Baby poop one month old
Normal Baby Poop Color and How Often Babies Poop
Written by Stephanie Watson
Reviewed by Dan Brennan, MD on February 22, 2022
Week 4
featureIf it seems like you're constantly changing diapers, you're not imagining it. By the end of this year, you'll have changed 2,300 diapers! Parents of twins -- double that number. Triplets ... you get the picture.
So you're not surprised when you open your baby's diaper, here's what to expect.
Breastfed babies:
- Make yellow poop that's speckled with little seeds--like mustard
- Poop one or more times a day, usually after they eat
Formula-fed babies:
- Have tan, yellow, or greenish poop
- Poop once a day, sometimes more often
What's normal:
- Poop can come in a rainbow of colors, changing to yellow, green, or brown.
- Some babies don't poop for a day or two -- even a week. You don't need to worry as long as your baby is still eating and gaining weight.
What's not normal (time to call your doctor):
- Poop that is filled with mucus, water, or blood could be a sign of an allergy or infection.
- Solid, hard poop means your baby is probably constipated.
Your Baby's Development This Week
You've seen a real transformation in the last month. Your little one has changed from a tiny newborn into a more active -- and interactive -- baby with a budding personality.
As they hit the big 1-month mark, here are just some of the new things they are able to do:
- Move their head from side to side while lying on their tummy
- Turn their head toward the sound of your voice
- Coordinate their movements well enough to bring their hand to their mouth
- Focus on a toy that's 12 inches away, although their eyes may still cross and that's OK
- Recognize the smell of their mother's milk
Week 4 Tips
tips- If your baby is constipated, try mixing a teaspoon of prune juice with breast milk or formula.

- Save the baby wipes for messy poop clean-ups. A damp washcloth is good enough for cleaning after a wet diaper.
- Your baby's neck muscles are getting stronger, but they still can't hold up their head on their own. Don't forget to support their neck whenever you carry them.
- Do not hold your baby while you are eating or drinking anything hot.
- When your baby seems ill, take their temperature with a rectal thermometer -- it's most accurate at this age.
- A rectal temperature at or above 100.4 degrees Fahrenheit is a sign your baby could be sick. Call the pediatrician right away.
- Your baby's one-month birthday is time for a well-baby visit. At the appointment, the doctor will measure your baby, check their health, discuss vaccines, ask how they have been eating and sleeping, and give some guidance for developmental goals.
- You've been focused on your baby for a month now. Don't forget about your partner. Get a babysittter so you can get some time alone with your partner.

Today on Grow
<blank>Recommended for You
Doctor-approved information to keep you and your family healthy and happy.
- Pregnancy & Baby Bulletin
- Parenting & Children's Health
Baby Poop: Colors, Types, and What They Mean
Baby poop is probably something you were expecting to deal with, but did anyone tell you how varied the contents of your little one’s diapers could be? Runny or firm, black, green, or yellow—even mucus in your baby’s poop can be part of the adventure. Those diaper changes are, of course, a regular part of your daily routine as a parent, but they can also help you keep an eye on your baby’s well-being. Learn what the color, consistency, and frequency of baby poop can tell you about your baby’s health and development.
Your Baby’s Poop — What’s Normal?
You might be wondering what healthy baby poop should look like. It’s a fair question, because the color and consistency of your baby’s poop changes over time depending on various things, especially what your baby is eating.
Here’s a rough guide to what you’re likely to find in your little one’s diapers over the first few days, weeks, and months after your baby is born.
Meconium
Your baby’s first few diapers will likely contain a gooey, dark-green, tar-like substance, with hardly any smell. This is called meconium.
This is a distinct type of poop made up of things like mucus, skin cells, lanugo hairs, and other particles your baby swallowed, along with the amniotic fluid, while still in the womb.
It takes a few days for your little one to pass all the meconium out of their system, but as this happens, they’ll start to have regular baby poops. The color will shift from being almost black to a yellowy green and there may be less mucus present. Speak to your baby’s healthcare provider if your baby’s first bowel movement doesn’t happen within the first 24 hours after birth.
Speak to your baby’s healthcare provider if your baby’s first bowel movement doesn’t happen within the first 24 hours after birth.
Regular Baby Poop
Once the meconium is out of your baby’s system, their regular poop can vary a lot, depending on how they’re being fed. Here is what you’ll probably find in your little one’s diapers:
Breastfed babies. If you’re breastfeeding your baby, their stools in the first few months may look a little like Dijon mustard, with a slightly runny consistency, and possibly with whiteish, seed-like fat particles. A little bit of mucus in baby poop is normal, too. The color of your baby’s poop may also change depending on what you’re eating. For example, if you eat green vegetables like spinach, you might see a green tint in the contents of your little one’s diapers.
Formula-fed babies. If your baby is getting their nourishment from formula, their poop won’t usually be as runny as that of a breastfed baby.
 It will have a more paste-like consistency (although it shouldn’t be firmer than peanut butter) and a darker yellow or tan color.
It will have a more paste-like consistency (although it shouldn’t be firmer than peanut butter) and a darker yellow or tan color.Babies in the weaning stage. When you start introducing solid foods to your little one, which is recommended from around 6 months, you’ll start to see (and smell!) some major changes in the contents of your baby’s poopy diapers. Their stools will get firmer, and the color will vary more widely, too.
If your child is eating finger foods, you might see undigested bits of food like the skins of peas or tomatoes. This is because your little one’s digestive system is still getting the hang of processing all these new foods. The weaning period is also when your little one’s poop will start to smell stronger, due to the extra fats and sugars in their diet.
What the Colors of Baby Poop May Mean
You might be surprised by a change in the color of your baby’s poop, which can range from the mustardy hues of breast-milk poop and the yellow-tan of formula-fed baby poop to various other shades of yellow, brown, and even green. You might also find mucus in baby poop, which can create a translucent or milky coloring.
You might also find mucus in baby poop, which can create a translucent or milky coloring.
Green Baby Poop
Green poop can be alarming the first time you see it, but it’s usually harmless. All sorts of things can cause it, from certain medicines (taken by your baby, or by you if you’re breastfeeding) to green foods eaten by your baby directly or passed on through your breast milk. Sometimes, what you see is simply a product of your little one’s normal digestion.
Generally, all the earth tones (yellow through green and brown) are OK, but if you ever need reassurance about the color of your baby’s poop, don’t be shy about reaching out to your baby’s healthcare provider for advice.
Warning Colors
Certain colors of stool can be a sign of a possible health issue. Always check in with your baby’s healthcare provider if your baby’s poop is any of the following colors:
Red. Traces of red can be due to blood in your baby’s poop, so it’s important for your baby’s healthcare provider to investigate what might be causing it.
 Keep in mind, though, that there are plenty of harmless reasons for red poop. In a newborn baby, a little blood may have been swallowed during delivery. If you’re breastfeeding, it might be that your nipples are bleeding, and the blood is mingling with your breast milk. If your little one is eating solids, it could be a certain food, such as beets, coloring their poop red.
Keep in mind, though, that there are plenty of harmless reasons for red poop. In a newborn baby, a little blood may have been swallowed during delivery. If you’re breastfeeding, it might be that your nipples are bleeding, and the blood is mingling with your breast milk. If your little one is eating solids, it could be a certain food, such as beets, coloring their poop red.Black. A black stool could, in some cases, be caused by blood, which may turn from red to black inside the intestines over time. It's important to know that very dark green poop can sometimes appear black. Green baby poop—even a dark shade of the color—is usually nothing to worry about. Meconium can also look black, and this isn’t a problem.
White or gray. Very pale white or clay-colored stools are very rare, but if you see poop this color in your baby’s diaper, call your baby’s healthcare provider, as it could be a sign of a liver condition that needs treatment.
Mucus in Baby Poop
As mentioned, mucus in baby poop is most often harmless and normal. Meconium almost always has it, and it’s not abnormal to find small amounts of mucus in your baby’s poop as they grow older and eat more varied foods. Mucus in baby poop is typically translucent or slightly milky in color.
Meconium almost always has it, and it’s not abnormal to find small amounts of mucus in your baby’s poop as they grow older and eat more varied foods. Mucus in baby poop is typically translucent or slightly milky in color.
However, if mucus in baby poop is accompanied by other symptoms, this could be an indication of an infection or digestive issues. Symptoms to look out for include blood in the poop, diarrhea, high fever, loss of appetite, vomiting, and weakness. If you notice any of these symptoms, especially alongside mucus in your baby’s poop, contact your baby’s healthcare provider.
Baby Poop Color Chart
To help you visualize the array of baby poop colors, here is a handy chart:
How Often Will Your Baby Poop?
The frequency of your baby’s poops will change as your little one grows and their digestive system develops, but it’s also affected by the feeding method that you use.
If You’re Breastfeeding
If your baby is breastfed, they’re likely to poop more frequently than their formula-fed peers. As a rule of thumb, after the first few days, you might see anything between 2 and 5 bowel movements a day, up until your little one is around 6 weeks old.
Keep in mind that after 3 to 6 weeks of age, your breastfed baby might sometimes go several days between bowel movements. This is because your baby’s digestive system is able to process breast milk very efficiently, leaving very little solid waste.
After 6 weeks, your baby may have fewer daily poops. One reason may be that, by this time, your breast milk usually no longer contains colostrum, which can act as a laxative.
If You’re Formula Feeding
If your little one is getting all or most of their daily nutrition through formula feeding, after the first few days they may start filling their diaper at least once a day, but it’s not out of the ordinary for them to sometimes go a day or two without a bowel movement. This is OK, provided their stools are soft when they do materialize.
This is OK, provided their stools are soft when they do materialize.
If you’re ever concerned about how many poops your little one is passing, consult your baby’s healthcare provider.
Can Your Baby Make Too Much Poop?
The amount of poop your baby makes each time can vary. As long as their weight gain is on track, and the stools are soft, all is probably fine.
If your baby’s poop seems watery or is filled with mucus, and they are pooping much more frequently than usual or has other symptoms, like a high temperature (100.4 degrees Fahrenheit or above), this could be diarrhea.
See your baby’s healthcare provider if you think your little one might have diarrhea, especially if they’re under 3 months.
It’s worth knowing that newborns and younger babies are more likely to produce lots of little poops one after the other. If you notice that your baby has just had a bowel movement, you might be able to save yourself an extra diaper change by waiting just a little longer in case there’s more to come.
Each one of those diaper changes could be earning you Pampers Cash that you can use toward gifts, coupons, and discounts. Download the Pampers Club app to get started right now!
When There’s No Poop — Constipation
With all the variation in how often your baby poops, you may sometimes wonder how you can tell if your little one is constipated.
Constipation in babies is more common after the introduction of solids, but it can occur in younger babies, too. Here are some typical signs of constipation:
In a newborn baby. Firm stools that come less than once a day.
In an older baby or toddler. Hard, compact stools that only come every three or four days.
In a baby or child of any age. Large, hard, and dry stools that are painful to pass; blood on or in your child’s stools; you child strains for more than 10 minutes without passing any stool at all.
What Can You Do About Constipation?
If you think your baby is constipated, see their healthcare provider for advice. Don’t give your baby any medication, including a laxative, unless it’s specifically prescribed by their provider.
Don’t give your baby any medication, including a laxative, unless it’s specifically prescribed by their provider.
Call their provider immediately if your little one doesn’t get better or has other symptoms like:
vomiting
fever
lethargy
loss of appetite
blood in the stool.
How to Tell if Your Baby Has Pooped
Your baby’s poop may not always smell much, especially in the first few weeks, so how can you tell when a diaper change is needed?
One tell-tale sign is straining: Passing a stool is hard work for small babies. You might notice your little one getting red in the face with the effort of pushing out that poop.
You’ll soon get to know your baby’s facial expression when they’re having a bowel movement, or—when they’re old enough to stand and walk—the squatting pose that they adopt when they need to go.
Use our handy Diaper Size and Weight Chart to make sure your baby's diapers always fit properly.
The Bottom Line
You might not have realized until now just how much there is to know about your baby’s poop, but don’t worry: There’s no need to go over every single dirty diaper with a magnifying glass! Once you get used to your little one’s bowel movement patterns, and the usual color and texture of their poops, you’ll probably notice any changes quickly.
Just keep an eye on color and consistency and together with your baby’s healthcare provider, you can take any steps needed to get things back to normal.
Fatty stools in a child
Fatty stools are associated with impaired absorption of fats, and can occur with both diarrhea and constipation.
Causes
Food fats (lipids) are digested in the intestine by the action of the enzyme lipase, which is produced mainly in the pancreas. Sometimes there is congenital lipase deficiency , but in newborns this deficiency is more often temporary, associated with immaturity of the pancreas . Due to this immaturity, the production of enzymes, including lipase, is insufficient. Especially often this deficiency occurs in premature babies and children with intrauterine growth retardation.
Due to this immaturity, the production of enzymes, including lipase, is insufficient. Especially often this deficiency occurs in premature babies and children with intrauterine growth retardation.
Meanwhile, nature has foreseen this situation and provided babies with reliable insurance: breast milk contains lipase, which facilitates the digestion of fats. However, if the infant is bottle-fed, pancreatic lipase immaturity may be clinically evident.
In addition to lipase, a certain composition of bile is necessary for the digestion of fats, therefore, disorders of fat metabolism can also be observed in children with diseases of the liver and biliary tract . Such diseases are characterized not only by fatty, but also lighter than usual stools.
Diagnosis and treatment
If a child has fatty stools, which is accompanied by constipation or diarrhea, the pediatrician or pediatric gastroenterologist first rule out a violation of the digestion of fats. For this, a coprological study is prescribed (i.e., a study of feces), the condition of the liver and pancreas is checked (ultrasound, biochemical and immunological studies).
For this, a coprological study is prescribed (i.e., a study of feces), the condition of the liver and pancreas is checked (ultrasound, biochemical and immunological studies).
In difficult cases, the child is examined in a hospital. Children are selected diet and drugs containing pancreatic enzymes and bile acids. Treatment is prescribed only by a doctor, since the composition and effectiveness of enzyme preparations are different, and there are certain indications and contraindications for them.
Celiac disease
One of the most serious causes of fatty stools is celiac disease.
Celiac disease is a genetic disorder in which an enzyme deficiency interferes with the absorption of a substance called gluten. Gluten is found in many grains and is found in many foods. With the use of such products in the body of a patient with celiac disease, toxic products of incomplete breakdown of gluten accumulate, which damage the mucosa of the small intestine. This damage is accompanied by a violation of the absorption of proteins, fats and carbohydrates, and the development of the so-called malabsorption syndrome.
As a rule, symptoms of celiac disease first appear in children some time after the introduction of cereals (semolina, oatmeal and other cereals) into the diet. This causes diarrhea, fatty stools. Such children do not grow well and put on weight, become capricious and irritable. Over time, symptoms of rickets may appear.
Treatment of celiac disease
Basic treatment of celiac disease - a diet with the complete elimination of products containing gluten. All cereals should be excluded from the diet, except for rice, buckwheat, corn, as well as foods that may contain them, including sausages, sausages, and some canned food. Usually the diet is supplemented with the exclusion of lactose and allergens.
Soy formulas or formulas based on casein hydrolyzate may be given to infants under 1 year of age.
In case of celiac disease, adherence to the diet should be lifelong, since a departure from it is not only fraught with a possible exacerbation of the process, but significantly increases the risk of developing malignant neoplasms, including intestinal lymphomas.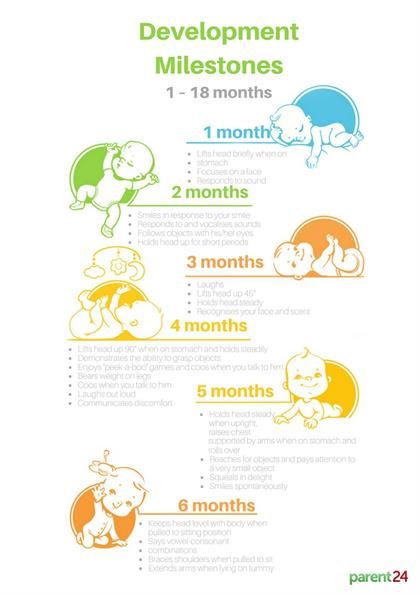
Strict adherence to the diet with timely initiation of treatment helps to ensure the normal development of the child. In the case of strict adherence to the diet and adequate additional therapy, children with celiac disease do not lag behind their peers either in physical or mental development.
References
- Oluwagbemigun K., O'Donovan AN., Berding K., Lyons K., Alexy U., Schmid M., Clarke G., Stanton C., Cryan J., Nöthlings U. Long-term dietary intake from infancy to late adolescence is associated with gut microbiota composition in young adulthood. // Am J Clin Nutr - 2021 - Vol113 - N3 - p.647-656; PMID:33471048
- Ye Q., Wang H., Xia X., Zhou C., Liu Z., Xia ZE., Zhang Z., Zhao Y., Yehenala J., Wang S., Zhou G., Hu K., Wu B., Wu CT., Wang S., He Y. Safety and efficacy assessment of allogeneic human dental pulp stem cells to treat patients with severe COVID-19: structured summary of a study protocol for a randomized controlled trial (Phase I / II).
 // Trials - 2020 - Vol21 - N1 - p.520; PMID:32532356
// Trials - 2020 - Vol21 - N1 - p.520; PMID:32532356 - Stallings VA., Tindall AM., Mascarenhas MR., Maqbool A., Schall JI. Improved residual fat malabsorption and growth in children with cystic fibrosis treated with a novel oral structured lipid supplement: A randomized controlled trial. // PLoS One - 2020 - Vol15 - N5 - p.e0232685; PMID:32384122
- Turkalj M., Matišić V., Šimić A., Juginović A., Erceg D., Tješić Drinković D., Höppner W., Primorac D. Cystic fibrosis presentation in del. F508 and p. Tyr109Glyfs compound heterozygote CFTR state: a case report. // Croat Med J - 2019 - Vol60 - N3 - p.246-249; PMID:31187952
- Stallings VA., Sainath N., Oberle M., Bertolaso C., Schall JI. Energy Balance and Mechanisms of Weight Gain with Ivacaftor Treatment of Cystic Fibrosis Gating Mutations. // J Pediatr - 2018 - Vol201 - NNULL - p.229-237.e4; PMID:30029855
- Ikuse T., Kudo T., Arai K., Fujii Y., Ida S., Ishii T., Mushiake S., Nagata K., Tamai H., Toki A.
 , Tomomasa T., Ushijima K., Yanagi T., Yonekura T., Taguchi T., Shimizu T. Shwachman-Diamond syndrome: Nationwide survey and systematic review in Japan. // Pediatr Int - 2018 - Vol60 - N8 - p.719-726; PMID:29804317
, Tomomasa T., Ushijima K., Yanagi T., Yonekura T., Taguchi T., Shimizu T. Shwachman-Diamond syndrome: Nationwide survey and systematic review in Japan. // Pediatr Int - 2018 - Vol60 - N8 - p.719-726; PMID:29804317 - Patni N., Quittner C., Garg A. Orlistat Therapy for Children With Type 1 Hyperlipoproteinemia: A Randomized Clinical Trial. // J Clin Endocrinol Metab - 2018 - Vol103 - N6 - p.2403-2407; PMID:29659879
- Zavala GA., Garcia OP., Camacho M., Ronquillo D., Campos-Ponce M., Doak C., Polman K., Rosado JL. Intestinal parasites: Associations with intestinal and systemic inflammation. // Parasite Immunol - 2018 - Vol40 - N4 - p.e12518; PMID:29364525
- Gianni ML., Roggero P., Baudry C., Fressange-Mazda C., le Ruyet P., Mosca F. No effect of adding dairy lipids or long chain polyunsaturated fatty acids on formula tolerance and growth in full term infants: a randomized controlled trial. // BMC Pediatr - 2018 - Vol18 - N1 - p.10; PMID:29357820
- Song XX.
 , Fang DH., Quan YQ., Feng DJ. The pathogenic detection for 126 children with diarrhea and drug sensitivity tests. // Eur Rev Med Pharmacol Sci - 2017 - Vol21 - N4 Suppl - p.95-99; PMID:29165756
, Fang DH., Quan YQ., Feng DJ. The pathogenic detection for 126 children with diarrhea and drug sensitivity tests. // Eur Rev Med Pharmacol Sci - 2017 - Vol21 - N4 Suppl - p.95-99; PMID:29165756
symptoms, diagnosis, treatment and prevention
What is colic?
The term "colic" refers to a disorder of the child's gastrointestinal tract, accompanied by frequent, intense and prolonged crying or pronounced anxiety of the baby.
Most often, colic occurs in infants 3-4 months old, but can also occur from 2 weeks of age.
Colic affects 10-40% of children worldwide, regardless of gender.
Causes of colic in a child
The exact cause of colic is unknown. From a parent's point of view, there may be no potential cause for concern. According to modern medical data, some internal and external factors can provoke colic. Let's consider them in more detail.
Underdevelopment of the digestive system
The digestive system of newborns is not always able to quickly and painlessly adapt to a new way of eating immediately after birth. Until recently, the child was fed through the umbilical cord, and now he must eat milk. Not surprisingly, in the first months, the muscle fibers of the gastrointestinal tract are forced to adapt to feeding through the mouth, and their spasms (excessively strong contractions) can cause colic in the meantime. This theory is also supported by a greater tendency to develop colic in preterm infants.
Until recently, the child was fed through the umbilical cord, and now he must eat milk. Not surprisingly, in the first months, the muscle fibers of the gastrointestinal tract are forced to adapt to feeding through the mouth, and their spasms (excessively strong contractions) can cause colic in the meantime. This theory is also supported by a greater tendency to develop colic in preterm infants.
Also at an early age, weakness of the sphincter located at the junction of the esophagus to the stomach can occur. Because of this, in the supine position and immediately after feeding, reflux occurs - the reverse flow of gastric contents into the esophagus. This provokes discomfort and heartburn, which is manifested by the anxiety of the baby.
Dysbacteriosis
An important component of normal digestion is the intestinal microflora. Immediately after birth, the intestines of the child are sterile, that is, they are not inhabited by any bacteria. Together with the first contacts with the outside world and feeding, the gastrointestinal tract of the child is gradually filled with the necessary microorganisms.
In the first months of a child's life, the composition of intestinal bacteria changes greatly, which can provoke digestive disorders and the development of colic.
Sensitivity to external influences
In infancy, any external influence can affect the condition of the infant. Therefore, factors such as cold or hot air, a wet diaper, loud sound or too bright light can provoke an overly active response of the nervous system, including colic.
Intolerance to mother's and cow's milk
Lactase deficiency is relatively rare in children - a deficiency of the lactase enzyme necessary for the breakdown and digestion of mother's milk. An allergy to casein, a cow's milk protein, may also be a likely cause.
In both observations, the process of digestion becomes uncomfortable and painful, which is accompanied by the appearance of colic in the child.
Important! In breastfeeding mothers who experience constant stress or emotional stress, the composition of breast milk may change under the influence of hormonal fluctuations.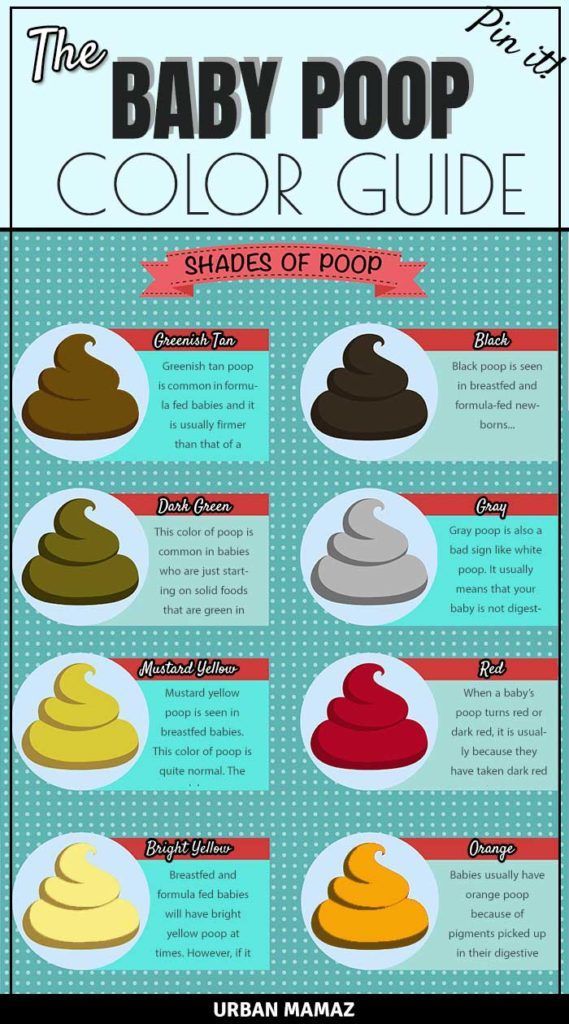 This is considered one of the potential causes of colic.
This is considered one of the potential causes of colic.
Infantile migraine
Infantile migraine is believed to be the cause of colic. This variant of migraine is caused by the adaptation of the central nervous system to an unfamiliar external world - sounds, images and objects. It can also be due to increased intracranial pressure, for example, after suffering birth injuries or with various encephalopathies.
Symptoms of colic in a child
Increased anxiety and crying are common in children in the first months after birth and for other reasons. Therefore, the criterion for colic is the state of crying for more than 3 hours a day, more than 3 days a week for more than 3 weeks in apparently healthy, not hungry and comfortable children.
Clinical features that can potentially help distinguish colic from other causes of crying include:
- Intense crying that may sound more like a cry or a reaction to pain.
- The appearance of crying for no apparent reason: hunger or the need to change a diaper.

- Great restlessness which persists even after the crying has ceased.
- Onset of symptoms predominantly in the evening.
- Concomitant discoloration of the skin of the face, such as redness of the face or paleness of the skin around the mouth.
- The appearance of muscle tension, manifested by pulling the legs to the stomach, pressing the arms to the body, clenching fists, arching the back or tension of the abdominal muscles.
- Disappearance or amelioration of symptoms after defecation or flatulence.
How to relieve colic at home?
Self-combating colic at home can be divided into two main stages: the elimination of direct violations of the gastrointestinal tract and the prevention of their recurrence.
The following actions are recommended during the onset of colic in a child:
Step 1. Light massage
Body contact helps to normalize the functioning of the muscles of the gastrointestinal tract. During the appearance of colic, it will be useful to perform a light massage of the baby's abdomen in a circular motion in a clockwise direction. Hands should be warm.
Step 2. Bicycle exercise
The classic bicycle exercise can also help to pass intestinal contents. To do this, you need to take the child by the feet and perform circular movements in such a way that he is pedaling.
Step 3. Heat on the baby's tummy
Heat can help with intestinal dysmotility and colic in a baby. To do this, you can use a bottle of liquid that is warm to the touch or a special heating pad.
Feeding your baby the right way
For formula-fed babies who are prone to colic, it is recommended to use milk formulas containing partially digested milk proteins. Most often they have a mark on the package like “tender”.
Important! To improve digestion, prebiotics (galactooligosaccharides for the development of intestinal microflora) are added to some milk formulas. Other mixtures are enriched with probiotics (Bifidobacterium lactis and other live bacteria).
When breastfeeding, it is important to pay attention to the correct attachment of the baby. His mouth should completely capture the areola of the nipple. When formula feeding, hold the bottle so that the milk or formula completely fills the nipple. This will prevent swallowing air, which also provokes colic.
Also, problems with swallowing air during feeding can be compensated by encouraging the baby to burp. To do this, you need to keep the baby for some time (about 15-20 minutes) after feeding in an upright position on the chest, tilting his head over his shoulder.
Also during feeding, avoid sudden movements, loud noises and flashes of light, which can distract the baby from the feeding process.
In addition to correct feeding, it is important to monitor the amount of milk or formula eaten. Overeating puts extra stress on the baby's digestive system, causing colic. One of the signs of overeating is frequent spitting up.
Nutrition of a nursing mother should also be balanced. It is recommended to give up foods that cause flatulence (legumes, onions, garlic, etc.), spicy, fried and fatty foods, as well as potential allergens - chocolate, citrus fruits, honey, eggs, seafood.
When to see a doctor?
The reason for visiting a doctor is the ineffectiveness of all the previously given recommendations and the persistence or increase in the symptoms of colic in a child. Children's crying can also be caused by other diseases or functional disorders, which can only be identified by a doctor with the help of additional studies.
You should also seek medical attention if your child has the following changes or symptoms:
- Vomiting blood or partially digested food.
- Loss of appetite.
- Delayed weight gain and growth.
- Respiratory failure, shortness of breath.
Treatment of colic in children
Colic resolves on its own, usually by 4 months of age. Since the exact cause of their development has not been established, there is also no clear treatment. The actions that are recommended in such cases are aimed at alleviating the condition of the child and preventing possible undesirable consequences.
Priority points in the treatment of colic in children are the observance of the daily regimen and nutrition of both the child and the mother.
If you need artificial feeding, in addition to choosing the appropriate mixtures, it is important to timely introduce into the diet special fermented milk products that contain prebiotics and probiotics.
Drug treatment of colic is represented by drugs that reduce gas formation in the intestines (for example, simethicone) or drugs that stimulate digestion and have antispasmodic properties (fennel extract and oil). Enzymes can also be used - creon, pancreatin, strictly according to the doctor's prescription.
Conclusion
Colic is often regarded as a temporary, normal condition that the baby will outgrow.