How to relieve child congestion
What Kind of Stuff Clears Up a Stuffy Nose?
AddictionAllergies & AsthmaAmbulatoryAudiologyAutismAwardsBC4TeensBehavioral HealthBehind the ScenesBurn CenterCancerCardiologyCenter for Healthy Weight and NutritionCenter for Injury Research and PolicyChild BehaviorChild DevelopmentColorectal and Pelvic ReconstructionCommunity EducationCommunity ResourcesCoronavirusDentistryDermatologyDiseases & ConditionsDiversity and InclusionEndocrinologyENTEpilepsyEverything MattersFertility and Reproductive Health ProgramFundraising EventsGastroenterologyGeneticsGynecologyHematologyHomecareHospiceHospital NewsInfants & NewbornsInfectious DiseaseKids & TeensLaboratory ServicesMake Safe HappenMarathonNeonatologyNephrologyNeurologyNeurosurgeryNew HospitalNICUNutrition & FitnessOccupational TherapyOphthalmologyOrthopedicsOur PatientsOur staffPalliative CareParentingPediatric NewsPharmacyPhysical Therapy - Sports and OrthopedicPlastic SurgeryPopulation HealthPregnancyPrimary CarePsychologyPulmonaryRadiologyReach Out and ReadRehabilitationResearchRheumatologySafety & PreventionSports MedicineSurgical ServicesThe Center for Family Safety and HealingTherapeutic RecreationTherapyTHRIVE ProgramToddlers & PreschoolersUrgent CareUrology
Aaron Barber, AT, ATC, PESAbbie Roth, MWCAbby Orkis, MSW, LSWAdam Ostendorf, MDAdriane Baylis, PhD, CCC-SLPAdrienne M. Flood, CPNP-ACAdvanced Healthcare Provider CouncilAila Co, MDAlaina White, AT, ATCAlana Milton, MDAlana Milton, MDAlecia Jayne, AuDAlena SchuckmannAlessandra Gasior, DOAlex Kemper, MDAlexandra Funk, PharmD, DABATAlexandra Sankovic, MDAlexis Klenke, RD, LDAlice Bass, CPNP-PCAlison PeggAllie DePoyAllison Rowland, AT, ATCAllison Strouse, MS, AT, ATCAmanda E. Graf, MDAmanda GoetzAmanda Smith, RN, BSN, CPNAmanda Sonk, LMTAmanda Whitaker, MDAmber Patterson, MDAmberle Prater, PhD, LPCCAmy Brown Schlegel, MDAmy Coleman, LISWAmy Dunn, MDAmy E. Valasek, MD, MScAmy Fanning, PT, DPTAmy Garee, CPNP-PCAmy Hahn, PhDAmy HessAmy Leber, PhDAmy LeRoy, CCLSAmy Moffett, CPNP-PCAmy Randall-McSorley, MMC, EdD CandidateAmy Thomas, BSN, RN, IBCLCAmy Wahl, APNAnastasia Fischer, MD, FACSMAndala HardyAndrea Brun, CPNP-PCAndrea M. Boerger, MEd, CCC-SLPAndrea Sattler, MDAndrea ShellowAndrew AxelsonAndrew Kroger, MD, MPHAndrew SchwadererAndria Haynes, RNAngela AbenaimAngela Billingslea, LISW-SAnn Pakalnis, MDAnna Lillis, MD, PhDAnnette Haban-BartzAnnie Drapeau, MDAnnie Temple, MS, CCC-SLP, CLCAnnie Truelove, MPHAnthony Audino, MDAnup D.
 Patel, MDAri Rabkin, PhDAriana Hoet, PhDArielle Sheftall, PhDArleen KarczewskiAshlee HallAshleigh Kussman, MDAshley Debeljack, PsyDAshley Ebersole, MDAshley EcksteinAshley Kroon Van DiestAshley M. Davidson, AT, ATC, MSAshley Minnick, MSAH, AT, ATCAshley Overall, FNPAshley Parikh, CPNP-PCAshley Parker MSW, LISW-SAshley Parker, LISW-SAshley Tuisku, CTRSAsuncion Mejias, MD, PhDAurelia Wood, MDBailey Young, DOBecky Corbitt, RNBelinda Mills, MDBenjamin Fields, PhD, MEdBenjamin Kopp, MDBernadette Burke, AT, ATC, MSBeth Martin, RNBeth Villanueva, OTD, OTR/LBethany Uhl, MDBethany Walker, PhDBhuvana Setty, MDBill Kulju, MS, ATBlake SkinnerBonnie Gourley, MSW, LSWBrad Childers, RRT, BSBrandi Cogdill, RN, BSN, CFRN, EMT-PBrandon MorganBreanne L. Bowers, PT, DPT, CHT, CFSTBrendan Boyle, MD, MPHBrian Boe, MDBrian K. Kaspar, PhDBrian Kellogg, MDBriana Crowe, PT, DPT, OCSBrigid Pargeon, MS, MT-BCBrittney Hardin, MOT, OTR/LBrooke Sims, LPCC, ATRCagri Toruner, MDCaitlin Bauer, RD, LDCaitlin TullyCaleb MosleyCallista DammannCallista PoppCami Winkelspecht, PhDCamille Wilson, PhDCanice Crerand, PhDCara Inglis, PsyDCarl H.
Patel, MDAri Rabkin, PhDAriana Hoet, PhDArielle Sheftall, PhDArleen KarczewskiAshlee HallAshleigh Kussman, MDAshley Debeljack, PsyDAshley Ebersole, MDAshley EcksteinAshley Kroon Van DiestAshley M. Davidson, AT, ATC, MSAshley Minnick, MSAH, AT, ATCAshley Overall, FNPAshley Parikh, CPNP-PCAshley Parker MSW, LISW-SAshley Parker, LISW-SAshley Tuisku, CTRSAsuncion Mejias, MD, PhDAurelia Wood, MDBailey Young, DOBecky Corbitt, RNBelinda Mills, MDBenjamin Fields, PhD, MEdBenjamin Kopp, MDBernadette Burke, AT, ATC, MSBeth Martin, RNBeth Villanueva, OTD, OTR/LBethany Uhl, MDBethany Walker, PhDBhuvana Setty, MDBill Kulju, MS, ATBlake SkinnerBonnie Gourley, MSW, LSWBrad Childers, RRT, BSBrandi Cogdill, RN, BSN, CFRN, EMT-PBrandon MorganBreanne L. Bowers, PT, DPT, CHT, CFSTBrendan Boyle, MD, MPHBrian Boe, MDBrian K. Kaspar, PhDBrian Kellogg, MDBriana Crowe, PT, DPT, OCSBrigid Pargeon, MS, MT-BCBrittney Hardin, MOT, OTR/LBrooke Sims, LPCC, ATRCagri Toruner, MDCaitlin Bauer, RD, LDCaitlin TullyCaleb MosleyCallista DammannCallista PoppCami Winkelspecht, PhDCamille Wilson, PhDCanice Crerand, PhDCara Inglis, PsyDCarl H. Backes, MDCarlo Di Lorenzo, MDCarly FawcettCarneshia EdwardsCarol Baumhardt, LMTCarolyn FigiCarrie Rhodes, CPST-I, MTSA, CHESCasey Cottrill, MD, MPHCasey TrimbleCassandra McNabb, RN-BSNCatherine Earlenbaugh, RNCatherine Sinclair, MDCatherine Trimble, FNPCatrina Litzenburg, PhDCharae Keys, MSW, LISW-SCharles Elmaraghy, MDChelsea Britton, MS, RD, LD, CLC Chelsea Kebodeaux, MDChelsie Doster, BSCheryl Boop, MS, OTR/LCheryl G. Baxter, CPNPCheryl Gariepy, MDChet Kaczor, PharmD, MBAChris MarreroChris Smith, RNChristina Ching, MDChristina DayChristine Johnson, MA, CCC-SLPChristine Koterba, PhDChristine Mansfield, PT, DPT, OCS, ATCChristine PrusaChristopher Goettee, PT, DPT, OCSChristopher Iobst, MDChristopher Ouellette, MDChristy Lumpkins, LISW-SCindy IskeClaire Kopko PT, DPT, OCS, NASM-PESCody Hostutler, PhDConnor McDanel, MSW, LSWCorey Rood, MDCorinne Syfers, CCLSCourtney Bishop. PA-CCourtney Brown, MDCourtney Hall, CPNP-PCCourtney Porter, RN, MSCristina Tomatis Souverbielle, MDCrystal MilnerCurt Daniels, MDCynthia Holland-Hall, MD, MPHDana Lenobel, FNPDana Noffsinger, CPNP-ACDane Snyder, MDDaniel Coury, MDDaniel DaJusta, MDDanielle Peifer, PT, DPTDavid A Wessells, PT, MHADavid Axelson, MDDavid Stukus, MDDean Lee, MD, PhDDebbie Terry, NPDeborah Hill, LSWDeborah Zerkle, LMTDeena Chisolm, PhDDeipanjan Nandi, MD MScDenis King, MDDenise EllDennis Cunningham, MDDennis McTigue, DDSDiane LangDominique R.
Backes, MDCarlo Di Lorenzo, MDCarly FawcettCarneshia EdwardsCarol Baumhardt, LMTCarolyn FigiCarrie Rhodes, CPST-I, MTSA, CHESCasey Cottrill, MD, MPHCasey TrimbleCassandra McNabb, RN-BSNCatherine Earlenbaugh, RNCatherine Sinclair, MDCatherine Trimble, FNPCatrina Litzenburg, PhDCharae Keys, MSW, LISW-SCharles Elmaraghy, MDChelsea Britton, MS, RD, LD, CLC Chelsea Kebodeaux, MDChelsie Doster, BSCheryl Boop, MS, OTR/LCheryl G. Baxter, CPNPCheryl Gariepy, MDChet Kaczor, PharmD, MBAChris MarreroChris Smith, RNChristina Ching, MDChristina DayChristine Johnson, MA, CCC-SLPChristine Koterba, PhDChristine Mansfield, PT, DPT, OCS, ATCChristine PrusaChristopher Goettee, PT, DPT, OCSChristopher Iobst, MDChristopher Ouellette, MDChristy Lumpkins, LISW-SCindy IskeClaire Kopko PT, DPT, OCS, NASM-PESCody Hostutler, PhDConnor McDanel, MSW, LSWCorey Rood, MDCorinne Syfers, CCLSCourtney Bishop. PA-CCourtney Brown, MDCourtney Hall, CPNP-PCCourtney Porter, RN, MSCristina Tomatis Souverbielle, MDCrystal MilnerCurt Daniels, MDCynthia Holland-Hall, MD, MPHDana Lenobel, FNPDana Noffsinger, CPNP-ACDane Snyder, MDDaniel Coury, MDDaniel DaJusta, MDDanielle Peifer, PT, DPTDavid A Wessells, PT, MHADavid Axelson, MDDavid Stukus, MDDean Lee, MD, PhDDebbie Terry, NPDeborah Hill, LSWDeborah Zerkle, LMTDeena Chisolm, PhDDeipanjan Nandi, MD MScDenis King, MDDenise EllDennis Cunningham, MDDennis McTigue, DDSDiane LangDominique R. Williams, MD, MPH, FAAP, Dipl ABOMDonna M. Trentel, MSA, CCLSDonna Ruch, PhDDonna TeachDoug WolfDouglas McLaughlin, MDDrew Duerson, MDEd MinerEdward Oberle, MD, RhMSUSEdward Shepherd, MDEileen Chaves, PhDElena CamachoElise Berlan, MDElise DawkinsElizabeth A. Cannon, LPCCElizabeth Cipollone, LPCC-SElizabeth Zmuda, DOEllyn Hamm, MM, MT-BCEmily A. Stuart, MDEmily Decker, MDEmily GetschmanEmma Wysocki, PharmD, RDNEric Butter, PhDEric Leighton, AT, ATCEric Sribnick, MD, PhDErica Domrose, RD, LDEricca L Lovegrove, RD, LDErika RobertsErin Gates, PT, DPTErin Johnson, M.Ed., C.S.C.S.Erin McKnight, MD, MPHErin Shann, BSN, RNErin TebbenFarah W. Brink, MDFatimah MasoodFrances Fei, MDGail Bagwell, DNP, APRN, CNSGail Besner, MDGail Swisher, ATGarey Noritz, MDGary A. Smith, MD, DrPHGeri Hewitt, MDGina Hounam, PhDGina McDowellGina MinotGrace Paul, MDGregory D. Pearson, MDGriffin Stout, MDGuliz Erdem, MDHailey Blosser, MA, CCC-SLPHanna MathessHeather Battles, MDHeather ClarkHeather L. Terry, MSN, RN, FNP-C, CUNPHeather Yardley, PhDHenry SpillerHenry Xiang, MD, MPH, PhDHerman Hundley, MS, AT, ATC, CSCSHilary Michel, MDHiren Patel, MDHolly Deckling, MSSW, LISWHoma Amini, DDS, MPH, MSHoward Jacobs, MDHunter Wernick, DOIbrahim Khansa, MDIhuoma Eneli, MDIlana Moss, PhDIlene Crabtree, PTIrene Mikhail, MDIrina Buhimschi, MDIvor Hill, MDJackie Cronau, RN, CWOCNJacqueline Wynn, PhD, BCBA-DJacquelyn Doxie King, PhDJaime-Dawn Twanow, MDJaimie D.
Williams, MD, MPH, FAAP, Dipl ABOMDonna M. Trentel, MSA, CCLSDonna Ruch, PhDDonna TeachDoug WolfDouglas McLaughlin, MDDrew Duerson, MDEd MinerEdward Oberle, MD, RhMSUSEdward Shepherd, MDEileen Chaves, PhDElena CamachoElise Berlan, MDElise DawkinsElizabeth A. Cannon, LPCCElizabeth Cipollone, LPCC-SElizabeth Zmuda, DOEllyn Hamm, MM, MT-BCEmily A. Stuart, MDEmily Decker, MDEmily GetschmanEmma Wysocki, PharmD, RDNEric Butter, PhDEric Leighton, AT, ATCEric Sribnick, MD, PhDErica Domrose, RD, LDEricca L Lovegrove, RD, LDErika RobertsErin Gates, PT, DPTErin Johnson, M.Ed., C.S.C.S.Erin McKnight, MD, MPHErin Shann, BSN, RNErin TebbenFarah W. Brink, MDFatimah MasoodFrances Fei, MDGail Bagwell, DNP, APRN, CNSGail Besner, MDGail Swisher, ATGarey Noritz, MDGary A. Smith, MD, DrPHGeri Hewitt, MDGina Hounam, PhDGina McDowellGina MinotGrace Paul, MDGregory D. Pearson, MDGriffin Stout, MDGuliz Erdem, MDHailey Blosser, MA, CCC-SLPHanna MathessHeather Battles, MDHeather ClarkHeather L. Terry, MSN, RN, FNP-C, CUNPHeather Yardley, PhDHenry SpillerHenry Xiang, MD, MPH, PhDHerman Hundley, MS, AT, ATC, CSCSHilary Michel, MDHiren Patel, MDHolly Deckling, MSSW, LISWHoma Amini, DDS, MPH, MSHoward Jacobs, MDHunter Wernick, DOIbrahim Khansa, MDIhuoma Eneli, MDIlana Moss, PhDIlene Crabtree, PTIrene Mikhail, MDIrina Buhimschi, MDIvor Hill, MDJackie Cronau, RN, CWOCNJacqueline Wynn, PhD, BCBA-DJacquelyn Doxie King, PhDJaime-Dawn Twanow, MDJaimie D. Nathan, MD, FACSJames Murakami, MDJames Popp, MDJames Ruda, MDJameson Mattingly, MDJamie Macklin, MDJamie ReedyJane AbelJanelle Huefner, MA, CCC-SLPJanice M. Moreland, CPNP-PC, DNPJanice Townsend, DDS, MSJared SylvesterJason JacksonJason P. Garee, PhDJaysson EicholtzJean Hruschak, MA, CCC/SLPJeff Sydes, CSCSJeffery Auletta, MDJeffrey Bennett, MD, PhDJeffrey Hoffman, MDJeffrey Leonard, MDJen Campbell, PT, MSPTJena HeckJenn Gonya, PhDJennie Aldrink, MDJennifer Borda, PT, DPTJennifer HofherrJennifer LockerJennifer PrinzJennifer Reese, PsyDJennifer Smith, MS, RD, CSP, LD, LMTJennifer Walton, MD, MPH, FAAPJenny Worthington, PT, DPTJerry R. Mendell, MDJessalyn Mayer, MSOT, OTR/LJessica Bailey, PsyDJessica Bogacik, MS, MT-BCJessica Bowman, MDJessica BrockJessica Bullock, MA/CCC-SLPJessica Buschmann, RDJessica Scherr, PhDJim O’Shea OT, MOT, CHTJoan Fraser, MSW, LISW-SJohn Ackerman, PhDJohn Caballero, PT, DPT, CSCSJohn Kovalchin, MDJonathan D. Thackeray, MDJonathan Finlay, MB, ChB, FRCPJonathan M.
Nathan, MD, FACSJames Murakami, MDJames Popp, MDJames Ruda, MDJameson Mattingly, MDJamie Macklin, MDJamie ReedyJane AbelJanelle Huefner, MA, CCC-SLPJanice M. Moreland, CPNP-PC, DNPJanice Townsend, DDS, MSJared SylvesterJason JacksonJason P. Garee, PhDJaysson EicholtzJean Hruschak, MA, CCC/SLPJeff Sydes, CSCSJeffery Auletta, MDJeffrey Bennett, MD, PhDJeffrey Hoffman, MDJeffrey Leonard, MDJen Campbell, PT, MSPTJena HeckJenn Gonya, PhDJennie Aldrink, MDJennifer Borda, PT, DPTJennifer HofherrJennifer LockerJennifer PrinzJennifer Reese, PsyDJennifer Smith, MS, RD, CSP, LD, LMTJennifer Walton, MD, MPH, FAAPJenny Worthington, PT, DPTJerry R. Mendell, MDJessalyn Mayer, MSOT, OTR/LJessica Bailey, PsyDJessica Bogacik, MS, MT-BCJessica Bowman, MDJessica BrockJessica Bullock, MA/CCC-SLPJessica Buschmann, RDJessica Scherr, PhDJim O’Shea OT, MOT, CHTJoan Fraser, MSW, LISW-SJohn Ackerman, PhDJohn Caballero, PT, DPT, CSCSJohn Kovalchin, MDJonathan D. Thackeray, MDJonathan Finlay, MB, ChB, FRCPJonathan M. Grischkan, MDJonathan Napolitano, MDJoshua Prudent, MDJoshua Watson, MDJulee Eing, CRA, RT(R)Julia Colman, MOT, OTR/LJulie ApthorpeJulie Lange, MDJulie Leonard, MD, MPHJulie Racine, PhDJulie Samora, MDJustin Indyk, MD, PhDKady LacyKaitrin Kramer, DDS, MS, PhDKaleigh Hague, MA, MT-BCKaleigh MatesickKamilah Twymon, LPCC-SKara Malone, MDKara Miller, OTR/LKaren A. Diefenbach, MDKaren Allen, MDKaren Days, MBAKaren Rachuba, RD, LD, CLCKari A. Meeks, OTKari Cardiff, ODKari Dubro, MS, RD, LD, CWWSKari Phang, MDKarla Vaz, MDKaryn L. Kassis, MD, MPHKasey Strothman, MDKatherine Deans, MDKatherine McCracken, MD FACOGKathleen (Katie) RoushKathryn Blocher, CPNP-PCKathryn J. Junge, RN, BSNKathryn Obrynba, MDKatia Camille Halabi, MDKatie Brind'Amour, MSKatie DonovanKatie Thomas, APRKatrina Hall, MA, CCLSKatrina Ruege, LPCC-SKatya Harfmann, MDKayla Zimpfer, PCCKaylan Guzman Schauer, LPCC-SKeli YoungKelley SwopeKelli Dilver, PT, DPTKelly AbramsKelly BooneKelly HustonKelly J. Kelleher, MDKelly McNally, PhDKelly N.
Grischkan, MDJonathan Napolitano, MDJoshua Prudent, MDJoshua Watson, MDJulee Eing, CRA, RT(R)Julia Colman, MOT, OTR/LJulie ApthorpeJulie Lange, MDJulie Leonard, MD, MPHJulie Racine, PhDJulie Samora, MDJustin Indyk, MD, PhDKady LacyKaitrin Kramer, DDS, MS, PhDKaleigh Hague, MA, MT-BCKaleigh MatesickKamilah Twymon, LPCC-SKara Malone, MDKara Miller, OTR/LKaren A. Diefenbach, MDKaren Allen, MDKaren Days, MBAKaren Rachuba, RD, LD, CLCKari A. Meeks, OTKari Cardiff, ODKari Dubro, MS, RD, LD, CWWSKari Phang, MDKarla Vaz, MDKaryn L. Kassis, MD, MPHKasey Strothman, MDKatherine Deans, MDKatherine McCracken, MD FACOGKathleen (Katie) RoushKathryn Blocher, CPNP-PCKathryn J. Junge, RN, BSNKathryn Obrynba, MDKatia Camille Halabi, MDKatie Brind'Amour, MSKatie DonovanKatie Thomas, APRKatrina Hall, MA, CCLSKatrina Ruege, LPCC-SKatya Harfmann, MDKayla Zimpfer, PCCKaylan Guzman Schauer, LPCC-SKeli YoungKelley SwopeKelli Dilver, PT, DPTKelly AbramsKelly BooneKelly HustonKelly J. Kelleher, MDKelly McNally, PhDKelly N. Day, CPNP-PCKelly Pack, LISW-SKelly Tanner,PhD, OTR/L, BCPKelly Wesolowski, PsyDKelly Wise, PharmDKent Williams, MDKevin Bosse, PhDKevin Klingele, MDKim Bjorklund, MDKim Hammersmith, DDS, MPH, MSKimberly Bates, MDKimberly Sisto, PT, DPT, SCSKimberly Van Camp, PT, DPT, SCSKirk SabalkaKris Jatana, MD, FAAPKrista Winner, AuD, CCC-AKristen Armbrust, LISW-SKristen Cannon, MDKristen E. Beck, MDKristen Martin, OTR/LKristi Roberts, MS MPHKristina Booth, MSN, CFNPKristina Reber, MDKristol Das, MDKyle DavisLance Governale, MDLara McKenzie, PhD, MALaura Brubaker, BSN, RNLaura Dattner, MALaura Martin, MDLaurel Biever, LPCLauren Durinka, AuDLauren Garbacz, PhDLauren Justice, OTR/L, MOTLauren Madhoun, MS, CCC-SLPLauryn Rozum, MS, CCLSLeah Middelberg, MDLee Hlad, DPMLeena Nahata, MDLelia Emery, MT-BCLeslie Appiah, MDLinda Stoverock, DNP, RN NEA-BCLindsay Kneen, MDLindsay Pietruszewski, PT, DPTLindsay SchwartzLindsey Vater, PsyDLisa GoldenLisa Halloran, CNPLisa M. Humphrey, MDLogan Blankemeyer, MA, CCC-SLPLori Grisez PT, DPTLorraine Kelley-QuonLouis Bezold, MDLourdes Hill, LPCC-S Lubna Mazin, PharmDLuke Tipple, MS, CSCSLynda Wolfe, PhDLyndsey MillerLynn RosenthalLynne Ruess, MDMaggy Rule, MS, AT, ATCMahmoud Kallash, MDManmohan K Kamboj, MDMarc P.
Day, CPNP-PCKelly Pack, LISW-SKelly Tanner,PhD, OTR/L, BCPKelly Wesolowski, PsyDKelly Wise, PharmDKent Williams, MDKevin Bosse, PhDKevin Klingele, MDKim Bjorklund, MDKim Hammersmith, DDS, MPH, MSKimberly Bates, MDKimberly Sisto, PT, DPT, SCSKimberly Van Camp, PT, DPT, SCSKirk SabalkaKris Jatana, MD, FAAPKrista Winner, AuD, CCC-AKristen Armbrust, LISW-SKristen Cannon, MDKristen E. Beck, MDKristen Martin, OTR/LKristi Roberts, MS MPHKristina Booth, MSN, CFNPKristina Reber, MDKristol Das, MDKyle DavisLance Governale, MDLara McKenzie, PhD, MALaura Brubaker, BSN, RNLaura Dattner, MALaura Martin, MDLaurel Biever, LPCLauren Durinka, AuDLauren Garbacz, PhDLauren Justice, OTR/L, MOTLauren Madhoun, MS, CCC-SLPLauryn Rozum, MS, CCLSLeah Middelberg, MDLee Hlad, DPMLeena Nahata, MDLelia Emery, MT-BCLeslie Appiah, MDLinda Stoverock, DNP, RN NEA-BCLindsay Kneen, MDLindsay Pietruszewski, PT, DPTLindsay SchwartzLindsey Vater, PsyDLisa GoldenLisa Halloran, CNPLisa M. Humphrey, MDLogan Blankemeyer, MA, CCC-SLPLori Grisez PT, DPTLorraine Kelley-QuonLouis Bezold, MDLourdes Hill, LPCC-S Lubna Mazin, PharmDLuke Tipple, MS, CSCSLynda Wolfe, PhDLyndsey MillerLynn RosenthalLynne Ruess, MDMaggy Rule, MS, AT, ATCMahmoud Kallash, MDManmohan K Kamboj, MDMarc P. Michalsky, MDMarcel J. Casavant, MDMarci Johnson, LISW-SMarcie RehmarMarco Corridore, MDMargaret Bassi, OTR/LMaria HaghnazariMaria Vegh, MSN, RN, CPNMarissa Condon, BSN, RNMarissa E. Larouere, MBA, BSN, RNMark E. Galantowicz, MDMark Smith, MS RT R (MR), ABMP PhysicistMarnie Wagner, MDMary Ann Abrams, MD, MPHMary Fristad, PhD, ABPPMary Kay SharrettMary Shull, MDMatthew Washam, MD, MPHMeagan Horn, MAMegan Brundrett, MDMegan Dominik, OTR/LMegan FrancisMegan Letson, MD, M.EdMeghan Cass, PT, DPTMeghan Fisher, BSN, RNMeika Eby, MDMelanie Fluellen, LPCCMelanie Luken, LISW-SMelissa and Mikael McLarenMelissa McMillen, CTRSMelissa Winterhalter, MDMeredith Merz Lind, MDMichael Flores, PhDMichael T. Brady, MDMichelle Ross, MHA, RD, LD, ALCMike Patrick, MDMindy Deno, PT, DPTMitch Ellinger, CPNP-PCMolly Dienhart, MDMolly Gardner, PhDMonica Ardura, DOMonica EllisMonique Goldschmidt, MDMotao Zhu, MD, MS, PhDMurugu Manickam, MDNancy AuerNancy Cunningham, PsyDNancy Wright, BS, RRT, RCP, AE-C Naomi Kertesz, MDNatalie DeBaccoNatalie I.
Michalsky, MDMarcel J. Casavant, MDMarci Johnson, LISW-SMarcie RehmarMarco Corridore, MDMargaret Bassi, OTR/LMaria HaghnazariMaria Vegh, MSN, RN, CPNMarissa Condon, BSN, RNMarissa E. Larouere, MBA, BSN, RNMark E. Galantowicz, MDMark Smith, MS RT R (MR), ABMP PhysicistMarnie Wagner, MDMary Ann Abrams, MD, MPHMary Fristad, PhD, ABPPMary Kay SharrettMary Shull, MDMatthew Washam, MD, MPHMeagan Horn, MAMegan Brundrett, MDMegan Dominik, OTR/LMegan FrancisMegan Letson, MD, M.EdMeghan Cass, PT, DPTMeghan Fisher, BSN, RNMeika Eby, MDMelanie Fluellen, LPCCMelanie Luken, LISW-SMelissa and Mikael McLarenMelissa McMillen, CTRSMelissa Winterhalter, MDMeredith Merz Lind, MDMichael Flores, PhDMichael T. Brady, MDMichelle Ross, MHA, RD, LD, ALCMike Patrick, MDMindy Deno, PT, DPTMitch Ellinger, CPNP-PCMolly Dienhart, MDMolly Gardner, PhDMonica Ardura, DOMonica EllisMonique Goldschmidt, MDMotao Zhu, MD, MS, PhDMurugu Manickam, MDNancy AuerNancy Cunningham, PsyDNancy Wright, BS, RRT, RCP, AE-C Naomi Kertesz, MDNatalie DeBaccoNatalie I. Rine, PharmD, BCPS, BCCCPNatalie Powell, LPCC-S, LICDC-CSNatalie Rose, BSN, RNNathalie Maitre, MD, PhDNationwide Children's HospitalNationwide Children's Hospital Behavioral Health ExpertsNeetu Bali, MD, MPHNehal Parikh, DO, MSNichole Mayer, OTR/L, MOTNicole Caldwell, MDNicole Dempster, PhDNicole Greenwood, MDNicole Parente, LSWNicole Powell, PsyD, BCBA-DNina WestNkeiruka Orajiaka, MBBSOctavio Ramilo, MDOliver Adunka, MD, FACSOlivia Stranges, CPNP-PCOlivia Thomas, MDOmar Khalid, MD, FAAP, FACCOnnalisa Nash, CPNP-PCOula KhouryPaige Duly, CTRSParker Huston, PhDPatrick C. Walz, MDPatrick Queen, BSN, RNPedro Weisleder, MDPeter Minneci, MDPeter White, PhDPitty JenningsPreeti Jaggi, MDPriyal Patel, DORachael Morocco-Zanotti, DORachel D’Amico, MDRachel Schrader, CPNP-PCRachel Tyson, LSWRajan Thakkar, MDRaymond Troy, MDRebecca Fisher, PTRebecca Hicks, CCLSRebecca Lewis, AuD, CCC-ARebecca M. Romero, RD, LD, CLC Reggie Ash Jr.Reno Ravindran, MDRichard Kirschner, MDRichard Wood, MDRobert A. Kowatch, MD, Ph.
Rine, PharmD, BCPS, BCCCPNatalie Powell, LPCC-S, LICDC-CSNatalie Rose, BSN, RNNathalie Maitre, MD, PhDNationwide Children's HospitalNationwide Children's Hospital Behavioral Health ExpertsNeetu Bali, MD, MPHNehal Parikh, DO, MSNichole Mayer, OTR/L, MOTNicole Caldwell, MDNicole Dempster, PhDNicole Greenwood, MDNicole Parente, LSWNicole Powell, PsyD, BCBA-DNina WestNkeiruka Orajiaka, MBBSOctavio Ramilo, MDOliver Adunka, MD, FACSOlivia Stranges, CPNP-PCOlivia Thomas, MDOmar Khalid, MD, FAAP, FACCOnnalisa Nash, CPNP-PCOula KhouryPaige Duly, CTRSParker Huston, PhDPatrick C. Walz, MDPatrick Queen, BSN, RNPedro Weisleder, MDPeter Minneci, MDPeter White, PhDPitty JenningsPreeti Jaggi, MDPriyal Patel, DORachael Morocco-Zanotti, DORachel D’Amico, MDRachel Schrader, CPNP-PCRachel Tyson, LSWRajan Thakkar, MDRaymond Troy, MDRebecca Fisher, PTRebecca Hicks, CCLSRebecca Lewis, AuD, CCC-ARebecca M. Romero, RD, LD, CLC Reggie Ash Jr.Reno Ravindran, MDRichard Kirschner, MDRichard Wood, MDRobert A. Kowatch, MD, Ph. D.Robert Hoffman, MDRochelle Krouse, CTRSRohan Henry, MD, MSRose Ayoob, MDRose Schroedl, PhDRosemary Martoma, MDRoss Maltz, MDRyan Ingley AT, ATCSamanta Boddapati, PhDSamantha MaloneSammy CygnorSandra C. Kim, MDSara Bentley, MT-BCSara Bode, MDSara Breidigan, MS, AT, ATCSara N. Smith, MSN, APRNSara O'Rourke, MOT, OTR/L, Clinical LeadSara Schroder, MDSarah A. Denny, MDSarah Cline, CRA, RT(R)Sarah Driesbach, CPN, APNSarah GreenbergSarah Hastie, BSN, RNC-NIC Sarah Keim, PhDSarah MyersSarah O'Brien, MDSarah SaxbeSarah Schmidt, LISW-SSarah ScottSarah TraceySarah VerLee, PhDSasigarn Bowden, MDSatya Gedela, MD, MRCP(UK)Scott Coven, DO, MPHScott Hickey, MDSean EingSean Rose, MDSeth Alpert, MDShalini C. Reshmi, PhD, FACMGShana Moore, MA, CCC-AShannon Reinhart, LISW-SShari UncapherSharon Wrona, DNP, PNP, PMHSShaun Coffman PT, DPT, OCSShawn Pitcher, BS, RD, USAWShawNaye Scott-MillerShea SmoskeSheena PaceSheila GilesShelly BrackmanSimon Lee, MDSini James, MDStacy Ardoin, MDStacy Whiteside APRN, MS, CPNP-AC/PC, CPONStefanie Bester, MDStefanie Hirota, OTR/LStephanie Burkhardt, MPH, CCRCStephanie CannonStephanie Santoro, MDStephanie Vyrostek BSN, RNStephen Hersey, MDSteve Allen, MDSteven C.
D.Robert Hoffman, MDRochelle Krouse, CTRSRohan Henry, MD, MSRose Ayoob, MDRose Schroedl, PhDRosemary Martoma, MDRoss Maltz, MDRyan Ingley AT, ATCSamanta Boddapati, PhDSamantha MaloneSammy CygnorSandra C. Kim, MDSara Bentley, MT-BCSara Bode, MDSara Breidigan, MS, AT, ATCSara N. Smith, MSN, APRNSara O'Rourke, MOT, OTR/L, Clinical LeadSara Schroder, MDSarah A. Denny, MDSarah Cline, CRA, RT(R)Sarah Driesbach, CPN, APNSarah GreenbergSarah Hastie, BSN, RNC-NIC Sarah Keim, PhDSarah MyersSarah O'Brien, MDSarah SaxbeSarah Schmidt, LISW-SSarah ScottSarah TraceySarah VerLee, PhDSasigarn Bowden, MDSatya Gedela, MD, MRCP(UK)Scott Coven, DO, MPHScott Hickey, MDSean EingSean Rose, MDSeth Alpert, MDShalini C. Reshmi, PhD, FACMGShana Moore, MA, CCC-AShannon Reinhart, LISW-SShari UncapherSharon Wrona, DNP, PNP, PMHSShaun Coffman PT, DPT, OCSShawn Pitcher, BS, RD, USAWShawNaye Scott-MillerShea SmoskeSheena PaceSheila GilesShelly BrackmanSimon Lee, MDSini James, MDStacy Ardoin, MDStacy Whiteside APRN, MS, CPNP-AC/PC, CPONStefanie Bester, MDStefanie Hirota, OTR/LStephanie Burkhardt, MPH, CCRCStephanie CannonStephanie Santoro, MDStephanie Vyrostek BSN, RNStephen Hersey, MDSteve Allen, MDSteven C. Matson, MDSteven Ciciora, MDSteven CuffSuellen Sharp, OTR/L, MOTSurlina AsamoaSusan Colace, MDSusan Creary, MDSwaroop Pinto, MDTabatha BallardTabbetha GrecoTabi Evans, PsyDTabitha Jones-McKnight, DOTahagod Mohamed, MDTamara MappTammi Young-Saleme, PhDTaylor Hartlaub, MD, MPHTenelle JonesTerry Barber, MDTerry Bravender, MD, MPHTerry Laurila, MS, RPhTheresa Miller, BA, RRT, RCP, AE-C, CPFTThomas Pommering, DOTiasha Letostak, PhDTiffanie Ryan, BCBA Tim RobinsonTim Smith, MDTimothy Cripe, MD, PhDTimothy Landers PhD RN APRN-CNP CIC FAANTracey L. Sisk, RN, BSN, MHATracie Steinke RD, LD, CDETracy Mehan, MATravis Gallagher, ATTrevor MillerTria Shadeed, NNPTyanna Snider, PsyDTyler Congrove, ATValencia Walker, MD, MPH, FAAPVanessa Shanks, MD, FAAPVenkata Rama Jayanthi, MDVidu Garg, MDVidya Raman, MDW. Garrett Hunt, MDWalter Samora, MDWarren D. Lo, MDWendy Anderson, MDWendy Cleveland, MA, LPCC-SWhitney McCormick, CTRSWhitney Raglin Bignall, PhDWilliam Cotton, MDWilliam J. Barson, MDWilliam Ray, PhDWilliam W.
Matson, MDSteven Ciciora, MDSteven CuffSuellen Sharp, OTR/L, MOTSurlina AsamoaSusan Colace, MDSusan Creary, MDSwaroop Pinto, MDTabatha BallardTabbetha GrecoTabi Evans, PsyDTabitha Jones-McKnight, DOTahagod Mohamed, MDTamara MappTammi Young-Saleme, PhDTaylor Hartlaub, MD, MPHTenelle JonesTerry Barber, MDTerry Bravender, MD, MPHTerry Laurila, MS, RPhTheresa Miller, BA, RRT, RCP, AE-C, CPFTThomas Pommering, DOTiasha Letostak, PhDTiffanie Ryan, BCBA Tim RobinsonTim Smith, MDTimothy Cripe, MD, PhDTimothy Landers PhD RN APRN-CNP CIC FAANTracey L. Sisk, RN, BSN, MHATracie Steinke RD, LD, CDETracy Mehan, MATravis Gallagher, ATTrevor MillerTria Shadeed, NNPTyanna Snider, PsyDTyler Congrove, ATValencia Walker, MD, MPH, FAAPVanessa Shanks, MD, FAAPVenkata Rama Jayanthi, MDVidu Garg, MDVidya Raman, MDW. Garrett Hunt, MDWalter Samora, MDWarren D. Lo, MDWendy Anderson, MDWendy Cleveland, MA, LPCC-SWhitney McCormick, CTRSWhitney Raglin Bignall, PhDWilliam Cotton, MDWilliam J. Barson, MDWilliam Ray, PhDWilliam W. Long, MD
Long, MD
14 Things to Try at Home for Your Kids’ Nasal Congestion │ Vicks Sinex
Tips to Keep Your Kid Comfortable While Dealing With Nasal Congestion
5. Keep your child hydrated
Your child may find it difficult to blow the thick mucus from their stuffy nose out, and frequent blowing can dry out their nasal passages. One way to keep nasal tissues moist is to keep your child hydrated. Give lots of water and encourage drinking by handing over a water bottle. Or treat them with 100% fruit popsicles either made at home or from your grocery store. Your child may even find them more appealing than water. Keep away from drinks containing caffeine, like soda, because they may worsen dehydration.
6. Add a humidifier to your child’s room
A cool-mist humidifier works by spraying mist into the surrounding area to make the air moist. A humidifier helps to prevent nostril dryness and thins out the mucus in the nose. Place it close to your child but not within reach. Also, be sure to regularly clean the humidifier daily to prevent bacteria or mold from growing in it.3
Place it close to your child but not within reach. Also, be sure to regularly clean the humidifier daily to prevent bacteria or mold from growing in it.3
7. Breathe in soothing Vicks Vapors with Vicks Non-Medicated Children’s VapoPatch
Give your child a calm, soothing environment to keep them comfortable. One way to do this is to use Vicks Non-Medicated Children’s VapoPatch. It provides soothing Vicks vapors in an easy-to-use aromatherapy patch. All you need to do is to peel, apply on their shirt, and let your child breathe in vapors that can soothe your child’s senses.
8. Let warm chicken soup work its wonders
Nothing says ‘sick day’ more than a chicken soup. Serve two generous bowls of chicken soup—one for you, and one for your stuffed-up kid.
9. Use a nasal aspirator to remove mucus
For infants, aspirators or bulb syringes can help remove mucus and provide comfort, especially because infants don’t yet know how to blow their noses. Bulb syringes are pretty straightforward to use. You squeeze out the air from the bulb syringe to make a vacuum, keep it squeezed while inserting it into your child’s nose and release it to suction out the mucus. Your baby will sleep better and more comfortably as a result.
Bulb syringes are pretty straightforward to use. You squeeze out the air from the bulb syringe to make a vacuum, keep it squeezed while inserting it into your child’s nose and release it to suction out the mucus. Your baby will sleep better and more comfortably as a result.
10. Use a nose ointment for dryness
Your kid may be blowing their nose constantly, trying to relieve their stuffy nose. This can make the skin around their nostrils dry and irritated. If your child is older than 6, Sinex Nasal Balm can heal and soothe the dry skin around their nose through intense moisturization. Rub a little amount on the dry skin around your child’s nose.
11. Check the pantry for honey if your child starts coughing
Lots of mucus from a stuffy nose can add coughing to your kid’s symptoms, too. Parents looking for a natural option can check the pantry for honey.4 It’s important to note, though, that this is not appropriate for children under a year old. The CDC recommends that you do not give honey to a child younger than 12 months. 5
5
12 Give them a long, warm bath
Get the bathroom steamy and get your child in the bath. Steam can help hydrate your child’s nasal passages. It travels into the nose and thins out the mucus. Having a warm bath at night will also signal to child’s body to wind down for bedtime.
13. Make sure they eat a balanced diet
Lots of kids prefer to pass on the veggies at dinnertime. But it’s important to give your child a balanced diet—with all nutrients they need to support their little body's growth and development. Blend or puree veggies into your kids’ favorite dishes, so that even when they’re fussing with a stuffy nose, they’re still eating a balanced diet.
14. Extra snuggles
Kids love cuddles! Sometimes the best home remedy is a good cuddle. Kids just want to feel loved and comforted when they’re feeling sick. Cuddling will calm your child, and if they’re calmer, they can rest and feel better or breathe easier. Those extra cuddles are so worth it!
Persistent nasal congestion in a child: what to give for a runny nose if the nose is blocked
Co-author, editor and medical expert - Alexander Alekseevich Maksimov.
Last updated: 11/24/2022
Views: 349,157.
Average reading time: 5 minutes.
Contents:
Causes of the disease
How to relieve nasal congestion in a child
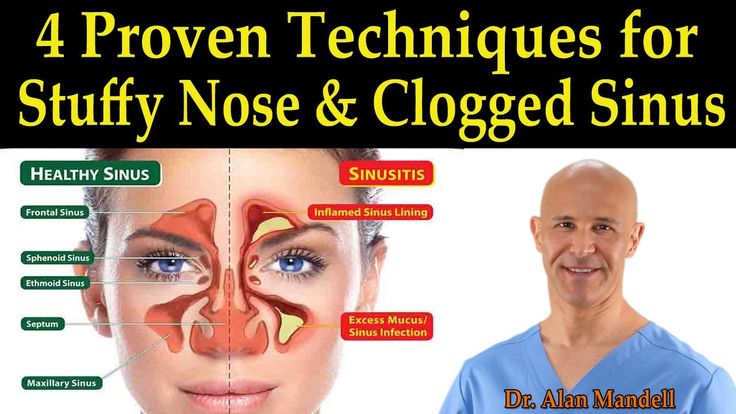
Parents often face the problem of difficulty in nasal breathing in babies 3.4 due to mucosal edema 4 . Nasal congestion in a child may also occur without signs of a runny nose 5 . Such a state not only leads to a deterioration in well-being and a bad mood, but also causes various consequences 3,4,7 . When the nose does not breathe, the child's sleep 3.7 and appetite are disturbed 3.4 , there is a threat of inflammation of the pharynx and bronchi due to inhalation of cold air through the mouth 4 . Babies can develop life-threatening sleep apnea 9 . Therefore, it is necessary to remove nasal congestion in a child, including for safety reasons.
Up to content
Causes of the disease
Currently, the most common causes of a runny nose with nasal congestion in a child are acute respiratory infections 2 and allergic reactions 8 . Enlargement of the adenoids and anomalies in the structure of the nose can also prevent the child from breathing normally 1 . nine0003
Enlargement of the adenoids and anomalies in the structure of the nose can also prevent the child from breathing normally 1 . nine0003
Predisposing factors for the appearance of nasal congestion are: 2
- hereditary burden for allergies 21 ;
- the presence of any type of allergy in the child himself 2.7 ;
- adverse environmental conditions 6.21 : living near an industrial area or highways, passive smoking 21 (when a child inhales tobacco smoke when adults smoke), excessive dryness of the air in the room 4 ;
- frequent irrational antibiotic therapy, which disrupts the composition of the microflora on the mucous membrane and weakens the immune system 13 ;
- artificial feeding 12 ;
- recurring viral infections 4.7 in the first 3 years of life 3 ;
- frequent unreasonable use of various drugs and mineral-vitamin complexes, which are often used without a doctor's prescription 6 ;
- foreign bodies 4.
 7 , due to which the lumen of the nasal passages narrows and the mucous membrane can swell 4 .
7 , due to which the lumen of the nasal passages narrows and the mucous membrane can swell 4 .
Up to content
How to relieve nasal congestion in a child
Even if nasal congestion does not occur for the first time, it is necessary to consult a doctor before starting treatment to find out the cause of the disease 4,8 . Allergic rhinitis and viral infection require different treatment regimens, and only a specialist will be able to quickly recognize the nature of the existing disorders 4.7 .
Nasal wash 3,4,12 . Can be used for any kind of runny nose 12 . This simple and affordable procedure helps to cleanse the mucous membrane of accumulated inflammatory secretions and microorganisms, reduce its swelling 3,4,12 . For washing use saline solutions 3 , sterile sea water 4 , antiseptic and anti-inflammatory agents 12 .
Inhalations 14 . For the treatment of nasal congestion in a child, it is allowed to use warm inhalations 14.15 . You can breathe over hot decoctions of medicinal plants 14 or use essential oils added to the water 15 . Even ordinary steam often helps to cope with nasal congestion with a runny nose in a child 14 . During inhalation, inflamed tissues are gently warmed up, mucus is liquefied, swelling is reduced, some pathogens are destroyed 14.15 . After this treatment, empty the nose by using an aspirator or by asking the child to blow his nose 3 .
Warming ointments 17 . In addition to other products, you can use warming ointments with essential oils. They are smeared on the feet, temples, bridge of the nose and wings of the nose 17 .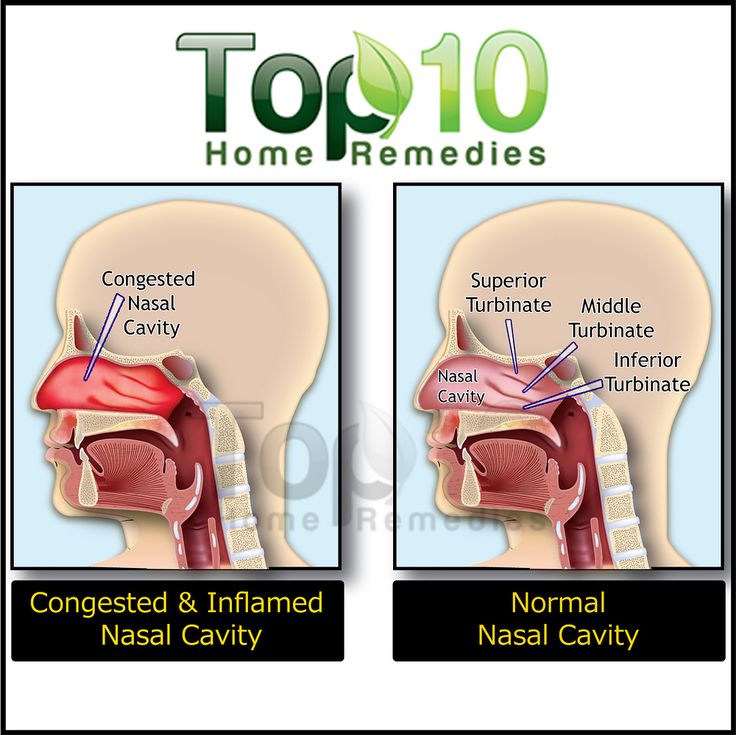
Acupressure 18.19 . This method is based on the acupuncture effect on certain points on the human body 18 . It is used to relieve nasal congestion in children and adults 19 . Essential oils are used to enhance the effect of acupressure. 22
Nasal drops and sprays. For viral respiratory diseases and allergic rhinitis, the treatment regimen includes the use of the latest generation of antihistamines 8 in the form of nasal drops and sprays 20 . They have a local effect and have a small number of contraindications 8 . Special products for children of the TIZIN ® line help to cope with congestion, facilitating nasal breathing and improving well-being. TIZIN ® Alergy contains antihistamines and is used in the treatment of hay fever and allergic rhinitis 11 . Hyaluronic acid, which is part of TIZIN ® Expert for Children, additionally moisturizes the nasal mucosa and contributes to its speedy recovery 10 .
The information in this article is for reference only and does not replace professional medical advice. For diagnosis and treatment, contact a qualified specialist.
See also:
Children's runny nose
Runny nose preparations for children
how to remove and treat at home
Often the nose does not breathe due to a cold or an allergy, but other reasons are possible. In any case, nasal congestion should not be ignored, as a serious diagnosis may be hidden here. To avoid negative consequences for the health of the child in the future, it is necessary to take measures appropriate to the problem. And for this you need to understand what factors affect the nasal mucosa and lead to the inability to breathe normally through the nose. nine0003
What you need to know about nasal congestion in a child
| Associated with cough | With a runny nose and nasal congestion, postnasal drip can occur: when a large amount of mucus accumulates, which does not go out, but flows down the back of the throat. This can cause coughing or throat discomfort (1). This can cause coughing or throat discomfort (1). |
| Nasal congestion can lead to other serious problems | If you have difficulty breathing through your nose, your hearing may be impaired and language development may be delayed. If the mucus clogs the passage between the nose and the ear, an ear infection and pain can result. Severe congestion keeps baby awake (1) |
| In infants, the runny nose is more severe than in older children | In infants, the small vertical size of the nasal cavity is narrow, so even with a slight swelling of the mucous membrane, nasal breathing is disturbed. The infection quickly passes into the nasopharynx, ear, bronchi and lungs. The younger the child, the higher the chance of complications (2) |
| Nasal congestion without mucus secretion can be a symptom of a dangerous disease | If a runny nose is ignored or treated incorrectly, atrophic rhinitis can develop. In this case, the nasal mucosa becomes thinner, the nerve endings and blood vessels in the nasal passages are affected. And this is fraught with a decrease in protective functions against viruses and bacteria And this is fraught with a decrease in protective functions against viruses and bacteria |
Types of nasal congestion in a child
Congestion in a child can occur in different ways. Sometimes it does not last long, but it can be permanent. In some cases, nasal congestion is accompanied by mucus discharge, in others there is no discharge from the nose. How the situations differ and what additional symptoms are possible, we will consider below.
Congestion without snot
Discharge from the nose may not be in the following cases:
- vasomotor rhinitis - as a result of an infection or on the background of an allergy; nine0061
- constant exposure to irritants on the nasal mucosa: poor ecology and polluted air, passive smoking;
- foreign body in nose;
- deviated septum;
- heart and circulation problems;
- long-term use of nasal vasoconstrictors.
Congestion with a runny nose
If a child is ill with SARS, then in addition to congestion, there will definitely be discharge from the nose. In this way, the body tries to get rid of viruses. The exception is the flu, in which a runny nose appears no earlier than 2-3 days. In the first days, only severe fever, headache and muscle aches are observed. nine0003
In this way, the body tries to get rid of viruses. The exception is the flu, in which a runny nose appears no earlier than 2-3 days. In the first days, only severe fever, headache and muscle aches are observed. nine0003
Severe nasal congestion
Severe nasal congestion is more common in allergic reactions. In such cases, breathing is difficult not because of the accumulated mucus, but because of the swelling of the mucous membrane caused by the allergen. This is usually accompanied by repeated sneezing. If such congestion is observed often, it is necessary to consult an allergist. The doctor will determine the cause, prescribe tests to identify the allergen and appropriate treatment.
Congestion without fever
Nasal congestion can be with SARS and without fever. This does not mean that immunity is weak, but depends on the virus that has entered the body. The rise in temperature also does not occur with allergies.
Congestion and temperature
Photo: pexels. com
com The child has stuffy nose and fever at the beginning of influenza and SARS. The presence of a cold is also indicated by other symptoms: malaise, headache, weakness and drowsiness. If after treatment the congestion does not go away, and the temperature rises again, then, most likely, a bacterial infection has joined. nine0003
Congestion and cough
Cough in combination with nasal congestion is possible in diseases of the upper respiratory tract: nose and throat. When a child develops allergic rhinitis with congestion, after a few months or years, bronchial asthma may develop with the addition of a cough. In this case, the first disease will aggravate the course of the second (3).
Permanent congestion
Nasal congestion does not go away for a long time if the disease has become chronic. The most common causes in children are adenoid hypertrophy and allergic rhinitis. Do not ignore problems with nasal breathing in a child, because chronic inflammation will have to be treated for a long time, expensively, and it will not always be possible to achieve a complete recovery. nine0003
nine0003
Causes of nasal congestion in a child
When a child has trouble breathing through the nose, it is important to determine the cause in order to prescribe the correct treatment. The culprit may be an acute, seasonal, or chronic illness, or sometimes another serious condition.
Allergic rhinitis
In allergic rhinitis, in addition to nasal congestion, sneezing and itching in the nasal passages are observed. In some cases, there is a headache and conjunctivitis, the sense of smell is disturbed. If a child reacts to flowering plants, then his symptoms worsen in spring, summer or autumn. All year round congestion is possible with allergies to dust in the apartment, pets, fungi, mold, cockroaches, rats, mice, feathers and fluff pillows. nine0003
Allergic rhinitis often develops by the age of 4-6, sometimes even earlier. With pronounced forms, the child's eyes become inflamed and redden, lips crack. However, the disease can be erased, with scratching of the nose and eyelids.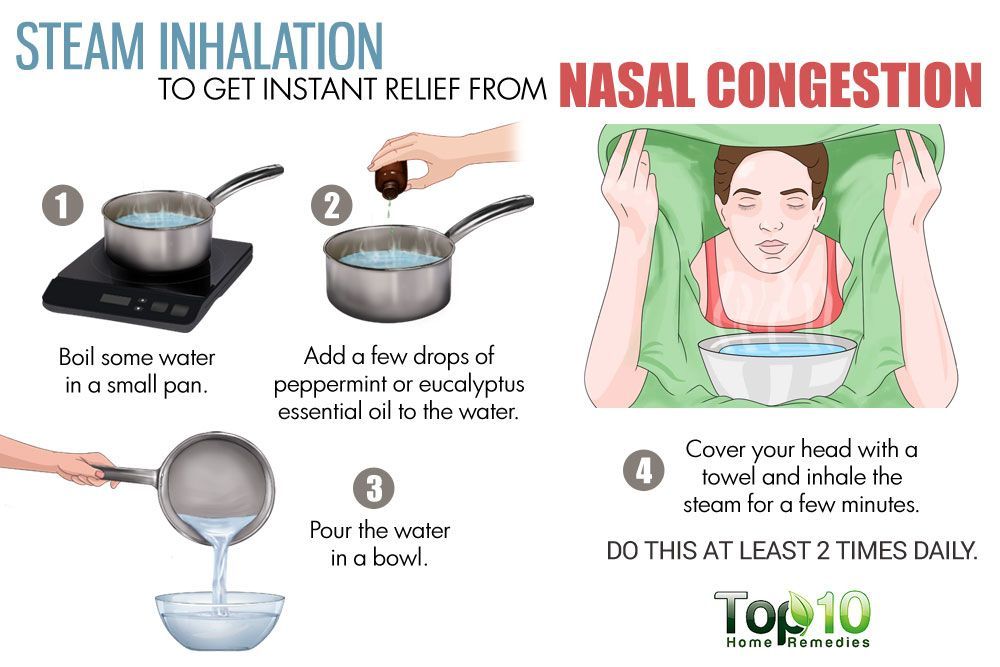 Often recurring rhinitis becomes chronic and causes more harm to the child's body. The child has restless sleep, increased fatigue, palpitations, sweating (4).
Often recurring rhinitis becomes chronic and causes more harm to the child's body. The child has restless sleep, increased fatigue, palpitations, sweating (4).
Learn more
Adenoid hypertrophy and inflammation
Adenoids — a tonsil located in the nasopharynx. Every child has adenoids from birth, by the age of 15-16 they are significantly reduced, and in adulthood they atrophy. If the baby is healthy, then the amygdala does not interfere with breathing in any way. Adenoids have gaps and depressions, so during the illness, the infection lingers in these folds. This is essential for a good immune response. However, during this process, the adenoids can become very enlarged. In children under 5-6 years old who attend kindergarten, one viral infection is often quickly replaced by another, which contributes to the constant hypertrophy of the adenoids - they simply do not have time to decrease. Adenoiditis causes nasal congestion, nasal congestion, and hard-to-remove thick mucus that the child coughs up after sleep and during physical activity (5). nine0003
nine0003
Learn more
Inflammatory diseases of the nose
Acute sinusitis is formed as a result of a complication after a viral infection. Main symptoms:
- nasal congestion,
- mucous and mucopurulent nasal discharge (mucus may also run down the back of the throat),
- headache,
- temperature.
Acute sinusitis, if not properly treated, becomes chronic and can last more than three months (6). nine0003
Nasal breathing is also disturbed in other inflammations of the nose and throat: rhinitis and nasopharyngitis, causing otitis.
Deviated septum
This pathology can be present from birth or appear with age. If no action is taken when the nasal septum is deviated, nasal congestion will progress. Treatment with nasal sprays will only give a temporary effect and when canceled, the nose will again be blocked. The correct decision would be to perform a surgical operation to repair the septum (7). nine0003
Foreign body
During play, a small child, left unattended, can stick a small part from a toy, a seed, a bead into the nose. A characteristic sign will be dry congestion in only one nostril.
A characteristic sign will be dry congestion in only one nostril.
Visit to a pool with chlorinated water
Photo: rajat sarki, unsplash.comChlorine is an aggressive chemical element. And children who are prone to allergies have sensitive airways. Therefore, exposure to chlorinated pool water can cause congestion, runny nose, and sneezing (8). nine0003
Secondhand smoke
Babies exposed to harmful substances from a smoking mother during pregnancy are more likely to develop allergic rhinitis. Nasal congestion due to allergies can develop in a child even after birth if parents smoke in the room where he is. Passive smoking can lead to frequent colds and the development of bronchial asthma. In both cases, sneezing and runny nose are observed (5, 9).
Even tertiary smoking is harmful. This is when parents smoke outside the home, but their skin, hair and clothes are also saturated with tobacco smoke components. nine0003
Teething
On average, teething begins at 4-6 months of age. During this period, blood rushes intensely to the gums, some children develop irritation of the mucous membrane and nasal congestion. If a runny nose lasts more than three days, then it's not about the teeth. Most likely, the baby caught a cold (10).
During this period, blood rushes intensely to the gums, some children develop irritation of the mucous membrane and nasal congestion. If a runny nose lasts more than three days, then it's not about the teeth. Most likely, the baby caught a cold (10).
Find out more
How to treat nasal congestion in a child
Treatment depends on the condition causing the nasal congestion. Therefore, first of all, visit a doctor: a pediatrician, an otolaryngologist or an allergist-immunologist. He will determine the cause and prescribe the right drug. nine0003
Anti-allergic drugs
Antihistamines help with itching and sneezing, but are ineffective for nasal congestion. Medicines for oral use (orally) are produced in the form of tablets, drops and syrups. For children, liquid forms are prescribed. Of these, it is worth paying attention to the new generation drugs - Claritin, Zirtek and Erius. They act quickly and have few side effects.
There are antihistamine nasal drops and sprays that are preferred in the acute phase of the illness. Some combination drugs in this category also have a vasoconstrictor component. nine0003
Some combination drugs in this category also have a vasoconstrictor component. nine0003
If antihistamines are not effective enough, hormonal nasal sprays may be needed. It is safe: the hormone works only on the nasal mucosa, is not absorbed into the blood and does not affect the entire body.
Hormonal drugs
Topical glucocorticosteroids are effective in allergic rhinitis, reduce inflammation and are well tolerated. Side effects are relatively rare. However, if the drug is used incorrectly, a perforation of the nasal septum may occur. nine0003
Aqueous solutions are usually given as they are less irritating to the nasal mucosa (11).
Vasoconstrictor drugs
Drops, sprays, aerosols constrict the vessels of the nasal mucosa, relieve swelling and restore nasal breathing. Popular drugs in this group: "Nazivin", "Snoop", "Sanorin". They should be used no more than 7 days in a row, and the dosage should not be exceeded, especially if a product in the form of drops is used. Otherwise, side effects develop:
Otherwise, side effects develop:
- dryness and burning,
- drug dependence,
- chronic congestion,
- agitation, headache, insomnia, nausea, increased heart rate, increased arterial or intraocular pressure,
- allergic reactions (2).
Saline solutions
For the treatment of nasal congestion in infants under 6 months of age, saline 0.9% is recommended. Doctors do not recommend using a hypertonic solution with a salt content of 2% or more without special indications, otherwise the runny nose, on the contrary, will drag on for a longer period. If you regularly carry out the toilet of the nose, then the swelling of the nasal mucosa will decrease and the protective function will be restored. nine0003
Antibiotic therapy
Antibiotics are used only in cases of proven bacterial infection, such as sinusitis. The onset can be acute or subacute, when the symptoms of nasal congestion persist for more than 10 days, progress and other signs are added to them: headache, earache, fever.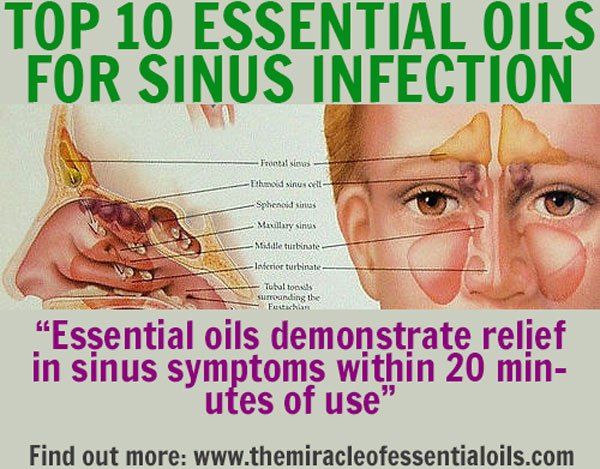
The first step is to pass an analysis for the sensitivity of pathogens to antibiotics. Based on the results of the analysis, a drug is prescribed that will help cure the underlying disease and save the child from congestion (6). nine0003
Deep treatment of the nasal passages
If the cause of nasal congestion is adenoiditis, then in the treatment it is important not only to choose a good and suitable drug, but also to use it correctly. With inflammation of this adenoid, it is necessary to apply drops so that they reach the nasopharynx and the tonsil itself. When carrying out manipulations, the child should lie down and throw his head back - only then can the maximum effect of the treatment be achieved (12).
Room conditioning
When your child's room is dry, humidify the air with one of these simple steps:
- wet clean more often,
- spray the apartment with water from a spray bottle,
- install a special device for humidifying and purifying the air at home,
- hang a wet towel in the nursery.
Gently massage your baby's face to relieve symptoms of congestion. Run your fingers from the top of your nose and down. To reduce blood flow and reduce swelling, put your baby to sleep on a high pillow. Perform inhalations with a saline nebulizer (13). nine0003
Prevention of nasal congestion in a child
As a preventive measure, the child needs to moisten and cleanse the mucous membranes of the nose with saline solution (for example, in the form of drops). It is especially important to carry out a wellness procedure in the following cases:
- unfavorable ecological situation in the city,
- the heating season has begun,
- nose surgery was performed.
After instillation, the mucus liquefies and freely exits the nasal passages, as a result, the body can more actively resist viruses and bacteria (2). nine0003
Ventilate the apartment where the child lives: the air temperature should not exceed 19C 0 and the humidity should be 45-50%.
Good hygiene practices must be followed: wash hands thoroughly with soap and water before meals, after going to the toilet and after returning from the street. You can carry out hardening procedures. It is also important that the child receives all the necessary vitamins and minerals from food, and takes vitamin D3. Play active games with your child, maintain the correct daily routine and good sleep. nine0003
Reviews of doctors
Comments Anna Kosova, allergist-immunologist at Lahta Clinic in St. Petersburg:
— It is important that you breathe through your nose, not your mouth. Pathogenic pathogens, together with the air, enter the upper respiratory tract and contact with the mucosa, where the first stage of the immune response occurs - connection with antibodies on the mucosa, the capture of pathogens by phagocytes. Further, the neutralized particles of pathogens are processed in the lymphoid tissue, namely in the adenoids and lymph nodes, and an immune memory is formed. The same immunity, thanks to which a new meeting with the same pathogen will no longer lead to the disease. nine0003
The same immunity, thanks to which a new meeting with the same pathogen will no longer lead to the disease. nine0003
In the treatment of nasal congestion from all drug groups, it is not recommended to use antiseptic solutions. Their frequent use leads to the removal of their own beneficial microflora, which should be on the nasal mucosa, taking up space and keeping pathogenic viruses and bacteria out. The most valuable immune components are also destroyed - special IgA proteins produced by the body and protecting the mucous membrane, interferons and other important proteins. The mucus itself contains natural antiseptics: lysozyme, lactoferrin. Therefore, saline solution is sufficient to facilitate the removal of mucus. nine0003
An observation from practice was shared by Dmitry Khrabrov, otolaryngologist at the Maria Frolova Medical Center in Moscow:
— Nasal congestion can be realized due to swelling of the mucous membrane or swelling of blood vessels. The vegetative control system of our body can implement both of these paths at the "order" of our brain. Children under 7 years of age, as part of adaptation to the environment, automatically copy the reactions of their mother's body. This is especially common in the spring, during allergy season. Mom starts allergic rhinitis, a small child also begins nasal congestion. Moreover, we examine the child and do not find any reasons for long-term congestion, including allergy is not confirmed. When the allergic season ends and the mother's nose begins to breathe well, the child also recovers. The family begins to breathe freely. nine0003
The vegetative control system of our body can implement both of these paths at the "order" of our brain. Children under 7 years of age, as part of adaptation to the environment, automatically copy the reactions of their mother's body. This is especially common in the spring, during allergy season. Mom starts allergic rhinitis, a small child also begins nasal congestion. Moreover, we examine the child and do not find any reasons for long-term congestion, including allergy is not confirmed. When the allergic season ends and the mother's nose begins to breathe well, the child also recovers. The family begins to breathe freely. nine0003
Popular questions and answers
It is not always easy and quick to restore nasal breathing in a child. It all depends on whether the doctor has chosen the right treatment tactics, and whether the parents follow the instructions for using the prescribed drugs. Otolaryngologist Dmitry Khrabrov and allergist-immunologist Anna Kosova talk about how to deal with congestion without harm to health and what will happen if it is not treated in any way.
What to do if nasal congestion persists? nine0254
— If the nose is blocked due to the manifestation of an acute respiratory disease, and if this process is short-lived, then symptomatic treatment is sufficient. To do this, we use vasoconstrictor drops for children under 2 years old or sprays (from 2 years old) based on oxymetazoline or xylometazoline. You can use them no more than 4 times a day with a duration of treatment of no more than 5 days, says Dmitry Khrabrov. - Another question is what to do if nasal congestion does not go away or is constantly bothering you. In this situation, the ENT doctor looks at what the difficulty in breathing is connected with. Most often it is a pronounced swelling of the nasal mucosa. In this case, you need to choose anti-edematous complex treatment. nine0003
— If the problem lasts for more than two weeks, it is better to see a doctor, Anna Kosova emphasizes. - In a child, the problem is most often associated with viral infections and hypertrophy of the adenoids, in some cases - with allergic rhinitis, and sometimes with a foreign body.
What folk remedies will help relieve nasal congestion in a child?
— In some cases, the use of sprays with sea water and applicators with essential oils is enough, — says Dmitry Khrabrov. - The latter usually contain eucalyptus, menthol. Inside, these essential components are practically not used in the treatment of children, only externally. In some cases, a decoction of sage or linden tea helps, which can replace a regular drink. nine0003
— From non-drug methods, except for irrigation of the nasal mucosa with saline, no folk remedies are recommended, — Anna Kosova shared her opinion. - You need to understand that folk remedies are methods of "treatment" that people invented out of hopelessness, when there is neither a doctor nor a pharmacy. Their seeming cheapness and simplicity can turn into big problems in the future - burns of the mucous membrane, perforation of the nasal septum, complete loss of smell.
Can congestion be related to adenoids? nine0254
- Nasal congestion may occur due to swollen adenoids.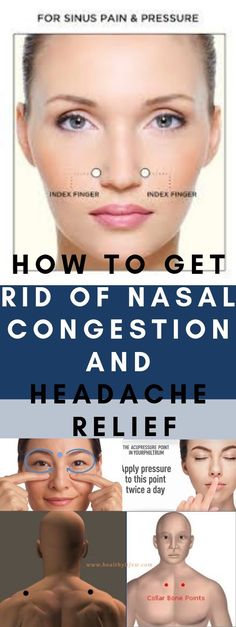 With their increase, therapy develops depending on the reasons that influenced this, - says Dmitry Khrabrov. - The first reason is the focus of inflammation inside the adenoids themselves, which disrupts the functioning of the immune system. Therefore, the child often gets sick, and the more often he gets sick, the larger the adenoids become. The second reason is the presence of allergic diseases, due to which the adenoids overreact to viruses and bacteria “running by”. The third common cause of enlarged adenoids are herpes viruses types 4, 5, 6, which can be active and lead to excessive growth of the tonsil. To diagnose the causes, the nasopharynx is examined with a camera, you also need to take a swab from the pharynx for the listed viruses and exclude allergic diseases with an allergist. nine0003
With their increase, therapy develops depending on the reasons that influenced this, - says Dmitry Khrabrov. - The first reason is the focus of inflammation inside the adenoids themselves, which disrupts the functioning of the immune system. Therefore, the child often gets sick, and the more often he gets sick, the larger the adenoids become. The second reason is the presence of allergic diseases, due to which the adenoids overreact to viruses and bacteria “running by”. The third common cause of enlarged adenoids are herpes viruses types 4, 5, 6, which can be active and lead to excessive growth of the tonsil. To diagnose the causes, the nasopharynx is examined with a camera, you also need to take a swab from the pharynx for the listed viruses and exclude allergic diseases with an allergist. nine0003
- Difficulty in nasal breathing in children under 5-6 years of age is often associated with enlarged adenoids. This is lymphoid tissue, which is only part of the lymphatic pharyngeal ring. But it is located in such a way that with hypertrophy of the adenoids, normal nasal breathing is partially, and in serious cases completely blocked, and the child is forced to breathe through the mouth, says Anna Kosova. - The fact is that at this age, the most active acquaintance with new viruses and bacteria transmitted by airborne droplets takes place in a person's life. Not always these meetings lead to illness. The inflammatory process can be of varying severity, but an immune response is always triggered for each new infectious object. This occurs in the lymphoid tissue of the entry gate, and an integral part of the immune response is the formation of specific clones of lymphocytes to each new pathogen. Therefore, in preschool children, it is always possible to palpate (feel - approx. Ed.) cervical lymph nodes, and an increase in the lymphoid tissue of the nasopharynx and specifically adenoid tissue can be manifested by difficulty in nasal breathing. This situation requires treatment.
But it is located in such a way that with hypertrophy of the adenoids, normal nasal breathing is partially, and in serious cases completely blocked, and the child is forced to breathe through the mouth, says Anna Kosova. - The fact is that at this age, the most active acquaintance with new viruses and bacteria transmitted by airborne droplets takes place in a person's life. Not always these meetings lead to illness. The inflammatory process can be of varying severity, but an immune response is always triggered for each new infectious object. This occurs in the lymphoid tissue of the entry gate, and an integral part of the immune response is the formation of specific clones of lymphocytes to each new pathogen. Therefore, in preschool children, it is always possible to palpate (feel - approx. Ed.) cervical lymph nodes, and an increase in the lymphoid tissue of the nasopharynx and specifically adenoid tissue can be manifested by difficulty in nasal breathing. This situation requires treatment. If conservative therapy does not help for several months, then a surgical operation is indicated - cutting the adenoid tissue. nine0003
If conservative therapy does not help for several months, then a surgical operation is indicated - cutting the adenoid tissue. nine0003
What complications can occur if a child's nasal congestion is left untreated for a long time?
- With prolonged nasal congestion, the auditory tubes may react, the fistulas of the sinuses may be blocked, which leads to otitis media and sinusitis. Therefore, with this problem, it is urgent to consult a doctor, advises Dmitry Khrabrov.
- If nasal congestion is not treated, then night snoring, sleep disturbance, sleep apnea appear. All this leads to a decrease in academic performance, a violation of concentration, - adds Anna Kosova. The nasopharynx communicates with the ear cavity through the auditory tube. Through this pipe, air must enter the tympanic cavity. If the lymphoid tissue blocks the auditory tube, then hearing is reduced. In the case of the transition of the inflammatory process from the nasal cavity to the auditory tube, eustacheitis develops. Recurrent average and even purulent otitis media can be the result of untreated adenoiditis. The child develops an adenoid type of face, which can no longer be corrected. nine0003
Recurrent average and even purulent otitis media can be the result of untreated adenoiditis. The child develops an adenoid type of face, which can no longer be corrected. nine0003
Sources
- Congestion or runny nose in children // Medlineplus. 2021.
URL: https://medlineplus.gov/ency/article/003051.htm - Rhinitis in young children. S. I. Erdes, N. M. Leonevskaya // Questions of modern pediatrics. 2009.
URL: https://cyberleninka.ru/article/n/rinity-u-detey-rannego-vozrasta/viewer - Asthma and rhinitis: chained together. O. Brodskaya // Asthma and Allergy. 2010.
URL: https://cyberleninka.ru/article/n/astma-i-rinit-skovannye-odnoy-tsepyu/viewer - Modern view on the problem of allergic rhinitis in children // Medical scientific and practical portal Lvrach. 2001.
URL: https://www.lvrach.ru/2001/03/4528609 - Is Secondhand Smoke as Dangerous as Smoking a Cigarette? // Healthline. 2020.
URL: https://www. healthline.com/health/secondhand-smoke-facts#bottom-line
healthline.com/health/secondhand-smoke-facts#bottom-line - Antibacterial therapy of sinusitis // Scientific and practical journal "Clinical Microbiology and Antimicrobial Chemotherapy". 1999.
URL: https://cmac-journal.ru/publication/1999/1/cmac-1999-t01-n1-p083/cmac-1999-t01-n1-p083.pdf - How to Treat a Child's Deviated Septum // Pediatric ent associates. 2019.
URL: https://www.pediatricentassociates.com/how-to-treat-a-childs-deviated-septum/ - Chlorine Allergy. ACAAI.
URL: https://acaai.org/allergies/allergic-conditions/chlorine-allergy/ - Association between prenatal or postpartum exposure to tobacco smoking and allergic rhinitis in the offspring: An updated meta-analysis of nine cohort studies // Tobacco Induced Diseases. 2022.
URL: http://www.tobaccoinduceddiseases.org/Association-between-prenatal-or-postpartum-exposure-to-ntobacco-smoking-and-allergic,146905,0,2.html - Teething and a Runny Nose: Is This Normal? // Healthline.