Severe acid reflux during pregnancy
Indigestion and heartburn in pregnancy
Indigestion, also called heartburn or acid reflux, is common in pregnancy. It can be caused by hormonal changes and the growing baby pressing against your stomach.
You can help ease indigestion and heartburn by making changes to your diet and lifestyle, and there are medicines that are safe to take in pregnancy.
Symptoms of indigestion and heartburn
Symptoms of indigestion and heartburn include:
- a burning sensation or pain in the chest
- feeling full, heavy or bloated
- burping or belching
- feeling or being sick
- bringing up food
Symptoms usually come on soon after eating or drinking, but there can sometimes be a delay between eating and developing indigestion.
You can get symptoms at any point during your pregnancy, but they are more common from 27 weeks onwards.
Things you can do to help with indigestion and heartburn
Changes to your diet and lifestyle may be enough to control your symptoms, particularly if they are mild.
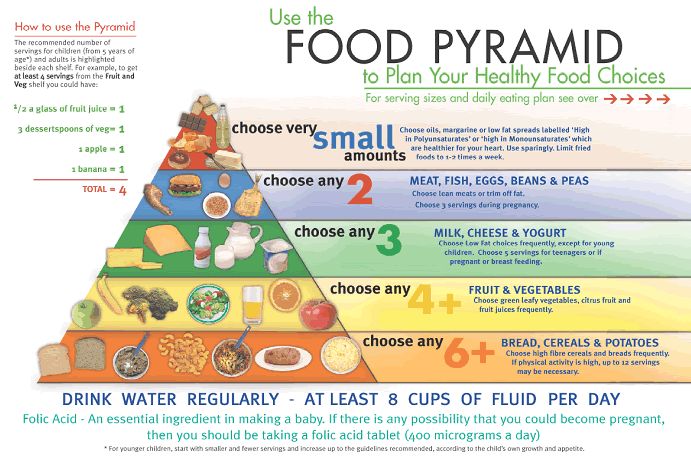
Eat healthily
You're more likely to get indigestion if you're very full.
If you're pregnant, it may be tempting to eat more than you would normally, but this may not be good for you or your baby.
Find out more about a healthy diet in pregnancy and foods to avoid.
Change your eating and drinking habits
You may be able to control your indigestion with changes to your eating habits.
It can help to eat small meals often, rather than larger meals 3 times a day, and to not eat within 3 hours of going to bed at night.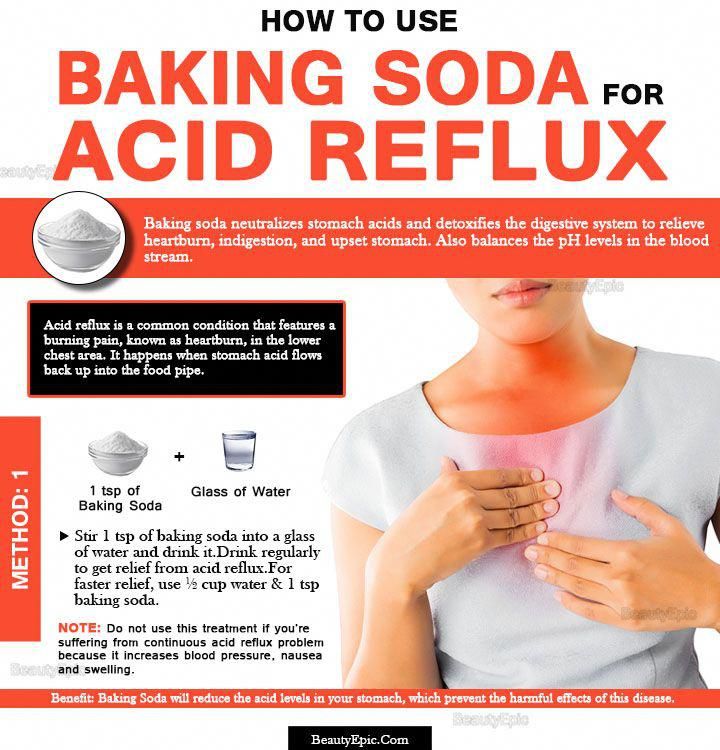
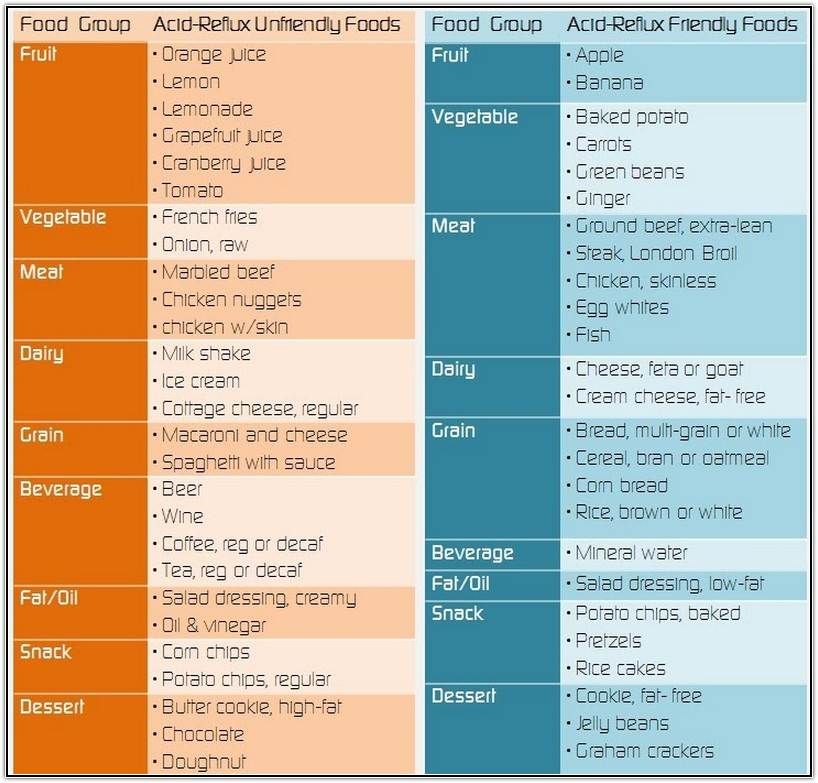
Cutting down on drinks containing caffeine, and foods that are rich, spicy or fatty, can also ease symptoms.
Keep upright
Sit up straight when you eat. This will take the pressure off your stomach. Propping your head and shoulders up when you go to bed can stop stomach acid coming up while you sleep.
Stop smoking
Smoking when pregnant can cause indigestion, and can seriously affect the health of you and your unborn baby.
When you smoke, the chemicals you inhale can contribute to your indigestion. These chemicals can cause the ring of muscle at the lower end of your gullet to relax, which allows stomach acid to come back up more easily. This is known as acid reflux.
Smoking also increases the risk of:
- your baby being born prematurely (before week 37 of your pregnancy)
- your baby being born with a low birthweight
- sudden infant death syndrome (SIDS), or "cot death"
There's lots of help available to stop smoking.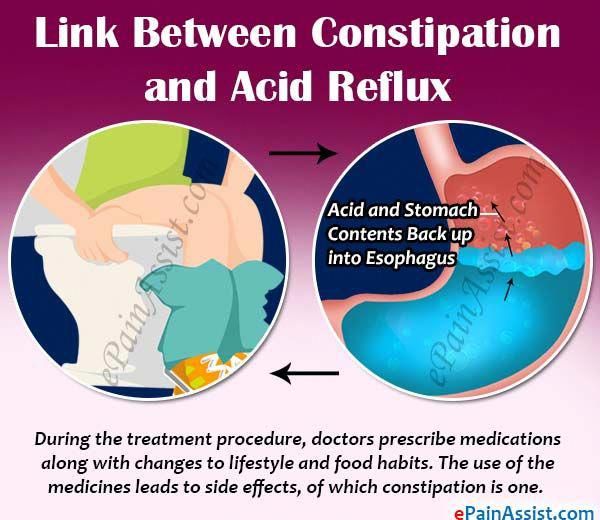 Talk to your midwife or call the NHS Smokefree helpline on 0300 123 1044. Find out more about stopping smoking in pregnancy.
Talk to your midwife or call the NHS Smokefree helpline on 0300 123 1044. Find out more about stopping smoking in pregnancy.
Avoid alcohol
Drinking alcohol can cause indigestion. During pregnancy, it can also lead to long-term harm to the baby. It's safest to not drink alcohol at all in pregnancy.
Find out more about alcohol and pregnancy
When to get medical help
See your midwife or GP if you need help managing your symptoms or if changes to your diet and lifestyle do not work. They may recommend medicine to ease your symptoms.
You should also see your midwife or GP if you have any of the following:
- difficulty eating or keeping food down
- weight loss
- stomach pains
Your midwife or GP may ask about your symptoms and examine you by pressing gently on different areas of your chest and stomach to see whether it's painful.
If you're taking prescription medicines
Speak to your GP if you're taking medicine for another condition, such as antidepressants, and you think it may be making your indigestion worse. They may be able to prescribe an alternative medicine.
Never stop taking a prescribed medicine unless you're advised to do so by your GP or another qualified healthcare professional who's responsible for your care.
Medicines for indigestion and heartburn
Medicines for indigestion and heartburn during pregnancy include:
- antacids – to neutralise the acid in your stomach (some are available over the counter from a pharmacist)
- alginates – to relieve indigestion caused by acid reflux by stopping the acid in your stomach coming back up your gullet
You may only need to take antacids and alginates when you start getting symptoms. However, your GP may recommend taking them before symptoms come on – for example, before a meal or before bed.
However, your GP may recommend taking them before symptoms come on – for example, before a meal or before bed.
If you're taking iron supplements as well as antacids, do not take them at the same time. Antacids can stop iron from being absorbed by your body.
If antacids and alginates do not improve your symptoms, your GP may prescribe a medicine to reduce the amount of acid in your stomach. 2 that are widely used in pregnancy and not known to be harmful to an unborn baby are:
- ranitidine – a tablet you take twice a day
- omeprazole – a tablet you take once a day
Causes of indigestion in pregnancy
Symptoms of indigestion come when the acid in your stomach irritates your stomach lining or your gullet. This causes pain and a burning feeling.
When you're pregnant, you're more likely to have indigestion because of:
- hormonal changes
- the growing baby pressing on your stomach
- the muscles between your stomach and gullet relaxing, allowing stomach acid to come back up
You may be more likely to get indigestion in pregnancy if:
- you had indigestion before you were pregnant
- you've been pregnant before
- you're in the later stages of pregnancy
Video: Eating well on a budget
In this video, a dietitian gives advice on how to eat healthily on a budget.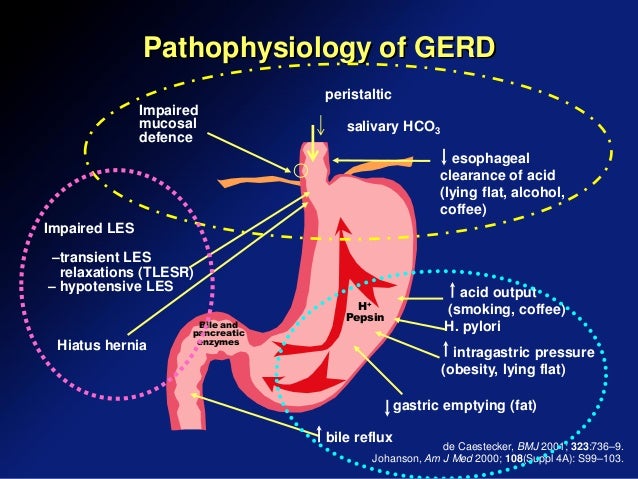
Media last reviewed: 13 January 2021
Media review due: 13 January 2024
Gastroesophageal Reflux Disease (GERD) and Heartburn During Pregnancy
Written by WebMD Editorial Contributors
Medically Reviewed by Nivin Todd, MD on August 26, 2022
In this Article
- Symptoms of Heartburn During Pregnancy
- Causes of Heartburn During Pregnancy
- Prevention of Heartburn During Pregnancy
- Treatment of Heartburn During Pregnancy
- Heartburn Medication to Avoid During Pregnancy
More than half of pregnant women get serious heartburn, particularly during their second and third trimesters. Heartburn, also called acid indigestion, is an irritation or burning sensation of the esophagus (the tube that carries food and liquid to your stomach when you swallow). It’s caused by stomach contents that reflux (come back up).
Symptoms of Heartburn During Pregnancy
If you have heartburn while you’re pregnant, you may:
- Feel burning or pain in your chest or throat, especially after you eat
- Have sensations of fullness, heaviness, or bloating
- Burp or belch
- Have a sour or bitter taste in your mouth
- Cough or have sore throat
Causes of Heartburn During Pregnancy
Heartburn in pregnancy may happen because of changing hormone levels, which can affect the muscles of the digestive tract.
Pregnancy hormones can cause your lower esophageal sphincter (the muscular valve between the stomach and esophagus) to relax, allowing stomach acids to flow back up into your esophagus. Also, as your baby grows, your enlarged uterus can crowd the abdomen, pushing stomach acids upward. Although it's rare, gallstones can also cause heartburn during pregnancy.
Prevention of Heartburn During Pregnancy
Some tips that may help you cut down on heartburn during your pregnancy include:
- Eat several small meals each day instead of three large ones.
- Eat slowly.
- Avoid fried, spicy, or rich (fatty) foods or any foods that seem to cause relaxation of the lower esophageal sphincter and increase the risk of heartburn.
- Don’t smoke tobacco or drink alcohol, which can make heartburn symptoms worse.
- Drink less while eating. Drinking large amounts while eating may increase the risk of acid reflux and heartburn.
- Don't lie down directly after eating.

- Keep the head of your bed higher than the foot of your bed. Or place pillows under your shoulders to help prevent stomach acids from rising into your esophagus.
- Wear loose-fitting clothing. Tight-fitting clothes can increase the pressure on your stomach and abdomen.
- Try to avoid constipation.
Treatment of Heartburn During Pregnancy
If your heartburn won’t go away, see your doctor. They may prescribe or recommend OTC medications that are safe to take during pregnancy. Heartburn usually disappears following childbirth.
Medications may include:
Over-the-counter antacids such as calcium carbonate or magnesium hydroxide. These are generally safe to use during pregnancy. You may find that liquid heartburn relievers are more effective in treating heartburn, because they coat the esophagus.
h3 blockers. These medications block chemical signals that produce stomach acid. They include cimetidine (Tagamet) and famotidine (Pepcid, Zantac 360), and they’re available in over the counter and prescription strengths.
Proton pump inhibitors (PPIs). Like h3 blockers, these drugs help cut down on stomach acid. PPIs, which include lansoprazole (Prevacid) and omeprazole (Prilosec), are available over the counter and by prescription.
If you take iron supplements, talk to your doctor before you take a PPI or h3 blocker. These medications can make the supplements less effective.
Heartburn Medication to Avoid During Pregnancy
Talk to your doctor before taking any antacids. Some contain ingredients that may harm you or your baby. Be sure to not to take these medications:
Ranitidine. In 2020, the FDA stopped sales of an h3 blocker called ranitidine (the ingredient in older Zantac products) because it was contaminated with a cancer-causing agent. If you take OTC ranitidine, stop your use. If you have a prescription for ranitidine, talk to your doctor about other options before you stop your medication.
Heartburn / GERD Guide
- Overview & Facts
- Symptoms & Complications
- Diagnosis & Tests
- Treatment & Care
- Living & Managing
 What is GERD during pregnancy?
What is GERD during pregnancy? IMPORTANT
The information in this section should not be used for self-diagnosis or self-treatment. In case of pain or other exacerbation of the disease, only the attending physician should prescribe diagnostic tests. For diagnosis and proper treatment, you should contact your doctor.
GERD during pregnancy is an acid-dependent disease of the esophagus caused by damage to the mucosa during the reflux of stomach contents, which has arisen or worsened under the influence of gestational factors. Manifested by heartburn, sour eructation, odynophagia, less often - nausea, vomiting, dysphagia, epigastric pain, cough, dysphonia, hypersalivation in sleep, taste perversions, depressed mood. It is diagnosed using alkaline and omeprazole tests, esophagoscopy, pH-metry, manometry. For treatment, alginates, antacids, selective histamine blockers, drugs that inhibit the proton pump, prokinetics are used.
ICD-10
K21 Gastroesophageal reflux
- Causes
- Pathogenesis
- Classification
- Symptoms of GERD during pregnancy
- Complications
- Diagnostics
- Treatment of GERD during pregnancy
- Prognosis and prevention
- Prices for treatment
General
GERD (gastroesophageal reflux disease, gastroesophageal reflux) is one of the most common diseases of the gastrointestinal tract, contributing to such a common symptom as pregnancy heartburn.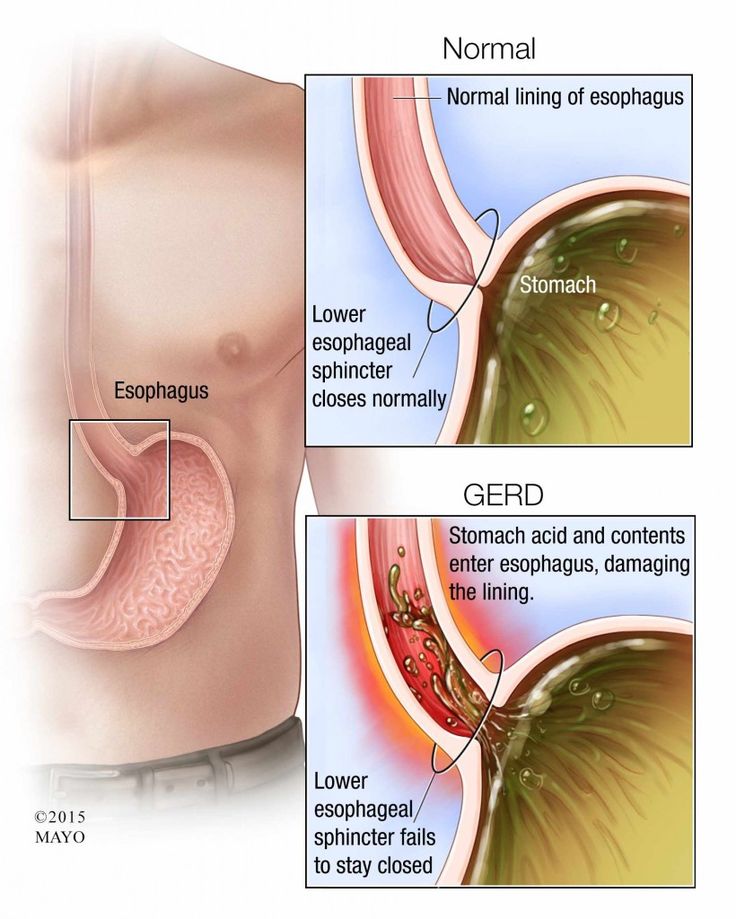 According to the observations of specialists in the field of obstetrics and gynecology, from 30 to 95% of patients during the period of bearing a child experience heartburn, which some experts even consider a natural manifestation of pregnancy. In 21-80% of patients suffering from GERD, the disease debuted precisely in connection with gestation.
According to the observations of specialists in the field of obstetrics and gynecology, from 30 to 95% of patients during the period of bearing a child experience heartburn, which some experts even consider a natural manifestation of pregnancy. In 21-80% of patients suffering from GERD, the disease debuted precisely in connection with gestation.
Women who have given birth multiple times are more susceptible to the disease. The relevance of timely detection of gastroesophageal reflux is due to a significant deterioration in the quality of life of a pregnant woman and the need to prescribe pharmacotherapy to almost half of the patients.
GERD during pregnancy
Causes
Gastroesophageal reflux of acidic gastric contents develops with a weakening of the cardiac sphincter, impaired motility of the esophagus and stomach, increased gastric secretion, and a decrease in the protective properties of the esophageal mucosa.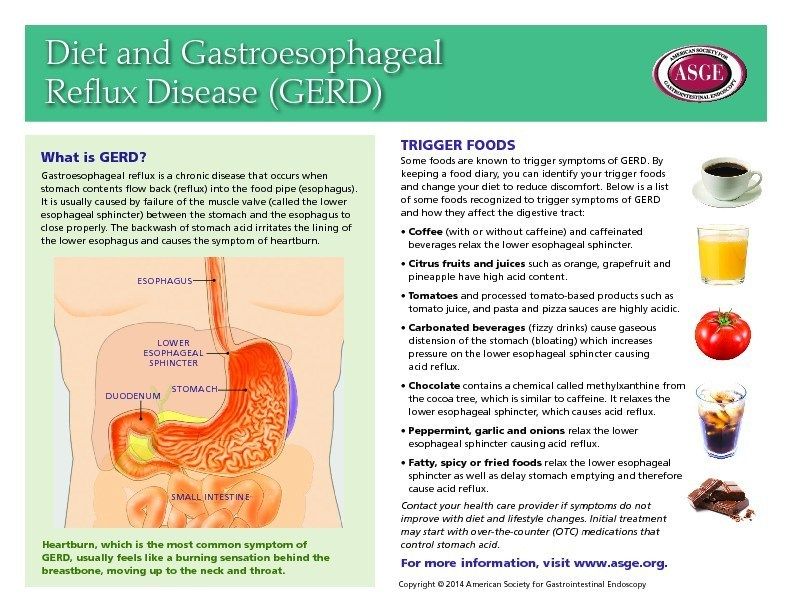 The occurrence of GERD is promoted by congenital and acquired hiatal hernia with displacement to the posterior mediastinum of the abdominal esophagus, part or all of the stomach, smoking, dietary errors, and obesity.
The occurrence of GERD is promoted by congenital and acquired hiatal hernia with displacement to the posterior mediastinum of the abdominal esophagus, part or all of the stomach, smoking, dietary errors, and obesity.
A certain role is played by the intake of nitrates, antidepressants, progestins, anticholinergics, calcium channel blockers and other drugs that cause transient relaxation of the esophageal sphincter. Specialists in the field of modern gastroenterology consider pregnancy as a separate prerequisite for the development of gastroesophageal reflux disease. The high incidence of GERD during gestation is associated with the action of factors such as:
- Increased progesterone levels. Under the action of progestins, the lower esophageal sphincter relaxes, the tone of which is restored only in the postpartum period. By reducing the tone of smooth muscle fibers and reducing the sensitivity of intestinal receptors to histamine and serotonin, physiological hyperprogesteronemia slows down gastrointestinal motility and impairs gastric emptying.
 As a result, reflux occurs more frequently.
As a result, reflux occurs more frequently. - Increased intra-abdominal pressure. During pregnancy, the relative position of the internal organs of the abdominal cavity is disturbed, which is associated with the development of the fetus and the growth of the uterus. When the stomach is displaced towards the diaphragm, evacuation stagnation of its contents is formed faster and the risk of diaphragmatic hernia formation increases. The factor of increasing intra-abdominal pressure is most significant in carrying multiple pregnancies and large fetuses.
Pathogenesis
The mechanism of development of GERD during pregnancy is based on the reflux of aggressive stomach contents into the lower esophagus. Gastroesophageal reflux usually occurs when the pressure of the cardiac sphincter is less than 2 mm Hg. Art. or an increase in intragastric pressure of more than 5 mm Hg. Art. Both of these factors are found in pregnant women. Refluxate containing hydrochloric acid, pepsin, and in some cases bile acids, has an irritating effect on the epithelium of the esophagus, causes a local inflammatory reaction, and in some patients provokes the onset of erosive processes.
Classification
When systematizing the forms of GERD in pregnant women, the same criteria are taken into account as outside the gestational period - the nature of the course of the disease and the condition of the esophageal mucosa. This approach makes it possible to develop optimal medical tactics aimed at eliminating clinical symptoms and the morphological basis of their occurrence without the risk of negative effects on the fetus. Depending on the time of existence of the disorder, acute gastroesophageal reflux disease is distinguished, lasting up to 3 months, and a chronic process that exists for 3 months or more. Taking into account the characteristics of damage to the esophageal mucosa, such forms of GERD are distinguished as:
- Gastroesophageal reflux without esophagitis. With a non-erosive variant of the disorder, detected in 55-70% of patients, there are no endoscopic signs of damage to the epithelium. Although the likelihood of complications in this case is lower, the patient's quality of life deteriorates in the same way as in the presence of erosions.
- Reflux esophagitis. In 30-45% of pregnant women with GERD during endoscopy, visible signs of esophagitis caused by the aggressive action of the contents of the stomach are determined. In the erosive form of gastroesophageal reflux, acute and long-term consequences of the disease are more often observed.
When predicting the outcome of GERD in a pregnant woman, the severity of the endoscopically positive variant of the disease according to the Los Angeles classification is also taken into account. The most favorable during pregnancy is reflux esophagitis A and B degrees, in which the defects extend to 1-2 folds of the mucosa, and their sizes, respectively, are up to or more than 5 mm. With C degree of GERD, less than 75% of the esophageal circumference is affected, and with D - 75% or more, which significantly increases the likelihood of a complicated course.
Symptoms of GERD during pregnancy
75% of patients with gastroesophageal reflux complain of heartburn, which gradually increases as labor approaches.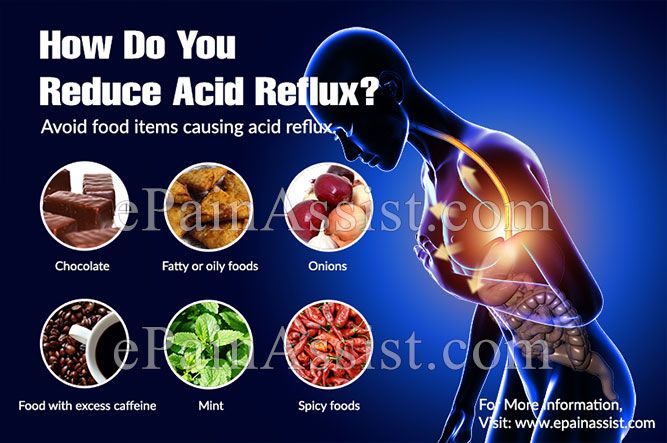 Discomfort and burning behind the sternum often occur after eating spicy, fatty, fried foods, overeating, exercise, lying down and bending over. Heartburn attacks can recur several times a day and last from minutes to several hours. Pregnant women suffering from GERD may experience sour or bitter belching, sensation of a lump in the throat, retrosternal pain when swallowing with irradiation to the precordial region, neck, lower jaw, interscapular space.
Discomfort and burning behind the sternum often occur after eating spicy, fatty, fried foods, overeating, exercise, lying down and bending over. Heartburn attacks can recur several times a day and last from minutes to several hours. Pregnant women suffering from GERD may experience sour or bitter belching, sensation of a lump in the throat, retrosternal pain when swallowing with irradiation to the precordial region, neck, lower jaw, interscapular space.
Sometimes in the II-III trimesters, nausea and vomiting are noted, it is extremely rare that swallowing solid and then liquid food is difficult. Extra-esophageal manifestations of reflux disease during pregnancy are a feeling of fullness in the epigastrium, rapid satiety, repeated attacks of coughing and suffocation, a hoarse voice, sore throat, increased salivation during sleep, burning cheeks and tongue, taste perversion, bad breath. Often, pregnant women experience a sad, depressed mood. Rarely, GERD is asymptomatic.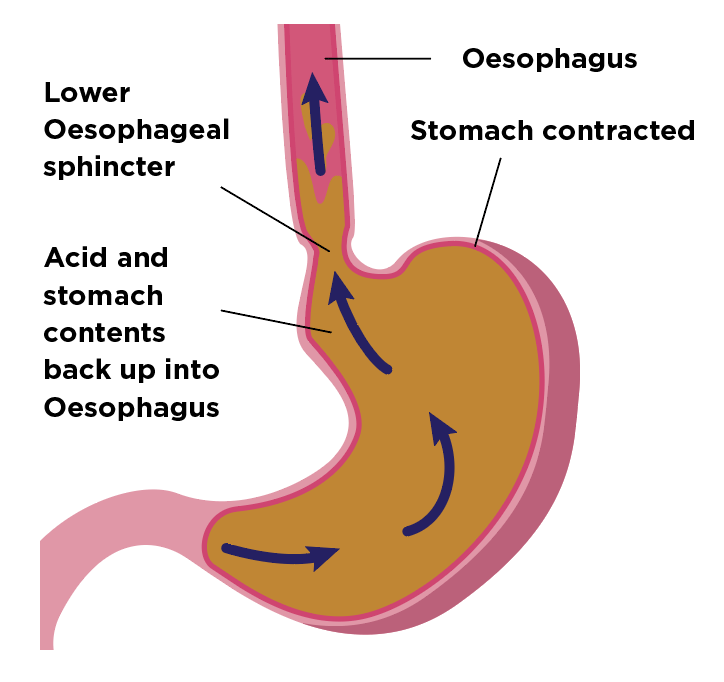
Complications
Usually, gastroesophageal reflux does not contribute to the occurrence of any obstetric complications, however, with extensive erosive damage to the esophagus, a more pronounced anemia of pregnant women may develop. In two thirds of patients, GERD worsens during pregnancy: in 10-11% of cases, a relapse occurs in the 1st trimester, aggravated by early toxicosis, in 33-34% - in the 2nd trimester, and in more than half of pregnant women - in the 3rd.
Rare specific complications that occur against the background of physiological immunodeficiency during pregnancy are acute esophagitis caused by candidal and herpes infections. There is a risk of ulceration of the mucosa with the development of esophageal bleeding. Long-term consequences of reflux disease are narrowing (strictures) of the esophagus, dysplasia and metaplasia of the epithelium (Barrett's esophagus) and esophageal adenocarcinoma.
Diagnostics
In pregnancy, the diagnosis of GERD is usually made on the basis of typical clinical symptoms with daily occurrence of heartburn. An obstetrician-gynecologist and a gastroenterologist are involved in the diagnosis. Instrumental methods traditionally used in the diagnosis of the disease are used to a limited extent in pregnant women due to the possible provocation of preterm labor and the aggravation of other complications (nephropathy, early toxicosis, preeclampsia, eclampsia). Recommended for diagnostic purposes:
An obstetrician-gynecologist and a gastroenterologist are involved in the diagnosis. Instrumental methods traditionally used in the diagnosis of the disease are used to a limited extent in pregnant women due to the possible provocation of preterm labor and the aggravation of other complications (nephropathy, early toxicosis, preeclampsia, eclampsia). Recommended for diagnostic purposes:
- Alkaline test. Reception of absorbable antacids quickly stops an attack of heartburn. The positive effect of alkaline preparations is associated with the neutralization of hydrochloric acid coming from the stomach into the esophagus. In the presence of extraesophageal manifestations, the study is supplemented with an omeprazole test aimed at eliminating symptoms by inhibiting gastric secretion.
- Endoscopy of the esophagus. Esophagoscopy is performed if extensive erosion, ulceration, esophageal bleeding, strictures are suspected, and neoplasia can be ruled out. In endoscopic examination, GERD is manifested by swelling and slight vulnerability of the esophageal mucosa, it is possible to identify areas of damaged epithelium.
 In some cases, it is possible to visualize the reflux of gastric juice.
In some cases, it is possible to visualize the reflux of gastric juice. - Intraesophageal pH-metry. The method is effective in non-erosive forms of gastroesophageal reflux. Electrometric determination of the acidity of the contents of the esophagus is carried out using a flexible intraesophageal probe attached to an acidogastrometer. pH-metry allows you to identify episodes of reflux of gastric juice and determine the conditions for their occurrence.
- Manometry. Registration of pressure in different parts of the gastrointestinal tract using special catheters with strain gauges verifies the weakening of the cardiac sphincter and dysmotility. A manometric study also provides an objective assessment of elasticity, tone, contractile activity of the esophageal wall, and pressure profiling in the esophagus.
If necessary, the examination is supplemented with gastrocardiomonitoring, gastrointestinal impedancemetry, bilemetry. X-ray studies of the esophagus during pregnancy are not performed.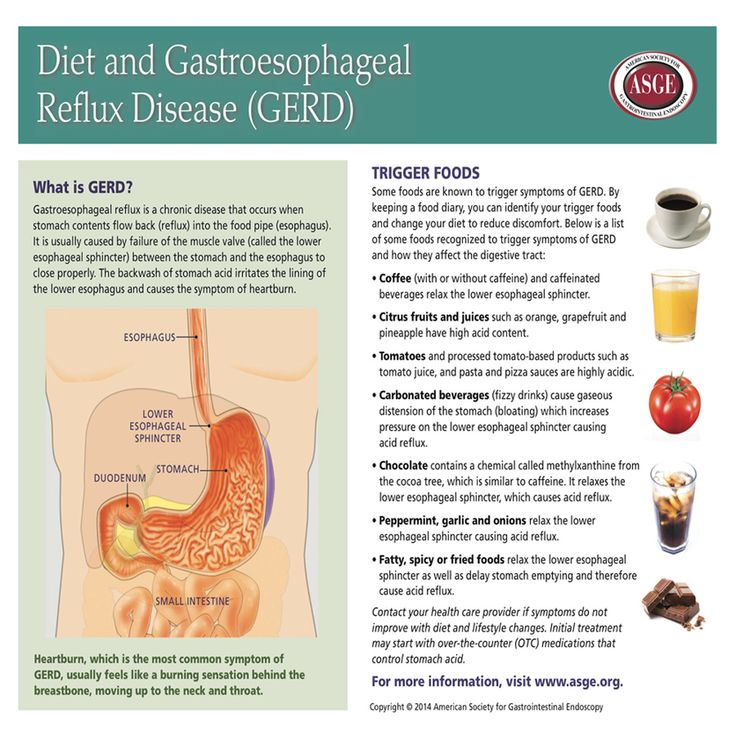 GERD is differentiated from functional dyspepsia, gastric and duodenal ulcers, acute infectious esophagitis, benign tumors and esophageal cancer. If extraesophageal symptoms are detected, differential diagnosis with angina pectoris, bronchial asthma may be required.
GERD is differentiated from functional dyspepsia, gastric and duodenal ulcers, acute infectious esophagitis, benign tumors and esophageal cancer. If extraesophageal symptoms are detected, differential diagnosis with angina pectoris, bronchial asthma may be required.
Treatment of GERD during pregnancy
Therapeutic tactics are aimed at the rapid elimination of clinical symptoms, restoration of the esophageal mucosa, prevention of complications and relapses. In 25% of cases, the condition can be improved by non-drug methods. Pregnant women with mild GERD are recommended to stop smoking, correct diet and diet with frequent small meals, reduce the amount of high-protein and low-lipid foods, and exclude citrus juices, chocolate, caffeine-containing drinks, spices, mint, and alcohol.
Care must be taken when using drugs that transiently reduce the tone of the cardia. Efficient sleep with a raised headboard, chewing chewing gum with calcium carbonate. Identification of severe clinical symptoms requires the appointment of special drug therapy. During pregnancy, some of the drugs used in standard treatment regimens for gastroesophageal reflux are used with caution due to possible effects on the fetus or the occurrence of obstetric complications. Patients with severe GERD are shown:
Identification of severe clinical symptoms requires the appointment of special drug therapy. During pregnancy, some of the drugs used in standard treatment regimens for gastroesophageal reflux are used with caution due to possible effects on the fetus or the occurrence of obstetric complications. Patients with severe GERD are shown:
- Nonabsorbable antacids and alginates. Considered 1st line drugs for the treatment of gastroesophageal reflux disease in pregnant women. By neutralizing hydrochloric acid, reducing the digestive capacity of pepsin, adsorbing lysolecithin, bile acids, improving the evacuation of stomach contents, stimulating the secretion of prostaglandins, antacids reduce the damaging effect of refluxate. Alginates have a protective effect on the esophageal mucosa.
- Histamine h3 receptor blockers. They are used when antacid therapy for GERD is ineffective. The antisecretory activity of selective histamine blockers is due to the action on the receptors of the parietal cells of the stomach.
 Due to inhibition of secretion, the acidity and volume of gastric contents decrease, which helps to reduce its aggressiveness and pressure on the cardiac sphincter. The effect of h3-histamine blockers on the fetus is not well understood, which limits their use.
Due to inhibition of secretion, the acidity and volume of gastric contents decrease, which helps to reduce its aggressiveness and pressure on the cardiac sphincter. The effect of h3-histamine blockers on the fetus is not well understood, which limits their use. - Proton pump inhibitors. High efficiency and rapid achievement of therapeutic results in the appointment of PPIs are based on blocking the secretion of hydrochloric acid at the level of the secretory tubules of parietal cells. The limited use of pump inhibitors is due to a decrease in the bactericidal properties of gastric juice, which, against the background of natural suppression of immunity, contributes to the development of food infections and impaired calcium absorption, which is necessary for the normal course of gestation.
As additional means, prokinetics that improve gastrointestinal motility and herbal enveloping preparations can be used. During gestation, surgical treatment of severe and complicated forms of GERD is not performed. Pregnancy is recommended to be completed by natural childbirth at a physiological time. Caesarean section is performed when obstetric indications are identified.
Pregnancy is recommended to be completed by natural childbirth at a physiological time. Caesarean section is performed when obstetric indications are identified.
Prognosis and prevention
With the appointment of adequate treatment, the damaged mucosa of the esophagus usually fully recovers after 4-12 weeks, with non-erosive variants of the disease, improvement occurs within 4-10 days. Prevention of gastroesophageal reflux involves the normalization of diet and lifestyle: giving up bad habits, adequate rest and sleep, controlling weight gain with a tendency to obesity, eliminating foods that irritate the esophageal mucosa or stimulate gastric hypersecretion, taking drugs that can disrupt gastrointestinal motility, only as directed and under medical supervision. To prevent recurrence of GERD in a pregnant woman, a 1-3-day intake of alginates and antacids "on demand" is recommended when symptoms appear.
You can share your medical history, what helped you in the treatment of GERD in pregnancy.
Sources
- Gastroesophageal reflux disease during pregnancy/ Elohina TB, Tyutyunnik VL// Experimental and clinical gastroenterology. - 2009 - No. 3.
- Pregnancy heartburn: an everyday trifle that must be endured, or gastroesophageal reflux disease that should be stopped? / Argunova IA// Gastroenterology. - 2015 - No. 3.
- Features of the course of gastroesophageal reflux disease in pregnant women/ Grishechkina IA, Kusakina AA, Miermanova MK// Young scientist. - 2015. - No. 13.
- Gastroesophageal reflux disease / Babak O.Ya., Fadeenko G.D. – 2000.
- This article was prepared based on the materials of the site: https://www.krasotaimedicina.ru/
IMPORTANT
Information from this section cannot be used for self-diagnosis and self-treatment. In case of pain or other exacerbation of the disease, only the attending physician should prescribe diagnostic tests. For diagnosis and proper treatment, you should contact your doctor.
Issues of treatment of gastroesophageal reflux disease in pregnant women
The duty of every doctor is to take care of the health of patients who turn to him for help. Responsibility becomes greater if you have to think about the health of both the mother and her unborn child at once. If in general therapeutic practice the decision on further tactics of treating a disease can be made relatively easily, then the obstetrician has to weigh all the pros and cons before choosing one or another treatment strategy. One of the diseases that often occurs in pregnant women and requires just such close attention is gastroesophageal reflux disease (GERD). Numerous studies suggest that mild forms of GERD during pregnancy can be treated with lifestyle changes, while more severe forms require medical intervention. This review reflects aspects of the use of the alginate antireflux drug Gaviscon forte® in the treatment of GERD during pregnancy.
Features of the course of GERD in pregnant women and / or the appearance of characteristic symptoms (heartburn, retrosternal pain, etc.
 ) [1]. Among pregnant women, heartburn is experienced daily by 48–79% of women [2], and the incidence of GERD in different trimesters is not the same and progressively increases with increasing gestational age. So, in a study of 607 pregnant women, it was found that in the first trimester heartburn was observed in 22%, in the second trimester - in 39% and in the third trimester - in 72% of patients. However, only 14% of women experienced heartburn before pregnancy [3].
) [1]. Among pregnant women, heartburn is experienced daily by 48–79% of women [2], and the incidence of GERD in different trimesters is not the same and progressively increases with increasing gestational age. So, in a study of 607 pregnant women, it was found that in the first trimester heartburn was observed in 22%, in the second trimester - in 39% and in the third trimester - in 72% of patients. However, only 14% of women experienced heartburn before pregnancy [3]. Diagnosis of GERD in pregnant women can be made with high accuracy in the presence of two main symptoms (heartburn and / or belching) and the absence of "alarming" symptoms, such as dysphagia, weight loss, hematemesis, etc. Complications in the form of esophagitis, esophageal stricture are extremely rare. Instrumental methods are usually not used: they are appropriate only if the disease is difficult to treat and / or there is a suspicion that some of the complications have nevertheless developed [4].
Of particular interest are studies of the causes of GERD in pregnant women. One of the first hypotheses was formulated, according to which an increase in the size of the uterus causes an increase in intra-abdominal pressure, which ultimately leads to the development of gastroesophageal reflux. However, a number of data do not confirm the key role of this mechanism in the formation of GERD. For example, it is not clear why GERD in pregnant women develops in the first trimester, when intra-abdominal pressure is not yet elevated? Moreover, D.H. van Thiel and A. Wald [5] studied the effect of pseudopregnancy on the formation of gastroesophageal reflux. The study included 10 men with tense ascites due to cirrhosis of the liver. Prior to the formation of diuresis in patients, when abdominal pressure was increased due to ascites, the pressure of the lower esophageal sphincter was also compensatory increased. After the induction of diuresis, ascites decreased, intra-abdominal pressure decreased, and the pressure of the lower esophageal sphincter returned to normal. None of the men had heartburn or proven acid reflux either before or after diuresis.
One of the first hypotheses was formulated, according to which an increase in the size of the uterus causes an increase in intra-abdominal pressure, which ultimately leads to the development of gastroesophageal reflux. However, a number of data do not confirm the key role of this mechanism in the formation of GERD. For example, it is not clear why GERD in pregnant women develops in the first trimester, when intra-abdominal pressure is not yet elevated? Moreover, D.H. van Thiel and A. Wald [5] studied the effect of pseudopregnancy on the formation of gastroesophageal reflux. The study included 10 men with tense ascites due to cirrhosis of the liver. Prior to the formation of diuresis in patients, when abdominal pressure was increased due to ascites, the pressure of the lower esophageal sphincter was also compensatory increased. After the induction of diuresis, ascites decreased, intra-abdominal pressure decreased, and the pressure of the lower esophageal sphincter returned to normal. None of the men had heartburn or proven acid reflux either before or after diuresis.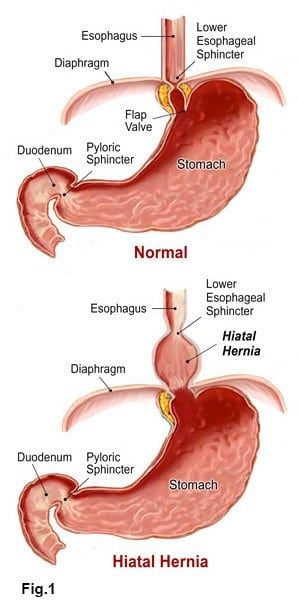 The authors concluded that increased intra-abdominal pressure during pregnancy cannot be the main causal factor in the development of GERD [5].
The authors concluded that increased intra-abdominal pressure during pregnancy cannot be the main causal factor in the development of GERD [5].
Today, the hormonal theory of the formation of GERD in pregnant women is generally accepted [4, 6]. The fact is that during gestation in the blood plasma in women, the content of progesterone and estrogen increases. Both hormones in the first trimester of pregnancy do not affect the basal tone of the lower esophageal sphincter, however, they reduce the pressure increase of this sphincter in response to a variety of physiological stimuli, including food intake [7]. In the second and third trimesters of pregnancy, progesterone and estrogen also reduce the basal tone of the lower esophageal sphincter. The magnitude of the decrease can be 50% of the initial level, the maximum decrease occurs at the 36th week of gestation [8]. Thus, at all stages of pregnancy, the hormonal background "weakens" the work of the lower esophageal sphincter, creating the preconditions for the formation of gastroesophageal reflux. After childbirth, the basal tone of the lower esophageal sphincter returns to normal [8].
After childbirth, the basal tone of the lower esophageal sphincter returns to normal [8].
The hormonal theory of the formation of GERD in pregnant women is also supported by the fact that women taking oral contraceptives (containing progesterone or a combination of progesterone and estrogen) also experience a decrease in the basal tone of the lower esophageal sphincter [9].
Numerous studies [4, 6] suggest that mild forms of GERD during pregnancy can be treated with lifestyle changes. Need to quit smoking; make adjustments to the diet: you should eat foods low in lipids and high in protein, avoid eating foods (citrus juices, tomato products, coffee, chocolate, alcohol) and medications (anticholinergics, sedatives, tranquilizers, theophylline, prostaglandins, blockers calcium channels) that provoke heartburn, it is recommended to chew chewing gums containing calcium carbonate, eat often (5-7 times), but in small portions during the day, the last meal should be taken 2-3 hours before bedtime; sleep with the head of the bed raised by 15 cm.
It is believed that if pregnant women with GERD follow the above rules, then in 25% of cases the symptoms of the disease will be leveled [10].
More severe forms of GERD in pregnant women require medical intervention (Fig. 1). First choice drugs include antacids, alginates, and metoclopramide and sucralfate (not all investigators agree on the inclusion of the latter two drugs in first choice therapy). If these drugs are ineffective, pregnant women can be prescribed histamine (h3) receptor blockers and proton pump inhibitors PPIs [6].
Antacids and alginates are considered the safest drugs used to treat GERD in pregnancy (although they have not yet been given a safety class by the US Food and Drug Administration). However, it must be remembered that antacids containing aluminum have the potential to cause neurotoxic effects on the fetus. Antacids containing magnesium should not be taken during the last weeks of pregnancy due to the tocolytic properties of magnesium. Antacids containing sodium bicarbonate are generally not used during pregnancy due to the risk of maternal and/or fetal metabolic alkalosis and fluid overload. Only antacids containing calcium did not show significant side effects [4].
Antacids containing sodium bicarbonate are generally not used during pregnancy due to the risk of maternal and/or fetal metabolic alkalosis and fluid overload. Only antacids containing calcium did not show significant side effects [4].
Most of the antacids listed are a much better alternative to alginates (see below).
H2 receptor blockers and the vast majority of proton pump inhibitors have been classified as safety class B by the US Food and Drug Administration (no adverse effects on the fetus have been identified in animal studies, but there are not enough well-designed and well-controlled studies in pregnant women , or side effects have been found in animal studies, but no risks to the fetus have been identified in well-designed and well-controlled studies in pregnant women). Therefore, these drugs should only be used when first-line drugs have failed [4].
Gaviscon forte® has established itself as an effective alginate antireflux drug
Gaviscon forte® is an alginate antireflux drug that was relatively recently introduced to the Ukrainian pharmaceutical market by the British company Reckitt Benckiser Healthcare. In our country, this is, in fact, the first and only drug of this class. However, alginate antireflux drugs have been used abroad for decades: during this time they have proven their clinical effectiveness and a high level of safety. The data accumulated to date allow us to treat Gaviscon forte with confidence and more actively introduce this drug into daily clinical practice.
In our country, this is, in fact, the first and only drug of this class. However, alginate antireflux drugs have been used abroad for decades: during this time they have proven their clinical effectiveness and a high level of safety. The data accumulated to date allow us to treat Gaviscon forte with confidence and more actively introduce this drug into daily clinical practice.
The main active ingredient of Gaviscon forte is sodium alginate, a natural product obtained from certain types of seaweed (in particular, kelp). In addition, the composition of the drug includes potassium bicarbonate and calcium carbonate.
When Gaviscon forte® is taken orally (1-2 teaspoons after meals and at bedtime), the drug passes unchanged into the stomach. Here, a chemical reaction takes place between sodium alginate and hydrochloric acid, resulting in the formation of alginic acid. The calcium ions released from the carbonate bind the alginic acid molecules into a high-strength polymer gel. And the carbon dioxide bubbles released from potassium bicarbonate are inside the gel and help to ensure that it is located on the surface of the gastric contents and does not mix with food until the stomach is empty [11].
And the carbon dioxide bubbles released from potassium bicarbonate are inside the gel and help to ensure that it is located on the surface of the gastric contents and does not mix with food until the stomach is empty [11].
Thus, Gaviscon forte® gel, "hovering" above the gastric contents (Fig. 2), creates a physical barrier that prevents the gastric and duodenal contents from being thrown into the esophagus or higher located departments. Accordingly, clinically this will be manifested by the elimination of symptoms of GERD.
In a comparative study of Gaviscon forte® and antacids, neither drug was found to interfere with the passage of food particles from the stomach to the intestines. However, Gaviscon forte remained in the stomach much longer than the antacid. Moreover, the antacid formed a homogeneous mixture with the contents of the stomach, while Gaviscon forte® formed a separate layer on the surface of the gastric contents, remaining here for at least 3 hours (according to some authors, at least 4 hours) [13].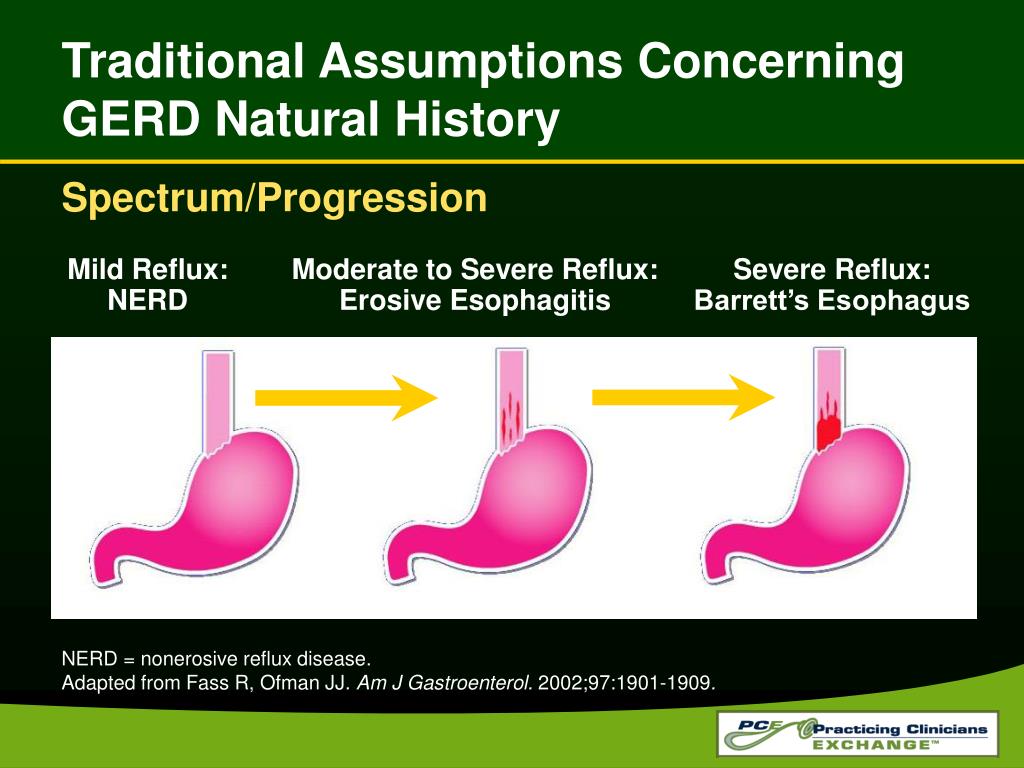
The use of Gaviscon forte® for the treatment of GERD in pregnant women
It is known that the ability of drugs to have a toxic effect on the body or cause side effects is closely related to their ability to penetrate into the systemic circulation. In order to gain a more complete picture of the safety profile of sodium alginate (the main active ingredient in Gaviscon forte®), it was decided to evaluate its ability to be absorbed into the blood and distributed to various organs and tissues. For this purpose, rats at the age of 10 weeks were used, which were given with food sodium alginate labeled with radioactive carbon 14C. The ratio of food and sodium alginate was 9: 1. As a result, it was found that from 85 to 91% of radioactivity was found in feces, 0.11–0.16% in urine, 0.21–0.42% in exhaled air and 0.002–0.007% in blood plasma. The authors concluded that the absorption of sodium alginate into the systemic circulation and subsequent entry into various organs is negligible [14].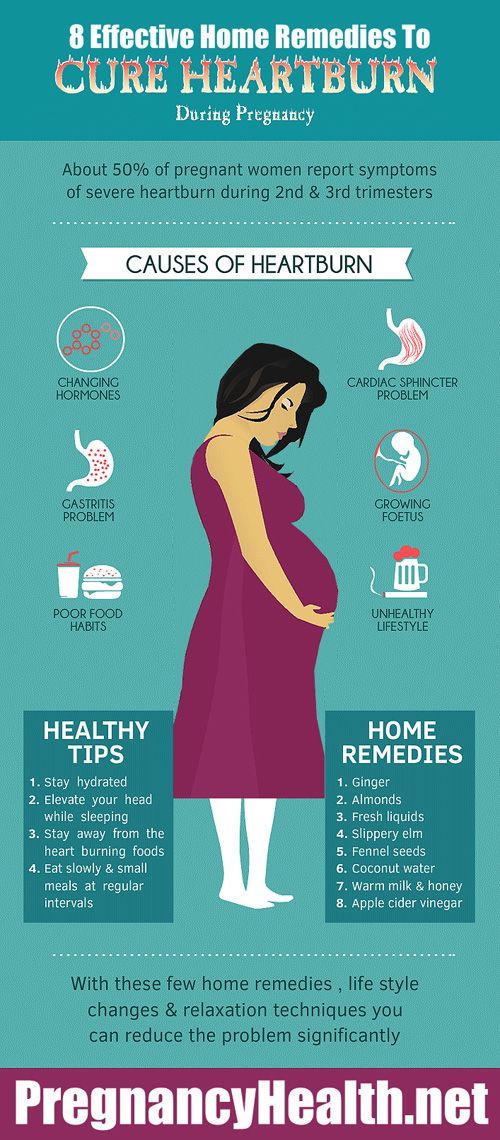 This may explain the low incidence of side effects when using Gaviscon forte®.
This may explain the low incidence of side effects when using Gaviscon forte®.
The effectiveness of Gaviscon® in the treatment of GERD in pregnant women was already found in the earliest clinical trials. Thus, one of the open studies [15] included 50 pregnant women in the second and third trimesters of gestation. Each of them had typical symptoms of GERD - heartburn, belching, etc. All women were treated with Gaviscon® for 1 month, the dose was 2 tablespoons of the drug 4 times a day after meals and at bedtime. When evaluating the results of the study after 1 month, a significant decrease in the frequency, intensity and duration of all symptoms was found. Doctors rated the treatment as effective in 98% of patients, while the pregnant women themselves considered the treatment effective in 70% of cases. The authors of the study additionally emphasize the excellent tolerability of the drug.
Similar data are obtained in the most recent studies. In 2003, the results of an open multicenter study were published, which took place in the UK and South Africa with the participation of general practitioners and antenatal clinics. All pregnant women (n = 150) were aged 18–40 years, gestational age ≤ 38 weeks, and suffered from heartburn. All women were prescribed Gaviscon forte® 5–10 ml to be taken as symptoms developed.
All pregnant women (n = 150) were aged 18–40 years, gestational age ≤ 38 weeks, and suffered from heartburn. All women were prescribed Gaviscon forte® 5–10 ml to be taken as symptoms developed.
The results of the study were quite impressive. After 4 weeks of therapy, doctors rated the effectiveness of treatment as "good" and "very good" in 88% of pregnant women, while the women themselves gave a similar assessment in 90% of cases (Fig. 3). The frequency and severity of both daytime and nighttime symptoms were reduced.
After taking Gaviscon forte®, a rapid decrease in the severity of symptoms was observed. Within 10 minutes after taking the drug, 57% of pregnant women reported relief of symptoms, while by the 20th minute symptoms were already reduced in 93% of women (Fig. 4).
The authors of the study concluded that Gaviscon forte® quickly and effectively relieves heartburn in pregnant women with GERD. Moreover, Gaviscon forte® does not pose any significant threat to the health of the mother and child.
Conclusions
1. The clinical picture of GERD in pregnant women is in many respects similar to the manifestations of GERD in the general population, with the exception that serious complications (esophagitis, esophageal stricture) develop rarely. The cause of the disease lies in the increase in plasma levels of progesterone and estrogen during pregnancy. The selection of therapy for GERD in pregnant women requires special care because of the threat to the health of the fetus.
2. Gaviscon forte® is the first alginate antireflux drug in Ukraine. Once in the stomach, Gaviscon forte® forms a gel that is located on the surface of the gastric contents and prevents the development of gastroesophageal reflux.
3. Gaviscon forte® is practically not absorbed into the systemic circulation, and therefore rarely leads to the development of side and toxic effects. The conducted studies indicate the high efficiency and rapid onset of action of Gaviscon forte® in the treatment of GERD in pregnant women.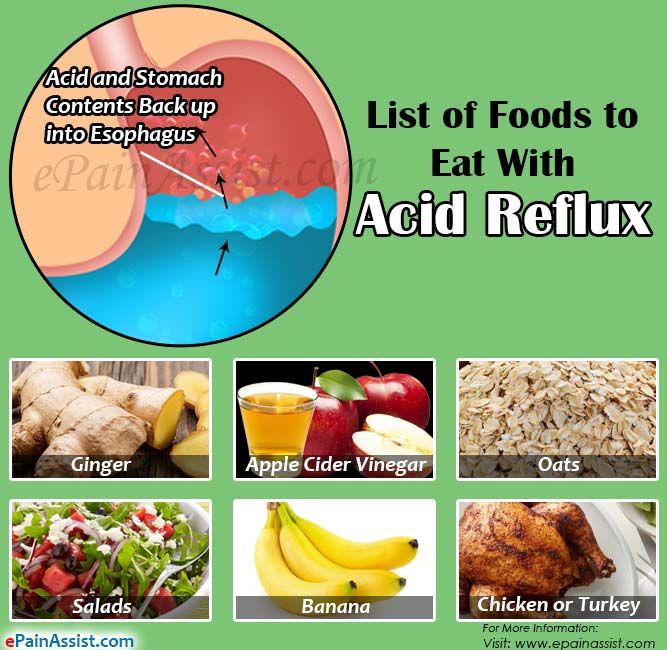
Bibliography
1. Elohina T.B., Tyutyunnik V.L. Gastroesophageal reflux disease during pregnancy // Russian Medical Journal. - 2008. - T. 16, No. 19. - S. 1243-1247.
2. Mandel K.G., Daggy B.P., Brodie D.A., Jacoby H.I. Review article: alginate-raft formulations in the treatment of heartburn and acid reflux // Aliment. Pharmacol. Ther. - 2000. - V. 14. - P. 669-690.
3. Marrero J.M., Goggin P.M., de Caestecker J.S. et al. Determinants of pregnancy heartburn // Brit. J. Obstetr. Gynaecol. - 1992. - V. 99. - P. 731-734.
4. Madanick R.D., Katz P.O. GERD and Pregnancy // Practical gastroenterology. - 2006. - V. 29, No. 6. - P. 30-39.
5. Van Thiel D.H., Wald A. Evidence refuting a role for increased abdominal pressure in the pathogenesis of the heartburn associated with pregnancy // Am. J. Obstet. Gynecol. - 1981. - V. 140, No. 4. - P. 420-422.
6. Richter J.E. Review article: the management of heartburn in pregnancy // Aliment. Pharmacol. Ther. - 2005. - V. 22. - P. 749-757.
Pharmacol. Ther. - 2005. - V. 22. - P. 749-757.
7. Fisher R.S., Roberts G.S., Grabowski C.J., Cohen S. Altered lower esophageal sphincter function during early pregnancy // Gastroenterology. - 1978. - V. 74, No. 6. - P. 1233-1237.
8. Van Thiel D.H., Gavaler J.S., Joshi S.N. et al. Heartburn of pregnancy // Gastroenterology. - 1977. - V. 72, No. 4 (Pt. 1). - P. 666-668.
9. Van Thiel D.H., Gavaler J.S., Stremple J. Lower esophageal sphincter pressure in women using sequential oral contraceptives // Gastroenterology. - 1976. - V. 71, No. 2. - P. 232-234.
10. Katz P.O., Castell D.O. Gastroesophageal reflux disease during pregnancy // Gastr. Clin. N.Amer. - 1998. - V. 27. - P. 153-167.
11. Gaviscon Advance: Product monograph. www.totalgordmanagement.co.uk
12. Marciani L., Young P., Tyler D.J. et al. Echo-Planar Imaging of Gaviscon Alginate Rafts in Vivo // Proc. Intl. soc. Mag. Reson. Med. - 2001. - V. 9. - P. 2047.
13. Wilson C.