Milk engorgement pain
Breast pain and breastfeeding - NHS
There are a number of reasons why you may experience breast pain while you're breastfeeding.
Always ask for help from your midwife, health visitor or breastfeeding specialist if you're having problems breastfeeding.
Here's how to deal with some of the most common causes.
Breast engorgement
Breast engorgement is when, for whatever reason, your breasts become overly full. They may feel hard, tight and painful.
In the early days, engorgement can be due to your milk coming in. Newborns need feeding little and often. It can take a few days for your milk supply to match your baby's needs.
If your baby is not well attached to the breast, it may be hard for them to take your milk when your breast is engorged.
The nipple can become a little overstretched and flattened, and possibly painful.
Ask your midwife, health visitor or a breastfeeding specialist for advice immediately to help your baby relieve the engorgement and prevent it happening again.
Find out more about positioning and attachment
Engorgement can still happen once you have learnt the skill of positioning and attachment, usually when your baby has not fed for a while.
Your baby usually knows when they need a feed, for how long and from which breast.
Early signs (cues) that your baby is ready to feed can include:
- moving their eyes rapidly
- putting their fingers into their mouth
- rooting (turning to 1 side with their mouth open as if seeking the breast)
- becoming restless
Crying is the very last sign that your baby needs feeding. Feeding them before they cry often leads to a much calmer feed.
Feeding them before they cry often leads to a much calmer feed.
Keeping your baby close so you can watch and learn their early feeding cues will help.
How to ease breast engorgement
To ease the discomfort of engorgement, apart from your baby feeding, you could try expressing a little breast milk by hand. Only express enough to relieve the discomfort because expressing more will make you produce more milk.
Ask your midwife, health visitor or breastfeeding specialist to show you how.
Find out more about expressing breast milk
You may also find it helps to:
- wear a well-fitting breastfeeding bra that does not restrict your breasts
- put warm flannels on your breasts just before hand expressing if they're leaking
- take some paracetamol or ibuprofen at the recommended dose to ease the pain (these are safe to take while you're breastfeeding)
Too much breast milk
Occasionally women make too much breast milk and their babies struggle to cope.
It's best to get your midwife, health visitor or breastfeeding specialist to watch a feed to see if they can spot why this is happening.
They can also suggest ways to decrease your supply.
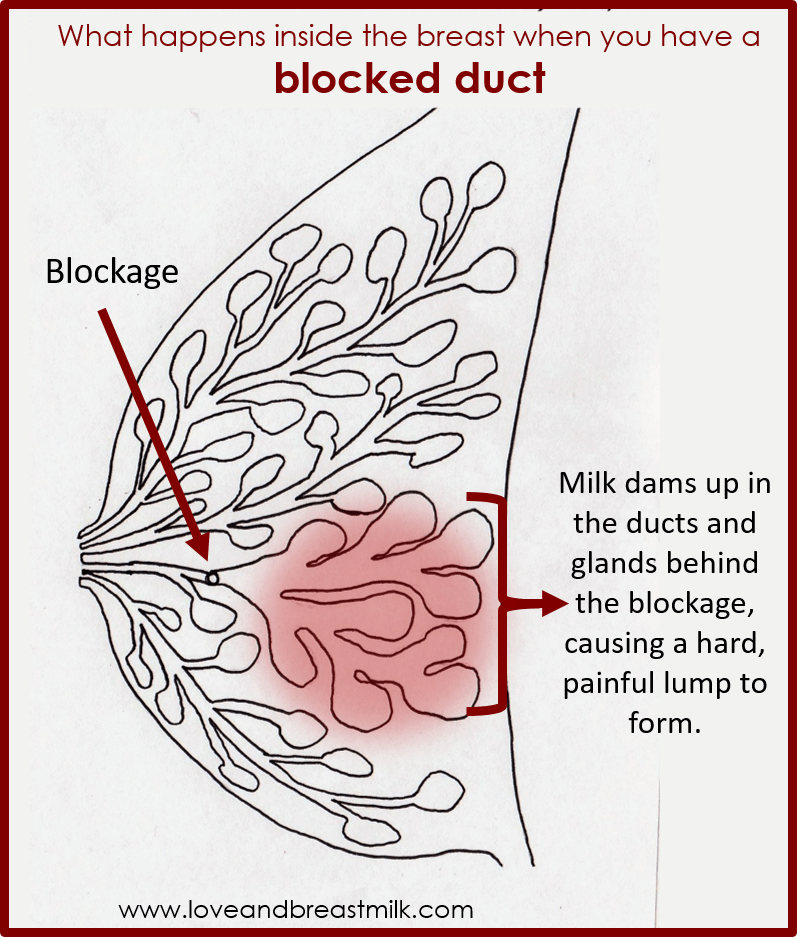
Blocked breast milk ducts
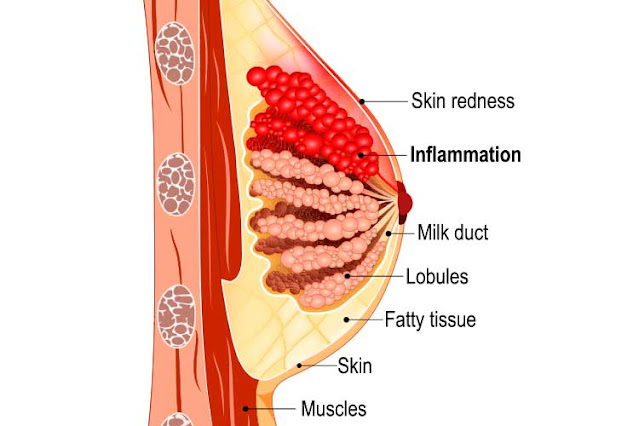
The milk-making glands in your breasts are divided up into segments, rather like an orange.
Narrow tubes called ducts carry the milk from each segment to your nipple.
If one of the segments is not drained properly during a feed (perhaps because your baby is not attached properly), this can lead to a blocked duct.
You may feel a small, tender lump in your breast.
Avoid wearing tight clothes or bras so your milk can flow freely from every part of your breast.
Other things that may help include:
- frequent feeding from the affected breast
- warm flannels or a warm shower to encourage the flow
- gently massaging the lump towards your nipple while your baby feeds
It's important to deal with a blocked duct quickly as, if left, it could lead to mastitis.
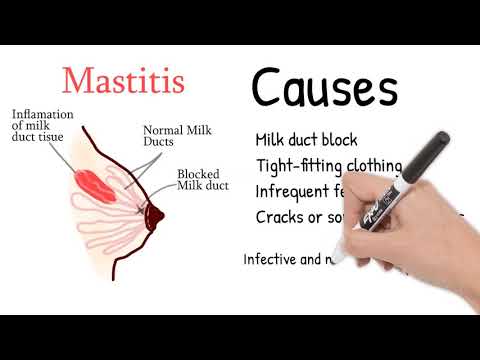
Mastitis
Mastitis (inflammation in the breast) happens when a blocked duct is not relieved.
It makes the breast feel painful and inflamed, and can make you feel very unwell with flu-like symptoms.
If you do not deal with the early signs of mastitis, it can turn into an infection and you'll need to take antibiotics.
Symptoms of mastitis include:
- a breast that feels hot and tender
- a red patch of skin that's painful to touch
- a general feeling of illness, as if you have flu
- feeling achy, tired and tearful
- a high temperature
If you think you're developing a blocked duct or mastitis, try the following:
- Carry on breastfeeding.
- Check your baby's positioning and attachment. Ask your midwife, health visitor or a breastfeeding specialist to watch a feed.
- Let your baby feed on the tender breast first.
- If the affected breast still feels full after a feed, or your baby cannot feed for some reason, express your milk by hand.
- Warmth can help the milk flow, so a warm flannel, or a warm bath or shower, can help.
- Get as much rest as you can. Go to bed if you can.
- Take paracetamol or ibuprofen to relieve the pain.
Contact your GP or NHS 111 if you feel worse at any time, or if you're no better within 12 to 24 hours.
You may need antibiotics, which will be fine to take while breastfeeding.
Stopping breastfeeding will make your symptoms worse, and may lead to a breast abscess.
Breast abscess
If a mastitis infection is not treated, it can lead to a breast abscess, which may need an operation to drain it.
This can also develop if the mastitis does not respond to frequent feeding plus a course of antibiotics.
You can carry on breastfeeding after an abscess has been drained.
Find out more about breast abscesses
Thrush
If you experience pain in both breasts, often after a period of pain-free breastfeeding, and the pain lasts for up to an hour after a feed, you may have developed thrush.
Find out more about thrush and breastfeeding
Got a breastfeeding question?
Chat to the Start4Life Breastfeeding Friend on Amazon Alexa, Facebook Messenger or Google Home for fast, friendly, trusted NHS advice any time, day or night.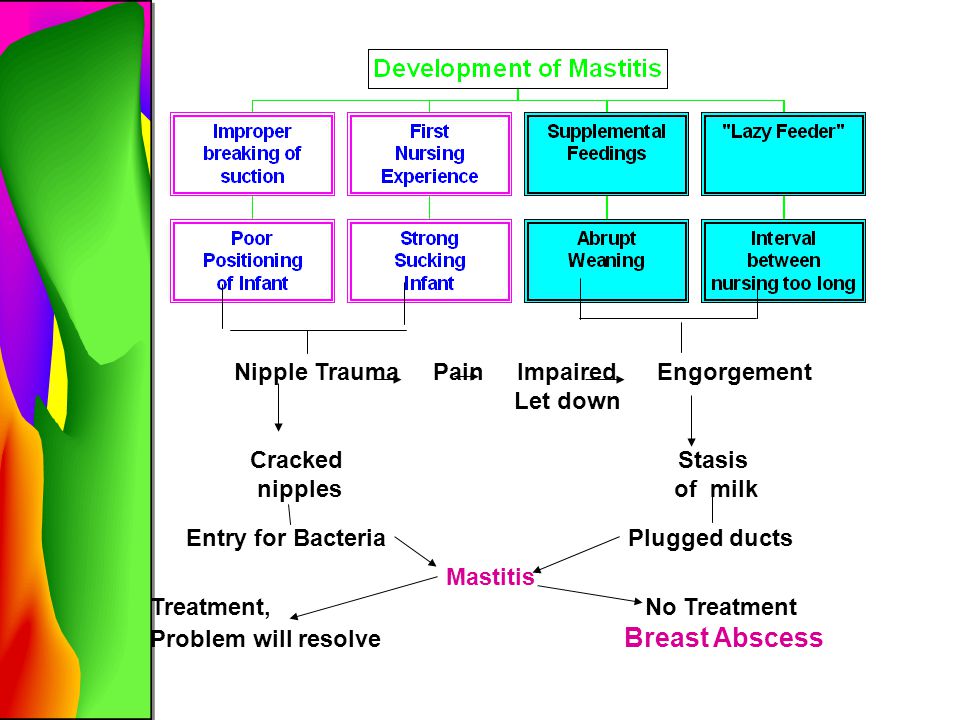
Engorged Breasts - avoiding and treating
You are here: Home / Breastfeeding information / Engorged Breasts – avoiding and treating
Engorged breasts are painful. They feel heavy, hard, warm and sensitive —as if they are ready to burst! As well as being painful, engorgement can lead to other breastfeeding problems if not treated. Being able to recognise engorgement will help you to treat it promptly, avoiding complications.
Most mothers experience some engorgement in the first weeks after birth. With changing hormone levels, your breasts swell and enlarge as milk production increases. It may seem as though they are filling up with milk, but engorgement is more than milk storage. Your body directs extra blood and fluids to your breasts to boost milk production. This causes congestion and swelling which will decrease as your body adjusts.
Minimizing early engorgement
Treat engorgement to…
When to treat engorgement
After the first few weeks
Causes of engorgement
Treating engorgment
Be sure your baby is sucking effectively
Reverse pressure softening
Keep comfortable
Watch out for signs of mastitis
Minimizing early engorgement
New mothers vary in how engorged their breasts become in the weeks after birth; some experience little engorgement, others describe their breasts as feeling like watermelons!
Try these suggestions
- Breastfeed your baby frequently from birth: at least 8–12 times in 24 hours.
 Keeping your baby close makes it easier to nurse every hour or two.
Keeping your baby close makes it easier to nurse every hour or two. - If your baby is sleepy, perhaps from a medicated birth, you may need to wake him and encourage him to nurse.
- Aim to be comfortable while breastfeeding, and learn how to get your baby latched on well.
- If your newborn is unable to breastfeed, hand express frequently until your milk ‘comes in’, then combine with using a hospital-grade electric breastpump to help establish your milk production and relieve engorgement. Your milk can be given to your baby until he is able to nurse.
Treat engorgement to…
Make breastfeeding easier
Even if you feel as though you have lots of milk, engorgement can make it harder for your baby to latch on to your breast and feed well. A poor latch-on can give you sore nipples. Your baby may also have trouble coping with the flow of milk from engorged breasts.
Protect milk production
When milk isn’t removed from your breasts, you will produce less milk.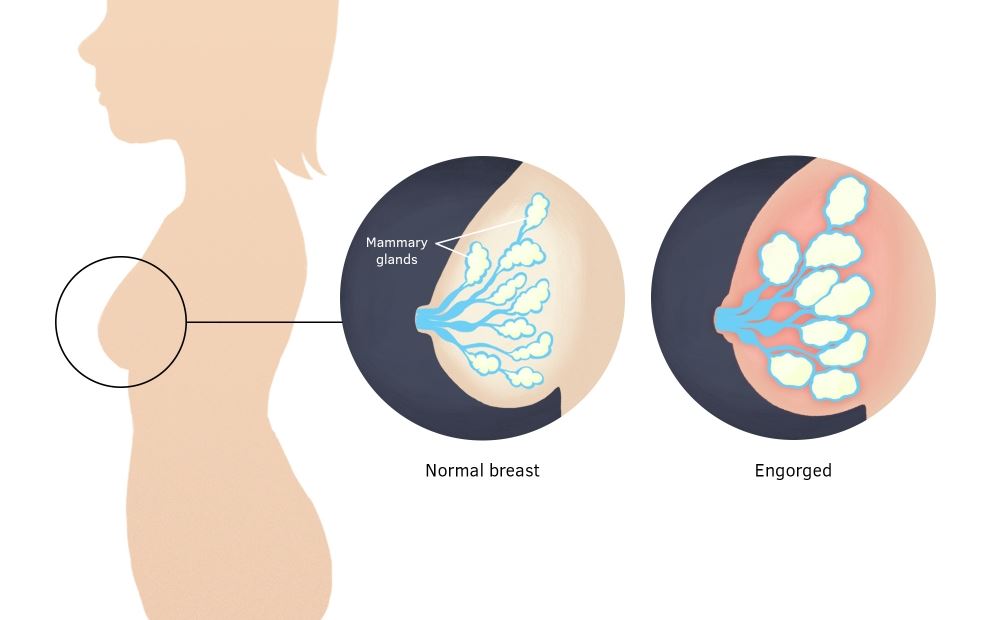 Treating engorgement gives your baby more milk now and helps protect milk production for when your baby is older.
Treating engorgement gives your baby more milk now and helps protect milk production for when your baby is older.
Avoid blocked ducts or mastitis
Engorgement can result in blocked ducts leading to mastitis.
When to treat
Take action to relieve engorgement if your breasts feel firm, hard, shiny or lumpy. When milk is removed, blood circulation improves and swelling reduces. Use the suggestions below to reduce swelling and keep your milk flowing. Many mothers have a slight temperature when their breasts are engorged. Temperatures under 38.4ºC are not usually associated with infection. Keep your baby close and continue breastfeeding.
Engorgement after the first weeks
Treat as outlined below while working out the cause so you can prevent it happening again.
Common causes of engorgement are:
- A missed feed or expressing session.
This can easily happen during holidays and festivities or when visitors arrive. Encourage your baby to feed more often, or express more frequently if you’re apart from your baby.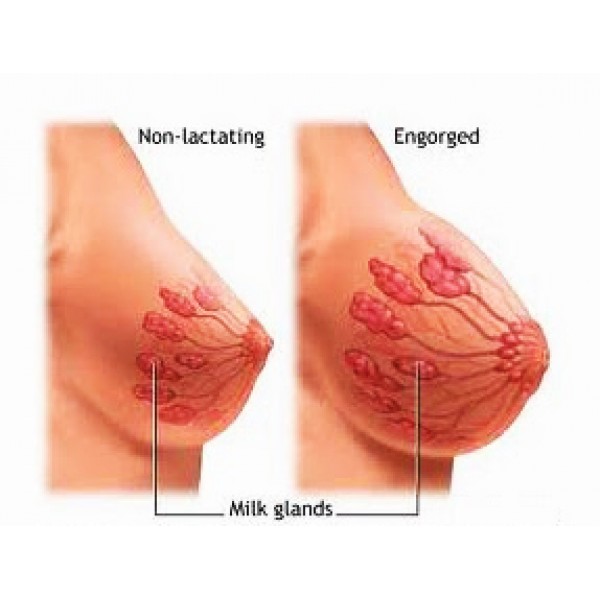
- Feeding a baby on a schedule
Recent research has revealed that mothers vary in how much milk their breasts can store without becoming uncomfortable. Mothers following routines often suffer from engorgement, mastitis and low milk production because their breasts are not drained often enough. - Expressing milk.
Some books advise expressing to keep milk production one step ahead of a baby’s needs. However, making more milk than your baby needs can increase your risk of engorgement and mastitis, especially if you go for several hours without feeding or expressing. - A baby who is unable or unwilling to nurse well for any reason
Expressing milk frequently until your baby can nurse well will help you maintain milk production and avoid blocked ducts or mastitis. - Weaning from the breast too quickly
If you experience engorgement during weaning, you may need to slow down the process. This will give your breasts time to adjust to the reduced demand for milk. If breastfeeding more often is not an option, try expressing just enough milk to relieve the fullness by hand or pump.
If breastfeeding more often is not an option, try expressing just enough milk to relieve the fullness by hand or pump.
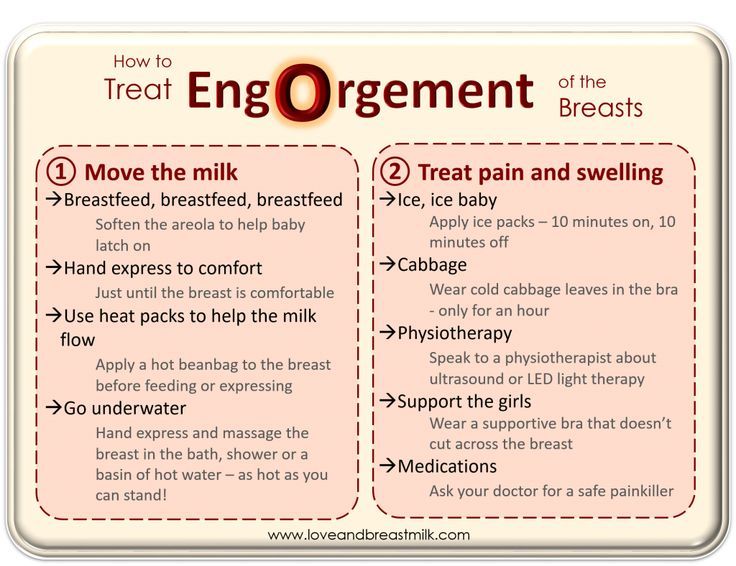
Treating engorgement
Reduce swelling and keep milk flowing:
- Aim to breastfeed every 1½ to 2 hours during the day, and at night every 2–3 hours from the start of one feed to the start of the next. Let your baby finish on the first breast before switching to the second
- Avoid using bottles or dummies. If a supplement is needed try using a spoon, flexible feeding cup or syringe.
- Between feeds, apply ice for 15–20 minutes at a time between feeds to reduce swelling. Use an ice pack, crushed ice in plastic bags or bags of frozen vegetables (that can be refrozen several times before being thrown away). Wrap them in a lightweight towel to protect your skin.
- Just before feeding, apply moist warmth to your breasts for up to two minutes to help milk flow. Try a warm wet towel, warm shower or immersing breasts in a bowl of warm water.
 Then, express to comfort if your baby isn’t ready to feed.
Then, express to comfort if your baby isn’t ready to feed. - Use gentle massage from the chest wall toward thenipple area in a circular motion.
Be sure your baby is sucking effectively:
Position your baby with his chest and tummy in full contact with your body. With his cheek in close contact with your breast, your baby can easily tip back his head to latch on. This way he’ll take a large mouthful of breast. Listen for swallowing as he feeds.
If your baby is finding it hard to latch on – when your baby bobs his head and licks the nipple, he naturally makes it easier to latch on.
For more information on getting your baby positioned and attached comfortably see here.
Reverse pressure softening
works by moving fluid away from the nipple area.
- Press all five fingertips of one hand around the base of the nipple. Apply gentle steady pressure for about a minute to leave a ring of small dimples on the areola.
- You can also press with the sides of fingers.
 Place your thumb on one side of the nipple and two fingers on the other side where your baby’s lips will be.
Place your thumb on one side of the nipple and two fingers on the other side where your baby’s lips will be. - If this isn’t enough, gently hand express a little milk before feeding to soften the areola. If you choose to use a breastpump, set it to minimum suction.
Keep comfortable:
- Ask your midwife or GP to recommend an over-the-counter, anti-inflammatory medication suitable for breastfeeding mothers to relieve pain and swelling.
- A well-fitting, supportive bra may help. Avoid bras (and underwires) that are tight or put pressure on specific areas of the breast.
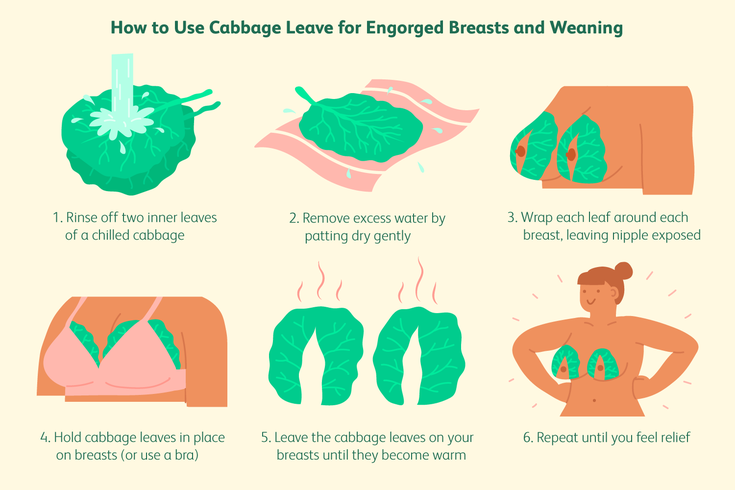
- Cold, raw cabbage leaves worn inside a bra can be soothing. Change when they become wilted or after about 2 hours. Use only until swelling goes down as long-term use may reduce milk supply. Stop use if a skin rash or other signs of allergy appear.
Watch out for symptoms of mastitis:
- Inflamed, hot, red or darkened localised areas of your breast, depending on your skin tone.
 Changes in breast appearance may be harder to spot in darker skin. You may still have engorged breasts without a noticeable red or darkened area.
Changes in breast appearance may be harder to spot in darker skin. You may still have engorged breasts without a noticeable red or darkened area. - Temperature over 38.4ºC or flu-like symptoms.
- Weaning can make a breast infection worse so continue to breastfeed frequently especially on the affected side and treat as for engorgement. Rest and drink fluids. If fever persists, continue breastfeeding and check with your GP as you may need antibiotics. More information on mastitis.
Engorgement should improve within a day or two. If not, contact an LLL Leader for further suggestions. You may need to improve your baby’s breastfeeding technique or find ways to reduce your milk supply. These are not difficult problems to solve, especially if treated promptly.
Written by Karen Butler, Sue Upstone & mothers of La Leche League Great Britain
Further Reading
The Womanly Art of Breastfeeding. LLLI. London: Pinter & Martin, 2010.
Beginning Breastfeeding
Comfortable Breastfeeding
Dummies and Breastfeeding
Hand Expression of Breastmilk
Mastitis
My Baby Won’t Breastfeed
Nipple Pain – why and what to do
Positioning and Attachment
Sleepy Baby – why and what to do
This information is available to buy in printed format from our shop
Copyright LLLGB 2016
Filed Under: Breastfeeding information, Common Concerns Tagged With: blocked ducts, engorgement, express, expressing, lumps, mastitis, milk, newborn / beginning breastfeeding, red, reverse pressure softening, swollen
What is breast swelling? | Breast swelling
Some mothers experience breast swelling when milk begins to flow in the first days after childbirth. Usually this phenomenon is temporary and easily eliminated. Read our article to find out how to help yourself.
Usually this phenomenon is temporary and easily eliminated. Read our article to find out how to help yourself.
Share this information
Sioned Hilton, health visitor, neonatal nurse and lactation consultant:
Schoned, a mother of three, has been supporting families with newborns and young children for over 30 years. She provides advice on breastfeeding and pumping, both in clinics and at home. In addition, Schoned writes articles for parenting magazines, attends conferences, and conducts seminars for attending physicians.
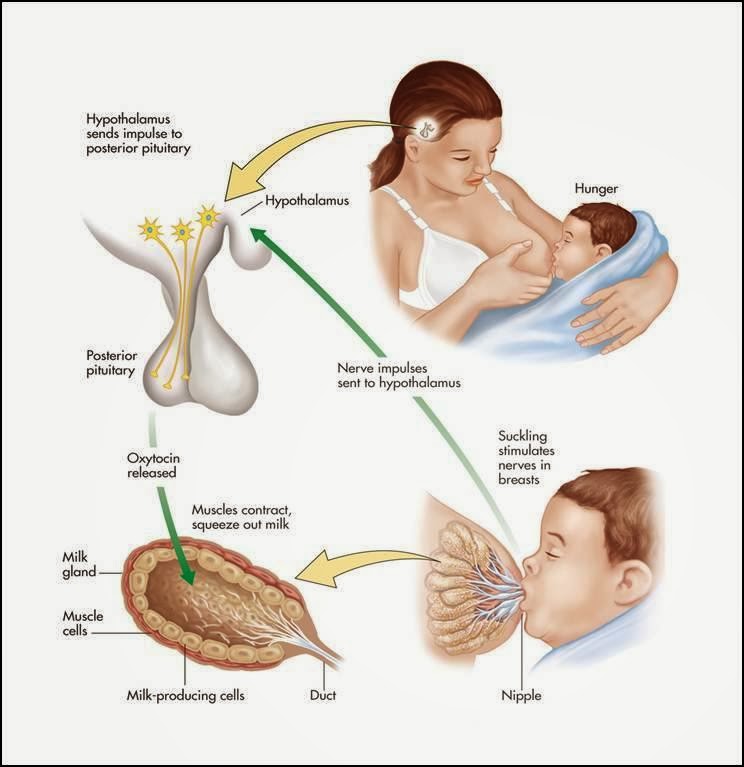
When you start breastfeeding, you first produce a small amount of colostrum, which gradually increases over the first few days. After about two to four days, production increases significantly. This phenomenon is called the "arrival" of milk. 1
One of the signs that milk is starting to come in is a change in the breast - it fills up and becomes firmer. This is due not only to an increase in the amount of milk, but also to increased blood flow and additional lymphatic fluid to the breast tissues. 2
2
If the child eats well and often, then for most mothers this feeling of heaviness disappears over time without any complications. However, some women produce so much milk that their breasts fill up and become painful and very hard. This condition is called breast swelling. And although everything usually passes in a day or two, this period can be quite painful.
How does breast swelling manifest itself?
Swelling may affect one or both breasts. It can cause swelling, sometimes down to the armpits, and a throbbing sensation. The chest becomes quite hot, sometimes lumps are felt in it. All this is due to the fact that a huge number of processes take place inside. You may also notice other symptoms, such as the skin on your breasts becoming shiny and tight, and your nipples becoming hard and flat. Swelling of the mammary glands can even cause a temperature to rise to 37.5–38.3°C (99–101°F). 3
In addition to painful sensations, breast swelling is also dangerous because it can make breastfeeding difficult, and this, in turn, will worsen the situation even more. If the baby finds it difficult to latch on because the nipples have become flat and the breast tissue is firmer, nipples may become inflamed. In addition, in the event of a poor grip, he will not be able to completely empty the chest. Thus, if left untreated, swelling of the mammary glands can lead to blockage of the milk ducts, mastitis, and reduced milk production.
If the baby finds it difficult to latch on because the nipples have become flat and the breast tissue is firmer, nipples may become inflamed. In addition, in the event of a poor grip, he will not be able to completely empty the chest. Thus, if left untreated, swelling of the mammary glands can lead to blockage of the milk ducts, mastitis, and reduced milk production.
What causes breast swelling?
Usually breast swelling is due to the fact that the child does not feed often enough (less than eight times a day). In principle, this can happen to any mother, but women who have undergone various breast surgeries, including breast augmentation, are more prone to swelling of the mammary glands. 2 Wearing a bra that is the wrong size or that is too tight can increase discomfort and lead to clogged milk ducts and even mastitis.
Breast swelling can occur in both breastfeeding mothers and mothers who are not or cannot breastfeed. The hormonal changes that occur after the birth of a baby and the release of the placenta and increase milk production are independent of whether you are breastfeeding or not. Swelling can also occur if the number of feedings is drastically reduced, for example, if the child becomes ill, sleeps longer, starts eating solid foods, or goes to nursery.
Swelling can also occur if the number of feedings is drastically reduced, for example, if the child becomes ill, sleeps longer, starts eating solid foods, or goes to nursery.
How to treat breast swelling?
2The best cure for swollen breasts is a hungry baby! Try to empty your breasts as much and as often as possible to facilitate the release of milk. To do this, feed your baby on demand, preferably eight to twelve times a day.
Maintain skin-to-skin contact with your baby, cuddling as often as possible during the day and at night when you are awake. This will allow him to smell the attractive smell of your milk and have easy access to the breast, and you will be able to better monitor signs that he is hungry and, accordingly, feed more often. Let the baby eat enough from one breast before offering the second.
It's a good idea to see a lactation consultant or specialist to check if your baby is properly grasped and positioned. It depends on how well he will eat and empty his chest. The tips below will also help you relieve the symptoms of breast swelling.
The tips below will also help you relieve the symptoms of breast swelling.
Tips for relief of breast swelling 2
- Breastfeed at least eight times a day.
- Make sure your baby is latching on well.
- Try other feeding positions.
- Gently massage your breasts during feeding to improve the flow of milk.
- Express some milk by hand or with a breast pump before feeding to soften the nipple and make it easier for your baby to latch on.
- If your breasts are still firm and full after a feed, pump more until you feel better.
- If your baby cannot breastfeed, express milk for him. Pumping must be continued until the breast becomes softer, and do this at least eight times a day.
- Try the areola pressure softening technique. This helps to remove excess fluid from the breast. A lactation consultant or specialist will show you how to do this.
- If milk leaks, try taking warm showers or applying warm flannel to your breasts just before feeding or pumping to soften your breasts and make it easier for your milk to flow.
 You should not, however, warm the chest for more than two minutes, as this can only increase swelling.
You should not, however, warm the chest for more than two minutes, as this can only increase swelling. - If your milk isn't leaking, try applying cold compresses, chilled gel pads, or even frozen green peas wrapped in a towel for ten minutes after feeding to reduce swelling and relieve pain.
- Put clean cabbage leaves in your bra. Yes Yes! For many moms, it really helps reduce swelling and discomfort, and there are scientific explanations for this. 4
- Take an anti-inflammatory pain reliever. While breastfeeding, you can take some medications, in consultation with your doctor. Always consult your doctor, follow the drug manufacturer's instructions and the pharmacist's recommendations. To learn more about medications and breastfeeding, read our article on breastfeeding when sick.
- Wear an appropriately sized and comfortable nursing bra, avoid underwire or no bra at all.
- Do not skip feedings or stop breastfeeding abruptly as this may increase breast swelling.
Seek medical advice if your 5 temperature rises above 38 °C or if your baby is unable to suckle due to breast swelling.
And in any case, try to remain calm. Your body is just getting used to producing milk and feeding your baby. Breast swelling should go away on its own soon after you both get comfortable with breastfeeding.
Literature
1 Pang WW, Hartmann PE. Initiation of human lactation: secretory differentiation and secretory activation. J Mammary Gland Biol Neoplasia. 2007;12(4):211-221. - Pang, W.W., Hartmann, P.I., "Lactation initiation in the lactating mother: secretory differentiation and secretory activation." G Mammary Gland Biol Neoplasia. 2007;12(4):211-221.
2 Berens P, Brodribb W. ABM Clinical Protocol# 20: Engorgement, Revised 2016. Breastfeed Med . 2016;11(4):159-163. - Behrens P, Brodrhibb W, "AVM Clinical Protocol #20: Engorgement, 2016 edition". Brestfeed Med (Breastfeeding Medicine). 2016;11(4):159-163.
Brestfeed Med (Breastfeeding Medicine). 2016;11(4):159-163.
3 Affronti M Low-grade fever: how to distinguish organic from non-organic forms. Int J Clin Pract. 2010;64(3):316-321. - Affronti M. et al., "Subfebrile temperature: how to distinguish organic from non-organic cases." Int Zh Klin Prakt. 2010;64(3):316-321.
4 Boi B et al. The effectiveness of cabbage leaf application (treatment) on pain and hardness in breast engorgement and its effect on the duration of breastfeeding. JBI Libr Syst Rev . 2012;10(20):1185-1213. - Boys B. et al., "Effectiveness of cabbage leaf (as a drug) for breast pain and engorgement, and its effect on the duration of breastfeeding." JBAi Libr Sist Rev. 2012;10(20):1185-1213.
5 NHS Choices. How do I take someone's temperature? [Internet]. UK: NHS Choices; updated 2016 June 29. Available from : www.nhs.uk/chq/pages/1065.aspx?categoryid=72 - NHS Choice. "How to measure the temperature?" [Internet]. United Kingdom: NHS Choice, 29 June 2016 edition Article linked: www.nhs.uk/chq/pages/1065.aspx?categoryid=72
UK: NHS Choices; updated 2016 June 29. Available from : www.nhs.uk/chq/pages/1065.aspx?categoryid=72 - NHS Choice. "How to measure the temperature?" [Internet]. United Kingdom: NHS Choice, 29 June 2016 edition Article linked: www.nhs.uk/chq/pages/1065.aspx?categoryid=72
Solving nine breastfeeding problems in the first month
Expert advice on solving major breastfeeding problems in the first month.
Share this information
Cathy Garbin, child health nurse, midwife and lactation consultant:
Cathy, a mother of two, was a research fellow at the renowned Human Lactation Research Institute, founded by Peter Hartmann, for seven years, providing support to breastfeeding mothers in clinics and at home. Today, she still works as a family counselor, and also conducts seminars for attending physicians and speaks at international conferences.
Breastfeeding is as much a skill as driving a car, and in the first month mother and baby may encounter some obstacles along the way. It takes time and experience to make it familiar to both of you. Solving breastfeeding problems in the first month helps to establish good milk production and increase the duration of breastfeeding in the future. Below you will find tips on how to overcome the main breastfeeding challenges that mothers often face from the end of the first week to the end of the first month after giving birth.
It takes time and experience to make it familiar to both of you. Solving breastfeeding problems in the first month helps to establish good milk production and increase the duration of breastfeeding in the future. Below you will find tips on how to overcome the main breastfeeding challenges that mothers often face from the end of the first week to the end of the first month after giving birth.
Problem #1. A painful lump appeared in the breast
Lumps and bumps in the breast of a nursing woman can appear for various reasons. One of the most common is blockage of the milk ducts, which results in a hard and painful lump that can become inflamed.
Solutions 1–3
- Massage the inflamed area, especially while breastfeeding or expressing, to clear the blockage.
- Gently place warm flannel on your breast or take a warm shower before feeding to relieve discomfort.
- Continue breastfeeding as usual to avoid milk accumulation that can cause mastitis.

- Try to express milk from the inflamed breast after feeding to ensure that it is completely emptied. This will help to remove the blockage and restore the patency of the duct. See what breast pumps* Medela has to offer and choose the right one for you.
- Try ultrasound therapy. If you have repeated blocked ducts, your lactation consultant or healthcare professional may suggest this procedure to help restore milk flow. The procedure is performed by a physiotherapist.
- Call your healthcare provider, if you notice signs of infection (breast redness and tenderness or flu-like symptoms such as fever, aches, malaise and headache), or if you think the lump is not related to breastfeeding .
Problem #2. The breast is red and sore
If one or both mammary glands are red and sore, and this is not due to blockage of the ducts, mastitis, that is, inflammation of the breast tissue, is not excluded. Mastitis is characterized by redness, burning, and soreness of the breasts, combined with flu-like symptoms: You feel hot and cold, your joints ache, and your temperature rises above 38.5 °C (101.3 °F). Seek medical attention immediately if you experience these symptoms. Mastitis needs to be treated as soon as possible, as your condition can worsen in just a few hours. 3
Mastitis is characterized by redness, burning, and soreness of the breasts, combined with flu-like symptoms: You feel hot and cold, your joints ache, and your temperature rises above 38.5 °C (101.3 °F). Seek medical attention immediately if you experience these symptoms. Mastitis needs to be treated as soon as possible, as your condition can worsen in just a few hours. 3
Mastitis can be caused by the following causes:
- no treatment for blocked ducts,
- Bacteria entering the breast through cracked and damaged nipples,
- improper attachment of the child to the breast,
- long periods between feedings,
- breasts too full,
- wearing a bra that is too tight or that cuts into the skin,
- Abrupt weaning,
- excess milk.
Solutions 3
In addition to seeking medical attention:
- Continue to breastfeed or express milk frequently.
 Your milk is still safe for your baby. Its release will help eliminate blockage of the ducts and prevent painful accumulation of milk. Sudden cessation of feeding or pumping may exacerbate symptoms. After feeding, it is advisable to express any remaining milk.
Your milk is still safe for your baby. Its release will help eliminate blockage of the ducts and prevent painful accumulation of milk. Sudden cessation of feeding or pumping may exacerbate symptoms. After feeding, it is advisable to express any remaining milk. - Give the child the inflamed breast first. This way the child can empty it completely. If it hurts too much, start feeding on the healthy breast, and when milk begins to flow, go back to the first one.
- Have a good rest, drink and eat. You need to get enough fluids and good nutrition.
- Massage the sore area under a warm shower or apply a warm flannel or warm pack to clear the blockage and relieve symptoms before breastfeeding or pumping.
- Apply a cooling pack after feeding, , to reduce inflammation.
Problem #3. My strength is running out
Breastfeeding in the first weeks can be very tiring and seem endless. The baby will ask for a breast every few hours, day and night, and you have not yet grown stronger after giving birth.
The baby will ask for a breast every few hours, day and night, and you have not yet grown stronger after giving birth.
Solutions
- Take care of yourself. This may be easier said than done when you have a newborn in your arms, but still try to get as much rest as possible, eat healthy and regular meals, and drink plenty of water. Do not refuse the help of your partner, relatives and friends, or even hire an assistant if you can afford it.
- Feed lying down. This will allow you to relax and reduce stress on sore spots, stitches or c-section scars.
- Do not skip feedings. Your partner may offer to bottle feed your baby while you are resting. However, despite this temptation, it should be remembered that milk production is best established in the first four weeks through breastfeeding. When breastfeeding is well established, you can give your baby expressed milk, but before that, ask family or friends to help you with other things so you can fully focus on breastfeeding.
Problem #4. How can I increase breast milk production?
It's easy to question whether your breastmilk supply is adequate, especially when your baby has developmental spikes between the third and fourth weeks. It may seem to you that the child asks for breasts more often because he does not have enough milk. However, if the number of wet and soiled diapers doesn't change—see Breastfeeding: What to Expect in the First Month—the baby is likely to breastfeed more often to calm down. The baby is surrounded by many new sounds and images that are easy to get tired of, and at the breast he feels safe. 4
Solutions 4.5
- Do not try to supplement your baby with formula, unless doctors are worried about weight gain or fluid loss. Continue breastfeeding your baby. This will help naturally increase breast milk production.
- Do not feed on a schedule. Feed your baby on demand.
 Thus, the production of breast milk will adapt to his needs.
Thus, the production of breast milk will adapt to his needs. - Use the breast pump, , to help increase breast milk production while continuing to breastfeed.
Problem #5. I have too much milk
Hyperlactation, or too much milk, can also be difficult for you and your baby. You may experience discomfort from swollen and leaking breasts, and your baby may have difficulty latch-on, choke on the milk flowing too fast, and be unable to empty the breast properly. 6
Solutions
- Express some breast milk at the start of a feed to reduce the force of the flush. Don't pump too much as this can aggravate the situation - pump only as much as needed to ease the discomfort. Try hand pumping or use a breast pump (check out the Medela* breast pump range and choose the right one for you).
- Use the towel or pad to soak up excess milk, or place the milk collection pad** on the other breast while you breastfeed first.
- The child must feel supported. Hold him firmly (this gives a sense of security) and in a comfortable position so that he can turn his head. Talk to the baby during the first rapid flush, then he will not be frightened by surprise and will not push the breast.
- Contact a lactation consultant or health care professional who will monitor you and suggest single-sided feedings or hourly breast changes (“breast duty”) to normalize your milk supply.
- Be patient . Problems with milk production usually go away after a few weeks.
Problem #6. I have different breasts!
You have noticed that the baby has a preference for one breast, or that one breast produces more milk than the other, and as a result, the mammary glands have acquired different sizes and shapes. This happens quite often and does not pose any problems for breastfeeding. If this does not bother you or your baby, you can leave everything as it is. If this makes you uncomfortable, try the following tricks.
If this makes you uncomfortable, try the following tricks.
Solutions
- Offer less demanded breasts first during feeding as babies usually suckle more vigorously at the beginning of a feed.
- Use the breast pump to increase breast milk production in the smaller breast.
- Don't give up on bigger breasts. Breastfeeding should continue with fuller breasts to avoid blocked ducts and mastitis.
- See a doctor. Sometimes an ear infection is the reason for a baby to latch on only one side. However, some positions may cause him discomfort, so try to keep the child more upright. In addition, a breast infection can change the taste of milk and cause milk to be rejected as well.
Problem #7. A blister has appeared on the nipple
With frequent feeding, sometimes painful friction occurs, and a blood bubble may appear on the breast,
nipple or areola. 7
7
Solutions
- Ask a lactation consultant or specialist to check the baby's latch on. A shallow grip can cause blistering of the nipples and areolas.
- Talk to your doctor about what medicine you can take to relieve pain if needed.
- Try other feeding positions to avoid pressure on the painful area.
- Lubricate inflammation with pure lanolin.
- Use Breast Pads** to avoid rubbing your blister with clothing and help it heal faster with air circulation, or try cooling hydrogel pads** to help relieve pain and promote healing.
- Try expressing milk. Using a breast pump can be an alternative way to get breast milk without bladder irritation. Choose the correct funnel size so that the nipple can move freely and the bubble does not rub against the walls of the tunnel.
- Do not pierce the vial as this may lead to infection.
- Seek medical attention, if the problem persists and causes you pain.
Problem #8. Painful white spot on nipple
When the opening of the milk duct is blocked by milk or a thin layer of skin grows over it, a small white or yellowish spot may appear on the tip of the nipple. For some, these blocked ducts, sometimes called milk vesicles or blisters, cause pinpoint pain, especially during feeding or pumping. Others do not experience any discomfort. White blisters may persist for several days or weeks until the skin breaks and hardened milk comes out. 8
Solutions
- Follow the tips above to solve friction bubble problems.
- Remove the blockage, if you see that the milk cork is starting to bulge. Try to squeeze it out very gently with clean nails.
- Continue breastfeeding or pumping, to clear the milk duct.
 If the milk duct clears during feeding, it will not harm the baby in any way.
If the milk duct clears during feeding, it will not harm the baby in any way. - Apply hot wet flannel to the vial just before feeding or pumping. This will help open the blocked duct. You can also try rubbing the area quickly with a clean, damp cloth.
- Manually express some milk before feeding, trying to push out hardened milk clots. If this does not help, feed the baby or express milk as usual. Repeat several times a day.
- Soak a cotton swab with olive oil and place it in the bra, pressing it against the bubble nipple. This will help soften the skin.
- Seek medical attention, if problem persists. Your doctor may remove the plug with a sterile needle. This should be done immediately after feeding, when the bubble is as inflated as possible.
Issue #9. My nipples hurt while breastfeeding
At the start of breastfeeding, my nipples may become more tender, sore, and even inflamed, but this usually goes away after a few days. If your baby's latch is checked by a specialist and the inflammation persists or the nipples hurt with every feeding, you may need medical attention to resolve this problem. 2.7
If your baby's latch is checked by a specialist and the inflammation persists or the nipples hurt with every feeding, you may need medical attention to resolve this problem. 2.7
The following symptoms and signs that appear on one or both breasts during or after feeding may indicate a bacterial infection or thrush:
- burning, itching or moderate to severe pain in the nipples
- pain in nipples aggravated by contact with clothing,
- nipple pain persists despite attempts to attach baby differently,
- nipples hurt to touch,
- stitching, shooting, burning or deep aching pain,
- chest pain during feeding and almost an hour after,
- hot pink nipples,
- discoloration and texture of the areola (hot pink color, darkening, dryness or peeling),
- white rash on chest or areola.
Also check if your child has any of the following symptoms and signs:
- thick white patches or coating on the tongue
- white indelible spots on the cheeks,
- bright red spotted rash on buttocks not helped by diaper rash creams.
Solutions 7
- Seek medical attention. He will most likely suggest testing for infections to make a diagnosis. Bacterial and fungal (yeast) infections are treated differently, so appropriate treatment should be started as soon as possible. There are other reasons that can cause similar nipple pain, such as eczema, psoriasis or vasospasm (narrowing of the blood vessels) in the mother and problems with latch or tongue frenulum in the child. Therefore, it is very important to make an accurate diagnosis.
- Strict hygiene. Wash hands before and after feeding and applying any medication, and after changing diapers. Change bra pads regularly, wash bras, tank tops and towels in high temperature water, thoroughly wash breast cups and anything your baby puts in her mouth, such as nipples.
- Let the nipples dry after feeding, as all infections love a warm and humid environment.
- See your doctor again if there is no improvement after a few days. Do not let the problem run its course, otherwise the situation may worsen.
Materials on the topic. Breastfeeding: what to expect in the first month
Breastfeeding: what to expect after the first month
Breastfeeding problems after the first month
Literature
1 Academy of Breastfeeding Medicine Protocol Committee. ABM clinical protocol # 20: Engorgement. Breastfeed Med. 2009;4(2):111-113.- Breastfeeding Academy Protocol Committee, "AVM Clinical Protocol #20: Breast engorgement." Brestfeed Med (Breastfeeding Medicine). 2009;4(2):111-113.
2 Jacobs A et al. S3-guidelines for the treatment of inflammatory breast disease during the lactation period. Geburtshilfe and Frauenheilkunde . 2013;73(12):1202-1208. - Jacobs A. et al., "Recommendations S -3 for the treatment of inflammatory diseases of the breast during breastfeeding. Geburtskhilfe und Frauenheilkünde. ABM Clinical Protocol# 4: Mastitis , Revized 2014. Breastfe 9009 H., Academy of Breastfeeding Protocol Committee, AVM Clinical Protocol #4: Mastitis, March 2014 edition of Brestfeed Med (Breastfeeding Medicine). 2014;9(5):239-243.
Geburtskhilfe und Frauenheilkünde. ABM Clinical Protocol# 4: Mastitis , Revized 2014. Breastfe 9009 H., Academy of Breastfeeding Protocol Committee, AVM Clinical Protocol #4: Mastitis, March 2014 edition of Brestfeed Med (Breastfeeding Medicine). 2014;9(5):239-243.
4 Kent JC et al. Principles for maintaining or increasing breast milk production. J Obstet , Gynecol , & Neonatal Nurs . 2012;41(1):114-121. - Kent J.S. et al., "Principles for Maintaining and Increasing Milk Production". G Obstet Ginecol Neoneutal Nurs. 2012;41(1):114-121.
5 Amir L. Breastfeeding managing ‘supply’ difficulties. Aust fam physician . 2006;35(9):686. - - Amir L., "Breastfeeding: problems of 'supply'.