End of miscarriage
Miscarriage | March of Dimes
Miscarriage is the loss of a pregnancy in the womb before 20 weeks of pregnancy. Some women have a miscarriage before they know they’re pregnant.
We don’t know all the causes of miscarriage, but chromosome problems are often to blame.
It can take a few weeks to a month or more for your body to recover from a miscarriage. It may take longer to recover emotionally.
Talk to your health care provider about having medical tests before you try to get pregnant again.
Most women who miscarry go on to have a healthy pregnancy later.
What is miscarriage?
Miscarriage (also called early pregnancy loss) is when there is pregnancy loss before 20 weeks. For women who know they’re pregnant, about 10 to 20 in 100 pregnancies (10 to 20 percent) end in miscarriage. Most miscarriages - 8 out of 10 (80 percent) - happen in the first trimester before the 12th week of pregnancy. Miscarriage in the second trimester (between 13 and 19 weeks) happens in 1 to 5 in 100 (1 to 5 percent) pregnancies. Pregnancy loss that happens after 20 weeks is called stillbirth.
Miscarriage is very common. Some research suggests that more than 30 percent of pregnancies end in miscarriage, and many end before a person even knows they’re pregnant. Most people who miscarry go on to have a healthy pregnancy later.
What is a threatened miscarriage?
This is when a pregnant person has bleeding, little or no pain, a closed (undilated) cervix and the baby may have a heartbeat. The cervix is the opening to the uterus that sits at the top of the vagina. Most of the time, threatened miscarriages turn out fine.
What is an incomplete miscarriage?
This is when a miscarriage has happened, but the body doesn’t push out all of the tissue from pregnancy. You may have bleeding, cramping and other signs and symptoms of miscarriage.
What is a complete miscarriage?
This is when your body pushes out all of the tissue from the pregnancy. You may pass tissue suddenly or after having medical treatment.
You may pass tissue suddenly or after having medical treatment.
What is an asymptomatic miscarriage?
This is when you have a miscarriage but don’t have bleeding or cramping and you don’t pass any tissue out of your body. It is sometimes called an empty sac pregnancy. You may need a procedure to empty the uterus or the cervix may dilate on its own and the tissue will be passed like a period.
What are repeat miscarriages?
Repeat miscarriages, or recurrent pregnancy loss, is the loss of two pregnancies in a row. About 1 in 100 pregnant people (1 percent) have repeat miscarriages. The risk of having a second miscarriage is 20 in 100 (20 percent). After two miscarriages in a row, the risk of another miscarriage increases to about 28 in 100 (28 percent). And after three or more miscarriages in a row, the risk of having another miscarriage is about 43 in 100 (43 percent).
What causes miscarriage and repeat miscarriages?
We don’t know what causes every miscarriage. But some miscarriages and repeat miscarriages can be caused by:
But some miscarriages and repeat miscarriages can be caused by:
Problems with chromosomes
Up to 7 in 10 (70 percent) of all miscarriages are caused when an embryo (fertilized egg) gets the wrong number of chromosomes. This usually happens by chance and is not caused by a problem that’s passed from parent to child through genes. Chromosomes are the structures in cells that holds genes. Each person has 23 pairs of chromosomes, or 46 in all. For each pair, you get one chromosome from your mother and one from your father. Miscarriages that happen in the first 3 months of pregnancy are often caused by chromosomal problems. Examples include::
- Blighted ovum. This is when an embryo implants in the body but doesn’t develop into a baby. If you have a blighted ovum, you may have dark-brown bleeding early in pregnancy.
- Intrauterine fetal demise. This is when an embryo stops developing and dies.
- Molar pregnancy.
 This is when tissue in the uterus forms into a grape-like structure or tumor at the beginning of pregnancy.
This is when tissue in the uterus forms into a grape-like structure or tumor at the beginning of pregnancy. - Translocation. This is when part of a chromosome moves to another chromosome. Translocation causes a small number of repeat miscarriages.
- Other chromosome issues, such as anencephaly (a type of neural tube defect), trisomies (a problem that can cause conditions such as Down syndrome), renal agenesis (a type of kidney defect) or hydrops (a type of thalassemia)
Problems with the uterus or cervix.
Problems with the uterus and cervix that can cause miscarriage after 12 weeks but before 20 weeks include:
- Septate uterus. This is when a band of muscle or tissue (called a septum) divides the uterus in two sections. If you have a septate uterus, your provider may recommend surgery before you try to get pregnant to repair the uterus to help reduce your risk of miscarriage.
 Septate uterus is the most common kind of congenital uterine abnormality. Septate uterus is a common cause of repeat miscarriages.
Septate uterus is the most common kind of congenital uterine abnormality. Septate uterus is a common cause of repeat miscarriages. - Asherman syndrome. If you have this condition, you have scars or scar tissue in the uterus that can damage the endometrium (the lining of the uterus). Before you get pregnant, your provider may use a procedure called hysteroscopy to find and remove scar tissue. Asherman syndrome may often cause repeat miscarriages that happen before you know you’re pregnant.
- Fibroids and polyps or scars from surgery on the uterus. Fibroids, polyps and scars can limit space for your baby or interfere with your baby’s blood supply. Before you try to get pregnant, you may need a surgery called myomectomy to remove them.
- Cervical insufficiency (also called incompetent cervix). This is when your cervix opens (dilates) too early during pregnancy, usually without pain or contractions.
 To help prevent this, your provider may recommend cerclage. This is a stitch your provider puts in your cervix to help keep it closed.
To help prevent this, your provider may recommend cerclage. This is a stitch your provider puts in your cervix to help keep it closed.
Infections
Infections can cause miscarriage. Common infections include:
- Parvovirus B19. Parvovirus causes fifth disease, a common childhood illness.
- Cytomegalovirus
- Sexually transmitted infections (STIs). STIs, such as genital herpes and syphilis, are infections you can get from having sex with someone who is infected. If you think you may have an STI, tell your health care provider right away. Early testing and treatment can help protect you and your baby.
- Listeriosis. Listeriosis is a kind of food poisoning. If you think you have listeriosis, call your provider right away. Your provider may treat you with antibiotics to help keep you and your baby safe.
Other possible causes of miscarriage include:
- Abnormal blood clots
- Placental abruption
- Premature rupture of the membranes (PROM).
 PROM is when the amniotic sac around your baby breaks (your water breaks) before labor starts.
PROM is when the amniotic sac around your baby breaks (your water breaks) before labor starts. - Preterm labor
Are you at risk for a miscarriage?
Some things may make you more likely than other pregnant people to have a miscarriage. These are called risk factors. Risk factors for miscarriage include:
- Having two or more previous miscarriages
- Being 35 or older. As you get older, your risk of having a miscarriage increases. The age of your partner also may increase the risk of miscarriage.
- Smoking, drinking alcohol or using street drugs. Street drugs include cocaine and methamphetamines. If you’re pregnant or thinking about getting pregnant and need help to quit, tell your provider.
- Being exposed to harmful chemicals. You or your partner having contact with harmful chemicals, like solvents, may increase your risk of miscarriage.
 A solvent is a chemical that dissolves other substances, like some detergent mixtures and paint thinner. Exposure to lead, arsenic, radiation or air pollution can also be harmful. Talk with your provider about what you can do to protect yourself and your baby.
A solvent is a chemical that dissolves other substances, like some detergent mixtures and paint thinner. Exposure to lead, arsenic, radiation or air pollution can also be harmful. Talk with your provider about what you can do to protect yourself and your baby.
Some health conditions may increase your risk for miscarriage. Treatment of these conditions before and during pregnancy can sometimes help prevent miscarriage and repeat miscarriages. If you have any of these health conditions, tell your health care provider before you get pregnant or as soon as you know you’re pregnant:
- Autoimmune disorders. These health conditions happen when the body attacks its own healthy tissue by mistake. Autoimmune disorders that may increase your risk of miscarriage include antiphospholipid syndrome and lupus (also called systemic lupus erythematosus or SLE). If you have antiphospholipid syndrome, your body makes antibodies that attack certain fats that line the blood vessels; this can sometimes cause blood clots.
 If you have antiphospholipid syndrome and have had repeat miscarriages, your provider may give you low-dose aspirin and a medicine called heparin during pregnancy and for a few weeks after you give birth to help prevent another miscarriage.
If you have antiphospholipid syndrome and have had repeat miscarriages, your provider may give you low-dose aspirin and a medicine called heparin during pregnancy and for a few weeks after you give birth to help prevent another miscarriage. - Obesity. This means your body mass index (also called BMI) is 30 or higher. BMI is a measure of body fat based on your height and weight. To find out your BMI, go to cdc.gov/bmi.
- Hormone problems, such as polycystic ovary syndrome (also called PCOS) and luteal phase defect. Hormones are chemicals made by the body. Progesterone is a hormone that helps regulate your periods and gets your body ready for pregnancy. Luteal phase defect is when you have low levels of progesterone over several menstrual cycles. If you have luteal phase defect, your provider may recommend treatment with progesterone before and during pregnancy to help prevent repeat miscarriages.
- Preexisting diabetes
- Preexisting hypertension
- Thyroid problems
- Severe kidney disease
- Congenital heart disease
- Severe malnutrition.
 This means not getting enough food or nutrients before getting pregnant.
This means not getting enough food or nutrients before getting pregnant. - Group B beta strep infection
- Certain prenatal tests, such as amniocentesis and chorionic villus sampling. These tests have a slight risk of causing a miscarriage. Your provider may recommend them if your baby is at risk for certain genetic conditions, such as Down syndrome.
Having an injury to your belly, like from falling down or getting hit, isn’t a high risk for miscarriage. Your body does a good job of protecting your baby in the early weeks of pregnancy.
Having an injury to your belly, such as from falling or getting hit or a motor vehicle accident, may be a risk for miscarriage depending on the force of the injury or fall. Your body usually does a good job of protecting your baby in the early weeks of pregnancy. If this happens contact your provider to make sure you and your baby are not injured.
Other factors that may increase your risk of miscarriage include:
- Certain medications. Some studies show that nonsteroidal anti-inflammatory medications (also called NSAIDS) including ibuprofen, naproxen and diclofenac may increase risk. NSAIDs are a type of medicine used to relieve pain and swelling. The acne medicine isotretinoin has also been linked to miscarriage and fetal abnormalities.
- Getting pregnant while using an intrauterine device (IUD). IUDs are devices placed in your body to prevent pregnancy. In rare cases, people can get pregnant while using an IUD.
- Stress. Both short, intense times of stress and long-term stress can increase the risk of miscarriage.
Socioeconomic status and other social determinants of health. Racial, ethnic or financial inequalities, being at risk for violence, being homeless or not having enough food can negatively affect your health. These factors increase your risk of developing other serious and chronic health conditions that can increase your chances of miscarriage.
You may have heard that getting too much caffeine during pregnancy can increase your risk for miscarriage. Caffeine is a drug found in foods, drinks, chocolate and some medicine. It’s a stimulant, which means it can help keep you awake. More research is needed to understand the effect of caffeine on pregnancy. Until we know more about how caffeine can affect pregnancy, it’s best to limit the amount you get to 200 milligrams each day. This is what’s in about one 12-ounce cup of coffee.
You also may have heard that having sex or exercising while pregnant can cause a miscarriage. There is no proof that this is true.
How can you prevent a miscarriage?
Miscarriages usually can’t be prevented, but being healthy before pregnancy can help prevent pregnancy complications. Good pre-pregnancy health includes getting a pre-pregnancy checkup and talking with your provider about health conditions that can affect your pregnancy. It also includes taking folic acid to help prevent birth defects and making changes in your life that may affect the health of your baby.
What are the signs and symptoms of miscarriage?
Signs and symptoms of miscarriage include:
- Bleeding from the vagina or spotting. Many people experience spotting early in their pregnancy. In most cases, it is not a sign of miscarriage. To be safe, if you have spotting or any of these signs or symptoms, call your provider.
- Cramps, like the ones you have with your period
- Severe belly pain
- No longer “feeling pregnant,” such as no longer feeling the baby move, feeling nauseated or no longer having breast tenderness
- Back pain
- Vaginal discharge with a bad smell
- Fever
Miscarriages can be dangerous if they’re not treated. Your provider may want to do some tests to make sure everything’s OK. These tests can include blood tests, a pelvic exam and an ultrasound.
Many pregnant people have these signs and symptoms in early pregnancy and don’t have a miscarriage.
What treatment do you get after a miscarriage or repeat miscarriages?
Treatment depends on how far along you were in your pregnancy, your overall health, your age and other factors. If you’ve had a miscarriage, your provider may recommend:
If you’ve had a miscarriage, your provider may recommend:
- Dilation and curettage (also called D&C). This is a procedure to remove any remaining tissue from the uterus. Your provider dilates (widens) your cervix and removes the tissue using an instrument called a curette.
- Dilation and extraction (also called D&E). This is a procedure to remove any remaining tissue from the uterus. Your provider dilates (widens) your cervix and removes the tissue using suction.
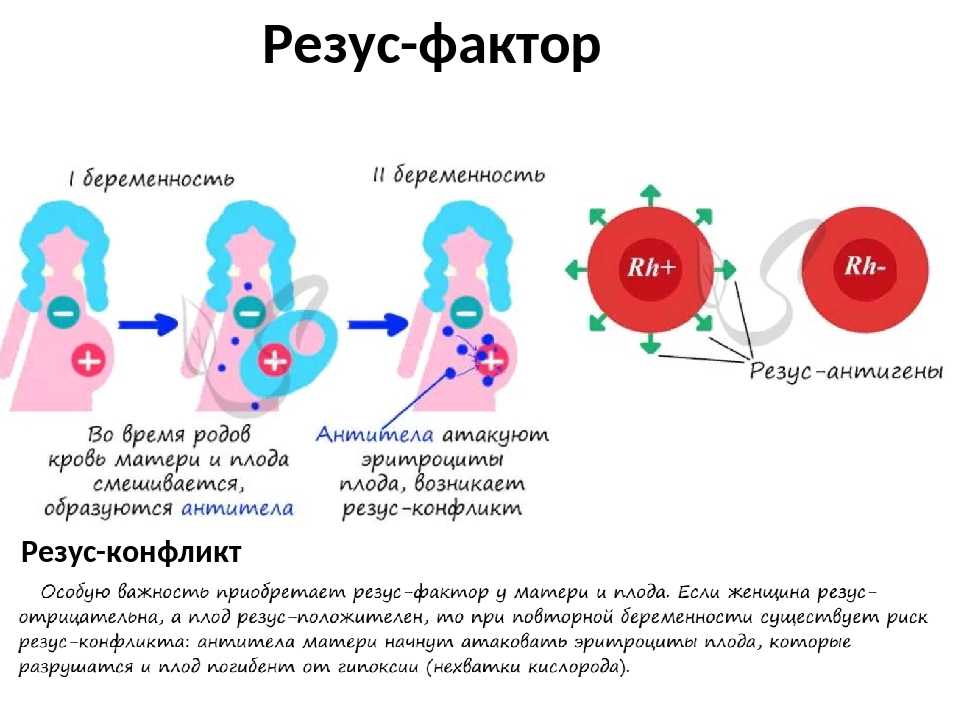
- Medicine. Your provider may recommend medicine that can help your body pass tissue that’s still in the uterus. If your blood type is Rh negative, you also may get a shot of Rh immunoglobulin after any miscarriage or bleeding episode in pregnancy. This can help prevent problems with future pregnancies. Rh immunoglobulin is a medicine that stops a person who is Rh negative from reacting to Rh-positive blood.
Do you need any medical tests after a miscarriage or repeat miscarriages?
If you miscarry in your first trimester, you probably don’t need any medical tests. Because we don’t often know what causes a miscarriage in the first trimester, tests may not be helpful in trying to find out a cause.
Because we don’t often know what causes a miscarriage in the first trimester, tests may not be helpful in trying to find out a cause.
If you have repeat miscarriages in the first trimester, or if you have a miscarriage in the second trimester, your provider usually recommends tests to help find out the cause. Tests can include:
- Chromosome tests. You and your partner can have blood tests, like karyotyping, to check for chromosome problems. Karyotyping can count how many chromosomes there are and check to see if any chromosomes have changed. If tissue from the miscarriage is available, your provider can test it for chromosomal conditions.
- Hormone tests. You may have your blood tested to check for hormone problems. You may also have a procedure called endometrial biopsy that removes a small piece of the lining of the uterus to check for timing in the cycle and hormones.
- Blood tests to check your immune system.
 Your provider may test you for autoimmune disorders like, APS and lupus.
Your provider may test you for autoimmune disorders like, APS and lupus. - Looking at the uterus. You may have an ultrasound, a hysteroscopy (when your provider inserts a special scope through the cervix to see your uterus) or a hysterosalpingography (an X-ray of the uterus) or other test.
How long does it take to recover from a miscarriage?
It can take a few weeks to a month or more for your body to recover from a miscarriage. Depending on how long you were pregnant, you may have pregnancy hormones in your blood for 1 to 2 months after you miscarry. Most women get their period again 4 to 6 weeks after a miscarriage. Talk to your provider about how to care for yourself during this time.
It may take longer to recover emotionally from a miscarriage. You may have strong feelings of grief about the death of your baby. Grief can make you feel sad, angry, confused or alone. It’s OK to take time to grieve after a miscarriage. Ask your friends and family for support, and find special ways to remember your baby. For example, if you already have baby things, like clothes and blankets, you may want to keep them in a special place. Do what’s right for you. Ask your provider about support groups or services that can help you to with recovery from grief.
For example, if you already have baby things, like clothes and blankets, you may want to keep them in a special place. Do what’s right for you. Ask your provider about support groups or services that can help you to with recovery from grief.
Certain things, such as hearing names you were thinking of for your baby or seeing other babies, can be painful reminders of your loss. You may need help learning how to deal with these situations and the feelings they create. A support group can help. Tell your provider if you need help to deal with your grief.
If you miscarry, when can you try to get pregnant again?
This is a decision for you to make with your partner and your provider. It’s probably OK to get pregnant again after you’ve had at least one normal period. Some studies show that trying to get pregnant again soon after a miscarriage can increase your chances of conceiving. Be sure to take a vitamin supplement that has 400mcg of folic acid even if you don’t get pregnant right away. If you’re having medical tests to try to find out more about why you miscarried, you may need to wait until after you’ve had these tests to try to get pregnant again.
If you’re having medical tests to try to find out more about why you miscarried, you may need to wait until after you’ve had these tests to try to get pregnant again.
You may not be emotionally ready to try again so soon. Miscarriage can be hard to handle, and you may need time to grieve. It’s OK if you want to wait a while before trying to get pregnant again.
More information
From Hurt to Healing (free booklet from the March of Dimes for grieving parents)
Centering Corporation (grief information and resources)
Compassionate Friends (resources for families after the death of a child)
Journey Program of Seattle Children’s Hospital (resources for families after the death of a child)
Lupus Research Alliance: Pregnancy and family planning
Share Pregnancy & Infant Loss Support (resources for families with pregnancy or infant loss)
Last reviewed: February 2023
What Happens After a Miscarriage? An Ob-Gyn Discusses the Options.
Miscarriage, the loss of a pregnancy that’s in the uterus, is common. It happens in about 1 in 10 women who know they’re pregnant. But many people don’t know what to expect afterward.
The vast majority of miscarriages happen in the first trimester, before 13 weeks of pregnancy. Most occur before 10 weeks. In this article, I’ll discuss the treatment options for first-trimester miscarriage, also called early pregnancy loss. Second-trimester miscarriage usually requires different treatments.
Here’s what to know about care and recovery.
There are three main treatments for early pregnancy loss. The goal for all three is to remove any pregnancy tissue left in the uterus. There are two nonsurgical treatments: expectant management (letting the tissue pass on its own) and medication. The third treatment is a surgical procedure called dilation and curettage (also known as D&C or suction curettage).
In many cases, patients can choose the option they prefer.
Expectant management is giving your body time to pass the tissue on its own. This doesn’t involve medication or surgery. Some women choose this because it’s the most natural option, but it is more unpredictable than other treatments.
Most women pass the tissue within 2 weeks of a miscarriage diagnosis, but it can take longer. If it takes too long, your ob-gyn may recommend medication to start the process. (Once the process starts and cramping and bleeding begin, most of the tissue passes within a few hours. More on that below.)
Sometimes, the body doesn’t pass all the tissue. When this happens, another treatment is recommended, usually a D&C. Expectant management is most likely to work when you already have some bleeding and cramping. This means your body has begun the process of passing the tissue.
Medication works faster and is more predictable. Some women choose medication that helps their body remove any leftover tissue. These drugs are absorbed through the cheek in the mouth or through the vagina. Cramping or bleeding usually starts within a few hours. Most women pass the tissue within 48 hours and don’t need any other treatment. (Some women may still not pass all the tissue and may need a surgical procedure.)
These drugs are absorbed through the cheek in the mouth or through the vagina. Cramping or bleeding usually starts within a few hours. Most women pass the tissue within 48 hours and don’t need any other treatment. (Some women may still not pass all the tissue and may need a surgical procedure.)
Medication gives you more control over the timing of the tissue passing. And it’s often quicker than waiting for the tissue to pass on its own.
Some women like to take the medication in the morning, so the process doesn’t start overnight. And some women like to have a support person, such as a friend or family member, with them when they take the medication.
You’ll have a similar experience whether the tissue passes on its own or you take medication. You’ll have bleeding and cramping that are heavier than your normal period. The pregnancy tissue may look like large blood clots, or it may look white or gray. It does not look like a baby. The process can be painful, and ob-gyns may prescribe medication to help with this discomfort. Your ob-gyn may also suggest over-the-counter pain medication. Talk with your ob-gyn about pain relief options.
Your ob-gyn may also suggest over-the-counter pain medication. Talk with your ob-gyn about pain relief options.
Most of the tissue passes within 2 to 4 hours after the cramping and bleeding start. Cramping usually stops within a day. Light bleeding or spotting can go on for 4 to 6 weeks. Two weeks after the tissue passes, your ob-gyn may do an ultrasound exam or other tests to make sure all the tissue has passed.
A D&C is the most predictable treatment. During a D&C, your ob-gyn passes a small tool through the cervix and into the uterus to remove the tissue. Some women choose this option because they want a faster, more certain treatment. And if you’re already bleeding heavily, it’s the safest option.
Some ob-gyns do D&Cs in an operating room using general anesthesia, which means you’ll be asleep. Some offer a form of pain relief called sedation, where you will be awake but comfortable. Others do the procedure in a normal exam room, with an injection of drugs that block pain in a specific area. Women often have some bleeding and intense cramping during a D&C. They usually have little discomfort afterward.
Women often have some bleeding and intense cramping during a D&C. They usually have little discomfort afterward.
Light spotting or bleeding can last up to a month. An antibiotic is prescribed to prevent infection. Other complications are rare, and most women don’t need any follow-up appointments.
Whichever option you choose, call your ob-gyn if you have very heavy bleeding, a fever, or feel unwell. Dangerous bleeding and infection are a risk of all treatments, but these problems are rare. Call your ob-gyn right away if you have any of these symptoms:
-
Your bleeding soaks through more than two large pads in an hour for 2 hours or more. This much bleeding is dangerous and needs immediate care.
-
You have a temperature higher than 100 °F.
-
You have chills, severe pain, or any other symptoms that concern you.
Physical recovery is usually quick. Most women resume their regular activities a day or two after they pass the tissue or have a D&C. For some, nausea and other pregnancy symptoms stop before their ob-gyn diagnoses a miscarriage. For others, these symptoms go away a few days after the tissue passes.
For some, nausea and other pregnancy symptoms stop before their ob-gyn diagnoses a miscarriage. For others, these symptoms go away a few days after the tissue passes.
To keep your infection risk low, don’t put anything into your vagina for a week—no douching (which is never a good idea at any time), vaginal sex, tampons, or menstrual cups. You can use pads to absorb the bleeding. Most women have their first period about 2 weeks after any spotting or light bleeding ends, which is usually about 2 to 3 months after you pass the tissue or have a D&C.
People have different emotional reactions. Some women feel sadness or grief. Others may feel relief. Some may feel a mixture of emotions. All these feelings are normal, and it’s important to allow yourself time to process them.
Talking about these feelings with friends, family, your ob-gyn, or a mental health professional can help. If you feel depressed or are thinking of hurting yourself, tell your ob-gyn or another doctor right away. Support groups and resources, such as Share Pregnancy & Infant Loss Support, may be helpful too.
Support groups and resources, such as Share Pregnancy & Infant Loss Support, may be helpful too.
Miscarriage isn’t your fault. Women often worry that they somehow caused their miscarriage. This is not the case. Physical activity, stress, and sex don’t cause miscarriages. Most happen because the pregnancy wasn’t developing normally. Often, the egg or sperm develops with more or fewer chromosomes than normal, which can lead to miscarriage. This is a random event that you cannot control.
Most women can have a healthy pregnancy after a miscarriage. Talk with your ob-gyn if you have concerns. Your ob-gyn can help ease your fears, answer any questions, and talk about preparing for your next pregnancy.
Published: June 2022
Last reviewed: June 2022
Copyright 2023 by the American College of Obstetricians and Gynecologists. All rights reserved. Read copyright and permissions information.
This information is designed as an educational aid for the public. It offers current information and opinions related to women's health. It is not intended as a statement of the standard of care. It does not explain all of the proper treatments or methods of care. It is not a substitute for the advice of a physician. Read ACOG’s complete disclaimer.
It offers current information and opinions related to women's health. It is not intended as a statement of the standard of care. It does not explain all of the proper treatments or methods of care. It is not a substitute for the advice of a physician. Read ACOG’s complete disclaimer.
Recurrent Miscarriages - Bahçeci IVF Clinic
View Full
struggling with infertility!
We are happy to share with you a video of our Bulgarian couple who recently had twins in Bahceci IVF Center in Istanbul!🌟 Don't you think...
Read more Watch the video
affordable prices for medicines
👉Treatment under the supervision of one doctor 👉Comfortable single rooms 👉 No queue 👉Quality service in your native language 👉 Discounted Hotels 👉Meet and greet at the airport …
Read more Watch the video
Good news today for a couple from America
We dreamed of a child for 4 years at the Bahçeci clinic Istanbul, we got a positive result from the first IV attempt!!!! 🌟 Our medical specialists performed an operation for …
Read more Watch the video
woman 46 years old
👉🏻 woman 46 years old 👉🏻0. 4 AMG value 👉🏻 Failed attempts at external centers ♥️ And a happy ending on the first try in Bahçeci! 👉Affordable prices for …
4 AMG value 👉🏻 Failed attempts at external centers ♥️ And a happy ending on the first try in Bahçeci! 👉Affordable prices for …
Read more Watch the video
Our miracles are not far away
This time the good news is going to East Africa. We started by creating a personalized treatment plan for our couple who came from afar to get their …
Read more Watch the video
Good news for Bulgaria!
Continue to get successful results with medication! Choose Bahçeci Istanbul for successful treatment of male infertility and azoospermia! We are waiting for you🙌v …
Read more Watch the video
Thank God and Bahçeci!
For 9 years we could not have children. Dozens of doctors, hundreds of tests, and no result. Realizing that we will not receive quality treatment at home, …
Read more
Malika and Bekdzhan
On behalf of our large family, let me express our deep gratitude to you for the help and support you provide to our children Malika and Bekdzhan. Our children …
Our children …
Image copyright, Getty Images
A court in El Salvador acquitted 21-year-old Evelyn Hernandez in a retrial, facing 40 years in prison for murder for miscarriage. This is a big victory for women's rights in El Salvador, human rights activists say.
"Thank God, justice has been done. In the future, I'm going to continue my studies and strive to achieve my goals. I'm happy," she said outside the courthouse after the trial was over.
Evelyn Hernandez maintained her innocence in court. According to her, when she was 18 years old, she was raped by a member of one of the local criminal gangs, but she did not know that she had become pregnant, and at the moment when she had a miscarriage, she lost consciousness. Prosecutors asked the court to sentence her to 40 years in prison. Women's rights activists both in El Salvador and abroad demanded that the girl be acquitted.
El Salvador has one of the most stringent anti-abortion laws in the world.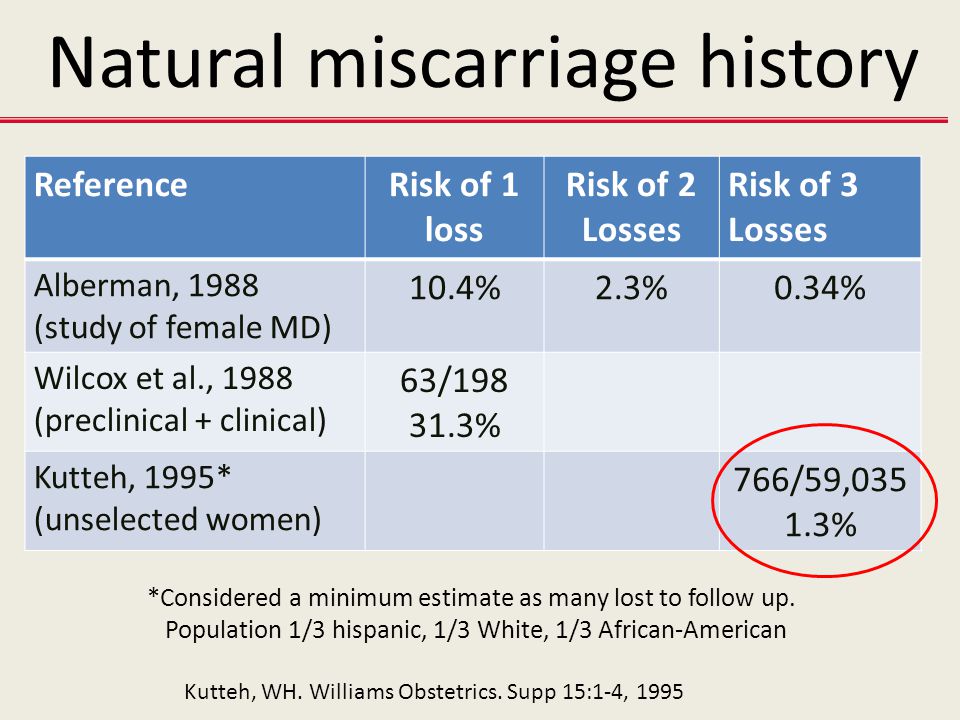 Abortion is illegal in the country under any circumstances. Those convicted of abortion in El Salvador face a prison sentence of two to eight years.
Abortion is illegal in the country under any circumstances. Those convicted of abortion in El Salvador face a prison sentence of two to eight years.
In some cases, as in the Hernandez case, the charge is reclassified to a more severe article of aggravated murder, the minimum sentence for which is 30 years in prison.
The Hernandez case was the first of its kind in El Salvador to receive a full trial.
Previously, women charged with abortions had their sentences commuted after their long sentences were deemed "disproportionate and immoral", but their sentences were never overturned.
Human rights activists now hope the Hernandez case will set a precedent that will allow other women imprisoned because of El Salvador's strict anti-abortion laws to fight for their convictions to be overturned.
"We can and will continue to fight because there are still accused women who urgently need justice," said lawyer Hernandez Berta Maria Deleon.
- "The Handmaid's Tale" - a dystopia or a reality of the future? Demography through the eyes of scientists
- Signed to church: how abortions are banned in the Belgorod region
Amnesty International called the verdict a "big win" for women's rights in El Salvador and called on the country's authorities to "put an end to the shameful and discriminatory" practice of criminalizing abortion. The Office of the United Nations High Commissioner for Human Rights has also previously called on El Salvador to reform its abortion laws.
How did it all start?
Skip the Podcast and continue reading.
Podcast
What was that?
We quickly, simply and clearly explain what happened, why it's important and what's next.
episodes
The End of the Story Podcast
On April 6, 2016, Evelina Hernandez, who was at her home in rural El Salvador at the time, experienced severe abdominal pain and began to bleed. She went to the toilet, located in the annex, and lost consciousness there.
She went to the toilet, located in the annex, and lost consciousness there.
Mother took Hernandez to the hospital, where doctors concluded that the girl had given birth. The body of the child was found in the toilet, after which Hernandez was arrested.
Hernandez has repeatedly declared her innocence. According to her, when she was 18 years old, she was raped by a member of one of the local criminal gangs, but she did not know that she was pregnant.
Hernandez reported that she confused pregnancy symptoms with abdominal pain and that she had intermittent bleeding that she thought was her period.
"If I had known that I was pregnant, I would have waited for the birth of a child with pride and joy," she said.
First, Hernandez was charged with abortion, then later the charge was reclassified as aggravated murder. Prosecutors claimed that the girl deliberately hid her pregnancy.
Image copyright Getty Images
In July 2017, a court ruled that Hernandez knew she was pregnant and found her guilty. The girl was sentenced to 30 years in prison, of which she served almost three years (33 months).
The girl was sentenced to 30 years in prison, of which she served almost three years (33 months).
The girl's defense appealed the court's decision. Lawyers insisted that the examination showed that the child died of natural causes, and not as a result of an abortion.
In February 2019, the Supreme Court of El Salvador overturned Hernandez's conviction due to lack of evidence against her and ordered a retrial with a new judge. The girl was released from prison pending a retrial, which began in July.
During the retrial, the prosecutors asked the court to give the girl an even harsher sentence than the first time - 40 years in prison.
Abortions in El Salvador
According to human rights activists, at least 17 more women convicted of abortions are currently in prisons in El Salvador. The Hernandez retrial was the first of its kind under El Salvador's new president, Nayib Bukele, who took office in June.