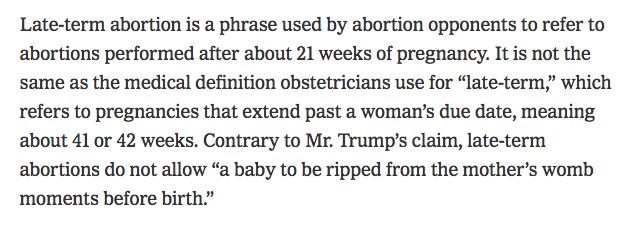
Define late term abortion
Abortions Later in Pregnancy | KFF
|
Introduction
Abortions occurring at or after 21 weeks gestational age are rare. They are often difficult to obtain, as they are typically costly, time-intensive and only performed by a small subset of abortion providers. Yet these abortions receive a disproportionate amount of attention in the news, policy and the law, and discussions on this topic are often fraught with misinformation; for example, intense public discussions have been sparked after several policymakers have theorized about abortions occurring “moments before birth” or even “after birth.” In reality, these scenarios do not occur, nor are they legal, in the U.S. Discussion of this topic is further obscured due to the terms sometimes used to describe abortions later in pregnancy– including “late-term,” “post-viability,” “partial birth,” “dismemberment” and “born-alive” abortions—despite many medical professionals criticizing and opposing their use. This fact sheet explains why individuals may seek abortions later in pregnancy, how often these procedures occur, how the concepts of viability and fetal pain play into this topic, and the various laws which regulate access to abortions later in pregnancy.
Clarifying Pregnancy Dating: pregnancies are measured using gestational age (GA), calculated in days and weeks since the first day of the last menstrual period (LMP). Since some people do not know the date of their LMP, ultrasound can also be used to calculate GA. Post-fertilization or fertilization age refers to the time since the egg and sperm fused to create a fertilized egg. Fertilization occurs approximately 2 weeks after menses, thus gestational age by LMP predates fertilization age by ~2 weeks. By convention, gestational age is used to discuss pregnancy dating as most pregnant individuals know their LMP, however certain abortion regulations reference fertilization age instead.
What is a so-called “late-term” abortion?
“Late term” abortion typically refers to abortions obtained at or after 21 weeks, however it is not an accepted medical term, nor is there a consensus around to which gestational ages it refers. Members of the medical community have criticized the term “late-term” abortion, as it implies abortions are taking place after a pregnancy has reached “term” (37 weeks) or “late term” (>41 weeks) which is false. In fact, the American College of Obstetricians and Gynecologists (ACOG) has written that “late-term abortion” has no medical meaning and should not be used in clinical or legal settings. As such, we will refer to abortions occurring at ≥21 weeks gestation as abortions later in pregnancy, but it should be noted that 21 weeks is a largely arbitrary cutoff based on how the CDC collects data on abortions. Abortions at this stage in pregnancy are sometimes referred to as “later abortions” by the medical community as well.
In fact, the American College of Obstetricians and Gynecologists (ACOG) has written that “late-term abortion” has no medical meaning and should not be used in clinical or legal settings. As such, we will refer to abortions occurring at ≥21 weeks gestation as abortions later in pregnancy, but it should be noted that 21 weeks is a largely arbitrary cutoff based on how the CDC collects data on abortions. Abortions at this stage in pregnancy are sometimes referred to as “later abortions” by the medical community as well.
What is viability? Why does it matter for abortions later in pregnancy?
Abortions later in pregnancy have been highly debated, in part because some people believe that this stage of pregnancy abuts the time around viability. In 1973, Roe v. Wade legalized abortion in the U.S., and in the process made “viability” the delineating factor in the abortion debate; before viability, a person has the right to obtain an abortion, whereas after viability, the state can restrict access to abortion in the interest of protecting the potential for human life, except in cases of health or life endangerment of the pregnant person.
The Supreme court made clear in Roe v. Wade that the courts are not in a position to assess when life begins and when viability has been reached, writing, “We need not resolve the difficult question of when life begins. When those trained in the respective disciplines of medicine, philosophy, and theology are unable to arrive at any consensus, the judiciary, at this point in the development of man’s knowledge, is not in a position to speculate as to the answer.” (Roe v. Wade) Given viability is case dependent and is only a possibility or probability of survival, rather than a guarantee of survival, the decision in Roe v. Wade left the right to an abortion after viability up to individual states to determine.
In a subsequent Supreme Court case on abortion, the court defined viability as follows:
“Viability is reached when, in the judgment of the attending physician on the particular facts of the case before him, there is a reasonable likelihood of the fetus’ sustained survival outside the womb, with or without artificial support.
Because this point may differ with each pregnancy, neither the legislature nor the courts may proclaim one of the elements entering into the ascertainment of viability – be it weeks of gestation or fetal weight or any other single factor – as the determinant of when the State has a compelling interest in the life or health of the fetus.” Colautti v. Franklin (1979)
Viability depends on many factors, including gestational age, fetal weight and sex, and medical interventions available. While viability does not refer to a specific gestational age, it is often presumed at 24 weeks gestation, with “periviability” referring to the time around viability (20 to 26 weeks gestation). For periviable births, the hospital at which the infant is delivered can greatly affect viability, and the patient’s insurance coverage may dictate where they can seek care. Infants born in resource-rich settings have a higher likelihood of survival than those born in resource-poor settings. This is in part due to access to neonatologists and maternal-fetal-medicine doctors, but also due to hospital-specific policies; in a study of 24 academic hospitals, active treatment for infants born at 22 weeks ranged from 0% to 100% depending on the hospital, showing that the criteria used to determine viability at one hospital may not be the same at another. If time allows and if the pregnant individual is clinically stable, they may be transferred to a facility better equipped for neonatal resuscitation before delivery, however this is not always possible. Further, insurance coverage and reimbursement for transfers in care varies by state and insurance plan.
This is in part due to access to neonatologists and maternal-fetal-medicine doctors, but also due to hospital-specific policies; in a study of 24 academic hospitals, active treatment for infants born at 22 weeks ranged from 0% to 100% depending on the hospital, showing that the criteria used to determine viability at one hospital may not be the same at another. If time allows and if the pregnant individual is clinically stable, they may be transferred to a facility better equipped for neonatal resuscitation before delivery, however this is not always possible. Further, insurance coverage and reimbursement for transfers in care varies by state and insurance plan.
At the time of Roe v. Wade, the Supreme Court wrote that viability “is usually placed at about seven months (28 weeks), but may occur earlier, even at 24 weeks.” With medical advances, extremely preterm infants can now survive at lower gestational ages than previously thought possible, particularly at hospitals with Level IV neonatal intensive care units (NICUs). The question we come up against is this: with viability possible at lower gestational ages, will abortions be prohibited at lower gestational ages as well? Many favor leaving that decision up to the patient and their provider, given viability depends on the individual pregnancy. Others, including some policymakers, desire early gestational age limits on abortion, well before the possibility of viability. In subsequent sections, we outline policies that regulate the provision of abortions later in pregnancy, including gestational age restrictions.
The question we come up against is this: with viability possible at lower gestational ages, will abortions be prohibited at lower gestational ages as well? Many favor leaving that decision up to the patient and their provider, given viability depends on the individual pregnancy. Others, including some policymakers, desire early gestational age limits on abortion, well before the possibility of viability. In subsequent sections, we outline policies that regulate the provision of abortions later in pregnancy, including gestational age restrictions.
How common are abortions later in pregnancy?
Abortions occurring at or after 21 weeks gestation are rare. According to the CDC’s Abortion Surveillance Data, the vast majority of abortions (91%) occur at or before 13 weeks gestation, while 7.7% occur from weeks 14 to 20 gestation, and just 1.2% of abortions are performed at or after 21 weeks (Figure 1). This amounts to approximately 5,200 abortions per year occurring at or after 21 weeks, however this is an underestimate as only 33 reporting areas report abortions to the CDC by gestational age. The percentage of abortions occurring at or before 13 weeks gestation has remained stable over the last few decades at 91-92%, however within this timeframe, more abortions are occurring earlier in pregnancy, at or before 8 weeks. This is likely in part due to the greater availability of medication abortions over the last two decades.
The percentage of abortions occurring at or before 13 weeks gestation has remained stable over the last few decades at 91-92%, however within this timeframe, more abortions are occurring earlier in pregnancy, at or before 8 weeks. This is likely in part due to the greater availability of medication abortions over the last two decades.
Figure 1: The Vast Majority of Abortions Occur Early in Pregnancy
The CDC does not elaborate on the breakdown by gestational age for abortions occurring past 21 weeks, but it is likely that the vast majority occur soon after 21 weeks rather than in the later in the pregnancy. While very limited data exists on this issue, a study from 1992 estimated 0.02% of all abortions occurred after 26 weeks gestation (320 to 600 cases per year). This may overestimate current day numbers, given the abortion rate is currently at a historic low, and restrictions on abortions later in pregnancy have increased.
Why do people have abortions later in pregnancy?
Non-Medical Reasons: Individuals seek abortions later in pregnancy for a number of reasons.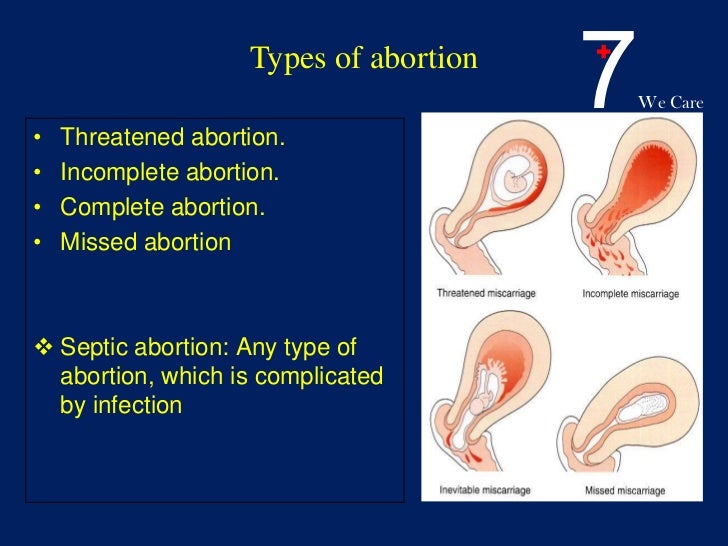 As part of the Turnaway study out of the University of California San Francisco, from 2008-2010 over 440 women were asked about why they experienced delays in obtaining abortion care, if any (Figure 2). Almost half of individuals who obtained an abortion after 20 weeks did not suspect they were pregnant until later in pregnancy, and other barriers to care included lack of information about where to access an abortion, transportation difficulties, lack of insurance coverage and inability to pay for the procedure. This is unsurprising, given abortions can be cost-prohibitive for many; in a study from 2011-2012, the median cost of a surgical abortion at 10 weeks was $495, jumping to $1,350 at 20 weeks (range $750-$5,000) excluding the cost of travel and lost wages. Yet the Federal Reserve Board found 40% of U.S. adults do not have enough in savings to pay for a $400 emergency expense, meaning many individuals may need to delay having an abortion until they can raise the necessary funds.
As part of the Turnaway study out of the University of California San Francisco, from 2008-2010 over 440 women were asked about why they experienced delays in obtaining abortion care, if any (Figure 2). Almost half of individuals who obtained an abortion after 20 weeks did not suspect they were pregnant until later in pregnancy, and other barriers to care included lack of information about where to access an abortion, transportation difficulties, lack of insurance coverage and inability to pay for the procedure. This is unsurprising, given abortions can be cost-prohibitive for many; in a study from 2011-2012, the median cost of a surgical abortion at 10 weeks was $495, jumping to $1,350 at 20 weeks (range $750-$5,000) excluding the cost of travel and lost wages. Yet the Federal Reserve Board found 40% of U.S. adults do not have enough in savings to pay for a $400 emergency expense, meaning many individuals may need to delay having an abortion until they can raise the necessary funds.
Figure 2: Many Factors Contribute to Delays in Obtaining Abortion Care
Additionally, of all the abortion-providing facilities in the U.S., only 34% offer abortions at 20 weeks and just 16% at 24 weeks, meaning individuals may need to travel a significant distance to find an available, trained provider. Abortions at this stage also typically require two days to complete with inpatient care, as opposed to outpatient or at-home management that is possible earlier in pregnancy.1 In the years since these data were collected, dozens of abortion restrictions have been enacted across the county, including mandated waiting periods; it is therefore possible that individuals seeking abortion today may face even more delays in care than these data reflect.
Fetal Anomalies: Individuals also seek abortions later in pregnancy due to medical reasons. With medical advances, many genetic fetal anomalies can be detected early in pregnancy; for example, chorionic villus sampling can diagnose Down Syndrome or cystic fibrosis as earlier as 10 weeks gestation. Structural fetal anomalies, however, are often detected much later in pregnancy. As part of routine care, a fetal anatomy scan is performed around 20 weeks, which entails ultrasound imaging of all the developing organs. Many structural anomalies are discovered at this time that would not have been apparent previously. A proportion of these are lethal fetal anomalies, meaning that the fetus will almost certainly die before or shortly after birth, meaning the fetus may be nonviable.2 In these cases, many individuals wish to terminate their pregnancies, rather than carrying the pregnancy until the fetus or newborn passes away. Very often these pregnancies are desired, making this decision exceedingly difficult for parents. Inadequate data exist to know how many abortions later in pregnancy occur due to fetal anomalies, but a study by Washington University Hospital showed almost all women whose fetuses had lethal fetal anomalies chose to terminate their pregnancies.
Structural fetal anomalies, however, are often detected much later in pregnancy. As part of routine care, a fetal anatomy scan is performed around 20 weeks, which entails ultrasound imaging of all the developing organs. Many structural anomalies are discovered at this time that would not have been apparent previously. A proportion of these are lethal fetal anomalies, meaning that the fetus will almost certainly die before or shortly after birth, meaning the fetus may be nonviable.2 In these cases, many individuals wish to terminate their pregnancies, rather than carrying the pregnancy until the fetus or newborn passes away. Very often these pregnancies are desired, making this decision exceedingly difficult for parents. Inadequate data exist to know how many abortions later in pregnancy occur due to fetal anomalies, but a study by Washington University Hospital showed almost all women whose fetuses had lethal fetal anomalies chose to terminate their pregnancies.
A study of maternal fetal medicine (MFM) doctors—specialists who manage pregnancies with fetal anomalies— found most agreed that termination of pregnancy due to a lethal fetal anomaly should be allowed in all circumstances (76%). The majority (75%) discuss abortion as a management option soon after diagnosing a lethal fetal anomaly, but services for terminating pregnancies in these scenarios are limited. Only 40% of MFMs worked at healthcare centers offering abortions past 24 weeks for lethal fetal anomalies. An additional 12% knew of available services <50 miles away.
The majority (75%) discuss abortion as a management option soon after diagnosing a lethal fetal anomaly, but services for terminating pregnancies in these scenarios are limited. Only 40% of MFMs worked at healthcare centers offering abortions past 24 weeks for lethal fetal anomalies. An additional 12% knew of available services <50 miles away.
Health Risk to the Pregnant Person: Life threatening conditions may also develop later in pregnancy. These include conditions like early severe preeclampsia, newly diagnosed cancer requiring prompt treatment, and intrauterine infection (chorioamnionitis) often in conjunction with premature rupture of the amniotic sac (PPROM). If these conditions arise before the fetus is viable, the pregnant individual may pursue termination of pregnancy to preserve their own health. If these conditions arise after the fetus is considered viable, Roe v. Wade still protects the right for these individuals to obtain an abortion in cases of health or life endangerment, however it may be difficult to find a provider for this service as previously mentioned. Typically every effort is made to save the life of both the pregnant individual and the fetus, pursuing delivery rather than abortion.
Typically every effort is made to save the life of both the pregnant individual and the fetus, pursuing delivery rather than abortion.
How do states regulate abortions later in pregnancy?
A few states have sought to expand access to abortions later in pregnancy. The New York Reproductive Health Act enacted in January 2019 expands protections for abortion providers and pregnant individuals who have abortions after 24 weeks in cases of health or life endangerment or lethal fetal anomalies. Virginia similarly proposed loosening restrictions on abortions later in pregnancy, by reducing the number of physicians who would need to approve an abortion after 28 weeks gestation from three to one, and by broadening maternal exceptions to include more general threats to mental and physical health. This bill failed to pass, but sparked national discussion about regulation of abortions later in pregnancy.
Many states have directed their efforts in the opposite direction, aiming to increase restrictions on abortions later in pregnancy. States most often do so by (1) placing gestational age limits on abortion, and/or (2) restricting the methods providers can use to perform abortions later in pregnancy. In discussion of these laws, it is important to note that most policymakers are not clinicians, therefore many of the terms used to discuss abortions later in pregnancy are designed to communicate a political message, not a precise medical concept. In the Appendix, we mention several terms written into policy and the law so that readers may be familiar with their meaning, but they are not medical terms.
States most often do so by (1) placing gestational age limits on abortion, and/or (2) restricting the methods providers can use to perform abortions later in pregnancy. In discussion of these laws, it is important to note that most policymakers are not clinicians, therefore many of the terms used to discuss abortions later in pregnancy are designed to communicate a political message, not a precise medical concept. In the Appendix, we mention several terms written into policy and the law so that readers may be familiar with their meaning, but they are not medical terms.
Abortion bans by gestational age
43 states prohibit abortions after a certain point in pregnancy, with almost half of states prohibiting abortion at “viability” or when viability is often presumed, at 24 weeks. Other states seek earlier gestational age limits on abortion. For example, so-called “heartbeat” bans propose banning abortion after the detectable presence of cardiac activity as early as 6 weeks gestation, months before viability. To date, all such “heartbeat” bans, along with others that seek to ban abortions before 20 weeks, are not in effect due to ongoing or resolved litigation. However, some states have enacted abortion bans from 20-22 weeks gestational age, using the rationale of fetal pain.
To date, all such “heartbeat” bans, along with others that seek to ban abortions before 20 weeks, are not in effect due to ongoing or resolved litigation. However, some states have enacted abortion bans from 20-22 weeks gestational age, using the rationale of fetal pain.
Fetal Pain
Many states restrict abortions at 22 weeks gestational age or 20 weeks post-fertilization, arguing the fetus has the ability to feel pain at this point in development, contrary to medical evidence. A systematic review of literature on fetal pain found that pain perception is unlikely before weeks 29 or 30 gestational age. ACOG has found “no legitimate scientific data or information” that supports the assertion that fetuses feel pain at 20 weeks post-fertilization, and the Royal College of Obstetricians and Gynecologists has also concluded fetal pain is not possible before 24 weeks, given immature brain development and neural networks.
Despite the medical evidence, policymakers have enacted gestational limits using the rationale that a fetus can feel pain at earlier stages in pregnancy. Mississippi bans abortion at 20 weeks gestation while abortion at 22 weeks gestation is banned by 17 other states (AL, AR, GA, IN, IA, KS, KY, LA, NE, ND, OH, OK, SC, SD, TX, WV, WI). Additionally, 13 states provide verbal or written counseling on fetal pain as part of pre-abortion counseling (AK, AR, GA, IN, KS, LA, MN, MO, OK, SD, TX, UT, WI) (Figure 3). Some states mandate this information be given to those seeking abortion later in pregnancy, while in others, this counseling is required at any stage of pregnancy. In Utah legislation was introduced, but not passed, that would have required providers to administer “fetal anesthesia” during abortions later in pregnancy. There is, however, no standard practice for how to provide fetal anesthesia during abortions, nor is there adequate safety data on how this would affect pregnant individuals.
Mississippi bans abortion at 20 weeks gestation while abortion at 22 weeks gestation is banned by 17 other states (AL, AR, GA, IN, IA, KS, KY, LA, NE, ND, OH, OK, SC, SD, TX, WV, WI). Additionally, 13 states provide verbal or written counseling on fetal pain as part of pre-abortion counseling (AK, AR, GA, IN, KS, LA, MN, MO, OK, SD, TX, UT, WI) (Figure 3). Some states mandate this information be given to those seeking abortion later in pregnancy, while in others, this counseling is required at any stage of pregnancy. In Utah legislation was introduced, but not passed, that would have required providers to administer “fetal anesthesia” during abortions later in pregnancy. There is, however, no standard practice for how to provide fetal anesthesia during abortions, nor is there adequate safety data on how this would affect pregnant individuals.
Figure 3: The Concept of Fetal Pain Plays a Role in Many Abortion Regulations
Bans on abortion methods used later in pregnancy
Almost all abortions performed at ≥21 weeks are performed by a dilation and evacuation (D&E) procedure (93–95% per CDC data). This involves dilating the cervix and evacuating the pregnancy tissue using forceps, with or without suction. D&Es can be performed safely up to at least 28 weeks gestational age, and when compared to their alternative of labor induction, have been found to be quicker and result in fewer complications; further, many women prefer surgical management as they will be sedated and do not have to undergo labor and delivery of the fetus.
This involves dilating the cervix and evacuating the pregnancy tissue using forceps, with or without suction. D&Es can be performed safely up to at least 28 weeks gestational age, and when compared to their alternative of labor induction, have been found to be quicker and result in fewer complications; further, many women prefer surgical management as they will be sedated and do not have to undergo labor and delivery of the fetus.
Several states have sought to ban D&E procedures, which would significantly limit how providers are able to perform abortions later in pregnancy. Currently, Mississippi and West Virginia have enacted D&E bans, while bans are temporarily enjoined in 6 states and over 25 states have attempted to pass such legislation. 20 states ban dilation and extractions (D&Xs), a rarely used abortion procedure also referred to as an intact D&E or a “partial birth abortion” by policymakers (Appendix). In total, 21 states have enacted bans on abortion methods used later in pregnancy (Figure 4).
Figure 4: Many States Ban Certain Abortion Procedures Used Later in Pregnancy
In addition to gestational age limits and method bans used for abortions later in pregnancy, it is important to remember these abortions are also subject to the same regulations that apply for abortions earlier in pregnancy, including mandatory waiting periods and physician and hospital requirements.
| The authors would like to acknowledge Jennifer Karlin, MD, PhD (University of California, San Francisco) for her review of an earlier draft of this fact sheet. |
Appendix
| Term | Description |
| Late-term abortion: | Non-medical term that typically refers to abortions occurring at or after 21 weeks gestational age, but does not consistently refer to a specific gestational age cutoff. |
| Post-viability abortion: | Non-medical term used to refer to abortions occurring after the fetus is considered viable, and sometimes used synonymously with late-term abortions. |
| Born-alive abortion: | Non-medical term used to refer to the exceedingly rare circumstance in which a newborn shows signs of life after an abortion, including breathing, a beating heart and voluntary movement. These cases are the subject of the proposed “Born-Alive Abortion Survivors Protection Act,” mandating healthcare workers provide care to infants who show signs of life after an attempted abortion. |
| Partial birth abortion: | Non-medical term often used to refer to a rarely used abortion procedure called dilation and extraction (D&X, also known an intact D&E). Has sometimes been used to refer to all dilation and evacuations (D&Es), the most common abortion procedure used from 14-28 weeks gestational age. |
| Dismemberment abortion: | Non-medical term sometimes used to refer to D&Es. |
NOTES: KFF does not endorse use of these terms. | |
The Reality of Late-Term Abortion Procedures
*To view as PDF: On Point – The Reality of Late-Term Abortion Procedures
Introduction
Of interest to the medical, moral, sociological, and political issues surrounding late-term abortion is the question of why women seek abortion after 20 weeks gestation. Any data considered to answer this question must be examined carefully for limitations. However, a greater understanding of the reasons why women choose these late-term procedures is valuable to those who seek to offer alternative, compassionate options.
The Reality of Late-Term Abortion Procedures
Abortions performed after 20 weeks gestation, when not done by induction of labor (which leads to fetal death due to prematurity), are most commonly performed by dilation and evacuation (D & E) procedures.[1] These particularly gruesome surgical techniques involve crushing, dismemberment and removal of a fetal body from a woman’s uterus, mere weeks before, or even after, the fetus reaches a developmental age of potential viability outside the mother. [2] In some cases, especially when the fetus is past the stage of viability, the abortion may involve administration of a lethal injection into the fetal heart in utero to ensure that the fetus is not pulled out alive or with the ability to survive.
[2] In some cases, especially when the fetus is past the stage of viability, the abortion may involve administration of a lethal injection into the fetal heart in utero to ensure that the fetus is not pulled out alive or with the ability to survive.
Late-term abortion is not an exact medical term, but it has been used at times to refer to surgical dilation & evacuation (dismemberment) abortions as well as intact dilation & extraction (partial-birth) abortions performed in the second (13-27 weeks) and third (27-39 weeks) trimesters. The graphic, unpalatable nature of abortion procedures performed on fetuses of such advanced gestation raises many objections, even among parties who might support abortion at earlier stages.[3] For these reasons, and because of the increased short-term health risks of these procedures for women,[4] numerous states have considered limiting late-term abortion procedures after 20 weeks gestation.[5] The actual number of surgical abortions performed after 20 weeks in the United States cannot be known due to a lack of national reporting. [6] CDC projections, based largely on voluntary state reporting and abortion provider survey data from the Guttmacher Institute, a former affiliate of Planned Parenthood, estimate that roughly 1%, or over 15,000, abortions are performed after 20 weeks annually in the U.S.[7] Thus, advocates of the women and unborn children affected by these procedures take great interest in mitigating the circumstances that drive women to seek late-term abortions.
[6] CDC projections, based largely on voluntary state reporting and abortion provider survey data from the Guttmacher Institute, a former affiliate of Planned Parenthood, estimate that roughly 1%, or over 15,000, abortions are performed after 20 weeks annually in the U.S.[7] Thus, advocates of the women and unborn children affected by these procedures take great interest in mitigating the circumstances that drive women to seek late-term abortions.
For many years, abortion-rights advocates have asserted that abortions after 20 weeks are performed because of maternal health complications or lethal fetal anomalies discovered late in pregnancy.[8] However, wider data from both the medical literature and late-term abortion providers indicates that most late-term procedures are not performed for these reasons. Previous survey studies of late-term abortion patients have confirmed that most late-term abortions are performed because of a delay in pregnancy diagnosis and for reasons similar to those given by first-trimester abortion patients: financial stressors, relationship problems, education concerns or parenting challenges. [9]
[9]
A recent paper entitled, “Who seeks abortion at or after 20 weeks?” supports these conclusions.[10] The study, published in Perspectives on Sexual and Reproductive Health, a journal of the Guttmacher Institute, marks a notable departure from previous statements by abortion rights advocates that late-term abortions were rarely elective. Authors Foster and Kimport highlight the characteristics of women seeking abortion at or after 20 weeks gestation. The authors acknowledge that, in fact, wider “data suggests that most women seeking later terminations are not doing so for reasons of fetal anomaly or life endangerment.”[11] The study explores reasons for delay in seeking abortion services, comparing first-trimester and late-term abortion groups. While there are numerous limitations to the study, the authors suggest that the characteristics of women who seek both first-trimester and late-term abortions are substantially similar.
Who Seeks Late-term Abortion?
To explore the characteristics of women who choose abortion after 20 weeks of pregnancy, Foster and Kimport used data from a larger abortion study, currently being conducted at the University of California, San Francisco. Interview and questionnaire data from over 400 women were gathered from 16 facilities that offer abortion procedures after 20 weeks gestation. A significant limiting factor of the study is the fact that the authors excluded women who sought abortion for reasons of fetal anomaly or life endangerment, without commenting on how large of a cohort this represented. Another significant limiting factor of the study is that only 44% of the eligible women participated (eligibility defined as women who obtained an abortion after 20 weeks gestation for reasons other than life endangerment or fetal anomaly), leaving room for significant selection bias.[12]
Interview and questionnaire data from over 400 women were gathered from 16 facilities that offer abortion procedures after 20 weeks gestation. A significant limiting factor of the study is the fact that the authors excluded women who sought abortion for reasons of fetal anomaly or life endangerment, without commenting on how large of a cohort this represented. Another significant limiting factor of the study is that only 44% of the eligible women participated (eligibility defined as women who obtained an abortion after 20 weeks gestation for reasons other than life endangerment or fetal anomaly), leaving room for significant selection bias.[12]
Of the patients interviewed, 272 had received an abortion at or after 20 weeks, while 169 had received a first-trimester abortion. The authors noted that the sample of participating women was “similar in race and ethnicity, age and parity to [the] population of women who receive abortions nationally.” Sixty-nine percent of the study participants were non-white. Women were grouped and compared according to those who had received first-trimester abortions and those who received abortions at or after 20 weeks. Interviews and questionnaires were completed with all women one week after their abortion procedures.
Women were grouped and compared according to those who had received first-trimester abortions and those who received abortions at or after 20 weeks. Interviews and questionnaires were completed with all women one week after their abortion procedures.
The characteristics of women who sought abortions after 20 weeks were generally similar to those who received first-trimester procedures. “The two groups did not differ by race or ethnicity, number of live births or abortions, mental or physical health history or substance abuse,” write the study authors. Nearly identical majorities of women from both groups were unmarried. Identical majorities from both groups had more than one previous live birth. Only small minorities of women in both groups reported heavy drinking, recreational drug use or a history of depression. [13]
The only statistically significant demographic differences between the first-trimester and late-term abortion recipients were age and employment.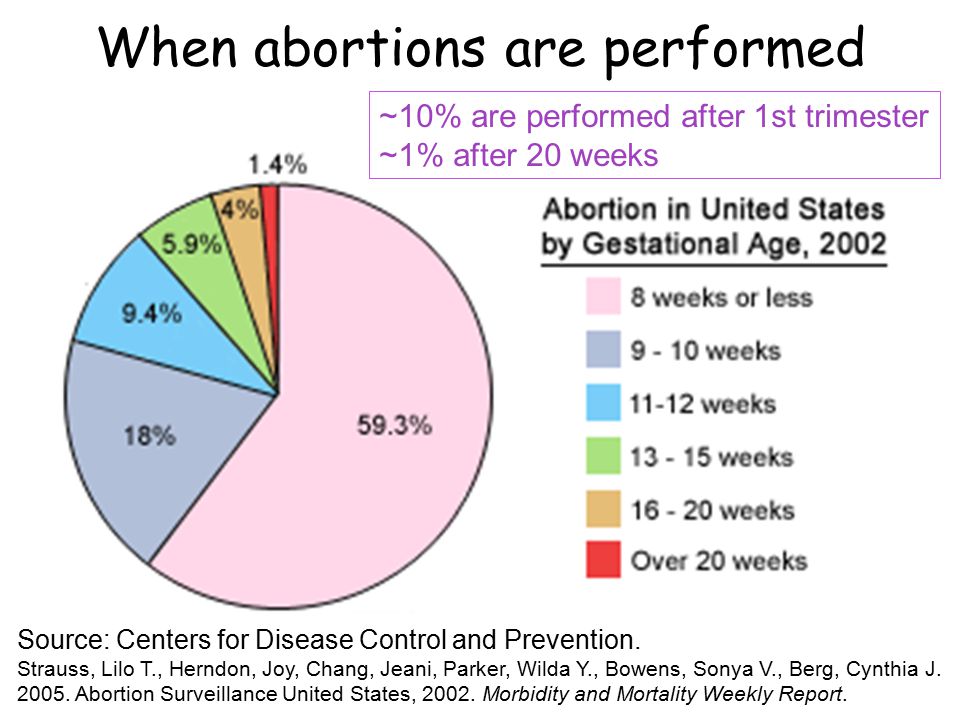 Seventy-five percent of women from both groups were between ages 20 and 34. However, women ages 20-24 were found more likely than women ages 25-34 to seek late-term abortions. Unemployed women were more likely to seek late-term abortions than employed women. However, among those women who sought a late-term abortion, equal numbers were employed and unemployed. Not surprisingly, women who sought later abortions were more likely than their first-trimester counterparts to have discovered their pregnancy after eight weeks. Yet, a sizeable percentage within the late-term abortion group, nearly 40%, reported that they knew about their pregnancy prior to eight weeks of gestation.[14]
Seventy-five percent of women from both groups were between ages 20 and 34. However, women ages 20-24 were found more likely than women ages 25-34 to seek late-term abortions. Unemployed women were more likely to seek late-term abortions than employed women. However, among those women who sought a late-term abortion, equal numbers were employed and unemployed. Not surprisingly, women who sought later abortions were more likely than their first-trimester counterparts to have discovered their pregnancy after eight weeks. Yet, a sizeable percentage within the late-term abortion group, nearly 40%, reported that they knew about their pregnancy prior to eight weeks of gestation.[14]
The study results also showed that, on average, women who obtained later abortions took twice as long as their first-trimester counterparts to obtain an abortion after discovering they were pregnant. Among women who received late-term abortions, the average time between pregnancy discovery and obtaining the abortion was over three months (14 weeks). Women receiving first-trimester abortions averaged a period of seven weeks between the time of pregnancy discovery and the time of their abortion. [15] The above results raise obvious questions as to why the timetable for obtaining an abortion was so much longer for women choosing late-term abortions.
Women receiving first-trimester abortions averaged a period of seven weeks between the time of pregnancy discovery and the time of their abortion. [15] The above results raise obvious questions as to why the timetable for obtaining an abortion was so much longer for women choosing late-term abortions.
As part of the study, participants were asked questions aimed at identifying possible reasons for delay in obtaining their abortion after discovering their pregnancy. The answers from both groups suggest that women share similar reasons for delaying abortion regardless of the gestational age at which they have the procedure. The majority of women in both groups gave at least one reason for delaying their abortion. Both groups cited the same seven reasons for delaying. Women in both groups reported “not knowing about the pregnancy,” “trouble deciding about the abortion,” and “disagreeing about the abortion with the man involved” with similar frequency.[16]
Among women in the late-term abortion group, the most commonly cited reason for delaying the procedure was “raising money for the procedure and related costs. ” Two thirds of women in the late-term abortion group gave this reason, compared with one-third of the women in the first-trimester group. It is worth noting that the average prices paid by women in the study were $2,014 for a late-term abortion compared to $519 for a first-trimester abortion, suggesting that, paradoxically, delaying for financial reasons required significantly more finances in the end. Women who received late-term abortions also cited “difficulty securing insurance coverage,” “difficulty getting to the abortion facility,” and “not knowing where to go for an abortion” as delaying reasons more often when compared to the first-trimester group. However, the two groups gave similar answers when asked how many abortion facilities they contacted before finding one willing to perform their abortion: the first-trimester group called an average of 1.7 facilities and the late-term group called a similar average of 2.2 facilities.[17]
” Two thirds of women in the late-term abortion group gave this reason, compared with one-third of the women in the first-trimester group. It is worth noting that the average prices paid by women in the study were $2,014 for a late-term abortion compared to $519 for a first-trimester abortion, suggesting that, paradoxically, delaying for financial reasons required significantly more finances in the end. Women who received late-term abortions also cited “difficulty securing insurance coverage,” “difficulty getting to the abortion facility,” and “not knowing where to go for an abortion” as delaying reasons more often when compared to the first-trimester group. However, the two groups gave similar answers when asked how many abortion facilities they contacted before finding one willing to perform their abortion: the first-trimester group called an average of 1.7 facilities and the late-term group called a similar average of 2.2 facilities.[17]
Conclusions
Abortion rights advocates have long insisted that late-term abortions are performed only in dire circumstances involving threats to a mother’s life or in cases of severe fetal anomaly. However, the above study, despite its limitations, suggests otherwise. The characteristic similarities and delay commonalities observed across first trimester and late-term abortion groups suggest that women who seek abortion share similar characteristics across gestational ages. The stressful circumstances of unprepared pregnancy, single-motherhood, financial pressure and relationship discord are primary concerns that must be addressed for these women. However, these circumstances are not fundamentally alleviated or ameliorated by late-term abortion. Indeed, late-term abortion places these women at greater risk of surgical complications, subsequent preterm birth, and mental health problems, while simultaneously ending the life of an unborn child.[18] As a medical profession and society, we rightly seek alternative, compassionate responses for the women seeking late-term abortion procedures for such challenging yet elective reasons.
However, the above study, despite its limitations, suggests otherwise. The characteristic similarities and delay commonalities observed across first trimester and late-term abortion groups suggest that women who seek abortion share similar characteristics across gestational ages. The stressful circumstances of unprepared pregnancy, single-motherhood, financial pressure and relationship discord are primary concerns that must be addressed for these women. However, these circumstances are not fundamentally alleviated or ameliorated by late-term abortion. Indeed, late-term abortion places these women at greater risk of surgical complications, subsequent preterm birth, and mental health problems, while simultaneously ending the life of an unborn child.[18] As a medical profession and society, we rightly seek alternative, compassionate responses for the women seeking late-term abortion procedures for such challenging yet elective reasons.
Elizabeth Ann M. Johnson, M.D. is an Associate Scholar for the Charlotte Lozier Institute. Johnson received her A.B. cum laude from Princeton University in public policy, and her M.D. from the University of Minnesota Medical School. She is currently a fellow in the Program for Human Rights and Health at the University of Minnesota School of Public Health.
Johnson, M.D. is an Associate Scholar for the Charlotte Lozier Institute. Johnson received her A.B. cum laude from Princeton University in public policy, and her M.D. from the University of Minnesota Medical School. She is currently a fellow in the Program for Human Rights and Health at the University of Minnesota School of Public Health.
[1] Dilation and evacuation procedures are used for 96% of abortions performed at >13 weeks gestation in the United States. Lohr PA, Hayes JL, Gemzell-Danielsson K. Surgical versus medical methods for second trimester induced abortion. Cochrane Database of Systematic Reviews. 2008; Issue 1, Art. No.: CD006714.
[2] The survival of very preterm infants has improved substantially in the past two decades, such that the gestational age at which at least half of very preterm infants survive has decreased to 23 weeks. Seri I, Evans J. Limits of viability: definition of the gray zone. J Perinatol. 2008;28(Suppl 1):S4–8.
2008;28(Suppl 1):S4–8.
[3] A recent study by the Lozier Institute examined gestational limits in 198 countries where abortion is legal; of those countries, only seven, including the United States, permit elective abortion after 20 weeks.
[4] Abortions performed after the first trimester have long been recognized to account for a disproportionate amount of abortion-related morbidity and mortality. Similar to other elective surgical or medical procedures, abortion procedures carry inherent risks of infection, bleeding, and damage to other genitourinary and gastrointestinal organs. They carry additional risks of incomplete emptying of the uterus, cervical laceration, and uterine perforation by the suction cannula or sharp curette. Additionally, abortions performed at later gestations are associated with higher odds of a subsequent preterm birth.
See: Lohr et al., 2008; Bartlett LA, Berg CJ, Shulman HB, Zane SB, Green CA, Whitehead S, Atrash HK. Risk factors for legal induced abortion-related mortality in the United States. Obstet Gynecol. 2004; 103(4):729-737; Hammond C, Recent advances in second trimester abortion: an evidence-based review. Am J Obstet Gynecol. 2009;200(4):347-356; Diedrich J, Steinauer J. Complications of Surgical Abortion. Clin Obstet Gynecol. 2009;52(2):205-212; Shah PS, Zao J. Induced termination of prepregnancy and low birthweight and preterm birth: a systemic review and meta-analysis. Brit J Obstet Gynecol. 2009;116(11):1425-1442.
Obstet Gynecol. 2004; 103(4):729-737; Hammond C, Recent advances in second trimester abortion: an evidence-based review. Am J Obstet Gynecol. 2009;200(4):347-356; Diedrich J, Steinauer J. Complications of Surgical Abortion. Clin Obstet Gynecol. 2009;52(2):205-212; Shah PS, Zao J. Induced termination of prepregnancy and low birthweight and preterm birth: a systemic review and meta-analysis. Brit J Obstet Gynecol. 2009;116(11):1425-1442.
[5] Jones RK, Jerman J. Abortion incidence and service availability in the United States. 2011. Perspectives Sexual Repro Hlth. 2014;46(1):3-14.
[6] Thorp JM, Jr. Public Health Impact of Legal Termination of Pregnancy in the US: 40 Years Later. Scientifica. 2012;2012:Article ID 980812, 16 pages.
[7] Thorp, 2012; Pazole K, Zane SB, Parker WY, Hall LR, Berg C, Cook DA., Abortion Surveillance—United States, 2008. Morbidity and Mortality Weekly Report. 2011;60(1):1-41.
[8] A fact sheet distributed by the National Abortion Federation during the 1995 debates over partial-birth abortion asked “Why do women seek abortions later in pregnancy?” and answered “Women seeking later abortions do so for very serious reasons. All abortions taking place in the third trimester are for reasons of serious fetal abnormality or a risk to the life of the woman. Many abortions that occur from 18 weeks’ gestation through the end of the second trimester are for this reason as well.” In 2013, a referendum in Albuquerque, New Mexico was proposed to place a limit of 20 weeks on abortions performed in the city. In the ensuing debate, advertising produced by NARAL Pro-Choice America featured a woman who chose “termination” due to a “severe fetal anomaly,” a condition stated in the ad to be “primarily” the reason for late abortions.
All abortions taking place in the third trimester are for reasons of serious fetal abnormality or a risk to the life of the woman. Many abortions that occur from 18 weeks’ gestation through the end of the second trimester are for this reason as well.” In 2013, a referendum in Albuquerque, New Mexico was proposed to place a limit of 20 weeks on abortions performed in the city. In the ensuing debate, advertising produced by NARAL Pro-Choice America featured a woman who chose “termination” due to a “severe fetal anomaly,” a condition stated in the ad to be “primarily” the reason for late abortions.
[9] Finer LB, Frohwirth LF, Dauphinee LA, Singh S, Moore AM., Reasons U.S. Women Have Abortions: Quantitative and Qualitative Perspectives. Perspectives Sexual Repro Hlth. 2005;37:110-118; Hammond, 2009
[10] Foster DG, Kimport K, Who Seeks Abortions at or After 20 Weeks? Perspectives Sexual Repro Hlth. 2013;45:210–218.
[11] Foster and Kimport, 2013.
[12] Foster and Kimport, 2013
[13] Foster and Kimport, 2013
[14] Foster and Kimport, 2013
[15] Foster and Kimport, 2013
[16] Foster and Kimport, 2013
[17] Foster and Kimport, 2013
[18] Thorp, 2012.
Late term abortion in St. Petersburg
What can a late term abortion look like?
Abortion after 12 weeks is performed by methods that are different from those used in the early stages, as the fetus grows large and the placenta is formed. Late abortion is carried out in the following ways:
- Medical. A woman takes drugs that stimulate labor and promote the release of the fetus from the uterus.
- Intrauterine (intraamnial) administration of fluids. The technique involves the suction of a certain volume of amniotic fluid using a thin needle, which is inserted through the cervical canal. Then the same amount of glucose or saline is injected into the fetal bladder, which leads to the death of the fetus.
 After a few hours, the patient begins labor and the fetus, along with the membranes, comes out.
After a few hours, the patient begins labor and the fetus, along with the membranes, comes out. - Small caesarean section. A dissection of the anterior wall of the abdomen and uterus is performed to remove the fetus and its membranes, then the uterus is scraped. When performing an abortion in the later stages, the child may already be viable, but due to the lack of medical care after removal from the uterus, he simply dies.
Indications
Late-term abortions are carried out only on doctor's orders. The reason for such an intervention may be serious illnesses of the mother or fetus, as well as a condition that makes normal child care impossible. A complete list of indications for the procedure is regulated by the relevant order of the Ministry of Health. Before performing an artificial termination of pregnancy in the later stages, a consultation with a doctor is required to decide its expediency and necessity. Possible indications for late abortion:
- pelvic cancer requiring emergency chemotherapy or radiotherapy;
- tuberculosis;
- diabetes mellitus with progressive retinopathy;
- severe mental illness;
- certain blood pathologies;
- active phase of Itsenko-Cushing's syndrome;
- severe form of Parkinson's disease, neurodystrophic pathologies;
- exacerbation of serious autoimmune diseases;
- severe malformations, chromosomal disorders in the fetus.

There are also social indications for artificial termination of pregnancy in the later stages:
- conception occurred as a result of rape;
- the patient's spouse has a 1-2 disability group or he died
- after pregnancy;
- if the woman is in prison;
- the presence of a court decision on the restriction and deprivation of the patient's parental rights regarding previously born children.
How is a late abortion performed?
The decision on such an intervention is sometimes difficult not only for a woman, but also for doctors. It is accepted by a commission, which includes an observing gynecologist, the head physician of a medical institution, as well as a specialized specialist who monitors the course of the pathology that made further gestation impossible.
For an abortion in the later stages, the patient is hospitalized in a gynecological hospital, where there is a resuscitation and intensive care unit.
Further actions depend on which method of interruption was determined by the council.
Rehabilitation period
Late abortion inflicts serious psychological trauma on the patient. Working with a psychologist will help to survive this condition and minimize mental health complications. Individual work with a psychologist or group sessions will be effective. After such an intervention, a woman does not lose her childbearing function, but she is allowed to re-pregnancy no earlier than six months later. The restoration of menstruation after artificial termination of pregnancy in the later stages occurs after 6-8 weeks.
Abortion and its consequences
Home / Articles / Consequences of abortion
Every woman knows what an abortion is, but how an abortion is done, what are the indications and contraindications, the consequences - not everyone knows.
An abortion is an abortion that occurs spontaneously or artificially for a period of up to 22 weeks with a fetus weighing up to 500 g. Why abortion is justified? Why create poverty? The pregnancy was the result of rape. Parents against the child or the husband says he will leave. If the mother can die in childbirth? If it is known that a sick child will be born? Parents are alcoholics. Other Reasons for Abortion... Pro-Abortion Slogans Every child should be wanted. Every woman has the right to control her own body. No one should impose his religious morality on others. Legalized abortion is safe. Abortion is not murder. the fetus is not human...
Why abortion is justified? Why create poverty? The pregnancy was the result of rape. Parents against the child or the husband says he will leave. If the mother can die in childbirth? If it is known that a sick child will be born? Parents are alcoholics. Other Reasons for Abortion... Pro-Abortion Slogans Every child should be wanted. Every woman has the right to control her own body. No one should impose his religious morality on others. Legalized abortion is safe. Abortion is not murder. the fetus is not human...
In the course of the process, abortions are distinguished:
· Spontaneous.
Artificial.
Spontaneous abortion is subdivided according to the term at which the pregnancy was terminated for various reasons:
1. Early spontaneous abortion - spontaneous abortion for up to 12 weeks.
2. Late - spontaneous interruption between 14 and 22 weeks.
3. Habitual - this is the name given to spontaneous interruption, repeated more than twice.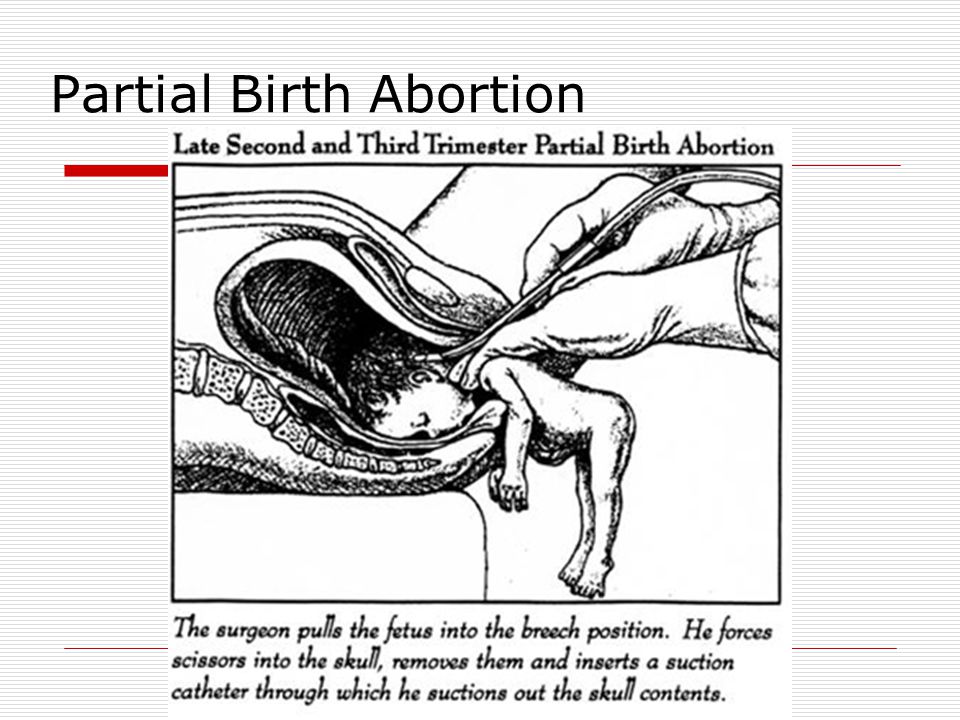
Artificial termination of pregnancy is also classified according to the conditions in which the manipulation was performed:
Safe abortion - performed in a specialized institution under the supervision of specialized specialists.
· Unsafe - performed under improper conditions, often by non-specialists. It is the manipulation in unsafe conditions that is the cause of postoperative complications, leading to sad consequences and ending in the death of a woman.
Interruption can be:
Medical.
Instrumental.
The instrumental solution, depending on the period and the chosen method of extraction, is of the following types:
· Vacuum extraction - used in the early stages up to 12 weeks.
· Dilatation, curettage - in its essence resembles a quite often performed gynecological procedure of separate curettage.
· Artificially induced labor - used later.
According to the peculiarities of the clinical course, abortions are divided:
Complete.
Incomplete.
· Failed.
· Launched, in progress.
Safe and unsafe abortions
Performing unsafe abortions is a rather complex and urgent problem of modern gynecology. Worldwide abortion statistics, according to WHO, show that despite the rapid development of modern medicine, the improvement and increase in the availability of medical care even in poor countries with low living standards, the annual number of unsafe abortions performed is more than 20 million cases. Of these, approximately 5 million end in bleeding, perforation of the uterus, septic complications, leading to the death of about 50 thousand women.
Even in developed countries, the mortality rate for women who have had unsafe abortions is 30 per 100,000 unsafe abortions. And for African countries, the rate reaches more than 500 deaths per 100,000 unsafe abortions.
The risk of complications from unsafe abortion increases progressively with increasing gestational age. As a rule, the likelihood of such an abortion is higher with limited availability of safe abortion, the lack of proper educational activities and promotion of contraceptives as an alternative to artificial termination of pregnancy.
Indications
In order to perform a safe abortion in a specialized medical facility, as well as for any medical intervention, there are indications:
1. Conscious choice of a woman. Within a period of up to 12 weeks, the woman's right to choose whether or not to terminate a pregnancy is legally enshrined.
2. Statement as a result of the performed examination of intrauterine death of the fetus, pathological conditions of the fetus.
3. Unforeseen complications during pregnancy that endanger the woman's life.
4. Examination confirmed ectopic pregnancy.
5. Critical changes in a woman's health that require immediate intervention, not directly related to the course of pregnancy: the need for organ transplantation, chemotherapy, radiation treatment in connection with an oncological disease detected during pregnancy. It should be noted that the described clinical situation is not an absolute indication for abortion. In all the cases described, the desire and the right are taken into account
women to continue pregnancy, despite the high risk of fatal outcomes for both mother and child.
6. The legal aspect of the right to terminate a pregnancy resulting from rape for up to 22 weeks.
Contraindications
General relative contraindications are:
Acute inflammatory, infectious diseases of the genital tract.
Diagnosed ectopic pregnancy.
· More than 12 weeks. The exception is the need to perform manipulations for medical reasons.
· The presence of Rhesus conflict during the first pregnancy.
Before an abortion is performed, there is a mandatory mandatory list of examinations.
Medical termination of pregnancy
WHO recommends the use of medical termination of pregnancy up to 9 weeks of pregnancy, but no more than 49 days after the last menstrual bleeding.
The indications for this type of abortion are:
The desire of the woman. (provided that the term allows the use of this method).
· Presence of medical indications identified before the specified date.
Contraindications are:
Intolerance to drugs.
Ectopic pregnancy.
Serious concomitant pathology in the acute phase, violation of the rheological properties of the blood.
Manipulation is carried out in a specialized institution, under the supervision of a specialist. As a rule, it does not require a woman's inpatient stay; medication can be taken on an outpatient basis.
Hospitalization is required in case of complications:
1. In the event of bleeding requiring urgent attention.
2. Incomplete abortion.
3. With the appearance of severe adverse reactions in the form of manifestations of allergies, dyspeptic disorders, uncontrollable vomiting, diarrhea, fever.
Medical interruption is 92 to 98% effective.
When prescribing this method of terminating an unwanted pregnancy, an important psycho-emotional factor should be taken into account: the drug effect is psychologically much easier for women than the use of instrumental methods.
Vacuum aspiration
Refers to instrumental methods. It is the WHO recommended way to safely terminate a pregnancy up to 12 weeks.
It is the WHO recommended way to safely terminate a pregnancy up to 12 weeks.
The effectiveness of this method is almost 100%, and the probability of complications according to statistical data does not exceed 0.1%.
Indications for vacuum aspiration are:
The patient wishes to terminate the pregnancy up to 12 weeks.
· Incomplete termination after a previous medical abortion.
Medical indication for termination before 12 weeks of pregnancy.
The procedure is performed in a specialized gynecological facility. Most often outpatient. Local anesthetics are used to relieve pain during the procedure.
Complications are:
· Uterine bleeding requiring surgical intervention if it is impossible to stop conservatively.
· Incomplete abortion - when it is impossible to perform ultrasound control after incision.
· Dizziness, nausea, vomiting, signs of severe weakness - are temporary, do not significantly affect long-term effects.
It is important to remember that after vacuum aspiration it is necessary to maintain sexual rest for at least 2-3 weeks.
Instrumental abortion (curettage)
Until recently, this was the only way to terminate an unwanted pregnancy.
Indication:
· To date, this method of interruption is used for periods of more than 12 weeks, exclusively taking into account medical indications.
In case of incomplete aspiration after minimally invasive manipulation, when visualizing the residual tissue of the fetal egg during ultrasound examination of the uterine cavity.
Requires a gynecological hospital for operating conditions. It is performed under general intravenous anesthesia.
The mechanism of abortion (curettage) is similar to separate curettage performed for diagnostic purposes: through the open external os and cervical canal, the entire functional layer of the uterus with the fetal egg is scraped out with a special tool (curette).
Complications are:
Uterine bleeding.
Injury to the walls of the uterus, perforation of the uterus, damage to the mucous membrane of the cervix with subsequent development of erosions.
· Occurrence of inflammatory processes in the organs of the reproductive system.
Artificial induction of labor
Performed at a later date. In essence, it is an abortion, but with significant differences:
· The presence of exclusively medical indications: a statement of the fact of intrauterine death of the fetus, the identification of severe anomalies in the development of the child incompatible with life.
· Complications of pregnancy, identified severe pathology in the mother, requiring urgent treatment, entailing the possibility of fatal consequences for the mother.
Long-term consequences of abortion
The consequences of abortion are divided into:
Early. These are early postoperative complications.
Remote.
It must be understood that termination of pregnancy in the absence of early complications does not mean at all that abortion is a harmless procedure that does not affect the body.
Long-term effects are:
1. Disturbances in the hormonal balance of the body, manifested by cycle disorders.
2. Occurrence of tumor formations of the mammary glands.
3. Tumor and pre-tumor background diseases of the female reproductive organs.
4. Chronic inflammatory diseases of the pelvic organs.
5. Occurrence of adhesive process in the small pelvis.
6. Infertility.
7. Psycho-emotional trauma, experiences. 8. Psychological consequences of abortion
Abortion leaves a mark not only on the body, but also on the soul of the mother. Women who have had an abortion are haunted by painful experiences that can lead to suicide. The psychological consequences of abortion are called "Post-abortion syndrome"...
9. Memories of women who have had an abortion If you want to have an abortion, listen to women who have already had it.