Is tongue tie genetic
Is Tongue-Tied Genetic? A Renowned Dentist Reveals the Truth
Vitamin A deficiency plays a role in oral development and tongue tie. Pre-natal nutrition is a pivotal part of newborn growth and dental development.For a long time in dental practice, I was unaware of what a tongue-tie was. Today, the signs of tongue-tie can sometimes even be predicted by one look at a patient’s face. And the cause of tongue-tie, in my opinion, relates to nutrition.
Tongue-ties are estimated to affect up to 10% of the population. The role of the tongue in early-childhood feeding is key to newborn development. And, yep you guessed it, tongue tie can impair a kid’s dental health.
The exact reason why tongue-ties occur in newborns is still unexplained.
As a focus of my dental practice, I always try to find the root cause of disease. After seeing many kids and adults with tongue-ties a question began to pop up in my head. Can we prevent tongue-ties in newborns?
A tongue-tie is a failure of the lingual frenum to resorb during pre-natal development. Why doesn’t the lingual frenum disappear in some kids?
In this article, we’ll explore why prenatal vitamin A deficiency may cause tongue-ties.
The WHO defines vitamin A deficiency as a global public health problem. At least one-third of kids are affected in developing countries. Vitamin A supplementation is a proven low-cost method against childhood blindness and diarrhea.
Vitamin A is known to be crucial for facial development and eyesight (night time blindness).
Can vitamin A deficiency be the root-cause of tongue-tie?
To explore these factors, we’re going to explore three points:
- Spina bifida is known as a nutritional birth defect, yet the precise mechanism is unknown.
- Cleft palate is a birth defect with links to both tongue-tie and vitamin A
- Vitamin A deficiency and webbed fingers both relate to tongue-tie
I.
 Spina bifida and folic acid deficiency
Spina bifida and folic acid deficiencySpina bifida was one of the first well-known nutritionally linked birth defects.
As the fetus grows, it develops different bodily systems. These include skeletal system, spinal cord, and all of its organs. A growing baby has a lot achieve through in its earliest periods of life.
Neural tube defect is where a newborn is born with a gap in the spine. During development, the neural tube fails to close in the womb.
Fetal development has a strict process that includes checkpoints. Like traffic lights, a growing fetus finishes developing certain parts of the body. Once completed, it moves to the next before moving on to the next.
When the spinal cord develops, it involves the neural tube. It is the embryonic source of the spinal cord, vessels, and bone tissue.
The neural tube should close around 23rd and 27th days of pregnancy. In spina bifida, this fails to happen, and the spinal cord is left open and unfinished.
Folate is a crucial building block of the nervous system. Folate deficiency in mothers is linked to spina bifida risk in newborns. It’s long been accepted that without adequate folate, the body fails to complete the spinal cord. By the 27th week, it must move to the other systems. Without enough folate, the job is left incomplete, and the child with an exposed spinal cord.
Folate deficiency in mothers is linked to spina bifida risk in newborns. It’s long been accepted that without adequate folate, the body fails to complete the spinal cord. By the 27th week, it must move to the other systems. Without enough folate, the job is left incomplete, and the child with an exposed spinal cord.
But spina bifida may not be only be caused by pure lack of raw materials for spinal development.
Does folate deficiency actually cause spina bifida?
In September 1992, the USPHS recommended that all women of childbearing age should take folic acid to prevent neural tube defects.
The relationship between spina bifida and folate seems simple right? Well, it’s more complicated than just folate deficiency.
Studies have since shown that folate deficiency alone doesn’t cause spina bifida. Folate status is linked to neural tube disorder risk. Yet, different people have a greater risk of spina bifida with folate deficiency.
Spina bifida has a genetic component. But studies haven’t found an exact genetic mutation that directly causes spina bifida. For example, mutations that relate to folate metabolism don’t translate to direct risk of spina bifida.
But studies haven’t found an exact genetic mutation that directly causes spina bifida. For example, mutations that relate to folate metabolism don’t translate to direct risk of spina bifida.
Also, the way that folic acid prevents spina bifida isn’t straight forward. Folate deficiency alone is not sufficient to cause a neural tube defect. And kids can be born with spina bifida from mothers in the absence of folic acid deficiency.
Both nutritional and genetic factors all play a role in spina bifida. But other, post gene expression factors seem to influence folate metabolism.
These may include the uptake, storage and use of folate by cells. Spina bifida seems to be a problem utilizing folic acid that has both genetic and environmental components.
Neural tube defect, while related to folate deficiency, has a mechanism that isn’t directly understood.
With this perspective, let’s proceed to look at tongue-tie and vitamin A.
II. Vitamin A deficiency and cleft palate
Cleft lip and palates are birth defects that result in an incomplete top lip or palate.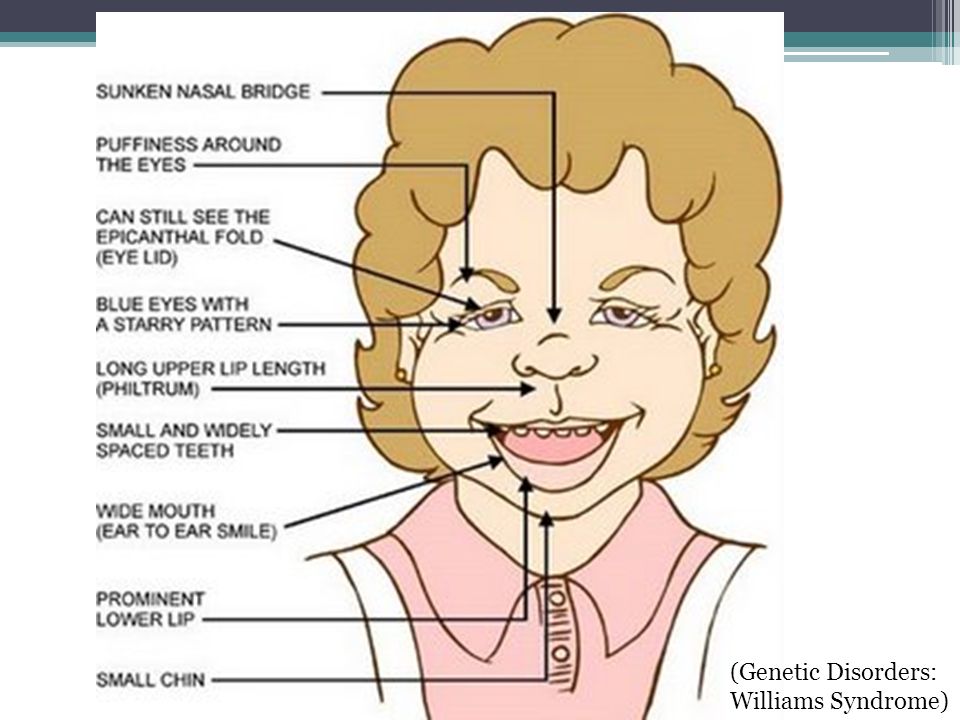 Called orofacial clefts, they share similar characteristics to spina bifida.
Called orofacial clefts, they share similar characteristics to spina bifida.
Studies have found a high proportion of male newborns with cleft palates also presents with tongue tie.
Cleft palate and lip involve the embryonic final touches of the face. It is the face ‘zipping’ up once development has finished. Cleft lip is where the top lip isn’t ‘closed’ and leaves the two sides of the upper lip open.
Both cleft lip and palate are similar to tongue tie as they are at the end of a developmental ‘traffic light.’ The two sides of the face link at the midline of the upper lip and palate. It should become seamless and look like one structure.
Likewise, the tongue develops by the joining two portions that make up the front and back of the tongue. The frenum is ‘eaten away’ so that the front two-thirds of the tongue is free to move.
There is also a genetic component to cleft palate risk. Increased risk for cleft palate is related to MTHFR mutations and folate deficiency. But the links aren’t clear, and the folic acid relationship is far weaker than spina bifida.
But the links aren’t clear, and the folic acid relationship is far weaker than spina bifida.
Cleft lip and palate, similar to spina bifida, involve development using core nutrients. Folic acid doesn’t have the same effect on clefts. But there is a weak association with multi vitamins and prevention of cleft lip.
Vitamin A, on the other hand, has a known role in facial growth and development. Excess vitamin A can produce cleft defects. Conversely, cleft palate is shown to be reduced with intake of vitamin A.
The exact relationship between cleft palate and vitamin A needs to be determined. But like spina bifida, it’s likely that genetic and environmental factors contribute to the risk of cleft palate.
III. Tongue-tie, vitamin A deficiency and webbed fingers syndrome
Webbed fingers are a birth defect known as syndactyly. They bear resemblance to tongue-tie as the flap of skin is not removed between the fingers. Ducks have webbed feet due to a lack of a lysosome to activate cell death to remove webs between digits on feet.
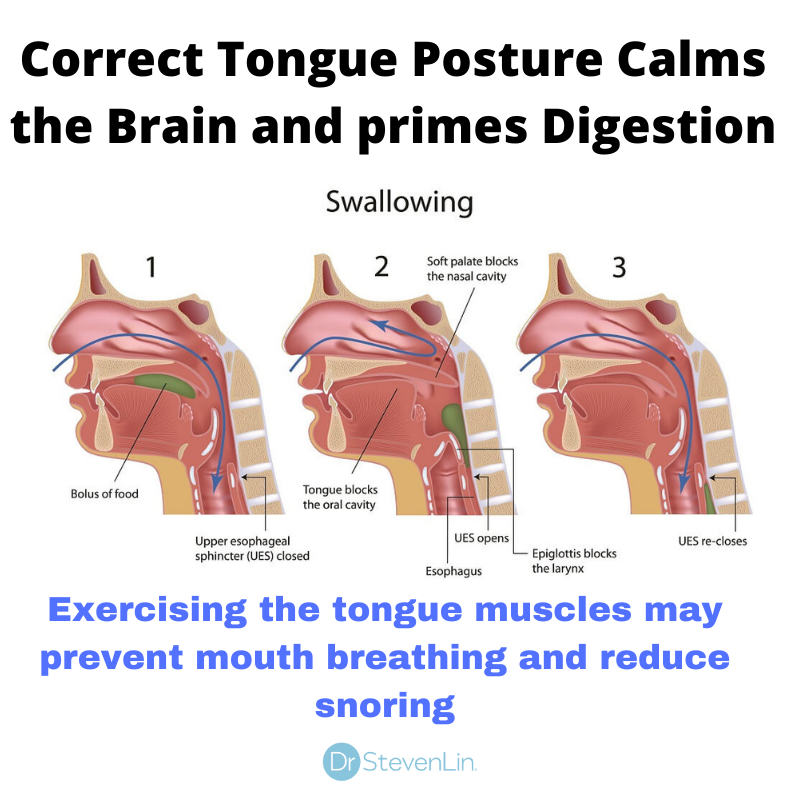
At week 13 in the womb, tongue formation is finalized with the cell death of the lingual frenulum. The step is crucial as it allows the front of the tongue to be free and function for swallowing and speech.
Both genetic and nutritional factors have been found to relate to tongue-ties.
Studies have found an X-linked genetic connection between cleft palates and tongue-tie. MTHFR mutations have also been implicated. But like spina bifida and cleft palate, the exact cause seems to go beyond just genetic mutations.
The role of vitamin A in cleft palate provide another clue as to the cause of tongue-tie.
Like webbed fingers, a tongue-tie is a lack of ‘cell death’ that removes the frenum under the tongue.
Vitamin A is known to activate genes involved in skin apoptosis or cell death. Webbed digits have been related to mice with vitamin A receptor genes mutations. They are also related to eyelid development and eyesight.
Vitamin A and sumoylation (SUMO-1 protein)
Genetic expression of vitamin A is critical for fetal development. Beyond genetic expression, there are post-gene factors that influence vitamin A. The body contains many vitamin A receptors, which are essential for embryonic development.
Beyond genetic expression, there are post-gene factors that influence vitamin A. The body contains many vitamin A receptors, which are essential for embryonic development.
Sumoylation is a process involving a set of proteins called SUMOs. SUMOs help genes transcript the cellular processes after genetic expression. They relate to the cell nucleus and cell cycles. SUMOs are crucial for a healthy pregnancy.
SUMOs describe a set of cellular processes that aren’t purely guided by one gene in particular. For example, SUMO-2 errors may contribute to auto-immune conditions.
Vitamin A and SUMO-1 show interesting connections to tongue-tie.
Retinoic acid (the active form of vitamin A) is crucial for human development. Excess vitamin A can impact left-right symmetry. Synthetic retinoid acid can modify cell apoptosis in cancer cells.
Faulty SUMO-1 proteins have been linked to risk of cleft palate.
In mice, SUMO-1 is also known to control the cell-death process which could link with tongue-tie.
SUMO-1 also influences the body’s use of Vitamin A. There are many different types of retinoic acid receptors (RXRs) that SUMO-1 interact with.
So it’s clear that sumoylation, probably in many ways, helps to direct vitamin A activity. Other studies have shown that SUMO-1 may be affected by inflammation.
Overall vitamin A status may be a risk factor for tongue-tie. But like spina bifida, the process is more complicated than a nutrient deficiency.
Another area of research for vitamin A and tongue tie are the fat-soluble vitamins D and vitamin K2. Both vitamin D and vitamin K2 can influence cell apoptosis that could prevent normal tongue development.
Tongue-tie a nutritional driven birth defect
Tongue-ties are a common birth defect in newborns today.
The purpose of this article was to outline the many inputs that may contribute to tongue-tie. Fetal development is a complex interaction between genes and nutrients.
The interplay between vitamin A and the SUMO-1 protein play vital roles in facial and dental development.
Vitamin A deficiency is a known worldwide epidemic. More studies are needed on vitamin A deficiency and facial development.
If you’re planning a pregnancy, you should consider getting tested for vitamin A levels. You should also eat a diet rich in vitamin A up to six months before conception.
These include foods such as:
- Organ meats
- Oily fish
- Eggs
- Butter, cheese and full cream from grass raised animals
- Carrots *
- Spinach *
*Pro-formed vitamin A which must be converted to pre-formed retinol in the body.
Would you like to eat a diet for better dental health? Get started today by downloading my free EBook.
Do you or any of your family members have a tongue-tie? Leave your questions in the comments below.
For more information on Dr. Lin’s clinical protocol that highlights the steps parents can take to prevent dental problems in their children: Click here.
Want to know more? Dr Steven Lin’s book, The Dental Diet, is available to order today.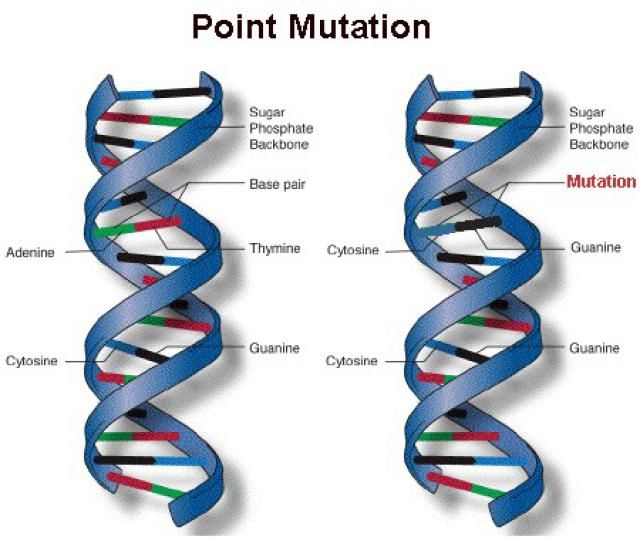 An exploration of ancestral medicine, the human microbiome and epigenetics it’s a complete guide to the mouth-body connection. Take the journey and the 40-day delicious food program for life-changing oral and whole health.
An exploration of ancestral medicine, the human microbiome and epigenetics it’s a complete guide to the mouth-body connection. Take the journey and the 40-day delicious food program for life-changing oral and whole health.
Click below to order your copy now:
US AMAZON
US Barnes & Noble
UK AMAZON
Australia BOOKTOPIA
Canada INDIGO
Tongue Tie: Causes, Symptoms, and Treatments
If you're curious about the causes, symptoms, and treatments of tongue tie syndrome, we've got you covered. Learn more about it here!
Does your baby have trouble latching on to feed?
If so, your baby may be suffering from tongue tie. Although most people will be concerned to hear this, tongue tie can be easily and quickly treated, as long as you get the right help.
Read on to learn all about tongue tie syndrome, it's causes, symptoms and treatments.
What Tongue Tie Is
Tongue tie (also called ankyloglossia) is congenital. This means the child is born with it. Usually, the lingual frenulum will separate before birth. This will give the tongue a free range of movement.
This means the child is born with it. Usually, the lingual frenulum will separate before birth. This will give the tongue a free range of movement.
Tongue tie is when the thin strip of tissue (the lingual frenulum) doesn't separate. Or it can happen when it stays shorter than it should be.
In these instances, the tongue is 'tied' and remains attached to the floor of the mouth. It's not known why this happens, but some cases can link back to certain genetic factors. Tongue tie can cause difficulties when breastfeeding, and issues with speech later on.
Signs and Symptoms
The most common symptom of tongue tie is the inability to breastfeed properly.
To breastfeed, babies need to latch onto the nipple and the breast tissue. For some babies with tongue tie, they cannot open their mouth enough to latch on right. If you're breastfeeding and your baby has tongue tie, they might:
- have difficulty latching on, or staying latched on.
- have issues gaining as much weight as they should, or as fast as they should gain it.
- feed for a lengthy period of time, stop for a short while, then keep feeding.
- make a "clicking" noise when feeding
- seem hungry all the time, and be restless and unsettled.
To protect the mother's nipple from damage, the tongue has to cover the lower gum. If tongue tie stops the baby from doing this, the mother will suffer with:
- recurring mastitis
- cracked and sore nipples
- reduced milk supply
There are other signs of tongue tie you should look out for. These include:
- inability or difficulty lifting their tongue or moving it side to side
- inability or difficult sticking their tongue out
- their tongue goes heart-shaped if they can stick it out.
If you notice any of these signs, you should speak with your GP. Your doctor will be able to diagnose this for you.
Tongue Tie Treatment Procedure — A Step by Step Guide
It's important that you get the issue diagnosed by your doctor. From then on tongue tie treatment is a quick and easy procedure. Here are the steps you'll need to go through:
From then on tongue tie treatment is a quick and easy procedure. Here are the steps you'll need to go through:
- Your specialist will assess your child to make sure the procedure is the right course of action. At Dental Studio 4 Kids, Dr. Denisse offers new moms a free assessment as early as a few days after birth.
- To start, an assistant swaddles the child and puts them in a position that keeps the airways open.
- A laser is a safe, efficient way to release the lingual frenulum. It provides consistent, predictable tissue responses, immediate hemostasis, and quick ablation. It's precise, clear, and bloodless.
- The laser starts beneath the tongue, aiming towards the frenulum. They will avoid the floor of the mouth because it's so delicate.
- Depending on what they need to do to release the tongue, the laser will cut the required tissue. This process usually takes less than a minute.
- The child will have tongue exercises they need to do. This is to reduce the chance of the frenulum reattaching.

FAQ
Here are some common questions and their answers.
Can a Child with Tongue Tie Stick Their Tongue Out?
Yes. Tongue tie may only affect certain motions of the tongue, or it will prohibit all normal motions. It will depend on the individual case. With babies and infants, the most important movement when feeding is up, not out. This is the movement you want to pay attention to.
Must a Child Do Stretches?
Yes. Stretches and tongue exercise are vital in preventing the frenulum reattaching. But, if the tongue tie was just releasing the anterior component, stretches may not matter as much. The wounds in a lip tie or the posterior tongue tie are too close together. Without stretching in these cases, it's likely they will stick back together.
Does Tongue Tie Cause Speech Issues?
Yes. It's most common to find the letters R, S, L, Z, D, CH, TH, and SH affected, but other sounds are difficult too. Some children will be able to sound out these letters in isolation. Tongue tie treatment has been found to improve speech skills in cases where the tongue did not have sufficient freedom of movement.
Tongue tie treatment has been found to improve speech skills in cases where the tongue did not have sufficient freedom of movement.
Will Untreated Tongue Tie Cause More Issues?
Yes. If it remained untreated, tongue tie can cause issues swallowing firmer foods. It can also alter jaw and dental development. This includes a high palate or narrow facial structures.
Those with tongue tie can suffer issues sleeping and breathing through the mouth. There may be an increase in bloating and gas. The tongue isn't coordinating and more air gets into the body through swallowing.
With restricted movement, the tongue cannot swipe across the teeth or spread saliva. These functions are both vital for oral cleaning, so untreated tongue tie may cause dental issues later in life.
What Are the Risks?
No procedure comes without risk, but with a frenectomy they are minor. There is a chance of infection, discomfort, and numbness. There may also be ulceration or restrictive scar tissue. But all these rank as uncommon to rare.
But all these rank as uncommon to rare.
Tongue Tie Doesn't Have to Cause a Panic
As you can see, tongue tie doesn't have to be something to panic about. Immediately speak with your doctor if you notice any of the symptoms, or think something is off.
A quick examination will reveal if the issue is tongue tie or not. And if it is, there is a quick, easy and permanent treatment.
If you're worried about tongue tie, contact us today. At Dental Studio 4 Kids in Lutz, FL we offer pain-free laser surgery tongue tie treatment.
Tongue tie in a child | Description of the disease
Short frenulum of the tongue in a child, or ankyloglossia, is not a disease, but a common physiological feature characterized by insufficient length of the hyoid ligament. However, this feature prevents the free movement of the tongue, makes it difficult for the child to suck on the mother's breast, and later causes problems with speech, the formation of malocclusion, and even the development of certain diseases. nine0005
nine0005
What causes frenulopia?
As a rule, the causes of tongue tie in a child are genetic. This feature is inherited from the father or mother. However, its occurrence may be due to violations of intrauterine development of the fetus.
Risk factors
In addition to hereditary predisposition, factors affecting the formation of a short frenulum of the tongue in a child include:
- negative impact on the embryo at 2-3 months of pregnancy; nine0016
- severe toxicosis in expectant mother;
- viral diseases transmitted by the mother during pregnancy;
- Pregnancy taking strong drugs such as antibiotics.
Symptoms and clinical picture of a child with a short frenulum of the tongue
Parents who are inexperienced or unaware of this pathology may not notice the signs of a short frenulum, usually the problem is detected by nurses and doctors in the maternity hospital. The characteristic manifestations of ankyloglossia are as follows:
- when trying to stick out the tongue, it takes an arched position;
- when the tongue is raised, the frenulum is pulled, as a result of which the body of the organ takes on the shape of a heart;
- The tongue is fixed at the bottom of the mouth and cannot fully "go out".
Since the symptoms of tongue tie in a child are not obvious, therefore, you should pay attention to the following nuances.
In the first year of life there are problems with breastfeeding. The child cannot properly clasp the nipple with his lips, squeezes it excessively with his gums or bites. This leads to malnutrition, hence anxiety and frequent crying. nine0005
Later, malocclusion may occur, with misalignment or initial malocclusion.
Difficulties are also noted at the time of speech formation, the child hardly pronounces hissing and upper articulation sounds, may burr.
At a later age, the described troubles are accompanied by frequent and very painful tears of the shortened ligament.
Methods of diagnosis
Diagnosis of a short frenulum of the tongue in a child is carried out mainly visually, by examining the oral cavity, but can also be based on the described symptoms and history taking. In most cases, the pathology is detected by the medical staff in the maternity hospital.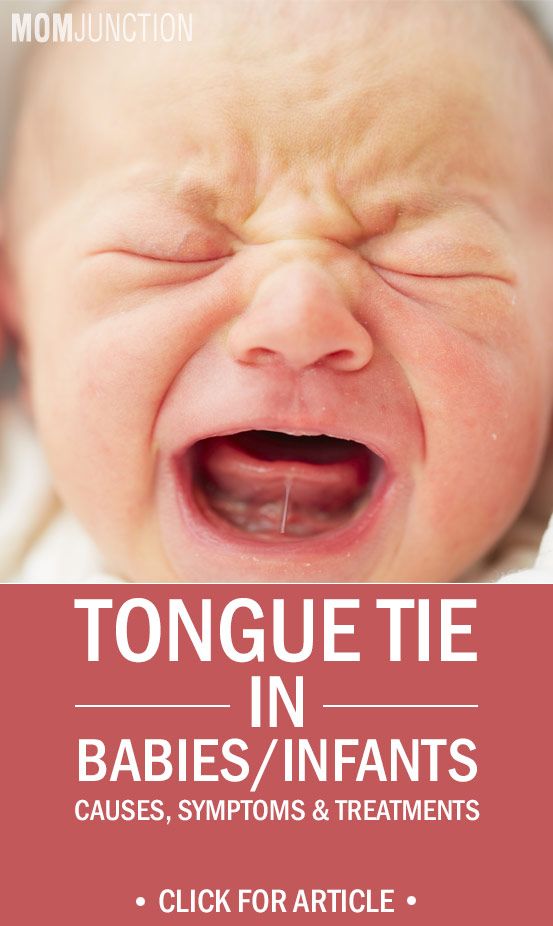 nine0005
nine0005
In an older child, the defect is identified by a specialist. Often, its presence is indicated by functional deviations, for example, the inability to lick lips, pronounce certain words or syllables.
Which doctor treats a frenulum breve?
A child's tongue tie is treated by a neonatologist or pediatric surgeon. However, a pediatrician can notice an anomaly. A dentist, an orthodontist, and in cases of minor deviations in length, even a speech therapist are able to assist in its elimination.
Treatment regimen for a child's tongue tie
The treatment for a child's tongue tie is to cut it, which ensures freedom of movement of the tongue. However, the complexity of this operation depending on age is different.
Main treatments and contraindications
Ideally, frenulum incision should be performed in the first days of a child's life, but there are 2 scenarios.
In infancy, the incision is made by a surgeon using scissors, which is absolutely painless at this stage of life, since there are no nerve endings in this area yet. After this, the baby is applied to the chest in order to calm and prevent the development of bleeding. nine0005
After this, the baby is applied to the chest in order to calm and prevent the development of bleeding. nine0005
How to treat tongue tie in older children? Also, only the operation will be more painful, as the membrane thickens over the years. Frenuloplasty is usually performed - transfer of the fusion site of the frenulum, followed by suturing.
Possible complications
Complications with a short frenulum of the tongue in a child occur when the pathology is ignored. It can be:
- incorrect jaw formation;
- gap between teeth;
- violation of the development of speech and diction;
- excessive salivation;
- gingivitis or periodontitis - inflammatory diseases of the gums;
- snoring;
- apnea.
Tongue frenulum: indications for surgery
Doctor checked the article: Kupriyanova Elena Nikolaevna
Consultation with a specialist:
Types of pathology of the frenulum of the tongue
Different types of ankyloglossia differ from each other in appearance and severity. There are five types of short frenums of the tongue: nine0005
There are five types of short frenums of the tongue: nine0005
-
transparent and thin, shortened sublingual folds, which lead to a slight impairment of mobility;
-
translucent, attached near the tip of the tongue;
-
dense and short folds;
-
soldered to the muscles of the tongue, thickened frenulum;
nine0015
inconspicuous stranded ligaments, the tissues of which are intertwined with muscle fibers.
According to the structure of the frenulum of the tongue can be mucous, fibrous and mixed, muco-fibrous. In the first case, the ligament is elastic and extensible, in the second - dense and elastic. The mixed type is characterized by density and extensibility of an average degree.
Call now
+7 (495) 215-56-90
Make an appointment with a dental surgeon
Causes of tongue frenulum pathology
The main cause of ankyloglossia is a genetic predisposition. About half of the cases are due to the inheritance of pathology from the mother or father.
About half of the cases are due to the inheritance of pathology from the mother or father.
Also, a short frenulum of the tongue can form as a result of adverse effects on the fetus during the first months of pregnancy. Factors that can lead to ankyloglossia include: nine0005
-
severe toxicosis;
-
viral diseases transferred to a pregnant woman;
-
taking certain medications: salicylates, certain groups of antibiotics;
-
contact with industrial hazards: paints and varnishes, chemical reagents, etc.;
nine0016 -
stress.
It is also noted that the likelihood of developing a short frenulum of the tongue in a child is higher at birth by a mother over 40 years old. It is possible that ankyloglossia may have other causes not yet identified by scientists.
Symptoms of the pathology of the frenulum of the tongue
Get expert advice:
- Dental surgeon
 The severity of the consequences depends on such features of the frenulum as its size, junction with the tongue and density.
The severity of the consequences depends on such features of the frenulum as its size, junction with the tongue and density. The first signs of pathology, as a rule, appear already in the first week of life. A short frenulum of the tongue in a newborn interferes with proper latch on of the breast, as a result of which the child constantly “loses” it during feeding. Wasting the pitchfork, the child often gets tired quickly and does not have time to get the right amount of milk. The result of malnutrition is poor weight gain, underweight. nine0005
Often, children with a short hyoid frenulum try to compensate for this violation by using lips and gums to capture the chest. The process of feeding becomes long and tiring, moreover, improper attachment provokes injury to the nipples, the formation of cracks on their surface. Since the baby does not suck out enough milk, then it is produced less than necessary for saturation. All these circumstances usually force mothers to transfer babies to mixed or completely artificial feeding. nine0005
nine0005
However, in some cases, a short frenulum of the tongue does not interfere with normal breastfeeding. Pathology may go unnoticed in infancy, but make itself felt during the development of speech. Due to the restriction of tongue movements, children cannot pronounce the letters "r" and "l", and sometimes some of the others. The child has difficulties in communication, as his speech is difficult for others to perceive.
A short frenulum under the tongue can cause the child to develop the following dental pathologies: nine0005
-
open bite, which is characterized by the absence of contact between the upper and lower frontal teeth when trying to close them;
-
prognathia - a pronounced displacement of the upper jaw forward in relation to the lower;
-
displacement of the dentition;
-
predisposition to the development of inflammatory diseases of the oral cavity; nine0005
-
increased sensitivity of teeth to various irritants.

If the necessary actions are not taken to treat the pathology, a short frenulum of the tongue in an adult becomes the cause of even more serious problems. Over time, a noticeable external defect is formed - the tip of the tongue in the shape of the letter V. During speech, increased salivation is observed. Patients are concerned about snoring and sleep apnea - episodes of respiratory arrest lasting no less than ten seconds. Sometimes ruptures are possible, which are accompanied by pain in the sublingual region and light bleeding. Also, the short frenulum of the tongue is more prone to the development of inflammation. nine0005
Cosmetic defects and speech disorders caused by ankyloglossia can cause self-doubt, neuroses and other psychological problems. In this regard, it is extremely important to timely identify and eliminate the defect at an early age.
Diagnosis of the pathology of the frenulum of the tongue
Usually the problem is detected in infancy or early childhood. Not only a pediatrician, but also a pediatric surgeon, speech therapist, dentist, otorhinolaryngologist can diagnose a short frenulum under the tongue of a child. nine0005
Not only a pediatrician, but also a pediatric surgeon, speech therapist, dentist, otorhinolaryngologist can diagnose a short frenulum under the tongue of a child. nine0005
During the examination of the newborn, the neonatologist pays attention to the structure of the hyoid fold. If the problem is not detected during routine examinations and during breastfeeding, then attentive parents can, even before the formation of speech begins, note that the child cannot lick his lips, fully stick out his tongue.
To diagnose frenulum pathology, doctors can use a special Alison Hazel Baker test. It includes parameters for assessing the appearance of the hyoid fold and the functionality of the tongue. For each of the points, a certain number of points is awarded: from 0 to 2. Summing up the results, the doctor concludes that the patient has or does not have this pathology, as well as the expediency of the operation. nine0005
Treatment of pathology of the frenulum of the tongue
A slight shortening of the hyoid fold in the vast majority of cases can be compensated for with regular sessions with a speech therapist. With the help of speech therapy massage, techniques of articulatory gymnastics, the frenulum is stretched and the sound pronunciation is normalized.
With the help of speech therapy massage, techniques of articulatory gymnastics, the frenulum is stretched and the sound pronunciation is normalized.
Indications for surgical treatment of infants are difficulties during breastfeeding. Older children will definitely need surgery for malocclusion, displacement of teeth. For the treatment of pathology, the following operations can be performed: nine0005
-
Frenulotomy - dissection, or cutting, of the frenulum. During the intervention, the surgeon performs a transverse incision, tightens it and sutures it.
-
Frenuloectomy - excision, removal of the frenulum.
-
Frenuloplasty. It is a movement of the place of attachment of the hyoid ligament to the tongue.
It is best to cut a short frenulum under the child's tongue even during the neonatal period, in the maternity hospital. In order to eliminate postoperative bleeding, the child is applied to the mother's breast. Frenulotomy is possible for babies up to 8-9 months. Further, as they grow older, the frenulum becomes more dense and frenuloplasty is necessary to eliminate the defect.
Frenulotomy is possible for babies up to 8-9 months. Further, as they grow older, the frenulum becomes more dense and frenuloplasty is necessary to eliminate the defect.
The choice of the method of anesthesia is made taking into account the age of the child, the state of health and the degree of mental maturity. Newborn intervention is performed without anesthesia. At an older age, local anesthesia is used. For children with increased emotional lability, general anesthesia may be required. nine0005
Preschoolers and schoolchildren after surgery need to undergo a rehabilitation course. Speech therapy classes, as well as the implementation of a complex of myogymnastics aimed at preventing cicatricial complications, will help the child to form the correct speech skills. To restore a normal bite, treatment by an orthodontist will be required.
Prevention of tongue frenulum pathology
To avoid the development of a birth defect associated with the action of harmful factors, following certain rules will help.