Herniated disc surgery while pregnant
Looking after your back during pregnancy
Looking after your back during pregnancy | Pregnancy Birth and Baby beginning of content4-minute read
Listen
Backache during pregnancy is very common, especially in the later stages when your ligaments loosen and the growing baby affects your posture. The stress on your body caused by pregnancy also puts you at greater risk of back injury.
One reason why your back is at particular risk of injury is that you gain a lot of weight in your abdomen. This puts extra strain on the arch in your lower back and it can also strain the joints.
The changes to your hormones during pregnancy cause your ligaments to relax, which can aggravate your lower spine and pelvis.
If you are unfit, overweight or if you smoke, you are more likely to experience backache or sciatica during pregnancy. Regular exercise can reduce this risk.
Treatment of back injury during pregnancy
If you injure your back while you are pregnant, simple exercises and using back support are usually enough to fix the injury. In very rare cases, pregnant women can have a serious injury such as a herniated disc. In this case you might need surgery. Back surgery is usually safe, however, both for you and your baby during pregnancy.
Many women have a pre-existing back condition before they become pregnant, such as scoliosis, spondylolisthesis or a lumbar disc condition. Sometimes your back problems get better during pregnancy, but sometimes they get worse. It's important to mention any back problems to the medical team who are looking after you.
Talk to your doctor if you need to take medicine to control back pain. Paracetamol is one of the safest painkillers during pregnancy. Do not take aspirin or non-steroidal anti-inflammatories such as Nurofen while you are pregnant.
Your back injury should not affect labour or pain relief during labour. It is also usually possible to have an epidural if you have a back injury. Tell the hospital about your condition because there are different positions you can use to ease back pain during labour.
It is also usually possible to have an epidural if you have a back injury. Tell the hospital about your condition because there are different positions you can use to ease back pain during labour.
How to protect your back
You can protect your back during pregnancy by avoiding or changing the way you do some things. This becomes more important the further along in your pregnancy you are.
- Avoid heavy lifting. If you have to lift something heavy, bend your knees, keep your back straight and tighten your pelvic floor and abdominal muscles. Make sure the object you are lifting stays close to your body. Allow toddlers to climb onto your lap or into the car or bath, and squat down next to them rather than picking them up.
- Always have a good posture. Try to keep your pelvis symmetrical. Stand with your weight evenly on both legs, your back straight and your pelvis tucked under. Avoid standing for a long time. Sit up straight with your bottom at the back of your chair and your feet on a stool if necessary.

- Avoid activities that might hurt your back. These include bending or twisting, climbing ladders, or walking up steep hills.
- Be careful in bed. Sleep on your side with a pillow between your knees. To get out of bed, roll onto your side with your knees together. Then use your arms for support as you swing your legs onto the floor.
- Wear shoes with low heels (not flats). These have good arch support. Avoid high heels.
- Consider a maternity support belt.
Strengthening your back
Regular physical activity is important when you are pregnant and can protect your back. If your doctor says it's OK, you can do some gentle exercise like walking or water exercise. Talk to a physiotherapist for specific exercises to strengthen your back.
Stretch your lower back by kneeling on all fours with your head in line with your back. Pull in your stomach and round your back. Hold the posture for a few seconds and then relax. Repeat 10 times.
Repeat 10 times.
Keep your tummy muscles strong with pelvic tilt exercises. Lie on your back with your knees bent and your feet flat on the ground. Tilt your pelvis and hips backwards so the curve of your back is flat to the floor. Hold for 3 to 5 seconds. You can also do this exercise standing up or sitting on a gym ball.
Strengthen your tummy muscles and pelvic floor by gently drawing in the lower part of your tummy (bellow the belly button) towards your spine. Keep breathing. Gradually lengthen the time you hold the posture. Brace these muscles whenever you lift, push or pull something heavy.
Complementary therapies such as yoga and pilates can help some women, but always talk to your doctor or midwife first.
When to see a doctor
Talk to your doctor if the back pain is severe or if it lasts for more than 2 weeks.
Sometimes back pain can be a sign of premature labour or a urinary tract infection. See your doctor straight away if you also have bleeding from your vagina, painful urination or any signs of premature labour.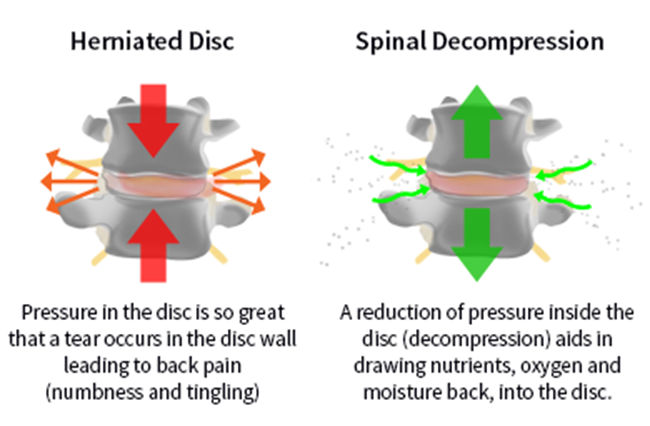
Sources:
The Royal Women's Hospital (Common concerns in early pregnancy), The Royal Women's Hospital (Back care & posture), Women's and Children's Health Network (Caring for your body in pregnancy - physiotherapy advice)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: February 2021
Back To Top
Related pages
- Yoga and Pilates during pregnancy
- Pelvic floor exercises
- Exercising during pregnancy
- Backache in pregnancy
Need more information?
Backache in pregnancy
There are several things you can do to help prevent backache from happening during your pregnancy, and to help you cope with an aching back if it does occur.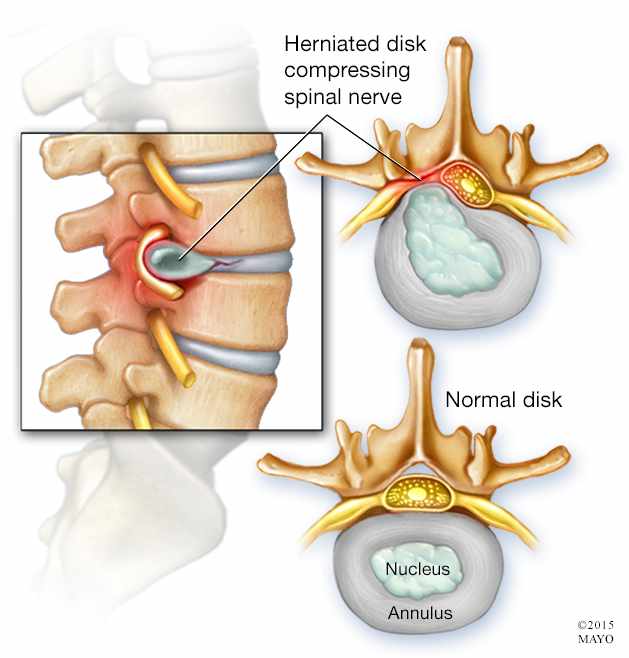
Read more on Pregnancy, Birth & Baby website
Exercising during pregnancy
Doing regular moderate physical activity has health benefits during pregnancy and also helps to prepare the body for childbirth. Read about getting fit during pregnancy.
Read more on Pregnancy, Birth & Baby website
Yoga and Pilates during pregnancy
Yoga and Pilates during pregnancy can be beneficial, but you should be careful to avoid some positions. Find out how yoga and Pilates can help you here.
Read more on Pregnancy, Birth & Baby website
Complementary therapy during pregnancy
About half of Australian women consult a complementary therapist while pregnant.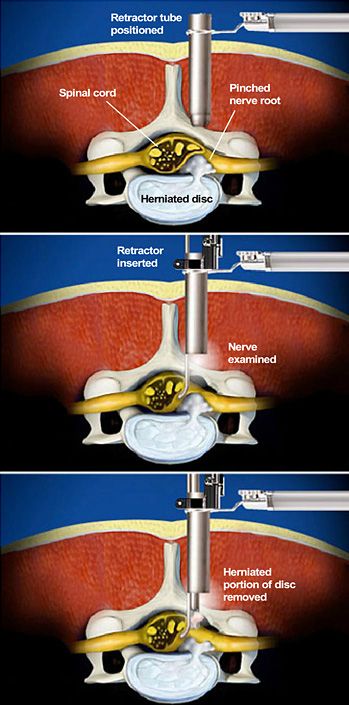 Here's what you should know about integrative medicine and pregnancy.
Here's what you should know about integrative medicine and pregnancy.
Read more on Pregnancy, Birth & Baby website
Antenatal Care during Pregnancy
Read more on RANZCOG - Royal Australian and New Zealand College of Obstetricians and Gynaecologists website
Pregnancy health problems & complications | Raising Children Network
Many pregnancy health problems are mild, but always call your doctor if you’re worried about symptoms. A healthy lifestyle can help you avoid health problems.
Read more on raisingchildren.net.au website
Multiple pregnancy (triplets or more)
Learning you're pregnant with triplets or more can be a shock, but overall, most parents find having multiple babies to be a positive experience.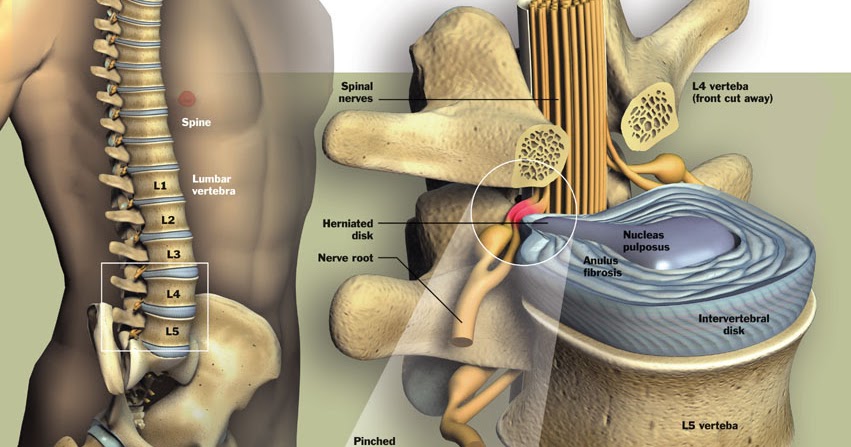
Read more on Pregnancy, Birth & Baby website
Pregnancy at week 33
Your baby's brain and nervous system are now fully developed, and the baby is continuing to gain weight. You'll probably also be feeling sore and tired.
Read more on Pregnancy, Birth & Baby website
Pregnancy at week 22
By week 22, some parts of your baby’s body are fully formed, while some women experience Braxton Hicks contractions about now.
Read more on Pregnancy, Birth & Baby website
Pregnancy at week 38
Your baby is now ready to be born and you could go into labour at any time. Make sure you have you plan for getting to the hospital and you have everything packed ready to go.
Read more on Pregnancy, Birth & Baby website
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now entering.
OKNeed further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
Surgery for lumbar disc herniation during pregnancy
Save citation to file
Format: Summary (text)PubMedPMIDAbstract (text)CSV
Add to Collections
- Create a new collection
- Add to an existing collection
Name your collection:
Name must be less than 100 characters
Choose a collection:
Unable to load your collection due to an error
Please try again
Add to My Bibliography
- My Bibliography
Unable to load your delegates due to an error
Please try again
Your saved search
Name of saved search:
Search terms:
Test search terms
Email: (change)
Which day? The first SundayThe first MondayThe first TuesdayThe first WednesdayThe first ThursdayThe first FridayThe first SaturdayThe first dayThe first weekday
Which day? SundayMondayTuesdayWednesdayThursdayFridaySaturday
Report format: SummarySummary (text)AbstractAbstract (text)PubMed
Send at most: 1 item5 items10 items20 items50 items100 items200 items
Send even when there aren't any new results
Optional text in email:
Create a file for external citation management software
Full text links
Wolters Kluwer
Full text links
Case Reports
. 2001 Feb 15;26(4):440-3.
2001 Feb 15;26(4):440-3.
doi: 10.1097/00007632-200102150-00022.
M D Brown 1 , A D Levi
Affiliations
Affiliation
- 1 Departments of Orthopaedics and Rehabilitation and Neurological Surgery, University of Miami School of Medicine, Miami, Florida, USA. [email protected]
- PMID: 11224893
- DOI: 10.1097/00007632-200102150-00022
Case Reports
M D Brown et al. Spine (Phila Pa 1976). .
. 2001 Feb 15;26(4):440-3.
doi: 10.1097/00007632-200102150-00022.
Authors
M D Brown 1 , A D Levi
Affiliation
- 1 Departments of Orthopaedics and Rehabilitation and Neurological Surgery, University of Miami School of Medicine, Miami, Florida, USA. [email protected]
- PMID: 11224893
- DOI: 10.1097/00007632-200102150-00022
Abstract
Study design: The case reports of three pregnant patients with lumbar disc herniation causing cauda equina syndrome or severe neurologic deficits are presented to illustrate that disc surgery during gestation is a safe method of management.
Objective: To emphasize the importance of recognizing and definitively treating lumbar disc displacement causing neurologic deficits during pregnancy.
Summary of background data: The advent of magnetic resonance imaging and modern surgical techniques for treatment of lumbar disc displacement allows safe management of this condition at any stage of gestation. A review of the literature on the risks of nonobstetric surgery and the risks of delaying disc surgery until delivery shows that operating at any stage during gestation for severe neurologic deficit secondary to lumbar disc displacement is justified.
Methods: A review of the literature on the use of magnetic resonance imaging scan and nonobstetric surgery during pregnancy was performed. Three case reports of the authors' patients who had lumbar disc displacement with cauda equina syndrome or severe neurologic deficit are presented. Patients were placed prone on a four-poster frame, and an epidural anesthetic agent was administered. A one-level hemilaminectomy, partial facetectomy, and disc excision were performed in all three cases.
Patients were placed prone on a four-poster frame, and an epidural anesthetic agent was administered. A one-level hemilaminectomy, partial facetectomy, and disc excision were performed in all three cases.
Results: The methods used for diagnosis and surgical treatment of three patients with disc herniation during pregnancy resulted in a satisfactory outcome for both mother and child. The medical literature supports surgical intervention in pregnant patients with cauda equina syndrome and severe and/or progressive neurologic deficit(s) from lumbar disc displacement at any state of gestation.
Conclusion: Although extremely rare, cauda equina syndrome and severe and/or progressive neurologic deficit caused by lumbar disc displacement can occur during pregnancy. The prevalence of symptomatic lumbar disc herniation during pregnancy may be on the increase because of the increasing age of patients who are becoming pregnant.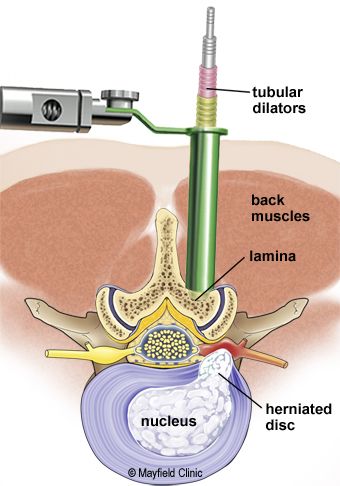 These cases showed, and the literature confirms, that pregnancy at any stage is no contraindication to magnetic resonance imaging scan, epidural and/or general anesthesia, and surgical disc excision.
These cases showed, and the literature confirms, that pregnancy at any stage is no contraindication to magnetic resonance imaging scan, epidural and/or general anesthesia, and surgical disc excision.
Similar articles
-
Cauda equina syndrome as a postoperative complication in five patients operated for lumbar disc herniation.
Henriques T, Olerud C, Petrén-Mallmin M, Ahl T. Henriques T, et al. Spine (Phila Pa 1976). 2001 Feb 1;26(3):293-7. doi: 10.1097/00007632-200102010-00015. Spine (Phila Pa 1976). 2001. PMID: 11224866
-
[Posterior migration of a lumbar disc herniation as a cause of cauda equina syndrome].
Elgamri A, Sami A, Aqqad A, Hilmani S, Ibahioin K, Naja A, El Kamar A, El Azhari A. Elgamri A, et al.
 J Radiol. 2009 Jun;90(6):731-3. doi: 10.1016/s0221-0363(09)74728-6. J Radiol. 2009. PMID: 19623126 French.
J Radiol. 2009 Jun;90(6):731-3. doi: 10.1016/s0221-0363(09)74728-6. J Radiol. 2009. PMID: 19623126 French. -
RE: Cauda equina syndrome as a postoperative complication in five patients operated for lumbar disc herniation. Spine 2001; 26: 293-7.
Fraser RD. Fraser RD. Spine (Phila Pa 1976). 2001 Nov 1;26(21):2404-5. doi: 10.1097/00007632-200111010-00026. Spine (Phila Pa 1976). 2001. PMID: 11679831 No abstract available.
-
Posterior epidural migration of a lumbar disc fragment: a series of 6 cases.
Akhaddar A, El-Asri A, Boucetta M. Akhaddar A, et al. J Neurosurg Spine. 2011 Jul;15(1):117-28. doi: 10.3171/2011.3.SPINE10832. Epub 2011 Apr 8. J Neurosurg Spine. 2011. PMID: 21476800 Review.
-
Posterior epidural migration of sequestered lumbar disc fragment causing cauda equina syndrome.
Tatli M, Güzel A, Ceviz A, Karadağ O. Tatli M, et al. Br J Neurosurg. 2005 Jun;19(3):257-9. doi: 10.1080/02688690500208593. Br J Neurosurg. 2005. PMID: 16482671 Review.
See all similar articles
Cited by
-
Microdiscectomy Under Local Anesthesia and Spinal Block in a Pregnant Female.
Babici D, Johansen PM, Newman SL, O'Connor TE, Miller TD. Babici D, et al. Cureus. 2021 Dec 7;13(12):e20241. doi: 10.7759/cureus.20241. eCollection 2021 Dec. Cureus. 2021. PMID: 35004056 Free PMC article.
-
Critical COVID-19 in a pregnant patient who presented in starvation ketoacidosis with a background history of acrorenal syndrome.

Brady A, Aglan A. Brady A, et al. BMJ Case Rep. 2021 Nov 2;14(11):e244117. doi: 10.1136/bcr-2021-244117. BMJ Case Rep. 2021. PMID: 34728503 Free PMC article.
-
Anaesthetic Management in Successive Spinal Surgeries During Pregnancy and Postpartum.
Coşkun D, Mahli A, Sabuncu Ü, Özdemir R, Emmez H, Günaydın DB. Coşkun D, et al. Turk J Anaesthesiol Reanim. 2020 Oct;48(5):420-422. doi: 10.5152/TJAR.2020.31698. Epub 2020 Feb 5. Turk J Anaesthesiol Reanim. 2020. PMID: 33103149 Free PMC article.
-
The Management of Symptomatic Lumbar Disc Herniation in Pregnancy: A Systematic Review.
Whiles E, Shafafy R, Valsamis EM, Horton C, Morassi GL, Stokes O, Elsayed S. Whiles E, et al. Global Spine J.
 2020 Oct;10(7):908-918. doi: 10.1177/2192568219886264. Epub 2019 Dec 26. Global Spine J. 2020. PMID: 32905728 Free PMC article.
2020 Oct;10(7):908-918. doi: 10.1177/2192568219886264. Epub 2019 Dec 26. Global Spine J. 2020. PMID: 32905728 Free PMC article. -
Medical and surgical management of acute spinal injury during pregnancy: A case series in a third-world country.
Zemmar A, Al-Jradi A, Ye V, Al-Kebsi I, Andrade-Barazarte H, Zemmar E, Avecillas-Chasin J, Cherian I, Krassioukov AV, Hernesniemi J. Zemmar A, et al. Surg Neurol Int. 2018 Dec 24;9:258. doi: 10.4103/sni.sni_380_18. eCollection 2018. Surg Neurol Int. 2018. PMID: 30687569 Free PMC article.
See all "Cited by" articles
Publication types
MeSH terms
Full text links
Wolters Kluwer
Cite
Format: AMA APA MLA NLM
Add to Collections
- Create a new collection
- Add to an existing collection
Name your collection:
Name must be less than 100 characters
Choose a collection:
Unable to load your collection due to an error
Please try again
Send To
How is the operation to remove the intervertebral disc herniation – Department of Vertebrology of the Central Clinical Hospital of the Russian Academy of Sciences
Herniated discs require surgery in only 30% of cases. If compression of the spinal cord and nerve roots occurs, surgery is indispensable. Several methods of surgical treatment are used, the choice depends on the characteristics of the clinical picture and is determined individually only after the examination.
If compression of the spinal cord and nerve roots occurs, surgery is indispensable. Several methods of surgical treatment are used, the choice depends on the characteristics of the clinical picture and is determined individually only after the examination.
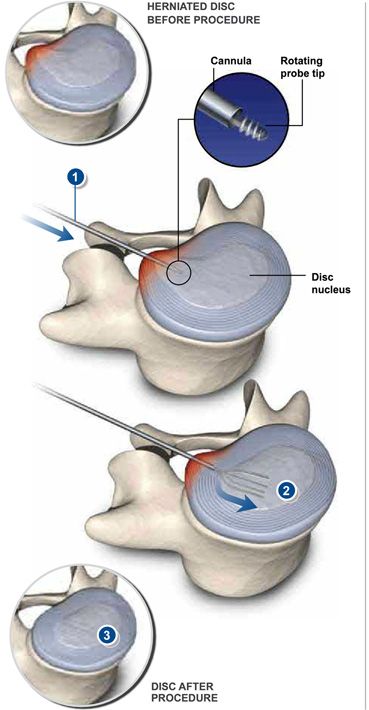
Microdiscectomy
The technology of modern microsurgery, involving the removal of a hernia through a minimal tissue incision. The procedure is considered one of the most gentle and safe interventions. The rehabilitation period is minimal, the patient returns to normal very quickly and returns to active life in less than a month after the operation.
The operation is performed with a high-tech instrument using a microscope for maximum precision. Due to this, hard and soft tissues remain undamaged, the squeezing effect on the nerves is eliminated.
Endoscopic removal
This technique uses fiber optic equipment, allowing the surgeon to move with maximum precision and control of the technique with high image resolution. The tissues are minimally injured, due to which the elimination of the pathology is effective, and the recovery process is not complicated by a full-scale intervention.
The tissues are minimally injured, due to which the elimination of the pathology is effective, and the recovery process is not complicated by a full-scale intervention.
A small incision is made to provide access to the back. The patient can walk normally a day after the intervention, the risk of complications is minimal.
Laser irradiation
A modern technique that involves the use of laser exposure. This is the latest approach to hernia repair, which is carried out in three stages:
- Insertion of a light guide into the spine.
- Heating fabrics that have been bulging.
- Evaporation of fluid that triggers the spine's own regeneration processes.
This effect helps to eliminate the problem without harming the intervertebral disc. The recovery is quite long, the pain can be felt for months after the operation, decreasing gradually. For rehabilitation, it is very important to perform physical therapy exercises.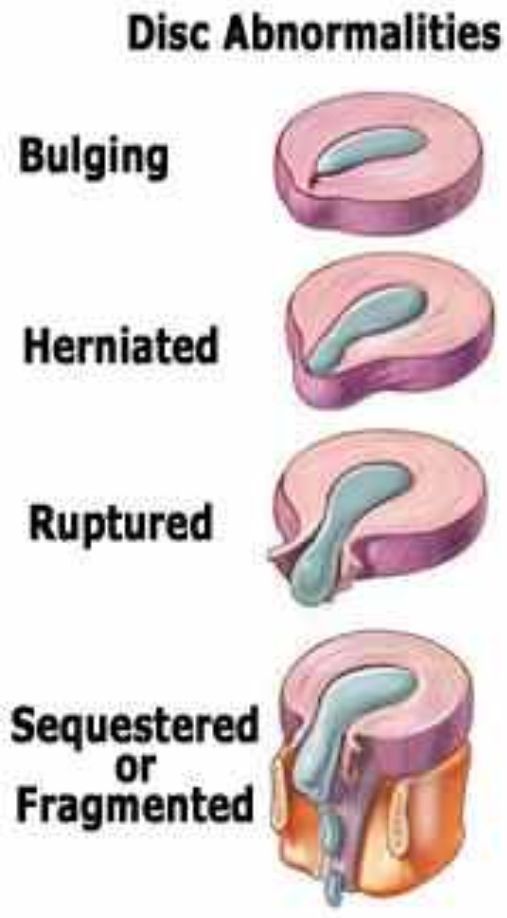
Vertebroplasty
Vertebroplasty is a plastic surgery on the vertebrae, which allows you to restore their shape and function by replenishing the missing tissues of the destroyed elements. Thus, it is possible to prevent destruction and stop the deformation, which will inevitably progress without surgery. Recovery of spinal functions is accelerated, recovery does not take much time.
Operation type selection
The method of the operation is chosen strictly individually, taking into account all the characteristics of the patient, the clinical picture, the complexity of the case and other points. First of all, the accuracy of the diagnosis is important. This requires a full examination, an MRI or CT scan of the spine, the exclusion of concomitant pathologies that may interfere with recovery.
Behavior after surgery
It is not so much the operation that plays a decisive role in the process of recovery, but the behavior of the patient after it. It is important to follow all the instructions of the doctor and attend the prescribed procedures. This can be physiotherapy exercises, a massage course, physiotherapy procedures, standard household restrictions during the restoration of the full functions of the spine. Compliance with the recommendation will ensure a quick recovery and a complete cure for the disease.
It is important to follow all the instructions of the doctor and attend the prescribed procedures. This can be physiotherapy exercises, a massage course, physiotherapy procedures, standard household restrictions during the restoration of the full functions of the spine. Compliance with the recommendation will ensure a quick recovery and a complete cure for the disease.
Microsurgical removal of spinal hernia (microdiscectomy)
Microsurgical operations to remove a hernia of the spine (microdisectomy) are performed according to medical indications, if conservative therapy does not give a positive result, and chronic pain in the extremities and back with concomitant neurological symptoms does not go away. The essence of this method of surgical treatment is that the herniated disc is removed through a small incision in the skin (2-3 cm), and the neurosurgeon uses magnifying optics and special microsurgical instruments during the intervention.
Currently, microsurgical removal of spinal hernia gives a good clinical result.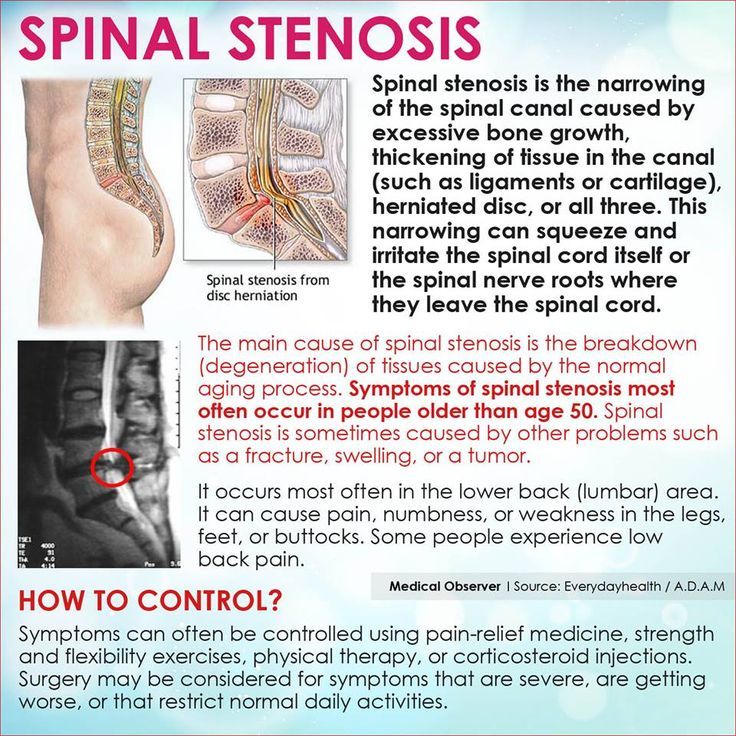 Traumatization of the skin during such an operation is insignificant, and the risk of damage to important neurovascular structures is minimized.
Traumatization of the skin during such an operation is insignificant, and the risk of damage to important neurovascular structures is minimized.
Recovery is relatively comfortable: patients recover quickly and return to normal life within 1-1.5 months.
It should be noted that the scope of microsurgical techniques is not limited to the elimination of hernia and associated pathological symptoms. Such an operation can be indicated for the treatment of spinal stenosis, spondylolisthesis and a number of other diseases.
The purpose of a microsurgical operation to remove a hernia of the spine is to remove the prolapsed nucleus or disc fragment, that is, to free the spinal canal - decompression of the spinal roots and nerve endings. As a result of such an operation, the pain in the arm or leg disappears, normal motor function is restored. It should be noted that our clinic has created conditions for interventional pain treatment, which is also aimed at eliminating painful sensations, which in some cases allows treating spinal hernia without surgery.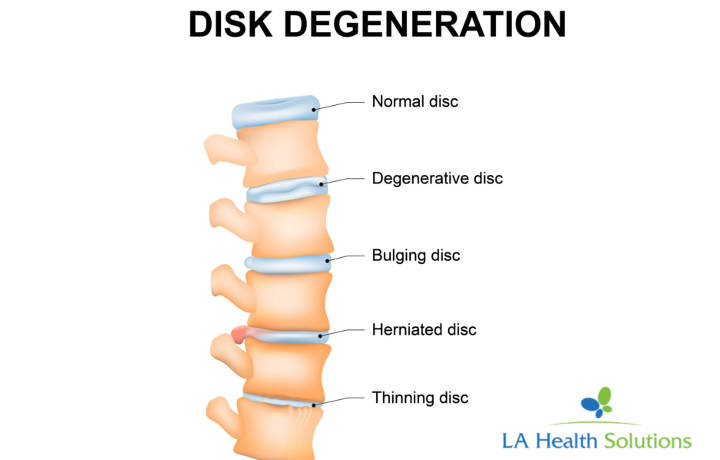 In most cases, if there are indications for surgical treatment of spinal diseases, we recommend endoscopic surgeries to patients, since they are minimally invasive, maximally safe and require an even shorter recovery. And for example, with a hernia in the cervical spine, endoscopic surgery allows you to avoid the installation of cages or implants, which are necessary if the operation is performed by a microsurgical method. However, in some patients, due to individual anatomical features and the specifics of the clinical picture, endoscopic interventions are inappropriate. In this case, microsurgery is the best alternative.
In most cases, if there are indications for surgical treatment of spinal diseases, we recommend endoscopic surgeries to patients, since they are minimally invasive, maximally safe and require an even shorter recovery. And for example, with a hernia in the cervical spine, endoscopic surgery allows you to avoid the installation of cages or implants, which are necessary if the operation is performed by a microsurgical method. However, in some patients, due to individual anatomical features and the specifics of the clinical picture, endoscopic interventions are inappropriate. In this case, microsurgery is the best alternative.
Since the case of each patient is special, the treatment tactics are determined after studying the current MRI images, complaints and anamnesis at the consultation of a neurosurgeon. On the eve of the operation, it is necessary to undergo a preoperative examination to identify possible contraindications and hidden risks.
Microsurgical hernia removal: how does this spinal surgery work?
Microsurgical removal of a spinal hernia (microdisectomy) is performed under general anesthesia. After X-ray marking, which allows you to determine the area of hernia localization as accurately as possible, the neurosurgeon makes an incision on the skin up to 3 cm and, under X-ray navigation, installs a special sparing retractor in the projection of the location of the intervertebral hernia or stenosis.
After X-ray marking, which allows you to determine the area of hernia localization as accurately as possible, the neurosurgeon makes an incision on the skin up to 3 cm and, under X-ray navigation, installs a special sparing retractor in the projection of the location of the intervertebral hernia or stenosis.
Surgical intervention is performed using magnifying optics and micro-instruments, which allows you to carefully bypass the muscles, ligaments and spinal nerves without damaging them. The hernia is removed with micronippers, after the intervention the wound is sutured. The duration of the operation is 30-90 minutes.
Recovery after herniated disc removal
After microsurgical removal of the spinal hernia, the patient is transferred to a comfortable ward. After 5-6 hours, he can walk on his own, but sitting is not recommended yet. Within 1-2 days, the patient is in the clinic under the supervision of doctors and nurses, and then the doctor can discharge him from the clinic home with individual recommendations for recovery.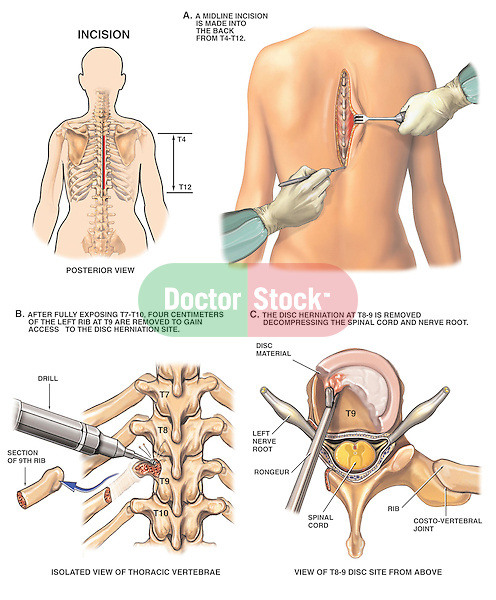 Dressings should be done daily. The suture is removed on the 10th day after the operation. In most patients, pain in the extremities resolves immediately after surgery. The feeling of numbness may persist for some time, depending on how long the patient tolerated the symptoms of a herniated disc. The sooner treatment is started, the higher the likelihood that numbness and paralysis of the limbs are reversible and will quickly pass after surgery.
Dressings should be done daily. The suture is removed on the 10th day after the operation. In most patients, pain in the extremities resolves immediately after surgery. The feeling of numbness may persist for some time, depending on how long the patient tolerated the symptoms of a herniated disc. The sooner treatment is started, the higher the likelihood that numbness and paralysis of the limbs are reversible and will quickly pass after surgery.
Recovery takes, on average, 1-1.5 months , however, patients return to normal life and non-physical work much faster. At first, you can not lift weights, and increased physical exertion should be avoided. Walking and swimming are recommended.
The price of a microsurgical operation to remove a hernia of the spine depends on a number of factors: on the location of the pathology (in the cervical, thoracic or lumbar spine), on whether the installation of a fixator (implant, interbody cage) is required, on the length of stay in the ward, etc. . It is possible to clarify the final cost of treatment after determining its tactics, that is, after consulting a neurosurgeon.
. It is possible to clarify the final cost of treatment after determining its tactics, that is, after consulting a neurosurgeon.
N.I. Pirogov?
The Department of Spinal Neurosurgery of the Pirogov Clinic is known in St. Petersburg and beyond due to its technological equipment and high professionalism of doctors. Find out more here and read our patient testimonials. The clinic has created conditions for:
Leading physician Amir Muratovich Meredzhi (Merzhoev) is the leader of positive reviews and is in the TOP-10 best neurosurgeons in St. Petersburg according to the independent platform Napopravku.ru. We highly value the health, safety and comfort of our patients, so we offer:
- Own laboratory equipped with the latest equipment.
 Accurate diagnostic results can be obtained in a short time, without queues and by e-mail.
Accurate diagnostic results can be obtained in a short time, without queues and by e-mail. - Day hospital, rooms of high comfort and class "Lux".
- Availability of all narrow-profile doctors (the highest category, candidates and doctors of sciences), as well as other medical specialists in one place;
- A system of cumulative discounts and special offers for endoscopic / microsurgical operations on the spine.
- Interest-free installment plan / treatment loan.
- Service under VHI policies.
WANT TO ASK A QUESTION ABOUT YOUR OCCASION? SEND YOUR MRI IMAGES
How to describe your complaints correctly:
- Describe in detail: the nature and localization of pain; the presence and localization of numbness and weakness in the limbs; conditions for the onset or intensification of pain; the presence of morning stiffness in the back; whether there is relief after "pacing"; whether the pain gets worse after prolonged sitting or standing; what worries more pain in the back / neck or leg / arm, it is desirable to evaluate both on a 10-point scale; whether the pain increases after flexion-extension; Is there relief after rest? whether there is an increase / increase in weakness / numbness in the legs after walking a certain distance with relief after stopping and bending or sitting down; is there a temperature; Is there an increase in pain at night and so on.
- Medical history: duration of the disease, provoking factors, what you attribute the onset of the disease to, the treatment being carried out, the dynamics of the condition.
- Presence of other diseases.
- What hinders you the most? what would you like to get rid of? What are your expectations from the operation, if it is necessary?
How to send MRI images correctly
MRI images (not a doctor's report, but images) must be on a disk, made on a device with a magnetic field voltage of at least 1.5 Tesla.
- Insert disc into CD-ROM.
- Copy folder with pictures in one file ENTIRELY to computer (right mouse button).
- Name the copied file with your last name.
- Add file to archive (right mouse button).
- To upload MRI images (DICOM files), use an external cloud storage, such as Yandex Disk, Dropbox or Google Drive. Paste in the field above the link to the file or archive from the cloud storage.