Second pregnancy after c section symptoms
Pregnancy and giving birth after a caesarean section
Getting pregnant after a c-section
It usually takes longer to recover from a c-section than a vaginal birth, even if the birth was straightforward. It’s important to give your body time to recover before you start trying to get pregnant again. You will need to wait at least 6 months but your doctor or midwife may advise you to wait for 12–18 months. The longer you leave your scar to heal, the stronger it will be.
It’s particularly important to make sure your scar has completely healed if you want to try for a vaginal birth next time. This is because it is possible that the scar may open slightly. This is known as uterine dehiscence. It may not cause any serious issues, but it may increase the chance of a uterine rupture (a tear in the wall of the uterus), which can cause serious problems for both the mum and baby. The chances of a uterine rupture is higher if you have a vaginal birth next time, but it is still rare.
It may help to think about how long it took you to recover after your last c-section, your current physical health now and if you’re feeling emotionally ready. There are lots of positive things you can do to prepare for a healthy pregnancy and baby. Find out more about planning a pregnancy.
Of course, pregnancy isn’t always planned. Or you may want to get pregnant sooner for your own reasons. If you have become pregnant within a year of having a c-section, you may still be able to give birth vaginally if you want to. Your doctor or midwife will explain your best options for giving birth.
Birth options after a c-section
If you’ve had a c-section before, you can have a vaginal birth after a c-section (VBAC) or an elective repeat c-section (ERCS). If you are fit and healthy, both are safe choices with very small risks.
Your midwife or obstetrician will talk to you about your birth options soon after your fetal anomaly scan at 18–21 weeks. An obstetrician is a doctor who specialises in care during pregnancy, labour and after birth.
They can help you decide how to give birth by talking to you about:
- why you had a c-section last time
- whether you have had a vaginal birth
- any complications during your last c-section or during your recovery
- the type of cut that was made in your womb – horizontal or vertical
- how you feel about your most recent birth experience
- how your current pregnancy is progressing and if there have been any issues or complications
- how many more babies you are hoping to have in the future – the risks increase with each c-section, so you may want to avoid another c-section if possible.
If possible, you will need to decide what type of birth you would like before 36 weeks of pregnancy.
“I would say listen to your medical professionals and keep an open mind. I wanted a VBAC after a traumatic emergency c-section, several miscarriages and a difficult pregnancy. Unfortunately, this didn’t happen but my elective c-section was wonderfully civilised and a complete contrast to the first birth!”
Amanda
Vaginal birth after a c-section (VBAC)
If you have only had one c-section before, you should be able to give birth vaginally if you’re carrying one baby and you go into labour after 37 weeks.
You’re more likely to have a successful vaginal birth if:
- you’ve had a vaginal birth before, especially if it was after a previous c-section
- labour starts naturally
- you were at a healthy weight when you got pregnant.
VBAC may not be suitable for you, for example, if you’re at risk of uterine rupture or there are problems with your baby’s health. Your doctor may advise you to have an elective repeat c-section (ERCS) instead.
“I had an emergency c-section with my first rainbow baby. When I fell pregnant with my second, I knew I wanted to try for a VBAC, but I had much more realistic expectations this time as it was a high-risk pregnancy. There was a moment during labour that I thought I would have another c-section, but thankfully I managed a vaginal birth. I did the same with my third and am hoping I can do it again with my fourth. I think every mum who has had a c-section should feel hopeful they can have a VBAC if that’s what they want, but be proud of themselves regardless.
”
Cara
What are the advantages of a VBAC?
- If vaginal birth is successful, you’re less likely to have complications than if you have an elective repeat c-section (ERCS).
- Your recovery is likely to be quicker.
- Your stay in hospital may be shorter.
- You will avoid the risks of an operation.
- You’re more likely to have a successful vaginal birth in future pregnancies.
- Your baby will have less chance of breathing problems in the days after birth.
What are the disadvantages of a VBAC?
- On average, about 1 in 4 women will need an emergency c-section during labour. This carries a higher risk of complications than an elective repeat c-section (ERCS). For women who have had a vaginal birth before, about 1 in 10 will need an emergency c-section.
- There’s a higher chance of the scar in your womb tearing (uterine rupture). This happens in about 1 in 200 women. The chance of this happening is lower if you have had a vaginal birth before but it is more likely if your labour is induced (started artificially).
 If it looks like that may happen, you’ll be offered an emergency c-section.
If it looks like that may happen, you’ll be offered an emergency c-section. - You have a slightly higher chance of needing a blood transfusion compared with women who choose a planned caesarean section.
- The risk to your baby of brain injury or stillbirth is higher than for a planned c-section, but is the same as if you were in labour for the first time.
"I had an emergency c-section with my first and desperately wanted a VBAC for my second. I went into labour naturally but did end up having a second emergency c-section. If we are lucky enough to have a third, it’s likely to be a planned c section and so I’m unlikely to ever experience vaginal birth. In the end, all that matters is that me and my baby are ok. Nothing about giving birth is easy so however I end up getting through it, I’ll be happy!"
Stacey
Where can I give birth?
You may need to give birth in hospital, where you have quick access to more facilities if you need them. For example, in case you need an emergency c-section or a blood transfusion, or if your baby needs help to breathe.
For example, in case you need an emergency c-section or a blood transfusion, or if your baby needs help to breathe.
This is especially important if you’re more likely to have complications, such as uterine rupture. This may be the case if your labour is induced or you have had more than one c-section before. Your doctor or midwife can help you decide what is best for you.
Can I have a vaginal birth if I have had more than one c-section?
If you have had more than one c-section, you should have the chance to talk to a senior obstetrician about the risks and benefits of a vaginal birth. Speak to your midwife as soon as possible to arrange a consultation with an obstetrician.
Going into labour before a VBAC
During your pregnancy, your doctor will explain what to do if you do or don’t go into labour before your VBAC. If you go into labour or your waters break, contact the hospital straight away. Once you start having regular contractions, the midwife will track your baby’s heartbeat.
You can choose your preferred type of pain relief during labour, including an epidural if you would like one.
If you don’t go into labour naturally by 41 weeks, your options may include:
- waiting for labour to start naturally
- inducing labour.
Inducing labour increases the chance of your previous c-section scar tearing, which could lead to you needing a c-section. The doctor and midwife will monitor you and your baby closely during labour. You can choose whether to have an induction or a c-section. Your doctor or midwife can explain the benefits and risks of both options to help you decide.
Elective repeat c-section (ERCS)
If you choose to have another c-section, you will usually have it after 39 weeks of pregnancy. Your obstetrician may suggest you have another c-section if you have:
- a vertical scar in your womb
- placenta praevia
- had a uterine rupture
- had uterine surgery.
What are the advantages and disadvantages of an ERCS?
Advantages of another c-section include:
- There’s a smaller risk of the c-section scar separating or tearing (1 in 1000).
- You will know the date of planned birth. But you may go into labour before this date or your healthcare team may need to change the date.
- The risk to your baby of brain injury or stillbirth is lower than for VBAC.
Disadvantages of an ERCS include:
- A repeat c-section usually takes longer than the first operation. This is because you will have scar tissue, which can make the operation more difficult. Scar tissue might also damage your bowel or bladder.
- You have a slightly higher risk of placenta praevia and/or placenta accreta in future pregnancies.
- You’re more likely to need a c-section in future pregnancies.
- Your baby has a slightly higher risk of breathing problems after birth if you have an ERCS before 39 weeks – you may have steroid injections before the birth to reduce this risk.
Read more about the benefits and risks of having a c-section.
What happens if I have an elective c-section planned but I go into labour?
Your doctor or midwife will help you plan what will happen if you go into labour before your elective c-section.
Tell your maternity team straight away if you start going into labour. They will help you decide on the safest option for you and your baby. This may be an emergency c-section, or if labour is very advanced it may be safer for you to have a vaginal birth.
Ask lots of questions so you have the information you need to make the right choice for you and your baby.
pregnancies after c-section — Blog — The Motherhood Collective
Allow me to start by saying if you have the option of a scheduled C-section, be sure you research the risk factors, procedure, recovery, and subsequent pregnancies. If you have a "normal" pregnancy with zero to minimal complications, you will likely not need a C-section. We were presented the option based on my family medical history, current condition of my health and the size of my baby so we decided to have a scheduled C-section in October of 2011. We made the best decision for the health of my baby and for myself and we have no regrets. It isn't the right choice for everyone but it was the right choice for us. ----
It isn't the right choice for everyone but it was the right choice for us. ----
Well, I'm knocked up again! This is my second pregnancy after my C-section 20 months ago (You can read my birth story here and here). Last summer, my pregnancy sadly ended in a miscarriage. (You can read my story here.)
I am now 19 weeks along and it's going very well - except for the extreme nausea, cramping and pain. In the world of pregnancy, these are usually good signs of a healthy pregnancy. In the world of pregnancy after a C-section, these are all totally normal. Yaaaay?! When I chose to deliver my giant baby via Caesarian, I did hours of research. I neglected to research what would happen during subsequent pregnancies - I only looked at subsequent births.
Nausea is not new for me and I've been able to take prescription meds to keep it as controlled as possible. When it comes to the cramping and pain, I was surprised that it felt very similar to the recovery of my C-section. It feels like my incision is being stretched with my uterus - and that's exactly what is happening according to my doctor and the inter webs. Engaging my core and lifting 20+ pounds proves to be more difficult with each day. Standing or sitting for long periods of time makes me want to lay down on my back - but then laying down on my back makes me cramp like a severe menstrual cycle. The most comfortable thing to do is lay elevated on the couch and watch The West Wing on Netflix. Oh yeah, and I have a toddler.
It feels like my incision is being stretched with my uterus - and that's exactly what is happening according to my doctor and the inter webs. Engaging my core and lifting 20+ pounds proves to be more difficult with each day. Standing or sitting for long periods of time makes me want to lay down on my back - but then laying down on my back makes me cramp like a severe menstrual cycle. The most comfortable thing to do is lay elevated on the couch and watch The West Wing on Netflix. Oh yeah, and I have a toddler.
Because my surgery was scheduled (at 40 weeks and 5 days), the doctors were able to take their time cutting horizontally along the "bikini line" and take their time stitching me back together. Some women with emergency C-sections or a vertical incision may not experience the same kind of discomfort because the weight isn't pulling down in one directional area. However, women with vertical incisions can sometimes acquire a "butt belly". Both incisions have their ups and downs (budum ching). Regardless of the incision, the recovery process sucks. Getting pregnant after a C-section is uncomfortable...and worth every moment.
Regardless of the incision, the recovery process sucks. Getting pregnant after a C-section is uncomfortable...and worth every moment.
So what are the options for pregnancies after a Caesarian? Knowing your limits, resting when possible, asking for help when its available, and lifting only when necessary. I have a medical belly brace to help with the weight distribution of my behbeh, but I personally don't feel much of a difference other than not being able to sit down. I can't babywear my toddler anymore so the stroller gets much more use now. The many stairs in our townhouse require additional planning but its doable. Rest happens whenever my toddler naps. And a bonus tip from me: Stay as regular as possible when it comes to your stomach! Eat well and often - and be sure you "go" well and often. Constipation for an already stressed out stomach is awful.
On a semi-related note, a VBAC (Vaginal Birth After Caesarian) is a very real possibility for many women. Your doctor and midwife are the best people to speak with about the risks and benefits associated with the procedure. Personally, I'm going to try to have a VBAC if the baby is projected to be under 9lbs and if my blood pressure is better this time. If history repeats itself, we'll be doing another Caesarian.
Your doctor and midwife are the best people to speak with about the risks and benefits associated with the procedure. Personally, I'm going to try to have a VBAC if the baby is projected to be under 9lbs and if my blood pressure is better this time. If history repeats itself, we'll be doing another Caesarian.
So here's to 20 more weeks of a healthy growing baby and an expanding uterus!
How to prepare for a second pregnancy
Preparation for a second pregnancy begins with planning. The first phase of preparation depends on when the new parents are planning their next child. If there is no intention of giving birth to baby-year-olds, a young mother should be protected during sex, even if she is breastfeeding. When breastfeeding, the level of hormones in a woman's body often prevents re-pregnancy, but not always. Already in the third or fourth month of a baby's life, a nursing mother can become pregnant again. Meanwhile, the ideal time interval between births is considered to be 2-3 years. nine0003
nine0003
When sexual life after childbirth is established, contraceptives are selected, and parents are firmly convinced that pregnancy will not occur by chance, you can proceed to further stages of planning. Parents should think over the social and economic aspects - how parents will earn money, how to build a career, where to live, which of the relatives can and will help them take care of the kids, and so on. Do not rely on chance, it is better to think over these issues in advance. If the family is provided with money and relatives, you can start planning at the level of physical health. nine0003
New pregnancy after first birth: what to expect
Motherhood changes a woman's body forever, even if there were no complications during pregnancy. Pregnancy is a big burden for all body systems. Therefore, when planning a second pregnancy, it is recommended to undergo a medical examination.
What to check when planning a second pregnancy:
- complete blood count;
- make an electrocardiogram; nine0016
- urinalysis;
- gynecological consultation;
- consultations of other specialists by appointment.
It is enough for a healthy mother to pass general tests and consult a gynecologist. But women who had chronic diseases before pregnancy, or symptoms appeared during it, need to consult with specialized specialists. For example, in case of diseases of the cardiovascular system, it is necessary to check the heart, and, if possible, track the dynamics of the condition by comparing the data before and after the first pregnancy. nine0003
Second pregnancy after caesarean section
More recently, giving birth by caesarean section has resulted in severe trauma for the woman. Due to the surgical invasion, a rough postoperative scar formed on the uterus, which made subsequent natural childbirth almost impossible. Fortunately, medical technology is advancing. Now, after a caesarean section, a small scar remains on the uterus, in which it is quite possible to give birth in a natural way.
Of course, if in the first birth a caesarean section was performed due to the anatomical narrow pelvis of the mother, in the second birth an operation will also be indicated. But if the cause of the caesarean was a problem associated with the pregnancy itself - for example, a transverse presentation of the fetus - then the second birth may be natural. nine0003
But if the cause of the caesarean was a problem associated with the pregnancy itself - for example, a transverse presentation of the fetus - then the second birth may be natural. nine0003
What you need to know about the first birth through caesarean section:
- how the operation was performed;
- by what method the scar was sutured and what suture material was used;
- were there any complications after the operation;
- what was the blood loss;
- what treatment was carried out after the operation.
These data will help the gynecologist to correctly assess the condition of the woman's body and draw a conclusion about the advisability of a caesarean section
Management of a second pregnancy after cesarean
The second pregnancy is usually easier for a woman, if only because she knows about the main stages of pregnancy and their features. But each subsequent pregnancy can proceed differently, and a woman may encounter many phenomena for the first time. Therefore, all recommendations remain the same: health monitoring, daily routine, proper nutrition, stress-free environment, courses for young parents, and so on. nine0003
Therefore, all recommendations remain the same: health monitoring, daily routine, proper nutrition, stress-free environment, courses for young parents, and so on. nine0003
In addition, it is necessary to monitor the condition of the scar on the uterus. The scar should be regularly examined visually and during ultrasound diagnostic sessions. By the last weeks of pregnancy, it will become clear whether a woman can give birth naturally.
When a repeat caesarean section is recommended:
- for an anatomically narrow or deformed pelvis;
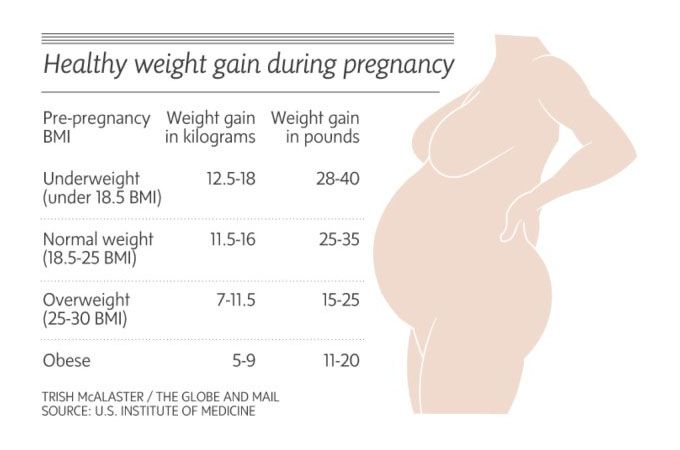
- with a child weighing over 4 kg,
- with incorrect (breech or transverse) presentation of the fetus; nine0016
- in multiple pregnancies;
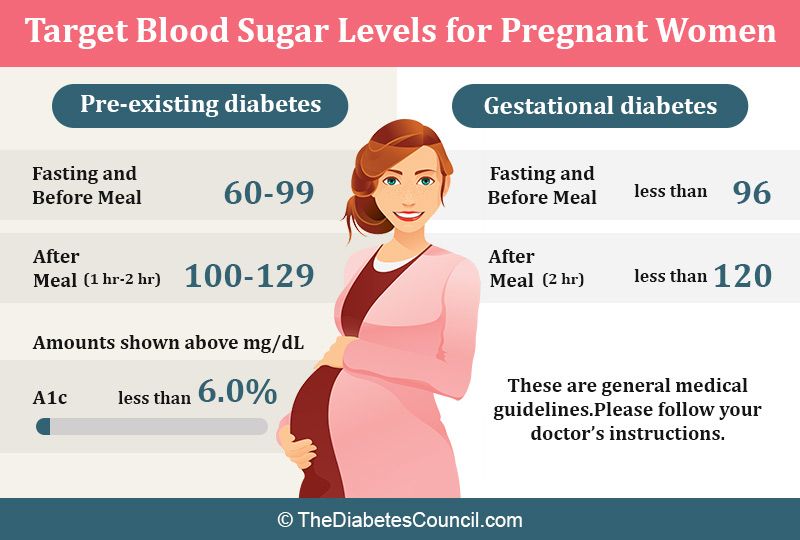
- for chronic diseases in the mother, for example, diabetes mellitus;
- for pathologies of the retina;
- with a transverse or defective scar on the uterus.
Even after repeated caesarean section, a woman can bear children and give birth if the operation was performed in a modern maternity hospital, by experienced specialists and with good equipment.
Second birth after caesarean section
"Can I have a baby after a caesarean section?" - this question is asked to doctors by women in anticipation of repeated births. Of course, yes, but ... And this “but” deserves a separate respectful attitude.
Doctor's consultation
You can get the consultation of the necessary specialist online in the Doctis application
Laboratory
You can undergo a comprehensive examination of all major body systems nine0003
- Pregnancy planning after caesarean section
- At what time is the birth plan determined with a scar on the uterus
- In what situations is the success of vaginal delivery with a scar more likely
- Use of anesthesia and stimulation in labor with a scar
- In what situations is the likelihood of complications of childbirth with a scar
Today, vaginal (natural) births with a uterine scar are becoming more common. Expectant moms are good informed about the expediency of such childbirth and insist on them, and the equipment of the majority maternity hospitals allows women to give birth through the birth canal after a previous caesarean sections. nine0003
Expectant moms are good informed about the expediency of such childbirth and insist on them, and the equipment of the majority maternity hospitals allows women to give birth through the birth canal after a previous caesarean sections. nine0003
Pregnancy after caesarean section
We are planning a second child. But I gave birth to the first one by caesarean section? When can I get pregnant? Are any examinations needed?
It is optimal to plan the next pregnancy 1-2 years after the previous caesarean section (if the attending not otherwise specified by the doctor).
Of course, it is necessary to assess the consistency of the scar on the uterus after caesarean section. In most cases during a planned gynecological ultrasound of the pelvic organs, doctors either do not describe the scar area on the uterus at all, or described as homogeneous, with no signs of thinning. nine0003
But if the area of the scar, according to the planned gynecological ultrasound, is in the form of a "niche" or thinned, a woman needs to contact an obstetrician-gynecologist to develop treatment tactics. Perhaps MRI of the pelvic organs, hysteroscopy.
Perhaps MRI of the pelvic organs, hysteroscopy.
How long can a doctor say for sure - whether natural childbirth is possible after previous ones by caesarean section?
If the scar is described as a "niche" in early pregnancy, and even more so if the gestational sac is in the "niche" area, doctors understand that natural childbirth is impossible. In these for months, gynecologists carefully monitor pregnancy and assess the risks of placenta ingrowth into a uterine scar and failure of the scar. In most cases, it is realistic to assess the possibility of natural childbirth with a scar on the uterus is possible only in the third trimester of pregnancy, at full term, at the 37th week. nine0003
The criteria for consistency of the scar on the uterus are its thickness and uniformity (they are assessed according to ultrasound data), the maturity of the birth canal, the independent onset of labor. During childbirth, discoordination of labor activity, its weakness, unsatisfactory condition of the fetus according to cardiotocography (CTG) are indirect signs of scar failure.
Natural delivery after caesarean section - features and recommendations
Are natural second births possible if the first child was born by cesarean sections? The firstborn was large, with a breech presentation.
The likelihood of a vaginal delivery is significantly lower if the woman has a large fetus during this pregnancy (and a caesarean section in previous births was performed due to a clinically narrow pelvis), breech presentation of the fetus, multiple pregnancy, acute cerebrovascular accident / stroke / brain masses, pelvic injury in the past. Another circumstance that forces us to abandon natural childbirth again is if in the previous caesarean section was made on the uterus by a corporal incision (that is, a longitudinal, not a standard one, transverse). nine0003
However, the success of vaginal delivery with a uterine scar is higher if regular labor activity began independently, subject to mature birth canals at full term pregnancy and if the indications for cesarean section in previous births were pelvic previa, placenta previa, genital herpes and other non-recurring situations.
The probability of successful vaginal delivery is lower in cases:
nine0014But remember that the final decision is still made individually, together with the obstetrician-gynecologist, leading the birth.
Is it true that in the case of natural childbirth after caesarean in the previous do anesthesia and labor stimulation?
Delivery with a scar on the uterus is possible with the use of epidural anesthesia. And here is the induction labor activity, preparation of the cervix by intracervical insertion of a Foley catheter reduce the likelihood success of natural childbirth. nine0003
nine0003
Complications in childbirth after caesarean section
There is an opinion that in our time no woman or child dies while uterine rupture. Why are doctors so afraid of women in labor with a scar on the uterus?
Speaking about the risks of uterine rupture along the scar, you need to understand that, subject to careful delivery in a specialized hospital, the risks are minimal. However, low risk does not mean no risk. Gap Probability uterus along the scar increases in parturient women:
- with large fruit,
- for labor activation with oxytocin,
- with a scar after two or more caesarean sections,
- with a scar after a corporal caesarean section,
- in case of complicated course of the postoperative period (with endometritis),
- when using prostaglandins.
If you have any questions, you can ask your doctor obstetrician-gynecologist online in Doctis app.