Baby too small
IUGR—Why Is My Baby Small and What Can Be Done About It?
What is IUGR?
IUGR stands for intrauterine growth retardation. This means that your baby is growing slowly and doesn't weigh as much as your doctor expected for this stage of pregnancy. If your unborn baby weighs less than most babies at this stage, your baby might have IUGR. IUGR is also used to describe a baby who weighs less at birth than most babies at the same stage. For babies who are born near their due date (meaning, they aren't premature), the dangerous weight is anything less than 5 pounds, 8 ounces.
Your doctor might suspect IUGR if he or she thinks your baby is growing slightly less than would be expected. IUGR is usually diagnosed during an ultrasound examination. Doctors most often find it during the 6th, the 7th or the 8th months of pregnancy.
It's important to know that IUGR only means slowed growing. These small babies aren't mentally slow or retarded. Most small babies grow up to be healthy children and adults.
Why is my baby small?
Doctors know many of the causes of IUGR but are only able to be sure about the cause in about one half of babies who have IUGR. The most common reasons for a baby to be small are the following:
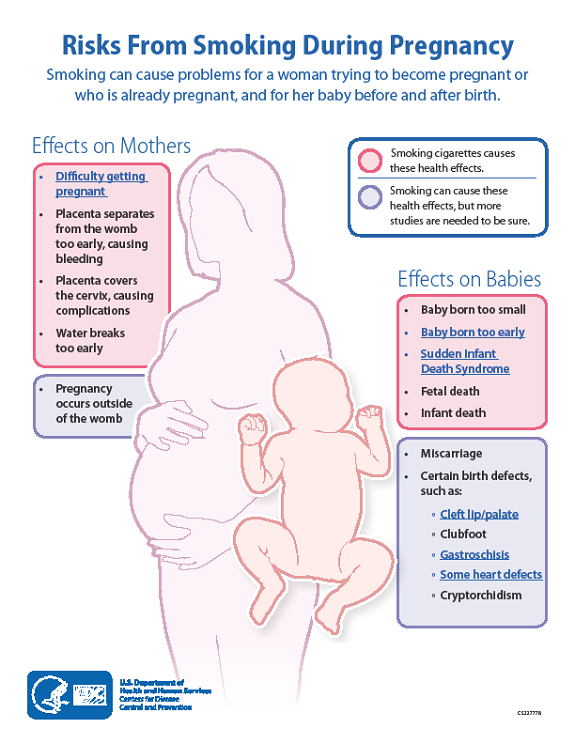
The mother smoked cigarettes during pregnancy.
The mother drank alcohol during pregnancy.
The mother had high blood pressure during pregnancy.

The mother had infections during pregnancy.
The baby has chromosomal abnormalities (like Down syndrome).
The mother used certain medicines during pregnancy.
The mother is small (less than 5 feet tall or weighing less than 110 pounds).
Why is my baby's size important?
The best predictor of a baby's survival and good health is its birth weight. Babies born with low birth weight might have problems near the time of birth. Because of the danger of some of these problems—such as difficulty holding a normal body temperature or fighting infection—your doctor will do some tests to find out if your baby is growing well, both before and after birth.
What tests might be done on my baby?
Two tests can find out if your baby has IUGR and keep track of your baby's growth in the womb. These tests are the ultrasound exam and the nonstress test. The first kind of test, the ultrasound exam, is used to find out if your baby has IUGR. This exam is done every three to four weeks to make sure your baby is still growing right. The ultrasound exams let your doctor look at your baby's internal organs and measure the amount of fluid around the baby.
This exam is done every three to four weeks to make sure your baby is still growing right. The ultrasound exams let your doctor look at your baby's internal organs and measure the amount of fluid around the baby.
Special ultrasound exams are called biophysical profiles. During a biophysical profile, the person who does the exam will also watch your baby's breathing, muscle tone and movements.
The other test is the nonstress test. This test is usually done in the doctor's office, but it might be done in a hospital. A nonstress test measures how fast your baby's heart is beating. A healthy baby normally has a heartbeat that gets faster as the baby moves around. A nonstress test takes about 20 to 30 minutes to do. It might take longer if your baby is asleep.
Sometimes your doctor wants to watch your baby's heartbeat while your uterus contracts (squeezes together). This is called a contraction stress test. There are two ways to help you have contractions for just a little while. First, your nipples will be warmed up. Sometimes this makes your uterus start contracting for a little while. If that doesn't work, you could take a special medicine (either oxytocin or pitocin), to make your uterus contract just for a little while.
First, your nipples will be warmed up. Sometimes this makes your uterus start contracting for a little while. If that doesn't work, you could take a special medicine (either oxytocin or pitocin), to make your uterus contract just for a little while.
What happens if a test isn't normal?
If one of the tests isn't normal, your doctor may want to do other tests. Your doctor may also try to start your labor early (induce labor) if you might have a problem.
What will the doctor do to help my baby?
If your baby is very small when it's born, your doctor can give it oxygen through a nose tube, fluids through a tube in a vein and, sometimes, antibiotics.
What can I do to help my baby?
You can do five important things to help your baby grow big enough before it's born:
If you smoke—quit now. Cigarettes hurt the placenta, which is your baby's only way to get “food.” It's never too late to quit smoking. Babies gain one half of their weight in the last three months before being born.

If you drink alcohol—quit now. Even one drink a day makes it more likely that you will have a small baby. You could even have a baby with brain damage caused by the alcohol. This can happen in all months of pregnancy.
If you use illegal drugs—quit now. Almost all illegal drugs make babies too small to be strong and healthy. You may need your doctor's help to quit so you don't have withdrawal problems.
Eat a good diet. Ask your doctor to tell you the best foods to eat.
Keep all your appointments for doctor visits and tests.
When is a baby too small? Managing third-trimester fetal growth restriction | Your Pregnancy Matters
×
What can we help you find?Refine your search: Find a Doctor Search Conditions & Treatments Find a Location
Appointment New Patient Appointment
or Call214-645-8300
MedBlog
Your Pregnancy Matters
July 6, 2021
Your Pregnancy Matters
Patricia Santiago-Munoz, M. D. Obstetrics and Gynecology
D. Obstetrics and Gynecology
The third trimester is generally considered the home stretch of pregnancy. For most patients, it’s a less stressful time regarding fetal health, since the risk of miscarriage drops significantly after the first trimester and most patients have had the opportunity to learn about the health of their baby through second trimester ultrasounds and screening tests.
However, it’s not uncommon for mild to moderate growth disruptions to occur in the third trimester. Often, these healthy babies are simply small because their parents are small in stature or they were small babies themselves. But in approximately one-third of small babies, we find a potentially serious health problem called fetal growth restriction (FGR), which is associated with low birthweight, developmental problems, and stillbirth.
FGR refers to babies who are below the 10th percentile for estimated fetal weight, which means they’re smaller than approximately 90 percent of babies at the same gestational age. There are many potential causes of FGR, which generally fall under maternal, fetal, or placental complications.
Every patient who gets prenatal care is screened for FGR at every visit by taking regular belly measurements. We’re checking your fundal height – from the top of your uterus to your pubic bone. This number helps estimate the baby’s size and whether it is growing as expected.
After 20 weeks, the fundal height should correlate approximately with how long you’ve been pregnant. For example, it should measure approximately 20cm at 20 weeks’ gestation, 30cm at 30 weeks, etc. If your baby measures smaller than expected, we’ll confirm its size with an ultrasound.
“Generally, growth restriction is associated with either maternal risk factors, fetal anomalies, or a problem with the placenta – and sometimes a combination of these situations.
Dr. Santiago-MunozSome risk factors can be controlled, and some cannot.”
Is my baby small-but-healthy? Or could it be FGR?
By definition, babies diagnosed with FGR fall below the 10th percentile for estimated fetal weight and fundal height. Even if the baby is growing steadily, they may be diagnosed with FGR if they are below that benchmark.
But following these definitions FGR is sometimes over-diagnosed. Longstanding best practices data show that babies in the 3rd percentile or lower are more likely to have an FGR-related complication, and those above the 3rd percentile are more likely to be constitutionally small (based on non-health-related family history of smaller stature).
The UT Southwestern MFM team follows standard of care protocols for babies below the 10th percentile. We investigate every scenario to avoid taxing patients with undue stress related to overdiagnosis and over-management of FGR. Our goal is to understand:
Our goal is to understand:
- Why your baby is small,
- Whether your pregnancy is at risk of serious complications, and
- Whether early delivery or continued monitoring is the safest choice for you and your baby.
To answer these questions, we rely on two diagnostic tools: amniotic fluid measurement and Doppler ultrasound examination of the umbilical cord. These evaluations may help determine the origin of the FGR and guide further management.
What can cause FGR?
Generally, growth restriction is associated with maternal risk factors, fetal anomalies, or a problem with the placenta – and sometimes a combination of these situations. Some risk factors can be controlled, and some cannot.
Maternal risk factors
Some of the most common maternal risk factors for FGR include:
- Certain autoimmune conditions, such as lupus
- Certain viral infections, such as rubella or malaria
- Pregestational diabetes
- Having twins or more
- Hypertension (high blood pressure)
- Smoking, drinking alcohol, and substance use
While it is tough to quit smoking, it’s best to quit before becoming pregnant. However, quitting smoking during pregnancy is proven safe and beneficial for you and the baby. Your prenatal care provider can connect you with effective, judgment-free smoking cessation or substance use treatment designed specifically for pregnant patients.
However, quitting smoking during pregnancy is proven safe and beneficial for you and the baby. Your prenatal care provider can connect you with effective, judgment-free smoking cessation or substance use treatment designed specifically for pregnant patients.
Fetal anomalies
Heart conditions are among the most common fetal problems that cause FGR. Genetic abnormalities such as trisomy 21 (Down syndrome) also tend to result in babies that are smaller compared with the general population. Fetal anomalies are also more frequently associated with stillbirth.
Problems with the placenta
The placenta, like any organ, can develop improperly. Sometimes the umbilical cord is inserted in the wrong place on the placenta or only one umbilical artery forms develops in the cord instead of two, situations associated with reduced placental blood flow to an otherwise healthy baby.
In rare cases, we see a placental tumor called a chorioangioma, disrupting normal function. Placental issues are often the cause of late-onset growth complications.
Placental issues are often the cause of late-onset growth complications.
How is FGR diagnosed?
The diagnosis is based on ultrasound, and most centers use the 10th percentile cutoff to raise the alarm of possible fetal growth restriction. The next step is to have a discussion with the patient about her health history and her prior obstetrical history.
If a patient’s previous baby was less than 6 pounds at birth but was full-term and healthy, her current baby simply may be constitutionally small. If this is her first, or if previous babies were bigger, we will be more concerned about FGR. In either case, we will check the amniotic fluid and umbilical blood flow to help in the evaluation of placental function.
What happens next?
If the amniotic fluid and Doppler ultrasound are normal, we’ll watch the baby over the next few weeks and, if steady growth continues with no new concerns, that’s a good sign. The actual delivery timing will depend on how well the baby continues to grow and whether the amniotic fluid and the Doppler testing remain normal.
We generally recommend delivering the baby as close to the due date as possible to reduce the risk of needing long-term, specialized care after delivery. If the baby is:
- Between the 3rd and 10th percentiles for size, we try to get them to 38 weeks gestation.
- Smaller than the 3rd percentile, we try to get them to 37 weeks.
Often, our specialized team can safely get babies to 38 or 39 weeks before delivery, provided they have no other risk factors. Centers with less FGR management expertise tend to deliver earlier to avoid the risk of stillbirth. However, the earlier a baby arrives, the longer they typically stay in the neonatal intensive care unit (NICU).
Since the causes and severity of IUG can be so varied, your care plan will be customized based on your needs. Some patients are hospitalized for daily fetal heart rate monitoring. If you are hospitalized, we may recommend a complete course of steroids to help support fetal lung development before delivery.
If you end up needing early delivery, it does not mean an automatic cesarean section (C-section). Many babies are otherwise healthy except for being small, so it is likely safe to try vaginal delivery. Babies that are severely growth restricted or that have abnormal Doppler patterns may not do well with labor, so C-section may be indicated. A discussion with your doctor is always recommended.
What care will the baby need after birth?
Depending on how premature the baby is and the severity of its health problems, the newborn may need to stay in the NICU. Sometimes, these babies have trouble breastfeeding at first because they burn so many calories trying to latch and nurse.
Babies who are growth restricted often need many extra calories – more than breast milk or regular formula can provide. Our NICU specialists will work with nutritionists to supplement your baby’s diet with specialized, calorie-rich formula.
Many babies who start out being bottle-fed after growth restriction can learn to latch and breastfeed once they grow stronger. Patients who want to breastfeed are welcome to begin pumping to start building their milk supply.
Patients who want to breastfeed are welcome to begin pumping to start building their milk supply.
It can be scary to learn that your baby is smaller than expected. Sometimes, babies simply grow on their own developmental curve. With specialized care during pregnancy and after delivery, most babies diagnosed with FGR in the third trimester have good outcomes.
To visit with a pregnancy care provider, call 214-645-8300 or request an appointment online.
More in: Your Pregnancy Matters
Mental Health; Your Pregnancy Matters
- Robyn Horsager-Boehrer, M.
 D.
D.
October 11, 2022
Prevention; Your Pregnancy Matters
- Robyn Horsager-Boehrer, M.D.
October 4, 2022
Mental Health; Your Pregnancy Matters
- Meitra Doty, M.
 D.
D.
September 27, 2022
Your Pregnancy Matters
- Robyn Horsager-Boehrer, M.D.
September 20, 2022
Men's Health; Women's Health; Your Pregnancy Matters
- Yair Lotan, M.
 D.
D.
September 6, 2022
Your Pregnancy Matters
August 29, 2022
Your Pregnancy Matters
- Patricia Santiago-Munoz, M.D.
August 23, 2022
Mental Health; Your Pregnancy Matters
August 11, 2022
Your Pregnancy Matters
- Emily Adhikari, M.
 D.
D.
August 2, 2022
More Articles
© 2022 The University of Texas Southwestern Medical Center
Member of Southwestern Health Resources
Growth disorders in children. Child grows too slowly or too quickly
home > Symptoms of childhood diseases: section information > Growth disorders in children. The child is growing too slowly or too quickly.
A B C D E F G H I K L M N O P R S T U F X C H W Shch E Yu Ya
How tall a child will be depends on several factors: nutrition, heredity and health. Growth rates are determined by the genes of the parents, so children, tall or small for their age, do not suffer from growth disorders. If the baby was born large, it does not mean that when he grows up, he will certainly be tall.
To determine whether the development of the baby is normal or not, the pediatrician measures the length and weight, chest and head circumference at each scheduled examination. For the proper development and growth of the baby, he needs to eat well and fresh air, and healthy sleep. With a slight lag in growth or advance, it is important that the growth rate be maintained. (For example, children of the first year of life, the first 3 months grow at 3 cm / month, then slow down the growth rate).
DOCTOR'S CONSULTATION
Call your pediatrician if you notice:
- the child does not grow, loses weight, or, conversely, he has an excess of mass
WARNING!
Children with sufficient physical activity develop and grow faster than children who spend a lot of time at the computer or TV, they have a sedentary lifestyle and grow more slowly.
| ASK YOURSELF | POSSIBLE CAUSE | WHAT TO DO |
| The growth rate of a 1-2 year old baby has slowed down sharply. | Hypotrophy | Pediatrician consultation required to find out the reasons (this may be due to nutrition, the influence of certain diseases, etc.) |
| The child has a normal growth rate, but compared to his peers, he lags behind in growth | Constitutional features (small stature) | Make sure your baby gets all the nutrition he needs and he has a normal physical activity. Discuss your concerns with your pediatrician at your scheduled check-up |
| The child has a slow growth rate, sharply lags behind peers in growth. | Endocrine disorders (lack of growth hormone, insufficient thyroid function, etc.) | Go for a consultation with a pediatrician , if necessary, you need an examination and endocrinologist consultation |
| The child is normally built and healthy, but ahead of peers in growth | Constitutional features (large stature) | Make sure your baby gets all the nutrition he needs and he has a normal physical activity. |
| After the disease, the child began to grow worse | Growth retardation after illness | Make sure your little one is getting all the nutritious food they need and is having normal exercise and being active. If appetite or weight gain does not return after recovery after a few weeks, then Pediatric consultation required . |
| The child has a chronic disease (kidney or thyroid disease, gastrointestinal disease (colitis, etc.), or congenital chromosomal disease | Chronic disease interferes with normal growth | Consultation pediatrician must make sure that the child receives everything necessary for the underlying disease, that he has a balanced diet and sufficient physical activity |
| The child has increased mobility in the joints, arms and legs are long and thin. | Congenital disease (Morfan's Syndrome), accompanied by developmental disorders of the skeleton and sometimes the heart | Consultation of a pediatrician is needed , if necessary, he will refer to a specialist |
| Sudden rapid growth in a child of preschool or school age, coarse features. The head and lower jaw, hands look disproportionately large. | Excess growth hormone | Make an appointment with the pediatrician , he will refer you to an endocrinologist for examination if necessary. |
 The child has begun to lose weight and is not gaining enough weight
The child has begun to lose weight and is not gaining enough weight  Discuss with your child the features of his growth, if he is shy, this will help him stop slouching.
Discuss with your child the features of his growth, if he is shy, this will help him stop slouching.  The child himself is tall and thin, mental development is normal, and muscular development is insufficient
The child himself is tall and thin, mental development is normal, and muscular development is insufficient
FOR INFORMATION
Help with certain growth disorders
The rapid and disproportionate growth of a child under adolescence is very rarely associated with a disease of the pituitary gland, where growth hormone is produced. In these cases, the growth of long bones (limbs) and the lower jaw is especially accelerated.
In these cases, the growth of long bones (limbs) and the lower jaw is especially accelerated.
On the contrary, with a lack of growth hormone, the child may remain very small. If the diagnosis is confirmed, replacement treatment may be needed to bring the child to an acceptable adult height. Such treatment is prescribed only for true hormonal disorders. In other situations, growth hormone is usually not used.
Children may be stunted as a result of exposure to infection, alcohol or drugs in utero; due to chromosomal disease; premature birth. In most cases, the diagnosis is made during fetal development or immediately after childbirth, and the necessary treatment is prescribed.
Pediatric appointment prices:
| Inspection by the Pediatrician of the child to receive a certificate + certificate | 1950 |
| Departure of a pediatrician, Consultation at home (Moscow) | 5400 |
| Consultation of a pediatrician at home for the second child | 1950 900 |
Pediatricians:
Avzalova Darya Evgenievna
Pediatrician, neonatologist
Experience: 18 years
Reviews: 7
Call to house
Barzenok Tatyana Arsenievna
Chief physician, head of the pediatric department, pediatrician of the first category
Experience: 28 years
Reviews: 17
Make an appointment Call to house
Belousova Elena Sergeevna
Pediatrician, Nephrologist
Experience: 18 years
Reviews: 14
Make an appointment Call to house
Bykov Mikhail Viktorovich
Pediatrician of the highest category, specialist in ultrasound diagnostics, candidate of medical sciences
Experience: 25 years
Reviews: 3
Make an appointment Call to house
Kazakova Liliya Valentinovna
Pediatrician, neonatologist, head of breastfeeding consultants service
Experience: 28 years
Reviews: 31
Make an appointment Call to house
Sedova Maria Sergeevna
Pediatrician, allergist-immunologist
Experience: 20 years
Reviews: 30
Make an appointment Call to house
Sergienko Tatyana Yakovlevna
Pediatrician, pediatrician on duty at the pediatric hotline
Experience: 39 years
Reviews: 21
Make an appointment
A complete list of symptoms (more than 70) that require the help of a pediatrician can be found here.
The materials presented in the handbook are advisory in nature and do not replace a consultation with a doctor!
You can make an appointment or call a pediatrician at home by calling the Center in Moscow:
+7(495) 229-44-10, +7(495) 954-00-46
Grow, grow, baby - articles from the specialists of the clinic "Mother and Child"
Important dimensions
Indeed, height, body weight, and also the size of the circumference of the head and chest are the main indicators by which the physical development of the newborn is assessed child. Small or, conversely, large weight, the ratio of the circumference of the head and chest, the height of the baby are not just dry numbers, they can be used to suggest or exclude some diseases of the newborn. That is why, as soon as the baby is born, it is immediately measured, weighed and entered into the medical record. Then, in the first year of life, the height, weight, circumference of the chest and head of the child should be measured once a month, since the baby is growing very rapidly at this time.
Then, in the first year of life, the height, weight, circumference of the chest and head of the child should be measured once a month, since the baby is growing very rapidly at this time.
Term newborns are usually 46–56 cm tall. Boys are generally longer than girls, but if the parents are tall, a newborn girl may be significantly taller than the average newborn boy.
What happens to the growth of children in the first year of life? During this period, the child grows most intensively - by as much as 20–25 cm! In the future, such a significant increase in growth will no longer be.
After the first year, the growth rate decreases slightly: in the second year of life, the child grows by 8-12 cm, in the third - by 10 cm. After three years, it is considered normal if the child grows at least 4 cm per year.
It is known that the height of children increases unevenly, jumps. For example, there are seasonal and daily dynamics. Many parents notice that during the summer the child stretches more than at other times of the year. The first growth spurt usually occurs at the age of 4-5 years. The next usually falls on adolescence - the beginning of puberty. At this time, children grow very quickly - up to 8-10 cm per year and even more. Moreover, this happens in boys and girls, at different ages - girls “start” 1–2 years earlier, but then boys catch up with them and overtake them.
The first growth spurt usually occurs at the age of 4-5 years. The next usually falls on adolescence - the beginning of puberty. At this time, children grow very quickly - up to 8-10 cm per year and even more. Moreover, this happens in boys and girls, at different ages - girls “start” 1–2 years earlier, but then boys catch up with them and overtake them.
Interesting fact: those parts of the body that are farthest from the head grow faster (that is, the baby’s foot grows faster than the lower leg, and the lower leg, in turn, faster than the thigh), this is due to the age-related change in body proportions child.
What influences growth
How a child will gain weight and grow in length depends on hereditary data, on his nutrition and on the quality of life in general. If mom and dad are tall, then the height of their son or daughter will most likely also be the same. Moreover, boys usually grow up in the same way as their dad (or a relative in the male line - uncle, grandfather), and girls follow the scenario of the "female line" (mother, grandmother, aunt). So if the father of a child up to a certain age was the last or penultimate in physical education in the ranks of his peers, and as a teenager he grew sharply in one summer, then it is likely that his son will also have the same growth rates.
So if the father of a child up to a certain age was the last or penultimate in physical education in the ranks of his peers, and as a teenager he grew sharply in one summer, then it is likely that his son will also have the same growth rates.
There are formulas that can calculate your child's genetic height. However, , depending on some other factors, the height of the child may be more or less, differ from the calculated one up to 10 cm!
Girls = (father's height in centimeters + mother's height in centimeters)/2 - 6.5 cm. 5 see
And, of course, the quality of a child’s life is of great importance: if he grows up in good living conditions, often goes out into the fresh air (sunbaths are especially important), if they take care of him a lot, pay attention to health, then growth and an increase in weight will correspond to the norm for his age.
It has also been established that children grow up in their sleep. Growth hormone is released into the blood at night when the baby is fast asleep. Most of the hormone is produced between 22 and 24 hours, and only during deep sleep. So in order for the child to grow well, he must sleep at this particular time, and not just sleep - his sleep must already be deep. In addition, sleep should still be long enough: up to 12-14 years old, a child needs to sleep at least 10 hours, teenagers - at least 8.
Growth hormone is released into the blood at night when the baby is fast asleep. Most of the hormone is produced between 22 and 24 hours, and only during deep sleep. So in order for the child to grow well, he must sleep at this particular time, and not just sleep - his sleep must already be deep. In addition, sleep should still be long enough: up to 12-14 years old, a child needs to sleep at least 10 hours, teenagers - at least 8.
The child's growth must be closely monitored. There is such a condition as growth hormone deficiency (somatotropic insufficiency) - often this is a congenital disease. A child's pituitary gland produces very little growth hormone (GH) from birth. A child is born with normal height and weight, and then begins to grow poorly: at 2 years old, instead of the average 80–85 cm, he has a height of 78–80 cm. By the age of five, this lag is more and more noticeable, and every year the child is more and more lags behind peers. If such a child is not treated, then as an adult he will have a small stature: men are less than 140 cm, women are less than 130 cm. he is growing well.
he is growing well.
Record your baby's growth about once a year at the same time. If a child grows 4 cm per year after 4 years, this is normal, but if less, then this is a cause for concern.
When getting the results of measuring your baby, you need to remember that all children are different, and it is not necessary for every baby to reach the average height by a certain age. It is necessary to take into account growth at birth, as well as the rate of increase of these indicators: for example, a newborn with a height of 48 cm can differ significantly in anthropometric indicators from a child born with a height of 55 cm and a weight of 4000 g. And this is completely normal - it’s good when there are diversity!
The norm for a newborn is :
height: from 46 to 56 cm
Increase in height by months cm)
3-6 months: 2.5 cm monthly (about 7.5 cm total)
6-9 months: 1.5-2 cm monthly (4.5-6 cm total)
9 -12 mo: 1 cm per month (total 3 cm)
Average 1-year growth:
height 75 cm
. It turns out that at this time a child of any age should not just sleep, but see the tenth dream - and deep. Therefore, in order to grow well, up to 12-14 years old you need to sleep at least 10 hours, teenagers - at least 8
It turns out that at this time a child of any age should not just sleep, but see the tenth dream - and deep. Therefore, in order to grow well, up to 12-14 years old you need to sleep at least 10 hours, teenagers - at least 8
Height may be affected by health problems. For example, chronic diseases of the respiratory system, heart and blood vessels, gastrointestinal tract, hormonal disorders. Regular intake of drugs containing glucocorticosteroid hormones (for example, to relieve asthma attacks) also slows down growth.
How to influence the growth of a child
- In order for a child to grow, the body needs amino acids, which can only be obtained from complete protein. 60% of the protein food should be dairy products, eggs, fish, poultry, meat - in general, animal products. They should not be very fatty, as fat inhibits the production of growth hormone.
- Carbohydrates provide energy for growth, but they must be obtained from cereals and grain dishes.
 Sweets, which do not contain fiber, slow down the production of growth hormone. Uncrushed cereals (buckwheat, millet, pearl barley, etc.), on the contrary, increase the synthesis of growth hormone.
Sweets, which do not contain fiber, slow down the production of growth hormone. Uncrushed cereals (buckwheat, millet, pearl barley, etc.), on the contrary, increase the synthesis of growth hormone. - Vitamins and minerals are also important for growth. Especially vitamin D, the lack of which develops rickets.
- Don't forget calcium and iodine. Calcium increases the volume and strength of bones, iodine is part of the thyroid hormones, which also affect growth.
- The general routine of the day is also important: the child should not be overloaded both physically and psychologically. He should walk a lot and sleep well.
Attention! Prices for services in different clinics may vary. To clarify the current cost, select a clinic
All areasSpecialist consultations (children)Massage/manual therapy for childrenTherapeutic research
01.