How late can a breech baby turn
Breech pregnancy | Pregnancy Birth and Baby
Breech pregnancy | Pregnancy Birth and Baby beginning of content8-minute read
Listen
How will I know whether my baby is in the breech position or not?
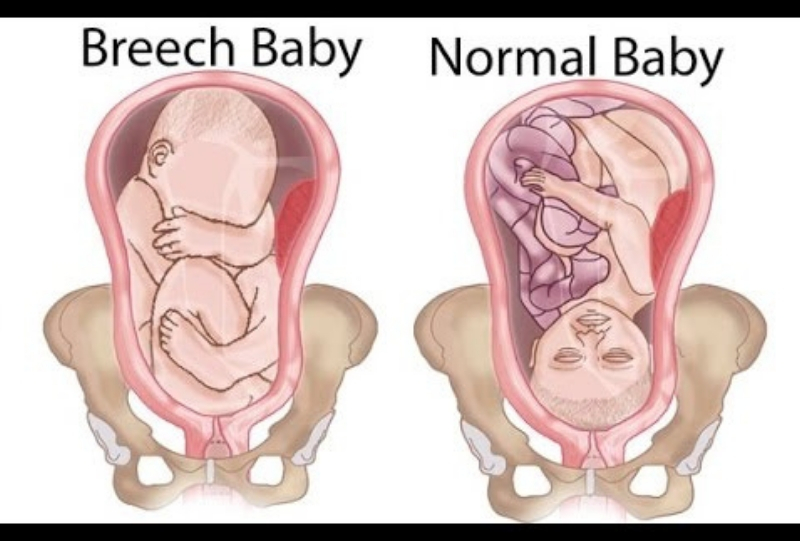
Most babies settle into a head-down position, ready for birth, by about the last month of pregnancy. Health professionals call this a ‘vertex’ or ‘cephalic’ position.
When a baby is positioned bottom-down late in pregnancy, this is called the breech position.
It is fairly common for a baby to be in a breech position before 35 to 36 weeks gestation, but most gradually turn to the head-down position before the last month.
Your doctor or midwife will feel your abdomen when you have your pregnancy check-ups in second and third trimesters — this is called an 'abdominal palpation'. When they feel your abdomen at 35 to 36 weeks, they will assess whether the baby has settled into a head-down position in preparation for birth. If they suspect your baby might be in a breech position, they can confirm this with an ultrasound scan.
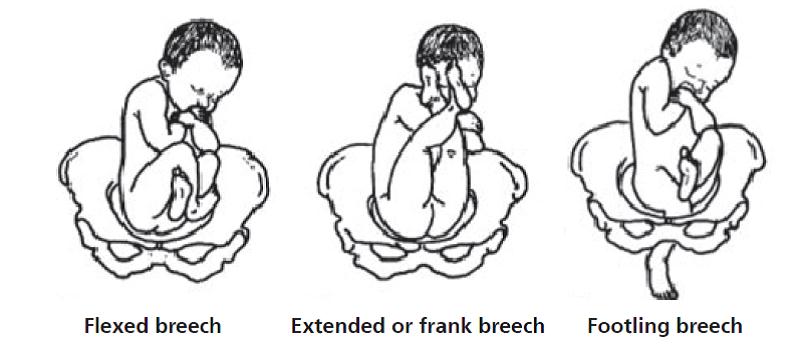
There are 3 main types of breech position. All of them involve the baby being in a bottom-down, head up, position. The variations of breech include:
- frank breech — the baby’s legs are straight up in front of its body in a V shape, so its feet are up near its face
- complete or flexed breech — the baby is in a sitting position with its legs crossed in front of its body and its feet near its bottom
- footling breech — one or both of the baby’s feet are hanging below its bottom, so the foot or feet are coming first
What does it mean for my baby?
While your baby is still in the womb, it is just as safe for them to be in a breech position as it is for them to be head-down. There are no long-term effects on children who were in a breech position during pregnancy. The birth process, however, is often more challenging when babies are still breech at the start of labour.
There are no long-term effects on children who were in a breech position during pregnancy. The birth process, however, is often more challenging when babies are still breech at the start of labour.
Why do some babies remain in a breech position?
Often it is unclear why a baby remains in a breech position. Some of the common reasons include:
- too much or too little amniotic fluid around the baby
- the length of the umbilical cord
- multiple pregnancy — for example, often one twin will be in a head-down position and the other in a breech position
- uterine fibroids
- an irregular size or shape of the mother’s uterus
Can my baby still turn after 36 weeks?
Some breech babies turn themselves naturally in the last month of pregnancy. If this is your first baby and they are breech at 36 weeks, the chance of the baby turning itself naturally before you go into labour is about 1 in 8. If you’ve already had a baby and this one is breech at 36 weeks, the chance of them turning naturally is about 1 in 3.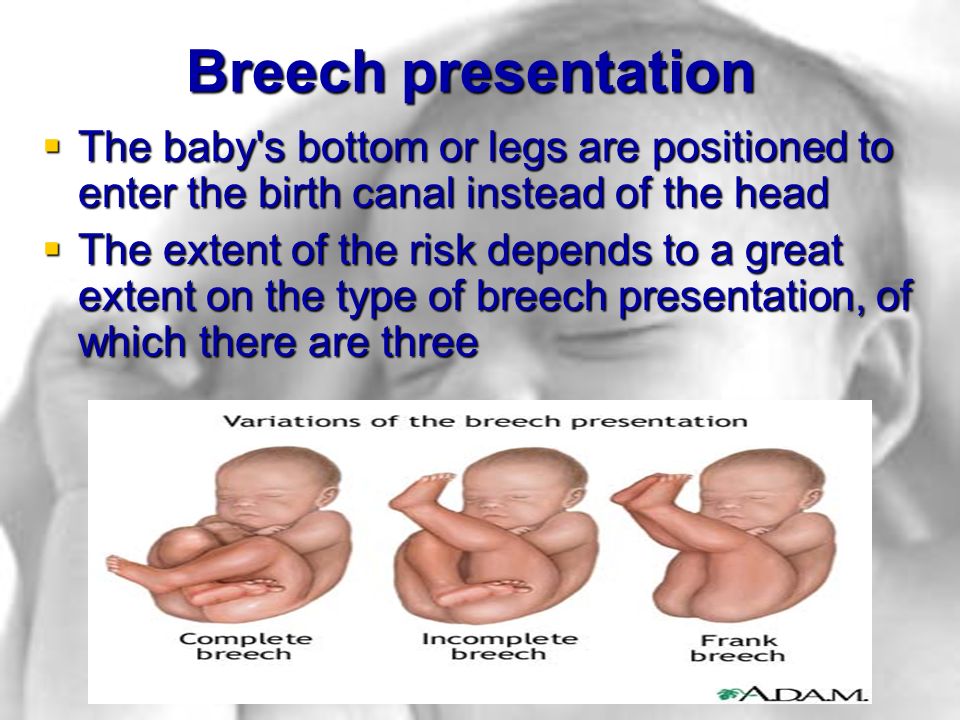
If your baby is in a breech position at 36 weeks, your doctor or midwife might suggest you think about an ECV, or external cephalic version, after 37 weeks. This will increase your chances of your baby turning to a head-down position. However, ECV is not suitable for everyone, so it’s important to discuss this option with your doctor or midwife.
Some people think that you might be able to encourage your baby to turn by holding yourself in certain positions, such as kneeling with your bottom in the air and your head and shoulders flat to the ground. Other options you might hear include acupuncture, a Chinese herb called moxibustion and chiropractic treatment. There is no good evidence that these work.
Talk to your doctor or midwife before trying any techniques to be sure they do not harm you or your baby.
What are my options if my baby is breech?
If you don’t have an ECV, or if you have it but it doesn’t work, then your options are to have an elective caesarean birth or to have a vaginal birth. Things may be different if you have had a caesarean section before — in this case, if you wish to explore the option of vaginal breech birth, you will need to discuss this with your obstetrician. You may be advised to have a caesarean section again.
Things may be different if you have had a caesarean section before — in this case, if you wish to explore the option of vaginal breech birth, you will need to discuss this with your obstetrician. You may be advised to have a caesarean section again.
Often, women are encouraged to have a caesarean birth if their baby is breech because it might be safer for the baby. But a vaginal birth is still an option in the right circumstances, such as:
- no other issues that would suggest a vaginal birth is unsafe, such as placenta praevia
- you are giving birth in facilities that can handle an emergency caesarean, if necessary
- you have an obstetrician or midwife who is skilled in vaginal breech births
What is involved in a vaginal breech birth?
When babies are in a cephalic (head-down position) ready for birth, the birth process is more straightforward because the crown of the baby’s head is born first. The head is the largest part of the baby’s body, so it makes way for the rest of the body to follow.
The birth process might be more challenging if your baby is breech. When a baby is born bottom first, the baby’s body is born before the largest part, its head. Often this doesn’t cause a problem. But there is a chance that the head, or the head and arms, may not follow easily, once the body is born. In this case, it is important that a midwife or obstetrician with skills and experience in breech births is present to assist your baby to be born.
Upright maternal positions, such as kneeling or a hands and knees position, are recommended when you give birth to a breech baby. The obstetrician or midwife will be standing by, observing closely, with a ‘hands off‘ approach, unless your baby's progress during the birthing process slows down. In such cases, there are a number of techniques that can be used to assist your breech baby to complete the birth vaginally, or it may be necessary to proceed to an emergency caesarean section.
The progress of your labour will be monitored closely. If there is any delay in the descent of your baby, a caesarean section might be recommended. This is because a delay in the baby’s descent inside may be an indication that the birth process could also be delayed, which is more risky for your baby.
If there is any delay in the descent of your baby, a caesarean section might be recommended. This is because a delay in the baby’s descent inside may be an indication that the birth process could also be delayed, which is more risky for your baby.
In many settings where vaginal breech births are offered, it is preferred that your baby is monitored continuously with a cardiotocograph (CTG). If available, you may prefer a cordless, waterproof CTG so you can remain upright and mobile, and so you can use the bath or shower for pain management during labour.
What should I ask my doctor or midwife?
It is worth discussing whether you might benefit from an ECV, because if this is successful, you can go on to try a vaginal birth.
You should also ask if:
- a vaginal birth is safe for the type of breech position your baby is in
- the health service you are planning to use can manage a breech vaginal birth
- your doctor or midwife has training and experience in managing a breech vaginal birth
Do all hospitals offer vaginal breech birth?
Not all hospitals have obstetricians and midwives on staff with the skills and experience in assisting women with a vaginal breech birth. If it is important to you, and your doctor or midwife can’t offer you a vaginal breech birth, you can ask to be referred to another health service.
If it is important to you, and your doctor or midwife can’t offer you a vaginal breech birth, you can ask to be referred to another health service.
What if I am planning a home birth and my baby is breech?
If you are planning a home birth, discuss options for your care with your midwife. The Australian College of Midwives and the Royal Australian and New Zealand College of Obstetricians and Gynaecologists recommend that you should be referred to an obstetrician if your baby is breech at the start of labour. This usually means being transferred to give birth in a hospital. In most cases, your midwife will be able to continue supporting you during your birth in hospital and also continue postnatal care at home after your baby is born.
Sources:
The Society of Obstetricians and Gynaecologists Canada (Breech childbirth), BioMed Central (Does moxibustion work? An overview of systematic reviews (BMC Research Notes 20103:284)), Department of Health (Clinical practice guidelines: Pregnancy care), Cochrane Library (Planned caesarean section for term breech delivery), NSW Health (Breech baby at term), SA Department for Health and Ageing (Perinatal practice guideline: Breech presentation), Australian College of Midwives (Transfer from planned birth at home guidelines), Royal Australian and New Zealand College of Obstetricians and Gynaecologists (Breech Presentation at the End of your Pregnancy)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: April 2020
Back To Top
Related pages
- External cephalic version (ECV)
Need more information?
Breech presentation and turning the baby
In preparation for a safe birth, your health team will need to turn your baby if it is in a bottom first ‘breech’ position.
Read more on WA Health website
Labour complications
Even if you’re healthy and well prepared for childbirth, there’s always a chance of unexpected problems. Learn more about labour complications.
Read more on Pregnancy, Birth & Baby website
Malpresentation
Malpresentation is when your baby is in an unusual position as the birth approaches. Sometimes it’s possible to move the baby, but a caesarean maybe safer.
Sometimes it’s possible to move the baby, but a caesarean maybe safer.
Read more on Pregnancy, Birth & Baby website
External cephalic version (ECV)
ECV is a procedure to try to move your baby if they are in a breech position to the head-down position.
Read more on Pregnancy, Birth & Baby website
Pregnancy at week 35
You'll probably be having lots of Braxton Hicks contractions by now. It's your body's way of preparing for the birth. They should stop if you move position.
Read more on Pregnancy, Birth & Baby website
Pregnancy at week 28
You are now in the third trimester and you'll probably be feeling many of the common discomforts of pregnancy, like a sore back, swelling, heartburn or cramps.
Read more on Pregnancy, Birth & Baby website
Anatomy of pregnancy and birth - pelvis
The pelvis helps carry your growing baby and is especially tailored for vaginal births. Learn more about the structure and function of the female pelvis.
Read more on Pregnancy, Birth & Baby website
Pregnancy at week 32
Your baby doesn't have a lot of room, but they will still be moving. The extra weight might cause you some back and pelvic pain which can make it difficult for you to move around.
Read more on Pregnancy, Birth & Baby website
Pregnancy at week 39
Your baby's weight gain should slow down since they are now ready to be born. You might soon start to notice the early signs of labour.
You might soon start to notice the early signs of labour.
Read more on Pregnancy, Birth & Baby website
Having a baby
The articles in this section relate to having a baby – what to consider before becoming pregnant, pregnancy and birth, and after your baby is born.
Read more on WA Health website
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now entering.
OKNeed further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.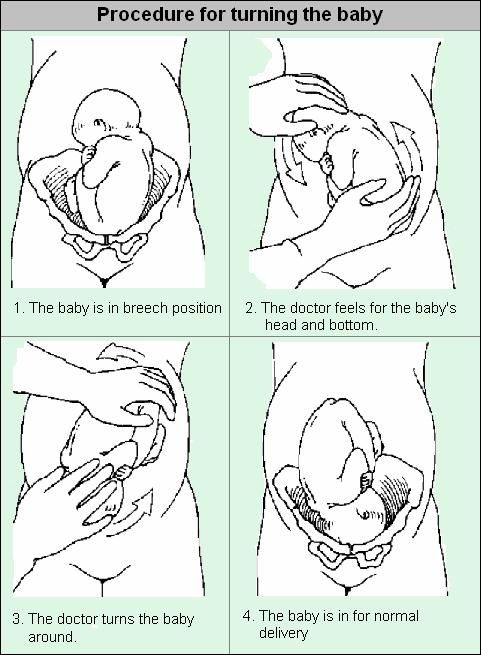
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
When Is Breech an Issue?
The later in pregnancy a baby is breech, the more difficult it is for the baby to flip head down. The baby’s size grows in relation to the uterus and there is a smaller percentage of amniotic fluid for the baby to move freely. The more complicated past births were due to fetal position, the earlier I suggest starting to get your muscles unwound and your pelvis aligned. If a previous baby remained either breech or posterior until birth, I suggest bodywork throughout the pregnancy.
If a previous baby remained either breech or posterior until birth, I suggest bodywork throughout the pregnancy.
In time, the breech baby’s head becomes heavy enough (between 5-7 months) for gravity to bring the head down in a symmetrical womb. The baby will move head down if there is room or if there is tone in the support to the uterus to direct the baby head down.
Common issues with breech:
- Health of the baby overall
- Safety of the birth
- Safety for the mother facing surgical birth
- Emotions of the birthing parent(s)
When should I be concerned about a breech position?
During the month before 30 weeks, about 15% of babies are breech. Since breech baby’s spine is vertical, the womb is “stretched” upwards. We expect babies to turn head down by 28-32 weeks.
Breech may not be an issue until 32-34 weeks. If you know your womb has an unusual limitation in shape or size, such as a bicornate uterus then begin body balancing before pregnancy and once 15 weeks in pregnancy. In this case, the baby needs to be head down much earlier so that the uterus still has the room for baby to turn. Every unique womb is unique so these dates are theoretical, not absolute.
In this case, the baby needs to be head down much earlier so that the uterus still has the room for baby to turn. Every unique womb is unique so these dates are theoretical, not absolute.
The timeline for breech
This is a timeline of what to do and when to do it in order to help a breech baby move head down:
- Before 24-26 weeks, most babies lie diagonally or sideways in the Transverse Lie position.
- Between 24-29 weeks, most babies turn vertical and some will be breech.
- By 30-32 weeks, most babies flip head down and bottom-up.
- By 34 weeks pregnant, the provider expects the baby to be head down.
- Between 36-37 weeks, a provider may suggest an external cephalic version.
- Full term is from 37-42 weeks gestation, and about 3-4% of term babies are breech.
The medical model of care addresses the breech position between 36-37 weeks, when baby’s survival outside the womb won’t include special nursery care to breathe or suck. Physicians Oxorn and Foote, however, recommend helping babies turn head down at 34 weeks. Some home birth midwives suggest interacting with a baby at 30-34 weeks to encourage a head-down position (vertex).
Women who have had difficult previous births due to posterior, asynclitism, or a labor that didn’t progress, may want to begin bodywork and the Forward-leaning Inversion as soon as the second trimester of pregnancy (after morning sickness is gone and extra things like fetal positioning activities can be thought about).
Here is a general guideline for the average pregnancy:
10-24 weeks gestationThis is the time when fetal position is generally determined, even though the baby’s final position isn’t typically set before 34 weeks gestation. How can this be? The body has a habit, so to speak, of how the soft tissues, ligaments, muscles, and alignment of the pelvis and whole body is set. The baby simply follows this basic pattern. By adding body balancing now, the baby has an increased chance of ideal positioning for labor at 34 weeks and beyond.
The baby simply follows this basic pattern. By adding body balancing now, the baby has an increased chance of ideal positioning for labor at 34 weeks and beyond.
Routine good posture with walking and exercise will help most babies be head down as the third trimester gets underway. A 30-second inversion is good practice for everyone. Unless you have a medical reason not to, please consider the Forward-leaning Inversion. If you have a history of car accidents, falls, uncomfortable pregnancies, hormonal imbalance, or a previous breech or posterior baby, then begin the inversion and body work before or during early pregnancy.
Oxorn and Foote recommend external version at 34 weeks, but most doctors want to wait for the baby’s lungs and suck reflex to be more developed in case the maneuver goes wrong and starts labor or pulls the placenta off the uterine wall. There is often enough amniotic fluid for an easy flip before 35 weeks.
- Inversion: Use of maternal positions that put the mother upside down may help a baby use gravity to flip.
 Get i
Get i Dad’s the hero in this “over the top” support to help his mate do a Breech Tilt in the comfort of a bed!
nto the position you want your baby to be in. Inversions give a static stretch to uterine ligaments which, when followed by a swing back up to sitting tall over a neutral pelvis helps realign cervical ligaments and may make more room for the baby’s head. Start with a 30-seconds to 2 minutes of Forward-leaning Inversion.
- Breech Tilt: Follow the FLI with the Breech Tilt for 10-20 minutes. This allows you to tuck your chin while upside down on a similar slanted surface. Use an ironing board against the couch, for instance.
- Open-knee Chest: Open-knee Chest has been studied and shown to help breeches flip. I like inversion positions that allow the mother to tuck her own chin. Myofascial workers tell me this relaxes her pelvis, whereas extending the chin tightens the pelvis.
- Professional bodywork: Acupuncture and Moxibustion both have good statistics for flipping breeches. Find out if there’s a Spinning Babies® Aware Practitioner in your area.
- Therapeutic massage: There are muscle/fascia attachments at the base of the skull, respiratory diaphragm, inguinal ligament, and even the hip sockets! We are whole organisms, not machines with reproductive parts.
- Chiropractic or Osteopathic: Spinal adjustmentsof the neck do improve pelvic alignment, especially if accompanied by fascial release. Not all chiropractors are trained in soft tissue body work, however. And not all soft tissue work is equal. This is why we promote our Aware Practitioner Workshops for bodyworkers.
Should manual external cephalic version be done earlier?
A few midwives recommend version (manually turning the breech baby to head down) at 30 –31 weeks.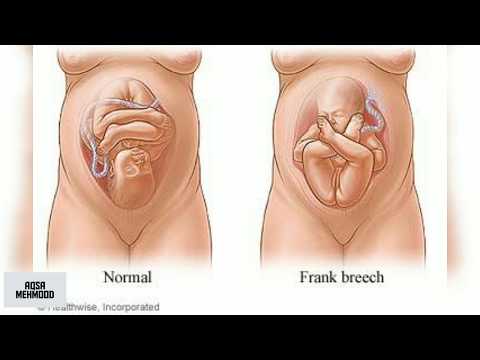 Anne Frye, author of Holistic Midwifery, reported a very low incidence of breech at term when her midwifery group manually rotated babies during this gestational age.
Anne Frye, author of Holistic Midwifery, reported a very low incidence of breech at term when her midwifery group manually rotated babies during this gestational age.
Attempting to turn the baby now is over a month before the medical model of turning breeches. Utmost gentleness must be the protective factor. If forcing a baby to turn harms the baby or placenta, the baby is too young to be cared for outside of the Neonatal Intensive Care Unit.
Midwives who turn babies now believe there is less chance of hurting a baby and proceed very carefully, stopping at once if there is resistance. Typically, there is less resistance from the uterus because there is more fluid and the baby is still very small.
Body work is suggested before attempting this, especially for first-time moms or women who had a difficult time with their first birth. There are risks to a manual version, so the baby should be monitored closely in between each 10-30 degrees of rotation.
35-36 weeksIf your baby is breech during this time your doctor or midwife will begin to talk about how to help the baby flip head down, and possibly about scheduling a manual version for 36-37 weeks. Getting body work and having acupuncture or homeopathy may help soften the ligaments and a tense uterus to either help the baby flip spontaneously or to allow more success in an attempt at a version.
Getting body work and having acupuncture or homeopathy may help soften the ligaments and a tense uterus to either help the baby flip spontaneously or to allow more success in an attempt at a version.
During this time, you can continue with the suggestions in the “Professional Help” page. Also, an obstetrician may suggest manually flipping the baby to a head down position at this time. A few midwives will also offer this, perhaps even earlier, at 30-34 weeks.
NOTE: Don’t let someone manually flip your baby without using careful monitoring of the baby’s heartbeat. Accidents can occur, even when there is good intention. The baby must be listened to and the version stopped immediately if the heart rate drops.
External cephalic version near the end of pregnancy
You may also agree to go through with a cephalic version at this time. The baby is in the womb with the cord and placenta and there is a small risk in turning the baby manually. This maneuver should be done with monitoring by experienced professionals, in a setting ready for a cesarean if needed.
This maneuver should be done with monitoring by experienced professionals, in a setting ready for a cesarean if needed.
There is about a 40-50% chance this will be successful. Sometimes the baby moves easily and sometimes the procedure is painful. I believe it’s important who performs it, and that ligament tightness would make this more uncomfortable. I suggest getting chiropractic, myofascial, acupuncture, homeopathy, or moxibustion (or all of these) before and after the version.
Doing the Three Sisters of BalanceSM (or following the Turning Your Breech Baby guidelines) daily beforehand and just before the procedure would be relaxing and helpful. More birth professionals are using our approach in the hours or the week before the procedure and report that fewer procedures are necessary and those that are seem to be easier than average to do when the baby is able to be turned.
38-40 weeksSometimes a woman and her caregiver don’t know the baby is breech until this point or until labor.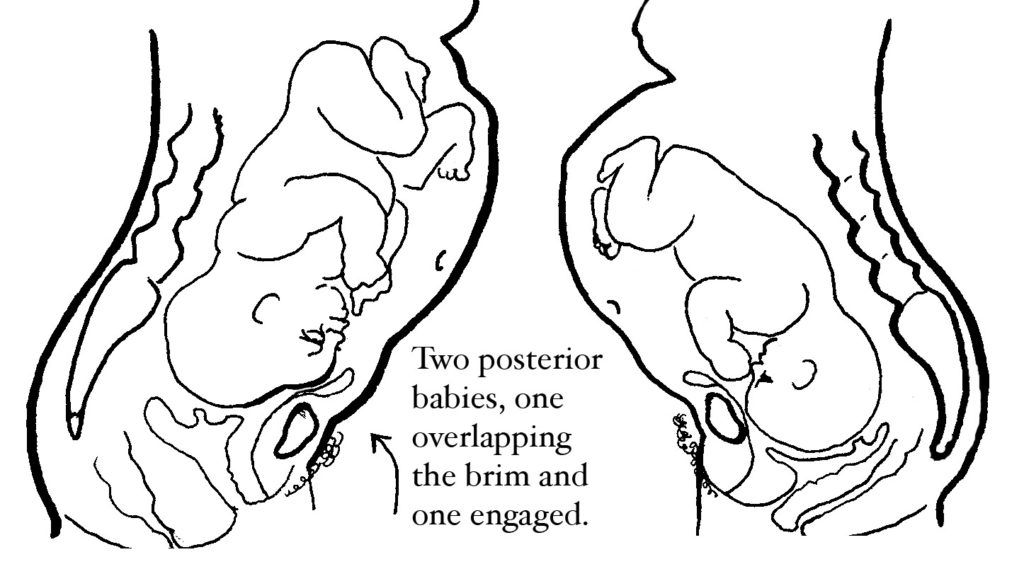 Rarely does a baby flip to breech this late in pregnancy but they can. Parents and providers may learn that baby is breech during a routine bio-physical ultrasound exam during this time or later in pregnancy.
Rarely does a baby flip to breech this late in pregnancy but they can. Parents and providers may learn that baby is breech during a routine bio-physical ultrasound exam during this time or later in pregnancy.
An external cephalic version may yet be successful, depending on the fluid level and the flexibility of the uterus, the baby’s head position and location, a uterine septum, where the placenta is, etc.
It is still possible that the baby flips doing body balancing activities or even labor itself (contractions might be the very action that turns baby in about 1% of breeches). You may find turning easier if you keep doing the activities listed above.
40-41 weeksThough many breeches are born about 37-39 weeks gestation, some will happily go to 41 or 42 weeks. For a head down baby, 41 weeks and 1 to 3 days is a common time for labor to begin on its own. SStarting labor at this gestation can certainly be normal for a healthy breechling, too.
If the pregnant person has a tendency to be somewhat overweight or lower energy, which can indicate low thyroid function, a longer pregnancy may be more likely.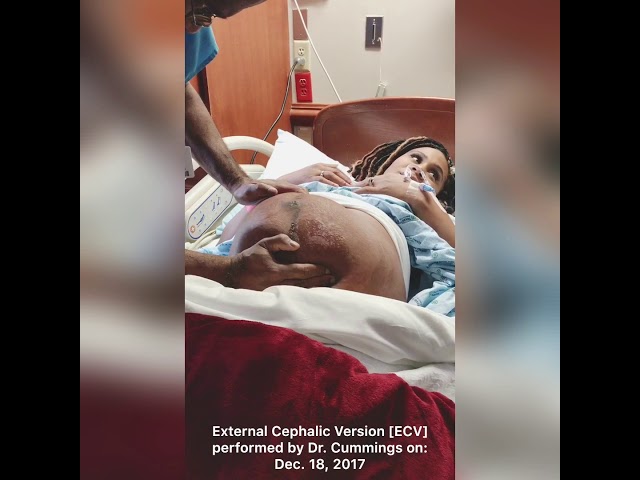 This tendency deserves looking after. Well-nourished and peppy women may also go a full pregnancy length, of course.
This tendency deserves looking after. Well-nourished and peppy women may also go a full pregnancy length, of course.
Going into labor and then having a planned cesarean is recommend by Dr. Michel Odent in his book, Cesarean. Going into labor spontaneously is safer for the breech vaginal birth, as well. Women who are trying to flip their baby often find it necessary to slow down the efforts and come to terms with a breech birth.
When facing a cesarean, it can be nurturing to you and your baby to plan a cesarean with skin-to-skin, delayed cord clamping, and breastfeeding on the operating room table or in the recovery room. Give yourself some time and compassion to feel your feelings and explore your options to adapt to the options you have available to you.
Postdates (after your due date) with a breechWith a breech, going all the way to 42 weeks may or may not be more of an issue. Some providers will have to end any plans for a vaginal birth by now. Midwifery statutes often limit midwifery care out of the hospital to 37-42 weeks (or 36-43, depending on where you live).
Midwifery statutes often limit midwifery care out of the hospital to 37-42 weeks (or 36-43, depending on where you live).
After 42 weeks, the baby’s skull bones are setting up more firmly and a vaginal birth is less favorable. I’ve been to a few breech births after 42 weeks gestation and everything went very well. But, I do sometimes wonder why labor isn’t starting and if metabolism is a reason, especially when there’s been regular bodywork for weeks.
For a person carrying a breech baby who does show signs of low thyroid function or otherwise a “sloshy” metabolism, I am inclined to transfer care to a kind hospital provider at 41.5 weeks. Intelligent and experienced monitoring may rule out issues that arise post dates that may complicate labor. With slow metabolism postdates issues with breech position may need extra attention before 42 weeks.
If Baby Does Not Turn
Not every breech baby will turn on their own. Not every attempt at an External Cephalic Version works (It’s often 50-50).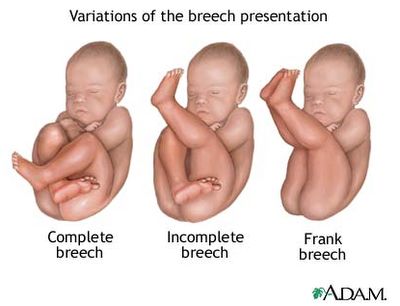 Adding body balancing has abundant anecdotal reporting to show success. But this balancing should be individualized if the pregnant person has followed general guidelines closely for 1-2 weeks without success.
Adding body balancing has abundant anecdotal reporting to show success. But this balancing should be individualized if the pregnant person has followed general guidelines closely for 1-2 weeks without success.
Be compassionate to you and your baby. You are both doing the best you can with the resources you have.
Choose your path. Sometimes it may feel like you don’t have a choice. Consider why it feels that way. Perhaps your choice is safety over manner of birth? That’s totally valid. Just because a vaginal birth might be available to some doesn’t mean it is your first choice, too.
Sometimes babies choose, too. The labor goes too fast to do surgery for the birth. Or, the baby doesn’t come into the pelvis and surgical birth is necessary. (Remember reaching in and pulling out the baby is not reasonable if a cesarean is available in the region unless this is a second twin (subsequent triplet) or travel is impossible due to weather, war, or whatever reason. Life is real. Babies don’t follow a script. Be real with your own experience.
Be real with your own experience.
Inducing a breech
Inducing a breech is not recommended in out of hospital settings. Even in the hospital, the risk rises. In some areas where breech is common, Pitocin/Syntocin inductions are done with outcomes that are good enough to keep the options open. Induction by herbs is also considered out of scope for breech.
We need to respect the breech and not stress the baby, especially in settings where we don’t have the rescue setup to solve any potential problems. Try body balancing and see if labor begins on its own. That would be a non-invasive, non-manipulating approach.
The Breech Turned During LaborIt is a rare possibility that the baby flips to head down during labor. I once assisted a midwife who’s laboring mother’s water had released. Her labor was mild and not picking up, so after 24 hours we transferred and found that the baby had flipped. The doctor thought we’d misdiagnosed, but the mother’s abdomen was so thin we could feel the baby’s knuckles and elbow and found the baby in the opposite direction after entering the hospital!
Another mother had Dynamic Body Balancing in early labor with one of Dr.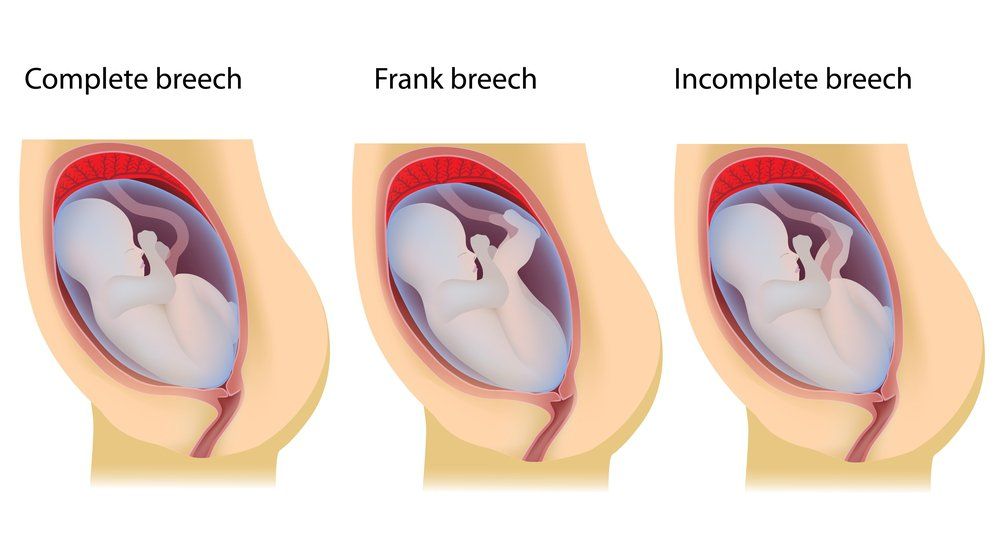 Carol Phillips students who was also a midwife. Her breech baby turned head down during transition phase of labor!
Carol Phillips students who was also a midwife. Her breech baby turned head down during transition phase of labor!
If the plan is to have a cesarean once labor begins, call the hospital and alert them of labor immediately. Go to the hospital right away. Breech births can go quite quickly and you want to be where people are ready to help you. If you plan to have a vaginal birth, don’t delay in getting to your birth location or getting your birth team to you.
While it can be totally normal to have a 24-hour or longer breech birth, many breech labors are quite short. Because the softer bottom is first, it may take you by surprise that you are progressing with such little pain (though some breech births are as painful as head down births). Just don’t base your decision to get to the hospital on your pain level!
A cesarean can be more complicated if the baby is wedged low in the pelvis. That is why there is a recommendation to have the cesarean in early labor. But cesareans are done everyday with head down babies low in the pelvis. Sometimes it’s how it is.
Sometimes it’s how it is.
Starting labor in and of itself doesn’t make the surgery more dangerous. Rushing around and doing things in a hurry might. Alert your hospital before labor and again once you start labor. Be firm that you know what you are about and that they need to get the Operating Room ready while you are on your way.
Mostly, a leisurely transition into the hospital can be sustained with a sense of humor and practicality. There can be a sense of calm while you and the staff take the steps to welcome your baby. This is your birth. Be present with how your experience unfolds.
After the birthWhile the concern about breech position is during the birthing, when the baby is breech for most of the third trimester, their skull bones become shaped by the inside of the upper womb (the fundus). This isn’t typically an issue but can be noticed.
Craniosacral therapy can gently (and without using force) reshape the baby’s head, ideally during the month or two after birth. Surgery on baby’s skull is seldom necessary after 3-6 sessions with a Craniosacral therapist. For most breech babies, this issue is not present. I list is here because I have heard some assumptions that can be dispelled.
Surgery on baby’s skull is seldom necessary after 3-6 sessions with a Craniosacral therapist. For most breech babies, this issue is not present. I list is here because I have heard some assumptions that can be dispelled.
A question about breech
Email from Wed, Feb 11, 2009:
…I’m 30 weeks and the baby is what I’d describe as oblique breech – his head is on my right side next to my belly button, his hips/butt are in my pelvis on the lower left side (my left) and his feet are in front of his face. I think he’s facing forward – towards my belly button. I’ve known this for weeks just because his big head is so hard I always bump that spot on accident. …. my first son was 9 lbs and born posterior, so I’m really hoping this baby is in the ideal position for delivery… so both of these things make me nervous that he won’t move. He has been in this position for a few weeks now. … Anyway, just wondering if I should worry and what, if anything, I can do to help him move now.
My Midwife suggested a Chiropractor that can do some adjustments. I’d like to do the couch inversion too. Would it help for me to walk more? Also, should I sleep more on one side than the other? Thanks for your help! Great site!
Gail’s reply:
Hi…. now is a good time to take action, not so much that your baby is breech, but because your first baby was OP. You see, a pelvic misalignment and/or round ligament spasms (they often go together) can result in either a breech or a posterior fetal position. So, a breech will often flip to a posterior position and may stay that way unless you resolve the underlying issue. Maternal positioning is often not enough by itself to correct a posterior fetal position when there is a history of previous posterior or breech babies. While certainly most breech babies flip head down, it’s beneficial to help correct the symmetry of your uterine ligaments now, while the baby is still small enough to have plenty of room to flip head down once the reason for the previous posterior position is remedied.
See some things a Chiropractor can do for breech and posterior by reading Professional Help.
Videos
Daily Essentials
Daily Essentials can be practiced daily throughout pregnancy to help bring balance and comfort — and an easier, shorter birth.
Learn More
Spinning Babies® Parent Class
Spinning Babies® Parent Class provides clear instructions on how to use Spinning Babies® for a more comfortable and confident pregnancy and labor.
Learn More
Featured Products
Shop Spinning Babies®
State children - Vlast - Kommersant
There are 72,000 orphans and children left without parental care in Russia. Once in the state system, these children often lose their rights.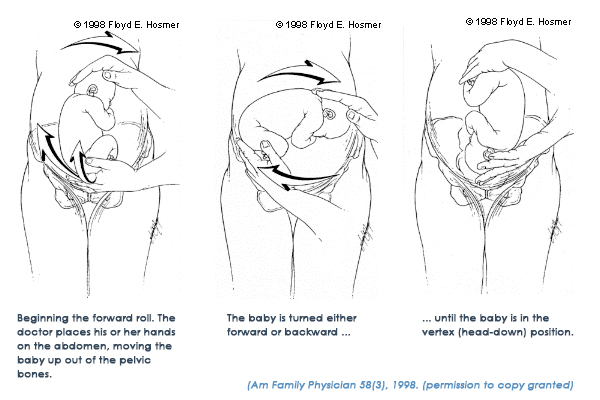 Despite the fact that the priority of the interests of the child is enshrined in Russian law, in real life, political or corporate interests are more important.
Despite the fact that the priority of the interests of the child is enshrined in Russian law, in real life, political or corporate interests are more important.
"Fortune smiled on the child - but he is denied the right to a normal human life for some strange reasons" (on the photo - Elya with Yulia Beisenova)
Photo: From the personal archive
Olga Allenova
"Because of some mythical threat, the child was locked up in the orphan system"
Elvira is four years old, she has been living in an orphanage in Primorsky Krai since birth. In June 2014, German residents Julia and Ali Beisenov found out about her. Julia is a Russian-speaking citizen of Germany, a programmer, Ali is a citizen of Kazakhstan, an individual entrepreneur. They have three biological children. “I was a volunteer in the Children in Need project of the Russian Foundation Volunteers to Help Orphans,” says Yulia. “As part of this program, we were looking for medical clinics for orphans with developmental disabilities and in need of treatment.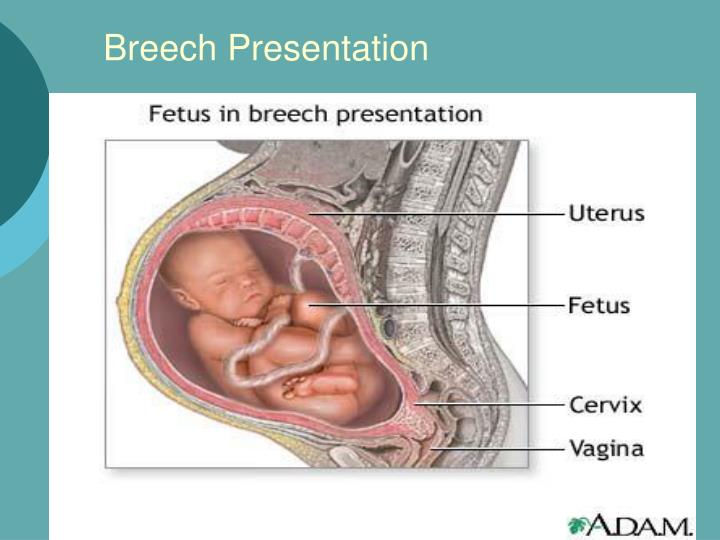 So I I learned that Elya lives in Primorye, whose arms and hands were deformed due to intrauterine disorders.The child cannot dress independently, fully play with her peers, because of this she lags behind in physical development, although she is a wonderful girl with great potential We found two clinics in Germany that specialize in the treatment of hand pathologies in children and are ready to accept Elya for treatment and rehabilitation." At first, the Beisenovs did not think about adopting Elvira - they just wanted to help her with treatment. “But we thought and talked a lot about her, and gradually, when we realized how much work the doctors had to do and what prospects Eli had, we decided that our family could help her,” says Yulia. “We have a large family, our parents live near us, they took our decision positively."
So I I learned that Elya lives in Primorye, whose arms and hands were deformed due to intrauterine disorders.The child cannot dress independently, fully play with her peers, because of this she lags behind in physical development, although she is a wonderful girl with great potential We found two clinics in Germany that specialize in the treatment of hand pathologies in children and are ready to accept Elya for treatment and rehabilitation." At first, the Beisenovs did not think about adopting Elvira - they just wanted to help her with treatment. “But we thought and talked a lot about her, and gradually, when we realized how much work the doctors had to do and what prospects Eli had, we decided that our family could help her,” says Yulia. “We have a large family, our parents live near us, they took our decision positively."
The Department of Education of the Primorsky Territory told the Beisenovs that Elvira could be adopted by foreign citizens, because during the four years of her life, none of the Russian candidates for adoptive parents wanted to take her into the family.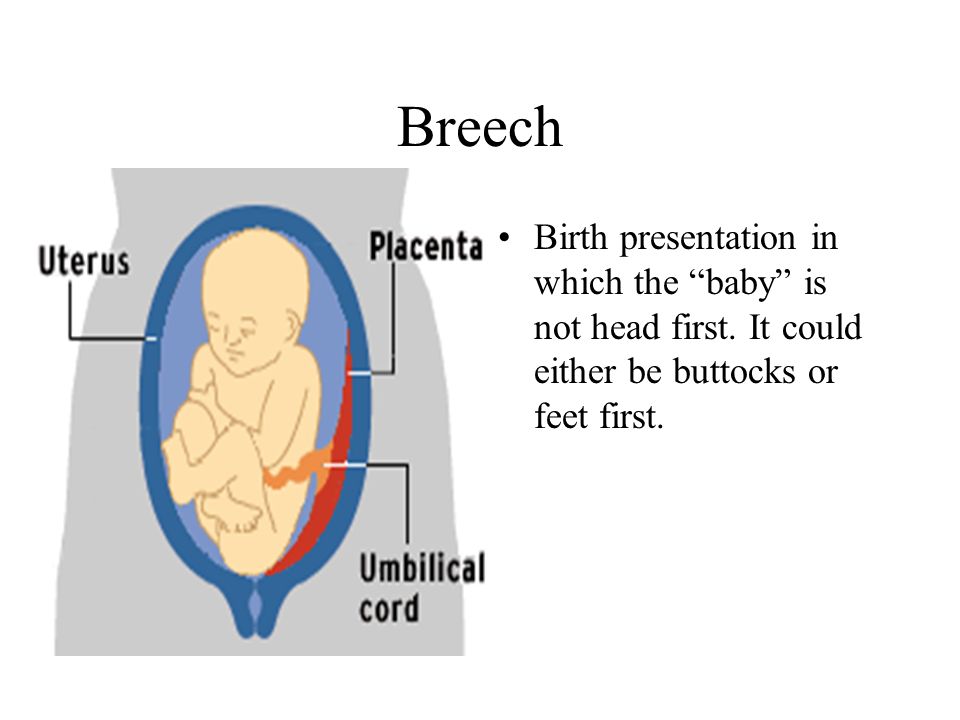 Then, in the court decision, an entry will appear: "In the period from 2011 to 2014, candidates for adoptive parents from Russian citizens (20 families) were familiarized with information about the child, but refused to be sent to visit him for health reasons." The Beisenovs began to collect documents: they went through the school of adoptive parents, visited doctors and social services. We went to a psychiatrist who gave a conclusion that they are a heterosexual couple and there is no evidence that they can change their orientation. By March 2015, the package of documents for the adoption of Elvira was ready, the Beisenovs received the status of candidates for foster parents in Russia and went to Primorsky Krai to get acquainted with the child. “We arrived at the orphanage and immediately realized that we were doing all this for good reason,” Yulia recalls. “This little man turned out to be so ours that we didn’t want to leave her. We couldn’t promise her anything, because we understood that everything depends from the court.
Then, in the court decision, an entry will appear: "In the period from 2011 to 2014, candidates for adoptive parents from Russian citizens (20 families) were familiarized with information about the child, but refused to be sent to visit him for health reasons." The Beisenovs began to collect documents: they went through the school of adoptive parents, visited doctors and social services. We went to a psychiatrist who gave a conclusion that they are a heterosexual couple and there is no evidence that they can change their orientation. By March 2015, the package of documents for the adoption of Elvira was ready, the Beisenovs received the status of candidates for foster parents in Russia and went to Primorsky Krai to get acquainted with the child. “We arrived at the orphanage and immediately realized that we were doing all this for good reason,” Yulia recalls. “This little man turned out to be so ours that we didn’t want to leave her. We couldn’t promise her anything, because we understood that everything depends from the court. We just told her: "We are Yulia and Alik, we came to visit you to play." But from the second we met, she began to tell everyone that we were her mom and dad."
We just told her: "We are Yulia and Alik, we came to visit you to play." But from the second we met, she began to tell everyone that we were her mom and dad."
In the spring of 2015, the Beisenovs met with Elya six times. In September, before the court session - again. From March to September, they called Elya and talked to her on the phone, sent her their videos, and from the orphanage they received video frames in which Elya sang songs for them.
At the court hearing on September 4, the prosecutor and guardianship authorities supported the Beisenovs, saying that adoption into this family was in the interests of the child. However, the Primorsky Regional Court refused to adopt Elvira to the Beisenovs. “We assumed that they might refuse us, because back in August we were told that it was possible not to come to the court session,” Yulia says. “But still we could not believe that this was possible. A child with a disability needs a family, care , treatment, and he was deprived of such an opportunity. They received the reasoning decision of the court only nine days later. It states that under German law, an adopted child can be re-arranged in another family, and since same-sex partnerships are allowed in Germany, theoretically a child may end up in a same-sex family. In addition, the court decision states that there is no cooperation agreement between the Russian Federation and Germany, which would stipulate that a decision to relocate a child to another family cannot be made without the consent of the relevant competent authority of the Russian Federation. According to the court, the inability to control the placement of Elvira in another family in the event of a need for reorganization violates the rights of the child.
They received the reasoning decision of the court only nine days later. It states that under German law, an adopted child can be re-arranged in another family, and since same-sex partnerships are allowed in Germany, theoretically a child may end up in a same-sex family. In addition, the court decision states that there is no cooperation agreement between the Russian Federation and Germany, which would stipulate that a decision to relocate a child to another family cannot be made without the consent of the relevant competent authority of the Russian Federation. According to the court, the inability to control the placement of Elvira in another family in the event of a need for reorganization violates the rights of the child.
Germany is not included in the list of countries where adoption from Russia is prohibited. The judge was just insured just in case
"We are young, we have a strong family, our relatives and parents live not far from us," says Yulia. values. It does not allow same-sex marriage. Yes, same-sex partnerships are allowed, but they are prohibited from adopting children. It turns out that due to some mythical threat of reorganization into a same-sex family, the child was locked up in the orphan system. If the court decision remains in force, until For 18 years, Elya will live in an orphanage, and then she will go through the stage - to a PNI or a home for the disabled.
Yes, same-sex partnerships are allowed, but they are prohibited from adopting children. It turns out that due to some mythical threat of reorganization into a same-sex family, the child was locked up in the orphan system. If the court decision remains in force, until For 18 years, Elya will live in an orphanage, and then she will go through the stage - to a PNI or a home for the disabled.
The Beisenovs' lawyer Alexander Golovanov calls the decision of the judge of the Primorsky Regional Court Solovieva "pure arbitrariness": "There are no grounds for refusing to adopt, I have not seen a more ideal family than the Beisenovs. This is a heterosexual family, immigrants from the USSR, they speak Russian, they have children, prosperity and a desire to help Ela. The child was lucky - but he is denied the right to a normal human life for some strange reasons. Germany is not on the list of countries where adoption from Russia is prohibited. The judge is just in case insured."
In October, Yulia Beisenova wrote an appeal to the Ministry of Education of the Russian Federation with a request to answer the question whether the adoption of Russian orphans to Germany is allowed. In November, she received a response from the department, which reported that in 2014, 44 children were adopted (adopted) by German citizens, of which two were disabled children, and as of November 26, 2015, German citizens adopted 30 children in Russia.
In November, she received a response from the department, which reported that in 2014, 44 children were adopted (adopted) by German citizens, of which two were disabled children, and as of November 26, 2015, German citizens adopted 30 children in Russia.
"If last year 44 children were adopted to Germany from Russia, then the question arises: who is right - the courts of the Russian Federation, which allowed German citizens to adopt Russian orphans 44 times in 2014 alone, or a judge of the Primorsky Regional Court? Well, not the state can make a mistake 44 times. It means that an erroneous decision was made in the case of Eli,” explains lawyer Golovanov. According to him, the concept of marriage is enshrined in German law - this is a union between a man and a woman: "Taking into account the humanistic approach to the individual, the German state made it possible for people to register same-sex partnerships in order to regulate relations by inheritance, joint use of property. But partnership is not a marriage, and the law forbids the adoption of children by such partners. If it were otherwise, Russia would not have allowed so many adoptions to Germany. I regard the decision of the Primorsky Regional Court as a deliberate act against the child, dooming the child to worsening his living conditions and slow dying. The judge violates the Russian legislation in which the interests of the child are declared a priority. I hope that the actions of the judge will be given an appropriate assessment by the Supreme Court of the Russian Federation."
If it were otherwise, Russia would not have allowed so many adoptions to Germany. I regard the decision of the Primorsky Regional Court as a deliberate act against the child, dooming the child to worsening his living conditions and slow dying. The judge violates the Russian legislation in which the interests of the child are declared a priority. I hope that the actions of the judge will be given an appropriate assessment by the Supreme Court of the Russian Federation."
The Beisenovs were supported by Pavel Astakhov, Commissioner for Children's Rights in the Russian Federation. Its conclusion states that the conclusions and decision of the Primorsky Regional Court are "erroneous", and the adoption of Elvira by the Beisenov spouses "will fully meet her interests." “If the Beisenov’s adoptive parents, for whatever reason, cannot fulfill their parental responsibilities in relation to Elvira, the child cannot be re-arranged in a “same-sex family,” since German law does not provide for the possibility of such a re-arrangement,” Astakhov said in the conclusion. In addition, the children's ombudsman considered groundless the judge's conclusions that Russia and Germany do not have an agreement on monitoring the living conditions and upbringing of children adopted in Russia. Such control on the territory of Germany is carried out by the organization "Centrumfür Adoptionen" - as Pavel Astakhov writes in the conclusion, the authority of the organization is confirmed by a certificate dated May 21, 2014, issued by the Central Department for Adoption of the Union of Communities for Youth Affairs and Social Policy of Baden - Württemberg. The representative office of the same organization in Russia has permission to exercise control from the Ministry of Education and Science of the Russian Federation (order N88 of February 1, 2010). Thus, interstate cooperation in matters of control over the fate of children adopted in Russia and living in Germany is confirmed.
In addition, the children's ombudsman considered groundless the judge's conclusions that Russia and Germany do not have an agreement on monitoring the living conditions and upbringing of children adopted in Russia. Such control on the territory of Germany is carried out by the organization "Centrumfür Adoptionen" - as Pavel Astakhov writes in the conclusion, the authority of the organization is confirmed by a certificate dated May 21, 2014, issued by the Central Department for Adoption of the Union of Communities for Youth Affairs and Social Policy of Baden - Württemberg. The representative office of the same organization in Russia has permission to exercise control from the Ministry of Education and Science of the Russian Federation (order N88 of February 1, 2010). Thus, interstate cooperation in matters of control over the fate of children adopted in Russia and living in Germany is confirmed.
The Beisenovs' appeal against the decision of the Primorsky Regional Court will be considered by the Supreme Court of the Russian Federation on 15 December. If the Supreme Court cancels the decision of the Primorsky Regional Court, Elya will be able to celebrate the New Year in the family and after some time will forget her state life, which depended on the decision of strangers who interpret the legislation in their own interests.
If the Supreme Court cancels the decision of the Primorsky Regional Court, Elya will be able to celebrate the New Year in the family and after some time will forget her state life, which depended on the decision of strangers who interpret the legislation in their own interests.
"There was no Lera's profile, but I know that she is in an orphanage"
Three years ago, the "Dima Yakovlev law" was adopted in Russia, which prohibits the adoption of Russian orphans in the United States. 196 children who met American candidates for foster parents and were awaiting adoption remained in Russia. "Vlast" followed the fate of these orphans for three years. The regional authorities tried to arrange children from the "American list" in the first place, because this topic turned out to be one of the most painful for Russian society. In the very first year, children without disabilities or children with disabilities, but with intact intelligence, were taken to families. The growth of domestic adoption was influenced by special measures taken by the government at the end of 2012: in particular, lump-sum federal payments for the adoption of children over seven years old and siblings, lump-sum regional payments, some simplification of the procedure for registration of custody and reporting of adoptive parents. In some regions, in order to stimulate adoption, the authorities even went to the issuance of social apartments to foster families. So, in Moscow, a foster family that has taken up at least five children, of which three are older children or children with disabilities, can count on a social apartment.
In some regions, in order to stimulate adoption, the authorities even went to the issuance of social apartments to foster families. So, in Moscow, a foster family that has taken up at least five children, of which three are older children or children with disabilities, can count on a social apartment.
However, children with Down syndrome or autism are still reluctant to be adopted by families. So, last year, 40 children remained on the "American list", about half of them with Down syndrome and complex genetic diagnoses, and the second half were children over ten years old, teenagers. By the end of 2015, the "American list" was significantly reduced: now there are only 15 children in it (their profiles are presented in the Federal Data Bank of Orphans and Children Left Without Parental Care, FBD). Pavel Astakhov, the commissioner for children's rights in the Russian Federation, claims that the list is much smaller, and the profiles of children placed in families have not yet been removed from the FBI.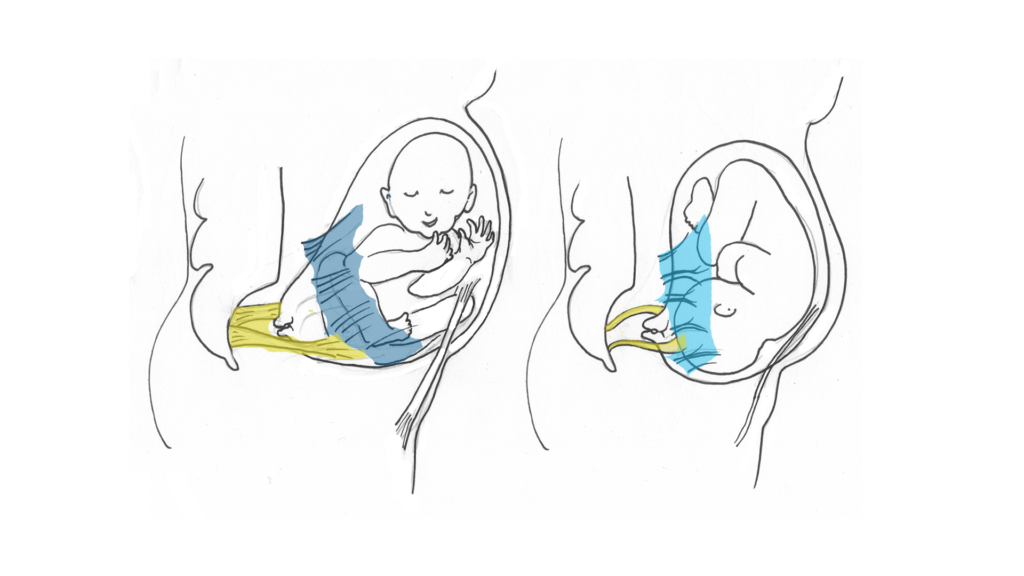 The head of the Adopt.ru portal, Armen Popov, confirms that two to three weeks pass on average between the family placement of a child and the removal of his profile from the FBI, and this depends on the efficiency of the work of regional data bank operators. Vlast will follow the FBI update in January.
The head of the Adopt.ru portal, Armen Popov, confirms that two to three weeks pass on average between the family placement of a child and the removal of his profile from the FBI, and this depends on the efficiency of the work of regional data bank operators. Vlast will follow the FBI update in January.
"For all children from the so-called list of Dima Yakovlev, requests were made to the heads of regions," Vlast explained in the office of the Ombudsman for Children in the Russian Federation. families. Two children from the Smolensk region are in a guest family. In Chuvashia, there is a unique experience of placing four brothers and sisters in a foster family. Their adoptive mother works as a paramedic, and their father is a former employee of the Ministry of Emergency Situations." According to the Children's Ombudsman of the Russian Federation, almost all children from "Dima Yakovlev's list" are arranged in the Jewish Autonomous Region. True, brother and sister Irina and Evgeny Kh. are placed in different families: "The children have developed a difficult relationship with each other, under such circumstances it was decided to transfer the children to different families. The guys keep in touch."
are placed in different families: "The children have developed a difficult relationship with each other, under such circumstances it was decided to transfer the children to different families. The guys keep in touch."
Most of the "American list" included children from St. Petersburg - 33. According to official data, two St. Petersburg children are now on the list: four-year-old Daria with Down's syndrome and 15-year-old Nastya, who "does not want to join a family herself." "According to the authorities of St. Petersburg, the rest of the children were placed in families," they say in the apparatus of the children's ombudsman of the Russian Federation.
At the beginning of December, American citizen Katrina Morris wrote to me that the profile of a ten-year-old orphan from St. Petersburg, Valeria, whom Katrina was going to adopt, had disappeared from the FBI. "I regularly checked her profile in the database," writes Katrina. I saw her in their story." Svetlana Agapitova, children's ombudsman in St.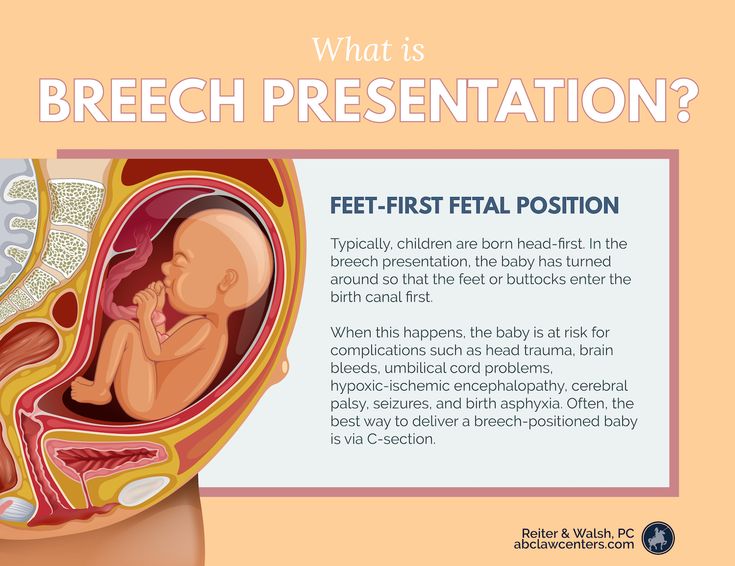 Petersburg, responded to Vlast's request about the fate of the children on the "American list": "Eight of the 33 children on the "American list" need to be clarified, including the girl Valeria." According to Agapitova, the city authorities provided her with verbal information that these children were placed in families, but her office is now checking this information: "As soon as I receive the information, I will provide it to the editors of Kommersant-Vlast."
Petersburg, responded to Vlast's request about the fate of the children on the "American list": "Eight of the 33 children on the "American list" need to be clarified, including the girl Valeria." According to Agapitova, the city authorities provided her with verbal information that these children were placed in families, but her office is now checking this information: "As soon as I receive the information, I will provide it to the editors of Kommersant-Vlast."
"Authorities" managed to get in touch with Valeriy Asikritov, director of orphanage N1. He said that Valeria still lives in the orphanage, but one of the employees of the boarding school issued a guest custody regime for her: "She sometimes takes Lera to visit for the weekend, the girl is very good, maybe they will get used to each other." The director of the orphanage took the information that Lera's profile was not in the database with surprise. Meanwhile, guest custody cannot be a reason for deleting a child's profile from the FBI, experts say. “The guest custody regime cannot be considered a family device,” explains the head of Adopt.ru, Armen Popov. continues to live in a children's institution and in the care of the state and is subject to family placement. The Office of the Commissioner for Children's Rights in the Russian Federation notes that four children from the "American list" now live in the guest custody mode, but their profiles are in the FBI, and the children have a chance to find a family. Considering that Lera's data from the FBI disappeared on the eve of the next anniversary of the "Dima Yakovlev law", it is not clear how many more Russian children from the "American list" are "arranged" in a family in this way.
“The guest custody regime cannot be considered a family device,” explains the head of Adopt.ru, Armen Popov. continues to live in a children's institution and in the care of the state and is subject to family placement. The Office of the Commissioner for Children's Rights in the Russian Federation notes that four children from the "American list" now live in the guest custody mode, but their profiles are in the FBI, and the children have a chance to find a family. Considering that Lera's data from the FBI disappeared on the eve of the next anniversary of the "Dima Yakovlev law", it is not clear how many more Russian children from the "American list" are "arranged" in a family in this way.
Chuvashia has a unique experience of placing four brothers and sisters in a foster family. Their adoptive mother works as a paramedic, their father is a former employee of the Ministry of Emergency Situations
Katrina Morris is very worried about Valeria and feels responsible for her.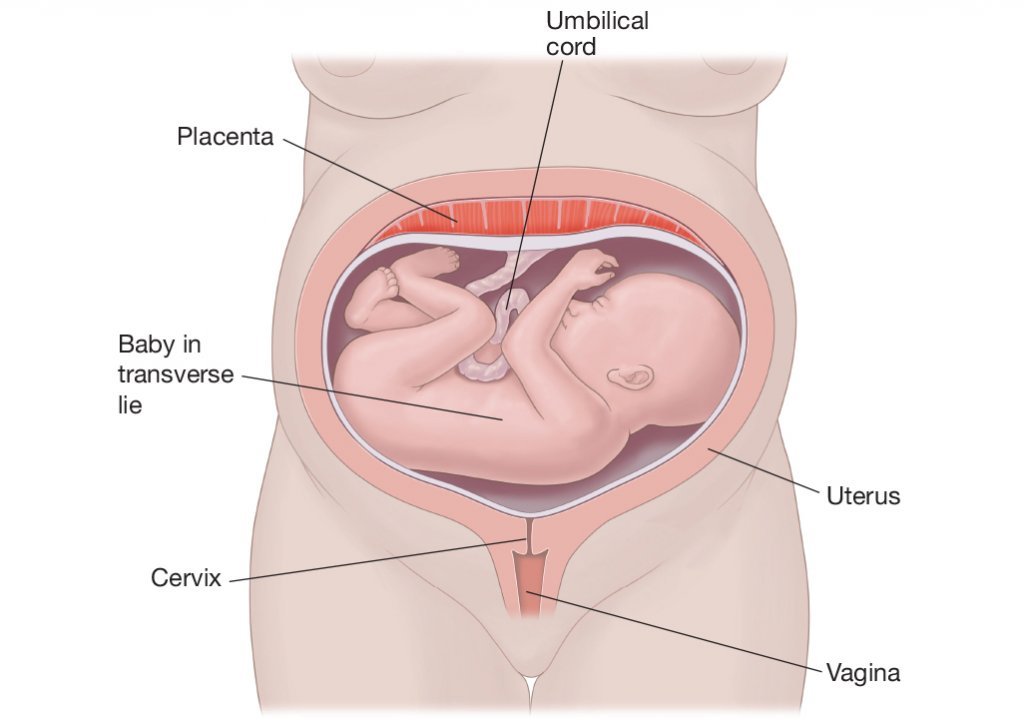 “I would really like to find a family for Valeria,” she says. “My husband and I have given up hope of taking her home. for your country, the decisions of the European Court. Therefore, all our hope now is on those people in Russia who could take Lera into the family. She really needs a family."
“I would really like to find a family for Valeria,” she says. “My husband and I have given up hope of taking her home. for your country, the decisions of the European Court. Therefore, all our hope now is on those people in Russia who could take Lera into the family. She really needs a family."
Nine-year-old Oksana with Down syndrome from the Vladimir region also remains in the orphanage system — she was supposed to go to Pennsylvania to live with a nurse, Jodi Johnson, but still lives in a boarding school for children with mental retardation in Kolchugino. The profile of six-year-old Vanya from the Smolensk region is also active in the FBI - he has a complex genetic disease, he was going to be adopted and treated by the Pardew family from Tennessee.
Five-year-old Katya with the same genetic disease as Vanya was not included in the "American list": candidates for foster parents did not have time to get to know her and only began to collect documents for adoption when the "Dima Yakovlev law" was adopted. Alena Sinkevich, a former specialist in foreign adoption, coordinator of the "Close People" program of the "Volunteers to Help Orphans" fund, says that children like Katya, who did not have time to see candidates for adoptive parents and were not included in the "American list", but had the prospect of leaving for an American family is quite a lot. However, it is impossible to know what their fate is. “When Dima Yakovlev’s law was passed, I worked with families who wanted to adopt six children from Russia,” says Sinkevich. “Four children were diagnosed with Down syndrome, two more with other genetic diseases. this is wonderful, but for their placement in families, administrative resources were often used.For example, one of the boys with Down syndrome was given "to the load": the family had already taken one child with Down syndrome, they were told in custody: "Take one more." they could not refuse. All this raises concerns about the future of children in families that did not have the proper motivation.
Alena Sinkevich, a former specialist in foreign adoption, coordinator of the "Close People" program of the "Volunteers to Help Orphans" fund, says that children like Katya, who did not have time to see candidates for adoptive parents and were not included in the "American list", but had the prospect of leaving for an American family is quite a lot. However, it is impossible to know what their fate is. “When Dima Yakovlev’s law was passed, I worked with families who wanted to adopt six children from Russia,” says Sinkevich. “Four children were diagnosed with Down syndrome, two more with other genetic diseases. this is wonderful, but for their placement in families, administrative resources were often used.For example, one of the boys with Down syndrome was given "to the load": the family had already taken one child with Down syndrome, they were told in custody: "Take one more." they could not refuse. All this raises concerns about the future of children in families that did not have the proper motivation. Although, in general, the fact that Russian families began to accept more children with disabilities makes me happy."
Although, in general, the fact that Russian families began to accept more children with disabilities makes me happy."
Katya is the only child from Sinkevich's personal "list" who has not yet been placed in a family. A complex genetic diagnosis and the need for regular surgical interventions scare away many potential adoptive parents. A few years ago, Katya underwent another operation, removing the "extra" overgrown bones of the skull. During another operation, her fingers were separated. Katya lay in the hospital alone and gnawed on bandages. The doctors didn't like it. They said so: "If she gnaws bandages all the time, we will not be able to operate on her again, we do not have enough personnel to monitor her." In fact, Katya does not need staff, but her own personal mother, but the chances of finding a mother for Katya were sharply reduced three years ago.
"We will always have time to deprive Katya of her rights"
Matvey was born in the Tula maternity hospital N1 on November 16, 2014. Three days later, the medical staff put him under a phototherapy lamp, the lamp exploded, the child received 75% burns to the body and 15% burns to the internal organs. Matvey survived and has since wandered between the Tula Regional Children's Clinical Hospital and the Speransky Children's City Clinical Hospital N9 in Moscow. On April 13, 2015, Matvey's blood mother Ekaterina refused to take the child home, writing her consent to his adoption by any other person. And on June 15, Natalya Tupyakova, a resident of Moscow, who saw a story about Matvey in a group of foster families on social networks, began to collect documents for the placement of a child in her family. Tupyakova has one birth child and two adopted children with disabilities, she has a medical background and has worked as a nurse in the past. Employees of the non-profit organizations accompanying her - the foundations "Volunteers to Help Orphans" and "Protect Life" - say that her children are adapted and socialized. In addition, Natalia is ready to maintain contact between Matvey and his blood mother Ekaterina.
Three days later, the medical staff put him under a phototherapy lamp, the lamp exploded, the child received 75% burns to the body and 15% burns to the internal organs. Matvey survived and has since wandered between the Tula Regional Children's Clinical Hospital and the Speransky Children's City Clinical Hospital N9 in Moscow. On April 13, 2015, Matvey's blood mother Ekaterina refused to take the child home, writing her consent to his adoption by any other person. And on June 15, Natalya Tupyakova, a resident of Moscow, who saw a story about Matvey in a group of foster families on social networks, began to collect documents for the placement of a child in her family. Tupyakova has one birth child and two adopted children with disabilities, she has a medical background and has worked as a nurse in the past. Employees of the non-profit organizations accompanying her - the foundations "Volunteers to Help Orphans" and "Protect Life" - say that her children are adapted and socialized. In addition, Natalia is ready to maintain contact between Matvey and his blood mother Ekaterina.
Within half a year, Natalia was denied three times by the Tula authorities the provisional guardianship of Matvey, although the law allows preliminary guardianship in order to speed up the procedure for the child's family placement. All this time, the guardianship department of the Moscow district of Yasenevo, where Natalya lives, did not give her the official status of a guardian, because she does not have her own housing in Moscow (she rents out her own housing in the region, and rents a three-room apartment in Moscow). According to the law, the absence of one's own housing cannot be a reason for refusing custody, but in practice this happens often. Natalya herself says that she does not feel the need for anything: there is remote work, child benefits, alimony for her eldest son. The "Protect Life" fund also intends to help her.
When Natalya Tupyakova finally received permission from the guardianship authorities in Yasenevo, it turned out that another guardian had been found for Matvey in Tula - an honorary citizen of the city Natalya Sarganova, who raised 38 foster children. She has both experience and positive characteristics, but she is 56 years old, and Matvey requires constant care. Representatives of the guardianship authorities of Tula were not embarrassed by the age of the candidate, and on July 15, Natalya Sarganova wrote her consent to accept the child into the family.
She has both experience and positive characteristics, but she is 56 years old, and Matvey requires constant care. Representatives of the guardianship authorities of Tula were not embarrassed by the age of the candidate, and on July 15, Natalya Sarganova wrote her consent to accept the child into the family.
However, Matvey never got into the family - on August 3, his birth mother Ekaterina withdrew her consent to the adoption of the child by other persons, and he again "stuck" in the orphan system. According to the head of the department of guardianship and guardianship of Tula, Olga Bolshakova, since August 3, "Katya has not appeared even once in the hospital." However, representatives of the guardianship authorities of Tula went to court with a lawsuit to recognize the child left without parental care only in October. The court granted this claim, and the decision came into force on November 21.
In October, Matvey was brought to Moscow to City Clinical Hospital N9, where volunteers saw him. Soon, the head of the Protect Life Foundation, actress Olga Budina, and the director of the documentary film about social orphanhood Bluff, or Happy New Year, Olga Sinyaeva, reported on social networks that the child, who suffered from the actions of Tula doctors, has not yet been transferred to the family, although there are candidates willing to accept it. According to public figures, the Tula authorities are deliberately delaying the procedure for Matvey's family placement, since the child's legal representative will be able to represent his interests in a criminal case against the maternity hospital, which has not yet been closed. As stated in the official response of the prosecutor's office of the Central District of Tula, today the protection of the rights and legitimate interests of Matvey in a criminal case is carried out by the body of guardianship and guardianship. "The preliminary investigation in this criminal case has not yet been completed," the department said in response to a request from public activists.
Soon, the head of the Protect Life Foundation, actress Olga Budina, and the director of the documentary film about social orphanhood Bluff, or Happy New Year, Olga Sinyaeva, reported on social networks that the child, who suffered from the actions of Tula doctors, has not yet been transferred to the family, although there are candidates willing to accept it. According to public figures, the Tula authorities are deliberately delaying the procedure for Matvey's family placement, since the child's legal representative will be able to represent his interests in a criminal case against the maternity hospital, which has not yet been closed. As stated in the official response of the prosecutor's office of the Central District of Tula, today the protection of the rights and legitimate interests of Matvey in a criminal case is carried out by the body of guardianship and guardianship. "The preliminary investigation in this criminal case has not yet been completed," the department said in response to a request from public activists.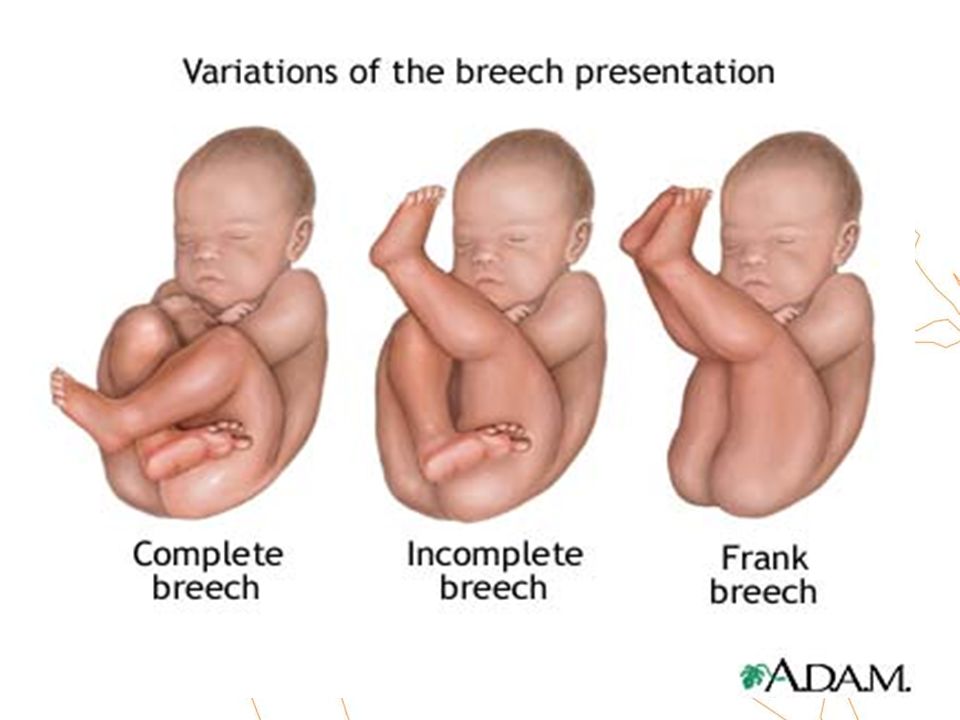 The prosecutor's office calls the volunteers' demand for the recovery of a monthly life allowance from the Tula maternity hospital N1 in favor of Matvey "premature", since the child is "on full state support."
The prosecutor's office calls the volunteers' demand for the recovery of a monthly life allowance from the Tula maternity hospital N1 in favor of Matvey "premature", since the child is "on full state support."
One of the boys with Down syndrome was given "to the load": the family had already taken one child with Down syndrome, they were told in custody: "Take one more." And they couldn't refuse
"A year has passed since the tragedy caused by the negligence of the medical staff and which broke the child's life," says Olga Sinyaeva. security rules? I think that the Tula authorities, afraid that Matvey's independent guardian would insist on investigating the crime, began to urgently look for a "managed" candidate for adoptive parents.
The scandal spread from social networks to the media, its participants were invited to the television program "Live Broadcast", where Matvey's blood mother Ekaterina said that she was not going to raise her son and did not understand people who want to take him into the family. From Ekaterina's words, it became clear that for the past year, representatives of the media and authorities have been putting pressure on her, trying to "give her a chance" to raise a child, although she herself did not want it. According to Sinyaeva, Matvey's mother needs professional help and support from a psychologist. Ekaterina's common-law husband states that she did not receive any psychological assistance. In turn, the head of the city department of guardianship and guardianship Olga Bolshakova in the program "Live" said that social services provided assistance to Catherine, but to no avail. Matvey's mother is still not deprived of parental rights. “We will always have time to deprive Katya of her rights,” says Bolshakova. To the questions of the participants in the public discussion, why the guardianship authorities do not think about the interests of the child, who is still not placed in a family, the representative of the guardianship did not answer. A noteworthy episode of the TV program was the statement of the Deputy Head of the Tula Region Representative Office under the Government of the Russian Federation Evgenia Shokhina.
From Ekaterina's words, it became clear that for the past year, representatives of the media and authorities have been putting pressure on her, trying to "give her a chance" to raise a child, although she herself did not want it. According to Sinyaeva, Matvey's mother needs professional help and support from a psychologist. Ekaterina's common-law husband states that she did not receive any psychological assistance. In turn, the head of the city department of guardianship and guardianship Olga Bolshakova in the program "Live" said that social services provided assistance to Catherine, but to no avail. Matvey's mother is still not deprived of parental rights. “We will always have time to deprive Katya of her rights,” says Bolshakova. To the questions of the participants in the public discussion, why the guardianship authorities do not think about the interests of the child, who is still not placed in a family, the representative of the guardianship did not answer. A noteworthy episode of the TV program was the statement of the Deputy Head of the Tula Region Representative Office under the Government of the Russian Federation Evgenia Shokhina.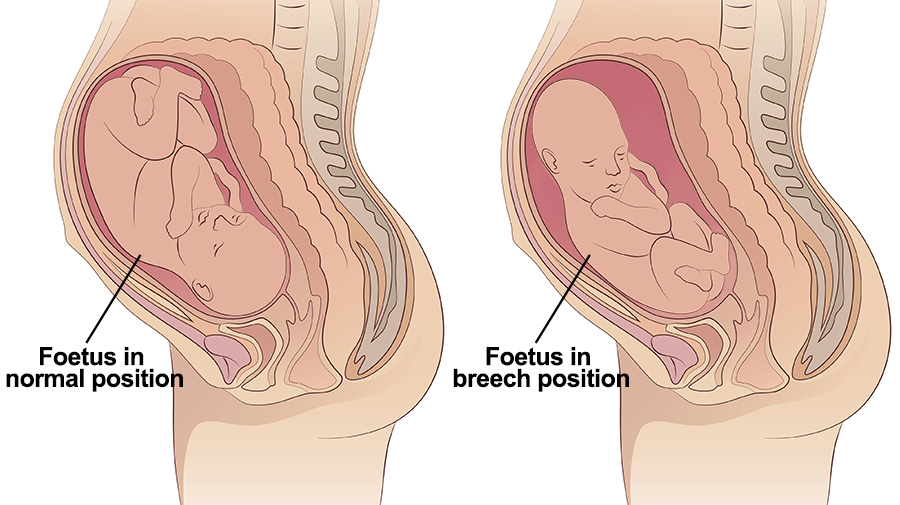 "I was contacted by another potential guardian from a prosperous Moscow family, she asks not to give her name, because she is a representative of a fairly large structure," she said. "And she is now collecting documents." It soon became known that the name of the new candidate for guardianship was Svetlana, and her Internet page was hosted on a domain registered to the RSPP Telecom organization. Svetlana herself wrote that she intended to adopt Matvey, but did not intend to disclose confidential information about herself.
"I was contacted by another potential guardian from a prosperous Moscow family, she asks not to give her name, because she is a representative of a fairly large structure," she said. "And she is now collecting documents." It soon became known that the name of the new candidate for guardianship was Svetlana, and her Internet page was hosted on a domain registered to the RSPP Telecom organization. Svetlana herself wrote that she intended to adopt Matvey, but did not intend to disclose confidential information about herself.
“We would like to know when she managed to pass the school of adoptive parents in such a short time and collect all the documents for the adoption of Matvey,” says Olga Budina. the desire to help the child, but other motives. In this case, Matvey may again end up in the orphanage, and we do not want this to happen. " After a story about Matvey was released on the REN TV channel, where, in particular, Svetlana was mentioned as an employee of the RSPP, the candidate deleted her page from the domain owned by this organization, saying that she would provide new information after adoption. And the administration of the Tula region wrote on its Facebook page that a mother was found for Matvey, and they thanked all the people who were not indifferent to this story. The fact that the candidate turned not to the guardianship authorities, but directly to Yevgenia Shokhina, that is, she used the "political channel" and not the procedure prescribed by law, did not bother the Tula authorities.
And the administration of the Tula region wrote on its Facebook page that a mother was found for Matvey, and they thanked all the people who were not indifferent to this story. The fact that the candidate turned not to the guardianship authorities, but directly to Yevgenia Shokhina, that is, she used the "political channel" and not the procedure prescribed by law, did not bother the Tula authorities.
On December 4, Natalya Tupyakova was registered with the territorial department of guardianship and guardianship of Tula as a candidate for Matvey's adoptive parents. However, the officials refused to give her a referral to visit Matvey in the hospital, because on December 2, another candidate, Svetlana, had already received such a referral to visit the child and wrote her consent to his adoption. Public activists note that on November 22, when volunteers raised a fuss on social networks about the fate of Matvey, there was no talk of any third candidate for adoptive parents, and the territorial body of guardianship and guardianship of Tula reported that there were only two candidates - Tupyakov and Sarganova. It turns out that the third candidate collected the necessary documents in less than two weeks. Recall that in order to become a candidate for foster parents, you must go through a foster parent school (on average, training lasts about two months), collect all medical documents, and also receive a certificate of no criminal record from the Ministry of Internal Affairs, which is done exactly one month. “They decided to hide everything that happened to Matvey behind the secret of adoption,” says Olga Sinyaeva. “The appearance of a third candidate is a brilliant move by the Tula authorities. They think that after Matvey’s adoption, no one will sue the Tula health care, and Matvey can be hidden altogether from society. Corporate interests were higher than the interests of a crippled child. "
It turns out that the third candidate collected the necessary documents in less than two weeks. Recall that in order to become a candidate for foster parents, you must go through a foster parent school (on average, training lasts about two months), collect all medical documents, and also receive a certificate of no criminal record from the Ministry of Internal Affairs, which is done exactly one month. “They decided to hide everything that happened to Matvey behind the secret of adoption,” says Olga Sinyaeva. “The appearance of a third candidate is a brilliant move by the Tula authorities. They think that after Matvey’s adoption, no one will sue the Tula health care, and Matvey can be hidden altogether from society. Corporate interests were higher than the interests of a crippled child. "
The criminal case initiated on November 21, 2014 against a maternity hospital nurse under Article 118 of the Criminal Code of the Russian Federation was terminated in May 2015 under an amnesty.