Heartburn during third trimester
Feeling the burn? Tips to manage heartburn, GERD in pregnancy | Your Pregnancy Matters
×
What can we help you find?Refine your search: Find a Doctor Search Conditions & Treatments Find a Location
Appointment New Patient Appointment
or Call214-645-8300
MedBlog
Your Pregnancy Matters
July 30, 2019
Your Pregnancy Matters
Robyn Horsager-Boehrer, M. D. Obstetrics and Gynecology
Alan Kramer, M.P.H. Assistant Vice President for Health System Emerging Strategies
The pregnancy hormone progesterone can increase heartburn, starting in the first trimester.Heartburn is common in adults – especially during pregnancy. While some research suggests women who have moderate heartburn during pregnancy give birth to babies with fuller heads of hair, having symptoms more than twice a week might be a sign of gastroesophageal reflux disease (GERD), or recurrent heartburn.
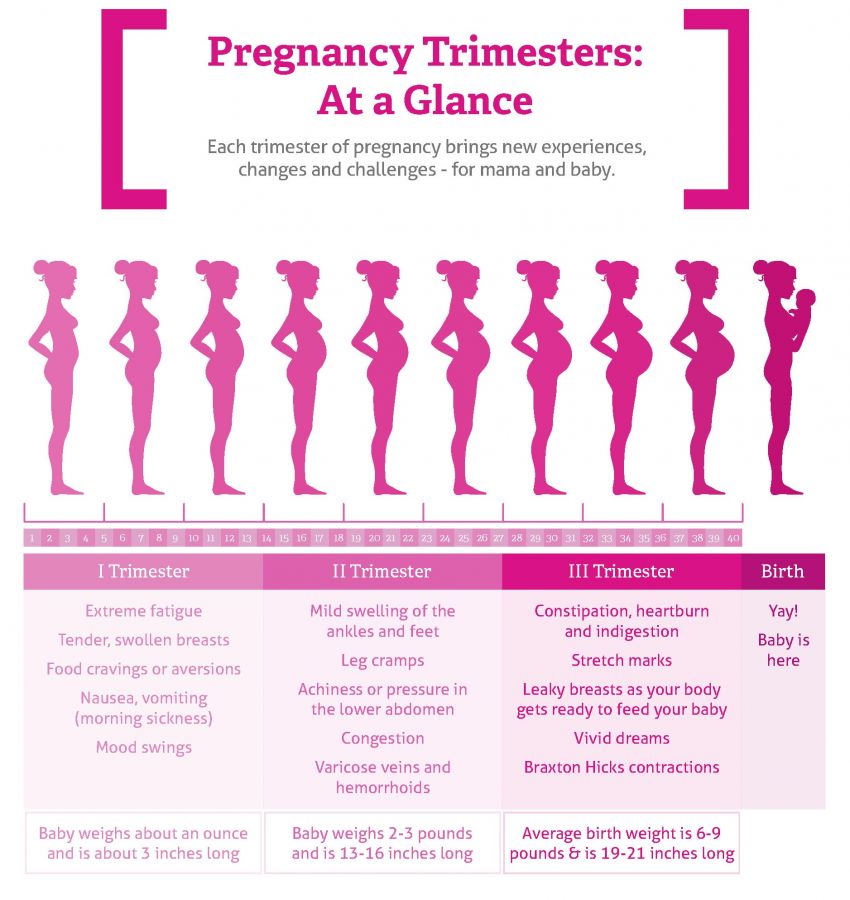
According to a study of 510 pregnant women, approximately 26% have GERD symptoms during the first trimester. The rate jumps to 36% in the second trimester and 51% during the third trimester. That’s substantial compared with the 20% of adults in the U.S. who experience heartburn.
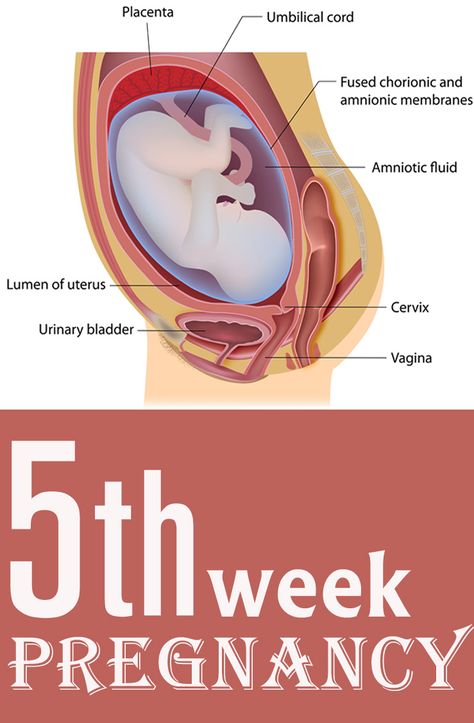
Why the increase in symptoms during pregnancy? Progesterone, a hormone that increases early in pregnancy, relaxes smooth muscle in the body. It helps your uterus stretch to accommodate the growing fetus, but also reduces the reliability of the esophageal sphincter – a ring-like structure that seals off stomach contents from the throat.
Increased pressure placed on the stomach externally from the growing uterus, especially in the third trimester, can also worsen heartburn symptoms such as:
- Burning pain in the center of the chest, especially after eating
- Sour or bitter taste in the mouth
- Sore throat or cough
Thankfully, there are several pregnancy-safe ways to deal with acute heartburn and ongoing cases of GERD.
"Progesterone, a hormone that increases early in pregnancy, also reduces the reliability of the esophageal sphincter, which means that certain foods such as spicy dishes may trigger heartburn symptoms."
Robyn Horsager-Boehrer, M.D.
Heartburn treatment options during pregnancy
Lifestyle changes
Consider these diet and sleep modifications to relieve or prevent heartburn:
- Avoid tobacco and alcohol. These substances worsen the symptoms, and it’s already recommended for all women during pregnancy to avoid smoking, vaping, and drinking alcohol. Need to quit? We offer a free tobacco cessation program.
- Shift your eating schedule. Smaller, more frequent meals fill the stomach less and may reduce symptoms. Also, avoid bending over or lying flat after meals to reduce acid reflux.

- Prop yourself up in bed. Try sleeping with an extra pillow under your head or a small wedge under your pillow. The incline can help prevent stomach acid from splashing into your lower esophagus.
- Skip the sauce or spice. If you notice that certain foods such as tomato sauces or spicy dishes trigger symptoms, avoid them until after the baby comes.
Medications
Heartburn and GERD symptoms are less severe when there is less acid in the stomach. That said, you need a certain amount of acid to properly digest food. Three types of medication can help create that balance.
Oral antacids like aluminum and magnesium hydroxide (think Maalox or Mylanta) and calcium carbonate (like TUMS) neutralize acid already present in the stomach. Calcium carbonate has the added benefit of supplementing calcium intake during pregnancy. It’s safe to follow the directions on the package – there’s no need to change the dosage or schedule due to pregnancy.
It’s safe to follow the directions on the package – there’s no need to change the dosage or schedule due to pregnancy.
On the flip side, two types of medications actually reduce acid production before it can enter the stomach.
h3-receptor antagonists (h3-blockers) reduce h3 histamine, which stimulates cells in the stomach to produce acid. Thus, less stomach acid is produced. Examples include ranitidine (Zantac), cimetidine (Tagamet HB), and famotidine (Pepcid). All of these are available over the counter and in generic forms.
Proton pump inhibitors (PPIs) block an enzyme in stomach cells that’s needed to produce acid. These drugs are available over the counter but can take several days to provide maximum relief, so you might consider trying an antacid or h3 blocker first. Examples of PPIs include lansoprazole (Prevacid) and omeprazole (Prilosec), as well as generic versions. Both brand name and generic are considered safe during pregnancy.
Please note, because stomach acid is necessary for iron absorption, h3 blockers and PPIs can decrease the effectiveness of iron supplements. Talk to your doctor if this might be an issue for you.
Talk to your doctor if this might be an issue for you.
Related reading: 4 common pregnancy-related GI issues
When to call the doctor
If heartburn symptoms are associated with headaches or swelling of the hands and face, talk with your provider before trying these remedies, especially if the symptoms are new and present in the last trimester of pregnancy.
Heartburn-like pain can be a symptom of preeclampsia, or dangerously high blood pressure during pregnancy. Preeclampsia puts mothers and babies at risk, and further evaluation may be necessary.
As mentioned, heartburn is very common in pregnancy. If your symptoms don’t resolve with diet changes or medication, let your provider know so you can find an effective treatment.
Tired of feeling the burn? Call 214-645-8300 or request an appointment online.
More in: Your Pregnancy Matters
Mental Health; Your Pregnancy Matters
- Robyn Horsager-Boehrer, M.
 D.
D.
October 11, 2022
Prevention; Your Pregnancy Matters
- Robyn Horsager-Boehrer, M.D.
October 4, 2022
Mental Health; Your Pregnancy Matters
- Meitra Doty, M.
 D.
D.
September 27, 2022
Your Pregnancy Matters
- Robyn Horsager-Boehrer, M.D.
September 20, 2022
Men's Health; Women's Health; Your Pregnancy Matters
- Yair Lotan, M.
 D.
D.
September 6, 2022
Your Pregnancy Matters
August 29, 2022
Your Pregnancy Matters
- Patricia Santiago-Munoz, M.D.
August 23, 2022
Mental Health; Your Pregnancy Matters
August 11, 2022
Your Pregnancy Matters
- Emily Adhikari, M.
 D.
D.
August 2, 2022
More Articles
© 2022 The University of Texas Southwestern Medical Center
Member of Southwestern Health Resources
Indigestion and heartburn in pregnancy
Indigestion and heartburn in pregnancy | Pregnancy Birth and Baby beginning of content3-minute read
Listen
Many women experience indigestion and heartburn while they are pregnant, which can be painful or uncomfortable. There are ways to help avoid or treat indigestion and heartburn, especially if it is mild. Sometimes the feeling of heartburn can be confused with a more serious condition called pre-eclampsia.
Indigestion, also called 'dyspepsia', is a feeling of pain or discomfort in the stomach (upper abdomen, or, tummy). This mostly occurs after eating or drinking but can happen some time after.
If you have indigestion in the early stage of your pregnancy, this may be caused by changes in your hormone levels. In the second or third trimester, indigestion becomes more common and may be caused by your baby pushing up against your stomach. As many as 8 in 10 women may have indigestion during their pregnancy.
Symptoms of indigestion may include:
- heartburn
- reflux or regurgitation (food coming back up from your stomach)
- burping
- feeling heavy, bloated or full
- feeling sick
- vomiting
Heartburn is a burning pain in the throat or chest, behind the breastbone, caused by stomach acid coming up the oesophagus (the tube that connects your mouth to your stomach) and irritating the lining.
In pregnant women, indigestion and heartburn can be caused by:
- eating a big meal
- eating high-fat foods
- eating chocolate or peppermint
- drinking fruit juice or caffeinated beverages (coffee, tea, cola drinks)
- doing physical activity soon after eating
- bending over
- feeling anxious
It's a good idea to take note of the particular foods, drinks or activities that give you indigestion while you are pregnant.
Avoiding indigestion and heartburn
If your symptoms are mild, it's possible that changes to your diet or lifestyle may help prevent indigestion and heartburn. You could try:
- eating smaller meals, more often
- avoiding eating just before bed
- avoiding foods and drinks that you suspect give you heartburn
- not drinking a lot of coffee at the end of the day
- avoiding eating and drinking at the same time, which can make your stomach more full
- sitting up straight while eating, and not lying down after a meal
- chewing gum, which may cause you to produce more saliva to help neutralise the acid
- stop smoking
- raise the head of your bed by 10 to 15cm
- sleep on your left side
If your indigestion is not helped by diet and lifestyle changes, or your symptoms are more severe, your doctor or midwife may suggest that you take a medicine for indigestion that is safe to use during pregnancy. Medicines can neutralise the acid in your stomach, reduce the amount of acid produced by your stomach and stop the acid rising into your oesophagus.
Heartburn symptoms and pre-eclampsia
If your heartburn symptoms don't go away with medicine, it's important to see your doctor as it may be a sign of something more serious, such as pre-eclampsia. A pregnant woman with pre-eclampsia usually has high blood pressure and problems with her kidneys. Pre-eclampsia could also seriously affect a woman's liver, blood and brain. Any pregnant woman can experience pre-eclampsia – almost 1 in 20 Australian women will develop it.
Because pre-eclampsia is dangerous for both you and your baby, you should let your doctor know if your heartburn medicine is not working. This is especially important if you're also feeling very unwell or you have:
- sudden swelling of your hands, feet or face
- a headache that doesn't go away with simple painkillers
- problems with your eyesight such as blurring or seeing flashing lights or dots
- a strong pain below your ribs
Find out more about how pre-eclampsia is treated here.
Call Pregnancy, Birth and Baby on 1800 882 436 to speak to a maternal child health nurse.
Sources:
Royal Australian and New Zealand College of Obstetricians and Gynaecologists (Pre-eclampsia and high blood pressure during pregnancy), Gastroenterological Society of Australia (Heartburn - Oesophageal Reflux), Gastroenterological Society of Australia (Heartburn - Reflux), King Edward Memorial Hospital (Minor symptoms or disorders in pregnancy), Raising Children Network (Health problems in pregnancy), Royal Australian and New Zealand College of Obstetricians and Gynaecologists (Antenatal care during pregnancy), Department of Health (Clinical Practice Guidelines: Pregnancy Care), Mater Mothers Hospital (Pregnancy information for women and families)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: May 2020
Back To Top
Related pages
- Pre-eclampsia
- Common discomforts during pregnancy
Need further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.
This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
Heartburn - a frequent companion of the third trimester of pregnancy
Other articles on topics: heartburn, gynecology, women's health
-
Analyzes for partners
-
Arterial pressure
-
Autism (RAS)
-
Pregnancy
-
Infertility
-
Sore throat
-
Lower back pain
-
vaginismus
-
papilloma virus
-
Ectopic pregnancy
-
Intrauterine surgery
-
Contraceptive issues
-
Questions to the pediatrician
-
Vulvitis
-
Urine excretion
-
Hymenoplasty
-
Hypertension during pregnancy
-
Hysteroresectoscopy
-
Hysteroscopy
-
Hormonal order
-
flu during pregnancy
-
Pediatric ophthalmologist
-
Ovarian dysfunction
-
Prolonged menstruation
-
Fatty hepatosis
-
Heartburn during pregnancy
-
Artificial insemination
-
Ovarian cyst
-
ovarian cysts
-
Climax
-
insidious syndrome
-
Conization of the cervix
-
Beautiful tan
-
A holiday romance
-
Laparoscopy
-
Treatment of uterine fibroids
-
Treatment of endometritis
-
oligohydramnios
-
Menstrual cup
-
Migraine during pregnancy
-
uterine fibroids
-
Myths in gynecology
-
Myths about diabetes
-
Myths about COC
-
Polyhydramnios
-
Uric acid
-
Tube obstruction
-
Ovulation
-
Ozone therapy
-
Prolapse of the uterus
-
oral contraception
-
Oral contraceptives
-
hypothermia
-
Nutrition for pregnant women
-
Plastic Long Lift
-
Preparing for pregnancy
-
Gender of the child
-
Uterine polyp
-
Pollinosis during pregnancy
-
Premenstrual syndrome
-
Items in the nose
-
Cancer shot
-
Habitual miscarriage
-
Uterine cancer
-
Hidden pregnancy
-
Dark stripe on belly
-
Pulls the stomach
-
Removal of uterine fibroids
-
Fasting
-
Phytopreparations
-
Chronic fatigue
-
Chronic endometritis
-
cystitis during pregnancy
-
IVF fertilization
-
endometriosis
-
Endometrial cyst
-
Enuresis
-
Cervical erosion
Heartburn is a frequent companion of the third trimester of pregnancy, more than half of pregnant women experience it.
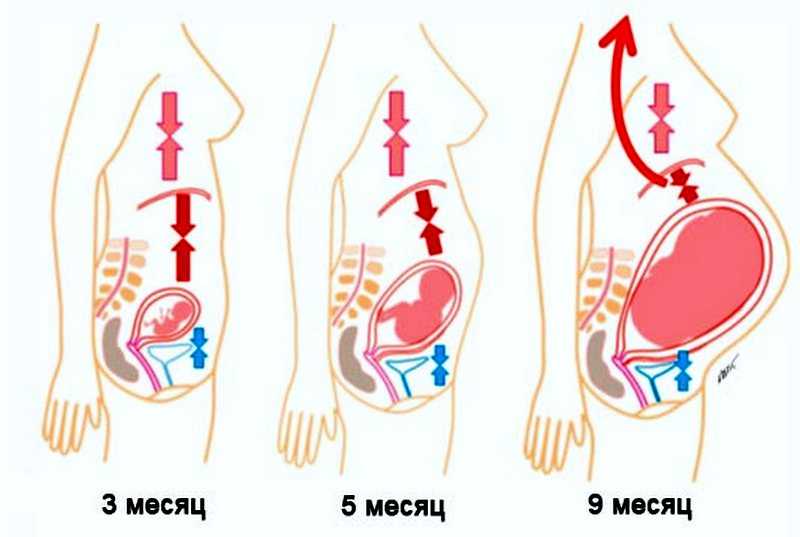 Heartburn develops when acidic contents of the stomach are thrown into the esophagus, the mucous membrane of which actually receives a chemical burn with hydrochloric acid of gastric juice, which causes these sensations.
Heartburn develops when acidic contents of the stomach are thrown into the esophagus, the mucous membrane of which actually receives a chemical burn with hydrochloric acid of gastric juice, which causes these sensations. During pregnancy, especially from the third trimester, very favorable conditions for the occurrence of heartburn: the internal volume of the abdominal cavity decreases, more and more space is occupied by the pregnant uterus and there is less and less room for the stomach. Due to the increase in the level of progesterone, as pregnancy progresses, the evacuation of gastric contents slows down and the tone of the gastroesophageal sphincter, the circular muscle, the main purpose of which is to prevent the contents of the stomach from being thrown into the esophagus, decreases.
Treatment of heartburn
Fortunately, there are ways to deal with this not too dangerous, but very unpleasant condition. They can be divided into non-drug and drug.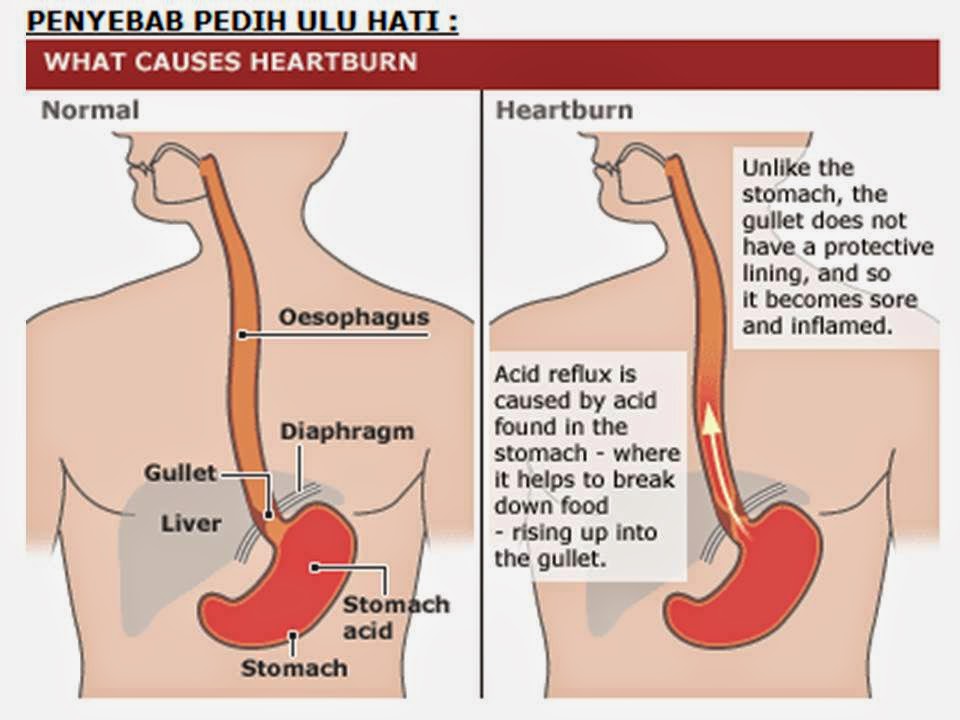
It is worth switching to medication only after all non-drug measures to relieve heartburn have been applied, if they have not brought a clear improvement.
What are these measures (you need to use them simultaneously, not in the order of writing):
- keep a food diary for a week, where to write down what was eaten and when heartburn occurred - this will help you independently identify those that are guaranteed to cause you heartburn products and, if possible, eliminate them from the diet. Very often provokes heartburn fatty, spicy and fried foods;
- change the diet - eat often and in small portions, eat as slowly as possible, reduce the amount of fluid you drink with meals;
- do not lie down or bend over for two hours after eating, maximum - you can sit back, reclining in an armchair or on a sofa;
- Raise the head of the bed 10 centimeters by placing something under the legs of the bed. If this is not possible, at least use pillows in such a way as to achieve the same effect.
 The upper half of your body should be elevated during sleep;
The upper half of your body should be elevated during sleep; - learn to sleep on the left side;
- do not wear tight clothing, preferring loose clothing;
- try to avoid constipation;
- Some foods can be used to stop heartburn attacks (they do not help everyone, but they are all worth trying): whole milk (if you can tolerate it), sour-milk products, puddings, grated raw carrots, sunflower seeds.
In case of insufficient effectiveness of the above measures, you should consult a doctor for a prescription drug therapy. Some antacids are used, with preference given to those that cause the least constipation (a common side effect of this group of drugs), as well as proton pump inhibitors, the most studied in terms of safety in pregnancy.
Make an appointment with a gynecologist
For more details, consult a qualified specialist at the Semeynaya clinic.
To find out the prices for a gynecologist's appointment or other questions, follow the link below:
Tags HeartburnWomen's HealthGynecologist
Heartburn during pregnancy - symptoms, causes and treatment of the disease
Contents
- Causes of heartburn during pregnancy
- What to do for heartburn during pregnancy?
- Preparations for heartburn during pregnancy
Heartburn is an unpleasant feeling of burning or warmth behind the breastbone or in the epigastric region. The symptom occurs after eating or on an empty stomach and is associated with food reflux, that is, the reflux of food processed by gastric juice back into the esophagus. Since the mucous membrane of the esophagus is not adapted to the action of gastric juice, it becomes irritated, which is subjectively felt in the form of heartburn.
The symptom occurs after eating or on an empty stomach and is associated with food reflux, that is, the reflux of food processed by gastric juice back into the esophagus. Since the mucous membrane of the esophagus is not adapted to the action of gastric juice, it becomes irritated, which is subjectively felt in the form of heartburn.
Heartburn in pregnant women is an independent symptom that appears only during the period of bearing a child against the background of the absence of chronic diseases that cause reflux of gastric juice 1 . According to statistics, 30-50% of pregnant women suffer from heartburn, there is evidence that more than 80% of pregnant women complain of heartburn, especially in the third trimester 4 .
Causes of heartburn during pregnancy
Heartburn in pregnancy is a condition that is caused by the changes that occur to the female body during the period of gestation. All factors that can cause heartburn in women in an interesting position can be divided into physiological (natural) and pathological (disease-related).
Physiological heartburn of pregnant women can occur for two reasons:
- Hormonal - associated with a weakening of the tone of the lower esophageal sphincter. This is the name of the circular muscle between the stomach and the esophagus, which regulates the flow of food into the stomach and prevents its movement in the opposite direction. During pregnancy, the level of progesterone in the blood rises, which relaxes the uterine muscle, simultaneously acting on all other muscles of the body, including the esophageal sphincter. As a result, the sphincter does not close after eating, but remains open. Any change in body position or contraction of the stomach causes food reflux 4 . Heartburn also occurs if it is disturbed by the movement of food through the esophagus, for example, if the frequency of "reverse" contractions of the esophagus increases in the direction from the stomach to the esophagus 1 .
- Physical - due to the increase in the size of the uterus, the location of the internal organs changes and intra-abdominal pressure increases, which is transmitted to the wall of the stomach and contributes to reflux 4 .

In connection with such changes in the gastrointestinal tract during pregnancy, all pathologies that cause heartburn can worsen.
Pathological causes of heartburn during pregnancy include the following:
- Gastroesophageal reflux disease (reflux esophagitis) is a pathology of the esophageal sphincter, which occurs more often with diaphragmatic hernia, when the natural curve between the esophagus and stomach disappears, preventing reverse reflux 4 .
- Other diseases of the gastrointestinal tract - gastritis, peptic ulcer of the stomach and duodenum, pancreatitis, diseases of the liver and biliary tract, inflammatory bowel disease 2 . With gastritis and ulcers, the acidity of the stomach increases, and pathologies of other digestive organs cause bloating, constipation, enlargement of the liver, which increases intra-abdominal pressure.
- Taking drugs that relax the lower esophageal sphincter - heart drugs, theophylline, anti-inflammatory drugs, progesterone, antidepressants 4 .
What to do about heartburn during pregnancy?
In the first two hours after eating, hydrochloric acid is produced in the stomach, which is needed for food processing. It is at this time that heartburn is more likely to torment, especially if a woman consumes fatty, fried and spicy foods 7 . Burning behind the sternum can last for several minutes or several hours. Heartburn may recur several times during the day. It is characterized by its strengthening in a horizontal position, with torso tilts, as well as when turning to the other side.
To reduce the severity of heartburn, you first need to adjust the diet and some habits. This helps to reduce the increased acidity of the stomach and prevent the reflux of food back into the esophagus.
Pregnant women should follow the following dietary recommendations 4 :
- Do not eat excessively high-calorie foods.
- Eliminate night snacks and especially overeating.
- Eat often and in small portions.
- Do not lie down immediately after eating, do not sleep in a strictly horizontal position, it is necessary to raise the head end of the bed.
- Walk for 30 minutes after eating.
- Eat dinner no later than 3-4 hours before going to bed.
- Do not lift weights, do not make strong and frequent torso bends, do not overstrain the abdominal muscles.
- Do not wear corsets, bandages, tight belts that increase intra-abdominal pressure.
From the diet for heartburn should be excluded 4 :
- Carbonated drinks (they increase pressure in the stomach and stimulate the formation of hydrochloric acid).
- Cream, whole milk, fatty meats, fatty fish, goose, pork (fatty foods take a long time to digest).
- Chocolate, cakes, pastries, spices (relaxes the lower esophageal sphincter).
- Citrus fruits, tomatoes, onions, garlic (irritate the mucous membrane of the esophagus).

For heartburn, pregnant women can eat the following foods 6 :
- wheat bread, dry biscuits, dry biscuits;
- baked pies with apples, boiled meat or fish;
- soups of meat, fish, vegetables;
- lean beef, poultry, fish;
- soft-boiled eggs and scrambled eggs;
- sugar, copper, butter cream;
- tea, cocoa, sweet fruit juices, jams, compotes.
Heartburn during pregnancy
In 80% of pregnant women, heartburn disappears after childbirth, but severe heartburn during pregnancy, especially if it lasts for several weeks, may persist after the birth of a child 4 .
Often, proper nutrition and adherence to lifestyle recommendations do not always help get rid of heartburn. If heartburn is caused by any disease, adequate treatment of the underlying pathology with medications helps to eliminate unpleasant symptoms.
The use of folk and non-traditional ways to eliminate heartburn during pregnancy is also not effective enough and even potentially dangerous. Many of the medicinal herbs during pregnancy can harm both the woman and her unborn child 4 .
Many of the medicinal herbs during pregnancy can harm both the woman and her unborn child 4 .
Therefore, it is advisable to discuss the choice of a drug with a doctor who will help you choose the right remedy for heartburn during pregnancy, paying attention from the standpoint of safety for the fetus and potential impact on the course of pregnancy 4
The results of epidemiological studies of Omez ® 10 mg in the treatment of heartburn in pregnant women show no clinically significant adverse effects on pregnancy and the health of the fetus or newborn 5 .
Omez ® 10 mg is dispensed without a doctor's prescription, but you can take it yourself without specialist advice for no longer than 14 days 5 .
THERE ARE CONTRAINDICATIONS, READ THE INSTRUCTIONS FOR MEDICAL USE OR CONSULT A DOCTOR.
References:
- Vyuchnova E.S., Yurenev G.