Signs of constipation in toddlers
Symptoms & Causes of Constipation in Children
What are the symptoms of constipation in children?
Symptoms of constipation in children may include your child
- having fewer than two bowel movements a week
- passing stools that are hard, dry, or lumpy
- having stools that are difficult or painful to pass
- telling you that he or she feels that not all stool has passed
- changing positions to avoid or delay having a bowel movement, including
- standing on tiptoes and then rocking back on his or her heels
- clenching his or her buttocks
- doing unusual, dancelike movements
- having a swollen abdomen, or bloating
- having daytime or nighttime wetting
- having stool in his or her underwear that looks like diarrhea
If your child avoids or delays having a bowel movement, he or she may develop a fecal impaction.
When should my child see a doctor?
Your child should see a doctor if his or her symptoms last for more than 2 weeks or do not go away with at-home treatment.
Take your child to a doctor right away if he or she has constipation and any of the following symptoms
- bleeding from his or her rectum
- blood in his or her stool
- bloating
- constant pain in his or her abdomen
- vomiting
- weight loss
What causes constipation in children?
Children most often get constipated from holding in their stool to avoid or delay having a bowel movement. When stool stays too long in the colon, the colon absorbs too much fluid from the stool. Then the stool becomes hard, dry, and difficult to pass. Learn more about the digestive system and how it works.
Your child may delay or avoid a bowel movement because he or she
- feels stressed about potty training
- feels embarrassed to use a public bathroom
- does not want to interrupt playtime
- fears having a painful or an unpleasant bowel movement

Certain medicines
Medicines and dietary supplements that can make constipation in children worse include
- antacids that contain aluminum and calcium
- anticholinergics and antispasmodics
- anticonvulsants—used to prevent seizures
- iron supplements
- narcotic pain medicines
- some medicines used to treat depression
Certain health and nutrition problems
Certain health and nutrition problems can cause constipation in children
- not eating enough fiber
- not drinking enough liquids or dehydration
- Hirschsprung disease
- celiac disease
- disorders that affect your brain and spine, such as spina bifida
- spinal cord or brain injuries
- conditions that affect their metabolism, such as diabetes
- conditions that affect their hormones, such as hypothyroidism
- problems that can block or narrow the colon or rectum, including tumors
Last Reviewed May 2018
Share this page
Facebook Twitter Email WhatsApp LinkedIn Reddit Pinterest
Previous: Definition & Facts
Next: Diagnosis
This content is provided as a service of the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), part of the National Institutes of Health. The NIDDK translates and disseminates research findings to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
The NIDDK translates and disseminates research findings to increase knowledge and understanding about health and disease among patients, health professionals, and the public. Content produced by the NIDDK is carefully reviewed by NIDDK scientists and other experts.
Constipation in Children | Johns Hopkins Medicine
What is constipation?
Constipation is when a child has very hard stools, and has fewer bowel movements than he or she normally does. It is a very common GI (gastrointestinal) problem.
Signs that a child has constipation include:
- Having fewer bowel movements than normal. Constipation is often defined as having fewer than 3 bowel movements a week. The number of bowel movements may be different for each child. But a change in what is normal for your child may mean there is a problem.
- Passing stool that is hard and sometimes large
- Having bowel movements that are difficult or painful to push out
What causes constipation?
Stool gets hard and dry when the large intestine (colon) takes in (absorbs) too much water.
Normally, as food moves through the colon, the colon absorbs water while it makes stool. Muscle movements (contractions) push the stool toward the rectum. When the stool gets to the rectum, most of the water has been soaked up. The stool is now solid.
If your child has constipation, the colon's muscle movements are too slow. This makes the stool move through the colon too slowly. The colon absorbs too much water. The stool gets very hard and dry.
Once a child becomes constipated, the problem can quickly get worse. Hard, dry stools can be painful to push out. So the child may stop using the bathroom because it hurts. Over time, the colon will not be able to sense that stool is there.
There are many reasons why a child may become constipated. Some common diet and lifestyle causes include:
Diet
- Eating too many foods that are high in fat and low in fiber. These include fast foods, junk foods, and soft drinks.
- Not drinking enough water and other fluids
- Having a change in diet.
 This includes when babies change from breastmilk to formula, or when they start eating solid foods.
This includes when babies change from breastmilk to formula, or when they start eating solid foods.
Lack of exercise
- Children who watch a lot of TV and play video games don’t get enough exercise. Exercise helps move digested food through the intestines.
Emotional issues
- Not wanting to use public bathrooms. Children may then hold in their bowel movements, causing constipation.
- Going through toilet training. This can be a difficult time for many toddlers.
- Having power struggles with parents. Toddlers may hold in their bowel movements on purpose.
- Feeling stressed because of school, friends, or family
Busy children
- Some children don’t pay attention to signals that their body gives them to have a bowel movement. This can happen when children are too busy playing. They forget to go to the bathroom.
- Constipation can also be a problem when starting a new school year.
 Children can’t go to the bathroom whenever they feel the need. They have to change their bowel routine.
Children can’t go to the bathroom whenever they feel the need. They have to change their bowel routine.
Underlying physical problem
In rare cases, constipation can be caused by a larger physical problem. These physical issues can include:
- Problems of the intestinal tract, rectum, or anus
- Nervous system problems, such as cerebral palsy
- Endocrine problems, such as hypothyroidism
- Certain medicines, such as iron supplements, some antidepressants, and narcotics such as codeine
What are the symptoms of constipation?
Symptoms can occur a bit differently in each child. They may include:
- Not having a bowel movement for a few days
- Passing hard, dry stools
- Having belly (abdominal) bloating, cramps, or pain
- Not feeling hungry
- Showing signs of trying to hold stool in, such as clenching teeth, crossing legs, squeezing buttocks together, turning red in the face
- Small liquid or soft stool marks on a child's underwear
The symptoms of constipation can be like other health conditions. Make sure your child sees his or her healthcare provider for a diagnosis.
Make sure your child sees his or her healthcare provider for a diagnosis.
How is constipation diagnosed?
The healthcare provider will ask about your child’s symptoms and health history. He or she will give your child a physical exam. Depending on how old your child is, you might be asked questions such as:
- How old was your baby when he or she had their first stool?
- How often does your child have a bowel movement?
- Does your child complain of pain when having a bowel movement?
- Have you been trying to toilet train your toddler lately?
- What foods does your child eat?
- Have there been any stressful events in your child's life lately?
- How often does your child poop in his or her pants?
Your child’s provider may also want to do some tests to see if there are any problems. These tests may include:
- Digital rectal examination (DRE). Your child’s provider puts a gloved, greased (lubricated) finger into your child’s rectum.
 The provider will feel for anything abnormal.
The provider will feel for anything abnormal. - Abdominal X-ray. This test checks how much stool is in the large intestine.
- Barium enema. This is an X-ray exam of the rectum, the large intestine, and the lower part of the small intestine. Your child will be given a metallic fluid called barium. Barium coats the organs so they can be seen on an X-ray. The barium is put into a tube and inserted into your child’s rectum as an enema. An X-ray of the belly will show if your child has any narrowed areas (strictures), blockages (obstructions), or other problems.
- Anorectal manometry. This test checks the strength of the muscles in the anus and the nerve reflexes. It also checks your child’s ability to sense that the rectum is full (rectal distension) and a bowel movement is needed. And it looks at how well the muscles work together during a bowel movement.
- Rectal biopsy. This test takes a sample of the cells in the rectum.
 They are checked under a microscope for any problems.
They are checked under a microscope for any problems. - Sigmoidoscopy. This test checks the inside of part of the large intestine. It helps to find out what is causing diarrhea, belly pain, constipation, abnormal growths, and bleeding. A short, flexible, lighted tube (sigmoidoscope) is put into your child’s intestine through the rectum. This tube blows air into the intestine to make it swell. This makes it easier to see inside.
- Colorectal transit study. This test shows how well food moves through your child’s colon. The child swallows pills (capsules) filled with small markers that can be seen on an X-ray. The child eats a high-fiber diet for the next few days. X-rays will be taken 3 to 7 days after your child takes the pills. The X-rays will show how the pills moved through the colon.
- Colonoscopy. This test looks at the full length of the large intestine. It can help check for abnormal growths, red or swollen tissue, sores (ulcers), and bleeding.
 The test uses a long, flexible, lighted tube (colonoscope). The tube is put into your child’s rectum up into the colon. This tube lets the provider see the lining of the colon and take out a tissue sample (biopsy) to test it. The provider may also be able to treat some problems that are found.
The test uses a long, flexible, lighted tube (colonoscope). The tube is put into your child’s rectum up into the colon. This tube lets the provider see the lining of the colon and take out a tissue sample (biopsy) to test it. The provider may also be able to treat some problems that are found. - Lab testing. Several tests may be done. These include tests to check for issues such as celiac disease, urinary tract infection, thyroid problems, metabolic problems, and blood lead level.
How is constipation treated?
Treatment will depend on your child’s symptoms, age, and general health. It will also depend on how severe the condition is.
Treatment may include diet and lifestyle changes, such as:
Diet changes
Often making changes in your child's diet will help constipation. Help your child to eat more fiber by:
- Adding more fruits and vegetables
- Adding more whole-grain cereals and breads. Check the nutrition labels on food packages for foods that have more fiber.

| Foods | Moderate fiber | High fiber |
| Bread | Whole-wheat bread, granola bread, wheat bran muffins, whole-grain waffles, popcorn | |
| Cereal | Bran cereals, shredded wheat, oatmeal, granola, oat bran | 100% bran cereal |
| Vegetables | Beets, broccoli, Brussels sprouts, cabbage, carrots, corn, green beans, green peas, acorn and butternut squash, spinach, potato with skin, avocado | |
| Fruits | Apples with peel, dates, papayas, mangoes, nectarines, oranges, pears, kiwis, strawberries, applesauce, raspberries, blackberries, raisins | Cooked prunes, dried figs |
| Meat substitutes | Peanut butter, nuts | Baked beans, black-eyed peas, garbanzo beans, lima beans, pinto beans, kidney beans, chili with beans, trail mix |
Other diet changes that may help include:
- Having your child drink more fluids, especially water
- Limiting fast foods and junk foods that are often high in fats.
 Offer more well-balanced meals and snacks instead.
Offer more well-balanced meals and snacks instead. - Limiting drinks with caffeine, such as soda and tea
- Limiting whole milk as directed by your child’s healthcare provider
It’s also a good idea to have your child eat meals on a regular schedule. Eating a meal will often cause a bowel movement within 30 to 60 minutes. Serve breakfast early. This will give your child time to have a bowel movement at home before rushing off to school.
Get more exercise
Having your child get more exercise can also help with constipation. Exercise helps with digestion. It helps the normal movements the intestines make to push food forward as it is digested. People who don’t move around much are often constipated. Have your child go outside and play rather than watch TV or do other indoor activities.
Good bowel habits
Try to get your child into a regular toilet habit. Have your child sit on the toilet at least twice a day for at least 10 minutes. Try to do this just after a meal. Be sure to make this a pleasant time. Don’t get mad at your child for not having a bowel movement. Use a reward system to make it fun. Give stickers or other small treats. Or make posters that show your child's progress.
Try to do this just after a meal. Be sure to make this a pleasant time. Don’t get mad at your child for not having a bowel movement. Use a reward system to make it fun. Give stickers or other small treats. Or make posters that show your child's progress.
In some cases these changes may not help. Or your child’s healthcare provider may detect another problem. If so, the provider may recommend using laxatives, stool softeners, or an enema. These products should only be used if recommended by your child's provider. Do not use them without talking with your child's provider first.
What are the complications of constipation?
Hard stools can irritate or tear the lining of the anus (anal fissures). This makes it painful to have a bowel movement. Your child may avoid having a bowel movement because it hurts. This can make constipation get worse.
Can constipation be prevented?
Constipation can be prevented by figuring out the times when it may occur, and making proper changes.
For instance, when babies start to eat solid food, constipation can result. This is because they don’t have enough fiber in their new diet. You can add fiber to your baby’s diet by giving pureed vegetables and fruits. Or try whole-wheat or multigrain cereals.
Constipation can also happen during toilet training. Children who do not like using a regular toilet may hold in their stool. This causes constipation.
All children should get the right amount of fiber and fluids. Other preventative measures include making sure your child has:
- Regular access to a bathroom
- Enough time to use the toilet
- Regular physical exercise
The same changes that can help treat constipation may also help to stop it from happening.
Living with constipation
Constipation can be either short-term (acute) or long-term (chronic). Children with intestinal diseases may have chronic constipation problems. But in most cases, constipation is a short-term condition. If your child has chronic constipation, work with his or her healthcare provider. Together you can create a care plan that is right for your child.
If your child has chronic constipation, work with his or her healthcare provider. Together you can create a care plan that is right for your child.
When should I call my child's healthcare provider?
Call your child's healthcare provider if you have any questions or concerns about your child's bowel habits or patterns. Talk with your child's provider if your child:
- Is constipated for more than 2 weeks
- Can’t do normal activities because of constipation
- Can’t get a stool out with normal pushing
- Has liquid or soft stool leaking out of the anus
- Has small, painful tears in the skin around the anus (anal fissures)
- Has red, swollen veins (hemorrhoids) in the rectum
- Has belly pain, fever, or vomiting
Key points about constipation
- Constipation is when a child has very hard stools, and has fewer bowel movements than they normally do.
- Constipation can be caused by a child’s diet, lack of exercise, or emotional issues.
- Once a child becomes constipated, the problem can quickly get worse.
- Making diet and lifestyle changes can help treat and help prevent constipation.
- Never give your child an enema, laxative, or stool softener unless the healthcare provider recommends this.
Next steps
Tips to help you get the most from a visit to your child’s health care provider:
- Before your visit, write down questions you want answered.
- At the visit, write down the names of new medicines, treatments, or tests, and any new instructions your provider gives you for your child.
- If your child has a follow-up appointment, write down the date, time, and purpose for that visit.
- Know how you can contact your child’s provider after office hours. This is important if your child becomes ill and you have questions or need advice.
Constipation in children. Prevention. Diet therapy
home
Articles
Health
Sabitova Vasily Ilyasovna Gastroenterologist
06/21/2019
Constipation is widespread among both adults and children (5-30% depending on the diagnostic criteria). Symptoms become chronic in more than 30% of patients, not only cause discomfort and pain to the child himself, but also disrupt the quality of life of his family.
Symptoms become chronic in more than 30% of patients, not only cause discomfort and pain to the child himself, but also disrupt the quality of life of his family.
CONSTIPATION - a condition manifested by an increase in the intervals between bowel movements (compared to the individual norm) or systematically slow, difficult and / or insufficient bowel movements. Constipation also includes stools with “gruel”, but after defecation was absent for up to 3 days.
Constipation can be related to functional or organic causes (abnormalities, inflammation). In children, 90-95% of constipation is functional. The peak incidence of functional constipation falls on 2-4 years, when they begin to accustom the child to the potty / toilet.
Main causes of functional constipation
- Pain
- Fever
- Dehydration
- Wrong diet of a nursing mother
- Insufficient drinking regime of a child with artificial feeding
- Insufficient drinking regimen of a breast-fed child with the introduction of complementary foods
- Early transition of the child to artificial feeding
- Fast transition of the baby from one mixture to another (less than 7 days)
- Irrational nutrition of the child (for a long time the child receives food with a large amount of proteins, fats and insufficient dietary fiber, abuse of drinks containing a large amount of astringents - tea, coffee, cocoa)
- Excessive use of baby hygiene products or the development of an allergic reaction of the skin of the perianal area
- Consequences of perinatal injuries of the nervous system
- Rickets, vitamin D deficiency
- Anemia
- Impaired thyroid function (deficiency - hypothyroidism)
- Food allergy, especially cow's milk protein allergy
- Forced potty training, period of adaptation to new conditions (nursery, kindergarten)
- Physical inactivity - a sedentary lifestyle
- Mental trauma or stress
- Systematic suppression of the urge to empty the bowels, associated, for example, with the beginning of attending a kindergarten, school, etc.
- Taking certain drugs
- Constipation in family members
Frequency of defecation in children of different ages
| Age | Number of bowel movements per week | Number of bowel movements per day |
| 0 – 3 months breastfeeding artificial feeding | 5 - 40 5 - 20 | 2.9 2.0 |
| 6 - 12 months | 5 - 28 | 1.8 |
| 1 - 3 years | 4-21 | 1.4 |
| 4 years and older | 3 - 14 | 1.0 |
In addition to the frequency of the chair, you should pay attention to its nature. For a more objective assessment, the “Bristol fecal shape scale” is convenient, since it is the shape of the feces, and not the frequency of the stool, that is more consistent with the time of intestinal transit.
Bristol stool chart
In accordance with this scale, 3 and 4 form of feces is regarded as normal, and 1 and 2 indicate delayed transit (constipation). Quite often, in practice, there are situations when a child has a bowel movement frequency within the normal range, but the stool is dense, fragmented, in a meager amount. These signs indicate incomplete emptying of the bowels and are considered as manifestations of constipation.
The consistency of the stool in newborns and infants should be mushy. From 6 months to 1.5 - 2 years, feces can be both formalized and mushy. From the age of two, the chair must be decorated.
Signs and symptoms of constipation
- abdominal pain, often bursting, aching, sometimes colicky
- bloating
- change in the shape and consistency of the stool
- excessive flatulence
- unpleasant smell of flatus and stool
- may have pain during bowel movements
- straining during bowel movements
- there may be blood in the stool - on the surface of the feces or in the form of traces on a napkin (indicates an anal fissure)
If you do not eliminate constipation and do not establish bowel movements, then there is a risk of coprostasis (formation of fecal stones) and fecal intoxication:
- loss of appetite
- lack of energy
- general malaise
- depression, irritability
- nausea, vomiting
- skin symptoms - dryness, rash, peeling
- fecal incontinence, stool spotting
- urinary retention and incontinence due to pressure from a crowded bowel on the bladder
- bleeding from fissures, hemorrhoids
The treatment of constipation involves the following goals:
1. Normalization of stool consistency (soft, painless stools)
Normalization of stool consistency (soft, painless stools)
2. Regularity of bowel movements (prevention of re-accumulation of feces)
The treatment of constipation is a sequential, complex, individual process and consists of several stages:
- child and parent education
- correction of nutrition and drinking regimen
- elimination of existing coprostasis with the help of medications
- maintenance therapy
It is necessary to exclude factors that provoke and contribute to constipation (normalization of motor and nutritional regimen, discontinuation of medications that can cause constipation, identification of a food allergen, exclusion or confirmation of neuromuscular disease, celiac disease, etc.).
Lifestyle normalization includes:
- development of a conditioned reflex
- active lifestyle
- gymnastics
- light abdominal massage training
- for small children - laying out on the stomach, bending the legs to the stomach.
Education is the first step in the treatment of functional constipation. It must be remembered that episodes of fecal smearing and encopresis (fecal incontinence) are not arbitrary and should not be blamed on the child, who may already be frightened and disoriented. In some cases, when the intra-family situation is difficult, the help of a family psychologist may be needed.
It is important to understand that the treatment of functional constipation can be lengthy, based on trust, partnership and requires patience. Modern laxatives that are legal in children will not make the intestines “lazy”, will not cause “addiction”, they enter the bloodstream in minimal amounts or are not absorbed at all and are safe for long-term use.
Correction of the behavior of a child with constipation is based on the development of a routine of visiting the toilet, in order to achieve regular defecation. Defecation should be every time at the same time. The urge to defecate is based on the gastrocecal reflex, which manifests itself in the morning 1 hour after eating. A child with constipation needs to spend 3-10 minutes in the toilet (depending on age). It is necessary to plant the child on a potty or offer to visit the toilet after each meal.
A child with constipation needs to spend 3-10 minutes in the toilet (depending on age). It is necessary to plant the child on a potty or offer to visit the toilet after each meal.
A prerequisite for effective defecation is to provide a good support for the legs (a low bench on which the child can put his feet), which helps to increase intra-abdominal pressure.
If the defecation is not successful, the child should never be punished and vice versa. The daily frequency of bowel movements can be noted in a diary, which can be analyzed at a scheduled visit to the doctor.
Treatment of constipation should begin with lifestyle changes, which include dietary modification, drinking regimen and physical activity.
Calculation of fluid volume for healthy children
Children under the age of 1 year should drink at least 100 ml of water per day.
For healthy children weighing 10 to 20 kg the water requirement is calculated using the formula:
100 ml (volume of water for children under 1 year old) + 50 ml per kg for body weight over 10 kg.
For example, with a mass of 12 kg: 100 ml + 2 x 50 ml = 200 ml.
A child weighing 20 kg should drink water: 100 ml + 50 x 10 = 600 ml
For children weighing over 20 kg the following formula is suggested for calculation:
600 ml (volume of water for a child weighing 20 kg) + 20 ml for each kg over 20 kg.
For children over 3-5 years old you can use the calculation of the amount of water: 30ml / kg of weight
Principles of diet therapy for constipation:
- satisfaction of physical needs for nutrients and energy
- exclusion of excessive consumption of proteins and fats, which can inhibit intestinal motility
- enrichment of the diet with dietary fiber
- normalization of intestinal microflora with pro- and prebiotics
If the child is breastfed, then the mother's nutrition is corrected (restriction of products that promote gas formation). With artificial feeding, special mixtures are shown. For constipation associated with an allergy to cow's milk protein, therapeutic mixtures are prescribed if the child is bottle-fed. If the child is breastfed, cow's milk and products based on it are completely excluded from the mother's diet.
For constipation associated with an allergy to cow's milk protein, therapeutic mixtures are prescribed if the child is bottle-fed. If the child is breastfed, cow's milk and products based on it are completely excluded from the mother's diet.
After the introduction of “thick” complementary foods, boiled water is necessary for all children, regardless of the type of feeding.
For older children, it is recommended to eat foods rich in vegetable fibers. It is not recommended to “smear food”, puree, “snacks”, “eating on the go”. Food should be crumbly, meat / poultry / fish - “piece”. A “bulk” breakfast is required to stimulate the “gastrocecal reflex”.
The main source of coarse-fiber vegetable fiber, containing a large amount of dietary fiber, is cereal bran, rye bread, as well as a number of vegetables and fruits. According to the principles of evidence-based medicine, a statistically significant increase in stool frequency and improvement in its consistency was demonstrated with the use of fiber compared with placebo.
Bran, as the main source of vegetable fiber, is recommended to be added to the second and third courses, after pouring boiling water over it and settling for 20 minutes. Bran can also be used in between meals, drinking plenty of fluids. For school-age children, the total amount of fluid when taking bran should be at least 1.5-2 liters per day, otherwise they mainly act as sorbents, absorbing fluid from the intestines, thereby increasing constipation. The dose is selected individually, it is recommended to start with 1 teaspoon 2-3 times a day, with a gradual increase to 40 g per day. When the effect is achieved, the dose is reduced and limited to one dose.
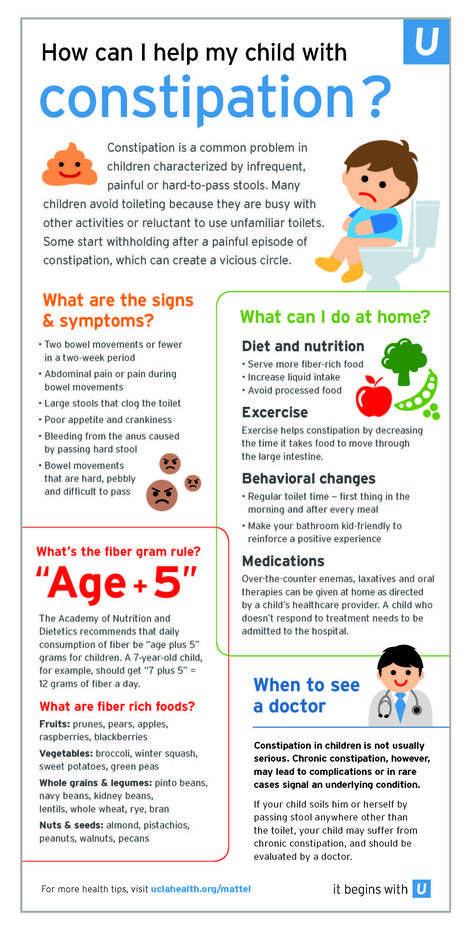
The American Academy of Pediatrics (2009) recommends a fiber intake of 0.5 g/kg/day (maximum 35 g/day) for all children. Fiber intake below the minimum recommended value has been shown to be a risk factor for chronic constipation in children.
However, long-term intake of a large amount of plant fibers due to fermentation by intestinal microflora is naturally accompanied by bloating and flatulence.
Children with constipation are shown to take cool liquids on an empty stomach (drinking and mineral water, juice, compotes, kvass), to enhance the laxative effect, it is possible to add honey, xylitol or sorbitol. It is very beneficial for bowel function to increase the intake of juices containing sorbitol/sorbitol, such as juice from plums, pears, apricots, peaches and apples,
With “sluggish” bowel function (hypomotor constipation), cool mineral water of medium and high mineralization is used, such as Essentuki 17, Batalinskaya, Arzni, Donat Magnesium, etc.; with spastic constipation (hypermotor constipation, stool form more often type 1) - warm and low mineralization (Essentuki 4). Calculation of mineral water - 3-5 ml / kg per day.
It is necessary to limit milk in its pure form and in dishes, as flatulence may occur with the appearance or intensification of abdominal pain. It is better to replace whole milk with sour-milk products - kefir, acidophilus, yogurt, yogurt, etc.
The diet of children with constipation includes dishes rich in vegetable fiber - salads from fresh vegetables, greens 2-3 times a day, baked apples, stewed vegetables, diluted vegetable and fruit juices with pulp. Food is cooked mostly unground, steamed or boiled in water.
It is preferable to take raw vegetables and fruits (in the absence of contraindications). Especially recommended are tomatoes, zucchini, pumpkin, carrots, beets, lettuce, cauliflower, apples. Dried fruits (prunes, dried apricots, figs) are given in soaked form and as part of cooked dishes. White cabbage, young green beans, green peas are allowed with good tolerance. Parsley, dill, celery are good to add to various dishes and salads.
If after reading the article you still have questions or you do not understand how to apply the recommendations in your particular case, we invite you and your child to be examined by a pediatric gastroenterologist at the DDC. For the convenience of parents, you can make an appointment with a pediatric gastroenterologist at the Children's Diagnostic Center on a weekday and on Saturdays.
We will be happy to help!
Who gets a tan, who gets a blow!
If a child has a fever, what should I do?
Return to the list
Features of constipation in children: what are the signs to look out for | Therapeutic diet
Author, editor and medical expert - Klimovich Elina Valerievna.
Views: 512 644
Last update date: 10.2022 G.
Average reading time: 17 minutes
Content:
- Symptoms
- Causes of constipation in children
- Varieties of constipation
- Organic or primary constipation
- Function locks 5
- Psychological constipation in children
- Transient constipation
- Treatment of childhood constipation
- Therapeutic diet
- Day mode
- Treatment of constipation in children with MICROLAX ®
Constipation (from Latin constipatio - congestion, piling up) in a child can occur at any age 1, 3 . It is associated with a slowdown in the movement of feces through the intestines 3, 4 . This is one of the most common "children's" problems 4 , but many parents do not recognize it or believe that a child at 3 or 4 years old will "go away" without medical help. Some parents do not go to the doctor in time also because 3, 5 , they cannot understand whether the baby goes to the toilet often enough, whether the density and volume of feces are normal 1, 3, 5 .
It is associated with a slowdown in the movement of feces through the intestines 3, 4 . This is one of the most common "children's" problems 4 , but many parents do not recognize it or believe that a child at 3 or 4 years old will "go away" without medical help. Some parents do not go to the doctor in time also because 3, 5 , they cannot understand whether the baby goes to the toilet often enough, whether the density and volume of feces are normal 1, 3, 5 .
Back to top
Symptoms
A child after 2 years of age may tell or show 3, 4 parents that he cannot go to the toilet or is in pain. But to recognize constipation in an infant at 1.5 - 2 years is not so easy 3, 4, 5 .
In the case of infants, doctors recommend focusing not on the frequency of stools, which varies greatly in infants 3.4 , but on the density of feces and the behavior of the baby during defecation 1, 4 .
If during defecation he does not cry, the stool passes gently, has a characteristic appearance and color 1, 4 , the tummy does not become dense, as if inflated, then it is considered that the infant does not have constipation, even if he soils the diaper 2 times per week 1, 4 .
It is possible to speak about probable constipation in an infant if the feces become denser, thicker, darker than usual 1, 4 . In children under one year old, the tummy is often swollen, when pressed on it, they cry or whimper, and at the moment the feces come out, they can tense up, scream 1, 4 .
After a year or more, signs of insufficient defecation are considered:
- The child began to go to the toilet "largely" less often than before 1, 3, 4 .
- During defecation, it is clear that he is in pain, he has to strain 1, 3, 4 .
- Passing less feces than usual 1, 3, 4 .

- Appears dry, hard, dense 1, 3, 4 .
If the child has previously had stool retention and has memorized 5 that it hurts, he begins to cramp his legs, knees, walk on his heels, tighten his buttocks, hold his breath for a short time - wait and suppress the urge. During defecation, it is clear that the process is difficult, and to facilitate it, one has to take different postures 3 , make considerable efforts, push 2 , actively work with the anterior abdominal wall 1, 4 .
If the child had one or more signs of constipation 2-3 times within 2 months 1, 6 , then you need to monitor the nature and frequency of the stool, and if the suspicions are confirmed, then consult a doctor to find a way to help the child with constipation, select a diet and treatment 1, 3 .
The table below provides information 4 on the approximate number of times children of different ages can have a bowel movement, as well as the characteristics of feces.
| Age | How many times a day there is a chair | Color and consistency of feces |
| 0-3 months breastfeeding | 1 to 5-6 times, sometimes up to 1 time in 4-7 days | Viscous, like a semi-liquid porridge. Color - yellow, yellowish green, golden yellow, usually uniform or with white lumps. |
| 0-3 months bottle feeding | 1 to 4 times | Pasty. Color yellow to light brown. |
| 6-12 months | 1-3 times | Soft, shaped or pasty, brown, light brown or dark yellow, brownish greenish. |
| 1-3 years | 1-2 times | Decorated, brown. |
| Over 3 years old | Once a day or at least 3 times a week | Decorated, brown, dark brown. |

Up the content of
Causes of constipation in children
The reasons for the lack of defecation in children are divided by 1, 6 into two groups:
- Organic 3 -arising against the background of any disease, pathology of the intestinal structure.
- Functional 3, 5 . They arise due to improper functioning of the gastrointestinal tract, due to reasons not related to problems of the digestive system.
The walls of the intestine periodically undulate. This is called peristalsis 2, 3 and is necessary to move digested food down and out. If the peristalsis slows down, becomes slow and lethargic, that is, the tone of the intestinal wall decreases, then they speak of atonic constipation 3, 6 . And if the tone becomes so strong that a spasm occurs and peristalsis stops, then such a state is called spastic 3, 6 .
Back to content
Types of constipation
Peristalsis disorders can occur 1, 3, 6 due to many factors.
Organic or primary constipation
In childhood associated with congenital diseases and intestinal disorders 1, 3 . These include Hirschsprung's disease, dolichosigmoid, megacolon, fusion of the rectum, stenosis of the large intestine and rectum, impaired development of the anal sphincter 1, 3, 4 . Stool retention with them is a symptom, a sign that the intestines are not working properly, its normal physiology is disturbed.
Primary stool retention also occurs due to an acquired violation of the structure and shape of the intestine, a decrease in its lumen 1, 2 . This can be caused by polyps, tumors, hemorrhoids, adhesions 3, 6 .
Stool retention in these cases disappears after treatment (if possible) or selection of a method for correcting the disease.
Up to contents
Functional constipation
5 This is the most common type of defecation disorder in children 5 , occurs from exposure to a provocative cause, due to which the intestinal tone is disturbed.
- Intestinal immaturity in young children 1 . Peristalsis is still getting better, the intestine does not immediately respond to food intake. Cal lingers, thickens.
- Eating disorders (alimentary) 1, 3, 5 . If there is not enough water in the daily menu, a lot of flour, cereals, sweets, then few dietary fibers necessary to stimulate peristalsis enter the intestines. As a result, the movement of a lump of feces slows down. In infants, alimentary disorders occur as a result of 4, 5 improper feeding, the introduction of supplementary foods, complementary foods.
- Hereditary tendency. Studies have shown 5 that if the baby's mom or dad suffered from constipation, then their child is more likely to have this problem too.
- Miscellaneous acute and chronic diseases not related to the digestive system 4, 5 .
- Hormonal diseases 1, 5 — congenital hypothyroidism, pheochromocytoma.

- Iron deficiency (anemia) rickets, helminthic invasions 5 .
- Stool retention due to atopy, such as food allergy 1, 5 .
- Dehydration. As a rule, it is associated with a painful state of the body - temperature, heat stroke. Due to lack of water, the feces become dry, move with difficulty through the intestines, linger in the rectum 1, 2, 5 .
- Inactivity. When moving, walking, the muscles of the abdominal cavity actively work and, as it were, massage the intestines, stimulate peristalsis 1, 2, 5 .
- Abuse of enemas, gas tubes 5 . The enema interferes with the natural mechanism of the act of defecation, the nerve endings of the intestine "wean" to respond to irritation, the urge disappears, the baby loses the skill of recognizing them 1, 5 .
- Reception 5 of some drugs that reduce intestinal motility.
Up to content
Psychological constipation in children
This is a functional disorder 5 , but due to the peculiarities of its formation and prevalence, it deserves to be separated into a separate group. For many parents, the absence of stool in a child due to psychological reasons comes as a big surprise 2, 3, 5 .
For many parents, the absence of stool in a child due to psychological reasons comes as a big surprise 2, 3, 5 .
Psychological constipation is called if there are no organic causes, there are no other painful conditions that could cause stool retention 2, 3, 5 . The source of problems with stools are psychological factors, especially the functioning of the nervous system in children.
The nervous system has a vegetative section that regulates the work of all internal organs. If a person is experiencing some kind of difficult situation for him, stress, then the reaction of the autonomic system can cause disturbances in the functioning of the intestines 5 . An example of such a situation is a pet’s illness, moving to a new place of residence, loss of a favorite toy. The child forgets to go to the toilet for several days, the stool becomes thicker, defecation becomes painful, difficult, and the baby begins to consciously avoid it 2, 3, 5 .
Examples of other situations that cause psychogenic constipation:
- The child consciously suppresses the desire to go to the toilet for various reasons 2, 5 home. A few days of such a conscious retention of the stool - and now the feces have thickened, it hurts to go to the potty. The child cannot yet establish a connection between cause and effect; he begins to avoid what caused pain, that is, defecation.
- Rejection of the potty 2, 5 due to unpleasant sensations when planting or rude, persistent attempts to accustom "do things" without fail to the potty with punishment for a mistake.
Another of the psychological reasons causing difficulty in defecation is prolonged exposure to difficult, mentally difficult circumstances 2, 3, 5 . Conflicts in the family, difficulties in relationships in a team or with teachers in a kindergarten or at school, embarrassment to go to the toilet in front of strangers, an uncomfortable bathroom outside the house, memory of past failures (did not have time; did not understand that the process was not yet completed; does not know how to having an intimate toilet after a bowel movement, etc. ) - all this and much more can cause psychological fear of defecation 2, 4, 5 .
) - all this and much more can cause psychological fear of defecation 2, 4, 5 .
Back to content
Transient constipation
Not always stool retention is associated with serious problems. Sometimes it is a transient or one-time retention of feces. It happens infrequently, less than once every 2 or 3 months 1, 4, 6 , and is usually associated with nutritional causes or acute illness: the child drank little for several days, sweated a lot in the heat or at a temperature, ate a lot fixing food - blueberries or bird cherry. After the resumption of fluid intake, correction of the diet, motor skills and stools are restored by themselves 1, 4, 5 .
Back to content
Treatment of constipation in children
Constipation in children requires 6 mandatory treatment. Here are just a few reasons why.
Accumulated feces cause intoxication — poisoning with decay products 3, 6 , which begin to be absorbed back into the blood, the child becomes restless or lethargic, his appetite, mood, physical activity decrease.
In case of intestinal disorders, food is poorly digested 3, 6 . The body does not receive the necessary nutrients, vitamins, minerals, and this is one of the reasons for the decrease in protective forces, the development of anemia 5, 6 .
Prolonged absence of stool causes constant discomfort, abdominal pain, physical and mental development of the child may be disturbed 3, 6 .
Due to the impossibility or difficulty of controlling urge and defecation, the development of 3, 4, 6 encopresis is likely - fecal incontinence. With it, small particles of feces involuntarily, at any time, come out, stain clothes 3, 6 . Encopresis becomes a powerful stress, exacerbates psychological problems.
If the feces are not excreted for a long time, then it stretches the intestinal walls, which increases the risk of developing rectal fissures, hemorrhoids, bleeding, inflammation of the large intestine 3, 6 .
The goal of treatment is to restore peristalsis, normalize the density and quantity of feces, frequency of defecation 2, 4, 6
other diseases, complaints, duration of the condition. The treatment consists of 1, 2, 6 :
- Correction of an existing disease.
- Development of a therapeutic diet.
- Organizations of a healthy lifestyle, including exercise therapy.
- Medical therapy.
The examination found that the child has constipation: what to do? If the cause is associated with any disease, then measures will be taken to treat it and at the same time a method will be selected to normalize the frequency of stools, taking into account the disease and other characteristics of the body.
Back to content
Therapeutic diet
One of the first therapeutic measures was the diet 4, 6 . Proper nutrition makes the feces softer, facilitates its movement, stimulates peristalsis. If it does not hurt during bowel movements, then the fear of having to go to the pot (to the toilet) will decrease or disappear.
If it does not hurt during bowel movements, then the fear of having to go to the pot (to the toilet) will decrease or disappear.
Nutrition should be appropriate for the age and needs of the growing organism. Breastfeeding should be continued, and for children on artificial or mixed feeding, the doctor will help you choose therapeutic and prophylactic mixtures, which include additives that normalize stool 1, 4, 6 .
Foods that stimulate peristalsis are recommended for feeding: pumpkin, squash, squash, Brussels sprouts and cauliflower, apricot puree, prunes 1, 2, 6 .
And if a child is one year old or older with constipation, what should be done with nutrition?
It is necessary to give a lot of clean water to drink - but not compotes, not juices. Water helps to soften accumulated feces, stimulates peristalsis 1, 2, 6 .
Bran, wholemeal bread, oatmeal and buckwheat support normal intestinal motility, accelerate the passage of stool 1, 2, 6 .
The diet must include fresh vegetables and fruits, foods high in fiber. However, sweet apples, bananas, blueberries, berry and fruit jelly do not give due to their astringent properties, the ability to make the feces dense 1, 2, 6 .
It is necessary to reduce to a minimum (or better to exclude) the consumption of sweets that slow down the work of the intestines, flour products, refined products 1, 2, 6 .
Whole milk, cereals on it, especially semolina and rice should be abandoned - they make the feces thick and the peristalsis sluggish 1, 2, 6 .
Cocoa, black and green tea, chocolate, coffee reduce intestinal activity, promote stool retention 1, 2, 4, 6 .
Peas and beans, white cabbage, grapes, pears, fresh onions are not recommended. These vegetables provoke gas formation, abdominal pain 1, 2, 4 .
As a basis for rational nutrition, it is possible to prescribe one of the therapeutic diets - table No. 3 or No. 4 according to Pevzner 1, 2, 4, 6 .
3 or No. 4 according to Pevzner 1, 2, 4, 6 .
Top of page
Daily routine
Daily routine, the habit of doing everything you need every day helps to normalize the work of the autonomic nervous system, instill the need for regular bowel movements at about the same time.
In the morning on an empty stomach, while still in bed, the child should be allowed to drink from 50 to 150 ml of clean drinking water at room temperature, and after 15-20 minutes have breakfast - just enough time to get dressed, wash, do exercises 1, 2, 4 .
After eating, you should try to induce a bowel movement, if the doctor allows, then with auxiliary means - enema, laxatives. Parents can develop a reward system for successful toilet visits, but there is no need to scold them for failure 1, 3, 4, 6 .
Children should move according to their abilities and age, play active games, walk. Useful cycling, skating and skiing, swimming, ball games. Your doctor or exercise therapist will advise you on suitable gymnastics or physical therapy exercises 1, 2, 4, 6 .
Your doctor or exercise therapist will advise you on suitable gymnastics or physical therapy exercises 1, 2, 4, 6 .
Top of page
Treatment of constipation in children with MICROLAX
®Drugs prescribed by a physician may be used to treat constipation in children 2, 4, 6 .
- Combined enzyme and choleretic preparations for the normalization of the digestive activity of the gastrointestinal tract.
- Prokinetics that restore intestinal motility.
- Spasmolytics for spastic pains 2, 4, 6 .
Laxatives are also included in the treatment of constipation in children. Some of them are taken by mouth, others - in the form of enemas. In childhood, it is recommended to use laxatives that do not irritate the intestinal receptors; do not increase stool volume 3, 6 . They must act quickly and predictably. One of these drugs is Microlax ® . 3, 7
These are microclysters containing sodium citrate, lauryl sulfoacetate and sorbitol. Sodium citrate promotes the displacement of water from the stool and its softening and emulsification, lauryl sulfoacetate dilutes the contents of the intestine and prevents the reverse adhesion of fecal lumps, sorbitol stimulates the flow of water into the intestinal lumen. This combination allows you to achieve softening of the fecal lump and physiologically remove it from the intestines 7 .
Sodium citrate promotes the displacement of water from the stool and its softening and emulsification, lauryl sulfoacetate dilutes the contents of the intestine and prevents the reverse adhesion of fecal lumps, sorbitol stimulates the flow of water into the intestinal lumen. This combination allows you to achieve softening of the fecal lump and physiologically remove it from the intestines 7 .
The action of the drug develops gently, emptying occurs within 5-15 minutes after its administration. Microlax ® can be used as an optimal treatment for acute and chronic constipation in children 3, 7 .
Microlax ® is administered rectally, into the rectum. For children under 3 years of age, Microlax ® with a shortened microclyster tip 47.3 mm long can be used.
The tip is inserted through the anus into the rectum to its full length, the tube is pressed and all its contents are squeezed out. Without opening the tube, remove it 7 .
For use in children and adults use a tube with a 60.6 mm universal tip.
Use it in the same way as for young children 7 .
It is important to follow the regimen and duration of treatment recommended by the doctor: early refusal of therapy makes it ineffective 4, 6 . Neglect of diet and regimen organization may render drug therapy ineffective or require its intensification 6 .
When the desired result is achieved, you should continue to adhere to the formed habits of rational nutrition and drinking regimen, a healthy lifestyle to prevent intestinal disorders in the future.
Back to Contents
The information in this article is for reference only and does not replace professional medical advice.