Can pregnancy cause anxiety
How can you manage anxiety during pregnancy?
Pregnancy is an exciting time. You will soon become a parent to an adorable, tiny human. You may expect to experience the rollercoaster of emotions during pregnancy, or emotions may catch you off guard. Some women feel joy at every flutter or kick, marveling at their changing bodies. For other women, pregnancy is hard, giving no reprieve as it brings severe fatigue, mood changes, and constant worries. You may notice that with every passing month, your thoughts are spiraling out of control, affecting your performance at work and your relationships at home. But how do you manage your anxiety, and should you treat it?
What causes anxiety during pregnancy?
Worries during pregnancy are universal. Hormonal changes of pregnancy, prior heartbreaking miscarriages, and sleep difficulties may all contribute to anxiety for mothers-to-be. You may worry about how a baby will affect your relationships with friends or family members, the health of your future child, the delivery experience, or the financial burden of an additional family member. All of these worries are completely normal. For humans, a certain amount of anxiety is protective; how else could we motivate ourselves to complete our work or run away from a bear?
What are the symptoms of anxiety disorders during pregnancy?
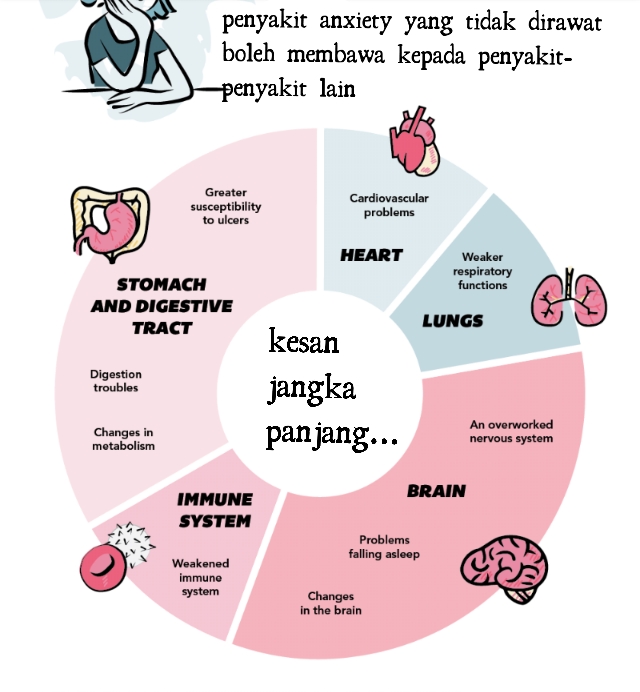
Although it’s normal to be worried about the health of your baby, in some cases this worry becomes debilitating and may require further attention. Thoughts about the health of the baby may become obsessive, even when doctors are reassuring. Worries may also appear as physical symptoms, such as a rapid heartbeat, difficulty breathing, or panic attacks. If this is the first time you experience a high level of anxiety, this may be frightening in itself. When anxiety starts to interfere with your day-to-day functioning, relationships, or job performance, it may be classified as an anxiety disorder — if your doctor picks up on it.
Anxiety can occur at any time during pregnancy, or it may first appear after delivery (perinatal anxiety is the term used for anxiety during pregnancy and after delivery). The rates of generalized anxiety disorder appear to be highest in the first trimester, likely due to hormonal changes. The most common symptoms of anxiety include constant worrying, restlessness, muscle tension, irritability, feeling dread, an inability to concentrate, and difficulties falling asleep due to worries. Some women also experience symptoms as a result of other anxiety disorders, including panic disorder, obsessive-compulsive disorder, or post-traumatic stress disorder.
The rates of generalized anxiety disorder appear to be highest in the first trimester, likely due to hormonal changes. The most common symptoms of anxiety include constant worrying, restlessness, muscle tension, irritability, feeling dread, an inability to concentrate, and difficulties falling asleep due to worries. Some women also experience symptoms as a result of other anxiety disorders, including panic disorder, obsessive-compulsive disorder, or post-traumatic stress disorder.
Unfortunately, two of the most common mental health screening tools in pregnancy (the Edinburgh Postnatal Depression Screen and Generalized Anxiety Disorder 7-item Scale) are not great at detecting anxiety in pregnancy. Although underdiagnosed, anxiety disorders during pregnancy and in the postpartum period are common, and may affect up to one in five women. Many women suffer in silence.
What are the effects of untreated anxiety on the fetus?
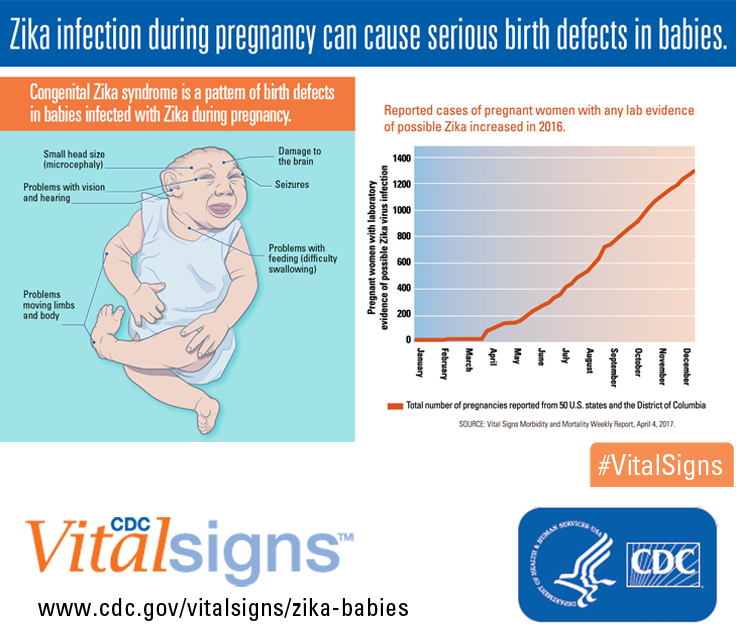
When thinking about management of anxiety, it is important to consider both the risks of treatment as well as the harms of untreated anxiety.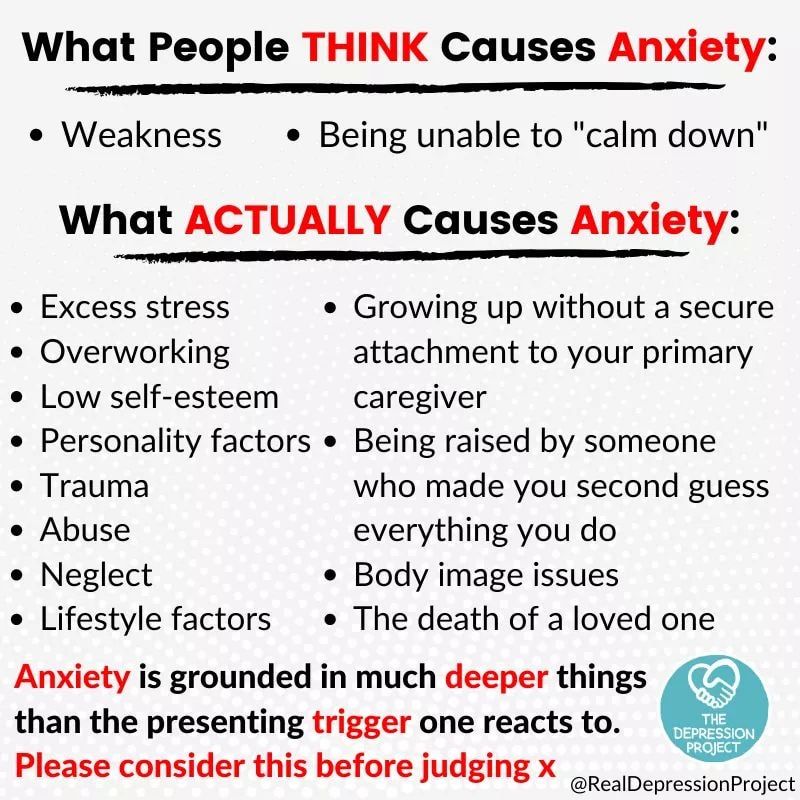 Although less studied than depression, research suggests that anxiety may negatively affect both the mother and the fetus. Anxiety increases the risk for preterm birth, low birthweight, earlier gestational age, and a smaller head circumference (which is related to brain size).
Although less studied than depression, research suggests that anxiety may negatively affect both the mother and the fetus. Anxiety increases the risk for preterm birth, low birthweight, earlier gestational age, and a smaller head circumference (which is related to brain size).
What are some treatments for anxiety during pregnancy?
Fortunately, there are many treatments that can reduce anxiety during pregnancy and help you feel better. For many women, anti-anxiety medication is not an option during pregnancy, as there is little information on the safety of such medication on the fetus. Some women who had previously taken medications for anxiety may wish to discontinue medications during pregnancy for personal reasons.
Therapies such as cognitive behavior therapy (CBT) demonstrate promise in the peripartum period (the period shortly before, during, and after giving birth). CBT focuses on challenging maladaptive thoughts, emotions, and actions, and it uses anxiety management strategies such as diaphragmatic breathing (adapted to pregnancy).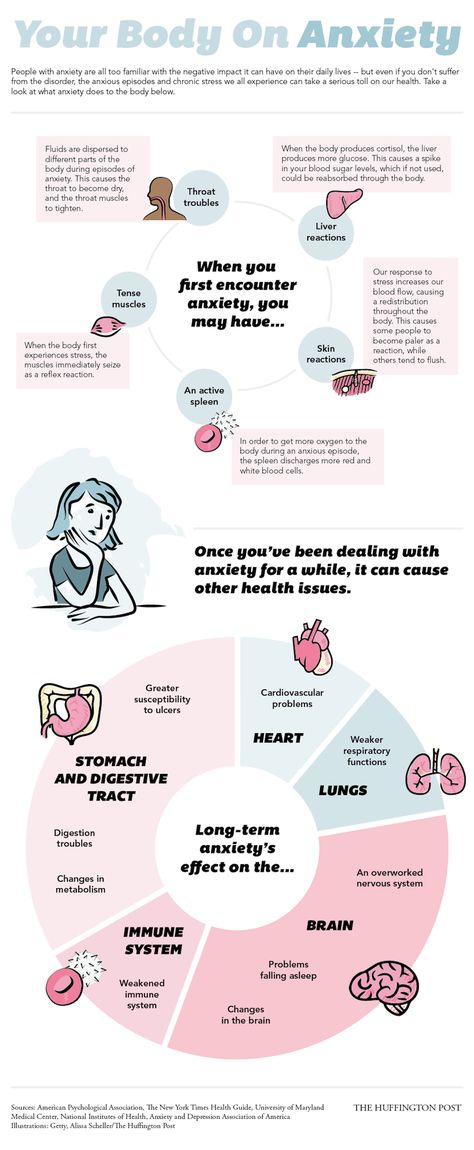
If your anxiety is severe, medications may be an option for you. Selective serotonin reuptake inhibitors (SSRIs) are commonly prescribed for depression and anxiety during pregnancy and after delivery. It does not appear that SSRIs are associated with an increased risk of major congenital malformations. However, SSRIs may be associated with transient neonatal symptoms such as jitteriness, tremor, crying, and trouble feeding, which resolve on their own in a few days.
The use of benzodiazepines such as lorazepam (Ativan) and alprazolam (Xanax) during pregnancy has long been a controversial topic. Although older studies showed an association between their use and an increased risk for cleft lip and palate, a more recent study looking at benzodiazepine use during pregnancy did not show this link when these medications were used alone (although there may be an increased risk when combined with antidepressants).
What else helps anxiety during pregnancy?
- Engage in regular physical activity.
 In general, it is safe to engage in physical activity during pregnancy. However, if you are at risk for preterm labor or have pregnancy complications, consult with your doctor first.
In general, it is safe to engage in physical activity during pregnancy. However, if you are at risk for preterm labor or have pregnancy complications, consult with your doctor first. - Ensure adequate sleep. Whether it’s a calming bedtime routine, pregnancy pillow, or a few nights in a bed away from your snoring partner, now is the time to learn what works for your sleep.
- Practice mindfulness. Research shows that mindfulness may reduce worries about labor, and it may even prevent postpartum depression.
- Journaling. Writing about your worries may help you brainstorm potential solutions, and it allows you to reflect on your concerns.
- Schedule worry time. We often worry because we do not want to forget something. Setting aside 30 minutes toward the end of the day provides you with a time to worry productively, but it frees you from holding onto your worries the rest of the day (practice reminding yourself "I’ll get to these thoughts later").
- Yoga, massage, meditation, and acupuncture. Finding relaxation techniques that work for you may take some experimentation — but their benefits will continue even after the baby arrives.
Recognizing Anxiety During Pregnancy - Anxiety Canada
Pregnancy is an emotional time, and anxiety is just one of many feelings that pregnant women experience. A moderate amount of new fears and worries is normal and expected during this time of change. If you are experiencing quite a bit of anxiety, it can be helpful to first learn more about what anxiety is, and how it can show up during pregnancy.
“Late in my pregnancy I feel so panicky all the time, my heart feels like it is always racing and I can’t even take deep breaths. I’m so scared to have another panic attack, I barely want to leave the house.” – Susan
“I know it’s not rational but since I’ve become pregnant I keep having this constant sense of dread.
Like something terrible is going to happen to my husband, and I will be left alone and pregnant. I text him several times a day to reassure myself he’s okay, but it doesn’t make me feel better for very long. I just hate being alone now.” – Anjali
What is Anxiety?
Anxiety is a natural, adaptive response we experience when we feel unsafe or threatened. We can experience many kinds of “threats” to the safety of ourselves and/or our loved ones. Sometimes we are anxious about something specific (e.g., waiting for the results of a diagnostic test). Some threats feel more vague, like a general sense that something bad will happen. We may also experience anxiety to a threat we are imagining in our heads, like picturing a loved one getting into an accident.
We can experience anxiety in these areas:
- In our bodies (increased heart rate, sore stomach, tight chest and throat, shallow breathing, loss of appetite, difficulty falling or staying asleep, etc.
 )
) - In our mind (racing thoughts about the future; imagining the worst-case scenario; ruminating; worrying and obsessing, etc.)
- In our actions or behaviours (avoiding certain situations, activities, places, or people; over-controlling; asking others for constant reassurance; checking things repeatedly; being extra careful and vigilant of danger, etc.)
Other possible signs of anxiety during pregnancy:
- loss of appetite
- difficulty sleeping
- irritability
- muscle tension (grinding teeth, neck and shoulder pain, back pain, muscle twitching)
- difficulty concentrating and focusing
- forgetfulness
How common is anxiety during pregnancy?
Anxiety is very common during pregnancy, and by some measures even more common than depression. Factors that could increase the chances of experiencing high anxiety during pregnancy include:
- history of high anxiety and/or depression
- perfectionism (believing you should not make any mistakes and do everything just right)
- history of miscarriage(s)
- high-risk pregnancy
- major life stressors (such as marital or financial problems)
Anjali’s Story
Anjali is a 28-year-old married woman in her second trimester of pregnancy.
Read more about this story
Susan’s Story
Susan is a 36-year-old mother in her third trimester of pregnancy. She also has a five-year-old son, Jacob.
Read more about this story
Evaluation of anxiety and related factors in pregnant women » Physician's Library
1) Department of Obstetrics, Jessenius Faculty of Medicine in Martin, Comenius University in Bratislava, Slovakia;
2) Department of Foreign Languages of the Jessenius Faculty of Medicine in Martin, Comenius University in Bratislava, Slovakia
Relevance. Pregnancy in the life of women is a difficult stage, which in many cases is accompanied by disturbing experiences.
Target. Study of anxiety symptoms and related factors in pregnant women. nine0003 Materials and methods. The cross-sectional study included 304 pregnant women with a normal pregnancy, the average age of which was 27±4.95 years. The Beck Anxiety Scale (BTS) was used to measure anxiety symptoms in pregnant women.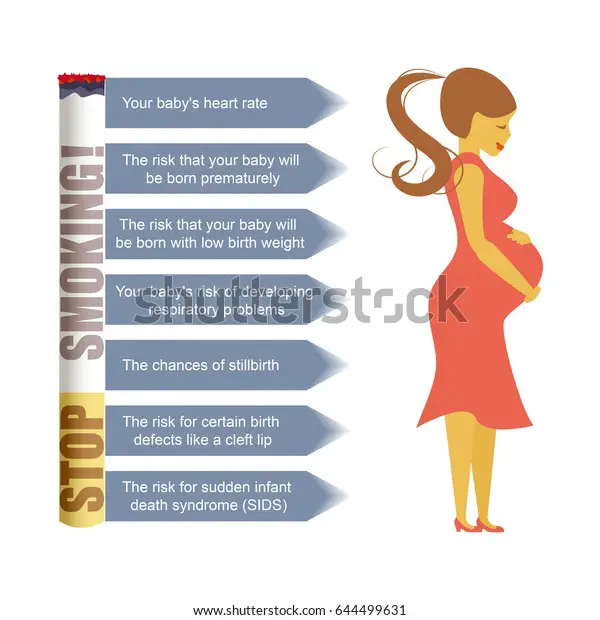 Additionally, age, parity, gestational age, health problems, and satisfaction with partner support were assessed, which are necessary to characterize the sample and assess the relationship between these indicators and anxiety. The data obtained were analyzed using descriptive statistics, the Kruskal–Wallis method, and the Wilcoxon test. nine0003 Results. Analysis of the results of STS showed the absence of anxiety symptoms in 10.53% of the respondents, while mild, moderate and severe anxiety disorders were identified in 50.66, 26.97 and 10.53% of the participants, respectively. Age and duration of pregnancy were not found to have a statistically significant effect on anxiety-related symptoms. The analysis showed that equity, satisfaction with partner support, and health problems are statistically significant for anxiety in pregnant women. nine0003 Conclusion. Anxiety disorders in pregnancy require not only early diagnosis in primary care settings, but also timely measures to be taken by healthcare professionals and partners of pregnant women to prevent anxiety during pregnancy in order to prevent adverse consequences for mother and child.
Additionally, age, parity, gestational age, health problems, and satisfaction with partner support were assessed, which are necessary to characterize the sample and assess the relationship between these indicators and anxiety. The data obtained were analyzed using descriptive statistics, the Kruskal–Wallis method, and the Wilcoxon test. nine0003 Results. Analysis of the results of STS showed the absence of anxiety symptoms in 10.53% of the respondents, while mild, moderate and severe anxiety disorders were identified in 50.66, 26.97 and 10.53% of the participants, respectively. Age and duration of pregnancy were not found to have a statistically significant effect on anxiety-related symptoms. The analysis showed that equity, satisfaction with partner support, and health problems are statistically significant for anxiety in pregnant women. nine0003 Conclusion. Anxiety disorders in pregnancy require not only early diagnosis in primary care settings, but also timely measures to be taken by healthcare professionals and partners of pregnant women to prevent anxiety during pregnancy in order to prevent adverse consequences for mother and child.
Pregnancy in a woman's life is a time of intense physical and mental stress that affects her well-being and causes a complex mixture of emotions: on the one hand, joy and expectation of what should happen, on the other, fear and anxiety of the unknown [1]. Women's increased anxiety during pregnancy is a common problem [2]. Women are known to be particularly prone to the onset or recurrence of anxiety disorders during pregnancy [3]. According to Madhavanprabhakaran G.K. et al. [4], the prevalence of anxiety disorders during pregnancy in different parts of the world varies from 14 to 54%. nine0004
Anxiety is characterized as a deep feeling of insecurity and powerlessness. The adverse effects of anxiety can turn pregnancy into a painful and unpleasant event in a woman's life, causing many physiological and psychosocial changes [5]. The emotions of a pregnant woman depend on her temperament and environment. The earliest manifestations of anxiety may include uncertainty about how a partner will react to pregnancy and how this will affect their life together and sexual relationship. In addition, a pregnant woman may face a wide variety of fears related to the progression of pregnancy, anxiety about the baby, lack of information about pregnancy and childbirth, or previous experience of pregnancy and childbirth. Anxiety during pregnancy can negatively affect the mental health of the mother and the outcome of childbirth. At the same time, it is considered as a risk factor for postpartum depression. Manifestations of anxiety include feelings of shyness, restlessness, and inner tension. These sensations are accompanied by physiological reactions affecting several functional systems and organs of a woman. There is evidence that anxiety during pregnancy not only affects a woman's health, but can also adversely affect the neuropsychic, cognitive and behavioral outcomes of a child's development [6, 7], his feelings of attachment. Anxiety disorders can affect the timing of pregnancy and increase the risk of preterm birth, caesarean section, or low birth weight [8, 9]. Research results indicate the need for early detection of maternal anxiety in the perinatal period and effective prevention [2].
In addition, a pregnant woman may face a wide variety of fears related to the progression of pregnancy, anxiety about the baby, lack of information about pregnancy and childbirth, or previous experience of pregnancy and childbirth. Anxiety during pregnancy can negatively affect the mental health of the mother and the outcome of childbirth. At the same time, it is considered as a risk factor for postpartum depression. Manifestations of anxiety include feelings of shyness, restlessness, and inner tension. These sensations are accompanied by physiological reactions affecting several functional systems and organs of a woman. There is evidence that anxiety during pregnancy not only affects a woman's health, but can also adversely affect the neuropsychic, cognitive and behavioral outcomes of a child's development [6, 7], his feelings of attachment. Anxiety disorders can affect the timing of pregnancy and increase the risk of preterm birth, caesarean section, or low birth weight [8, 9]. Research results indicate the need for early detection of maternal anxiety in the perinatal period and effective prevention [2].
Given the prevalence of anxiety disorders in pregnant women and their strong association with adverse pregnancy and childbirth outcomes, early detection and treatment of anxiety is important [10, 11]. Health professionals have the ability to identify anxiety in pregnant women and reduce anxiety levels, as well as provide emotional support [12]. nine0004
The aim of the study was to investigate anxiety symptoms and related factors in pregnant women.
Materials and methods
We conducted a cross-sectional study of 304 pregnant women with normal pregnancies who were willing to cooperate and signed a written informed consent to participate in the study.
Participants were selected using the convenience sampling method. The study was conducted in three gynecological polyclinics in the Zhilinsky district of Slovakia. The choice of polyclinics was determined by their availability, as well as the consent of their gynecologists. Pregnant women were contacted personally during antenatal counseling at polyclinics. The comprehensibility of the questionnaire was tested in a pilot study involving 5 respondents. Based on the results of the pilot study, the problematic formulations of a formal-stylistic nature were modified. A combined survey method was chosen. Pregnant women attending antenatal clinics were personally approached by trained nurses who were instructed by the research team about the study, data collection method and study inclusion criteria, and how to complete the questionnaire. Pregnant women who agreed to participate in the study signed an informed consent and subsequently received a link to an online questionnaire by email. The questionnaire could be completed in print or electronic form. A total of 340 questionnaires were issued, 80 of which were handed in personally in gynecological clinics, the response to them was 87.5% (70 questionnaires). The remaining 260 questionnaires were sent electronically to email addresses and the response rate was 95.38% (248 questionnaires). The overall percentage of completed questionnaires was 93.
The comprehensibility of the questionnaire was tested in a pilot study involving 5 respondents. Based on the results of the pilot study, the problematic formulations of a formal-stylistic nature were modified. A combined survey method was chosen. Pregnant women attending antenatal clinics were personally approached by trained nurses who were instructed by the research team about the study, data collection method and study inclusion criteria, and how to complete the questionnaire. Pregnant women who agreed to participate in the study signed an informed consent and subsequently received a link to an online questionnaire by email. The questionnaire could be completed in print or electronic form. A total of 340 questionnaires were issued, 80 of which were handed in personally in gynecological clinics, the response to them was 87.5% (70 questionnaires). The remaining 260 questionnaires were sent electronically to email addresses and the response rate was 95.38% (248 questionnaires). The overall percentage of completed questionnaires was 93. 53%. Of the 318 completed questionnaires, 14 questionnaires were excluded because of incorrect or incomplete answers, or because they did not meet the inclusion criteria. As a result, 304 questionnaires were used in the study.
53%. Of the 318 completed questionnaires, 14 questionnaires were excluded because of incorrect or incomplete answers, or because they did not meet the inclusion criteria. As a result, 304 questionnaires were used in the study.
To determine the level of anxiety in pregnant women, the standardized Beck Anxiety Scale (STS) was used [13]. The STB questionnaire consists of 21 items. Each item includes one of the typical symptoms...
Psycho-emotional disorders during pregnancy. The need for their correction | Tyutyunnik V.L., Mikhailova O.I., Chukhareva N.A. nine0001
Currently, more and more attention is paid to the influence of a woman's psycho-emotional state on reproductive function, pregnancy and perinatal outcomes [2,4,14]. In recent years, in developed countries, there has been an increase in the frequency of various mental disorders in women of reproductive age, the proportion of patients taking psychotropic drugs has increased, including among women who are planning a pregnancy and pregnant women [3,6,9].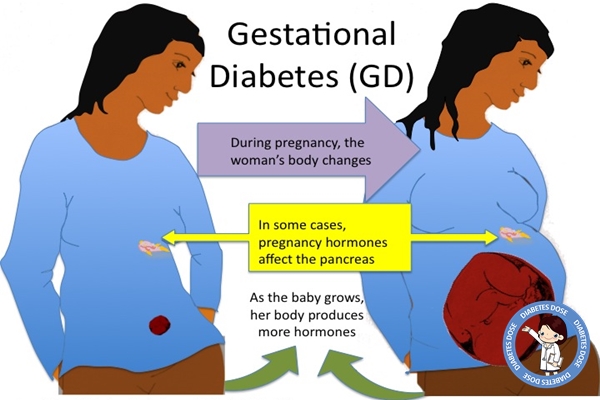
Almost all pregnant women are subject to sharp emotional swings, since the expectation of a child is associated with changes - both physical and emotional. Hormonal changes during pregnancy lead to the fact that the mood of a pregnant woman changes dramatically almost every hour. nine0003 A future mother can get rid of such emotional swings and feel calm during pregnancy by observing the rules of emotional health. Emotional balance and physical fitness are equally important for a pregnant woman, they equally help her prepare for motherhood. Due to the lack of maternal experience, a pregnant woman may experience sudden emotional outbursts. The first pregnancy is a new experience that is quite difficult to comprehend. Ignoring the fact that the emotions of a woman who is expecting a child is much more complex and sharper than usual, can lead to a number of problems, including in relations with her spouse. Acceptance of this fact is the basis of emotional health during pregnancy [1,5,11]. nine0003 Also, if a woman is pregnant for the first time, she experiences many fears, which include fear of childbirth and untimely termination of pregnancy, concern about the health of the unborn child and her own health, fear of labor pains and inevitable pain, fear of partner / spouse disappointment due to changes occurring with body. Modern women have to worry about careers, financial problems, and many additional costs associated with the appearance and upbringing of a new family member. nine0003 All these fears can lead to many negative emotions, such as anxiety, depression, irritation, anxiety, stress, anger, feelings of loneliness, confusion. Most often, changes in the psycho-emotional background during pregnancy lead to the development of depressive and anxiety disorders. Until the end, the pathogenesis of these changes is unclear, several theories are discussed, it is believed that changes in the hormonal background during pregnancy, including a significant increase in estrogens, and especially progesterone, in the blood serum can exacerbate existing emotional disorders [5,7,15].
nine0003 Also, if a woman is pregnant for the first time, she experiences many fears, which include fear of childbirth and untimely termination of pregnancy, concern about the health of the unborn child and her own health, fear of labor pains and inevitable pain, fear of partner / spouse disappointment due to changes occurring with body. Modern women have to worry about careers, financial problems, and many additional costs associated with the appearance and upbringing of a new family member. nine0003 All these fears can lead to many negative emotions, such as anxiety, depression, irritation, anxiety, stress, anger, feelings of loneliness, confusion. Most often, changes in the psycho-emotional background during pregnancy lead to the development of depressive and anxiety disorders. Until the end, the pathogenesis of these changes is unclear, several theories are discussed, it is believed that changes in the hormonal background during pregnancy, including a significant increase in estrogens, and especially progesterone, in the blood serum can exacerbate existing emotional disorders [5,7,15]. As a rule, minor manifestations in the form of irritability, tearfulness, resentment accompany manifestations of early toxicosis in the first trimester of pregnancy - nausea, vomiting, etc. [6,10]. After the disappearance of these symptoms, the neuropsychic state of pregnant women usually improves. At the same time, an important role in the development of anxiety states is played by certain physical discomfort and psychological factors, which include forced changes in lifestyle, communication in the family and with work colleagues, concern for the health of the unborn child, financial difficulties - all this contributes to the appearance or exacerbation of psycho-emotional disorders during pregnancy. For some women, the onset of pregnancy is unexpected and not always desirable, however, due to the circumstances, a decision is made to prolong this pregnancy, which can lead to a further increase in stress and anxiety [5,8,12]. It should be noted that additional psychotraumatic factors may appear during pregnancy, such as the occurrence of pregnancy complications requiring hospitalization, or the detection of congenital malformations in the fetus, which can cause negative images and feelings [1,10,12].
As a rule, minor manifestations in the form of irritability, tearfulness, resentment accompany manifestations of early toxicosis in the first trimester of pregnancy - nausea, vomiting, etc. [6,10]. After the disappearance of these symptoms, the neuropsychic state of pregnant women usually improves. At the same time, an important role in the development of anxiety states is played by certain physical discomfort and psychological factors, which include forced changes in lifestyle, communication in the family and with work colleagues, concern for the health of the unborn child, financial difficulties - all this contributes to the appearance or exacerbation of psycho-emotional disorders during pregnancy. For some women, the onset of pregnancy is unexpected and not always desirable, however, due to the circumstances, a decision is made to prolong this pregnancy, which can lead to a further increase in stress and anxiety [5,8,12]. It should be noted that additional psychotraumatic factors may appear during pregnancy, such as the occurrence of pregnancy complications requiring hospitalization, or the detection of congenital malformations in the fetus, which can cause negative images and feelings [1,10,12]. nine0003 The state of psycho-emotional stress with the presence of anxiety of various levels is observed in 40% of women with a normal pregnancy [2,7,11]. Borderline neuropsychiatric disorders can be presented in the form of hypochondriacal and hysterical syndromes. However, there are other forms of gestational borderline neuropsychiatric disorders, their features are the invariable inclusion in the clinical picture of certain psychopathological phenomena directly related to pregnancy: various fears for the successful course of pregnancy, obsessive fears for the fate of the fetus, expectation of childbirth, conditioned reflex fears associated with unfavorable past pregnancies and childbirth [5,6,8]. A study of pregnant women who do not have signs of borderline neuropsychiatric disorders showed that character accentuation was established only in a quarter of women. The first trimester of pregnancy is usually characterized to some extent by the sharpening of existing character traits. Soft, vulnerable, insecure women become even more impressionable, sometimes excessively tearful, and anxious (those women who have had miscarriages in the past or this pregnancy are not going well, in this case, the fear of another abortion can become simply obsessive) ).
nine0003 The state of psycho-emotional stress with the presence of anxiety of various levels is observed in 40% of women with a normal pregnancy [2,7,11]. Borderline neuropsychiatric disorders can be presented in the form of hypochondriacal and hysterical syndromes. However, there are other forms of gestational borderline neuropsychiatric disorders, their features are the invariable inclusion in the clinical picture of certain psychopathological phenomena directly related to pregnancy: various fears for the successful course of pregnancy, obsessive fears for the fate of the fetus, expectation of childbirth, conditioned reflex fears associated with unfavorable past pregnancies and childbirth [5,6,8]. A study of pregnant women who do not have signs of borderline neuropsychiatric disorders showed that character accentuation was established only in a quarter of women. The first trimester of pregnancy is usually characterized to some extent by the sharpening of existing character traits. Soft, vulnerable, insecure women become even more impressionable, sometimes excessively tearful, and anxious (those women who have had miscarriages in the past or this pregnancy are not going well, in this case, the fear of another abortion can become simply obsessive) ).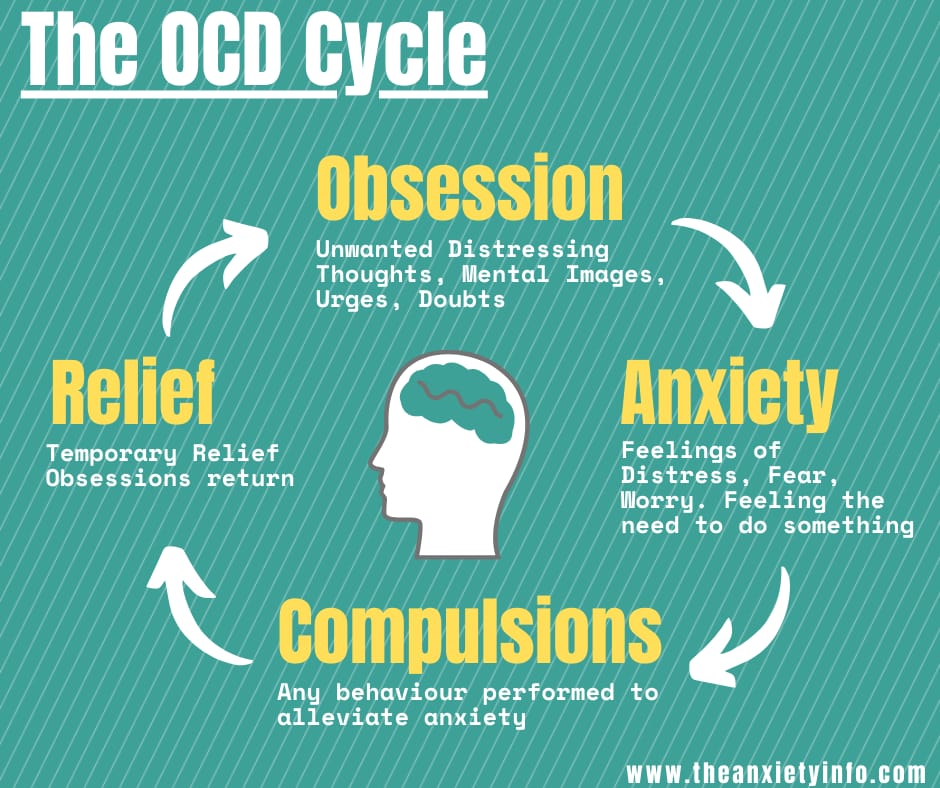 Powerful women with a sharp character can become even more aggressive, irritable and demanding. In the third trimester of pregnancy, emotional swings may begin again in connection with the expectation of childbirth, and with them fear - especially women who have to experience this event for the first time are susceptible to it [5,6,11]. nine0003 Anxiety disorders may first appear during pregnancy, there may be a change in the course of already existing disorders. In one retrospective study in women with panic attacks, 20% of cases showed a decrease in symptoms during pregnancy, 54% remained unchanged, and 26% worsened the course of the disease [12]. The detection of depression in pregnant women is difficult. Many symptoms, such as emotional lability, increased fatigue, changes in appetite and cognitive decline, are often found in physiologically normal pregnancy. Under stress, the hormones of the adrenal glands of the mother release catecholamines (stress hormones) into the blood, and during the experience of positive emotions (joy, calm, etc.
Powerful women with a sharp character can become even more aggressive, irritable and demanding. In the third trimester of pregnancy, emotional swings may begin again in connection with the expectation of childbirth, and with them fear - especially women who have to experience this event for the first time are susceptible to it [5,6,11]. nine0003 Anxiety disorders may first appear during pregnancy, there may be a change in the course of already existing disorders. In one retrospective study in women with panic attacks, 20% of cases showed a decrease in symptoms during pregnancy, 54% remained unchanged, and 26% worsened the course of the disease [12]. The detection of depression in pregnant women is difficult. Many symptoms, such as emotional lability, increased fatigue, changes in appetite and cognitive decline, are often found in physiologically normal pregnancy. Under stress, the hormones of the adrenal glands of the mother release catecholamines (stress hormones) into the blood, and during the experience of positive emotions (joy, calm, etc. ), the hypothalamic structures produce endorphins, which, penetrating through the placental barrier, directly affect the fetus. Consequently, mother and child are a single neurohumoral organism, and each of them equally suffers from the adverse influence of the outside world, which is recorded in long-term memory, affecting the entire subsequent life of the child. Positive maternal emotions cause an increase in the growth of the fetus and an increase in the level of its sensory perception. nine0003 According to the literature [2,5,11,15], a significant effect of anxiety disorders on the course of pregnancy and perinatal outcomes has been noted: the frequency of placental insufficiency, fetal growth retardation, premature birth, the birth of children with low body weight, which subsequently affects negatively on long-term forecast for them.
), the hypothalamic structures produce endorphins, which, penetrating through the placental barrier, directly affect the fetus. Consequently, mother and child are a single neurohumoral organism, and each of them equally suffers from the adverse influence of the outside world, which is recorded in long-term memory, affecting the entire subsequent life of the child. Positive maternal emotions cause an increase in the growth of the fetus and an increase in the level of its sensory perception. nine0003 According to the literature [2,5,11,15], a significant effect of anxiety disorders on the course of pregnancy and perinatal outcomes has been noted: the frequency of placental insufficiency, fetal growth retardation, premature birth, the birth of children with low body weight, which subsequently affects negatively on long-term forecast for them.
Thus, emotional swings are dangerous not only for the woman herself, but also for her unborn child. When a pregnant woman experiences stress, her body produces more of the hormone cortisol, the main “stress hormone”. Cortisol increases blood pressure and blood sugar levels, negatively affects the strength of the immune system - which, of course, adversely affects the health of the child. nine0003 Stress during pregnancy is dangerous for a variety of reasons. Chronic stress experienced for several weeks can slow down the development of the cells of the body of the embryo, the growth of the fetus. This increases the risk of miscarriage or spontaneous abortion or premature birth. Elevated levels of stress hormones can damage the brain of an unborn baby and lead to parenting problems later on.
Cortisol increases blood pressure and blood sugar levels, negatively affects the strength of the immune system - which, of course, adversely affects the health of the child. nine0003 Stress during pregnancy is dangerous for a variety of reasons. Chronic stress experienced for several weeks can slow down the development of the cells of the body of the embryo, the growth of the fetus. This increases the risk of miscarriage or spontaneous abortion or premature birth. Elevated levels of stress hormones can damage the brain of an unborn baby and lead to parenting problems later on.
Psychological stress in the perinatal period brings with it a whole range of problems that require serious attention to the psychological sphere of a pregnant woman in order to avoid obstetric and other complications. However, diagnostic criteria for the transition of the stress syndrome from the link of adaptation to the link of pathogenesis of various diseases have not yet been found [2,4,15]. nine0003 Emotional control is necessary to maintain normal emotional balance during pregnancy.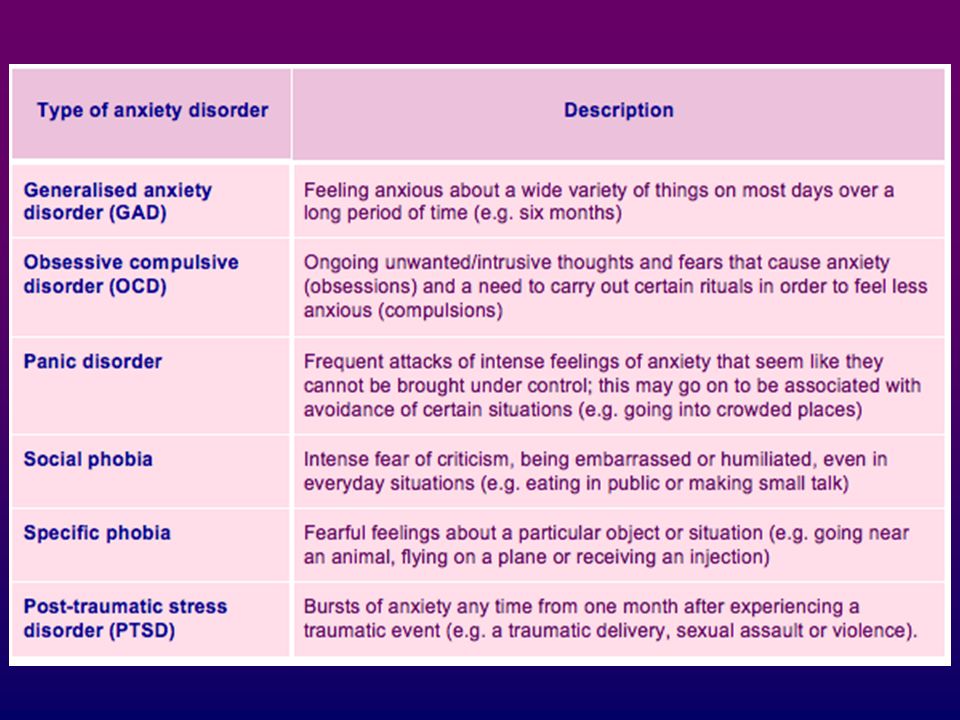 A pregnant woman who successfully manages her emotions is aware of the changing emotional balance and is ready to accept what is happening to her.
A pregnant woman who successfully manages her emotions is aware of the changing emotional balance and is ready to accept what is happening to her.
There are several basic rules that will help to cope with emotional imbalance:
• You must come to terms with the fact that physical and emotional changes are an inevitable part of the pregnancy period. You need to understand that this is a temporary stage that will last only a few months and end a maximum of 1-2 months after the birth of the child. nine0003 • Each trimester of pregnancy brings new changes, both in the body and in the emotional state. The main source of information about pregnancy is special literature and the experience of women who have recently given birth, who can share their feelings and experiences.
• A pregnant woman is responsible for the emergence of a new life. Taking care of yourself means taking care of your child. Proper nutrition, rest and self-indulgence are essential.
• A pregnant woman should be open to dialogue and not be afraid to discuss her problems with a gynecologist, partner or friends - anyone who can provide emotional support. You should not keep fears and worries in yourself - this will only aggravate internal tension. nine0003 • Changes associated with pregnancy can lead to low energy and, as a result, rapid fatigue. You need to slow down, re-prioritize your work, and give yourself a break.
You should not keep fears and worries in yourself - this will only aggravate internal tension. nine0003 • Changes associated with pregnancy can lead to low energy and, as a result, rapid fatigue. You need to slow down, re-prioritize your work, and give yourself a break.
• Emotional tension and negative emotions can be overcome by being distracted by pleasant activities or hobbies. When emotions overwhelm you, try to analyze what is bothering you, and then find an adequate solution.
• Engaging in certain physical activities designed specifically for expectant mothers will help improve both physical and emotional health. nine0003 • The main components of emotional health during pregnancy are rest and comfort.
However, unfortunately, during pregnancy, a woman cannot always cope with nervous tension, irritability, anxiety, excitement and other symptoms of stress on her own. Therefore, in some situations, she needs medical help.
The relative risk of using drugs during pregnancy makes it difficult to choose therapy, therefore, for the correction of psycho-emotional disorders that occur during pregnancy, herbal drugs that have practically no side effects can be considered as highly safe therapy. nine0003 The basis of anti-anxiety complex herbal remedies is valerian. It has been used in traditional medicine for many years for its hypnotic and sedative effects and remains a highly sought after remedy to this day. The mild hypnotic effect of valerian makes it possible to use it for the relief of shallow insomnia caused by anxiety. In addition, the vegetotropic effect of valerian is well known, its ability to have a uniform effect on both mental and somatic (vegetative) symptoms of anxiety. Valerian preparations also have anxiolytic and neuroprotective effects. The spectrum of side effects of valerian is very narrow and practically limited only to allergic reactions. Although valerian extract is metabolized by the cytochrome P450 system, it has virtually no effect on the metabolism of other drugs, and thus unwanted drug interactions are excluded. nine0003 Among the phytopreparations used by clinicians for the treatment of psycho-emotional disorders, Persen, a modern combined sedative preparation of plant origin, is widely used to relieve stress symptoms (anxiety, irritability and emotional stress) without causing drowsiness.
nine0003 The basis of anti-anxiety complex herbal remedies is valerian. It has been used in traditional medicine for many years for its hypnotic and sedative effects and remains a highly sought after remedy to this day. The mild hypnotic effect of valerian makes it possible to use it for the relief of shallow insomnia caused by anxiety. In addition, the vegetotropic effect of valerian is well known, its ability to have a uniform effect on both mental and somatic (vegetative) symptoms of anxiety. Valerian preparations also have anxiolytic and neuroprotective effects. The spectrum of side effects of valerian is very narrow and practically limited only to allergic reactions. Although valerian extract is metabolized by the cytochrome P450 system, it has virtually no effect on the metabolism of other drugs, and thus unwanted drug interactions are excluded. nine0003 Among the phytopreparations used by clinicians for the treatment of psycho-emotional disorders, Persen, a modern combined sedative preparation of plant origin, is widely used to relieve stress symptoms (anxiety, irritability and emotional stress) without causing drowsiness. Along with valerian, the composition of the drug includes dry extracts of medicinal plants with pronounced anxiolytic activity - peppermint and lemon balm (Table 1). The additional antispasmodic effect of peppermint makes it possible to successfully use the drug in patients with a pronounced somatic component of the anxiety syndrome. In addition, lemon balm has a nootropic (increased concentration and speed of problem solving), antioxidant effect. Persen is administered orally to adults and adolescents over 12 years old, 2-3 coated tablets, 2-3 times / day, Persen forte - inside to adults and adolescents over 12 years old, 1-2 capsules 2-3 times / day. nine0003 The advantages of Persen over other sedatives are:
Along with valerian, the composition of the drug includes dry extracts of medicinal plants with pronounced anxiolytic activity - peppermint and lemon balm (Table 1). The additional antispasmodic effect of peppermint makes it possible to successfully use the drug in patients with a pronounced somatic component of the anxiety syndrome. In addition, lemon balm has a nootropic (increased concentration and speed of problem solving), antioxidant effect. Persen is administered orally to adults and adolescents over 12 years old, 2-3 coated tablets, 2-3 times / day, Persen forte - inside to adults and adolescents over 12 years old, 1-2 capsules 2-3 times / day. nine0003 The advantages of Persen over other sedatives are:
• the preparation contains only natural ingredients;
• the effectiveness and safety of herbal ingredients Persena are well studied;
• does not contain alcohol and bromine;
• can be combined with any psychotropic drugs, including antidepressants;
• effective as a fast-acting symptomatic remedy when it is necessary to stop the symptoms of anxiety, agitation, and during a course of treatment for stress conditions, anxiety and phobic disorders. nine0003 Due to the natural components of plant origin that are part of Persen, this drug can be used during pregnancy. In each case, the doctor must evaluate the benefits and risks of taking Persen and other drugs, depending on the severity of the symptoms of the disease.
nine0003 Due to the natural components of plant origin that are part of Persen, this drug can be used during pregnancy. In each case, the doctor must evaluate the benefits and risks of taking Persen and other drugs, depending on the severity of the symptoms of the disease.
Thus, to prevent possible development, as well as to treat psycho-emotional disorders in pregnant women, it is advisable to use sedatives, the effect of which softens the damaging effects of psychogenic factors. nine0004
Literature
1. Abramchenko V.V., Kovalenko N.P. Perinatal psychology: Theory, methodology, experience. Petrozavodsk, 2004. 350s.
2. Avedisova A.S. Anxiety disorders // Alexandrovsky Yu.A. "Mental disorders in general medical practice and their treatment". M: GEOTAR-MED. 2004, pp. 66–73.
3. Voznesenskaya T.G., Fedotova A.V., Fokina N.M. Persen-forte in the treatment of anxiety disorders in patients with psychovegetative syndrome // Treatment of nervous diseases. 2002. No. 3 (8). pp. 38–41. nine0003 4. Vorobieva O.V. Psychovegetative syndrome associated with anxiety (issues of diagnosis and therapy) // Russian Medical Journal. 2006. V.14. No. 23. S. 1696-1699.
2002. No. 3 (8). pp. 38–41. nine0003 4. Vorobieva O.V. Psychovegetative syndrome associated with anxiety (issues of diagnosis and therapy) // Russian Medical Journal. 2006. V.14. No. 23. S. 1696-1699.
5. Grandilevskaya I.V. Psychological features of women's response to the identified pathology of pregnancy: Abstract of the thesis. dis. ... cand. psychol. Sciences. SPb., 2004.
6. Kasyanova O.A. Socio-psychological factors in preparing women for pregnancy, childbirth and motherhood: Abstract of the thesis. dis. ... cand. psychol. Sciences. Yaroslavl, 2005.
7. Kovalenko N.P. Psychoprophylaxis and psychocorrection of women during pregnancy and childbirth: Abstract of the thesis. dis. … doc. psychol. Sciences. SPb., 2001.
8. Filippova G.G. Psychological readiness for motherhood // Reader on perinatal psychology: Psychology of pregnancy, childbirth and the postpartum period. M., Izd-vo URAO, 2005. 328 p.
9 Davidson J.R.T. Pharmacotherapy of generalized anxiety // J.