Abdominal muscles during pregnancy
Anatomy of pregnancy and birth - abdominal muscles
Anatomy of pregnancy and birth - abdominal muscles | Pregnancy Birth and Baby beginning of content3-minute read
Listen
The most obvious physical sign that a woman is pregnant is the growing abdomen – or, ‘baby bump’ – which affects the abdominal muscles. Understanding how the abdominal muscles work is helpful for pregnant women. Strengthening your abdominal muscles during and after pregnancy helps these muscles work as they should.
What are abdominal muscles?
The abdominal muscles are those in the front of the torso (also referred to as the trunk), between the ribs and the pelvis. The abdominal muscles in both pregnant and non-pregnant people are designed to support the torso. This allows movement, such as walking and bending. The strength of the abdominal muscles holds the internal organs in place.
There are 4 types of abdominal muscles — the external and internal obliques, and the transversus and rectus abdominis — which come in pairs (one on either side of the torso), and work together to:
- stabilise the torso and keep organs in place
- support movements between the rib cage and the pelvis
- allow the torso to twist
The term 'core muscles' is commonly used to describe the deepest abdominal muscles and the muscles in the back, which attach to the spine or pelvis. The core muscles are responsible for keeping the body stable and balanced, and to protect the spine.
What happens to abdominal muscles during pregnancy and birth?
During pregnancy, the growing baby stretches the abdominal muscles. The mother's abdomen changes shape during the pregnancy because of the growth and movement of the baby, and so her abdominal muscles are also affected. For instance, the abdominal muscles progressively stretch as the pregnancy proceeds as the womb expands.
For instance, the abdominal muscles progressively stretch as the pregnancy proceeds as the womb expands.
During the birth, most of the pushing is done by the uterus, not the abdominal muscles. After the birth, the abdominal muscles will feel weak and stretched, but these muscles should eventually become toned again.
How can abdominal muscles be strengthened during pregnancy?
Abdominal muscles overstretch during the pregnancy since the baby rests forward on them, so it is important that these muscles are exercised. Strengthening the abdominals can help pregnant women stay active and use the abdominal muscles for day-to-day activities, such as support and movement. Exercising abdominal muscles during pregnancy also helps them return to their original length and shape after the baby is born.
Safety tip: Sit-ups and crunches are not recommended during pregnancy. This is because the stretched abdominal muscles in a pregnant woman do not work the same way as when she is not pregnant. These exercises are usually done while lying on your back. This position can cause dizziness in pregnant women because the weight of the baby rests on major blood vessels.
These exercises are usually done while lying on your back. This position can cause dizziness in pregnant women because the weight of the baby rests on major blood vessels.
A safe way to work the abdominal muscles and improve core strength is to draw in the muscles without moving your spine – as though sucking your belly button in, towards the spine.
Pregnancy-specific exercise classes can also help build and maintain core strength, such as yoga and Pilates classes for pregnant women. They tend to focus on low impact exercises and feature movements that help with core strength, breathing and relaxation, strengthening abdominal muscles, the pelvic floor and relieving lower back pain.
What problems can happen to abdominal muscles in pregnancy?
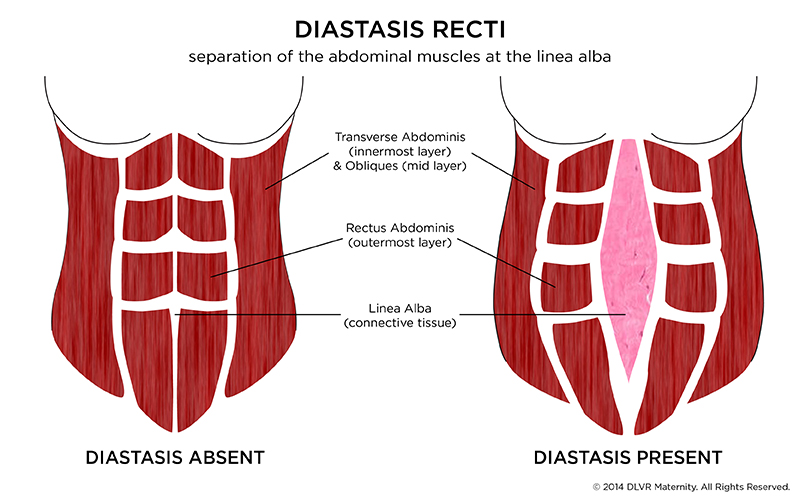
The enlarging uterus causes the abdominal muscles to stretch. It may cause the two bands of muscles that meet in the middle of the abdomen to separate. This condition is called 'diastasis recti'. This muscle separation can sometimes appear as a bulge in the middle of the abdomen. The condition may cause pain in the lower back or it might become hard to lift things or do other physical activities. Abdominal muscle separation is usually managed after childbirth with exercise and physiotherapy. Occasionally surgery is required.
The condition may cause pain in the lower back or it might become hard to lift things or do other physical activities. Abdominal muscle separation is usually managed after childbirth with exercise and physiotherapy. Occasionally surgery is required.
If you think you may have diastasis recti, see your doctor or maternal health service.
Sources:
Royal Women's Hospital (Abdominal muscles), Mayo Clinic (Why do abdominal muscles sometimes separate during pregnancy?), Better Health Channel (Abdominal muscles), Physical Therapy (Structure and Function of the Abdominal Muscles in Primigravid Subjects During Pregnancy and the Immediate Postbirth Period)Learn more here about the development and quality assurance of healthdirect content.
Last reviewed: October 2020
Back To Top
Related pages
- Anatomy of pregnancy and birth - uterus
- Anatomy of pregnancy and birth - perineum and pelvic floor
- Anatomy of pregnancy and birth - pelvis
- Anatomy of pregnancy and birth - cervix
- Anatomy of pregnancy and birth
Need more information?
Abdominal muscles - Better Health Channel
The abdominal muscles support the trunk, allow movement and hold organs in place by regulating internal abdominal pressure.
Read more on Better Health Channel website
Postnatal exercise - sample workout - Better Health Channel
Make sure your abdominal muscles have healed before you do any vigorous tummy exercises, such as crunches.
Read more on Better Health Channel website
Abdominal separation (diastasis recti)
Abdominal separation (‘diastasis recti’) occurs when the stomach muscles weaken and separate during and after pregnancy. Here's how to recognise and treat it.
Read more on Pregnancy, Birth & Baby website
The Abdominal Brace · Core exercises · Pelvic Floor First
The Abdominal Brace. Pelvic floor friendly exercises, Core exercises, The Abdominal Brace.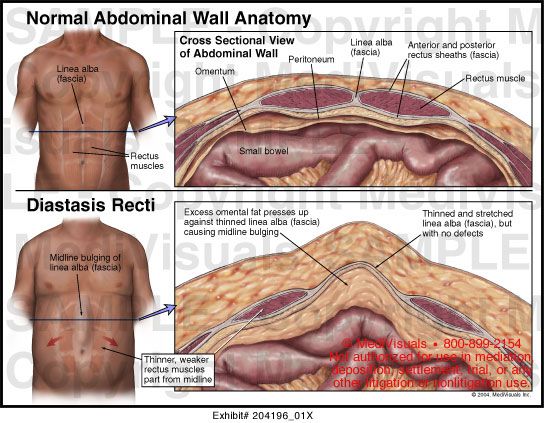 ‘Brace your abs’, ‘Lock on your core’, ‘Switch on your core’. These are all popular phrases used in group exercises classes and by personal trainers.
‘Brace your abs’, ‘Lock on your core’, ‘Switch on your core’. These are all popular phrases used in group exercises classes and by personal trainers.
Read more on Continence Foundation of Australia website
Hernia
A hernia is the protrusion of organs, such as intestines, through a weakened section of the abdominal wall.
Read more on Queensland Health website
Abdominal pain in children - Better Health Channel
Children may feel stomach pain for a range of reasons and may need treatment
Read more on Better Health Channel website
The pelvic floor and core exercises · Pelvic floor friendly exercises · Pelvic Floor First
The pelvic floor muscles form the base of the group of muscles commonly called the ‘core’.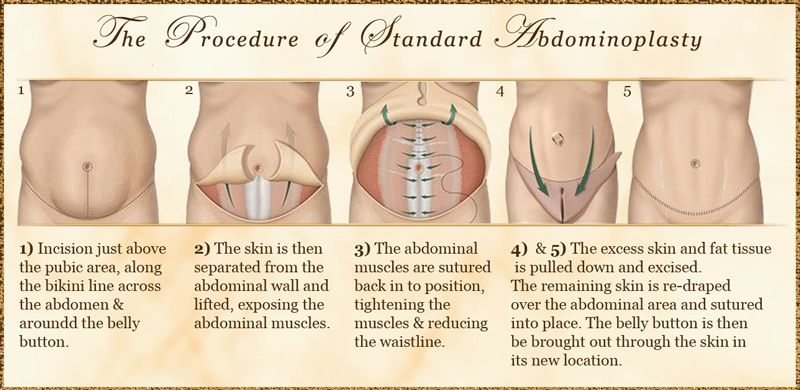
Read more on Continence Foundation of Australia website
The pelvic floor and core · The pelvic floor · Pelvic Floor First
The pelvic floor muscles form the base of the group of muscles commonly called the ‘core’.
Read more on Continence Foundation of Australia website
The pelvic floor · Pelvic Floor First
The pelvic floor is the base of the group of muscles referred to as your ‘core'.
Read more on Continence Foundation of Australia website
Working your pelvic floor · The pelvic floor · Pelvic Floor First
Your pelvic floor muscles can be consciously controlled and therefore trained
Read more on Continence Foundation of Australia website
Disclaimer
Pregnancy, Birth and Baby is not responsible for the content and advertising on the external website you are now entering.
Need further advice or guidance from our maternal child health nurses?
1800 882 436
Video call
- Contact us
- About us
- A-Z topics
- Symptom Checker
- Service Finder
- Linking to us
- Information partners
- Terms of use
- Privacy
Pregnancy, Birth and Baby is funded by the Australian Government and operated by Healthdirect Australia.
Pregnancy, Birth and Baby is provided on behalf of the Department of Health
Pregnancy, Birth and Baby’s information and advice are developed and managed within a rigorous clinical governance framework. This website is certified by the Health On The Net (HON) foundation, the standard for trustworthy health information.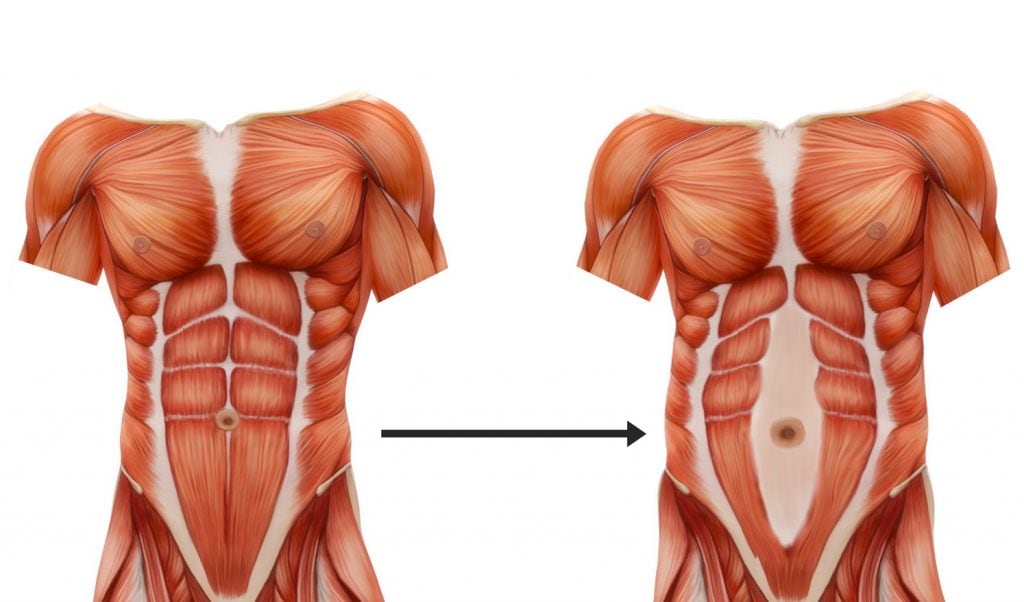
This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.
This information is for your general information and use only and is not intended to be used as medical advice and should not be used to diagnose, treat, cure or prevent any medical condition, nor should it be used for therapeutic purposes.
The information is not a substitute for independent professional advice and should not be used as an alternative to professional health care. If you have a particular medical problem, please consult a healthcare professional.
Except as permitted under the Copyright Act 1968, this publication or any part of it may not be reproduced, altered, adapted, stored and/or distributed in any form or by any means without the prior written permission of Healthdirect Australia.
Support this browser is being discontinued for Pregnancy, Birth and Baby
Support for this browser is being discontinued for this site
- Internet Explorer 11 and lower
We currently support Microsoft Edge, Chrome, Firefox and Safari. For more information, please visit the links below:
For more information, please visit the links below:
- Chrome by Google
- Firefox by Mozilla
- Microsoft Edge
- Safari by Apple
You are welcome to continue browsing this site with this browser. Some features, tools or interaction may not work correctly.
The abdominal muscles | The Royal Women's Hospital
Because your abdominal muscles stretch over the growing baby and uterus, they can become less effective.
The abdominal muscles support your abdominal organs and spine. When the abdominal muscles contract they produce spinal movement so you can bend and twist, or hold the spine stable so you can stand upright. This is called ‘core stability’. Because your abdominal muscles stretch over the growing baby and uterus, they can become less effective at doing their normal support and movement tasks. If they are not exercised at all, they can overstretch as the uterus rests forward onto them. Then they maybe unable to return to their original length and shape after birth.
Then they maybe unable to return to their original length and shape after birth.
Sit-ups, or ‘crunches’ are the usual exercises associated with abdominal training. These are inappropriate and ineffective during pregnancy – ineffective because the stretch on your abdominal muscles means they cannot work the way they did before you were pregnant; and inappropriate because the exercise is done lying on your back. In this position the baby rests on major blood vessels and may block blood flow, causing dizziness.
Tummy exercises in pregnancy
The best way to exercise the abdominals and gain core stability is to draw them in without moving your spine. Think of cuddling you baby with your abdominal muscles or sucking your bellybutton towards your backbone.
- Get on your hands and knees. Let your tummy relax.
- Breathe in gently. As you breathe out, gently draw in the lower part of your stomach firmly, lifting your baby as you draw in. Hold for the count of three or more if you can.
 Let go.
Let go. - Repeat this movement up to 10 times with a few seconds rest between each one.
- Build up gradually until you can hold the muscles strongly for 10 seconds and repeat the exercise 10 times, and can also do a 60-second-long hold.
- When this exercise becomes easy, challenge yourself by lifting one arm alternately while keeping you abdominals ‘switched on’, then one leg, then opposite arm and leg, then same side arm and leg. With each of these variations, build up your hold time as you did with the initial exercise.
Hint: Don’t move your back at any time during the exercise. You should be able to breathe and talk as you do this exercise. You can also squeeze your pelvic floor muscles at the same time.
Group exercise during pregnancy
If you are exercising in a group or at a gym, choose to do clinical pilates, a fitball class, boxercise, aquarobics, or a ‘Pump’ class (with light weights) for the best abdominal workout.
The Women’s does not accept any liability to any person for the information or advice (or use of such information or advice) which is provided on the Website or incorporated into it by reference. The Women’s provide this information on the understanding that all persons accessing it take responsibility for assessing its relevance and accuracy. Women are encouraged to discuss their health needs with a health practitioner. If you have concerns about your health, you should seek advice from your health care provider or if you require urgent care you should go to the nearest Emergency Dept.
Physiological changes during pregnancy
Anatomy
Muscles, joints and bones
The pelvis is the part of the skeleton that attaches the lower limbs to the trunk. In women, the pelvis is wider and lower than in men, making it more suitable for accommodating the fetus both during pregnancy and childbirth. It protects and supports the internal organs, provides muscle attachment and transfers weight from the trunk to the legs in a standing position and to the ischial tuberosities in a sitting position.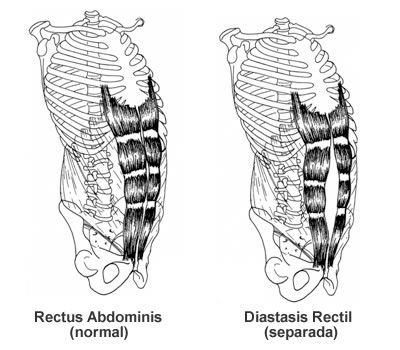 nine0007
nine0007
Cross-sectional anatomy of a female pelvis showing five bones: two pelvic bones, sacrum, coccyx, and two femurs. Each pelvic bone is formed by the fusion of three bones: the ilium, pubis, and ischium. The sacrum and coccyx are also made up of several smaller bones. The sacrum is made up of the fusion of five sacral vertebrae (S1-S5) and the coccyx is made up of the fusion of four coccygeal vertebrae. The femur articulates with the pelvic bone through the hip joint.
The pelvic joints are supported by some of the strongest ligaments in the body, which become more relaxed during pregnancy, resulting in increased mobility and less efficient transfer of load through the pelvis. The exit from the cavity of the small pelvis has a narrower transverse diameter compared to the entrance. The exit from the cavity of the small pelvis is formed by the coccyx, sacrotuberous ligaments, branches of the ischial bones, ischial tuberosities, lower branches of the pubic bones and the pubic symphysis. nine0007
nine0007
Four pairs of abdominal muscles form the anterior and lateral abdominal walls (they are also called the abdominal corset). The transverse abdominis muscle is located under the internal and external oblique abdominal muscles, as well as under the rectus abdominis muscle, which is located in the center and most superficially. The internal oblique muscle of the abdomen, the external oblique muscle of the abdomen and the transverse abdominal muscle are connected in the middle along the white line of the abdomen.
The deep abdominal muscles, together with the pelvic floor muscles, the multifidus muscles and the diaphragm, can be considered as a whole, they are also called the lumbopelvic cylinder. This "cylinder" provides support for the contents of the abdominal cavity and maintains intra-abdominal pressure. nine0007
The main function of the rectus abdominis is to flex the lumbar spine, while the obliques provide lateroflexion and rotation.
Muscles of the back include the quadratus lumborum, latissimus dorsi, serratus posterior inferior, extensor spinae, interspinous muscles, and transverse spinal muscles.
The muscles that are related to the femur can be divided into three sections: anterior, medial and posterior. The anterior compartment includes the iliopsoas, quadratus femoris, sartorius, and pectus muscles. The medial portion consists of the adductor magnus, adductor longus, adductor short, obturator externus, and gracilis. The posterior section consists of the biceps femoris, semitendinosus, and semimembranosus muscles. The muscles of the gluteal region are the gluteus maximus, medius, and minimus, the tensor fascia lata, the piriformis, the gemellus superior and inferior, and the obturator internus. nine0007
The pelvic floor includes the levator ani, bulbospongiosus, and deep transverse perineal muscles. See also the article: Anatomy of the pelvic floor.
Female reproductive system
The organs of the female reproductive system, located in the small pelvis, are divided into internal and external genital organs. Internal organs include the uterus, fallopian tubes, ovaries, and vagina. The external genital organs include the pubis, clitoris, labia majora and labia minora, and Bartholin's glands. nine0007
The external genital organs include the pubis, clitoris, labia majora and labia minora, and Bartholin's glands. nine0007
Changes in the musculoskeletal system
Posture
The overall balance of the spine and pelvis changes during pregnancy, but there is still controversy as to the exact nature of any pregnancy-related postural adaptation. With weight gain, increased blood volume and ventral growth of the fetus, the center of gravity no longer passes through the feet, and women have to lean backward to achieve balance, which leads to disorganization of the spinal curves. nine0007
Observed postures may include decreased lumbar lordosis, increased both lumbar lordosis and thoracic kyphosis, or flattening of the thoracolumbar junction of the spine. Compensatory changes in posture in the thoracic and cervical spine will also be observed, and this, combined with an increase in the weight of the mammary glands, can lead to a displacement of the shoulder girdle and thoracic spine posteriorly, as well as an increase in cervical lordosis.
Joints and Ligaments
Altered levels of relaxin, estrogen and progesterone during pregnancy lead to changes in collagen metabolism and increased flexibility and extensibility of connective tissue. Consequently, the ligaments relax, which is accompanied by a decrease in the passive stabilization of the joints. The pubic symphysis and sacroiliac joints are especially susceptible to changes. Weakness of the ligaments may persist for up to six months after childbirth. Biomechanical changes in the spine and pelvic joints can lead to an increase in the true conjugate, an increase in the lumbosacral angle, an anterior inclination of the innominate bones, and an anterior and downward inclination of the pubic symphysis. nine0007
Normally, the gap of the symphysis pubis is 4-5 mm, and during pregnancy it can increase by 3 mm. Relaxation of the pelvic joints begins at the 10th week of pregnancy, and they return to normal only 4-12 weeks after birth. The sacrococcygeal joints also relax.
By the last trimester of pregnancy, the abductors and extensors of the hip, as well as the plantar flexors of the foot, increase their power during walking, which is accompanied by an increase in the load on the hip joints by 2.8 times, especially when working while standing at the table. As the uterus rises towards the diaphragm, the rib cage expands laterally and its diameter can increase by 10-15 cm.
Muscular system
During pregnancy, the enlargement of the uterus causes the abdominal muscles to lengthen and the rectus abdominis muscles to diverge along the linea alba.
Decreased passive joint stabilization alters afferent input from their mechanoreceptors and likely affects motor neuron recruitment. A decrease in muscle strength and, therefore, an active component of joint stabilization may be the result of a change in the work of the muscle spindle, which is especially true for the muscles of the pelvic girdle. nine0007
These changes can lead to poor recruitment of the muscles responsible for pelvic stability (particularly the gluteus maximus and medius), which is often accompanied by gait disturbance and lumbosacral pain.
Changes in other body systems
Cardiovascular system
The heart largely adapts to the increasing workload that occurs during pregnancy. Cardiac output increases early and peaks in the third trimester, usually 30-50% above baseline. Estrogen increases cardiac output by increasing preload and stroke volume, mainly by increasing total blood volume (which increases by 40–50%). The heart rate increases, but usually does not exceed 100 beats per minute. The total systemic vascular resistance is reduced by 20% due to the secondary vasodilating action of progesterone. In general, systolic and diastolic blood pressure drops by 10–15 mm. rt. Art. in the first trimester and then returns to baseline in the second half of pregnancy. All of these cardiovascular adaptations can lead to complaints such as palpitations, decreased exercise tolerance, and dizziness. nine0007
Gastrointestinal
Progesterone causes smooth muscle relaxation, which slows down gastrointestinal motility and decreases lower esophageal sphincter tone.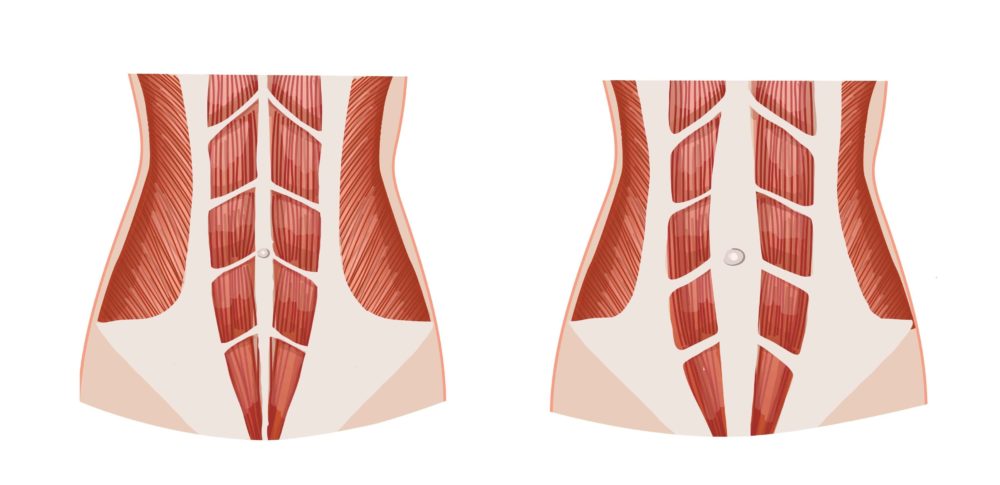 As a result, an increase in intragastric pressure, combined with a decrease in the tone of the lower esophageal sphincter, leads to gastroesophageal reflux, which often occurs during pregnancy. Nausea and vomiting during pregnancy, commonly known as "morning sickness," is one of the most common symptoms of GI changes during pregnancy. It starts between 4 and 8 weeks of pregnancy and usually resolves by 14 to 16 weeks. The exact cause of nausea is not fully understood, but it correlates with an increase in the level of human chorionic gonadotropin, progesterone, and as a result of this, relaxation of the smooth muscles of the stomach occurs. Also during pregnancy, constipation and hemorrhoids can occur. nine0007
As a result, an increase in intragastric pressure, combined with a decrease in the tone of the lower esophageal sphincter, leads to gastroesophageal reflux, which often occurs during pregnancy. Nausea and vomiting during pregnancy, commonly known as "morning sickness," is one of the most common symptoms of GI changes during pregnancy. It starts between 4 and 8 weeks of pregnancy and usually resolves by 14 to 16 weeks. The exact cause of nausea is not fully understood, but it correlates with an increase in the level of human chorionic gonadotropin, progesterone, and as a result of this, relaxation of the smooth muscles of the stomach occurs. Also during pregnancy, constipation and hemorrhoids can occur. nine0007
Eating behavior
Both protein and carbohydrate metabolism change during pregnancy. One kilogram of additional protein is deposited, with half going to the needs of the fetus and placental growth, and the other half being spent on uterine contractile proteins, breast glandular tissue, blood plasma protein and hemoglobin.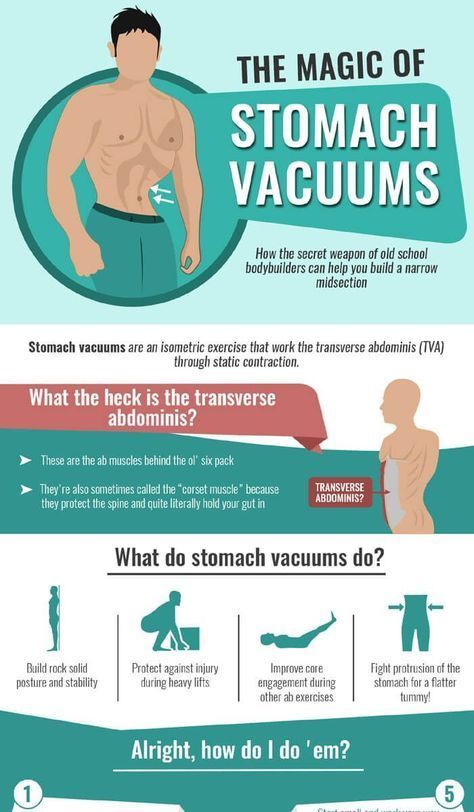
Increased nutrient requirements due to fetal growth and fat deposition. These changes are caused by steroid hormones, lactogen and cortisol. Pregnant women need to increase the calorie content of food. Over the entire period of pregnancy, weight gain can reach 9.1 - 13.6 kg.
Urinary system
A pregnant woman may experience an increase in the size of the kidneys and ureters due to an increase in the vascular system and blood volume. Physiological hydronephrosis and hydroureter may also develop, which is a normal process.
Problems during pregnancy
- Pelvic floor muscle dysfunction.
- Dysfunction of the pubic symphysis.
- Pain in the region of the ribs.
- Back pain.
- Compression neuropathy.
- Carpal tunnel syndrome.
- Muscle spasms.
- Morning sickness.
- Edema.
Contraindications to exercise
If you are thinking about exercising regularly, you should consult your doctor.
Contact sports and activities that carry a high risk of falls or injury to the abdomen should be avoided. Scuba diving should also be avoided.
Adjust the intensity level and duration of your workouts yourself. It is important to keep the shock activity low. Wear suitable footwear to reduce stress on the musculoskeletal system. Drink plenty of fluids to prevent dehydration and avoid exercise during hot and humid weather or if hyperthermia is present. Warming up and cooling down must be carried out for at least five minutes. Do not resort to stretching (due to the effects of relaxin). nine0007
Ask for advice on specific exercises (eg pelvic floor muscles). Avoid ballistic exercises, deep squats, cross steps, and quick changes of direction. Do not exercise in the supine position after 16 weeks of pregnancy to avoid aorto-caval compression. Eat according to your appetite, no calorie restrictions. To avoid overtraining, work in the direction of the adjacent load; finish your workouts before fatigue sets in. nine0007
nine0007
Friends, Marina Osokina's seminar “Women's Health: Opportunities for Restorative Fitness and Physical Therapy” will take place very soon. Learn more...
Women who are not accustomed to regular exercise should be informed of the following:
- do not start an exercise program until after 13 weeks of pregnancy;
- consider starting with low-intensity exercise, such as a pregnancy pool; nine0076
- start with simple and basic exercises, gradually moving to more complex ones (under the supervision of a qualified specialist).
Contraindications to exercise
- Cardiovascular, respiratory, kidney or thyroid disease.
- Diabetes (type 1 if uncontrolled).
- History of miscarriage or preterm birth, fetal growth retardation, cervical incompetence.
- Arterial hypertension, vaginal bleeding, decreased fetal mobility, anemia, breech presentation, placenta previa. nine0076
All women should stop exercising immediately and see a doctor if they experience:
- abdominal pain;
- bleeding from the vagina;
- shortness of breath, dizziness, weakness, severe headache, palpitations or tachycardia;
- pain in the pelvis, which can also lead to difficulty walking.
Source: Physiopedia — Physiological changes during pregnancy.
Diastasis of the rectus abdominis muscles and diastasis of the womb. Solvable problems of pregnancy. Interview with Doctor of Medical Sciences, Professor M.A. Chechnyova
— What is muscle diastasis and what is pubic diastasis?
— Pregnancy is an amazing and wonderful time, but it is also a period of additional loads, which undoubtedly becomes a test of strength for the female body.
The previously existing household point of view that pregnancy rejuvenates and gives strength is not confirmed by anything. During the bearing of a child, significant additional loads are placed on the mother's body, which often lead to the manifestation of problems that were invisible before pregnancy. nine0007
Diastasis of the rectus abdominis muscles is a divergence of the inner edges of the muscles along the white line of the abdomen (connective tissue structure) at a distance of more than 27 mm. Pubic diastasis is one of the manifestations of pregnancy-associated pelvic girdle pain. This pathology affects the entire pelvic ring, sacroiliac joints and symphysis. And they certainly have common causes for the appearance.
Pubic diastasis is one of the manifestations of pregnancy-associated pelvic girdle pain. This pathology affects the entire pelvic ring, sacroiliac joints and symphysis. And they certainly have common causes for the appearance.
The formation of such problems is facilitated by a decrease in the strength of connective tissue collagen. One of the reasons is an innate predisposition, the so-called connective tissue dysplasia, when the tissues are very elastic, extensible. During pregnancy, the body of a woman increases the production of the hormone relaxin, which reduces the synthesis of collagen and enhances its breakdown. This is provided by nature to create maximum elasticity of the birth canal. However, other structures, such as the anterior abdominal wall and the pubic symphysis, also fall under the action of relaxin. nine0007
— How does diastasis of the muscles and diastasis of the pubis affect pregnancy and childbirth?
— Divergence of the rectus abdominis occurs in about 40% of pregnant women.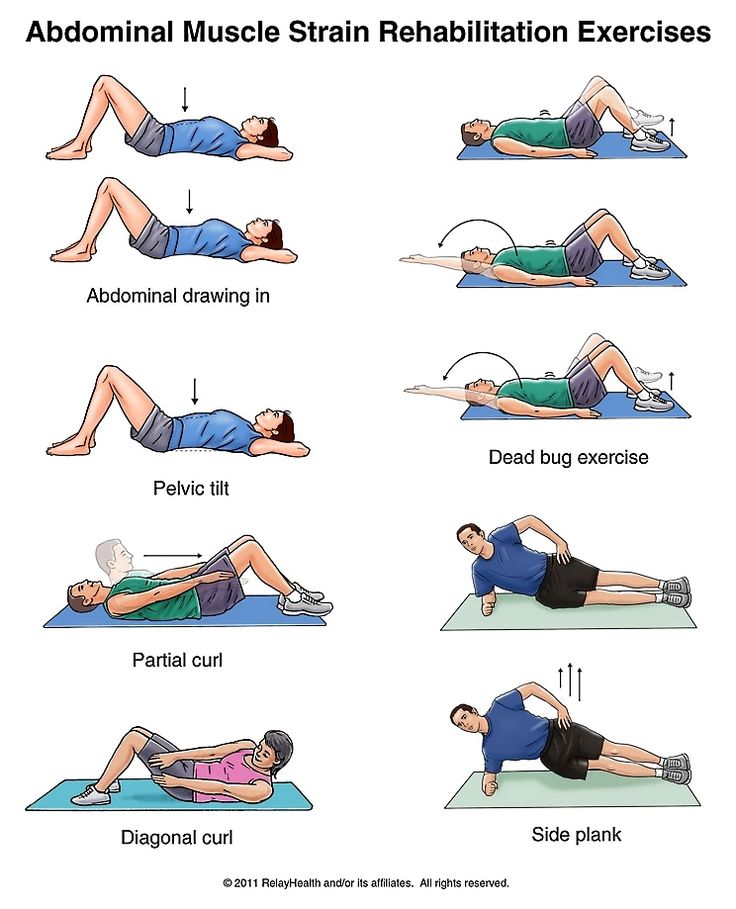 During pregnancy, it does not give serious complications that threaten the life of the mother or the condition of the fetus. However, the inferiority of the work of the rectus abdominis muscles forces the redistribution of the load on the back muscles, which can lead to lumbar-pelvic pain and, accordingly, discomfort in the back. During childbirth, the abdominal muscles are involved in attempts, and the violation of their anatomy and function can affect the birth act. nine0007
During pregnancy, it does not give serious complications that threaten the life of the mother or the condition of the fetus. However, the inferiority of the work of the rectus abdominis muscles forces the redistribution of the load on the back muscles, which can lead to lumbar-pelvic pain and, accordingly, discomfort in the back. During childbirth, the abdominal muscles are involved in attempts, and the violation of their anatomy and function can affect the birth act. nine0007
With diastasis of the pubis, things are more complicated. As already mentioned, this is only one of the manifestations of a violation of the structure and function of the pubic joint (symphysiopathy) during pregnancy. It occurs in about 50% of pregnant women in varying degrees of severity: in 25% of cases it leads to restriction of the mobility of the pregnant woman, in 8% - to severe disorders up to disability.
With symphysiopathy, the ligaments of the pubic articulation and cartilage that connect the pubic bones suffer. All this leads to severe pain in the pubic joint, pelvic bones, lower back, as well as to a violation of gait and the inability to stand up or lie down without outside help. Women with pelvic girdle pain syndrome experience significant levels of discomfort, disability, and depression, with associated social and economic problems. These include impaired sexual activity during pregnancy, chronic pain syndrome, risk of venous thromboembolism due to prolonged immobility, and even seeking early induction of labor or caesarean section to stop pain. nine0007
All this leads to severe pain in the pubic joint, pelvic bones, lower back, as well as to a violation of gait and the inability to stand up or lie down without outside help. Women with pelvic girdle pain syndrome experience significant levels of discomfort, disability, and depression, with associated social and economic problems. These include impaired sexual activity during pregnancy, chronic pain syndrome, risk of venous thromboembolism due to prolonged immobility, and even seeking early induction of labor or caesarean section to stop pain. nine0007
During childbirth, this patient may experience a rupture of the pubic symphysis and may require surgery to repair it.
— How to prevent the development of muscle and pelvic diastasis during pregnancy and childbirth? What factors increase the likelihood of its development?
- There is no recipe that will be one hundred percent. There is a wonderful term in the medical literature called "lifestyle modification".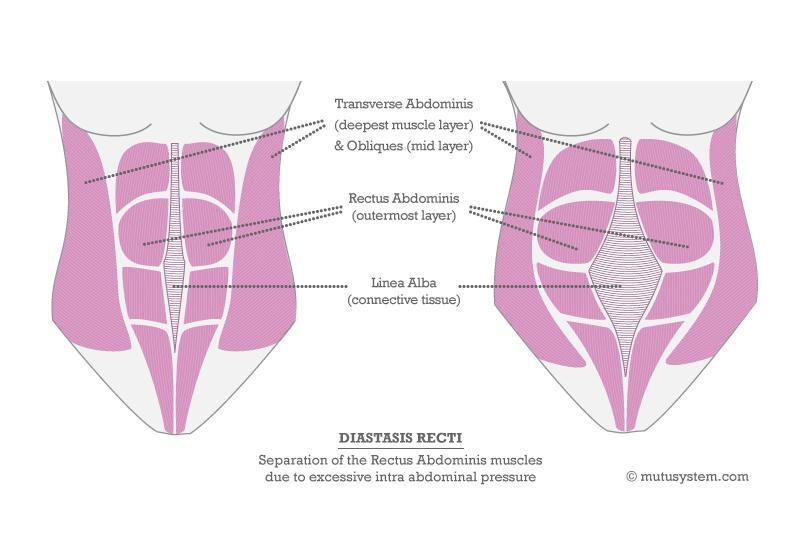 Whatever diseases we study, be it symphysiopathy, diabetes mellitus or preeclampsia, the risk group for pathology is always overweight women. You need to prepare for pregnancy, you need to be in good physical shape. During pregnancy, weight gain should be monitored. The recommendation to "eat for two" is not just wrong, but extremely harmful. Pregnant women should maintain reasonable physical activity. Weak and flabby abdominal muscles, combined with the large size of the fetus, undoubtedly increase the risk of diastasis. nine0007
Whatever diseases we study, be it symphysiopathy, diabetes mellitus or preeclampsia, the risk group for pathology is always overweight women. You need to prepare for pregnancy, you need to be in good physical shape. During pregnancy, weight gain should be monitored. The recommendation to "eat for two" is not just wrong, but extremely harmful. Pregnant women should maintain reasonable physical activity. Weak and flabby abdominal muscles, combined with the large size of the fetus, undoubtedly increase the risk of diastasis. nine0007
The risk factors for symphysiopathy in numerous studies are heavy physical labor and previous injuries of the pelvic bones. Factors such as time elapsed from previous pregnancies, smoking, use of hormonal contraception, epidural anesthesia, mother's ethnicity, number of previous pregnancies, bone density, weight and gestational age of the fetus (post-term fetus) are not associated with an increased risk of symphysiopathy.
— How to diagnose diastasis recti and diastasis pubis? nine0148
— In most cases, diastasis rectus abdominis can be diagnosed clinically. It happens that inspection, palpation and simple measurements are enough.
It happens that inspection, palpation and simple measurements are enough.
In the standing position, you can see the divergence of the muscles when the woman does not have subcutaneous fat. In this case, diastasis is defined as a vertical defect between the rectus muscles.
With tension of the abdominal press, a longitudinal protrusion is observed in the diastasis zone. Such a protrusion is especially noticeable if the patient in the supine position is asked to raise her head and legs. If necessary, you can measure the width of the defect simply with a ruler. nine0007
Ultrasound may be the most accurate diagnostic method. With ultrasound, the inner edges of the rectus muscles are clearly visible and the distance between them at different levels can be measured.
Computed tomography is used in the diagnosis of diastasis extremely rarely, mainly in scientific research.
For the diagnosis of symphysiopathy and diastasis pubis there is no one test as a "gold standard".
The first place, of course, is the questioning and examination of the patient. We pay attention to the gait of the pregnant woman, to how she sits down, lies down and how she gets up. Symphysiopathy is characterized by a “duck gait”, when a pregnant woman rolls from foot to foot. On palpation in the area of the womb, pain and swelling are noted. The so-called pain provocative tests are used, for example, a mat-test (pulling up an imaginary rug, mat with your foot towards you). nine0007
The following questionnaires are used to assess quality of life, pain and disability: Health-Related Quality of Life (HRQL), Oswestry Disability Index (ODI), Disability Rating Index (DRI), Edinburgh Postpartum Depression Scale (EPDS), Pregnancy Mobility Index (PMI), and Pelvic Ring Score (PGQ).
Of the instrumental methods, ultrasound is the most widely used, less often computed or magnetic resonance imaging. Ultrasound allows you to assess the condition of the ligaments of the pubic joint and the interpubic disc, the severity of the changes and the risk of natural childbirth.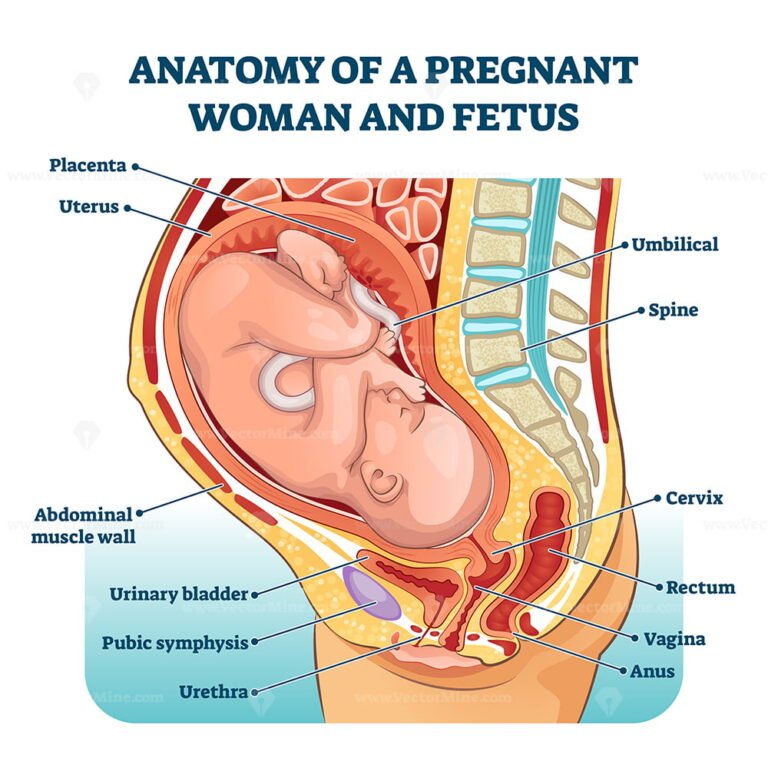 nine0007
nine0007
— What is the treatment for diastasis recti or pubis?
— Primary prevention: when planning and during pregnancy, it is necessary to strengthen all muscle groups of the pelvic girdle, as well as the pelvic diaphragm.
More often, diastasis of the rectus muscles disappears on its own during the first months after childbirth. Special physical exercises to correct the work of muscles, to tone them and restore their basic functions should be performed under the guidance of a competent instructor. There are types of physical exercises that can, on the contrary, worsen the situation with diastasis of the rectus abdominis muscles. In some cases, when there is no effect from physiotherapy exercises, it is necessary to resort to surgical correction of the defect. Currently, both endoscopic and open surgery are practiced. The choice of method depends on the size and localization of the defect. nine0007
With symphysiopathy, therapeutic exercises reduce lumbar and pelvic pain.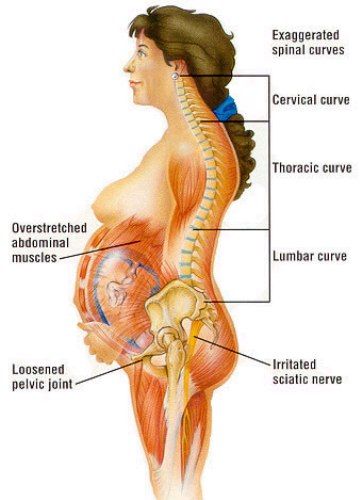 Acupuncture and wearing a pelvic bandage have a positive effect on symphysiopathy.
Acupuncture and wearing a pelvic bandage have a positive effect on symphysiopathy.
Initial treatment of pubic symphysis should be conservative even if symptoms are severe. Treatment includes bed rest and the use of a pelvic brace or corset that tightens the pelvis. Early appointment of physiotherapy with dosed therapeutic exercises will help to avoid complications associated with prolonged immobilization. Walking should be done with assistive devices such as walkers. nine0007
In most cases (up to 93%), the symptoms of dysfunction of the pelvic ring, including the pubic joint, progressively subside and completely disappear six months after birth. In other cases, it persists, becoming chronic. However, if the diastasis exceeds 40 mm, then surgical treatment may be required. Most studies recommend surgery only after failure of conservative treatment, inadequate enlargement of diastasis, or its recurrence. Several procedures have been described, including external fixation and open reduction of the pubic bones with internal fixation.