Labor starts and stops
Prodromal Labor: Definition, Symptoms, and More
Prodromal Labor: Definition, Symptoms, and MoreMedically reviewed by Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT — By Becky Young on August 22, 2017
What is prodromal labor?
Prodromal labor is labor that starts and stops before fully active labor begins. It’s often called “false labor,” but this is a poor description. Medical professionals recognize that the contractions are real, but they come and go and labor may not progress.
So, prodromal labor is real in terms of contraction pain and regularity. What makes these contractions different from contractions seen in active labor is that they start and stop.
Prodromal labor contractions will often come and go at the same time each day or at regular intervals. Many mothers, even experienced ones, end up calling their birth team or going to the hospital, thinking labor has begun.
Prodromal labor is really common and can start days, weeks, or even a month or more before active labor begins. Your health care provider will want you to deliver as close to 40 weeks (your due date) as possible. Prodromal labor isn’t an indication for induction or cesarean delivery.
Prodromal labor vs. Braxton-Hicks
Prodromal labor is often mistaken for Braxton-Hicks contractions, but they’re not the same thing. The majority of pregnant women will experience this type of contraction at some stage during their pregnancy. Braxton-Hicks are essentially practice contractions. They’re your body’s way of preparing for labor.
Braxton-Hicks contractions can cause a very tight, uncomfortable sensation, but they’re not typically regular or intense. They rarely last a long time or grow in intensity. Prodromal labor can follow a very regular pattern. The contractions can vary and grow in intensity.
It’s sometimes possible to ease Braxton-Hicks contractions by drinking water, eating, or relaxing. These activities won’t help ease prodromal labor contractions. Your cervix can also slowly dilate or efface during prodromal labor. This doesn’t usually happen with Braxton-Hicks contractions.
This doesn’t usually happen with Braxton-Hicks contractions.
Prodromal labor vs. active labor
Prodromal labor contractions usually occur less than every five minutes and may stop for long periods. Once active labor begins, your contractions will become more and more frequent and will no longer start and stop.
The closer together your contractions are, the closer you are to meeting your baby. Real labor contractions get longer, stronger, and closer together and progress to delivery without stopping or slowing. Once labor is progressing well (usually once the mother is over 4 centimeters dilated), the labor won’t stop.
What causes prodromal labor?
There are several theories as to what causes prodromal labor, but the medical community hasn’t identified a specific cause. Most researchers seem to agree that prodromal labor is the body’s way of preparing for active labor. There are several potential contributing factors:
- The position of your baby: You may be more likely to experience prodromal labor if your baby is in breech position.
 The theory is that the uterus attempts to move the baby with contractions for a period of time and then stops if it doesn’t work.
The theory is that the uterus attempts to move the baby with contractions for a period of time and then stops if it doesn’t work. - Physical factor: An uneven pelvis or uterine abnormality may lead to these contractions.
- Feeling anxious or afraid: Apprehensive emotions either about your pregnancy or other things in your life may cause prodromal labor.
- History of previous pregnancies: This may be related to the way the uterus changes or relaxes after multiple pregnancies.
Prodromal labor isn’t usually a cause for concern and doesn’t mean that your baby is in distress. But if you do have concerns, you should always contact your healthcare provider.
Does prodromal labor mean active labor is near?
Prodromal labor can occur any time within the last month of your pregnancy. However, it doesn’t necessarily mean active labor is going to happen in the next day or even week. Labor and birth are unpredictable, so there’s really no good way to predict exactly when it will begin. Here are some common telltale signs that may signal that baby will soon be on the way.
Here are some common telltale signs that may signal that baby will soon be on the way.
Seeking help
Whether or not you need to contact your doctor or midwife will depend on your individual situation. In general, if your pregnancy is low risk, you likely won’t need to contact your healthcare provider if you’re experiencing prodromal labor.
However, it may be difficult to tell if your contractions are a sign of active labor or prodromal labor. You should always reach out to your healthcare providers if you have concerns and to rule out other problems.
What you can do to manage this condition
If you are close to your due date, try to stay active during contractions. This could include:
- staying upright
- walking around
- using a birthing ball
- dancing
Rest during periods where contractions have ceased. Remember to stay hydrated and nourished to keep your energy levels up. Use this time to practice your coping mechanisms for getting through each contraction. Breathing and relaxation techniques can be really useful.
Breathing and relaxation techniques can be really useful.
Last medically reviewed on August 22, 2017
- Parenthood
- Pregnancy
- 3rd Trimester
How we vetted this article:
Healthline has strict sourcing guidelines and relies on peer-reviewed studies, academic research institutions, and medical associations. We avoid using tertiary references. You can learn more about how we ensure our content is accurate and current by reading our editorial policy.
- Angelini DJ, et al. (2013). Obstetric triage and emergency care protocols.
books.google.com/books?hl=en&lr=&id=A4f_gtPEOXcC&oi=fnd&pg=PA159&dq=prodromal+labor+pregnancy&ots=mrHcMRgTTI&sig=80ViknEOKy4VEvWp0OZr2gBaizw#v=onepage&q&f=false - Clark EAS, et al. (2015). Late preterm birth: An iatrogenic epidemic.
ajceog.us/files/ajceog0004598.pdf - True vs.
 false labor. (2016).
false labor. (2016).
my.clevelandclinic.org/health/articles/true-vs-false-labor
Our experts continually monitor the health and wellness space, and we update our articles when new information becomes available.
Current Version
Aug 22, 2017
By
Becky Young
Edited By
Nizam Khan (TechSpace)
Medically Reviewed By
Debra Rose Wilson, PhD, MSN, RN, IBCLC, AHN-BC, CHT
Share this article
Medically reviewed by Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT — By Becky Young on August 22, 2017
related stories
Abnormal Labor
When to Go to the Hospital for Labor
Labor and Delivery
6 Telltale Signs of Labor
What Is a Nurse Midwife and How to Tell If They Are Right for You
Read this next
Abnormal Labor
Medically reviewed by Nicole Galan, RN
Abnormal labor is labor that slows down or stops altogether.
 Learn why abnormal labor may occur and how it’s diagnosed.
Learn why abnormal labor may occur and how it’s diagnosed.READ MORE
When to Go to the Hospital for Labor
Medically reviewed by Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT
Is it early labor or active labor? Is it true labor or false labor? Here are the signs that will tell you when to go to the hospital for labor.
READ MORE
Labor and Delivery
Medically reviewed by Bobbie Sue Whitworth, Ph.D., MSN, RNC
Labor and delivery tends to occupy the minds of expectant parents the most. Read on if you have questions about the signs and length of labor.
READ MORE
6 Telltale Signs of Labor
Medically reviewed by Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT
While every pregnancy and labor is different, here are six signs that labor is on the way.
 Talk to your doctor if you experience any of the following…
Talk to your doctor if you experience any of the following…READ MORE
What Is a Nurse Midwife and How to Tell If They Are Right for You
Medically reviewed by Meredith Wallis, MS, APRN, CNM, IBCLC
A nurse midwife is a nurse with education, training, and certification to provide prenatal, delivery, and women's care.
READ MORE
Your 6-Week Ultrasound: What to Expect
Medically reviewed by Valinda Riggins Nwadike, MD, MPH
We'll tell you all about the 6-week ultrasound, including why your doctor may have ordered it, what the risks are, and what it means if no heartbeat…
READ MORE
Does Swaddling Increase the Risk of SIDS?
Medically reviewed by Mia Armstrong, MD
Is swaddling safe, or is it a risk factor for SIDS? Here's what the most recent research says.
READ MORE
How to Relieve and Prevent Hip Pain During Pregnancy
Medically reviewed by Holly Ernst, PA-C
Hip pain is a common complication of pregnancy. Here are stretches, other home remedies, causes, and what you can do to prevent it.
READ MORE
Antidepressants in Pregnancy Aren't Linked to Increased Neurological Issues in Children
A cohort study of antidepressant use in pregnancy found that the rate of neurological disorders in children born to those who took antidepressant…
READ MORE
These Guided Pregnancy Journals Will Help You Document All the Feels
Medically reviewed by Meredith Wallis, MS, APRN, CNM, IBCLC
The pregnancy and postpartum periods are full of emotions (rightfully so!), and these pregnancy journals are a great place to document it all.
READ MORE
Prodromal Labor: Definition, Symptoms, and More
Prodromal Labor: Definition, Symptoms, and MoreMedically reviewed by Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT — By Becky Young on August 22, 2017
What is prodromal labor?
Prodromal labor is labor that starts and stops before fully active labor begins. It’s often called “false labor,” but this is a poor description. Medical professionals recognize that the contractions are real, but they come and go and labor may not progress.
So, prodromal labor is real in terms of contraction pain and regularity. What makes these contractions different from contractions seen in active labor is that they start and stop.
Prodromal labor contractions will often come and go at the same time each day or at regular intervals. Many mothers, even experienced ones, end up calling their birth team or going to the hospital, thinking labor has begun.
Prodromal labor is really common and can start days, weeks, or even a month or more before active labor begins. Your health care provider will want you to deliver as close to 40 weeks (your due date) as possible. Prodromal labor isn’t an indication for induction or cesarean delivery.
Your health care provider will want you to deliver as close to 40 weeks (your due date) as possible. Prodromal labor isn’t an indication for induction or cesarean delivery.
Prodromal labor vs. Braxton-Hicks
Prodromal labor is often mistaken for Braxton-Hicks contractions, but they’re not the same thing. The majority of pregnant women will experience this type of contraction at some stage during their pregnancy. Braxton-Hicks are essentially practice contractions. They’re your body’s way of preparing for labor.
Braxton-Hicks contractions can cause a very tight, uncomfortable sensation, but they’re not typically regular or intense. They rarely last a long time or grow in intensity. Prodromal labor can follow a very regular pattern. The contractions can vary and grow in intensity.
It’s sometimes possible to ease Braxton-Hicks contractions by drinking water, eating, or relaxing. These activities won’t help ease prodromal labor contractions. Your cervix can also slowly dilate or efface during prodromal labor. This doesn’t usually happen with Braxton-Hicks contractions.
This doesn’t usually happen with Braxton-Hicks contractions.
Prodromal labor vs. active labor
Prodromal labor contractions usually occur less than every five minutes and may stop for long periods. Once active labor begins, your contractions will become more and more frequent and will no longer start and stop.
The closer together your contractions are, the closer you are to meeting your baby. Real labor contractions get longer, stronger, and closer together and progress to delivery without stopping or slowing. Once labor is progressing well (usually once the mother is over 4 centimeters dilated), the labor won’t stop.
What causes prodromal labor?
There are several theories as to what causes prodromal labor, but the medical community hasn’t identified a specific cause. Most researchers seem to agree that prodromal labor is the body’s way of preparing for active labor. There are several potential contributing factors:
- The position of your baby: You may be more likely to experience prodromal labor if your baby is in breech position.
 The theory is that the uterus attempts to move the baby with contractions for a period of time and then stops if it doesn’t work.
The theory is that the uterus attempts to move the baby with contractions for a period of time and then stops if it doesn’t work. - Physical factor: An uneven pelvis or uterine abnormality may lead to these contractions.
- Feeling anxious or afraid: Apprehensive emotions either about your pregnancy or other things in your life may cause prodromal labor.
- History of previous pregnancies: This may be related to the way the uterus changes or relaxes after multiple pregnancies.
Prodromal labor isn’t usually a cause for concern and doesn’t mean that your baby is in distress. But if you do have concerns, you should always contact your healthcare provider.
Does prodromal labor mean active labor is near?
Prodromal labor can occur any time within the last month of your pregnancy. However, it doesn’t necessarily mean active labor is going to happen in the next day or even week. Labor and birth are unpredictable, so there’s really no good way to predict exactly when it will begin. Here are some common telltale signs that may signal that baby will soon be on the way.
Here are some common telltale signs that may signal that baby will soon be on the way.
Seeking help
Whether or not you need to contact your doctor or midwife will depend on your individual situation. In general, if your pregnancy is low risk, you likely won’t need to contact your healthcare provider if you’re experiencing prodromal labor.
However, it may be difficult to tell if your contractions are a sign of active labor or prodromal labor. You should always reach out to your healthcare providers if you have concerns and to rule out other problems.
What you can do to manage this condition
If you are close to your due date, try to stay active during contractions. This could include:
- staying upright
- walking around
- using a birthing ball
- dancing
Rest during periods where contractions have ceased. Remember to stay hydrated and nourished to keep your energy levels up. Use this time to practice your coping mechanisms for getting through each contraction. Breathing and relaxation techniques can be really useful.
Breathing and relaxation techniques can be really useful.
Last medically reviewed on August 22, 2017
- Parenthood
- Pregnancy
- 3rd Trimester
How we vetted this article:
Healthline has strict sourcing guidelines and relies on peer-reviewed studies, academic research institutions, and medical associations. We avoid using tertiary references. You can learn more about how we ensure our content is accurate and current by reading our editorial policy.
- Angelini DJ, et al. (2013). Obstetric triage and emergency care protocols.
books.google.com/books?hl=en&lr=&id=A4f_gtPEOXcC&oi=fnd&pg=PA159&dq=prodromal+labor+pregnancy&ots=mrHcMRgTTI&sig=80ViknEOKy4VEvWp0OZr2gBaizw#v=onepage&q&f=false - Clark EAS, et al. (2015). Late preterm birth: An iatrogenic epidemic.
ajceog.us/files/ajceog0004598.pdf - True vs.
 false labor. (2016).
false labor. (2016).
my.clevelandclinic.org/health/articles/true-vs-false-labor
Our experts continually monitor the health and wellness space, and we update our articles when new information becomes available.
Current Version
Aug 22, 2017
By
Becky Young
Edited By
Nizam Khan (TechSpace)
Medically Reviewed By
Debra Rose Wilson, PhD, MSN, RN, IBCLC, AHN-BC, CHT
Share this article
Medically reviewed by Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT — By Becky Young on August 22, 2017
related stories
Abnormal Labor
When to Go to the Hospital for Labor
Labor and Delivery
6 Telltale Signs of Labor
What Is a Nurse Midwife and How to Tell If They Are Right for You
Read this next
Abnormal Labor
Medically reviewed by Nicole Galan, RN
Abnormal labor is labor that slows down or stops altogether.
 Learn why abnormal labor may occur and how it’s diagnosed.
Learn why abnormal labor may occur and how it’s diagnosed.READ MORE
When to Go to the Hospital for Labor
Medically reviewed by Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT
Is it early labor or active labor? Is it true labor or false labor? Here are the signs that will tell you when to go to the hospital for labor.
READ MORE
Labor and Delivery
Medically reviewed by Bobbie Sue Whitworth, Ph.D., MSN, RNC
Labor and delivery tends to occupy the minds of expectant parents the most. Read on if you have questions about the signs and length of labor.
READ MORE
6 Telltale Signs of Labor
Medically reviewed by Debra Rose Wilson, Ph.D., MSN, R.N., IBCLC, AHN-BC, CHT
While every pregnancy and labor is different, here are six signs that labor is on the way.
 Talk to your doctor if you experience any of the following…
Talk to your doctor if you experience any of the following…READ MORE
What Is a Nurse Midwife and How to Tell If They Are Right for You
Medically reviewed by Meredith Wallis, MS, APRN, CNM, IBCLC
A nurse midwife is a nurse with education, training, and certification to provide prenatal, delivery, and women's care.
READ MORE
Your 6-Week Ultrasound: What to Expect
Medically reviewed by Valinda Riggins Nwadike, MD, MPH
We'll tell you all about the 6-week ultrasound, including why your doctor may have ordered it, what the risks are, and what it means if no heartbeat…
READ MORE
Does Swaddling Increase the Risk of SIDS?
Medically reviewed by Mia Armstrong, MD
Is swaddling safe, or is it a risk factor for SIDS? Here's what the most recent research says.
READ MORE
How to Relieve and Prevent Hip Pain During Pregnancy
Medically reviewed by Holly Ernst, PA-C
Hip pain is a common complication of pregnancy. Here are stretches, other home remedies, causes, and what you can do to prevent it.
READ MORE
Antidepressants in Pregnancy Aren't Linked to Increased Neurological Issues in Children
A cohort study of antidepressant use in pregnancy found that the rate of neurological disorders in children born to those who took antidepressant…
READ MORE
These Guided Pregnancy Journals Will Help You Document All the Feels
Medically reviewed by Meredith Wallis, MS, APRN, CNM, IBCLC
The pregnancy and postpartum periods are full of emotions (rightfully so!), and these pregnancy journals are a great place to document it all.

READ MORE
false or real / “Waiting for a baby”
February
Shortly before the birth, the expectant mother may be disturbed by training contractions, rhythmic contractions of the uterus, which quickly pass and appear occasionally. How to distinguish them from real contractions, and why they are needed, we will try to find out.
For the first time, the phenomenon of temporary contractions was described by the English doctor John Braxton Hicks. That is why they are called - Braxton Hicks contractions or false, training contractions, precursor contractions. In his scientific work of 1872, he argued that these contractions are short-term (from half a minute to 2 minutes) contractions of the muscles of the uterus, which are felt by a pregnant woman as an increase in the tone of the uterus. They appear after the 20th week of pregnancy. And during the day they happen often, but the expectant mother in the daytime may not even notice them. However, as time goes on, they intensify, becoming more and more obvious.
However, as time goes on, they intensify, becoming more and more obvious.
WHAT DO YOU NEED FALSE BROUGHT
The uterus is a muscular organ. And like any muscle that has to perform the work allotted to it in the body, it needs training. After all, if she hangs for all forty weeks like a bag, she will not cope with the load in childbirth. Thus, the purpose of training or false contractions is to prepare the uterus and cervix for childbirth. That is why one of the names of training bouts is contractions harbingers - harbingers of an approaching birth.
ARE FALSE PARTS PAINFUL?
As a rule, false contractions are painless, but with increasing duration they become more noticeable and bring more discomfort. However, in all women, they manifest themselves in different ways, someone does not feel them at all, and someone does not sleep at night, tossing and turning and trying to find a comfortable position for sleeping. It all depends on the pain threshold. The main thing in this situation is to stop being nervous about this and calm yourself with the thought that such training is necessary for the most important upcoming event - the birth of your crumbs. And to calm down a little and sleep better, ask your doctor to prescribe a sedative for you and get a special pillow for expectant and nursing mothers. With her, falling asleep and experiencing the discomfort of the last weeks of pregnancy will be much easier!
The main thing in this situation is to stop being nervous about this and calm yourself with the thought that such training is necessary for the most important upcoming event - the birth of your crumbs. And to calm down a little and sleep better, ask your doctor to prescribe a sedative for you and get a special pillow for expectant and nursing mothers. With her, falling asleep and experiencing the discomfort of the last weeks of pregnancy will be much easier!
HOW TO LIVE WITH FREQUENT PARTS
Some expectant mothers complain that their Braxton Hicks contractions are frequent and cause significant discomfort, even when they are doing housework or other light physical activity. In such a situation, obstetricians are advised to lie down or vice versa, take an easy walk, in any case, change the type of activity. If training contractions bother you a lot, it is recommended to drink a glass of water, juice or herbal tea, calm down and get some rest. Ask someone close to give you a massage. Lie in silence. And to also benefit from training fights, try doing breathing exercises: practice breathing techniques in childbirth in practice.
Lie in silence. And to also benefit from training fights, try doing breathing exercises: practice breathing techniques in childbirth in practice.
HOW TO DIFFERENTIATE TRAINING FROM LIVING
The most important thing to understand is that real contractions are much more painful than Braxton Hicks contractions. You will understand it right away. In addition, the contractions that bring you closer to childbirth are more regular. The contractions begin in the lower back, spread to the front of the abdomen, and occur every 10 minutes (or more than 5 contractions per hour). Then they occur with an interval of about 30-70 seconds and over time the intervals between them are reduced. Some women describe the sensations of labor pains as severe menstrual cramps, or sensations during diarrhea, when the pain rolls in waves in the abdomen. These contractions, unlike false ones, continue even after a change in position and when walking, constantly intensifying. As soon as you feel all these symptoms, call your ob-gyn - hour X has arrived. If in doubt, also do not be afraid to disturb the doctor. The doctor will ask you a few questions that will help him determine the type of contractions and eliminate all your doubts and worries. After all, it is always better to consult a doctor and trust his professional experience.
If in doubt, also do not be afraid to disturb the doctor. The doctor will ask you a few questions that will help him determine the type of contractions and eliminate all your doubts and worries. After all, it is always better to consult a doctor and trust his professional experience.
You should seek help if:
• you have more than four contractions an hour and they happen regularly
• contractions are accompanied by pain in the lower spine
• contractions are accompanied by watery or bloody vaginal discharge
• the contractions are so strong that it is very difficult for you to endure them
• there is a marked change in the child's movement, or less than 10 movements every 2 hours
• you think your waters have started to break
Alla Misyutina, Consultant Physician, Independent Laboratory INVITRO
Dear women, during labor, the body needs a lot of oxygen, so proper breathing is very important. A large influx of oxygen into the blood of mother and baby alleviates the condition of the crumbs, which during childbirth experiences oxygen starvation. Special breathing techniques help to properly open the birth canal and make contractions and attempts as effective as possible.
A large influx of oxygen into the blood of mother and baby alleviates the condition of the crumbs, which during childbirth experiences oxygen starvation. Special breathing techniques help to properly open the birth canal and make contractions and attempts as effective as possible.
Different types of breathing should be used at different stages of labor.
• During "false" contractions, breathing should be deep and slow. During the period when the contractions become more intense, it is necessary to use "pain-relieving breathing". This breathing is slow, deep, the inhalation is done through the nose, it should be longer than the exhalation through the mouth. More details: inhale is done at the expense of 1-2-3-4, and exhale - at the expense of 1-2-3-4-5-6. With the help of such breathing: mom relaxes, distracts from pain, focuses on the score; the baby receives as much as possible, so he needs oxygen.
• In breaks from contractions, you need to rest and breathe evenly without any effort, so that you can then easily follow the doctor's recommendations.
• During attempts, you need to exhale all the air from the lungs, then take a deep breath and push for up to 6-9 seconds. Quickly exhale all the air, quickly take a deep breath and again hold your breath for 6-9 seconds, and so on - about three times per attempt.
• In breaks from attempts to rest and breathe deeply, evenly and relaxed.
• It is very important to only push on the perineum and never push on the head. In this case, all efforts are wasted and will appear in the form of burst vessels in the eyes and on the face.
• In the period after the birth of the head, it is necessary to stop pushing and breathing shallowly, some call this breathing “dog-like”, deep breathing can harm both mom and baby. Then everything goes on as usual, the main thing is to obey the doctor.
• After the baby was born, within half an hour the last stage of labor begins - the birth of the placenta. Special breathing is no longer required, at the doctor's command, push a little into the perineum and EVERYTHING! Dear women, pain during childbirth is good, it means that your baby will be born soon. There is no need to resist the pain, this is a mistake that brings a woman and a child nothing but fatigue. On the contrary, it is necessary to concentrate and help in every possible way to give birth to a healthy baby.
There is no need to resist the pain, this is a mistake that brings a woman and a child nothing but fatigue. On the contrary, it is necessary to concentrate and help in every possible way to give birth to a healthy baby.
BIRTH AGAIN
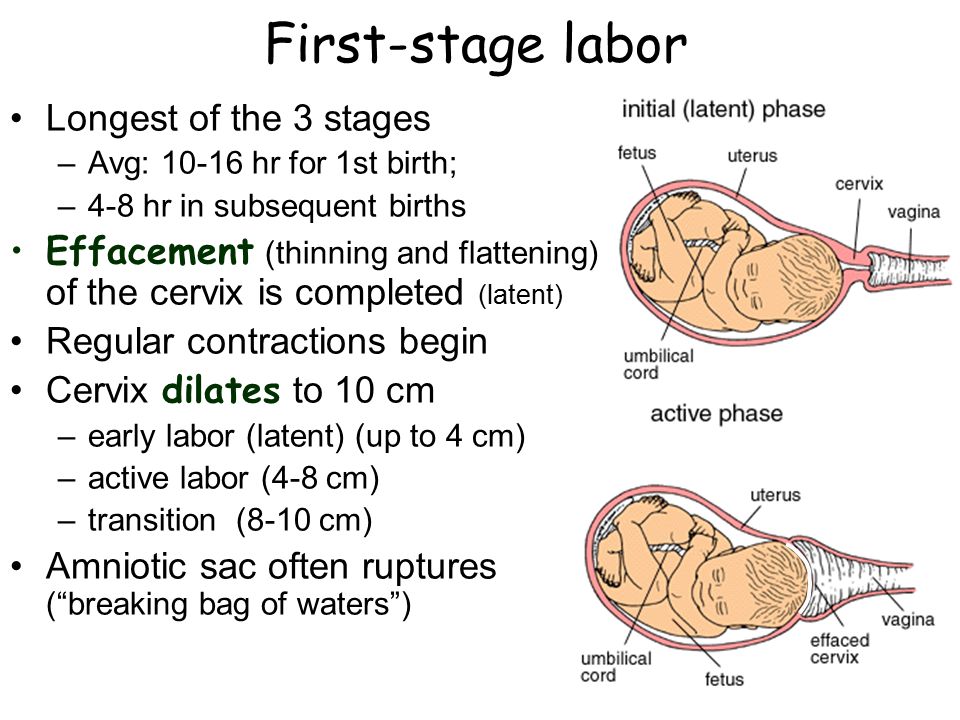
So, you have decided that this is no longer a “teaching”, but the beginning of childbirth. In addition to contractions, the onset of labor can be indicated by the outflow of amniotic fluid and the passage of a mucous plug that closes the lumen of the cervix. The mucous plug can also come off 2-3 days before delivery. However, her departure does not always mean that it is time to go to the hospital. During pregnancy, the cervix is tightly closed. With the onset of labor pains, its opening begins: the cervix of the uterus gradually expands to 10-12 cm in diameter (full disclosure). The birth canal is preparing to "release" the child from the womb. Intrauterine pressure increases during contractions as the uterus shrinks. And in the end, this leads to rupture of the fetal bladder and the outflow of part of the amniotic fluid.
The first, preparatory, period of labor for women giving birth for the first time takes an average of 12 hours, and 2-4 hours less for those who have second births. At the beginning of the second stage of labor, contractions join the contractions - contractions of the muscles of the abdominal wall and diaphragm. In addition to the fact that different muscle groups are involved in contractions and attempts, they have one more important difference: contractions are an involuntary and uncontrollable phenomenon, neither their strength nor frequency depend on the woman in labor, while attempts to a certain extent obey her will , it can delay or strengthen them. Therefore, at this stage of childbirth, a lot depends on the expectant mother and her ability to quickly and correctly follow the commands of the obstetrician taking delivery. And most importantly - to tune in correctly and not allow panic and thoughts about something bad. Obstetricians and gynecologists recommend that mothers perceive childbirth as a holiday, a baby's birthday. Then it will be easier to concentrate on the fact that now your main task is to help the baby be born. If, during childbirth, the expectant mother panics, the concentration of adrenaline in her blood will increase significantly. Which will not have a very good effect on the process of childbirth. Adrenaline affects the synthesis of oxytocin, which significantly weakens contractions and slows down the process of childbirth. In addition, adrenaline completely blocks the production of endorphins, which will increase the feeling of pain during contractions and attempts. That is why it is so important to properly tune in, concentrate and help the baby to be born as soon as possible.
Then it will be easier to concentrate on the fact that now your main task is to help the baby be born. If, during childbirth, the expectant mother panics, the concentration of adrenaline in her blood will increase significantly. Which will not have a very good effect on the process of childbirth. Adrenaline affects the synthesis of oxytocin, which significantly weakens contractions and slows down the process of childbirth. In addition, adrenaline completely blocks the production of endorphins, which will increase the feeling of pain during contractions and attempts. That is why it is so important to properly tune in, concentrate and help the baby to be born as soon as possible.
Lilia Egorova
Harbingers of childbirth - How do you know when it's time to go to the hospital?
January 10, 2017
Alekseeva Inna
Obstetrician-gynecologist, Doctor of the highest category
Subscribe to our Instagram! Useful information about pregnancy and childbirth from leading obstetricians and gynecologists in Moscow and foreign experts: https://www. instagram.com/roddompravda/
instagram.com/roddompravda/
Tips and opinions from leading child professionals: https://www.instagram.com/emc.child/
Every pregnant woman with excitement and joy awaits the upcoming birth. The closer the cherished date, the more attentively the expectant mother listens to the changes taking place in her body and in the behavior of the baby. Of course, the expectant mother wants to know by what signs it is possible to understand that childbirth is just around the corner.
It is customary to call the harbingers of childbirth external, really tangible changes in the body, which are direct preparation for the onset of labor. The tissues of the birth canal - the cervix, vagina, vulva, perineum - become quite elastic, extensible, but at the same time - very strong and resistant to tearing. The cervix is located in the center of the vaginal vault, shortens by almost half its normal length and softens significantly. The cervical canal - the lumen of the cervix connecting the uterine cavity with the vagina - opens slightly, as a result, the diameter of the cervical canal is approximately 2-2. 5 cm. Of course, such a significant "perestroika" takes more than one day.
5 cm. Of course, such a significant "perestroika" takes more than one day.
Female sex hormones are responsible for preparing for childbirth. During the nine months of pregnancy, progesterone "reigns" in the body of the expectant mother. It ensures the normal tone of the uterus (relaxed state of the muscles), the production of cervical mucus - a mucous plug in the cervix that protects the fetus from infection. The amount of progesterone during pregnancy largely determines the normal development and growth of the fetus, the necessary concentration of nutrients and oxygen in the mother's blood, as well as their timely and uninterrupted delivery to the baby.
Shortly before childbirth, the production of progesterone decreases markedly, it is replaced by estrogens - female sex hormones. The increase in estrogen in the blood is caused by the need to prepare the body for the upcoming birth. It is these hormones that are responsible for the elasticity and patency of the birth canal. The rate of cervical dilatation in the first stage of labor depends on them. In the second period, when the cervix is fully opened and the fetus passes through the birth canal, it is also very important how elastic and extensible the walls of the vagina are - this will largely determine the duration of the straining period. Finally, the onset of labor itself depends on the level of estrogen: contractions occur as a result of a nerve impulse that is caused by a certain level (“peak”) of estrogen accumulation.
The rate of cervical dilatation in the first stage of labor depends on them. In the second period, when the cervix is fully opened and the fetus passes through the birth canal, it is also very important how elastic and extensible the walls of the vagina are - this will largely determine the duration of the straining period. Finally, the onset of labor itself depends on the level of estrogen: contractions occur as a result of a nerve impulse that is caused by a certain level (“peak”) of estrogen accumulation.
These changes are normal and do not require an unscheduled visit to the doctor or hospitalization. Harbingers of childbirth are manifestations of a planned restructuring in the body of a future mother, the “finishing touches” of preparation for the upcoming joyful event.
The absence of clearly perceptible changes on the eve of the expected date of birth is also not a pathology. Not all expectant mothers note those changes in well-being that are commonly called harbingers.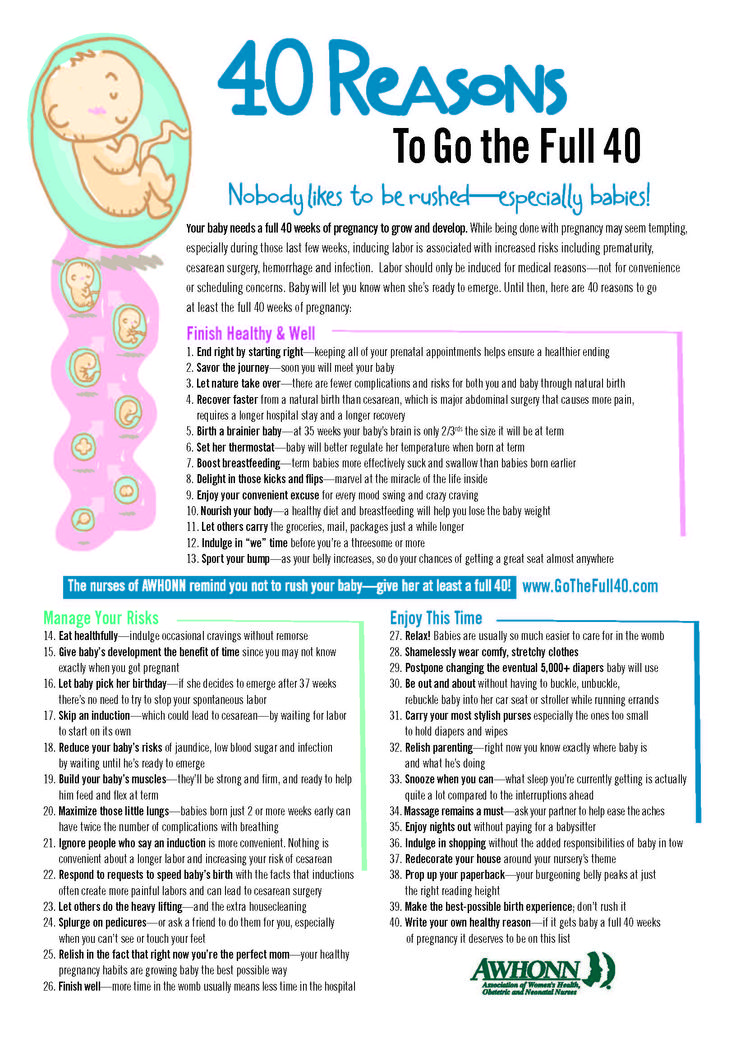 However, this does not mean that there is no preparation. In some cases, the “final preparations” go unnoticed by the pregnant woman. Therefore, do not worry or urgently contact a specialist.
However, this does not mean that there is no preparation. In some cases, the “final preparations” go unnoticed by the pregnant woman. Therefore, do not worry or urgently contact a specialist.
The appearance of any of the "harbingers" indicates the likelihood of the development of regular labor activity over the next two hours - two weeks. None of the sensations described gives a 100% guarantee that a woman will become a mother within the next 24 hours. Hormonal changes before childbirth begin approximately two weeks before the expected birth. Theoretically, during these two weeks, at any time, a pregnant woman can notice certain changes in her state of health. Consequently, the absence of labor activity an hour, a day, or even a week after the first noted changes is not a pathology and does not require special medical advice.
- Scarlet discharge from the genital tract in any amount.
- Severe abdominal pain.
- Increased blood pressure (above 130/80 mmHg).

- An increase in body temperature to 37.5 ° C and above.
- Increased heart rate (more than 100 beats per minute).
- Severe headache, vomiting, blurred vision.
- Significant increase in edema.
- Absence, sharp decrease, sharp increase in fetal movements.
- Suspicion of amniotic fluid leakage.
Weight loss . Shortly before the expected date of delivery, the expectant mother may notice some “weight loss”. Weight loss during this period is associated with the removal of excess fluid from the body, that is, a general decrease in edema. The more pronounced the fluid retention during pregnancy, the more mass the pregnant woman will “lose” on the eve of childbirth. During pregnancy, water is retained in the body of all expectant mothers to a greater or lesser extent. The reason is progesterone - a hormone whose main function is to support the processes of pregnancy. Before childbirth, progesterone is replaced by estrogen. It is estrogen that removes excess fluid from the body. The first results are visible on the hands, feet and legs. Depending on the severity of edema, weight loss before childbirth varies from 0.5 to 2.5 kg.
Before childbirth, progesterone is replaced by estrogen. It is estrogen that removes excess fluid from the body. The first results are visible on the hands, feet and legs. Depending on the severity of edema, weight loss before childbirth varies from 0.5 to 2.5 kg.
Change of stool. Increased frequency and change in the consistency of physiological functions on the eve of childbirth is also associated with an increase in estrogen levels and the removal of fluid from the body of the future mother. Similar changes in the body of a non-pregnant woman are observed during menstruation. The chair can become more frequent up to 2-3 times a day, at the same time there may be some liquefaction of the feces. More frequent urge to defecate, a sharp change in the color and smell of feces, combined with nausea and vomiting, is a reason for consulting a doctor - food poisoning can be masked under such "harbingers".
Fundal prolapse. Shortly before delivery, the baby presses the presenting part (most often the head) against the lower segment of the uterus and pulls it down, pressing against the entrance to the small pelvis. The fetus "groups", taking the most advantageous position for itself at the time of the onset of contractions. As a result of such "preparations" from the side of the fetus, the uterus "sags", and its upper part - the bottom - ceases to exert pressure on the internal organs. After lowering the bottom of the uterus, the pregnant woman has no shortness of breath (it becomes easier to breathe, there is a feeling of a full breath). If in the last month the expectant mother had belching, heartburn, a feeling of heaviness in the stomach after eating, these phenomena disappear when the bottom of the uterus descends. However, lowering down to the pelvic area, the uterus will put more pressure on the internal organs located there. The pelvic organs, in particular, include the bladder. It is located directly in front of the uterus, in its lower part.
Shortly before delivery, the baby presses the presenting part (most often the head) against the lower segment of the uterus and pulls it down, pressing against the entrance to the small pelvis. The fetus "groups", taking the most advantageous position for itself at the time of the onset of contractions. As a result of such "preparations" from the side of the fetus, the uterus "sags", and its upper part - the bottom - ceases to exert pressure on the internal organs. After lowering the bottom of the uterus, the pregnant woman has no shortness of breath (it becomes easier to breathe, there is a feeling of a full breath). If in the last month the expectant mother had belching, heartburn, a feeling of heaviness in the stomach after eating, these phenomena disappear when the bottom of the uterus descends. However, lowering down to the pelvic area, the uterus will put more pressure on the internal organs located there. The pelvic organs, in particular, include the bladder. It is located directly in front of the uterus, in its lower part. Behind the uterus, at a distance of several centimeters, there is an ampulla of the rectum - the output section of the intestine. It is not difficult to guess what the result of pressure on the bladder and rectum will be: the urge to go to the toilet before childbirth can become noticeably more frequent.
Behind the uterus, at a distance of several centimeters, there is an ampulla of the rectum - the output section of the intestine. It is not difficult to guess what the result of pressure on the bladder and rectum will be: the urge to go to the toilet before childbirth can become noticeably more frequent.
Isolation of the mucous plug. During pregnancy, the glands of the mucous membrane of the cervical canal (the lumen of the cervix) secrete a special secret. It is a thick, sticky, jelly-like mass that forms a kind of cork. The mucous plug completely fills the cervical canal, preventing the penetration of bacterial flora from the vagina into the uterine cavity. Thus, cervical mucus, or the mucous plug of the cervix, protects the fetus from ascending infection. Before childbirth, when the cervix begins to soften under the influence of estrogen, the cervical canal opens slightly and the cervical mucus contained in it can be released. In this case, the expectant mother may find small clots of yellowish-brownish mucus, transparent, jelly-like, odorless. The mucous plug can stand out at once or depart in parts during the day. In the latter case, slight discomfort is sometimes noted in the form of "sipping" in the lower abdomen, reminiscent of sensations before or during menstruation. However, most often, the release of the mucous plug is not accompanied by tangible changes in the well-being of the expectant mother. After the discharge of the mucous plug, it is not recommended to visit the pool, swim in the reservoirs and in the bath. When immersed in water, it fills the vagina; thus, in the absence of a mucous plug, the risk of infection of the fetus and membranes through the ajar cervix increases.
The mucous plug can stand out at once or depart in parts during the day. In the latter case, slight discomfort is sometimes noted in the form of "sipping" in the lower abdomen, reminiscent of sensations before or during menstruation. However, most often, the release of the mucous plug is not accompanied by tangible changes in the well-being of the expectant mother. After the discharge of the mucous plug, it is not recommended to visit the pool, swim in the reservoirs and in the bath. When immersed in water, it fills the vagina; thus, in the absence of a mucous plug, the risk of infection of the fetus and membranes through the ajar cervix increases.
Training contractions. Training or false contractions are called such contractions that appear shortly before childbirth and are not actually labor activity, since they do not lead to the opening of the cervix. A contraction is essentially a single contraction of the uterine wall; this contraction usually lasts a few seconds. At the time of the contraction, the expectant mother feels a gradually increasing and then gradually decreasing tension in the abdomen. If at this moment you put your hand on your stomach, you can notice that the stomach becomes very hard, but after the contraction it completely relaxes and becomes soft again. In addition to involuntary tension of the uterus, other changes in the well-being of the expectant mother during false contractions are usually not noted. It is not difficult to distinguish training fights from real ones. In most cases, false contractions are weak, painless, irregular or alternating at a significant interval (30 minutes or more). Labor pains, on the contrary, are distinguished by regularity and a gradual increase in intensity. Unlike false contractions, real contractions lead to a visible result - the opening of the cervix. In doubtful cases, a simple obstetric examination will be enough to make an accurate diagnosis. In other cases, training contractions, like all harbingers of childbirth, do not require a visit to a doctor or hospitalization.
At the time of the contraction, the expectant mother feels a gradually increasing and then gradually decreasing tension in the abdomen. If at this moment you put your hand on your stomach, you can notice that the stomach becomes very hard, but after the contraction it completely relaxes and becomes soft again. In addition to involuntary tension of the uterus, other changes in the well-being of the expectant mother during false contractions are usually not noted. It is not difficult to distinguish training fights from real ones. In most cases, false contractions are weak, painless, irregular or alternating at a significant interval (30 minutes or more). Labor pains, on the contrary, are distinguished by regularity and a gradual increase in intensity. Unlike false contractions, real contractions lead to a visible result - the opening of the cervix. In doubtful cases, a simple obstetric examination will be enough to make an accurate diagnosis. In other cases, training contractions, like all harbingers of childbirth, do not require a visit to a doctor or hospitalization. False contractions may recur for several hours and then stop. Most often, they disturb a pregnant woman in the evening and morning hours for several days.
False contractions may recur for several hours and then stop. Most often, they disturb a pregnant woman in the evening and morning hours for several days.
Discomfort. In the last weeks before giving birth, many pregnant women report discomfort in the lower abdomen and in the area of the sacrum (the area slightly below the waist). Such changes in
the well-being of the expectant mother is caused by sprain of the pelvic ligaments and increased blood flow to the pelvic organs. Usually these minor sensations, described as a feeling of "light languor" in the lower abdomen, are comparable to similar phenomena in the period before or during menstruation. Discomfort, like training contractions, more often disturbs the expectant mother in the morning and evening hours. The level of discomfort is minimal, it should not worry the expectant mother and does not require medical intervention.
All harbingers of childbirth can appear during the last two weeks before childbirth, their presence, as well as their absence, is the norm and does not require a visit to a doctor.