pregnant tummy doesn’t love to be hit with large amounts of food to digest in one go. Make things easier on your gut by eating several small meals throughout the day instead of three large ones.
- Eat slowly. Wolfing down those small meals will defeat the purpose of spreading them out. Eating quickly increases the risk of acid reflux, so slow down and enjoy your food.
- Wear loose clothing. Tight-fitting clothes are not your stomach’s best friend when you’re trying to prevent heartburn – particularly during pregnancy. Wear clothing that offers support without being restrictive.
- Drink your liquids between meals.
 If you’re the type of person who likes to take a swig of their drink between each bite, it’s time to change course. Drinking liquids during meals can exacerbate heartburn symptoms, so take little sips if you’re thirsty at mealtime.
If you’re the type of person who likes to take a swig of their drink between each bite, it’s time to change course. Drinking liquids during meals can exacerbate heartburn symptoms, so take little sips if you’re thirsty at mealtime.
Someday, scientists may very well invent a miracle medication that promises permanent pregnancy heartburn relief. Unfortunately, that hasn’t happened yet.
So, if you’re wondering how long you can expect to deal with heartburn while you’re pregnant, it will probably be throughout your entire pregnancy. (Now may be a good time to remind yourself that you get a cute little baby out of this when you’re done.)
However, just because there’s no cure, that doesn’t mean you can’t find some relief in the meantime.
If severe pregnancy heartburn is getting in the way of everyday life, it’s time to see a doctor.
Intermountain Healthcare offers individualized and compassionate pregnancy care for women of all ages and health needs.
To get the care you need, search for a provider or find an Intermountain Healthcare location near you.
Intermountain Moms Women's Health, Baby Your Baby, Pregnancy, Women and Newborn
Last Updated: 5/21/2021
-
Intermountain Moms
-
Intermountain Moms
Copyright ©2022, Intermountain Healthcare, All rights reserved.
Treatment and prevention of gastroesophageal reflux disease
Treatment and prevention of gastroesophageal reflux disease (GERD)
Gastroesophageal reflux disease (GERD) common but rarely self-diagnosed and therefore untreated since GERD usually responds well to treatment.
GERD is treated gradually. The doctor will help you choose the right course of treatment. If the disease is mild, it will be enough for the patient to follow a certain diet, give up certain activities, and sometimes take over-the-counter medications.
In cases where symptoms are more persistent (daily heartburn, symptoms that come on at night), prescription medication may be required. Surgery is a reasonable alternative to permanent medication, especially if the disease is acquired at an early age.
Surgery is also recommended if medication does not help. However, today there is a new generation of drugs that can effectively control gastroesophageal reflux.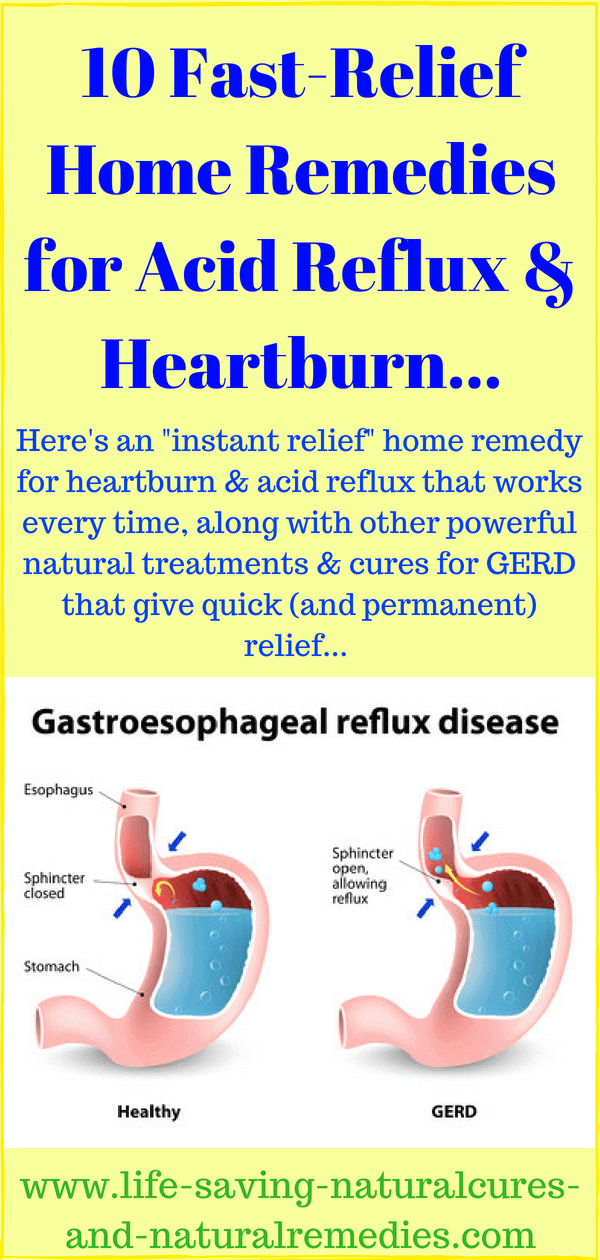
If symptoms are still uncomfortable after taking strong drugs, GERD is most likely not the cause. Most gastroenterologists and surgeons do not recommend surgery in such cases, since the symptoms still continue to disturb after it.
Lifestyle changes
Gastroesophageal reflux treatment begins with lifestyle changes. First you need to understand what affects the occurrence of symptoms.
If you have symptoms of GERD, use the following tips:
- Avoid foods and drinks that stimulate the lower esophageal sphincter to relax, such as foods flavored with mint, chocolate, and alcohol.
- Lose weight if you are overweight. Being overweight and obese contributes to GERD because being overweight increases pressure on the stomach and lower esophageal sphincter, causing acidic stomach acid to reflux into the esophagus and irritate the esophageal mucosa.
- Do not lie down for at least two or three hours after eating.
 After eating it is good to take a walk. This not only prevents the onset of GERD symptoms, but also burns extra calories.
After eating it is good to take a walk. This not only prevents the onset of GERD symptoms, but also burns extra calories.
- Avoid foods that trigger GERD symptoms. Do not eat fatty or fried foods, creamy sauces, mayonnaise or ice cream. Other foods that may exacerbate symptoms include coffee, tea, sodas, tomatoes, and citrus fruits.
- Stop smoking. Smoking disrupts the digestive system and, according to some studies, relaxes the lower esophageal sphincter. Smoking also reduces the amount of bicarbonate in saliva and reduces its ability to protect the esophagus from stomach acid. Some types of nicotine replacement therapy (nicotine patch, nicotine gum) can cause indigestion, stomach pain, and vomiting. Talk to your doctor about possible side effects of these products before use.
- Do not wear clothes that put pressure on your belly, such as tight belts, tight jeans, and elastic waistbands that put pressure on your stomach and lower esophageal sphincter.
- Raise the head of the bed 15-20 cm or use a wedge-shaped pillow to force acid into the stomach by gravity.
- Do not bend over after eating. If you need to pick something up from the floor, it's better to squat on half-bent knees and try not to bend at the waist. Do not engage in sports and physical labor after eating.
- Check your medications. Some medications can make symptoms worse. These drugs include theophylline, calcium channel blockers, alpha and beta blockers, anticholinergics that may be present in drugs used to treat Parkinson's disease, asthma, and some over-the-counter cold and cough medicines. If you think a drug you are taking is affecting your symptoms, talk to your doctor about alternatives. Do not interrupt the prescribed treatment without consulting a doctor.
Medication for gastroesophageal reflux
Your doctor may prescribe medication for GERD. Because GERD is often a chronic condition, you will need to take medication for the rest of your life. In some cases, long-term treatment is not required.
Because GERD is often a chronic condition, you will need to take medication for the rest of your life. In some cases, long-term treatment is not required.
Be patient, it takes time to find the right drug and dosage. If the symptoms do not go away even after taking the drugs, or if they reappear immediately after completing the course, consult your doctor. If GERD symptoms appear during pregnancy, contact your obstetrician before starting medication.
The following is information about drugs commonly prescribed to treat GERD:
Over-the-counter antacids
These drugs help with mild and rare symptoms. Their action is to neutralize the acidic gastric juice. Antacids are usually fast-acting and can be taken as needed. Because they do not last long, they do not prevent heartburn and are less effective for symptoms that often occur.
Most antacids contain calcium carbonate (Maalox) or magnesium hydroxide. Sodium bicarbonate, or baking soda, helps with heartburn and indigestion. It should be mixed with at least 120 ml of water and taken one to two hours after meals so as not to overload a full stomach. Talk to your doctor about the need for this treatment. Do not use this method for more than two weeks and use it only in extreme cases, since soda can lead to metabolic disorders (pH) and the formation of erosions in the esophagus and stomach. Before using it on children under 12 years of age, consult a doctor.
Sodium bicarbonate, or baking soda, helps with heartburn and indigestion. It should be mixed with at least 120 ml of water and taken one to two hours after meals so as not to overload a full stomach. Talk to your doctor about the need for this treatment. Do not use this method for more than two weeks and use it only in extreme cases, since soda can lead to metabolic disorders (pH) and the formation of erosions in the esophagus and stomach. Before using it on children under 12 years of age, consult a doctor.
Another type of antacid contains alginate or alginic acid (eg Gaviscon). The advantage of such an antacid is that it does not allow fluid to seep back into the esophagus.
Antacids can interfere with the body's ability to absorb other drugs, so if you are taking other drugs, check with your doctor before taking antacids.
Ideally, you should take antacids at least 2-4 hours after taking other drugs to minimize the chance of them not being absorbed. People with high blood pressure should avoid taking high sodium antacids (Gaviscon).
People with high blood pressure should avoid taking high sodium antacids (Gaviscon).
Finally, antacids are not a reliable treatment for erosive esophagitis, a disease that must be treated with other drugs.
Hydrochloric Acid Suppressants
These drugs reduce the amount of acid produced by the stomach and are available with or without a prescription. Usually, the same drugs are dispensed on prescription, but in a larger dosage. They may help those who are not helped by antacids. Most patients get better if they take drugs that suppress the production of hydrochloric acid and make lifestyle changes.
The mechanism of action distinguishes between two groups of such drugs:
-Blocks H 2 -gistamine reticators
-Proton pump inhibitors
Most likely, the doctor recommends taking the drug within a few weeks in a standard dose, and then if it is not possible to achieve the desired effect, prescribe a drug with a higher dosage.
Traditional h3 blockers include:
- nizatidine (Axid AR Axid AR)
- famotidine (Pepcid AS Pepcid AC)
- cimetidine (Tagamet HB Tagamet HB)
- ranitidine 75 (Zantac 75)
Pepcid Complete is a combination of famotidine, calcium carbonate and magnesium hydroxide found in antacids.
Conventional proton pump inhibitors include:
- lansoprazole (Prevacid)
- omeprazole (Prilosec, Prilosec)
- rabeprazole (AcipHex, AcipHex, Pariet)
- pantoprazole (Protonix Protonix, Nolpaza Nolpaza)
- esomeprazole (Nexium) , Nexium)
- omeprazole + sodium bicarbonate ("Zegeride" Zegerid)
- dexlansoprazole ("Dexilant" Dexilant)
Proton pump inhibitors (PPI) also reduce acidity, but are more powerful than h3- blockers. Proton pump inhibitors are most commonly prescribed to treat heartburn and acid reflux.
These drugs block the secretion of acid from the cells of the gastric mucosa and significantly reduce the amount of stomach acid. They don't work as fast as antacids, but they can relieve reflux symptoms for hours.
They don't work as fast as antacids, but they can relieve reflux symptoms for hours.
PPIs are also used to treat inflammation of the esophagus (esophagitis) and erosions of the esophagus. Studies have shown that the majority of patients with esophagitis who took these drugs recovered after 6-8 weeks. It is likely that your doctor will re-evaluate your health after 8 weeks of taking proton pump inhibitors and, according to the results, reduce the dosage or stop treatment. If symptoms do not return within three months, you will only need to take medication occasionally. People with liver disease should consult their doctor before taking these drugs.
Prokinetics
Prokinetics, e.g. They also increase the contractions of the esophagus and stomach to some extent, so that the stomach is emptied more quickly. These drugs may be used as an adjunctive treatment for people with GERD.
Surgical treatment of GERD
Surgery is an alternative to conservative treatment of GERD. Surgery is most commonly performed on young patients (because they would otherwise require long-term treatment) with typical GERD symptoms (heartburn and belching) who are helped by medication but are looking for an alternative to daily medication.
Surgery is most commonly performed on young patients (because they would otherwise require long-term treatment) with typical GERD symptoms (heartburn and belching) who are helped by medication but are looking for an alternative to daily medication.
Patients with atypical symptoms or patients who are not responding to medical treatment should undergo surgery only when there is no doubt about the diagnosis of GERD and the relationship between symptoms and reflux is confirmed by research results.
Fundoplication is used in most cases. During this operation, the upper part of the stomach is wrapped around the lower esophageal sphincter, which increases its tone. These days, minimally invasive (laparoscopic) techniques are commonly used instead of traditional "open" surgery. One of the benefits of a fundoplication is that the hiatal hernia can also be repaired during the operation.
Surgery is not always effective and some patients still need to take medication after surgery. The results of this surgery are usually positive, but complications can still occur, such as difficulty swallowing, bloating and gas, difficult recovery after surgery, and diarrhea that occurs due to damage to the nerve endings that are adjacent to the stomach and intestines.
The results of this surgery are usually positive, but complications can still occur, such as difficulty swallowing, bloating and gas, difficult recovery after surgery, and diarrhea that occurs due to damage to the nerve endings that are adjacent to the stomach and intestines.
Prevention of GERD
First of all, you need to pay attention to lifestyle and avoid situations that can trigger the onset of the disease.
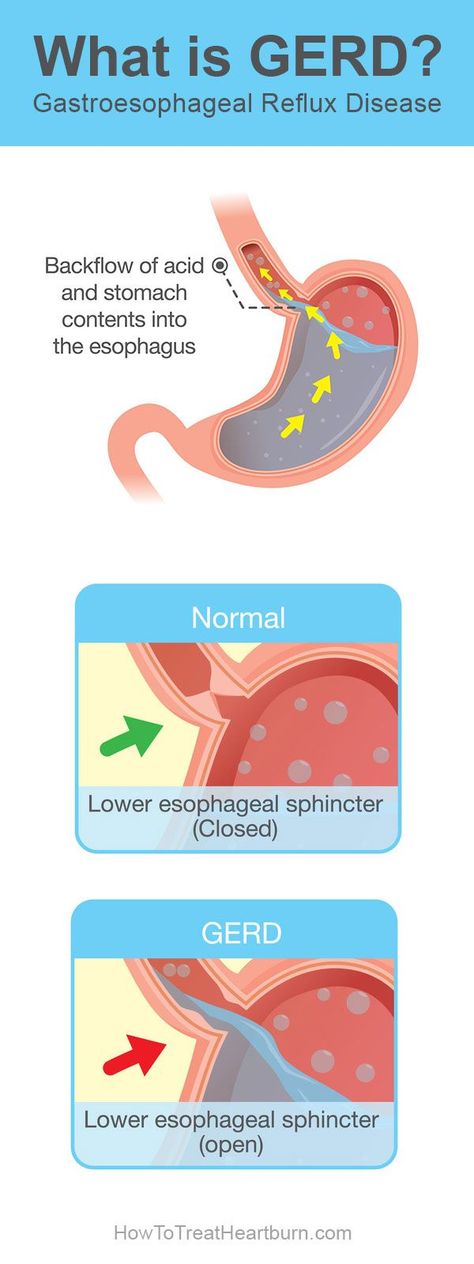
Remember that GERD happens when stomach acid backs up into the esophagus, which connects the throat to the stomach.
To keep the lower esophageal sphincter functioning properly, follow these guidelines:
Avoid bending over and other physical exercises that increase pressure on the abdominal cavity. Don't exercise on a full stomach.
Do not wear clothes that are tight around the waist, such as elastic waistbands and belts, which can increase pressure on the stomach.
Do not lie down in the field of food. If you lie on your back after a large meal, it will be easier for the contents of the stomach to pass into the esophagus. For a similar reason, don't eat before bed. The head of the bed should rise 15-20cm so that gravity keeps the acid in the stomach where it should be while you sleep.
If you lie on your back after a large meal, it will be easier for the contents of the stomach to pass into the esophagus. For a similar reason, don't eat before bed. The head of the bed should rise 15-20cm so that gravity keeps the acid in the stomach where it should be while you sleep.
Do not overeat. Due to the fact that there is a large amount of food in the stomach, pressure on the lower esophageal sphincter increases, as a result of which it opens.
To keep your lower esophageal sphincter and esophagus functioning properly, follow these tips:
Quit smoking and avoid products containing tobacco. Smoking relaxes the lower esophageal sphincter, reduces the amount of acid-neutralizing saliva in the mouth and throat, and damages the esophagus.
Avoid foods that aggravate symptoms, such as tomato sauces, mints, citrus fruits, onions, coffee, fried foods, and carbonated drinks.
Do not drink alcoholic beverages.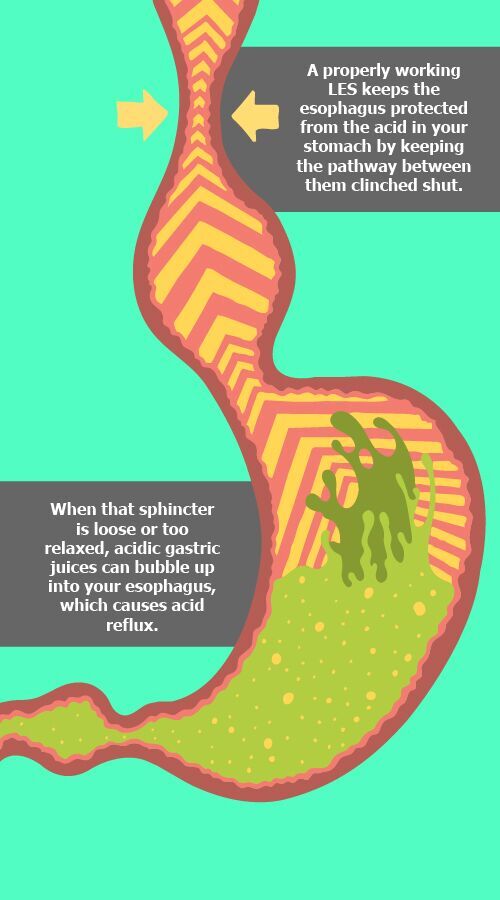 Alcohol causes the lower esophageal sphincter to relax, and the esophagus may begin to contract unevenly, causing acid to reflux into the esophagus and cause heartburn.
Alcohol causes the lower esophageal sphincter to relax, and the esophagus may begin to contract unevenly, causing acid to reflux into the esophagus and cause heartburn.
Check your medications. Some medications can make symptoms worse. Do not interrupt the prescribed treatment without consulting your doctor. Drugs that have this effect include asthma and emphysema drugs (such as theophylline), anticholinergics for Parkinson's disease and asthma, sometimes found in over-the-counter drugs, some calcium channel blockers, alpha blockers, and beta-blockers to treat heart disease or high blood pressure, some drugs that affect the nervous system, iron supplements.
While some drugs exacerbate GERD symptoms, others can cause drug-induced esophagitis, a condition that causes the same symptoms as GERD but is not due to reflux. Drug esophagitis happens when a pill is swallowed but does not reach the stomach because it sticks to the wall of the esophagus. Because of this, the mucous membrane of the esophagus is corroded, chest pain, esophageal ulcers and pain during swallowing occur.
Drugs that cause drug-induced esophagitis include aspirin, non-hormonal anti-inflammatory drugs (NSAIDs) such as ibuprofen (Mortin Motrin, Aleve Aleve), alendronate (Fosamax Fosamax), potassium, and some antibiotics (especially tetracycline). and doxycycline).
You can get more detailed information about the symptoms of gastroesophageal reflux disease from the gastroenterologists of the Health 365 clinic in Yekaterinburg.
Related articles:
pain in the abdomen
abdominal ultrasound
Gastroscopy (FGS)
Colonoscopy
Storemoroscopy
The main misconceptions for capsule endoscopy, FGS and colonoscopy
Preparation for endoscopic studies 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9000 9,000 9,000 9,000 9,000 9,000 9,000,0002 Gastric ulcer
Gastritis
Pancreatitis
Pancreas
Irritable bowel syndrome (IBS)
Non-specific ulcerative colitis
Cholecystitis
Crohn's disease
Gastroenteritis
Acid related diseases in pregnancy | Rassvet Clinic
Heartburn during pregnancy is a very common complaint. It is known that up to 80% of pregnant women experience symptoms characteristic of gastroesophageal reflux disease (GERD) (heartburn, dysphagia, belching, and others), and the frequency of heartburn in the first trimester is 7.2%, in the second - 18.2%, in the third - 40%.
It is known that up to 80% of pregnant women experience symptoms characteristic of gastroesophageal reflux disease (GERD) (heartburn, dysphagia, belching, and others), and the frequency of heartburn in the first trimester is 7.2%, in the second - 18.2%, in the third - 40%.
The main factors behind this high prevalence of GERD in pregnancy include hormonal changes such as hyperprogesteronemia (increased levels of the hormone progesterone) and hyperestrogenemia (increased levels of estrogen hormones), as well as increased intra-abdominal pressure due to the growth of the uterus and fetus.
The action of gestational hormones in the first trimester of pregnancy is due to the fact that they, without affecting the basal tone of the lower esophageal sphincter (LES), reduce the increase in pressure of this sphincter in response to a variety of physiological stimuli, including food intake. In the second and third trimesters of pregnancy, progesterone and estrogen reduce the basal tone of the LES to 50% of the initial level, the maximum decrease occurs at 36 weeks of gestation. After a successful delivery, the tone of the LES in women who did not suffer from GERD before pregnancy, as a rule, returns to normal - in connection with this, this condition is called "pregnancy heartburn."
After a successful delivery, the tone of the LES in women who did not suffer from GERD before pregnancy, as a rule, returns to normal - in connection with this, this condition is called "pregnancy heartburn."
Pregnancy heartburn usually does not lead to the development of esophagitis, complications of GERD (strictures, ulcers, bleeding) and does not require serious medical treatment.
If a woman had GERD before pregnancy, the complaints may worsen during pregnancy and require examination and medication.
The diagnosis of GERD during pregnancy is established primarily on the basis of complaints, anamnesis data and objective examination. X-ray examination in pregnant women - due to possible damaging effects on the fetus - is not used, pH-metry and manometry can be used, but the need for its use is doubtful.
Esophagogastroduodenoscopy (EGD) is the method of choice for diagnosing GERD in pregnant women, but it should only be used for strict indications, such as a history of complications of GERD and the ineffectiveness of ongoing drug therapy.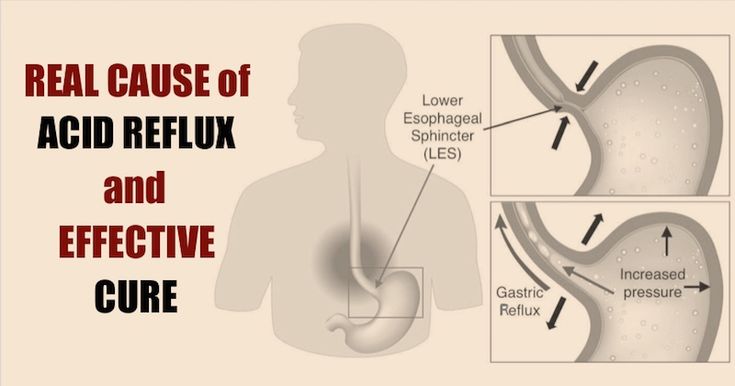
Treatment of GERD in pregnant women should be based on changes in lifestyle and nutrition: exclusion of a horizontal position of the body immediately after meals, sleeping with the head end of the bed elevated (by 15 cm), exclusion of physical activity that increases intra-abdominal pressure (including wearing corsets, tight belts, bandages). The last meal should take place no later than 3 hours before bedtime, you need to eat in small portions, pay special attention to the normalization of the stool.
First-line drugs for the treatment of GERD in pregnant women include antacids and alginates. With the ineffectiveness of these drugs, it is permissible to prescribe prokinetics (metoclopramide), blockers of histamine h3 receptors and (according to strict indications) proton pump inhibitors (PPIs).
H2-histamine blockers are the most commonly prescribed group of drugs for pregnant women. They are classified as risk category B by the US Food and Drug Administration (FDA) ( "drugs taken by a limited number of pregnant women without evidence of their effect on the incidence of congenital anomalies or damaging effects on the fetus") . In Russian instructions, only cimetidine and ranitidine are allowed with a caveat: use during pregnancy is possible only if the expected effect of therapy outweighs the potential risk to the fetus. Famotidine and nizatidine in the Russian Federation are contraindicated for pregnant women.
In Russian instructions, only cimetidine and ranitidine are allowed with a caveat: use during pregnancy is possible only if the expected effect of therapy outweighs the potential risk to the fetus. Famotidine and nizatidine in the Russian Federation are contraindicated for pregnant women.
Although most PPIs are also classified by the FDA as risk category B, in Russia there are more stringent restrictions on the use of this group of drugs in pregnant women. So, lansoprazole is contraindicated in the first trimester, in the second and third trimesters it can be used only if the expected benefit of therapy outweighs the potential risk to the fetus. The use of pantoprazole and esomeprazole is possible only under strict indications, when the benefit to the mother outweighs the potential risk to the fetus. Rabeprazole during pregnancy is contraindicated.
Pregnancy has a beneficial effect on the course of peptic ulcer disease: 75-80% of women experience remission of the disease, and it does not have a noticeable effect on its outcome. However, some patients may experience an exacerbation. This is most often observed in the first trimester of pregnancy (14.8%) and the third trimester (10.2%), as well as 2-4 weeks before the due date or in the early postpartum period. Uncomplicated peptic ulcer does not adversely affect the development of the fetus.
However, some patients may experience an exacerbation. This is most often observed in the first trimester of pregnancy (14.8%) and the third trimester (10.2%), as well as 2-4 weeks before the due date or in the early postpartum period. Uncomplicated peptic ulcer does not adversely affect the development of the fetus.
Treatment of peptic ulcer in pregnant women includes adherence to generally accepted "regime" measures and diet; taking in the usual therapeutic doses of non-absorbable antacids (1 sachet 3 times a day 1 hour after meals and adsorbents 1 sachet 3 times a day 1 hour after meals). If there is no effect, h3-blockers are prescribed (ranitidine 150/300 mg once a night), in case of their insufficient effectiveness, as well as with the development of complications, we can take PPIs (omeprazole 20-40 mg, lansoprazole 30-60 mg, pantoprazole 40 mg). mg in the morning before the first meal). Bismuth preparations are contraindicated for pregnant women. Eradication therapy for H.