Abdominal wall separation
Abdominal separation (diastasis recti) | Pregnancy Birth and Baby
Abdominal separation (diastasis recti) | Pregnancy Birth and Baby beginning of content4-minute read
Listen
What is abdominal separation?
Some women find their stomach muscles weaken and separate during and after pregnancy. This is known as abdominal separation, ‘diastasis recti’ or ‘recti divarication’. It is a common condition and often gets better in the first 8 weeks after having your baby.
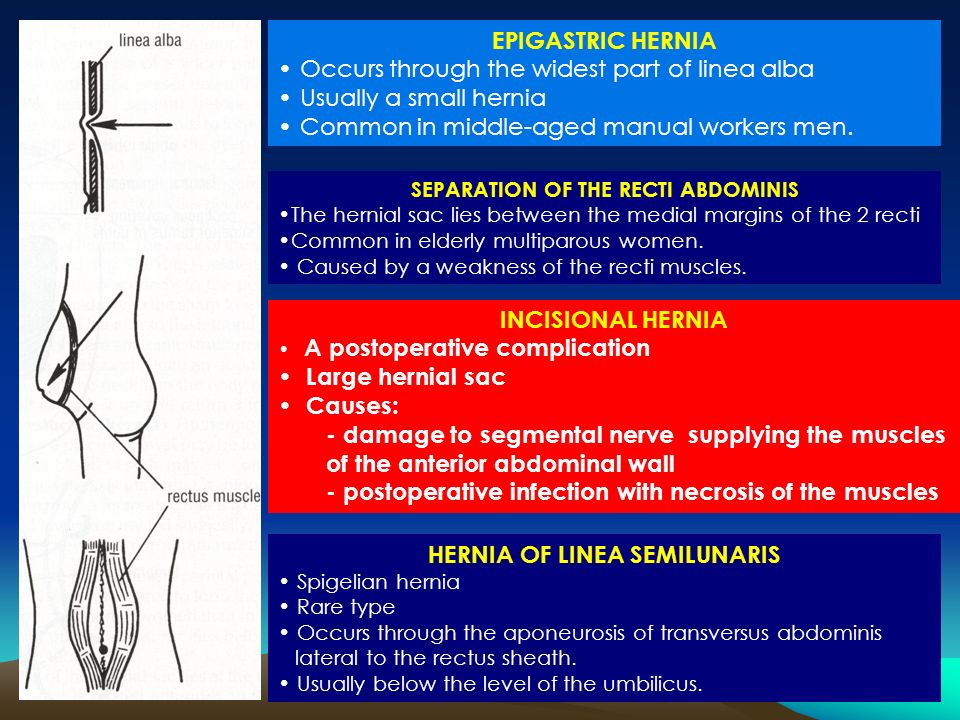
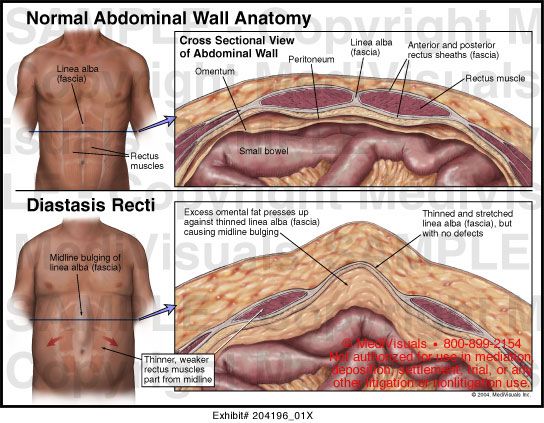
Abdominal separation occurs when the growing uterus causes the 2 long, parallel muscles of your stomach to separate from each other. These muscles run from your chest to your pelvis, just under the skin, down the middle of your belly.
Abdominal separation is partly due to the pressure of your growing baby, and partly due to the hormonal changes that take place during pregnancy. It usually starts in the second half of pregnancy.
Abdominal separation is more common in women who have had more than 1 child, are aged over 35 or who are having twins or triplets (or more). It can also occur in a small-statured woman who is having a larger-than-average baby.
It is sometimes known as ‘DRAM’ (diastasis of rectus abdominis muscle).
What are the signs and symptoms of abdominal separation?
If you have abdominal separation after the birth of your baby, you may be able to see a gap between the two bands of abdominal muscles. You can see this gap more clearly if you lie flat on your back and lift your head up.
You might also notice a physical canoe-shaped bulge in the middle of your stomach, especially when your abdominal muscles are active.
Some women with abdominal separation also get lower back pain, as the separation prevents the stomach muscles from supporting the back.
How is abdominal separation diagnosed?
Your GP, midwife or physiotherapist can check how big your abdominal separation is by measuring it with their fingers or a measuring tape, or by doing an ultrasound.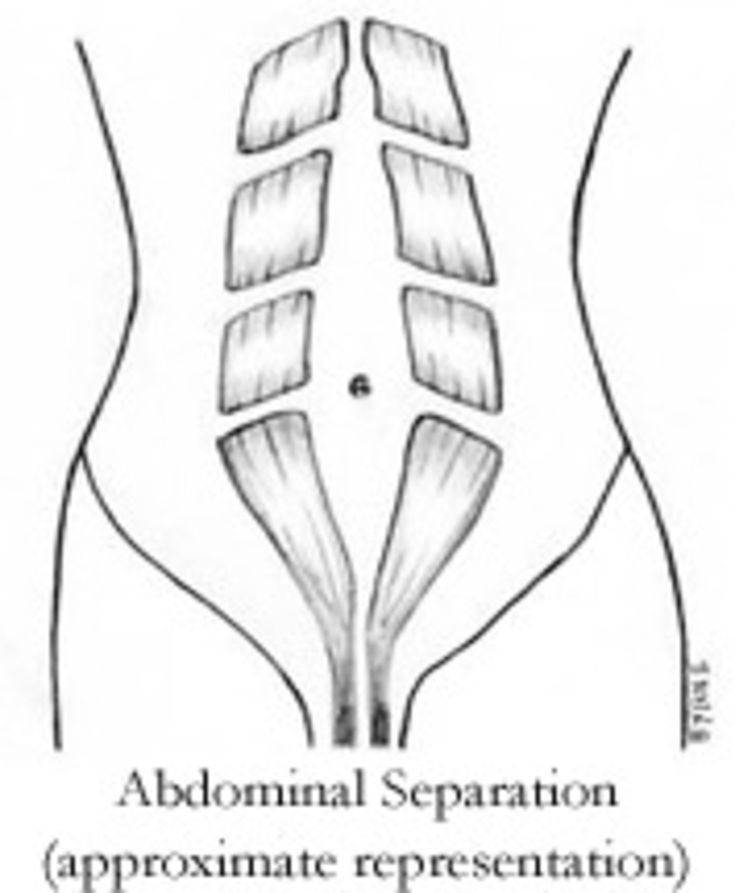
Does abdominal separation go away by itself?
Abdominal separation usually goes away after the birth of the baby. That said, up to 1 in 3 women still report problems with abdominal separation 12 months after the birth.
How can abdominal separation be prevented during pregnancy?
Strengthening your core muscles before you get pregnant or in the early stages of pregnancy might help prevent abdominal separation.
It’s best to avoid putting excess strain on your abdominal muscles while pregnant. Avoid sit-ups or planks. Try to avoid constipation and if you have a cough, get it treated.
How is abdominal separation after the birth treated?
It’s important to stop the separation from getting worse. Try these tips:
- Avoid lifting anything heavier than your baby.
- Roll onto your side when getting out of bed or sitting up.
- Choose gentle exercises (rather than intense ones) that strengthen the deeper stomach muscles.

- Skip activities and movements that can make abdominal separation worse, such as sit-ups (crunches), oblique curls and some yoga poses (ask your GP, midwife or physiotherapist for advice).
You can also wear a supportive brace or compression underwear to help support your back and resolve the muscle separation.
There is a good chance that with time and care, the muscles will come back together. If that doesn’t work as well as you’d like, surgery after you’ve had your baby is an option.
Surgery often involves using stitches to repair the abdominal wall and reduce the gap between the muscles. This can improve quality of life and muscle strength, especially when separation is wider than 3cm.
Where to get help
If you notice anything unusual about your stomach muscles or experience any symptoms, see your GP, midwife or physiotherapist. You can find a physiotherapist near you using the healthdirect service finder.
You can also contact Pregnancy, Birth and Baby on 1800 882 436 to speak with a maternal child health nurse.
Sources:
Royal Women’s Hospital (Abdominal muscle separation), Surgical Endoscopy (The general surgeon’s perspective of rectus diastasis), King Edward Memorial Hospital (Physiotherapy after childbirth), Pelvic Floor First (Re-thinking abdominal training in pregnant and postnatal women)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: September 2020
Back To Top
Related pages
- Yoga and Pilates during pregnancy
- Looking after your body after having a baby
- Pelvic floor exercises
- Safe return to exercise after pregnancy
- Exercising during pregnancy
- Physiotherapy advice after pregnancy
Need more information?
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now entering.
Need further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari.![]() For more information, please visit the links below:
For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
Diastasis Recti (Abdominal Separation): Symptoms & Treatment
Overview
Diastasis recti happens when a person's abdomen stretches during pregnancy and creates a gap in the abdominal muscles.What is diastasis recti?
Diastasis recti (diastasis rectus abdominis or diastasis) is the separation of the rectus abdominis muscles during and after pregnancy. The rectus abdominis runs vertically along the front of your stomach. It's frequently referred to as someone's "six-pack abs." It's divided into left and right sides by a band of tissue called the linea alba that runs down the middle. As your uterus expands during pregnancy, the abdominals are stretched and the linea alba thins and pulls apart.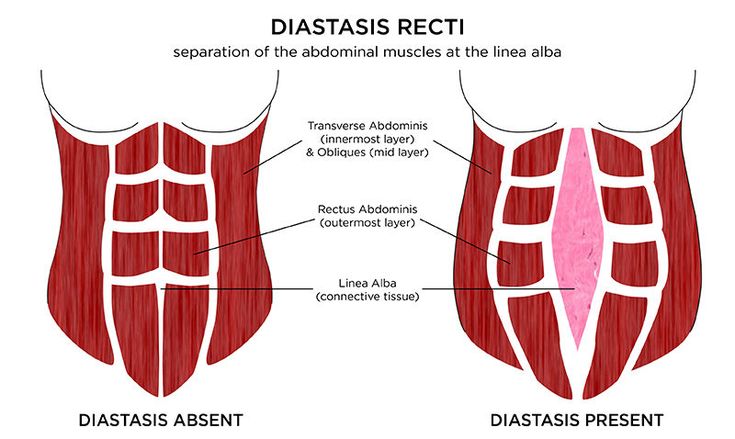 This band of tissue gets wider as it's pushed outward.
This band of tissue gets wider as it's pushed outward.
Once you deliver your baby, the linea alba can heal and come back together. It's highly elastic and retracts backs (like a rubber band). When the tissue loses its elasticity from being overstretched, the gap in the abdominals will not close as much as it should. This is diastasis recti.
If you have diastasis, your belly may appear to stick out just above or below the belly button, making you appear pregnant months or years after giving birth.
Why does diastasis recti happen?
Pregnancy puts a lot of pressure on your abdomen (abs). The abdomen is made up of left and right ab muscles and a thin band of connective tissue (linea alba) in between. They are pushed outward and stretched to make room for the growing baby. Diastasis recti occurs when the linea alba is overstretched and doesn't come back together. The left and right sides of the abdominals stay separated. It's also referred to as an "ab gap" or abdominal separation.
Who gets diastasis recti?
Diastasis recti is most common in pregnant and postpartum women (it can also be seen in men and infants). Diastasis recti usually develops in the third trimester. There is increased pressure on the abdominal wall because the baby is growing quickly during this time. Most people don't notice diastasis recti until the postpartum period.
How common is diastasis recti?
Diastasis recti is extremely common in those who are pregnant and during the postpartum period. It affects 60% of people. It usually resolves itself within eight weeks of delivery. About 40% of those who have diastasis recti still have it by six months postpartum.
Symptoms and Causes
What are the symptoms of diastasis recti?
Most people don't notice signs of diastasis recti until they are postpartum. You can have diastasis recti during pregnancy, but it's hard to distinguish because your abdomen is stretched.
Common signs of diastasis recti during the postpartum period are:
- A visible bulge or "pooch" that protrudes just above or below the belly button.

- Softness or jelly-like feeling around your belly button.
- Coning or doming when you contract your ab muscles.
- Difficulty lifting objects, walking or performing everyday tasks.
- Pain during sex.
- Pelvic or hip pain.
- Low back pain.
- Poor posture.
- Urine leaking when you sneeze or cough.
- Constipation.
- Feeling weak in your abdominals.
What does diastasis recti feel like?
Diastasis recti is not painful. You may feel pain associated with some of the side effects of diastasis, but the ab separation itself doesn't hurt. You may feel weakness in your core when doing once easy tasks, like lifting a laundry basket. Some people feel a jelly-like texture in the space between the left and right abdominals when contracting the ab muscles.
How do I know if I have diastasis recti?
There are some common signs that can signal you have diastasis recti. One of the most common signs of diastasis recti is a bulge in your midsection that doesn't go away, even after exercising or losing weight gained during pregnancy. Another sign is that your belly cones or domes when you lean back on a chair or get up out of bed. You can check for diastasis recti on your own, but it is always a good idea to speak with your healthcare provider about your symptoms.
Another sign is that your belly cones or domes when you lean back on a chair or get up out of bed. You can check for diastasis recti on your own, but it is always a good idea to speak with your healthcare provider about your symptoms.
What are the risk factors for developing diastasis recti?
Several factors can increase your risk for developing diastasis recti:
- Having multiple pregnancies (especially back-to-back).
- Being over 35 years old.
- Having multiples (such as twins or triplets).
- Having a heavy or big baby.
- Being extremely petite.
- Vaginal delivery. Pushing can increase abdominal pressure.
Diagnosis and Tests
How is diastasis recti diagnosed?
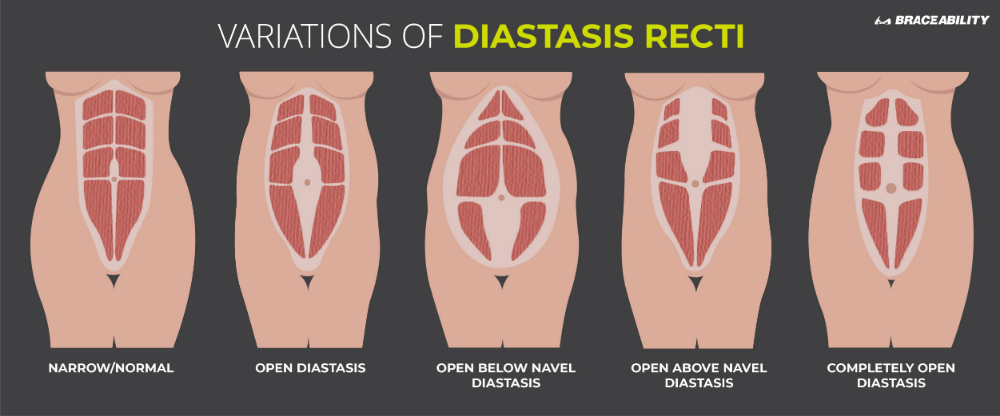
Your healthcare provider will evaluate if diastasis is present, where it's located and how severe it is. Diastasis recti can occur above the belly button, below the belly button and at the belly button.
Your provider will use their hands and fingers to feel the abdominal area for gaps and muscle tone. Some providers may use ultrasound, measuring tape or a tool called a caliper for a more accurate measurement. This exam typically occurs at your postpartum appointment before being cleared for exercise.
Some providers may use ultrasound, measuring tape or a tool called a caliper for a more accurate measurement. This exam typically occurs at your postpartum appointment before being cleared for exercise.
An abdominal gap wider than 2 centimeters is considered diastasis recti. Diastasis recti is also measured in finger widths, for example, two or three fingers' separation.
Your healthcare provider may recommend movements for diastasis recti or they may refer you to a specialist for additional treatment.
How do I test myself for diastasis recti?
You can test yourself for diastasis recti:
- Lie on your back with your knees bent and feet flat on the floor.
- Lift your shoulders slightly off the ground, keeping one hand behind your head for support. Almost like you are doing a sit-up. Look down at your belly.
- Move your other hand above your belly button area, palms down and fingers towards your toes.
- Use your fingers to feel for a gap between the abs.
 See how many fingers can fit in the gap between your right and left abdominals.
See how many fingers can fit in the gap between your right and left abdominals.
If you feel a gap of two or more finger widths, discuss your concerns with your healthcare provider. They should confirm diastasis recti with a proper diagnosis and recommend appropriate care.
Management and Treatment
How can I fix diastasis recti?
To fix diastasis recti, you'll need to perform gentle movements that engage the abdominal muscles. Before starting an exercise program, be sure it's safe for diastasis recti. Work with a fitness professional or physical therapist who has experience with diastasis recti. They can create a treatment plan to make sure you are performing the movements correctly and progressing to more challenging movements at the right time.
Certain movements will make abdominal separation worse. During the postpartum period, there are some modifications you should make:
- Avoid lifting anything heavier than your baby.
- Roll onto your side when getting out of bed or sitting up.
 Use your arms to push yourself up.
Use your arms to push yourself up. - Skip activities and movements that push your abdominals outward (like crunches and sit-ups).
Some people use binding devices (elastic belly bands) to help hold their belly in and support the lower back. Wearing binders can't heal diastasis recti and will not strengthen your core muscles. It can be a good reminder of your diastasis recti and promote good posture.
Can you fix diastasis recti without surgery?
Yes, it's possible to fix diastasis recti without surgery. Surgery is rarely performed to fix diastasis recti. Healthcare providers will recommend physical therapy or at-home exercises to help heal diastasis before surgical methods. Surgery is performed in cases of hernia (when an organ pushes through the linea alba) or if a woman wants diastasis recti surgery (a tummy tuck).
What are the best exercises for diastasis recti?
The best exercises for diastasis recti are those that engage the deep abdominals. Most diastasis recti exercises involve deep breathing and slow, controlled movements. Unfortunately, many of the most common ab exercises (like crunches) can worsen your diastasis. Before starting abdominal exercises, ask your healthcare provider to check you for diastasis recti.
Most diastasis recti exercises involve deep breathing and slow, controlled movements. Unfortunately, many of the most common ab exercises (like crunches) can worsen your diastasis. Before starting abdominal exercises, ask your healthcare provider to check you for diastasis recti.
What movements make diastasis recti worse?
Any movement that bulges the abdominal wall forward can cause more damage to your diastasis recti. Everyday movements like getting out of bed or up off a chair can worsen diastasis. Try to be mindful about how you are using your abdominals as you go about your day.
These exercise movements should be avoided if you have diastasis recti:
- Crunches or sit-ups of any kind.
- Planks or push-ups (unless using modifications).
- Downward dog, boat pose and other yoga poses.
- Double leg lifts, scissors and other Pilates moves.
- Any exercise that causes your abdominals to bulge, cone or dome.
Prevention
How do I prevent diastasis recti?
Some abdominal separation is normal and expected with pregnancy.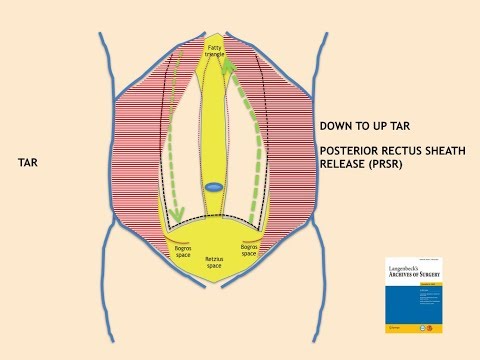 There are some things you can do to lower your risk for developing diastasis recti:
There are some things you can do to lower your risk for developing diastasis recti:
- Healthy weight gain during pregnancy: Exercising and eating healthy foods to keep weight gain within a healthy range.
- Proper posture and deep breathing: Stand up straight with your shoulders back. Take deep breaths that allow your ribs to expand and not just your belly.
- Safe core exercises: Avoid exercises like sit-ups and crunches that put pressure on your abdominals after 12 weeks of pregnancy and postpartum.
- Don't strain while lifting: Certain day-to-day activities like lifting grocery bags or your children can put undue strain on your abdominals.
- Log roll when getting out of bed: If you're pregnant or postpartum, roll to one side and use your arms to push up out of bed.
Outlook / Prognosis
How long will it take to heal my diastasis recti?
The amount of time it takes to heal diastasis recti depends on the amount of ab separation and how consistent you are with strengthening exercises. After several weeks postpartum, this gap will start to close as your muscles regain strength. If you're making modifications to your lifestyle and performing exercises with good form, you're more likely to notice progress.
After several weeks postpartum, this gap will start to close as your muscles regain strength. If you're making modifications to your lifestyle and performing exercises with good form, you're more likely to notice progress.
Can I get diastasis recti again?
Yes, you can heal your diastasis recti and get it again. Your risk for diastasis recti increases the more times you are pregnant. Think of the linea alba as a rubber band that is continuously stretched. Over time, the rubber band will lose its elasticity. The linea alba may not regain its original shape or form after being stretched through multiple pregnancies.
Is it too late to fix my diastasis recti?
It's never too late to repair your diastasis recti. With the proper exercises, you can fix your ab separation years after you've delivered your last baby.
Are there complications from diastasis recti?
If left untreated or in severe cases of diastasis recti, complications can include:
- Umbilical hernia.
- Increase in back pain.
- Pain during sex.
- Urinary incontinence.
- Pelvic and hip pain.
Living With
When should I see my healthcare provider?
Diastasis recti is a common and easily treated condition. If you have more than a two-finger gap between your abdominals or are experiencing pain, contact your healthcare provider for a diagnosis. They may want you to see a physical therapist or pelvic floor specialist to help strengthen your abdominal muscles.
A note from Cleveland Clinic:
Diastasis recti can make you appear pregnant years after your last baby. Discuss your concerns with your healthcare provider so they can diagnose and treat you. Getting treatment can help you feel more confident in your body and correct any pain you are experiencing.
Girard-Spasokukotsky method
Simultaneously suturing the medial flap of the aponeurosis external oblique muscle of the abdomen and free edges of the internal oblique and transverse muscles abdomen to the inguinal ligament. Then lateral aponeurosis flap is sutured over medial.
Then lateral aponeurosis flap is sutured over medial.
Benefits: not flare of the inguinal ligaments.
Weaknesses: retained tissue heterogeneity.
Girard-Spasokukotsky method with Kimbarovsky suture
Needle with a nylon thread pierce the medial aponeurosis flap of the external oblique muscle abdomen, stepping back from the free edge to 1–1.5 cm, capture the lower edges in the seam internal oblique and transverse muscles abdomen and return back, piercing flap of aponeurosis at its very edge. Then the inguinal is sewn with the same thread. ligament and tighten the ligature. After tying a knot medial edge aponeurosis of the external oblique abdominal muscle tucked, and to the inguinal ligament the edges of the muscles, shrouded in aponeurosis. Then the outer flap aponeurosis of the external oblique muscle of the abdomen impose on the medial and hem, creating a duplication of the aponeurosis.
Advantages:
one. connect homogeneous tissues;
connect homogeneous tissues;
2. a strong scar is formed;
3. the inguinal gap decreases.
Ways to strengthen the posterior wall of the inguinal canal Liechtenstein's way (non-stretch)
Method Liechtenstein - "gold standard" treatment of inguinal hernia At the stage of plasty behind the seminal the cord is inserted polypropylene mesh size approx. 6x12 cm. Bottom it is sewn to the upper pubic and inguinal ligaments. Laterally she is cut, a “window” is made for passage of the spermatic cord, then stitched again. Attached to the top internal oblique and transverse muscles, medially - to the edge of the rectus muscle. Subsequently, the mesh sprouts connective tissue, and intraperitoneal pressure spreads through it evenly.
phs bulk prosthesis method
For plastics of the posterior wall of the inguinal canal use a three-dimensional prosthesis, consisting from suprafascial and subfascial flaps, as well as a special connector.
Bassini method
are moving spermatic cord downwards and outwards. To the inguinal ligament is sutured with the lower free edges of the internal oblique and transverse muscles abdomen together with the underlying dissected transverse fascia. The last stitch in the medial corner of the wound is sutured aponeurosis of the rectus abdominis muscle to the pubis tubercle and inguinal ligament, thanks to what the edges of the broad muscles are reduced to inguinal ligament without undue tension. The spermatic cord is placed on the newly the created back wall and on top of it the edges of the aponeurosis are sutured with an external oblique abdominal muscles.
To the inguinal ligament is sutured with the lower free edges of the internal oblique and transverse muscles abdomen together with the underlying dissected transverse fascia. The last stitch in the medial corner of the wound is sutured aponeurosis of the rectus abdominis muscle to the pubis tubercle and inguinal ligament, thanks to what the edges of the broad muscles are reduced to inguinal ligament without undue tension. The spermatic cord is placed on the newly the created back wall and on top of it the edges of the aponeurosis are sutured with an external oblique abdominal muscles.
Methods of femoral hernia repair
Ways femoral hernia repair can be divided into two groups:
one. ways to close the hernial gate with sides of the thigh;
2. ways to close the hernial gate with sides of the inguinal canal.
Bassini method
Operational access - from the side of the thigh.
Produce plasty of the inner femoral ring canal by suturing the inguinal ligament to the crest ligament. In this way, the femoral ring is closed. Second a series of sutures are placed on the semilunar margin subcutaneous fissure and pectinate fascia.
In this way, the femoral ring is closed. Second a series of sutures are placed on the semilunar margin subcutaneous fissure and pectinate fascia.
Faults: inguinal the ligament is displaced downwards and thereby the inguinal gap increases, which creates conditions for the formation of inguinal hernia
Diastasis of the rectus muscles
All types of operations for suturing, or rather plastic surgery of the anterior abdominal wall in diastasis can be divided into two types - open and minimally invasive (laparoscopic and endoscopic).
Open surgery in most cases is a complete reconstruction of the anterior abdominal wall together with abdominoplasty. This allows not only to eliminate diastasis and the hernias that accompany it, but also to remove excess skin, and if you supplement the operation with liposuction, you can get an almost perfect shape of the abdomen, correct the “hanging” of the skin over the scar after a cesarean section.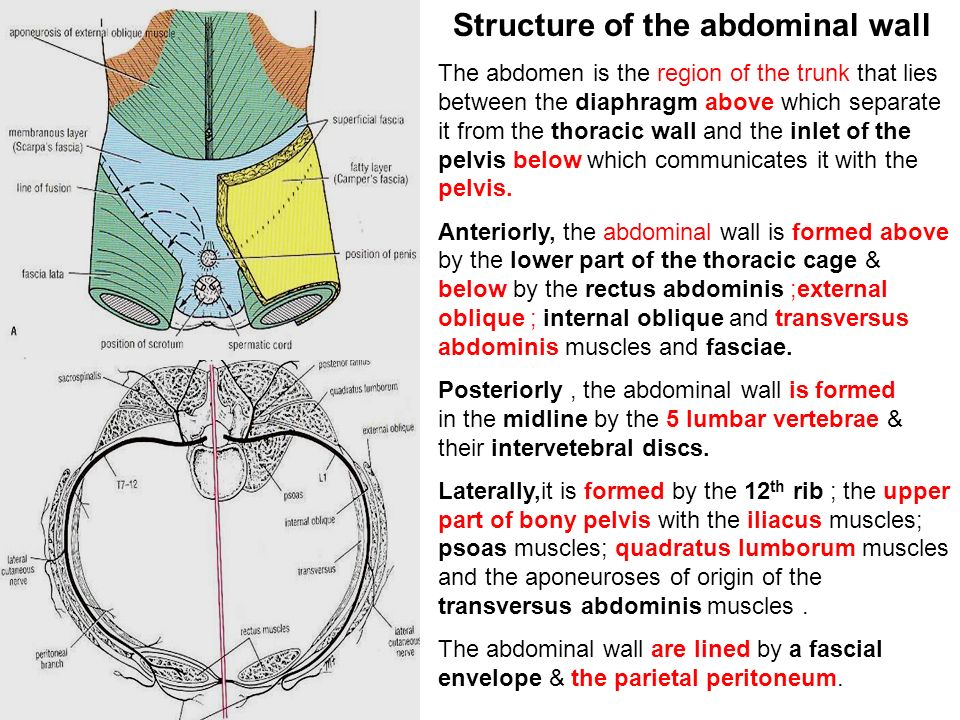 The elimination of diastasis with this approach is the most reliable, as it provides ample opportunities for choosing the optimal method for its correction.
The elimination of diastasis with this approach is the most reliable, as it provides ample opportunities for choosing the optimal method for its correction.
Most often, we perform this operation together with a plastic surgeon. In our opinion, this approach is optimal, since a plastic surgeon rarely has experience working with deep layers of the anterior abdominal wall, and an abdominal surgeon rarely knows all the subtle nuances of working with a skin-fat flap, and even more so, the liposuction technique. Joint work, when each surgeon deals with his part of the intervention, allows you to get the best result, combining the reliability of diastasis and hernia repair and the excellent cosmetic effect of the operation.
With this type of intervention, the plastic surgeon marks the anterior abdominal wall, performs liposuction, performs an access in the lower abdomen, just below the scar from the caesarean section. After mobilization of the skin-fat flap, the abdominal surgeon enters the work, performing plastic surgery of diastasis, hernial defects, most often strengthening the anterior abdominal wall with a mesh implant, placing it in the deepest layer of the anterior abdominal wall - the retromuscular space and restoring the white line of the abdomen.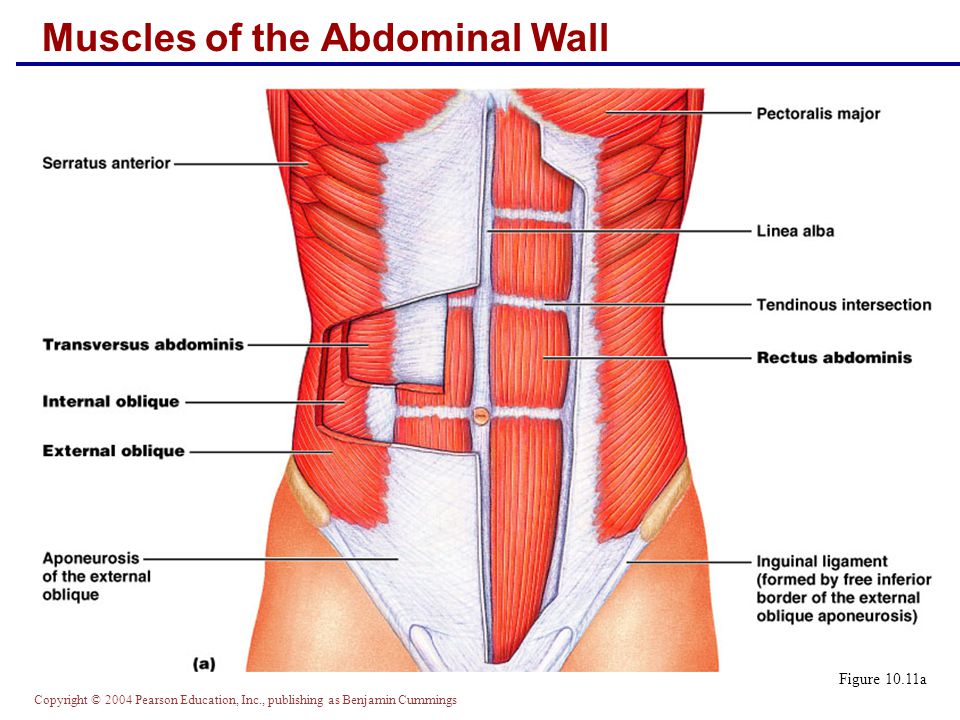 After that, the “helm” again passes to the plastic surgeon, who removes excess skin and subcutaneous tissue and applies cosmetic sutures. After the operation, it is mandatory to wear special compression underwear for a month.
After that, the “helm” again passes to the plastic surgeon, who removes excess skin and subcutaneous tissue and applies cosmetic sutures. After the operation, it is mandatory to wear special compression underwear for a month.
If abdominoplasty is not required, we prefer minimally invasive endoscopic methods for diastasis correction. There are several varieties, each with its own advantages and disadvantages. The choice of a specific type of plastic surgery occurs after an in-person consultation and obtaining all the necessary information about a specific clinical situation.
Techniques when diastasis correction is carried out from the abdominal cavity are used by us quite rarely. For all its apparent simplicity, the strengthening of the white line with the placement of the implant in the abdominal cavity is accompanied by a small but real risk of the formation of adhesions in the postoperative period, even despite the use of high-tech and rather expensive combined implants with an anti-adhesion coating.