How to produce breast milk before birth
Causes & How It Works
Overview
Lactation is the process of making human milk. It's driven by hormones and results in milk coming from your nipple.What is lactation?
Lactation is the process of producing and releasing milk from the mammary glands in your breasts. Lactation begins in pregnancy when hormonal changes signal the mammary glands to make milk in preparation for the birth of your baby. It’s also possible to induce lactation without a pregnancy using the same hormones that your body makes during pregnancy. Lactation ends once your body stops producing milk.
Feeding your baby directly from your breasts is called breastfeeding (or sometimes chestfeeding) or nursing. You can also feed your baby milk that you have expressed or pumped from your breast and saved in a bottle.
Where does human milk come from?
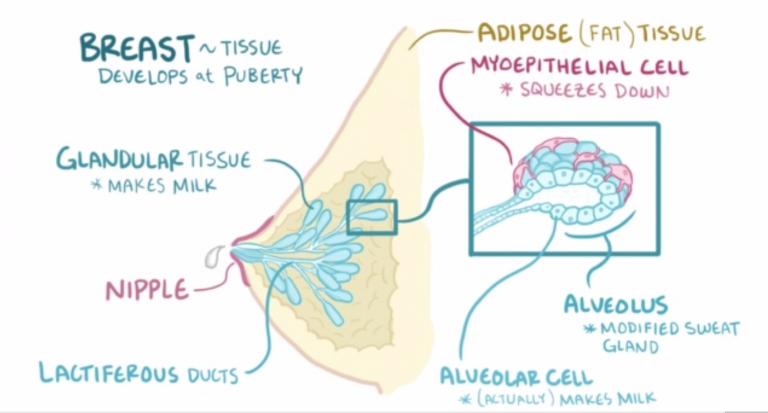
Human milk comes from your mammary glands inside your breasts. These glands have several parts that work together to produce and secrete milk:
- Alveoli: These tiny, grape-like sacs produce and store milk.
A cluster of alveoli is called lobules, and each lobule connects to a lobe.
- Milk ducts: Each lobe connects to a milk duct. You can have up to 20 lobes, with one milk duct for every lobe. Milk ducts carry milk from the lobules of alveoli to your nipples.
- Areola: The dark area surrounding your nipple, which has sensitive nerve endings that lets your body know when to release milk. To release milk, the entire areola needs stimulation.
- Nipple: Your nipple contains several tiny pores (up to about 20) that secrete milk. Nerves on your nipple respond to suckling (either by a baby, your hands or a breast pump). This stimulation tells your brain to release milk from the alveoli through the milk ducts and out of your nipple.
It helps to think of the lactation system as a large tree. Your nipple is the trunk of the tree. The milk ducts are the branches. The leaves are the alveoli.
Why do people lactate?
The primary reason people lactate is to feed a baby. Lactation is a biological, hormonal response that occurs during and after pregnancy to feed a newborn baby. Your body triggers specific hormones to initiate milk production and ejection (releasing of milk). All mammals lactate for this purpose and it’s possible to induce lactation in men and in non-pregnant women using the right hormone medications.
Lactation is a biological, hormonal response that occurs during and after pregnancy to feed a newborn baby. Your body triggers specific hormones to initiate milk production and ejection (releasing of milk). All mammals lactate for this purpose and it’s possible to induce lactation in men and in non-pregnant women using the right hormone medications.
Function
What triggers lactation?
A series of hormonal events, which begin when you’re pregnant, trigger the lactation process. That process is called lactogenesis.
Stage one lactogenesis: This begins around the 16th week of pregnancy and lasts until a few days after you give birth.
- Estrogen and progesterone rise and cause your milk ducts to grow in number and size. This causes your breasts to become fuller. Your mammary glands begin to prepare for milk production.
- Your nipples darken and your areolas become larger.
- Your Montgomery glands (small bumps on the areola) secrete oil to lubricate your nipple.

- Your body begins making colostrum. It’s highly nutritious and filling and serves as your baby’s first milk.
Stage two lactogenesis: This stage starts about two or three days postpartum (after giving birth). It’s when milk production intensifies.
- Once your baby and placenta are delivered, a sudden drop in your estrogen and progesterone causes the hormone prolactin to take over.
- Prolactin is the hormone that produces milk.
- You’ll notice your milk production increases dramatically at this stage. It’s often referred to as milk “coming in.”
- Your breasts are often engorged (or overly full of milk) to the point where they feel sore, painful or tender.
Stage three lactogenesis: This describes the rest of the time you lactate.
- Lactation generally continues as long as milk is removed from your breast.
- The more milk that’s removed, the more milk your body makes to replace it. Frequent feeding or pumping will cause your body to make more milk.

Hormones for lactation
The hormone prolactin controls the amount of milk you produce, and your body begins producing prolactin early in pregnancy. At first, the high levels of estrogen, progesterone and other pregnancy hormones suppress prolactin. Once you deliver the placenta, those pregnancy hormones drop and prolactin takes charge.
When your baby suckles, it stimulates nerves that tell your body to release prolactin and oxytocin. Prolactin causes the alveoli to make milk and oxytocin causes muscle contractions that push out of the alveoli and through the milk ducts.
When milk is released, it’s called a “letdown,” and it takes about 30 seconds of suckling before the letdown occurs. Because you can’t control which breast receives the hormones, the letdown can cause milk to drip from both nipples.
Inducing lactation in people who aren’t pregnant requires medication that mimics hormones your body makes during pregnancy. Suckling from the nipple can initiate lactation, either with a breast pump or by a baby. This is a complex process that involves working closely with a healthcare provider who understands the needs of non-pregnant people and has experience initiating lactation.
This is a complex process that involves working closely with a healthcare provider who understands the needs of non-pregnant people and has experience initiating lactation.
When do you lactate during pregnancy?
Lactation begins as early as a few weeks into the second trimester of your pregnancy. As estrogen and progesterone levels rise, your body prepares for lactation by increasing the number of milk ducts in your breasts, and those milk ducts will transport milk from the alveoli to your nipples. About midway through pregnancy, your body creates colostrum, which is your baby’s first milk.
Can you lactate when you’re not pregnant?
Yes, it’s possible to lactate if you’re not pregnant. Inducing lactation is a complex process that usually involves using hormone-mimicking drugs for several months to produce milk. The second part of lactation is expressing the milk through your nipple. Stimulation from infant suckling, pumping with a breast pump or hand-expressing signals the brain to release the milk. It’s common for people in this situation to receive assistance from a healthcare provider who understands the needs of non-pregnant people and has experience initiating lactation.
It’s common for people in this situation to receive assistance from a healthcare provider who understands the needs of non-pregnant people and has experience initiating lactation.
How do you stop lactation?
There are many reasons why you might need to stop producing milk, and you can stop lactating either naturally or with the help of hormonal drugs.
Natural milk suppression
Lactation is a supply-and-demand process. Your milk supply gradually goes down as your baby relies less on breast milk, or as you reduce the number of times you nurse or pump. Generally, if you decrease the volume of milk removed from your breasts, your body will slow milk production.
Suppressing your milk can feel uncomfortable and most people will become engorged (the term for overfilled breasts). You may also leak milk or develop a clogged milk duct. However, you can treat that pain by taking an over-the-counter pain reliever, wearing a firm bra or using an ice pack on your breasts.
Medication suppression
Medications can also be an option if you need to stop producing milk. Your healthcare provider can explain more about lactation-suppressing drugs, as well as the benefits and possible side effects.
Anatomy
Where are the mammary glands located?
Mammary glands are commonly called breasts and both genders have them. They are located on your chest and are composed of connective tissue, fat and special glandular tissue that makes milk. A woman’s glandular tissue is slightly different because it contains the alveoli and lobules necessary for producing milk. Women also have much more glandular tissue.
Conditions and Disorders
What are common conditions that affect your ability to lactate?
The ability to lactate and the length of time you’re able to produce milk varies. Some can produce milk for years, while others have trouble producing enough milk for their baby.
Some common factors that can impact lactation or breastfeeding are:
- Hormonal levels and conditions.

- Medications.
- Undergoing radiation therapy in the past.
- Trauma to your breast or nipples.
- Breast augmentation, reconstruction or other breast surgeries.
- Other medical conditions like HIV infection.
- Use of drugs and alcohol.
If you’re nursing or pumping your milk to bottle-feed your baby, you should always consult with your healthcare provider before starting any new medications or treatments. Many medications can pass to your baby through breast milk, which may have dangerous effects on your baby.
What is lactational amenorrhea?
Lactation amenorrhea (ah-men-oh-re-uh) means you aren’t menstruating (getting a period) due to lactation. When you’re lactating, your body produces prolactin, the hormone that produces milk. Prolactin reduces the amount of luteinizing hormone (LH) in your body, which helps trigger the release of an egg during ovulation. If you aren’t producing enough LH, you can’t ovulate or get your period. The length of time you can be amenorrheic due to lactation varies from a few months or until you’re completely done lactating.
The length of time you can be amenorrheic due to lactation varies from a few months or until you’re completely done lactating.
Does lactation reduce my risk of any diseases?
Studies have shown that breastfeeding reduces a woman’s risk of ovarian and breast cancers. It can also lower your risk for Type 2 diabetes and high blood pressure.
Care
How do you maintain milk production?
Maintaining lactation is mostly based on supply and demand. The more your baby breastfeeds or the more milk you express with a breast pump, the more your body will make. There are ways to suppress lactation with hormones or oral contraceptives. If you wish to maintain lactation, some things you should do are:
- Continue nursing on-demand or pump milk frequently (approximately every four hours).
- Eat a healthy diet with enough calories. Low-calorie diets can decrease milk supply.
- Drink plenty of water to stay hydrated. Human milk is primarily water.
- Avoid smoking, drugs or alcohol.
 These can reduce your supply and transfer to your milk.
These can reduce your supply and transfer to your milk.
Frequently Asked Questions
What is the difference between lactation and colostrum?
Lactation describes the process of making and secreting milk from your breast. Colostrum is the first milk your breasts create during lactation and the first milk your baby drinks. It’s thick, yellow and commonly called “liquid gold.” Colostrum is high in protein, minerals, vitamins and antibodies.
What is hormone therapy for inducing lactation?
Couples or families who wish to induce lactation, maybe because of adoption, surrogacy or other reasons, can try hormone therapy. Induced lactation means you’re creating a milk supply without being pregnant. It’s a process that involves taking estrogen and progesterone for several months to make your body believe it’s pregnant. This helps prepare your breasts for lactation. Some medications and herbs are believed to help establish a milk supply, too.
Several weeks before your baby arrives, begin pumping your breasts with a breast pump. This encourages your body to release prolactin, which produces milk. Ideally, you express your milk several times a day, just like you would if you had a baby. This helps establish a supply. You can also freeze any milk you produce for use once your baby arrives.
This encourages your body to release prolactin, which produces milk. Ideally, you express your milk several times a day, just like you would if you had a baby. This helps establish a supply. You can also freeze any milk you produce for use once your baby arrives.
If you’re considering this as an option, you should talk to your healthcare provider about your desire to feed your baby with human milk. Induced lactation works for many people, but not all.
A note from Cleveland Clinic
If you want to feed your baby human milk, it’s helpful to understand the process of lactation so you know what to expect. Talk to your healthcare provider about how to best prepare for nursing or expressing milk. Remember, lactation can look different for everyone depending on your circumstances and health history. If you struggle with lactation at any point, you may feel embarrassed or even ashamed. But struggling with lactation is very common, and lactation specialists and other healthcare providers can help you as you try to overcome these difficulties.
Breastfeeding Without Giving Birth - La Leche League International
Alyssa Schnell, St. Louis, Missouri, USA
Alyssa Schnell is an International Board Certified Lactation Consultant (IBCLC) based in the United States. She speaks internationally about inducing lactation and relactation and specializes in helping parents who have not given birth (non-gestational parents) to breastfeed their babies. In this article Alyssa discusses how parents who have not given birth can breastfeed by inducing lactation and how La Leche League Leaders can support them.
Breastfeeding is a special gift a baby receives from their gestational parent[1]. However, many non-gestational parents—adoptive parents, intended parents (through surrogacy), parents whose partner is birthing, and transwomen—are finding out that this wonderful experience is also available to them. Because parents who haven’t given birth do not have the hormones of pregnancy to get their bodies started with making milk, they need more information and support to make breastfeeding a reality.
- Attachment. Breastfeeding helps the parent and baby form a secure attachment, a particular concern when babies are separated from their gestational parent or gestational carrier (in surrogacy).
- Nutrition. Human milk provides the optimal nutrition and necessary immunities for human babies.
Healing. Breastfeeding can help heal the heartache of infertility, and provides a biological connection between mother/parent and baby. Breastfeeding is much more than breast milk. Breastfeeding is a close, intimate, physical and emotional relationship between two or more people who love each other. - Sharing. When both parents are breastfeeding, they share the caregiving role.
Facts about breastfeeding without birthing
- Women have breastfed babies they did not birth throughout history.
 With the easy availability and common use of bottles and infant formula in modern developed countries, culture has largely lost track of how breastfeeding can also be an option for non-gestational parents.
With the easy availability and common use of bottles and infant formula in modern developed countries, culture has largely lost track of how breastfeeding can also be an option for non-gestational parents. - Non-gestational parents can start preparing for breastfeeding as soon as they decide to grow their family[2], after an adoption match has occurred or once their partner or gestational carrier is pregnant. They can even wait until the baby is in their arms.
- The amount of milk produced when inducing lactation can vary widely. While some parents make no milk and others make all the milk their babies need, most will make a partial milk supply. Fortunately, breastfeeding is possible no matter how much or little milk is produced—even if it is none at all! Human milk feeding can be simulated with a nursing supplementer: a bag or bottle that holds human milk or formula carried to the nipple via a tiny feeding tube. Parents who are not making any milk may also choose to feed with a bottle while their baby comforts and connects with them by suckling at the (dry) breast.

- Newborn babies are wired to initiate breastfeeding, but with gentle and patient encouragement, along with a few handy tools and techniques, even older babies can learn to breastfeed.
- Some mothers will take medications or herbs to help them make more milk, but this is not essential. The only necessary component to induce lactation—the official term for making milk without pregnancy and birth—is to stimulate and drain the breasts. That stimulation or emptying can happen with baby breastfeeding, with an electric breast pump, or using a variety of manual techniques.[3]
- The composition of milk produced by inducing lactation is comparable to that produced following birth.[4],[5] The milk does not contain dangerous levels of artificial hormones—in fact, it very rarely contains any artificial hormones at all. In most cases, the only artificial hormones that are taken are estrogen and/or progesterone before there is milk production (Step 1 below.
 ) Progesterone and estrogen levels are high during pregnancy and taking these hormones artificially may help to make the body think it is pregnant. Estrogen and progesterone play a role in breast development in pregnancy.
) Progesterone and estrogen levels are high during pregnancy and taking these hormones artificially may help to make the body think it is pregnant. Estrogen and progesterone play a role in breast development in pregnancy. - It is not necessary to be fertile—or even to have ovaries or a uterus—to breastfeed. The hormones responsible for milk production (prolactin) and milk ejection (oxytocin) are released from the pituitary gland located at the base of the brain.
- Both parents, whether or not one has given birth, can share the breastfeeding role. This is called co-nursing.
As stated above, the primary way to induce lactation is through breast emptying: breastfeeding, pumping, or hand expression. The effectiveness of these physical techniques can be enhanced with the use of galactogogues: medications, herbs and homeopathic remedies that support the production of milk. These tools can be put together in a variety of ways to be effective and applicable to each individual parent. While the use of medications, herbs or homeopathic preparations is an individual choice, parents should always discuss their individual situation with their health care providers.
While the use of medications, herbs or homeopathic preparations is an individual choice, parents should always discuss their individual situation with their health care providers.
Generic protocols are available (such as Dr Jack Newman’s protocol) or an experienced International Board Certified Lactation Consultant (IBCLC) can work with parents to develop a personalized protocol customized to meet their specific health history, circumstances, and values. The process can be broken down into three steps:
Step 1: Preparing the Breasts for Lactation
This step mimics the hormonal and breast changes that occur during pregnancy. This step is not about making milk; it is about growing and developing the glandular breast tissue in preparation for making milk. Many parents will take hormone therapy for a period of time to achieve this. However, this step is optional.
Step 2: Starting to Make Milk Before Baby Arrives
Milk is often produced very, very slowly when lactation is induced compared with the sudden increase in milk supply between days 3-5 following birth. In order to have a milk supply by the time baby arrives, parents will often start the process of growing their milk production several weeks or months before. The main component of Step 2 for many parents is frequent pumping. Ideally, parents will express their milk as frequently as a baby nurses—just like for birthing parents, frequent breast drainage “places the order” for healthy milk production. Parents can store any milk they produce for use when baby arrives.
In order to have a milk supply by the time baby arrives, parents will often start the process of growing their milk production several weeks or months before. The main component of Step 2 for many parents is frequent pumping. Ideally, parents will express their milk as frequently as a baby nurses—just like for birthing parents, frequent breast drainage “places the order” for healthy milk production. Parents can store any milk they produce for use when baby arrives.
Step 3: Feeding Baby and Continuing to Grow Milk Production
This is the big payoff! Baby is here and the parent can begin feeding baby their milk. This step generally involves putting baby to breast.
Not every parent’s protocol will use all three steps. Each parent’s needs and circumstances determine which steps will be appropriate for them. For most parents with adequate information and support, milk production begins within 6-8 weeks of beginning the process of inducing lactation.
What is the role of a La Leche League Leader?Although extremely rewarding, inducing lactation can be a challenging breastfeeding situation. Mothers/parents need and deserve all of the support they can get. While working with an International Board Certified Lactation Consultant (IBCLC) is highly recommended, La Leche League Leaders can also play a very valuable role. As always, Leaders provide essential information and encouragement. More specifically, La Leche League Leaders may:
Mothers/parents need and deserve all of the support they can get. While working with an International Board Certified Lactation Consultant (IBCLC) is highly recommended, La Leche League Leaders can also play a very valuable role. As always, Leaders provide essential information and encouragement. More specifically, La Leche League Leaders may:
- Refer parents to resources on inducing lactation (see below).
- Provide support for inducing lactation.
- Facilitate La Leche League Group meetings where older babies who are bottle-feeding can observe breastfeeding babies, and parents can participate in a breastfeeding culture. Group meetings are also opportunities for parents to connect with other mothers who are nursing in a variety of situations.
- Facilitate healthy social media information and interaction.
- Share information about donor milk.
Breastfeeding without birthing may not be easy, but it is possible and it is powerful. La Leche League Leaders can be part of the team supporting these parents and their babies.
- La Leche League Inducing Lactation and Relactation Facebook Group
- “Breastfeeding an Adopted Baby”, LLLI website
- Breastfeeding Without Birthing by Alyssa Schnell
- Breastfeeding Outside the Box podcast or other podcast app
Alyssa Schnell has been helping parents and babies with breastfeeding for the past 17 years, first as a La Leche League Leader and now as an International Board Certified Lactation Consultant (IBCLC). Her private practice, Sweet Pea Breastfeeding Support, provides individual lactation consultations either in person or by phone or video-conference for parents throughout the United States and beyond. Alyssa is also the co-host of the Breastfeeding Outside the Box podcast, which is devoted to families breastfeeding or chestfeeding in extraordinary situations. Alyssa enjoys working with all parents and babies, but she has a special place in her heart for helping non-gestational parents to breastfeed/chestfeed their babies. She is the author of Breastfeeding Without Birthing: A Breastfeeding Guide for Mothers Through Adoption, Surrogacy, and Other Special Circumstances and is an international speaker on the topics of inducing lactation, relactation, and other related topics. Alyssa lives in St. Louis, Missouri, USA and is the proud mother of three breastfed children—two by birth and one by adoption.
She is the author of Breastfeeding Without Birthing: A Breastfeeding Guide for Mothers Through Adoption, Surrogacy, and Other Special Circumstances and is an international speaker on the topics of inducing lactation, relactation, and other related topics. Alyssa lives in St. Louis, Missouri, USA and is the proud mother of three breastfed children—two by birth and one by adoption.
[1] Some notes about language: The term “gestational” is used throughout this article instead of “biological.” In surrogacy, the intended mother is often the biological mother (baby is often conceived with her egg) even though she is not gestating (pregnant with) the baby. And oftentimes same-sex female couples will conceive baby via in vitro fertilization (IVF) using the egg of one parent (biological parent) implanted in the uterus of the other parent (gestational parent). This article also attempts to use gender-inclusive language such as parent versus mother and breastfeeding/chestfeeding versus breastfeeding. Some of the parents referred to in this article may be cis male, trans male, or non-binary.
Some of the parents referred to in this article may be cis male, trans male, or non-binary.
[2] Note: inducing lactation with medication should not be started unless the parent has an approximate timeline for their baby’s arrival. Taking medication without a definite end could be hazardous.
[3] Other manual approaches might include breast massage, nipple manipulation (gently pulling out and twisting of the nipple), and a partner suckling.
[4] Kulski, J. K., Hartmann, P. E., Saint, W. J., Giles, P. F., & Gutteridge, D. H. (1981). Changes in the milk composition of nonpuerperal women. American journal of obstetrics and gynecology, 139(5), 597-604.
[5] Perrin, M. T., Wilson, E., Chetwynd, E., & Fogleman, A. (2015). A pilot study on the protein composition of induced nonpuerperal human milk. Journal of Human Lactation, 31(1), 166-171.
Breast milk production | Baby's needs
Did you know that the amount of breast milk adapts to your baby's needs? In this article, you will learn amazing facts about breast milk production in the first days, weeks and months.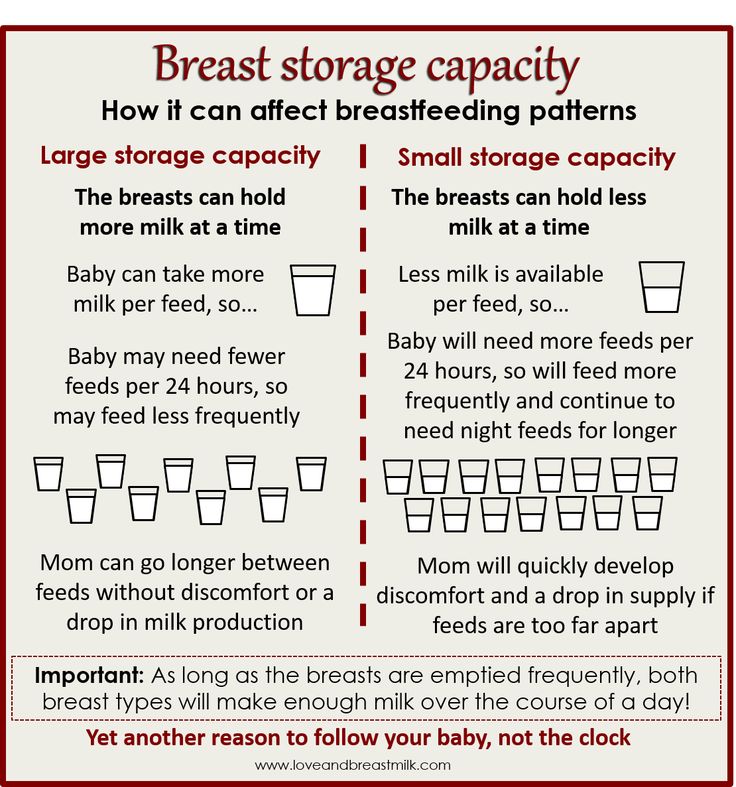
Share this information
Your body is capable of producing breast milk for your baby at every stage of development. Understanding how milk production “turns on”, what happens to milk when you feed your baby, and why production adjusts to his needs as he grows, will help you start this amazing process in the right way.
Day one: milk production at birth
The baby is usually ready to breastfeed from birth. When he grabs the breast and begins to suck rhythmically, the milk-producing cells “turn on” and the formation of the first breast milk, colostrum, starts. 1 Try to feed your baby as much as possible in the first hour of his life, and then as soon as he shows interest in feeding. This will help lay the foundation for good milk production later on. 2
The first days: the arrival of milk
At this stage, your body's level of progesterone, the
pregnancy hormone, which begins to fall after the placenta comes out, is reduced, and the hormones responsible for milk production - prolactin, insulin and hydrocortisone - are included in the work. These hormones will help start milk production. 3 Around the third day of your baby's life, milk will begin to come in and you will feel that your breasts have filled up and become noticeably firmer. 1
These hormones will help start milk production. 3 Around the third day of your baby's life, milk will begin to come in and you will feel that your breasts have filled up and become noticeably firmer. 1
First month: shaping milk production
During the first weeks, your body will be especially sensitive to the amount of milk produced as it learns to produce the right amount. Prolactin levels increase dramatically each time you empty your breasts, thereby helping shape the lactation process. It also contributes to the maturation of your milk in terms of composition. At this stage, transitional milk is produced and the amount continues to grow. 3.4
For good long-term milk production, it is very important that you are close to your baby during the first few weeks. The more often you breastfeed, the more milk will be produced. This process resembles the law of supply and demand. Each time after emptying the breast, whether it is feeding the baby or pumping, even more milk will be produced.
Remember that it is normal for newborns to eat frequently, perhaps even every 45 minutes, and this does not mean that they are not getting enough milk. Frequent feedings help shape milk production, so feed your baby on demand, not on a schedule.
“In the first few weeks you may feel like you don’t have enough milk because your baby will be feeding all the time, but that’s okay,” says UK mom-of-two Jo, “We tend to think that the baby wants to eat every few hours, but that is not necessarily the case."
Don't forget that babies also breastfeed for comfort. Breastfeeding helps them calm down and adjust to their new life outside the womb. In addition, feeding helps to establish a connection between you.
Stable milk production in the first month
If you follow your baby's needs and feed him as often and for as long as he wants, milk production should adjust. 5
Some mothers try to increase the period between feedings so that the breasts can produce more milk during this time, but this should not be done, as this may have the opposite effect. 2
2
If you are unable to breastfeed directly for the first two weeks, express your milk to build and maintain your milk supply during this critical period and beyond.
Did you know that feeding your baby extra formula unnecessarily can reduce your milk production? The chest will not receive a signal to increase production, because it will not be emptied. In addition, if the baby sleeps longer after formula, he may miss his usual next feeding time.
This is a kind of “supplementing trap”. After three to four days of formula supplementation, during which the breasts have emptied less, the body will receive a signal that breastfeeding has stopped, and the amount of milk produced will begin to decrease. As a result, the baby will remain hungry and will need additional formula supplementation. And so on in a circle ... As a result, this will lead to really low milk production, and the baby will eat mainly the mixture.
Breast milk production after six weeks
After a month of breastfeeding, post-feeding bursts of prolactin secretion begin to decrease, milk matures, and the body gets used to producing as much milk as your baby needs. In fact, the chest begins to work "on autopilot." 4 You may also notice at this time that your breasts are softer and your milk flow has stopped.
In fact, the chest begins to work "on autopilot." 4 You may also notice at this time that your breasts are softer and your milk flow has stopped.
At this stage, women often have fears of "losing milk".
However, this only means that milk production has been established and now fully meets the needs of the child. It is noteworthy that although the baby continues to grow, he will consume approximately the same amount of milk both at six weeks and at six months. You may notice that the baby began to suckle the breast longer, but less often. On some days he may eat a little less than usual - his appetite changes in the same way as an adult.
Now your body will produce exactly the amount of milk,
as much as your baby needs. Therefore, the more milk the baby
drinks (or you express), the more it will produce.
How does this happen? The reason for this is thought to be the so-called "feedback lactation inhibitor" that controls milk production. The more milk in the breast, 2 the higher the inhibitor level, so a full breast produces less milk than one that has been emptied.
The more milk in the breast, 2 the higher the inhibitor level, so a full breast produces less milk than one that has been emptied.
What is the rate of milk production?
Mothers often worry about their milk supply and think about how to increase it. However, if the baby is healthy and growing well, problems usually do not arise.
“I was worried that my newborn daughter was not getting enough milk as she was feeding very quickly and always from one breast even though I offered both,” says Marjorie, mother of two in the UK, “But when I pumped from using a breast pump, I was surprised at how much milk I produced, and calmed down. I just had to keep feeding her little and often.”
Keep in mind, however, that not all mothers are able to express a lot of milk right away. You can also try hand expressing milk and see if there is a change in breast fullness.
If you're worried about your milk supply, read our tips for symptoms of too little or too much milk.
Literature
1 Pang WW, Hartmann PE. Initiation of human lactation: secretory differentiation and secretory activation. J Mammary Gland Biol Neoplasia 2007;12(4):211-221. - Pang, W.W., Hartmann, P.I., "Lactation initiation in the lactating mother: secretory differentiation and secretory activation." G Mammary Gland Biol Neoplasia. 2007;12(4):211-221.
2 Kent JC et al. Principles for maintaining or increasing breast milk production. J Obstet Gynecol Neonatal Nurs . 2012;41(1):114-121. - Kent J.S. et al., "Principles for Maintaining and Increasing Milk Production". F Obstet Ginecol Neoneutal Nurs. 2012;41(1):114-121.
3 Ostrom KM. A review of the hormone prolactin during lactation. Prog Food Nutr Sci . 1990;14(1):1-43. - Ostrom KM, "Review of the role of the hormone prolactin during lactation." Prog Food Nutr Sai. 1990;14(1):1-43.
1990;14(1):1-43. - Ostrom KM, "Review of the role of the hormone prolactin during lactation." Prog Food Nutr Sai. 1990;14(1):1-43.
4 Cox DB et al. Blood and milk prolactin and the rate of milk synthesis in women. Exp Physiol. 1996;81(6):1007-1020. - Cox D.B. et al., Effects of blood and milk prolactin on milk production in women. Exp Physiol. 1996;81(6):1007-1020.
5 Kent JC et al. Volume and frequency of breastfeedings and fat content of breast milk throughout the day. Pediatrics. 2006;117(3): e 387-95. - Kent J.S. et al., "Amount and frequency of breastfeeding and fat content of breast milk during the day." Pediatrix (Pediatrics). 2006;117(3): e 387-95.
Transitional milk | Stages of breast milk production
During the first couple of weeks after birth, the composition of breast milk changes dramatically. Learn about the amazing properties of this transitional milk.
Share this information
A newborn changes literally every day, and the same can be said about breast milk. With the advent of milk, the breast can increase to an impressive size, and changes occur not only on the outside, but also inside. During the first week, the milk-producing cells and the connections between them are rebuilt and prepare the breast for the upcoming feeding. 1 From now until about the end of the second week, they will produce what is called transitional milk. 2
“After the placenta is delivered, levels of progesterone, the pregnancy hormone, begin to decline rapidly,” explains Professor Peter Hartmann of the University of Western Australia, a leading authority on the composition of breast milk. “As progesterone levels decrease, milk synthesis increases and the composition is approaching the norm, although a couple more weeks are needed for the full maturation of the milk.
Breastmilk Stages: An Intermediate Phase
If colostrum is your baby's very first food and mature milk is his main food for a long time, then transitional milk is a kind of bridge between them.
They should be considered as three different stages of milk production, not three types of milk. The main components remain unchanged throughout breastfeeding, only their quantity changes depending on the circumstances. During the transition period, the composition of milk undergoes the most significant changes, and this happens every day in accordance with the changing needs of the child.
Milk changes because it contains bioactive components, including cells, hormones and beneficial bacteria. The transition to mature milk does not happen all at once: the composition changes gradually and in strict accordance with the developmental needs of the baby. 3.4
“The amount of milk produced by the mother has a major influence on the composition of milk,” says Professor Hartman. “The composition of milk at low and higher levels of production is different.”
“The composition of milk at low and higher levels of production is different.”
Transitional milk: increase in quantity
As the baby grows, it needs more food and a different ratio of nutrients. The amount of milk produced during this period also increases significantly. You can produce 600-700 ml per day, 5 which is a very impressive amount compared to the small amount of colostrum that was produced in the early days.
"The composition of milk in all mammals varies according to the needs of the young"
Your breasts are now in “boosting” mode: your body is learning to produce the amount of milk your baby needs. The breast becomes more mature, as does the milk. Compared to colostrum, transitional milk contains more fat and lactose, a natural sugar that gives your baby energy. 2
“The level of lactose rises sharply in the first two or three days after birth,” says Prof. Hartmann, “The composition of fats also changes: the content of medium-chain fatty acids C10 and C12 increases. They are an easily digestible source of energy and have antiviral properties. In addition, sodium and chloride levels are greatly reduced during this period, so that the milk has a very low salt content.”
They are an easily digestible source of energy and have antiviral properties. In addition, sodium and chloride levels are greatly reduced during this period, so that the milk has a very low salt content.”
Protein: the right ratio
The protein content of breast milk does not stay the same either. There are two types of proteins in human milk: casein and whey. Under the influence of acid in the child's stomach, casein turns into a solid mass (cottage cheese) and gives a feeling of satiety for a longer time. It also has antimicrobial properties. Whey, on the other hand, is rich in antibodies and remains liquid, so it is easily absorbed, which is especially important for newborns. As the child's gastrointestinal tract strengthens, the ratio of casein to whey in milk gradually changes. If in colostrum it is about 90:10, then after a month it reaches 60:40, and after a year of breastfeeding, the balance is set at 50:50. 6
This ratio of proteins is ideal for humans, as our body grows relatively slowly and the brain is constantly growing and becoming more complex. In addition, it promotes the supply of all the essential amino acids that a child needs for the healthy development of the brain, eyes and other organs.
In addition, it promotes the supply of all the essential amino acids that a child needs for the healthy development of the brain, eyes and other organs.
The amount of whey protein in human milk is significantly higher than that of other mammals. In cow's milk, the ratio of whey and casein is the opposite: 20:80 (therefore, it is not suitable for feeding children under one year old). 7
“Milk is designed to perform a specific task,” continues Professor Hartmann, “Some components are present in all milk, such as proteins and fats, but if you look at which proteins and which fats, it becomes clear which animal belongs to milk. The composition of milk in all mammals varies depending on the needs of the young.
Changing the protective properties of transitional milk
Although your baby is still very young, already in the first couple of weeks he begins to develop his own immune system, and now he needs your direct protection a little less.
The concentration of protective enzymes and antibodies in breast milk changes accordingly. The content of some substances, in particular lactoferrin (protective enzyme) and secretory immunoglobulin A (antibody), decreases, while other substances, such as the antibacterial enzyme lysozyme, on the contrary, increase. 8
The content of some substances, in particular lactoferrin (protective enzyme) and secretory immunoglobulin A (antibody), decreases, while other substances, such as the antibacterial enzyme lysozyme, on the contrary, increase. 8
“The protein content of milk decreases around the same time,” says Prof. Hartmann, “The synthesis of protective proteins occurs at the same rate, but they are more diluted due to increased milk production.”
The concentration of minerals such as zinc, copper and magnesium, which support the development of the child's immune system, also decreases as the immune system strengthens. 9
When breast milk becomes fully mature
During the transition period, the composition of breast milk changes significantly. By the end of the first month, it becomes fully mature. This means that the child will be able to eat them further as they grow. The composition of milk will no longer change much, no matter how long you continue breastfeeding - a few months, a year or more.
Would you like to know more? Read our free e-book Surprising Breast Milk Facts or article on mature milk.
Literature
1 Pang WW, Hartmann PE. Initiation of human lactation: secretory differentiation and secretory activation. J Mammary Gland Biol Neoplasia. 2007;12(4):211-221. - Pang, W.W., Hartmann, P.I., "Lactation initiation in the lactating mother: secretory differentiation and secretory activation." F Mammary Gland Biol Neoplasia. 2007;12(4):211-221. 2 Ballard O, Morrow AL. Human milk composition: nutrients and bioactive factors. Pediatr Clin North Am . 2013;60(1):49-74. - Ballard O., Morrow A.L., "Composition of breast milk: nutrients and biologically active factors." Pediatrician Clean North Am. 2013;60(1):49-74. 3 Munblit D et al. 4 Pons SM et al. Triacylglycerol composition in colostrum, transitional and mature human milk. Eur J Clin Nutr . 2000;54(12):878-882. — Pons SM, "Triacylglycerol in colostrum, transitional and mature human milk". Yur J Klin Nutr. 2000;54(12):878-882. 5 Neville MC et al. Studies in human lactation: milk volumes in lactating women during the onset of lactation and full lactation. Am J Clin Nutr . 1988;48(6):1375-1386. 6 Kunz C, Lönnerdal B. Re-evaluation of the whey protein/casein ratio of human milk. Acta Paediatr. 1992;81(2):107-112. Kunz S, Lonnerdal W. Act Pediatr.1992;81(2):107-112. - Kuntz S., Lönnerdahl B., "New Evaluation of Whey Protein/Casein in Breast Milk". Akta Pediatr. 1992;81(2):107-112. 7 Martin CR et al. Review of infant feeding: key features of breast milk and infant formula. Nutrients. 2016;8(5). - Martin S.R. et al., Review of Infant Feeding Issues: Key Features of Breast Milk and Infant Formula. Nutrients. 2016;8(5). 8 Lönnerdal B et al. Longitudinal evolution of true protein, amino acids and bioactive proteins in breast milk: a developmental perspective. Colostrum and mature human milk of women from London, Moscow, and Verona: determinants of immune composition. Nutrients. 2016; 8(11): 695. - Moonblit, D. et al., "Colostrum and mature breast milk from women in London, Moscow, and Verona: major factors in immune composition." Nutrients. 2016; 8(11): 695.
Colostrum and mature human milk of women from London, Moscow, and Verona: determinants of immune composition. Nutrients. 2016; 8(11): 695. - Moonblit, D. et al., "Colostrum and mature breast milk from women in London, Moscow, and Verona: major factors in immune composition." Nutrients. 2016; 8(11): 695.  - Neville M.S. et al., "Female Lactation Study: Milk Quantity in Lactating Women at the Beginning and Peak of Lactation." Am F Clean Nutr. 1988;48(6):1375-1386.
- Neville M.S. et al., "Female Lactation Study: Milk Quantity in Lactating Women at the Beginning and Peak of Lactation." Am F Clean Nutr. 1988;48(6):1375-1386.